Can surgery be used to reduce someone’s risk of breast cancer?
Yes. Risk-reducing (also called preventive or prophylactic) surgery can lower the risk of breast cancer in people who are at very high risk, such as women who carry a harmful mutation in a breast cancer susceptibility gene such as BRCA1, BRCA2, TP53, or PTEN.
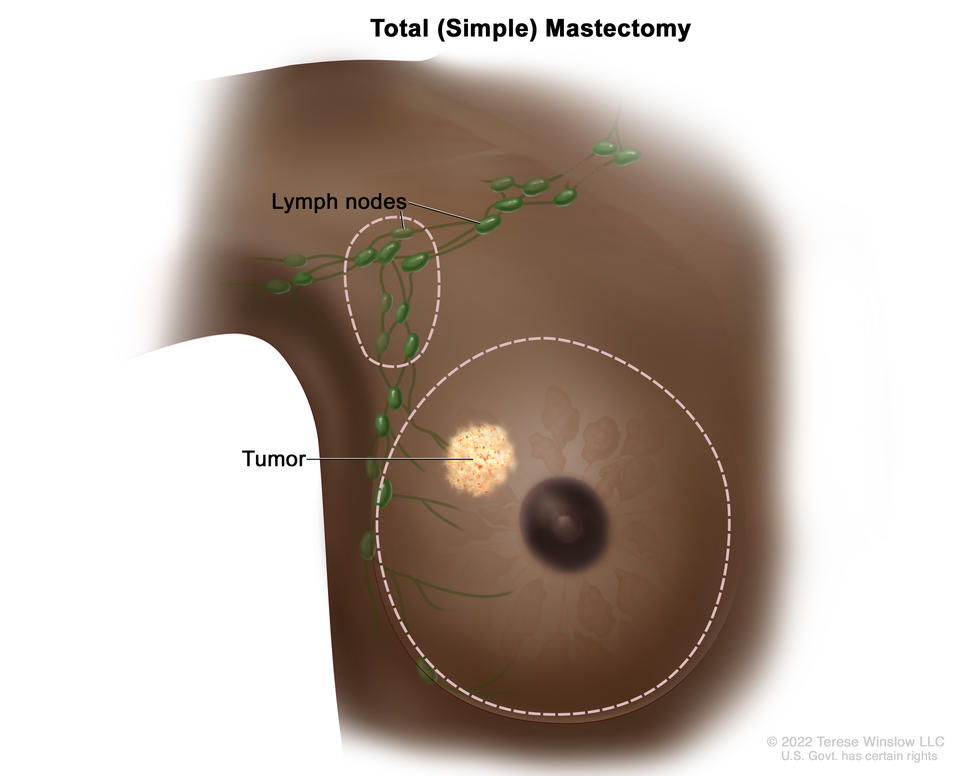
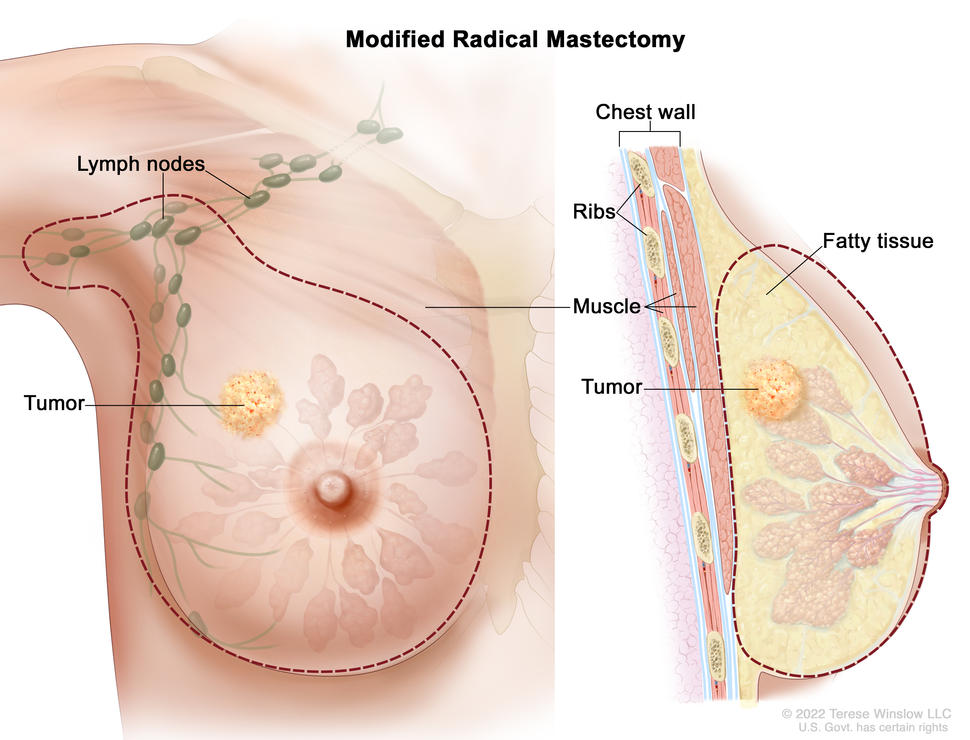
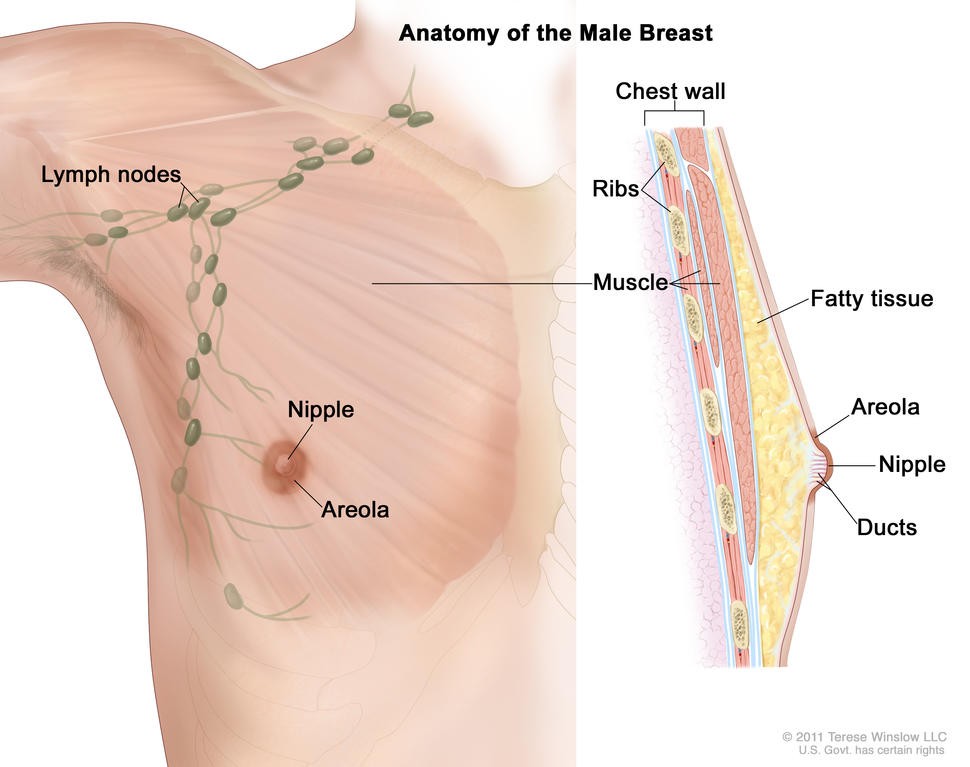
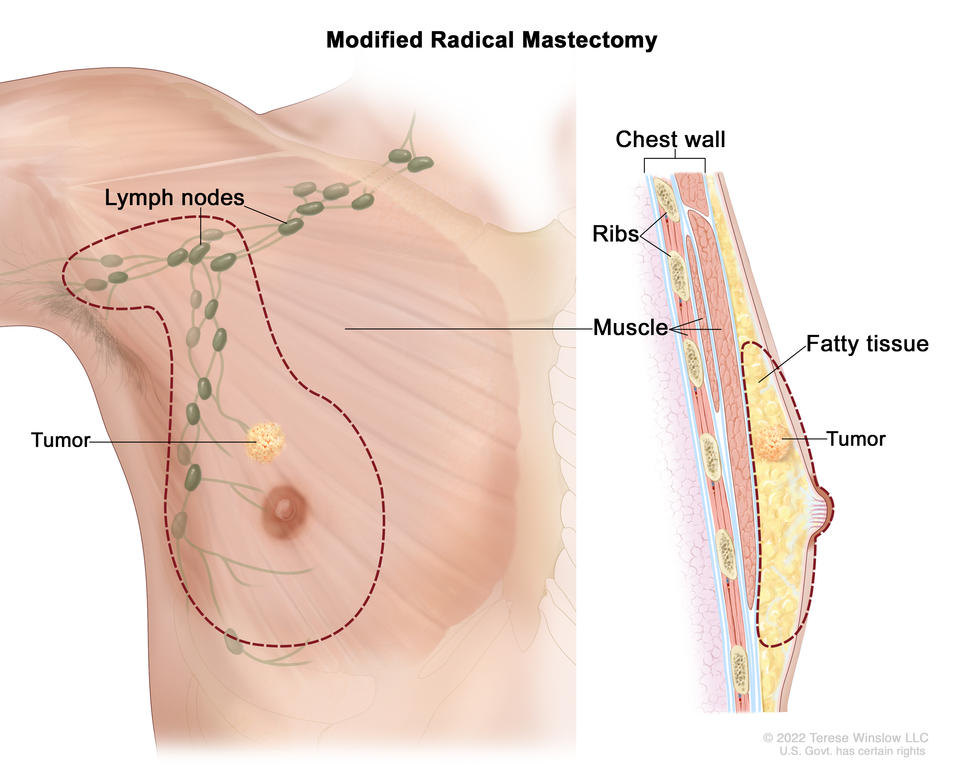
The main type of surgery to reduce breast cancer risk is the removal of both breasts, called bilateral risk-reducing mastectomy (or bilateral prophylactic mastectomy). The surgery may be a total mastectomy, in which the nipple and areola are removed, or a nipple-sparing mastectomy, which preserves the nipple and areola. Total mastectomy provides slightly more risk reduction, whereas nipple-sparing mastectomy allows for more natural-looking breasts after breast reconstruction surgery (1).
A second type of risk-reducing surgery is the removal of both ovaries (bilateral prophylactic oophorectomy) or of the ovaries and the fallopian tubes (bilateral prophylactic salpingo-oophorectomy, also called risk-reducing salpingo-oophorectomy). This surgery is often used to reduce the risk of ovarian and fallopian tube cancer in those who are at high risk for the disease because of inherited harmful changes in BRCA1, BRCA2, and several other genes. Some studies have suggested that risk-reducing salpingo-oophorectomy also reduces the risk of breast cancer in women at high risk, but other studies have not shown such a reduction (2–5).
