It’s important to talk with your health care provider about side effects you are experiencing and any concerns you have.
Credit: iStock
Stomach cancer and its treatments may cause physical and emotional side effects. When you first learn that you have stomach cancer, you may wonder how you’re going to cope with the upcoming changes in your life. One step you can take is to be informed of the changes that may occur and what resources are available to help you. Speaking up about any problems you have can give you a greater sense of control. Your health care team can talk with you about ways to reduce these side effects so you feel better.
Stomach cancer and its treatments may affect your ability to eat enough food or absorb the nutrients from food. If part or all of your stomach has been removed, you might need to eat smaller amounts of food more often or make changes to what you eat. Your doctor or dietitian may recommend that you stay upright for some time after eating. They can also help you adjust your diet to make sure you get the nutrition you need.
Stomach cancer and its treatment can change how you look and feel about yourself. Know that you aren’t alone in how you feel. Coping with changes to your body and the way you see yourself can be hard. But, over time, many people learn to adjust and move forward.
Many people who have been treated for stomach cancer need to visit their doctor regularly to get follow-up exams or tests. Planning and scheduling these appointments can be stressful and time-consuming. Waiting for test results can cause anxiety and an ongoing fear of recurrence. The added costs of things such as copays, medicines, and parking and transportation fees only add to the stress. For tips on how to deal with the fear of cancer coming back, see the section Coping with Fear of Recurrence on our A New Normal page.
Cancer is one of the most costly diseases to treat in the United States. Even if you have health insurance, you may face major financial challenges and need help dealing with the costs of stomach cancer treatment. The problems a person has related to the cost of treatment is known as financial toxicity. For tips and ways to cope, see Managing Cancer Costs and Medical Information. To learn about financial toxicity and find out if you are at risk, see Financial Toxicity (Financial Distress) and Cancer Treatment.
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. It is important to know the stage of the stomach cancer to plan the best treatment.
There are several staging systems for cancer that describe the extent of the cancer. Stomach cancer staging usually uses the TNM staging system. You may see your cancer described by this staging system in your pathology report. Based on the TNM results, a stage (I, II, III, or IV, also written as 1, 2, 3, or 4) is assigned to your cancer. When talking to you about your cancer, your doctor may describe it as one of these stages.
For information about how doctors stage stomach cancer, see the tests to stage stomach cancer section on Stomach Cancer Diagnosis. Learn more about Cancer Staging.
The information on this page is about staging for adenocarcinoma of the stomach, the most common type of stomach cancer.
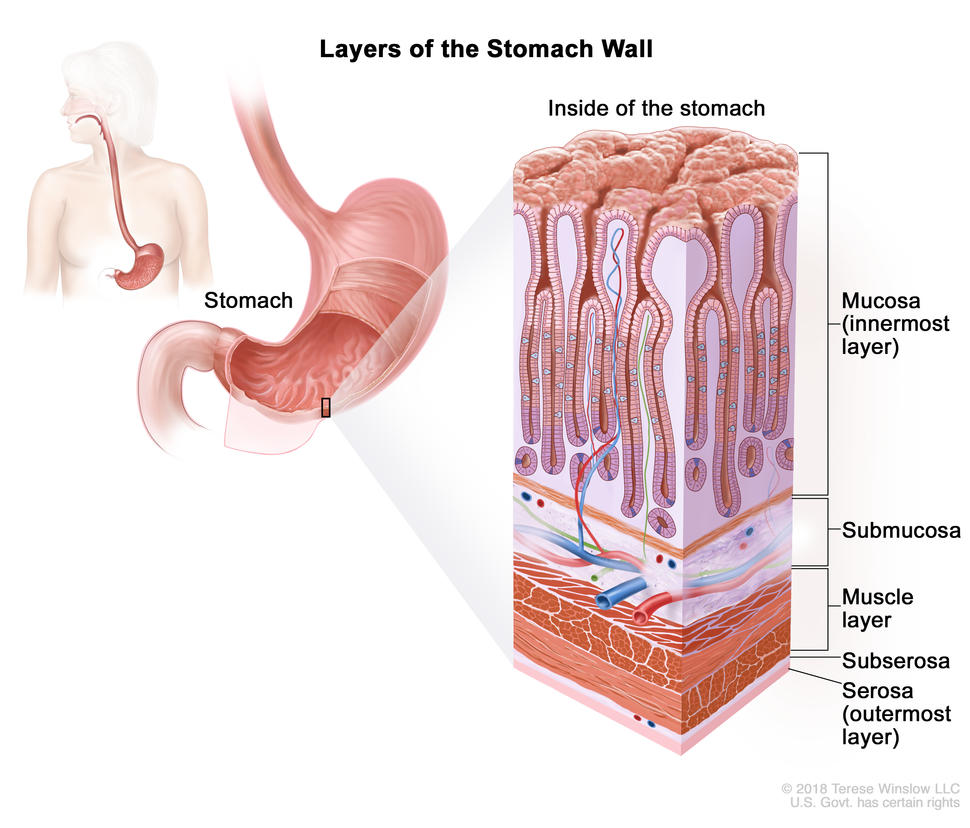
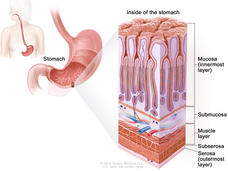
Layers of the stomach wall
The stomach wall is made up of five layers of tissue and muscle. Knowing about these layers can help you understand the stage of your cancer.
Layers of the stomach wall. The wall of the stomach is made up of the mucosa (innermost layer), submucosa, muscle layer, subserosa, and serosa (outermost layer). The stomach is an organ in the upper abdomen.
The mucosa is the innermost layer of the stomach wall. It is made of both epithelial cells and glandular cells. The glandular cells make mucus to protect the stomach lining and digestive juices to help break down food. Most stomach cancers start in glandular cells of the mucosa. Cancers that start in glandular cells are adenocarcinomas.
