What is male breast cancer?
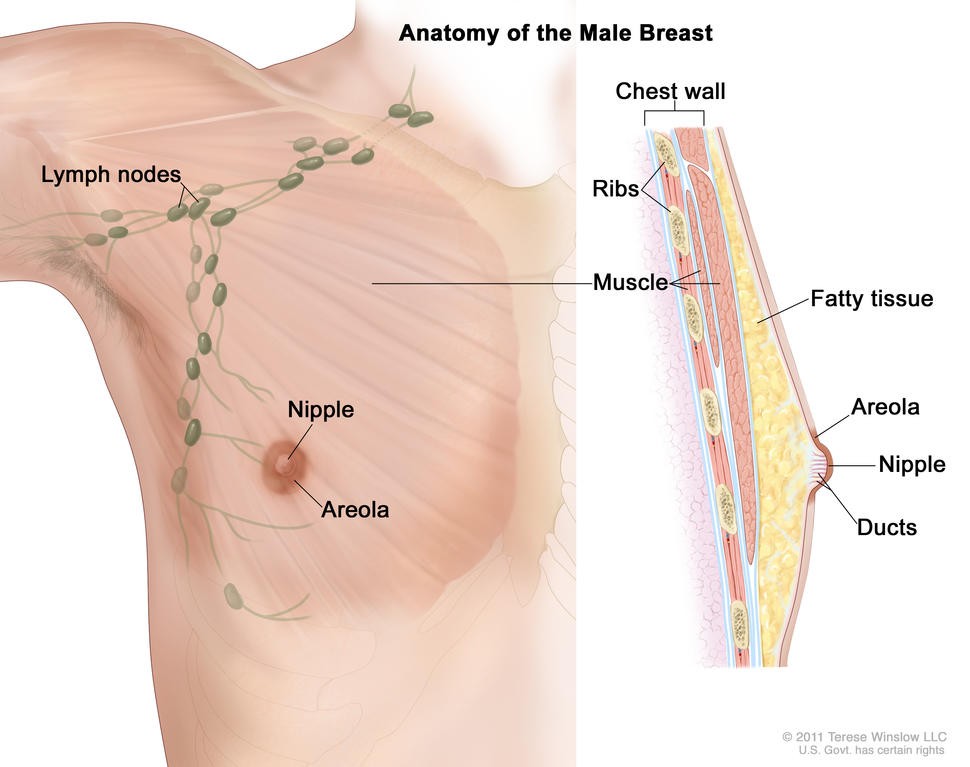
Anatomy of the male breast. The nipple and areola are shown on the outside of the breast. The lymph nodes, fatty tissue, ducts, and other parts of the inside of the breast are also shown.
Credit: © Terese Winslow
Male breast cancer is breast cancer that develops in men. Breast cancer is much more common in women, but men can get breast cancer because they also have breast tissue where cancer can start. Fewer than 1 in 100 breast cancers in the United States occur in men. Men of any age can get breast cancer, but it usually occurs at a later age in men than in women.
