

Treatment for cancer may cause changes to a male’s fertility.
Credit: National Cancer Institute
Cancer treatments can cause infertility or lower your fertility. Talk with your doctor about whether your cancer or its treatment may affect your fertility. Sometimes you may need to start this conversation.
At a time when you and your health care team are focused on planning cancer treatment, it may feel overwhelming to think about making fertility-related decisions. However, research has found that survivors were less regretful if they had met with a fertility specialist, regardless of whether they decided to preserve their fertility.
If having a biological child one day may be important to you, consider talking with your doctor and a fertility specialist before starting cancer treatment for information that will help you decide what is best for you.
- Ask about how the proposed cancer treatments could affect your fertility.
- Get a referral to a fertility specialist, such as an oncofertility specialist or reproductive endocrinologist, to learn about all of your options.
What is fertility?
Fertility is the ability to produce children. A male’s fertility depends on a functioning reproductive system that makes and ejaculates healthy sperm and an endocrine system that makes hormones.
Factors that may affect your fertility
Whether your fertility is affected by cancer or its treatment depends on:
- the type of cancer treatment(s)
- the amount (dose) of treatment
- the length (duration) of treatment
- your age at the time of treatment
- the amount of time that has passed since treatment
- the type of cancer and if the tumor is near the reproductive organs
- your baseline fertility status, including any fertility problems in the past
- other personal health conditions and factors
Cancer treatments may cause infertility or lower your fertility
Cancer treatments may affect your fertility by harming reproductive organs and endocrine glands that control fertility. Changes to your fertility may be temporary or permanent.
Chemotherapy and fertility
Chemotherapy destroys cancer cells but can also harm healthy cells, such as germ cells. Germ cells are reproductive cells that become sperm. Some types of chemotherapy pose a high risk to your fertility. For example, alkylating agents present a high risk to your fertility because they can damage sperm in adult males and sperm-forming cells (germ cells) in young males. You may be at greater risk of infertility if you receive high doses of chemotherapy or several chemotherapy drugs at the same time.
Hormone therapy and fertility
Hormone therapy, also called endocrine therapy, adds, blocks, or removes hormones, such as testosterone, androgen, and progesterone. It may be used to stop or slow the growth of cancer that uses hormones to grow. However, hormone therapy can decrease sperm count.
Immunotherapy and fertility
Immunotherapy stimulates or suppresses your immune system to fight cancer. The effects of immunotherapy on fertility are still being studied. If your doctor recommends immunotherapy, ask what is known about the type of immunotherapy you will receive and how it may affect your fertility.
Radiation therapy and fertility
Radiation therapy destroys cancer cells or slows their growth. Radiation to your reproductive organs, pelvic region, or central nervous system can affect your fertility. The dose of radiation, the part of your body receiving radiation, and your age also play a role in whether your fertility is affected. The type of radiation therapy used is also a factor. For example, proton beam radiation therapy and intensity-modulated radiation therapy may have less of an effect on your fertility than standard radiation therapy.
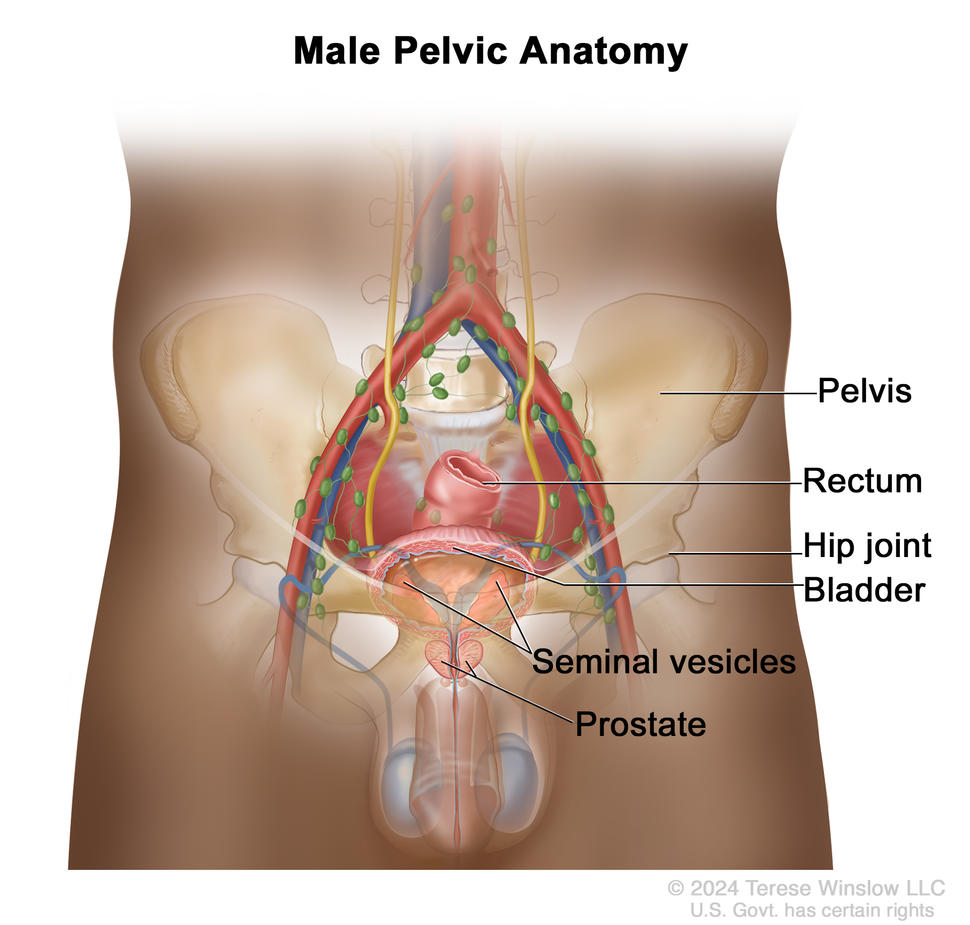
The pelvis is the area of the body below the abdomen that contains the hip bones, bladder, and rectum. In males, it also contains the prostate and seminal vesicles.