The muscle layer is the next layer. The muscle layer helps the stomach mix food with digestive juices and move it into the small intestine, where nutrients are absorbed.
The subserosa is a thin layer of connective tissue between the muscle layer and the serosa.
The serosa is the outermost layer of the stomach wall.
Stomach cancers become more advanced as they spread from the mucosa to the outer layers.
Stage 0 refers to carcinoma in situ. This means that abnormal cells are found in the mucosa. These abnormal cells may become cancer and spread into nearby normal tissue.
cancer may have spread to the submucosa or to the muscle layer and has spread to 16 or more nearby lymph nodes; or
cancer has spread to the subserosa or to the serosa and has spread to 7 to 15 nearby lymph nodes; or
cancer has spread to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer has also spread to 1 to 6 nearby lymph nodes.
In stage IIIC,
cancer has spread to the subserosa or to the serosa, and to 16 or more nearby lymph nodes; or
cancer has spread to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer also has spread to 7 or more nearby lymph nodes.
In stage IV, cancer has spread to other parts of the body, such as the lungs, liver, distant lymph nodes, and the tissue that lines the abdomen wall.
Stage IV stomach cancer is also called metastatic stomach cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if stomach cancer spreads to the lung, the cancer cells in the lung are actually stomach cancer cells. The disease is called metastatic stomach cancer, not lung cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
Recurrent stomach cancer is cancer that has recurred (come back) after it has been treated. Stomach cancer may come back in the stomach, lymph nodes, or other parts of the body, such as the liver, lung, or bone. Tests will be done to help determine where the cancer has returned in your body. The type of treatment that you have for recurrent stomach cancer will depend on where it has come back.
Different types of treatments are available for stomach cancer. You and your cancer care team will work together to decide your treatment plan, which may include more than one type of treatment. Many factors will be considered, such as the stage of the cancer, your overall health, and your preferences. Your plan will include information about your cancer, the goals of treatment, your treatment options and the possible side effects, and the expected length of treatment.
Talking with your cancer care team before treatment begins about what to expect will be helpful. You’ll want to learn what you need to do before treatment begins, how you’ll feel while going through it, and what kind of help you will need. To learn more, see Questions to Ask Your Doctor about Your Treatment.
Endoscopic mucosal resection is a procedure that uses an endoscope to remove carcinoma in situ and early-stage cancer from the lining of the digestive tract. An endoscope is a thin, tube-like instrument with a light and a lens and tools to remove tissue.
Surgery
Surgery is a common treatment for stomach cancer. The type of surgery depends on where the cancer is located.
Other treatments may be given in addition to surgery:
Treatment given before surgery is called preoperative therapy or neoadjuvant therapy. Chemotherapy may be given before surgery to shrink the tumor and reduce the amount of tissue that needs to be removed during surgery. Chemoradiation given before surgery, to shrink the tumor, is being studied.
Treatment given after surgery, to lower the risk that the cancer will come back, is called adjuvant therapy. After the doctor removes all the cancer that can be seen, some patients may be given chemotherapy, radiation therapy, or both to kill any cancer cells that are left.
Gastrectomy, the removal of part or all of the stomach, is the main surgery for stomach cancer:
Subtotal gastrectomy is the removal of the part of the stomach that contains cancer, nearby lymph nodes, and parts of other tissues and organs near the tumor. The spleen may also be removed.
Total gastrectomy is the removal of the entire stomach, nearby lymph nodes, and parts of the esophagus, small intestine, and other tissues near the tumor. The spleen may also be removed. Then the surgeon attaches the esophagus to the small intestine so the patient can continue to eat and swallow.
Endoluminal stent placement
Endoluminal stent placement may be done when the tumor blocks the passage into or out of the stomach. In this procedure, the surgeon places a stent (a thin, expandable tube) from the esophagus to the stomach or from the stomach to the small intestine to allow the patient to eat normally.
Endoluminal laser therapy
Endoluminal laser therapy is a procedure in which an endoscope (a thin, lighted tube) with a laser attached is used as a knife to open a gastrointestinal blockage.
Gastrojejunostomy
Gastrojejunostomy is the removal of the part of the stomach with cancer that is blocking the opening into the small intestine. Then the surgeon connects the stomach to the jejunum (a part of the small intestine) to allow food and medicine to pass from the stomach into the small intestine.
Radiation therapy
Radiation therapy uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. Stomach cancer is sometimes treated with external radiation therapy. This type of radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Chemotherapy (also called chemo) uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing.
Chemotherapy for stomach cancer is usually systemic, meaning it is injected into a vein or given by mouth. When given this way, the drugs enter the bloodstream to reach cancer cells throughout the body.
Chemotherapy drugs used to treat stomach cancer include
Targeted therapy uses drugs or other substances to identify and attack specific cancer cells. Your doctor may suggest biomarker tests to help predict your response to certain targeted therapy drugs. Learn more about Biomarker Testing for Cancer.
Targeted therapies used to treat stomach cancer include
Immunotherapy helps a person’s immune system fight cancer. Your doctor may suggest biomarker tests to help predict your response to certain immunotherapy drugs. Learn more about Biomarker Testing for Cancer.
Immunotherapy drugs used to treat stomach cancer include
These drugs work in more than one way to kill cancer cells. They are also considered targeted therapy because they target specific changes or substances in cancer cells.
Regional chemotherapy is a method of placing chemotherapy directly into an organ or a body cavity, such as the abdomen, to mainly affect cancer cells in those areas.
A type of regional chemotherapy called hyperthermic intraperitoneal chemotherapy, or hot chemotherapy, is being studied to treat stomach cancer and may be offered at certain treatment centers. After the surgeon has removed as much of the cancer as possible during surgery, a chemotherapy drug, such as mitomycin or cisplatin, is warmed and pumped directly into the peritoneal cavity through a thin tube for about 2 hours. The surgeon then drains the chemotherapy from the abdomen and rinses the abdomen before closing the incision.