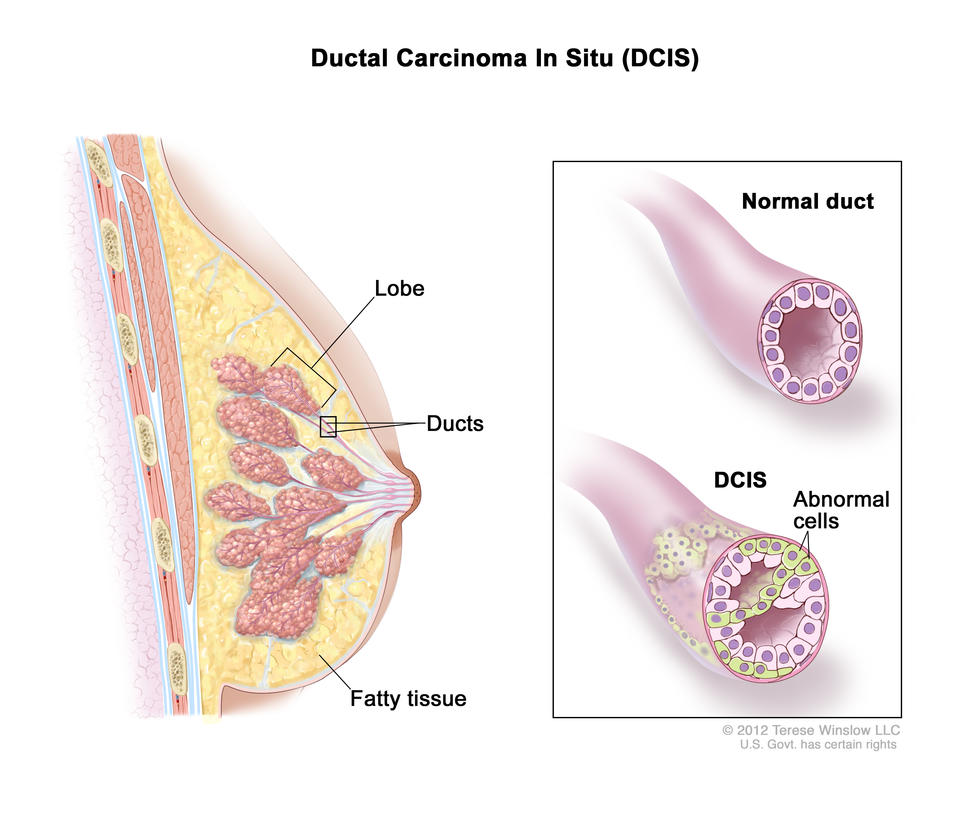
Most male breast cancers start in the milk ducts of the breast and are called ductal cancers. Both female and male breasts have milk ducts, but in male breasts, milk ducts do not develop in the same way as they do in female breasts. Male breasts may also have milk glands called lobules, but far fewer than in female breasts. Cancers that start in the lobules, called lobular cancers, are rare in men.
Other types of breast cancer are extremely rare in men, but they can happen. These include phyllodes tumor, Paget disease of the breast, and inflammatory breast cancer.
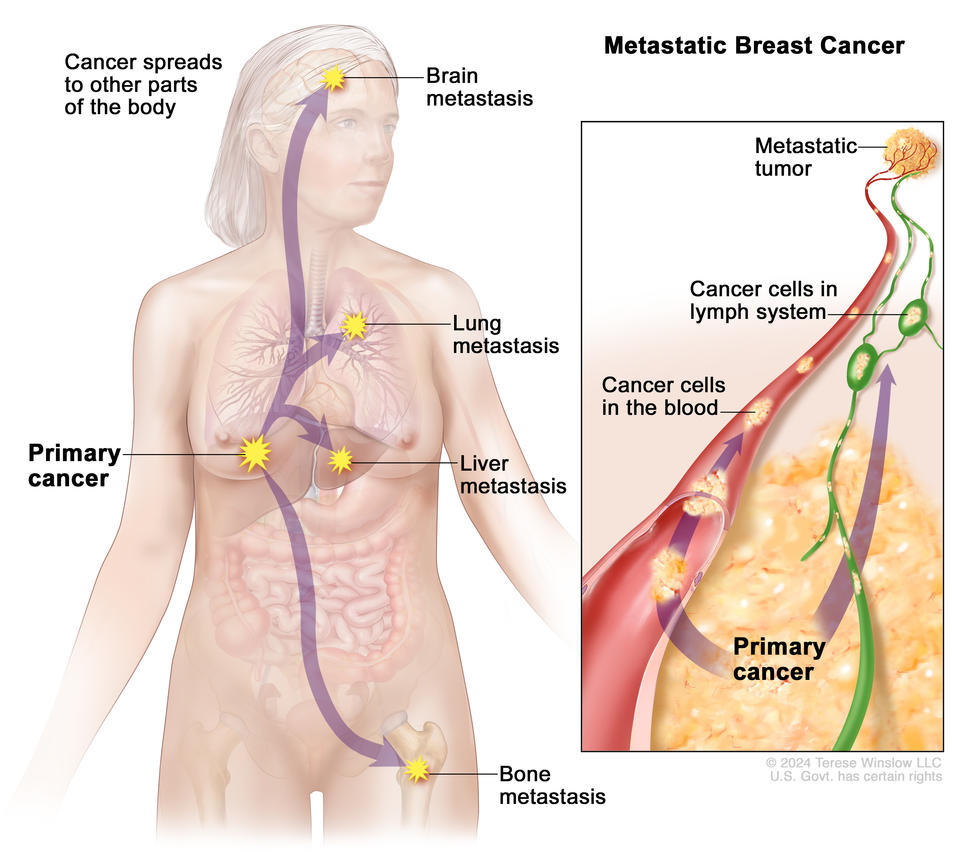
When abnormal cells are found in the ducts and have not spread to other tissues in the breast, it is called ductal carcinoma in situ. Invasive cancers have spread into surrounding breast tissue and can spread to nearby lymph nodes or other organs throughout the body. Most breast cancers in men are invasive.