Credit: © Terese Winslow
Pelvic region: External-beam radiation therapy to the pelvis (such as to the anus, bladder, penis, or prostate) and brachytherapy can affect your sexual function and your fertility. If blood vessels or nerves are damaged, it may be difficult to get or keep an erection. This is called erectile dysfunction. If the prostate is damaged, you may have a dry orgasm, also called retrograde ejaculation.
Central nervous system: Radiation therapy to the brain may affect glands such as the pituitary gland and hypothalamus that produce hormones needed for fertility. Lower hormone levels can cause fertility issues.
Learn about procedures that can help protect your fertility during radiation therapy in the section Fertility preservation methods for males.
Stem cell transplant and fertility
Before having a stem cell transplant, also called a bone marrow transplant or hematopoietic cell transplant, you may receive high doses of chemotherapy, radiation therapy, or both. These treatments can damage sperm and sperm-forming cells and cause infertility.
Surgery and fertility
The type, size, and location of the tumor are important factors in whether surgery affects your fertility. Some cancers may require surgeries that could affect your fertility:
- Surgery for reproductive system cancers such as prostate, penile, testicular, and urethral cancers can affect the production of semen. Surgeries that may impair your fertility including surgery for prostate cancer, such as radical prostatectomy, surgery for testicular cancer, such as bilateral orchiectomy, and surgery for penile cancer such as penectomy.
- Surgery for anal, colon, and rectal cancers can affect nearby reproductive organs, nerves, and pelvic lymph nodes. This may cause retrograde ejaculation, a condition in which semen is made, but not released during orgasm, also called a dry orgasm.
- Surgery for bladder cancer such as a radical cystectomy to remove the bladder and nearby organs, such as the prostate gland and seminal vesicles, may cause infertility. If nearby nerves are damaged, this may cause erectile dysfunction.
Talk with your doctor to learn whether the advised surgery may affect your fertility.
Targeted therapy and fertility
Targeted therapy uses drugs or other substances to block proteins or other molecules that control how cancer cells grow, divide, and spread. While the effects of targeted therapies on fertility are still being studied, some studies have found that tyrosine kinase inhibitors (TKIs) may lower fertility because they affect the production of sperm and decrease hormone production. If targeted therapy is recommended, talk with your doctor about how the specific type of targeted therapy may affect your fertility.
Cancers that may affect your fertility
Some cancers pose a risk to your fertility. Males diagnosed with testicular cancer, prostate cancer, and other germ cell cancers are sometimes found to have poor semen quality and low sperm count at diagnosis. Males with Hodgkin lymphoma may have low sperm count or no sperm in the semen.
Cancers that affect young people, including children, adolescents, and young adults are associated with fertility-related problems. These cancers include lymphoma, leukemia, and central nervous system tumors. Learn about cancer in adolescents and young adults and childhood cancers.
Fertility preservation methods for males
Fertility preservation is the process of saving or protecting sperm or testicular tissue in order to have biological children in the future. Fertility treatments and procedures that help preserve your ability to father a child are also called assisted reproductive technology. These procedures may be available at the hospital or cancer center where you receive treatment or at a fertility clinic. You can also learn about fertility clinics in the Oncofertility Consortium’s Clinic Finder.
The success rate, financial cost, and availability of these procedures vary. Learn about states that require insurance companies to cover fertility preservation methods.
