A lump or change in the breast can be a symptom of breast cancer.
Credit: iStock
Signs and symptoms of breast cancer may include a lump or change in your breast. Signs and symptoms may vary, based on the type of breast cancer as well as how advanced the cancer is. However, early breast cancer often has no symptoms, which is why breast cancer screening is important.
What are the symptoms of breast cancer?
Although most breast changes are not cancer, it is important to check with your doctor if you notice unusual changes, including:
Breast lump, such as:
- a lump in or near your breast
- a lump under your arm
- thick or firm area (or mass) in or near your breast or under your arm
- a change in the size or shape of your breast
Nipple changes or discharge, such as:
- fluid or discharge that is not breast milk
- changes in the shape of the nipple or the direction it points or flattening of the nipple
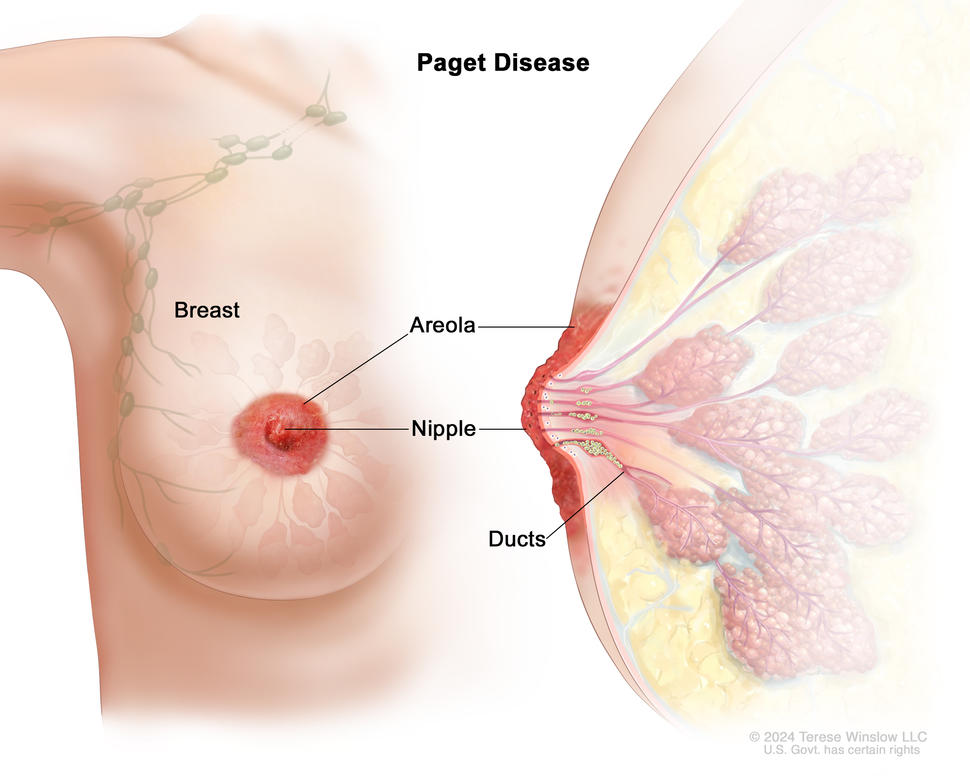
Skin changes on your breast(s), such as:
- scaly or swollen skin on the breast, nipple, or areola
- redness or darkening of the skin on the breast, nipple, or areola
- itching or tingling in the nipple or areola
- general swelling on your breast; there may not be a lump
- skin rash
- dimples or puckering
Depending on your symptoms, your doctor may suggest that you have a diagnostic mammogram or another test to find out if the symptoms are due to cancer or to a benign (not cancer) condition. Learn more about How Breast Cancer Is Diagnosed.
Most breast changes are not a sign of breast cancer. Learn about Benign and Precancerous Breast Lumps and Conditions.
Is pain a symptom of breast cancer?
Breast cancer does not usually cause pain. Several conditions that are not cancer, such as breast cysts and hormonal changes before your period, can cause breast soreness or pain, as can certain medications. If you have breast pain that persists, it’s important to see a doctor.