Clinical trials
A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. For some patients, taking part in a clinical trial may be an option.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Get live help finding a clinical trial at 1-800-4-CANCER. NCI offers free information on cancer topics in English and Spanish.
Follow-up testing
Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests. These tests are sometimes called follow-up tests or check-ups.
You may also have blood tests for tumor markers such as CEA and CA 19-9. Increased levels of these markers may mean your stomach cancer has come back. Learn more about Tumor Markers.
Chemotherapy works by killing fast-growing cancer cells and is one method used to treat stomach cancer.
Credit: iStock
Cancer stage is an important factor in deciding the best treatment for stomach cancer. Other factors, such as your preferences and overall health, are also important.
For some people, taking part in a clinical trial may be an option. Clinical trials of new cancer drugs or treatment combinations may be available. To learn more about clinical trials, including how to find and join a trial, see Clinical Trials Information for Patients and Caregivers.
Treatment of stage 0 stomach cancer (carcinoma in situ)
Gastrectomy (surgery to remove all or part of the stomach and nearby lymph nodes) is the main treatment for stage 0 stomach cancer (carcinoma in situ).
Endoscopic mucosal resection uses an endoscope to remove abnormal growths or tissue from the lining of the digestive tract without open surgery. It may be done in people with small tumors that have a low risk of spreading to nearby lymph nodes.
Gastrectomy (surgery to remove all or part of the stomach and nearby lymph nodes) is the main treatment for stage I stomach cancer. Some people may receive chemotherapy and/or radiation therapy before or after surgery. Giving chemotherapy at the same time as radiation therapy may help the radiation therapy work better.
Endoscopic mucosal resection is a less invasive procedure that may be used in people with small tumors that have a low risk of spreading to nearby lymph nodes.
Gastrectomy (surgery to remove all or part of the stomach and nearby lymph nodes) is the main treatment for stage II stomach cancer and stage III stomach cancer. Some people may receive chemotherapy and/or radiation therapy before or after surgery. Giving chemotherapy at the same time as radiation therapy may help the radiation therapy work better.
There are many chemotherapy drugs used for stage II and stage III stomach cancer, including capecitabine, cisplatin, docetaxel, epirubicin, fluorouracil (5-FU), leucovorin, and oxaliplatin. These drugs may be given alone or in combination.
Treatment of stage IV stomach cancer, stomach cancer that cannot be removed by surgery, and recurrent stomach cancer
Treatment of stage IV stomach cancer, any stage of stomach cancer that cannot be removed by surgery, and recurrent stomach cancer is palliative. Palliative therapy is treatment meant to improve the quality of life of people who have a serious or life-threatening disease, such as cancer. Many of the same treatments for cancer, such as chemotherapy or other kinds of drugs and radiation therapy, can also be used for palliative therapy to help a patient feel more comfortable. Learn more about Palliative Care in Cancer.
There are many chemotherapy drugs used as palliative therapy for advanced stomach cancer, including capecitabine, cisplatin, docetaxel, doxorubicin, epirubicin, etoposide, fluorouracil (5-FU), irinotecan, leucovorin, oxaliplatin, paclitaxel, and trifluridine and tipiracil. These drugs may be given alone or in combination.
A specific way of giving chemotherapy called hyperthermic intraperitoneal chemotherapy, or HIPEC, may be an option at some treatment centers. This treatment uses warmed chemotherapy to wash the inside of the abdomen during surgery.
If you have side effects from the cancer or its treatment, you may be given other treatments to help reduce those side effects so you are more comfortable. For example, if you have a blockage in your stomach, you may receive endoluminallaser therapy or endoluminal stent placement to relieve the blockage or a gastrojejunostomy to bypass the blockage. Radiation therapy or surgery may be done to stop bleeding, relieve pain, or shrink a tumor that is blocking the stomach.
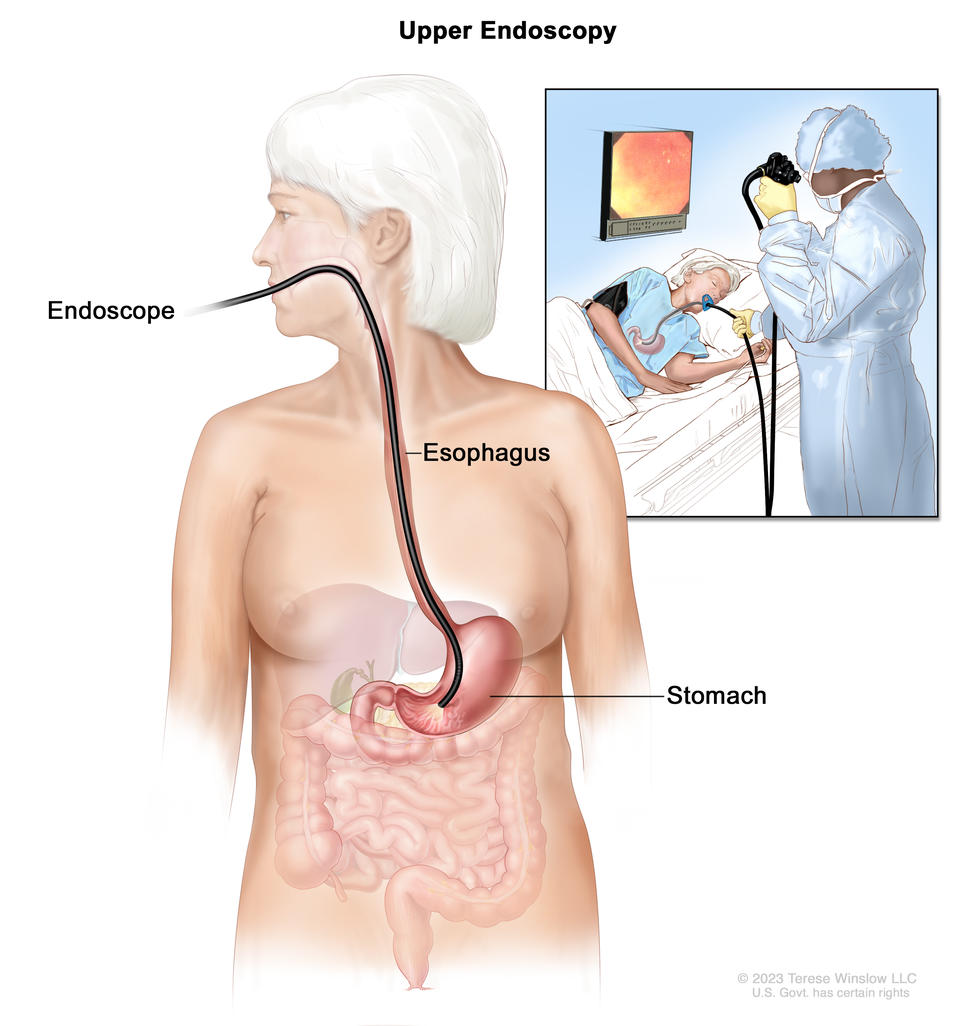
Upper endoscopy. A thin, lighted tube called an endoscope is inserted through the mouth and down the throat to check for abnormal areas in the esophagus, stomach, and first part of the small intestine.