What are risk factors for male breast cancer?
Older age is a risk factor for most cancers, including breast cancer in men. In addition, if you are male, you may have an increased risk of breast cancer if you have:
- a history of radiation therapy directed at the chest
- one or more female relatives who have had breast cancer
- inherited changes in the BRCA1 or BRCA2 genes or in other genes that increase breast cancer risk
- a condition linked to higher-than-normal estrogen levels in the body:
- Klinefelter syndrome
- liver disease (cirrhosis)
- testicular problems, including inflamed testicles (orchitis), an undescended testicle, or surgery to remove one or both testicles
- obesity
Screening for male breast cancer
If you think you may have risk factors for male breast cancer, talk to your doctor. Screening mammograms are not usually recommended for men, even those who are at increased risk of breast cancer. But your doctor may suggest staying alert to any changes in your breast or the skin of your breast and getting regular clinical breast exams.
What are the symptoms of breast cancer in men?
Signs and symptoms of breast cancer in men include:
- a lump or thickening in or near the breast (most common)
- a nipple that changes in shape or the direction it is pointing
- a nipple that is inverted
- fluid from the nipple that may be clear or bloody
- an open wound (ulcer) in the skin of the breast
- scaly, red, or swollen skin on the breast, nipple, or areola
- dimpling or ridges on the skin that resemble an orange peel
- swollen lymph nodes under the arm or near the collarbone
Many breast changes in men are signs of less serious or benign conditions, but it is important to check with your doctor if you notice any unusual breast changes.
How is breast cancer diagnosed in men?
If you are male and have symptoms of breast cancer, your doctor will need to find out if they are due to cancer or another condition. Your doctor may:
- do a physical exam, including a clinical breast exam
- ask about your personal and family medical history to learn more about your symptoms and risk factors for breast cancer
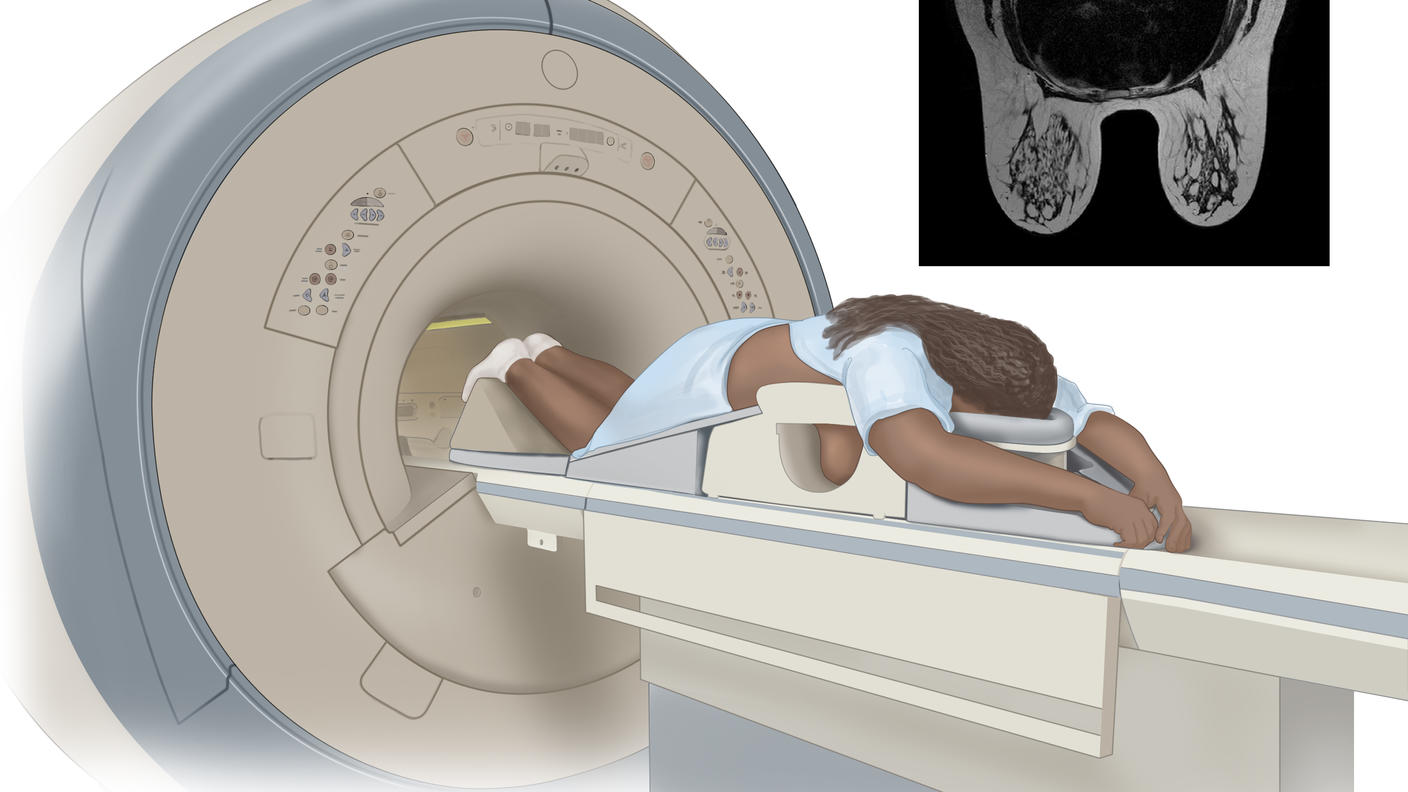