How effective is risk-reducing mastectomy?
Bilateral mastectomy has been shown to reduce the risk of breast cancer by at least 95% in women who have a harmful (disease-causing) variant in the BRCA1 gene or the BRCA2 gene and up to 90% in women who have a strong family history of breast cancer (6–9). (It is important to keep in mind that mastectomy is not 100% effective at reducing risk because it is impossible to remove all the breast tissue that may be at risk of becoming cancerous in the future.)
Who should consider having surgery to reduce their risk of breast cancer?
People who are known to have inherited a harmful mutation that greatly increases their risk of developing breast cancer may consider having bilateral risk-reducing mastectomy to reduce this risk.
People who have a high risk of breast cancer but are not known to have inherited a harmful mutation may want to discuss with their doctors the possible benefits and harms of risk-reducing mastectomy in their situation. Such people include those with pleomorphic lobular carcinoma in situ (PLCIS) plus a strong family history of breast cancer and those who have had radiation therapy to the chest (including the breasts) before age 30 years.
Can a person have risk-reducing surgery if they have already been diagnosed with breast cancer?
Yes. Some people who have been diagnosed with cancer in one breast, particularly those who are known to be at very high risk, may consider having the other breast (called the contralateral breast) removed as well, even if there is no sign of cancer in that breast. Removal of the contralateral breast during breast cancer surgery (known as contralateral prophylactic mastectomy) reduces the risk of breast cancer in that breast (1,6,8,9).
However, doctors often discourage contralateral prophylactic mastectomy for people with cancer in one breast who do not have a high risk of developing a contralateral breast cancer. That is because their risk of developing another breast cancer, either in the same or the other breast, is very small (10), especially if their treatment included adjuvant chemotherapy or hormone therapy (11,12). Contralateral mastectomy may also increase the risk of complications and could result in delays in treatment for the known cancer. Moreover, the evidence to date does not indicate that contralateral prophylactic mastectomy reduces mortality.
People with a harmful BRCA variant who have surgery to treat breast cancer may also consider having risk-reducing salpingo-oophorectomy to improve their long-term outcomes. The risk of dying from any cause after breast cancer surgery for patients with a BRCA variant was reduced by more than half if they also received prophylactic salpingo-oophorectomy (13). The risk reduction was greater for those with a harmful variant in BRCA1 than for those with a harmful variant in BRCA2.
What are the potential harms of risk-reducing surgeries?