Upper endoscopy is a procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope (a thin, lighted tube) is passed through the mouth and down the throat into the esophagus. It may also have a tool to remove a sample of cells or tissue (biopsy) so a pathologist can view it under a microscope to check for signs of cancer.
The sample of tissue may be checked for Helicobacter pylori (H. pylori) infection and used for biomarker testing.
Talk with your doctor to learn what to expect during and after your biopsy.
To learn about the type of information that can be found in a pathologist’s report about the cells or tissue removed during a biopsy, see Pathology Reports.
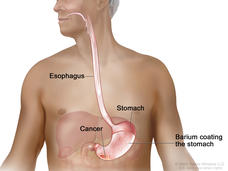
Barium swallow
Barium swallow is a series of x-rays of the esophagus and stomach. The patient drinks a liquid that contains barium (a silver-white metallic compound). The liquid coats the esophagus and stomach, and x-rays are taken. This procedure is also called an upper GI series.
CT (CAT) scan
A CT scan uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography. To learn more, see Computed Tomography (CT) Scans and Cancer.
Biomarker testing
Biomarker testing is a way to look for genes, proteins, and other substances (called biomarkers or tumor markers) that can provide information about cancer. Some biomarkers affect how certain cancer treatments work. Biomarker testing may help you and your doctor choose a cancer treatment for you.
To check for these biomarkers, samples of tissue containing stomach cancer cells are removed during a biopsy or surgery. The samples are tested in a laboratory to see whether the stomach cancer cells have these biomarkers.
For stomach cancer, biomarker testing includes the following:
HER2: The cancer cells may have larger than normal amounts of a protein called HER2.
Microsatellite instability: The cells may have microsatellite instability. This may be caused by mistakes that don’t get corrected when DNA is copied in a cell.
Find information about a specific stage of stomach cancer, a factor that affects treatment.
If you’re diagnosed with stomach cancer, you will be referred to a gastrointestinal oncologist. This is a doctor who specializes in diagnosing and treating cancers of the stomach and intestines. Your doctor will recommend tests to find out if the cancer has spread and if so, how far. Sometimes the cancer is only in the stomach. Or, it may have spread from the stomach to other parts of the body. The process of learning the extent of cancer in the body is called staging. It is important to know the stage of the stomach cancer to plan treatment.
The following imaging tests and procedures may be used to find out your stage:
Endoscopic ultrasound is a procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
PET-CT scan combines the pictures from a positron emission tomography (PET) scan and a computed tomography (CT) scan. The PET and CT scans are done at the same time on the same machine. The pictures from both scans are combined to make a more detailed picture than either test would make by itself.
For the PET scan, a small amount of radioactive glucose is injected into a vein. The scanner rotates around the body and makes a picture of where glucose is being used in the body. Cancer cells show up brighter in the picture because they are more active and take up more glucose than normal cells.
For the CT scan, a series of detailed x-ray pictures of areas inside the body is taken from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly.
Magnetic resonance imaging (MRI) with gadolinium is a procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Laparoscopy is a surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of cancer. A solution may be washed over the surface of the organs in the abdomen and then removed to collect cells. These cells are also looked at under a microscope to check for signs of cancer.
Getting a second opinion
You may want to get a second opinion to confirm your stomach cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get important medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans before giving a recommendation. The doctor who gives the second opinion may agree with your first doctor, suggest changes or another approach, or provide more information about your cancer.
Get live help with finding a doctor, hospital, or getting a second opinion at 1-800-4-CANCER. NCI offers free information on cancer topics in English and Spanish.
Screening is looking for cancer before a person has any symptoms. This can help detect cancer at an early stage. When abnormaltissue or cancer is found early, it may be easier to treat.
In the United States, there are no standard or routine screening tests to detect stomach cancer in people at average risk. Researchers are working to develop such tests. If a test reduces the number of deaths from stomach cancer, it may become a standard screening test.
Upper endoscopy. A thin, lighted tube called an endoscope is inserted through the mouth and down the throat to check for abnormal areas in the esophagus, stomach, and first part of the small intestine.
Upper endoscopy is a procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope is passed through the mouth and down the throat into the esophagus. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue, which is checked under a microscope for signs of disease.
Risks of stomach cancer screening
Talk with your doctor about whether stomach cancer screening is right for you.
Potential risks of stomach cancer screening include:
False-negative test results. Screening test results may appear to be normal even though stomach cancer is present. A person who receives a false-negative test result (one that shows there is no cancer when there really is) may delay seeking medical care even if there are symptoms.