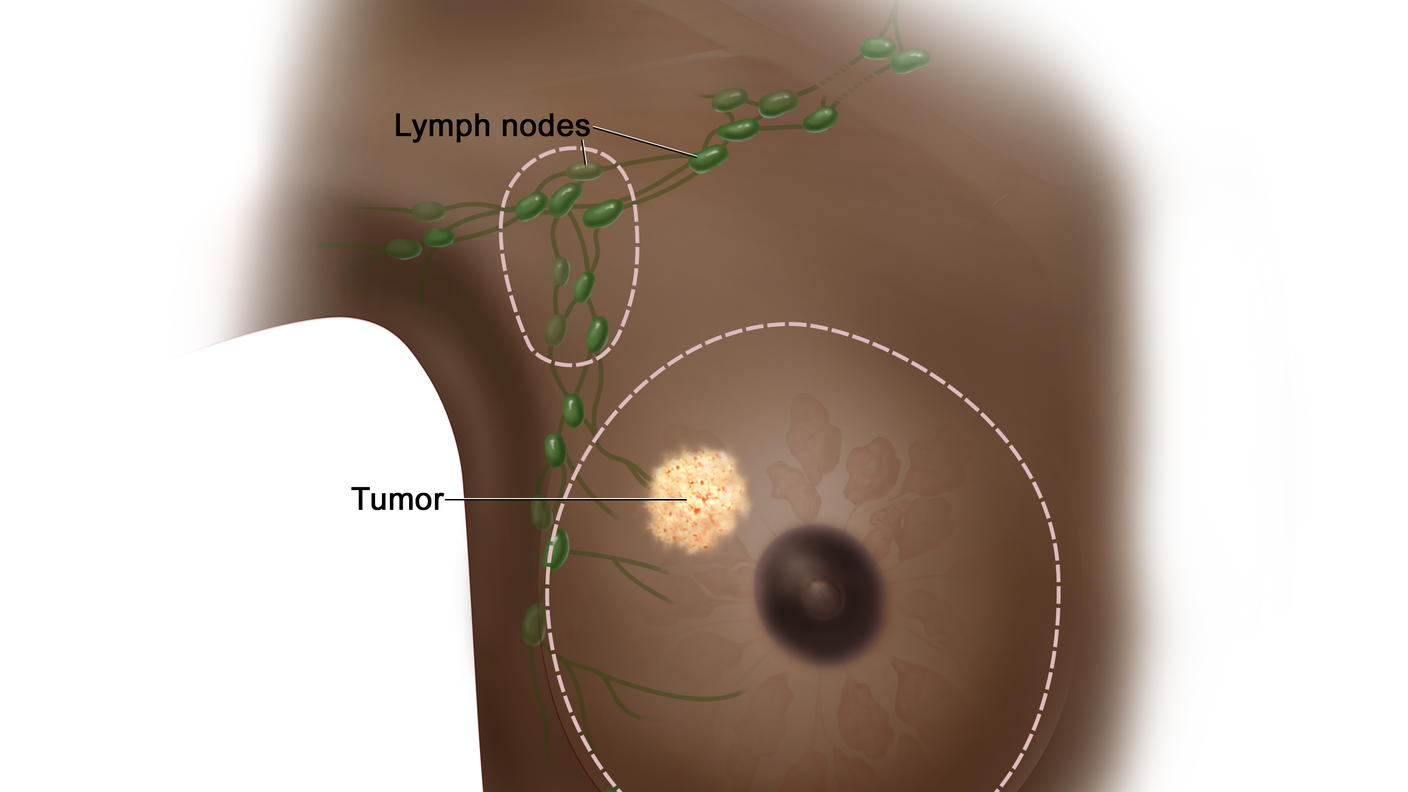
What are symptoms of metastatic breast cancer?
Breast cancer can sometimes spread beyond the breast, at which point it may be described as advanced breast cancer. It can spread to organs near the breasts, or it can metastasize (spread) through the blood or lymph system to distant sites, including the brain, bones, liver, lungs, or other organs.
If breast cancer is advanced or metastatic, it may cause signs and symptoms such as back pain, bone pain or bone fractures, shortness of breath, a constant dry cough, abdominal pain, swelling, jaundice, severe headaches, seizures, or vision changes. Symptoms depend on where the cancer has spread.
Learn more about Metastatic Breast Cancer, also called stage IV breast cancer.
What should I do if I find a breast change?
If you or your doctor find a breast lump or other breast change, keep in mind that breast changes are common and most are not symptoms of breast cancer. But it’s important to follow up with your doctor when you notice a breast change, even if you had a recent normal mammogram.