As with any other major surgery, bilateral prophylactic mastectomy and bilateral prophylactic salpingo-oophorectomy have potential complications or harms, such as bleeding or infection (14). Also, both surgeries are irreversible.
Breast removal can also affect psychological well-being due to a change in body image and the loss of normal breast functions. Although most people who choose to have this surgery are satisfied with their decision, they can still experience anxiety and concerns about body image (15,16). People who undergo total mastectomies lose nipple sensation, which may hinder sexual arousal.
The sudden drop in estrogen production caused by bilateral prophylactic salpingo-oophorectomy induces early menopause (this is also called surgical menopause). The abrupt onset of menopausal symptoms, including hot flashes, insomnia, anxiety, and depression, can be distressing.
People who have severe menopausal symptoms after undergoing bilateral prophylactic salpingo-oophorectomy may consider using short-term menopausal hormone therapy after surgery to alleviate these symptoms. Learn more about the health effects of menopausal hormone therapy.
What can someone at very high risk of breast cancer do if they do not want to undergo risk-reducing surgery?
Options for some people who are at very high risk of breast cancer (or of contralateral breast cancer, if they have previously been treated for breast cancer) and wish to avoid risk-reducing surgery include:
- More frequent breast cancer screening (also called enhanced surveillance). For example, they may have yearly mammograms and yearly magnetic resonance imaging (MRI) screening—with these tests staggered so that the breasts are imaged every 6 months—as well as clinical breast examinations performed regularly by a health care professional (17).
- Risk-reducing medications (sometimes called chemoprevention). Tamoxifen and raloxifene are approved by the U.S. Food and Drug Administration (FDA) to reduce breast cancer risk in women who, based on their personal and family medical history, have an increased risk of breast cancer. Whether these medications can be used to prevent breast cancer in women with inherited harmful mutations in BRCA1, BRCA2, or other genes associated with breast cancer risk is not yet clear (18). However, tamoxifen may lower the risk of contralateral breast cancer among BRCA1 and BRCA2 variant carriers previously diagnosed with breast cancer (19).
What can people at very high risk of ovarian cancer do to reduce their risk?
Risk-reducing salpingo-oophorectomy greatly reduces the risk of ovarian cancer and is the most effective approach. However, it has serious side effects, such as inducing early menopause in premenopausal women. Since many ovarian cancers are thought to start in the fallopian tubes, researchers are investigating the use of just salpingectomy to see if this also reduces the risk of ovarian cancer while sparing women from early menopause. However, this is not yet an option in clinical practice.
Another potential option is the use of oral contraceptives. Studies have consistently shown that women who have ever used oral contraceptives have a 30% to 50% lower risk of ovarian cancer than women who have never used oral contraceptives (20–22). A reduction in ovarian cancer risk with use of oral contraceptives has been seen not just among women in general but also among women who carry a harmful variant in the BRCA1 or BRCA2 gene (23–25).
These hormone-containing medications are thought to reduce the risk of ovarian cancer by preventing ovulation, which reduces exposure to naturally occurring female hormones that fuel the growth of ovarian cancer cells.
Does health insurance cover the cost of risk-reducing surgery?
Many health insurance companies have official policies about whether and under what conditions they will pay for risk-reducing surgeries for breast and ovarian cancer risk reduction. However, the criteria used for considering these procedures as medically necessary may vary among insurance companies. Some insurance companies may require a second opinion or a letter of medical necessity from the health care provider before they will approve coverage of any surgical procedure. A person who is considering risk-reducing surgery should discuss insurance coverage issues with their doctor and insurance company before choosing to have the surgery.
Who should a person talk to when considering surgery to reduce their risk of breast cancer?
If someone has a strong family history of breast cancer, ovarian cancer, or both, they and other members of their family should talk with a genetic counselor to understand whether they are truly at very high risk (that is, are likely to have a harmful variant in BRCA1, BRCA2, or another gene linked to breast cancer). A genetic counselor or other health care provider trained in genetics can review the family’s risks of disease and help family members obtain genetic testing for harmful changes in cancer-predisposing genes, if appropriate.
The decision to have any surgery to reduce the risk of breast cancer is a major one. Someone who is at high risk of breast cancer may wish to get a second opinion on risk-reducing surgery as well as on alternatives to surgery. For more information on getting a second opinion, see NCI’s Finding Health Care Services page.
A person who is considering risk-reducing mastectomy may also want to talk with a breast surgeon and a surgeon who specializes in breast reconstruction. Other health care professionals, including a breast health specialist, medical social worker, or cancer clinical psychologist or psychiatrist, can also help someone consider their options for reducing their risk of breast cancer.