- do imaging tests, such as a breast ultrasound and mammogram
- do a breast biopsy, usually a core biopsy
If it is cancer, additional tests may include:
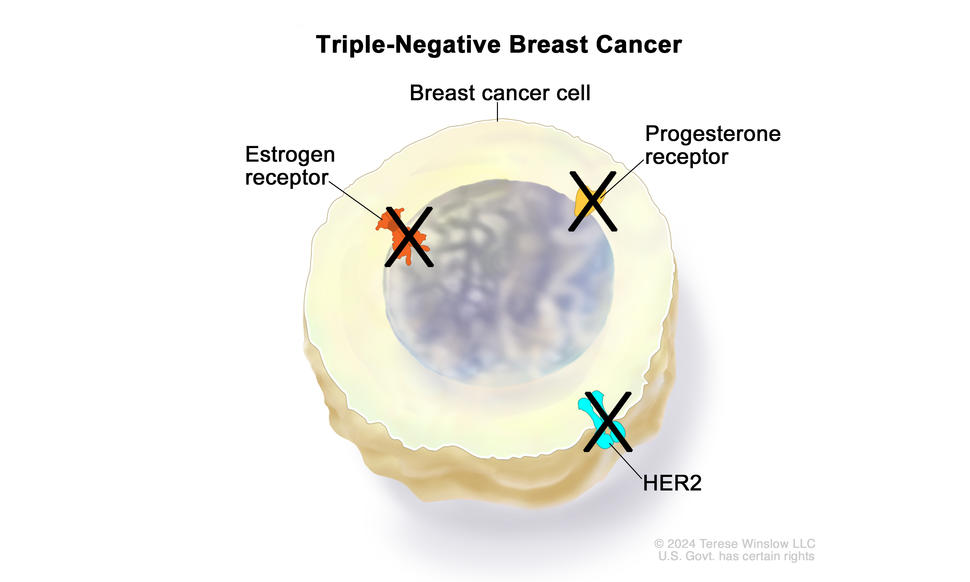
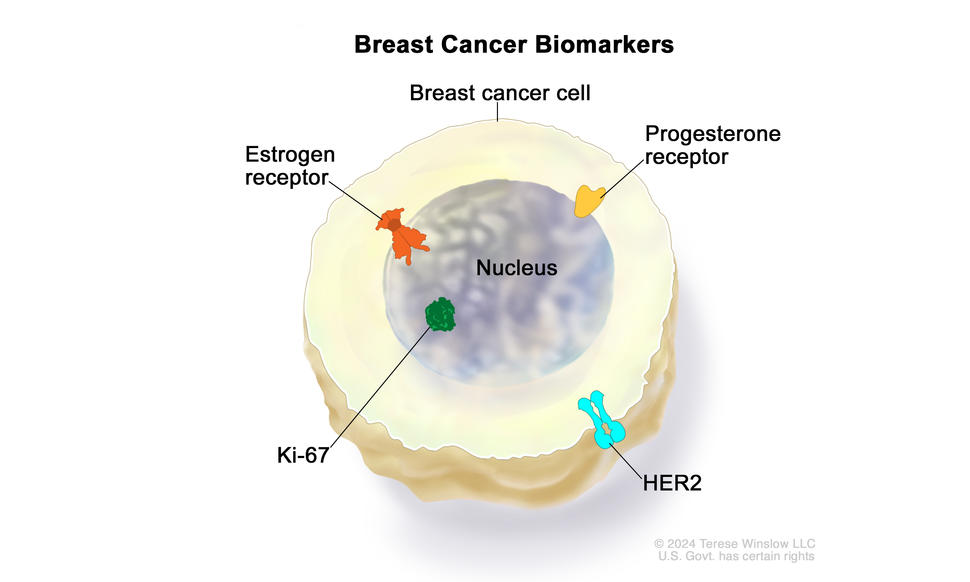
- Biomarker tests check the cancer cells for hormone receptors and HER2 protein that may help plan treatment. Male breast cancer is almost always hormone receptor positive. Learn more about Tests for Breast Cancer Biomarkers.
- Bone scan checks to see if cancer has spread to your bones.
- PET scan or CT scan are imaging tests that help determine the extent of spread of the cancer.
- Genetic testing looks for inherited mutations in BRCA1, BRCA2, and several other genes that increase the risk of breast cancer. Such mutations, if present, can affect treatment decisions. They also have implications for family members.
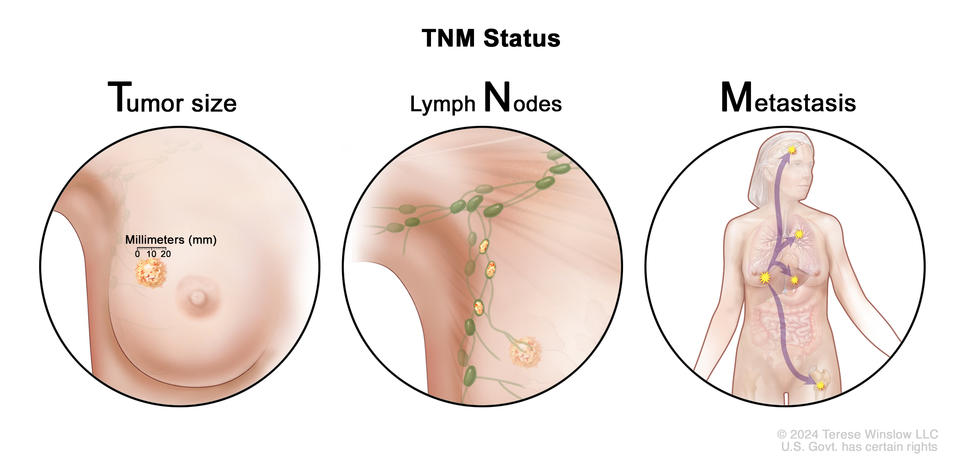
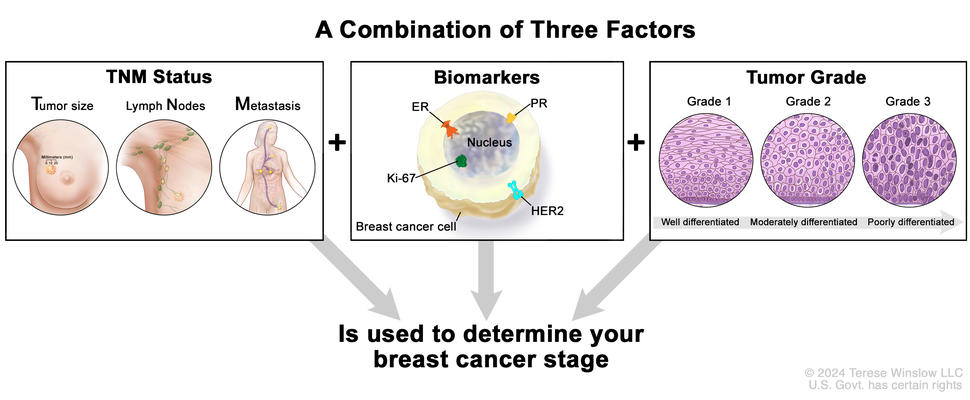
Your doctor will assign a stage to the cancer based on a combination of the extent of spread, hormone receptor and HER2 status, and other tumor features, such as tumor grade.