False-positive test results. Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn’t) can cause anxiety and is usually followed by more tests and procedures which also have risks.
Risks of the screening test itself. Upper endoscopy may cause the following rare, but serious, complications:
a small hole (puncture) in the esophagus or stomach
heart problems
breathing problems
lung infection from inhaling food, fluid, or stomach acid into the lung
severe bleeding that needs to be treated at a hospital
Stomach pain or discomfort can be a symptom of stomach cancer.
Credit: iStock
Early on, stomach cancer usually doesn’t have symptoms, making it hard to detect. Symptoms usually begin after the cancer has spread.
When symptoms of early-stage stomach cancer do occur, they may include
indigestion and stomach discomfort
a bloated feeling after eating
mild nausea
loss of appetite
heartburn
Symptoms of advanced stomach cancer (cancer has spread beyond the stomach to other parts of the body) may include the symptoms of early-stage stomach cancer and
These symptoms may be caused by many conditions other than stomach cancer. It’s important to check with your doctor if you have any of these symptoms. Your doctor will ask when your symptoms started and how often you’ve been having them. If it is stomach cancer, ignoring symptoms can delay treatment and make it less effective.
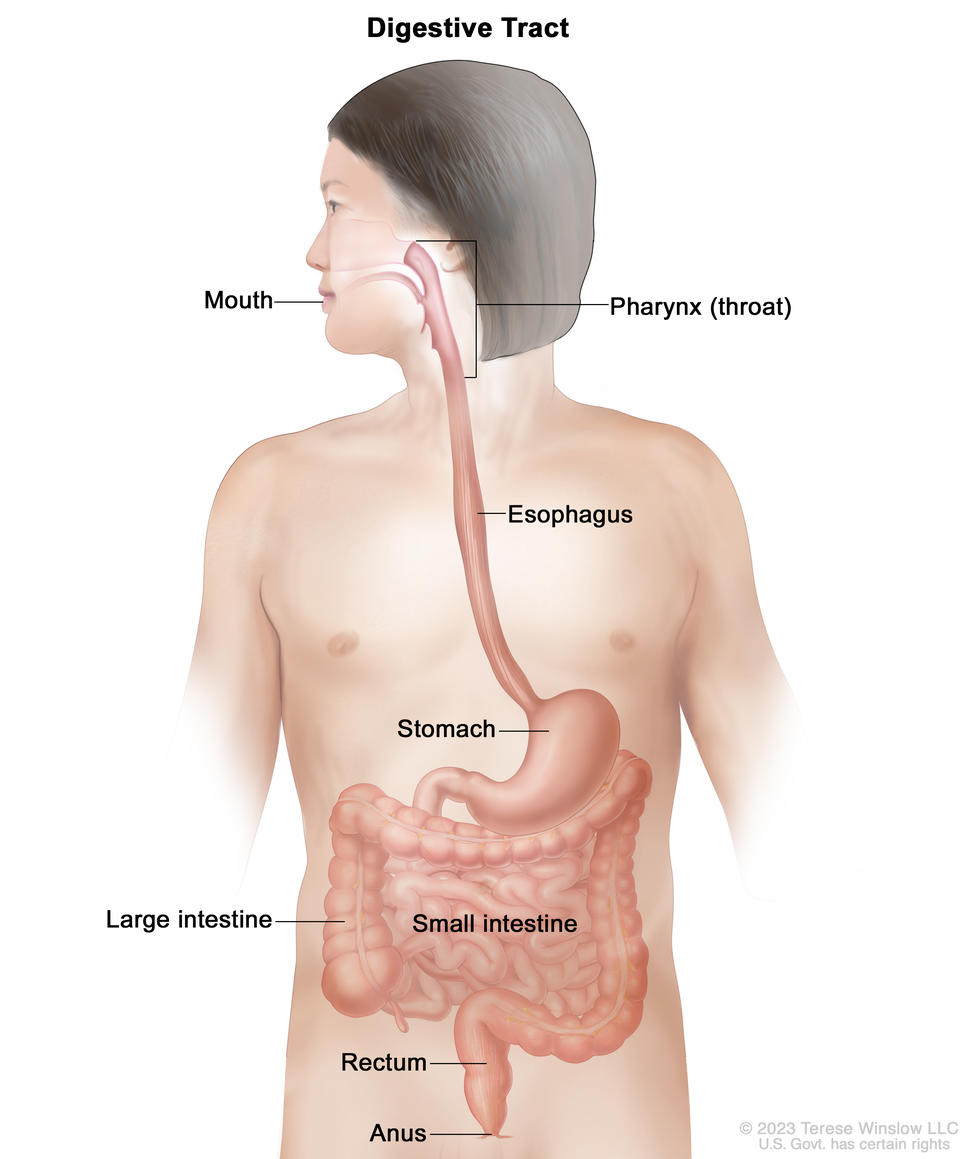
Anatomy of the digestive tract. The digestive tract is made up of organs that food and liquids travel through when they are swallowed, digested, absorbed, and leave the body as feces. These organs include the mouth, pharynx (throat), esophagus, stomach, small intestine, large intestine, rectum, and anus.
Stomach (gastric) cancer is cancer that starts in the cells lining the stomach. The stomach is an organ on the left side of the upper abdomen that digests food. The stomach is part of the digestive tract, a series of hollow, muscular organs joined in a long, twisting tube from the mouth to the anus. The digestive tract processes nutrients in foods that are eaten and helps pass waste material out of the body:
Food moves from the throat to the stomach through a tube called the esophagus.
After food enters the stomach, it is broken down by stomach muscles that mix the food and liquid with digestive juices.
The end of the large intestine, called the rectum, stores the waste from the digested food until it is pushed out of the anus during a bowel movement.
Types of stomach cancer
Adenocarcinoma of the stomach begins in the mucus-producing cells in the innermost lining of the stomach. Nearly all stomach cancers are adenocarcinomas.
