We offer evidence-based supportive and palliative care information for health professionals on the assessment and management of cancer-related symptoms and conditions.
EnlargeMultiple myeloma. Multiple myeloma cells are abnormal plasma cells (a type of white blood cell) that build up in the bone marrow and form tumors in many bones of the body. Normal plasma cells make antibodies to help the body fight infection and disease. As the number of multiple myeloma cells increases, more antibodies are made. This can cause the blood to thicken and keep the bone marrow from making enough healthy blood cells. Multiple myeloma cells also damage and weaken the bone.
Plasma cell neoplasms are diseases in which abnormal plasma cells form tumors in the bones or soft tissues of the body. The plasma cells also make an antibody protein, called M protein, that is not needed by the body and does not help fight infection. These antibody proteins build up in the bone marrow and can cause the blood to thicken or can damage the kidneys.
Plasma cell neoplasms can be benign (not cancer) or malignant (cancer).
Monoclonal gammopathy of undetermined significance (MGUS)
In this type of plasma cellneoplasm, less than 10% of the bone marrow is made up of abnormal plasma cells and there is no cancer. The abnormal plasma cells make M protein, which is sometimes found during a routine blood or urine test. In most patients, the amount of M protein stays the same and there are no signs, symptoms, or health problems.
In isolated plasmacytoma of bone, one plasma cell tumor is found in the bone, less than 10% of the bone marrow is made up of plasma cells, and there are no other signs of cancer. Plasmacytoma of the bone often becomes multiple myeloma.
In extramedullary plasmacytoma, one plasma cell tumor is found in soft tissue but not in the bone or the bone marrow. Extramedullary plasmacytomas commonly form in tissues of the throat, tonsil, and paranasal sinuses.
In bone, the plasmacytoma may cause pain or broken bones.
In soft tissue, the tumor may press on nearby areas and cause pain or other problems. For example, a plasmacytoma in the throat can make it hard to swallow.
As the number of myeloma cells increases, fewer red blood cells, white blood cells, and platelets are made. The myeloma cells also damage and weaken the bone.
Sometimes multiple myeloma does not cause any signs or symptoms. This is called smoldering multiple myeloma. It may be found when a blood or urine test is done for another condition. Signs and symptoms may be caused by multiple myeloma or other conditions. Check with your doctor if you have any of the following:
A tumor can damage the bone and cause hypercalcemia (too much calcium in the blood). This can affect many organs in the body, including the kidneys, nerves, heart, muscles, and digestive tract, and cause serious health problems.
Hypercalcemia may cause the following signs and symptoms:
Multiple myeloma and other plasma cell neoplasms may cause a condition called amyloidosis.
In rare cases, multiple myeloma can cause peripheral nerves (nerves that are not in the brain or spinal cord) and organs to fail. This may be caused by a condition called amyloidosis. Antibody proteins build up and stick together in peripheral nerves and organs, such as the kidney and heart. This can cause the nerves and organs to become stiff and unable to work the way they should.
Amyloidosis may cause the following signs and symptoms:
Anything that increases a person’s chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop plasma cell neoplasms, and they will develop in people who don’t have any known risk factors. Talk with your doctor if you think you may be at risk.
Plasma cell neoplasms are most common in people who are middle aged or older. For multiple myeloma and plasmacytoma, other risk factors include the following:
Blood and urine immunoglobulin studies: A procedure in which a blood or urine sample is checked to measure the amounts of certain antibodies (immunoglobulins). For multiple myeloma, beta-2-microglobulin, M protein, free light chains, and other proteins made by the myeloma cells are measured. A higher-than-normal amount of these substances can be a sign of disease.
Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for abnormal cells. EnlargeBone marrow aspiration and biopsy. After a small area of skin is numbed, a long, hollow needle is inserted through the patient’s skin and hip bone into the bone marrow. A sample of bone marrow and a small piece of bone are removed for examination under a microscope.
The following tests may be done on the sample of tissue removed during the bone marrow aspiration and biopsy:
Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of bone marrow are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
FISH (fluorescence in situ hybridization): A laboratory test used to look at and count genes or chromosomes in cells and tissues. Pieces of DNA that contain fluorescent dyes are made in the laboratory and added to a sample of a patient’s cells or tissues. When these dyed pieces of DNA attach to certain genes or areas of chromosomes in the sample, they light up when viewed under a fluorescent microscope. The FISH test is used to help diagnose cancer and help plan treatment.
Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s bone marrow are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
Skeletal bone survey: In a skeletal bone survey, x-rays of all the bones in the body are taken. The x-rays are used to find areas where the bone is damaged. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
The portion of the blood sample made up of red blood cells.
Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances, such as calcium or albumin, released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
Twenty-four-hour urine test: A test in which urine is collected for 24 hours to measure the amounts of certain substances. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. A higher than normal amount of protein may be a sign of multiple myeloma.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI). An MRI of the spine and pelvis may be used to find areas where the bone is damaged.
PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the spine, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
PET-CT scan: A procedure that combines the pictures from a positron emission tomography (PET) scan and a computed tomography (CT) scan. The PET and CT scans are done at the same time with the same machine. The combined scans give more detailed pictures of areas inside the body, such as the spine, than either scan gives by itself.
Certain factors affect prognosis (chance of recovery) and treatment options.
Whether there are signs, symptoms, or health problems, such as kidney failure or infection, related to the disease.
Whether the cancer responds to initial treatment or recurs (comes back).
Stages of Plasma Cell Neoplasms
Key Points
There are no standard staging systems for monoclonal gammopathy of undetermined significance (MGUS) and plasmacytoma.
After multiple myeloma has been diagnosed, tests are done to find out how much cancer is in the body.
The stage of multiple myeloma is based on the levels of beta-2-microglobulin and albumin in the blood.
The following stages are used for multiple myeloma:
Stage I multiple myeloma
Stage II multiple myeloma
Stage III multiple myeloma
Plasma cell neoplasms may not respond to treatment or may come back after treatment.
There are no standard staging systems for monoclonal gammopathy of undetermined significance (MGUS) and plasmacytoma.
After multiple myeloma has been diagnosed, tests are done to find out how much cancer is in the body.
The process used to find out the amount of cancer in the body is called staging. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used to find out how much cancer is in the body:
Skeletal bone survey: In a skeletal bone survey, x-rays of all the bones in the body are taken. The x-rays are used to find areas where the bone is damaged. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the bone marrow. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Bone densitometry: A procedure that uses a special type of x-ray to measure bone density.
The stage of multiple myeloma is based on the levels of beta-2-microglobulin and albumin in the blood.
Plasma cell neoplasms may not respond to treatment or may come back after treatment.
Plasma cell neoplasms are called refractory when the number of plasma cells keeps going up even though treatment is given. Plasma cell neoplasms are called relapsed when they have come back after treatment.
Treatment Option Overview
Key Points
There are different types of treatment for patients with plasma cell neoplasms.
The following types of treatment are used:
Chemotherapy
Other drug therapy
Targeted therapy
High-dose chemotherapy with stem cell transplant
Immunotherapy
Radiation therapy
Surgery
Watchful waiting
New types of treatment are being tested in clinical trials.
New combinations of therapies
Treatment for plasma cell neoplasms may cause side effects.
Supportive care is given to lessen the problems caused by the disease or its treatment.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with plasma cell neoplasms.
Different types of treatments are available for patients with plasma cellneoplasms. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
The following types of treatment are used:
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Several types of targeted therapy may be used to treat multiple myeloma and other plasma cell neoplasms. There are different types of targeted therapy:
Proteasome inhibitortherapy: This treatment blocks the action of proteasomes in cancer cells. A proteasome is a protein that removes other proteins no longer needed by the cell. When the proteins are not removed from the cell, they build up and may cause the cancer cell to die. Bortezomib, carfilzomib, and ixazomib are proteasome inhibitors used in the treatment of multiple myeloma and other plasma cell neoplasms.
Monoclonal antibody therapy: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Daratumumab and elotuzumab are monoclonal antibodies used in the treatment of multiple myeloma and other plasma cell neoplasms. Denosumab is a monoclonal antibody used to slow bone loss and reduce bone pain in patients with multiple myeloma.
How do monoclonal antibodies work to treat cancer? This video shows how monoclonal antibodies, such as trastuzumab, pembrolizumab, and rituximab, block molecules cancer cells need to grow, flag cancer cells for destruction by the body’s immune system, or deliver harmful substances to cancer cells.