Learn more about the different stages of breast cancer and tests used to diagnose it at Breast Cancer Stages and How Breast Cancer Is Diagnosed.
How is male breast cancer treated?
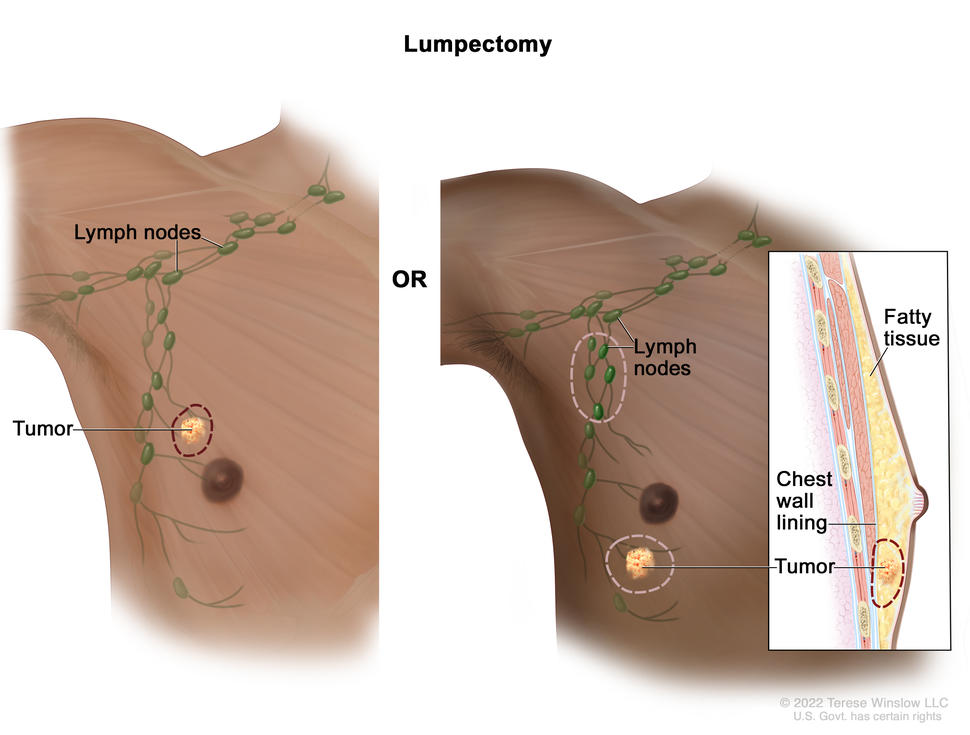
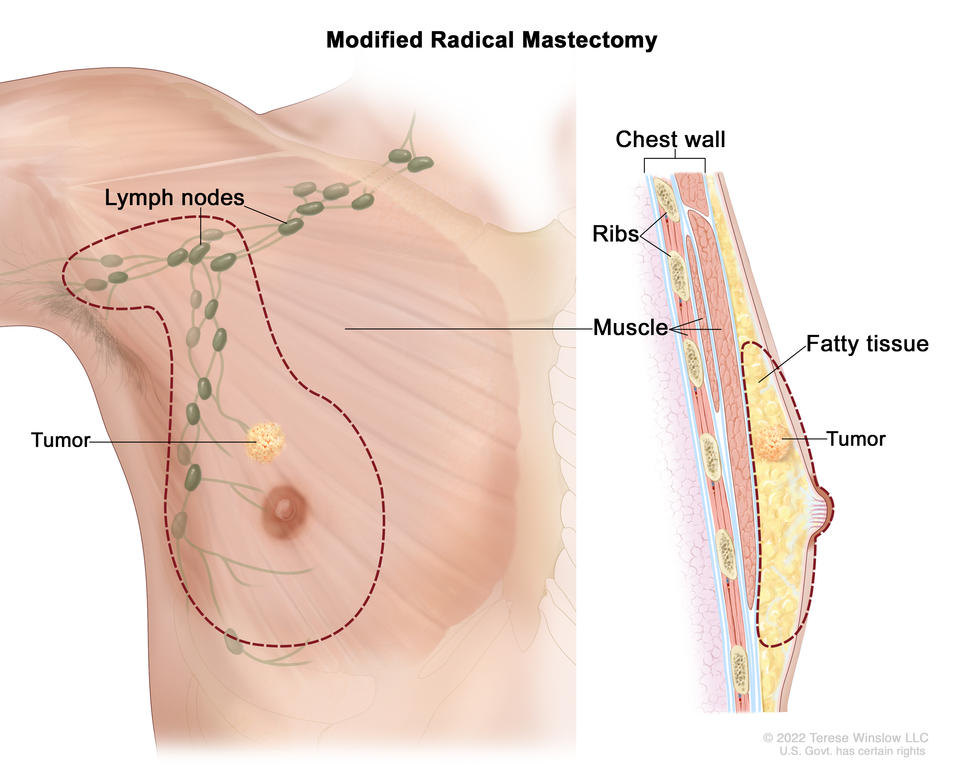
Male breast cancer is usually treated in the same way as breast cancer in women. However, men are more likely than women to have a mastectomy (surgery to remove the whole breast) rather than a lumpectomy (breast-conserving surgery) to remove the cancer because they have less breast tissue. But some male breast cancers can be treated with a lumpectomy, depending on the size of the cancer, the amount of breast tissue the person has, and other factors.
Learn more about breast cancer treatment at:
What is the survival rate and prognosis for men with breast cancer?
Doctors estimate the prognosis for men with breast cancer by using statistics collected over many years. One common statistic is the 5-year relative survival rate. The 5-year relative survival rate tells you what percent of people with the same type and stage of male breast cancer are alive 5 years after their cancer was diagnosed, compared with people in the overall population.
Men with breast cancer have a slightly lower 5-year survival rate than their female peers. This may be because male breast cancer is often diagnosed at a later stage than female breast cancer. Race also affects survival. Black men are usually diagnosed with a later stage of breast cancer than White men and are more likely to die of their disease.
More research is needed to find better treatments for male breast cancer and to better understand differences between male and female breast cancers.
The 5-year relative survival rates for people with male breast cancer are:
- 95% for localized male breast cancer (cancer is in the breast only)
- 84% for regional male breast cancer (cancer has spread beyond the breast to nearby lymph nodes or organs)
- 20% for metastatic male breast cancer (cancer has spread beyond the breast to a distant part of the body)
To learn more about factors that affect breast cancer prognosis, visit Breast Cancer Prognosis and Survival Rates.