Adenocarcinoma of the stomach is divided into two main classes, depending on where it forms in the stomach:
Gastric cardia cancer begins in the top inch of the stomach, just below where it meets the esophagus.
Non-cardia gastric cancer is cancer that begins in all other sections of the stomach.
Adenocarcinoma of the stomach also may be described as intestinal or diffuse, depending on how the cells look under a microscope:
Intestinal adenocarcinomas are well differentiated, meaning the cancer cells look similar to normal cells under a microscope.
Diffuse adenocarcinomas are undifferentiated or poorly differentiated, meaning the cancer cells look different from normal cells under a microscope. Diffuse adenocarcinomas tend to grow and spread more quickly than the intestinal type and be harder to treat.
Gastroesophageal junction adenocarcinoma (GEJ) is a cancer that forms in the area where the esophagus meets the gastric cardia. GEJ may be treated similarly to stomach cancer or esophageal cancer.
Gastrointestinal neuroendocrine tumors are cancers that begin in neuroendocrine cells (a type of cell that is like a nerve cell and a hormone-making cell) that line the gastrointestinal tract. Neuroendocrine cells make hormones that help control digestive juices and the muscles used in moving food through the stomach and intestines. Learn about gastrointestinal neuroendocrine tumors.
Gastrointestinal stromal tumors (GIST) begin in nerve cells that are found in the wall of the stomach and other digestive organs. GIST is a type of soft tissue sarcoma. Learn about gastrointestinal stromal tumors.
Primary gastric lymphoma is a type of non-Hodgkin lymphoma that forms in the stomach. Most primary gastric lymphomas are either mucosa-associated lymphoid tissue (MALT) gastric lymphoma or diffuse large B-cell lymphoma of the stomach.
Symptoms of stomach cancer may include common conditions like indigestion and stomach pain. Learn more to recognize early and advanced stomach cancer symptoms.
Stage refers to the extent of your cancer, such as how large the tumor is and if it has spread. Learn about stomach cancer stages, an important factor in deciding your treatment plan.
Stomach cancer treatments can include surgery, radiation therapy, chemotherapy, immunotherapy, and more. Learn about the different ways stomach cancer can be treated.
Certain aspects of stomach cancer diagnosis and treatment are of special concern. Gain a greater sense of control by knowing what to expect and what resources are available to help you cope.
Stomach cancer is caused by certain changes to the way stomach cells function, especially how they grow and divide into new cells. There are many risk factors for stomach cancer, but many do not directly cause cancer. Instead, they increase the chance of DNA damage in cells that may lead to stomach cancer. To learn more about how cancer develops, see What Is Cancer?.
A risk factor is anything that increases the chance of getting a disease. Some risk factors for stomach cancer, like tobacco use, can be changed. However, risk factors also include things people cannot change, like their age and family history. Learning about risk factors for stomach cancer is important because it can help you make choices that might prevent or lower your risk of getting it.
Who gets stomach cancer
Stomach cancer is the fifth most common cancer worldwide. It is more common in countries in East Asia, Eastern Europe, and South and Central America than in the United States and other Western countries.
Anyone can get stomach cancer. In the United States, the disease occurs more often among Black, Hispanic, Asian/Pacific Islander, and American Indian/Alaska Native individuals than among White individuals. Males are nearly twice as likely as females to be diagnosed with stomach cancer, and Black males are nearly twice as likely as White males to die of it. In recent years, stomach cancer rates have been increasing in younger females, particularly among Hispanic females. Stomach cancer can be diagnosed at any age, but the risk increases as a person gets older.
Risk factors for stomach cancer
There are several risk factors for stomach cancer. Different risk factors may increase the risk of cancer in different parts of the stomach. For example, Helicobacter pylori(H. pylori)infection increases the risk of cancer in the lower and middle part of the stomach, while obesity and gastroesophageal reflux disease (GERD) increase the risk of cancer in the upper stomach.
Chronic infection of the mucosal layer of the stomach with H. pylori is a major risk factor for stomach cancer. This bacterium spreads from person to person through direct contact with saliva, vomit, or stool. Although many people with chronic H. pylori infections do not have symptoms, some develop stomach ulcers or an inflammation of the stomach called atrophic gastritis. In some people, atrophic gastritis leads to increasingly severe changes in the stomach lining and eventually to stomach cancer or gastric MALT lymphoma (see What Is Stomach Cancer?). Treatment of H. pylori infections reduces the risk of these types of stomach cancer.
Other medical conditions
The risk of stomach cancer is increased in people who have
chronic atrophic gastritis (thinning of the stomach lining caused by long-term inflammation of the stomach)
atrophic gastritis with intestinal metaplasia (a condition in which the cells that line the stomach are replaced by cells that normally line the intestines)
Eating a diet that is low in fruits and vegetables or that is high in salted, smoked, or poorly preserved foods may increase the risk of stomach cancer.
The risk of stomach cancer is increased in people who
work in the rubber or coal industry
have been exposed to very high levels of radiation
Having one or more of these risk factors does not necessarily mean you will get stomach cancer. Many people with risk factors never develop stomach cancer, whereas others with no known risk factors do. Talk with your doctor if you think you might be at increased risk.
Stomach cancer screening or preventive surgery may be available to people at very high risk of stomach cancer, such as those with certain genetic conditions or family histories. Learn about stomach cancer screening.
Gallbladder cancer is a rare type of cancer that starts in the tissues of the gallbladder.
Signs and symptoms of gallbladder cancer include jaundice, fever, and pain.
Gallbladder cancer is difficult to detect (find) and diagnose early.
Tests that examine the gallbladder and nearby organs are used to detect (find), diagnose, and stage gallbladder cancer.
Certain factors affect the prognosis (chance of recovery) and treatment options.
Gallbladder cancer is a rare type of cancer that starts in the tissues of the gallbladder.