BCL2 inhibitor therapy: This treatment blocks a protein called BCL2. Blocking this protein may help kill cancer cells and may make them more sensitive to anticancer drugs. Venetoclax is a BCL2 inhibitor being studied in the treatment of relapsed or refractory multiple myeloma.
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient (autologous) or a donor (allogeneic) and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body’s blood cells.
EnlargeDonor stem cell transplant. (Step 1): Four to five days before donor stem cell collection, the donor receives a medicine to increase the number of stem cells circulating through their bloodstream (not shown). The blood-forming stem cells are then collected from the donor through a large vein in their arm. The blood flows through an apheresis machine that removes the stem cells. The rest of the blood is returned to the donor through a vein in their other arm. (Step 2): The patient receives chemotherapy to kill cancer cells and prepare their body for the donor stem cells. The patient may also receive radiation therapy (not shown). (Step 3): The patient receives an infusion of the donor stem cells.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This cancer treatment is a type of biologic therapy.
Immunomodulator therapy: Thalidomide, lenalidomide, and pomalidomide are immunomodulators used to treat multiple myeloma and other plasma cell neoplasms.
CAR T-cell therapy: This treatment changes the patient’s T cells (a type of immune system cell) so they will attack certain proteins on the surface of cancer cells. T cells are taken from the patient and special receptors are added to their surface in the laboratory. The changed cells are called chimeric antigen receptor (CAR) T cells. The CAR T cells are grown in the laboratory and given to the patient by infusion. The CAR T cells multiply in the patient’s blood and attack cancer cells. CAR T-cell therapy is being studied in the treatment of multiple myeloma that has recurred (come back). EnlargeCAR T-cell therapy. A type of treatment in which a patient’s T cells (a type of immune cell) are changed in the laboratory so they will bind to cancer cells and kill them. Blood from a vein in the patient’s arm flows through a tube to an apheresis machine (not shown), which removes the white blood cells, including the T cells, and sends the rest of the blood back to the patient. Then, the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. Millions of the CAR T cells are grown in the laboratory and then given to the patient by infusion. The CAR T cells are able to bind to an antigen on the cancer cells and kill them.
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Surgery
Surgery to remove the tumor may be done. After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
New combinations of therapies
Clinical trials are studying different combinations of immunotherapy, chemotherapy, steroid therapy, and drugs. New treatment regimens using selinexor are also being studied.
Treatment for plasma cell neoplasms may cause side effects.
Supportive care is given to lessen the problems caused by the disease or its treatment.
This therapy controls problems or side effects caused by the disease or its treatment, and improves quality of life. Supportive care is given to treat problems caused by multiple myeloma and other plasma cell neoplasms.
Supportive care may include the following:
Plasmapheresis: If the blood becomes thick with extra antibody proteins and interferes with circulation, plasmapheresis is done to remove extra plasma and antibody proteins from the blood. In this procedure blood is removed from the patient and sent through a machine that separates the plasma (the liquid part of the blood) from the blood cells. The patient’s plasma contains the unneeded antibodies and is not returned to the patient. The normal blood cells are returned to the bloodstream along with donated plasma or a plasma replacement. Plasmapheresis does not keep new antibodies from forming.
Induction therapy with stem cell transplant: If amyloidosis occurs, treatment may include induction therapy followed by stem cell transplant using the patient’s own stem cells.
Immunotherapy: Immunotherapy with thalidomide, lenalidomide, or pomalidomide is given to treat amyloidosis.
Targeted therapy: Targeted therapy with proteasome inhibitors is given to decrease how much immunoglobulin M is in the blood and treat amyloidosis. Targeted therapy with daratumumab is given with or without other drugs to treat amyloidosis. Targeted therapy with a monoclonal antibody is given to slow bone loss and reduce bone pain.
Radiation therapy: Radiation therapy is given for bone lesions of the spine.
Bisphosphonate therapy: Bisphosphonate therapy is given to slow bone loss and reduce bone pain. For more information on bisphosphonates and problems related to their use, see Oral Complications of Cancer Therapies.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Treatment of Monoclonal Gammopathy of Undetermined Significance
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Older, unfit patients who are not eligible for a stem cell transplant.
Patients younger than 65 years are usually considered younger and fit. Patients older than 75 years are usually not eligible for a stem cell transplant. For patients between the ages of 65 and 75 years, fitness is determined by their overall health and other factors.
two autologous stem cell transplants followed by an autologous or allogeneic stem cell transplant, in which the patient receives stem cells from the blood or bone marrow of a donor; or
one allogeneic stem cell transplant.