If you choose to take steps to preserve your fertility, your cancer treatment team and a fertility specialist will work together to help you develop a cancer treatment plan that includes fertility preservation. Your health care team will advise you on the timing of fertility procedures and advise you on the impact, if any, of delaying the start of cancer treatment to undergo a fertility preservation procedure.
Sperm banking
Sperm banking (also called sperm cryopreservation) is the most common fertility preservation method for males who have gone through puberty. Samples of semen are collected during masturbation at home or in a private room at the hospital or fertility clinic. Sperm may also be collected using a procedure called electroejaculation, which may induce ejaculation in males who are unable to ejaculate due to neurological damage, surgery, or other conditions. The sperm is then frozen and stored (banked) for the future. Sperm can be frozen for an indefinite amount of time. Later, the sperm can be thawed and used during in vitro fertilization (IVF). IVF is the most common type of assisted reproductive technology.
Testicular shielding
During testicular shielding (also called gonadal shielding), a protective cover is placed on the outside of the body to shield the testicles from scatter radiation to the pelvic region during radiation. Other names for this procedure are radiation shielding and gonadal preservation.
Testicular sperm extraction (TESE)
Testicular sperm extraction (TESE) is a type of sperm retrieval method. It’s an option for young males who have not yet gone through puberty or men who are not able to produce semen, have a low sperm count, or do not have sperm in the semen. TESE is a surgery that removes a small sample of testicular tissue. Sperm cells are then collected and frozen for future use or used right away to fertilize eggs. TESE may be done at the same time as surgery to treat cancer, such as testicular cancer. Microdissection TESE (microTESE) is a similar procedure, but it removes less testicular tissue than TESE.
Testicular sperm aspiration (TESA)
Testicular sperm aspiration (TESA) is a type of sperm retrieval method. TESA may be useful for males who have a blockage that prevents sperm from being ejaculated. During TESA, a sample of sperm cells and tissue are removed from the testicle through a small needle attached to a syringe. The sperm is then separated from the tissue and can be used right away to fertilize eggs or frozen for future use.
Testicular tissue freezing
Testicular tissue freezing (also called testicular tissue banking and testicular tissue cryopreservation) is an option for young boys who have not gone through puberty or men who are unable to give a sperm sample. Clinical trials are currently ongoing for testicular tissue cryopreservation. Talk with your doctor about the availability of this procedure at a hospital or fertility center near you.
Using birth control during cancer treatment
Even though cancer and cancer treatments can lower your fertility, there may still be a chance you could make a female pregnant. Some cancer treatments may be harmful or cause a miscarriage. Your doctor may advise using condoms and other forms of birth control during treatment.
Questions to ask your doctor about fertility
Before starting treatment, talk with your doctor about whether the recommended cancer treatment may affect your fertility:
- Could the proposed cancer treatment increase the risk of or cause infertility? Are there cancer treatments that might not cause infertility or might cause fewer fertility problems?
- Would you recommend a fertility specialist, such as a reproductive endocrinologist, that I could talk with to learn more about methods to preserve my fertility? And who could I talk with to learn about issues related to insurance and cost?
- Which fertility preservation method(s) would you advise for me? What fertility preservation methods are available at this hospital? At a fertility clinic?
- Is condom use advised, based on the treatment I will be receiving?
After completing treatment, ask your doctor:
- Should birth control be used after treatment? If so, for how long?
- What are the chances that people who have this treatment are fertile afterwards?
- How long might it take for my fertility to return?
Getting personalized care and support
It’s important to make decisions that reflect what is important to you. If having biological children is important, talk with your health care team about how the proposed cancer treatment may affect your ability to make a female pregnant. Keep in mind that a growing number of hospitals and cancer centers have social workers and cancer patient navigator programs to help you learn about fertility-related resources, including fertility specialists and financial support.
If you are the parent of a young boy or teen with cancer, this video of fertility options for young male cancer patients from the Children’s Hospital of Philadelphia may help you talk with your son’s health care team.
While many people want to have children at some point in their life, others don’t or choose to build families in different ways. For support reach out to your health care team and to professionally led cancer support groups. Learn more about coping with cancer at Emotional Support for Young People with Cancer.
Finding resources, financial support, and clinical trials
These organizations have information about fertility preservation options for people with cancer, as well as access to patient navigators and information about the costs of these procedures:
- Oncofertility Consortium: Learn more about fertility preservation options, connect with a patient navigator, and find community resources.
- Alliance for Fertility Preservation: Comprehensive information on fertility preservation, including answers to commonly asked questions and laws and legislation in some states that require insurance companies to cover the cost of fertility preservation for people with cancer.
- Livestrong Fertility: Access financial support and find a fertility clinic in your area. Learn about a discount program for qualifying patients.
Use the clinical trials search to find NCI-supported clinical trials related to fertility and cancer treatment. Clinical trials supported by other organizations can be found at ClinicalTrials.gov.