Gallbladder cancer occurs when cells in the gallbladder start to grow out of control. The gallbladder is a pear-shaped organ that lies just under the liver in the upper abdomen. The gallbladder stores bile, a fluid made by the liver to digest fat. When food is being broken down in the stomach and intestines, bile is released from the gallbladder through a tube called the common bile duct, which connects the gallbladder and liver to the first part of the small intestine.
EnlargeAnatomy of the gallbladder. The gallbladder is just below the liver. Bile is stored in the gallbladder and flows through the cystic duct and the common bile duct into the small intestine when food is being digested.
The wall of the gallbladder has 4 main layers of tissue:
Gallbladder cancer is difficult to detect (find) and diagnose early.
Gallbladder cancer is difficult to detect and diagnose because:
People rarely have signs or symptoms in the early stages of gallbladder cancer.
The symptoms of gallbladder cancer, when present, are like the symptoms of many other illnesses.
The gallbladder is hidden behind the liver.
Gallbladder cancer is sometimes found when the gallbladder is removed for other reasons. Although gallstones are the most common risk factor for developing gallbladder cancer, the overall risk is low. Most people with gallstones do not develop gallbladder cancer.
Tests that examine the gallbladder and nearby organs are used to detect (find), diagnose, and stage gallbladder cancer.
Procedures that make pictures of the gallbladder and the area around it help diagnose gallbladder cancer and show how far the cancer has spread. The process used to find out if cancer cells have spread within and around the gallbladder is called staging.
To plan treatment, it is important to know if the gallbladder cancer can be removed by surgery. Tests and procedures to detect, diagnose, and stage gallbladder cancer are usually done at the same time. In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
Liver function tests: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by the liver. A higher-than-normal amount of a substance can be a sign of liver disease that may be caused by gallbladder cancer.
Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. An abdominal ultrasound is done to diagnose gallbladder cancer.
PTC (percutaneous transhepatic cholangiography): A procedure used to x-ray the liver and bile ducts. A thin needle is inserted through the skin below the ribs and into the liver. Dye is injected into the liver or bile ducts and an x-ray is taken. If a blockage is found, a thin, flexible tube called a stent is sometimes left in the liver to drain bile into the small intestine or a collection bag outside the body.
ERCP (endoscopic retrograde cholangiopancreatography): A procedure used to x-ray the ducts (tubes) that carry bile from the liver to the gallbladder and from the gallbladder to the small intestine. Sometimes gallbladder cancer causes these ducts to narrow and block or slow the flow of bile, causing jaundice. An endoscope (a thin, lighted tube) is passed through the mouth, esophagus, and stomach into the first part of the small intestine. A catheter (a smaller tube) is then inserted through the endoscope into the bile ducts. A dye is injected through the catheter into the ducts and an x-ray is taken. If the ducts are blocked by a tumor, a fine tube may be inserted into the duct to unblock it. This tube (or stent) may be left in place to keep the duct open. Tissue samples may also be taken.
MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Endoscopic ultrasound (EUS): A procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
Laparoscopy: A surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples for biopsy. Laparoscopy helps to find out if the cancer is within the gallbladder only or has spread to nearby tissues and if it can be removed by surgery.
Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The biopsy may be done after surgery to remove the tumor. If the tumor clearly cannot be removed by surgery, the biopsy may be done using a fine needle to remove cells from the tumor.
Certain factors affect the prognosis (chance of recovery) and treatment options.
the stage of the cancer (whether the cancer has spread from the gallbladder to other places in the body)
whether the cancer can be completely removed by surgery
the type of gallbladder cancer (how the cancer cell looks under a microscope)
whether the cancer has just been diagnosed or has recurred (come back)
Treatment may also depend on the age and general health of the patient and whether the cancer is causing signs or symptoms.
Gallbladder cancer can be cured only if it is found before it has spread, when it can be removed by surgery. If the cancer has spread, palliative treatment can improve the patient’s quality of life by controlling the symptoms and complications of this disease.
Stages of Gallbladder Cancer
Key Points
Tests and procedures to stage gallbladder cancer are usually done at the same time as diagnosis.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
The following stages are used for gallbladder cancer:
Stage 0 (Carcinoma in Situ)
Stage I
Stage II
Stage III
Stage IV
For gallbladder cancer, stages are also grouped according to how the cancer may be treated. There are two treatment groups:
Localized (Stage I)
Unresectable, recurrent, or metastatic (Stage II, Stage III, and Stage IV)
Tests and procedures to stage gallbladder cancer are usually done at the same time as diagnosis.
Learn more about tests and procedures used to detect, diagnose, and stage gallbladder cancer in the General Information section.
There are three ways that cancer spreads in the body.
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if gallbladder cancer spreads to the liver, the cancer cells in the liver are actually gallbladder cancer cells. The disease is metastatic gallbladder cancer, not liver cancer.
Many cancer deaths are caused when cancer moves from the original tumor and spreads to other tissues and organs. This is called metastatic cancer. This animation shows how cancer cells travel from the place in the body where they first formed to other parts of the body.
The following stages are used for gallbladder cancer:
Stage 0 (Carcinoma in Situ)
In stage 0, abnormal cells are found in the mucosa (innermost layer) of the gallbladder wall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage I
In stage I, cancer has formed in the mucosa (innermost layer) of the gallbladder wall and may have spread to the muscle layer of the gallbladder wall.
Stage II
Stage II is divided into stages IIA and IIB, depending on where the cancer has spread in the gallbladder.
In stage IIA, cancer has spread through the muscle layer to the connective tissue layer of the gallbladder wall on the side of the gallbladder that is not near the liver.
In stage IIB, cancer has spread through the muscle layer to the connective tissue layer of the gallbladder wall on the same side as the liver. Cancer has not spread to the liver.
Stage III
Stage III is divided into stages IIIA and IIIB, depending on where the cancer has spread.