Maintenance therapy: After the initial treatment, maintenance therapy is often given to help keep the disease in remission for a longer time. Several types of treatment are being studied for this use, including the following:
Chemotherapy.
Immunotherapy (lenalidomide).
Corticosteroid therapy (prednisone or dexamethasone).
Targeted therapy with a proteasome inhibitor (bortezomib or ixazomib) or a monoclonal antibody (daratumumab).
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Relapsed or Refractory Multiple Myeloma
A different treatment than treatment already given, for patients whose tumor kept growing during treatment. See Multiple Myeloma treatment options.
The same drugs used before the relapse may be used if the relapse occurs one or more years after initial treatment. See Multiple Myeloma treatment options.
A clinical trial of targeted therapy with a small molecule inhibitor (selinexor) and corticosteroid therapy.
A clinical trial of targeted therapy with a BCL2 inhibitor (venetoclax).
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Plasma Cell Neoplasms
For more information from the National Cancer Institute about multiple myeloma and other plasma cell neoplasms, see the following:
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about treatment of plasma cell neoplasms (including multiple myeloma). It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Plasma Cell Neoplasms (Including Multiple Myeloma) Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/myeloma/patient/myeloma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389437]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
There are several types of plasma cell neoplasms. These diseases are all associated with a monoclonal (or myeloma) protein (M protein). They include monoclonal gammopathy of undetermined significance (MGUS), isolated plasmacytoma of the bone, extramedullary plasmacytoma, and multiple myeloma.
Estimated new cases and deaths from multiple myeloma in the United States in 2025:[1]
New cases: 36,110.
Deaths: 12,030.
Clinical Presentation and Evaluation
Table 1. Clinical Presentation of Plasma Cell Neoplasms
Plasma Cell Neoplasm
M Protein Type
Pathology
Clinical Presentation
Ig = immunoglobulin; MGUS = monoclonal gammopathy of undetermined significance.
MGUS
IgG kappa or lambda; or IgA kappa or lambda
<10% plasma cells in bone marrow
Asymptomatic, with minimal evidence of disease (aside from the presence of an M protein) [2]
Isolated plasmacytoma of bone
IgG kappa or lambda; or IgA kappa or gamma
Solitary lesion of bone; <10% plasma cells in marrow of uninvolved site
Asymptomatic or symptomatic
Extramedullary plasmacytoma
IgG kappa or lambda; or IgA kappa or gamma
Solitary lesion of soft tissue; most commonly occurs in the nasopharynx, tonsils, or paranasal sinuses [3]
Asymptomatic or symptomatic
Multiple myeloma
IgG kappa or lambda; or IgA kappa or gamma
Often, multiple lesions of bone
Symptomatic
Evaluation of patients with monoclonal (or myeloma) protein (M protein)
Idiotypic myeloma cells can be found in the blood of patients with myeloma in all stages of the disease.[4,5] For this reason, when treatment is indicated, systemic treatment must be considered for all patients with symptomatic plasma cell neoplasms. Patients with MGUS or asymptomatic smoldering myeloma do not require immediate treatment but must be followed carefully for signs of disease progression.
The major challenge is to separate the stable asymptomatic group of patients who do not require treatment from patients with progressive, symptomatic myeloma who may need to be treated immediately.[6–8]
Patients with an M protein in the serum and/or urine are evaluated by some of the following criteria:
Measure and follow the serum M protein by serum electrophoresis or by specific Ig assays; however, specific Ig quantification always overestimates the M protein because normal Ig are included in the result. For this reason, the preference is often that baseline and follow-up measurements of the M protein be done by the same method.[9] Quantitative serum free light chains (FLC) may be helpful to follow response when an M protein is not apparent.
Measure and follow the amount of M protein light chains excreted in the urine over 24 hours. Measure the total amount of protein excreted over 24 hours and multiply this value by the percentage of urine protein that is M protein, as determined by electrophoresis of concentrated urine protein. An easier, but less accurate, method uses a spot-urine protein electrophoresis.
Identify the heavy and light chain of the M protein by immunofixation electrophoresis.
Measure the hemoglobin, leukocyte, platelet, and differential counts.