In stage IIIA, cancer has spread through the connective tissue layer of the gallbladder wall and one or more of the following is true:
Cancer has spread to the serosa (layer of tissue that covers the gallbladder).
In stage IIIB, cancer has formed in the mucosa (innermost layer) of the gallbladder wall and may have spread to the muscle, connective tissue, or serosa (layer of tissue that covers the gallbladder) and may have also spread to the liver or to one nearby organ or structure (such as the stomach, small intestine, colon, pancreas, or the bile ducts outside the liver). Cancer has spread to one to three nearby lymph nodes.
In stage IVA, cancer has spread to the portal vein or hepatic artery or to two or more organs or structures other than the liver. Cancer may have spread to one to three nearby lymph nodes.
In stage IVB, cancer may have spread to nearby organs or structures. Cancer has spread:
to four or more nearby lymph nodes; or
to other parts of the body, such as the peritoneum and liver.
For gallbladder cancer, stages are also grouped according to how the cancer may be treated. There are two treatment groups:
Localized (Stage I)
Cancer is found in the wall of the gallbladder and can be completely removed by surgery.
Unresectable, recurrent, or metastatic (Stage II, Stage III, and Stage IV)
Unresectable cancer cannot be removed completely by surgery. Most patients with gallbladder cancer have unresectable cancer.
Recurrent cancer is cancer that has recurred (come back) after it has been treated. Gallbladder cancer may come back in the gallbladder or in other parts of the body.
Metastasis is the spread of cancer from the primary site (place where it started) to other places in the body. Metastatic gallbladder cancer may spread to surrounding tissues, organs, throughout the abdominalcavity, or to distant parts of the body.
Treatment Option Overview
Key Points
There are different types of treatment for patients with gallbladder cancer.
The following types of treatment are used:
Surgery
Radiation therapy
Chemotherapy
New types of treatment are being tested in clinical trials.
Radiation sensitizers
Targeted therapy
Immunotherapy
Treatment for gallbladder cancer may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up care may be needed.
There are different types of treatment for patients with gallbladder cancer.
Different types of treatments are available for patients with gallbladder cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
The following types of treatment are used:
Surgery
Gallbladder cancer may be treated with a cholecystectomy, surgery to remove the gallbladder and some of the tissues around it. Nearby lymph nodes may be removed. A laparoscope is sometimes used to guide gallbladder surgery. The laparoscope is attached to a video camera and inserted through an incision (port) in the abdomen. Surgical instruments are inserted through other ports to perform the surgery. Because there is a risk that gallbladder cancer cells may spread to these ports, tissue surrounding the port sites may also be removed.
If the cancer has spread and cannot be removed, the following types of palliative surgery may relieve symptoms:
Biliary bypass: If the tumor is blocking the bile duct and bile is building up in the gallbladder, a biliary bypass may be done. During this operation, the doctor will cut the gallbladder or bile duct in the area before the blockage and sew it to the small intestine to create a new pathway around the blocked area.
Endoscopicstent placement: If the tumor is blocking the bile duct, surgery may be done to put in a stent (a thin tube) to drain bile that has built up in the area. The doctor may place the stent through a catheter that drains the bile into a bag on the outside of the body or the stent may go around the blocked area and drain the bile into the small intestine.
Percutaneous transhepatic biliary drainage: A procedure done to drain bile when there is a blockage and endoscopic stent placement is not possible. An x-ray of the liver and bile ducts is done to locate the blockage. Images made by ultrasound are used to guide placement of a stent, which is left in the liver to drain bile into the small intestine or a collection bag outside the body. This procedure may be done to relieve jaundice before surgery.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward area of the body with cancer.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic therapy).
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Radiation sensitizers
Clinical trials are studying ways to improve the effect of radiation therapy on tumor cells, including:
Hyperthermia therapy: A treatment in which body tissue is exposed to high temperatures to damage and kill cancer cells or to make cancer cells more sensitive to the effects of radiation therapy and certain anticancer drugs.
Radiosensitizers: Drugs that make tumor cells more sensitive to radiation therapy. Giving radiation therapy together with radiosensitizers may kill more tumor cells.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. The following targeted therapies are being studied in patients with gallbladder cancer that is locally advanced and cannot be removed by surgery or has spread to other parts of the body:
Ivosidenib is a type of targeted therapy that blocks a specific mutation in a gene called IDH1. It works by slowing or stopping the growth of cancer cells.
Pemigatinib is a type of targeted therapy that blocks specific changes in a gene called FGFR2. This may help keep cancer cells from growing and may kill them.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer.
PD-1 and PD-L1 inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells.
Pembrolizumab is a type of PD-1 inhibitor that may be used in patients whose cancer is locally advanced and cannot be removed by surgery or has spread to other parts of the body.
Durvalumab is a type of PD-L1 inhibitor that is being studied in combination with chemotherapy in previously untreated patients whose cancer is locally advanced, recurrent, or has spread to other parts of the body.
EnlargeImmune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
Immunotherapy uses the body’s immune system to fight cancer. This animation explains one type of immunotherapy that uses immune checkpoint inhibitors to treat cancer.
Treatment for gallbladder cancer may cause side effects.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up care may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Treatment of Localized and Locally Advanced Gallbladder Cancer
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Unresectable, Metastatic, or Recurrent Gallbladder Cancer
A clinical trial of new ways to give palliative radiation therapy, such as giving it together with hyperthermia therapy, radiosensitizers, or chemotherapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of gallbladder cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Gallbladder Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/gallbladder/patient/gallbladder-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389400]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.













 to PD-1 (on the T cell), which keeps T cells from killing tumor cells in the body. Also shown are a tumor cell antigen and T cell receptor. The panel on the right shows immune checkpoint inhibitors (anti-PD-L1 and anti-PD-1) blocking the binding of PD-L1 to PD-1, which allows the T cells to kill tumor cells.")