Determine the percentage of marrow plasma cells. Be aware that marrow plasma-cell distribution may vary in different sites. Bone marrow is often sent for cytogenetics and fluorescence in situ hybridization testing for genetic markers of high-risk disease. For more information, see the Genetic factors and risk groups section.
Measure serum free kappa and lambda light chains. This is especially useful in cases of oligosecretory plasma-cell dyscrasia or for following cases of light-chain amyloidosis.[10] The FLC ratio of over 100 can predict a greater than 70% progression within 2 years in patients with smoldering myeloma.[11]
If clinically warranted, obtain needle aspirates of a solitary lytic bone lesion, extramedullary tumor(s), or enlarged lymph node(s) to determine whether these are plasmacytomas.
Evaluate renal function with serum creatinine and a creatinine clearance.
Electrophoresis of concentrated urine protein is very helpful in differentiating glomerular lesions from tubular lesions. Glomerular lesions, such as those resulting from glomerular deposits of amyloid or light-chain deposition disease, result in the nonselective leakage of all serum proteins into the urine; the electrophoresis pattern of this urine resembles the serum pattern with a preponderance of albumin.
In most patients with myeloma, the glomeruli function normally allows only the small molecular weight proteins, such as light chains, to filter into the urine. The concentration of protein in the tubules increases as water is reabsorbed. This leads to precipitation of proteins and the formation of tubular casts, which may injure the tubular cells. With tubular lesions, the typical electrophoresis pattern shows a small albumin peak and a larger light-chain peak in the globulin region; this tubular pattern is the usual pattern found in patients with myeloma.
Measure serum levels of calcium, alkaline phosphatase, lactic dehydrogenase, and, when indicated by clinical symptoms, cryoglobulins and serum viscosity.
Obtain radiographs of the skull, ribs, vertebrae, pelvis, shoulder girdle, and long bones.
Obtain a spinal magnetic resonance imaging (MRI) scan (or spinal computed tomography [CT] or positron emission tomography [PET]–CT scan depending on availability) if the skeletal survey is negative.[12–14] At diagnosis, whole-body PET scan or MRI of the total spine and pelvis appears to be equally efficacious in the detection of bone lesions.[15,16]
If amyloidosis is suspected, perform a needle aspiration of subcutaneous abdominal fat and stain the bone marrow biopsy for amyloid as the easiest and safest way to confirm the diagnosis.[17]
Measure serum albumin and beta-2-microglobulin as independent prognostic factors.[18,19]
The presence of circulating myeloma cells is considered a poor prognostic factor.[20] Primary plasma cell leukemia has a particularly poor prognosis.[21,22]
These initial studies are often compared with subsequent values at a later time, when it is necessary to decide whether the disease is stable or progressive, responding to treatment, or getting worse.
Monoclonal Gammopathy of Undetermined Significance (MGUS)
Patients with MGUS have an M protein in the serum without findings of multiple myeloma, macroglobulinemia, amyloidosis, or lymphoma and have fewer than 10% of plasma cells in the bone marrow.[2,23–25] Patients with smoldering myeloma have similar characteristics but may have more than 10% of plasma cells in the bone marrow.
These types of patients are asymptomatic and do not need to be treated. However, patients with MGUS and risk factors for disease progression must be followed carefully because they are more likely to develop myeloma (most commonly), amyloidosis, lymphoplasmacytic lymphoma, or chronic lymphocytic leukemia. These patients may then require therapy.[25–27]
Virtually all cases of multiple myeloma are preceded by a gradually rising level of MGUS.[28–30] The annual risk of progression of MGUS to a lymphoid or plasma cell malignancy ranges from 0.5% to 1.0% in population-based cohorts.[31,32] This risk ranges from 2% to more than 20% in higher-risk patients.
The following risk factors predict disease progression:
A high level of serum M protein (≥1.5 g/dL).[31,33]
A Swedish cohort study confirmed that an abnormal serum FLC ratio and a high level of serum monoclonal protein are high-risk factors.[32] The study described the additional risk factor of immunoparesis, which is defined as the reciprocal depression of the other Ig classes (i.e., if a patient has an IgG kappa M protein, the IgM and IgA would be below normal levels with immunoparesis). Incorporation of gene-expression profiles to better assess risk is under clinical evaluation.[34]
Monoclonal gammopathies that cause organ damage, particularly to the kidney, heart, or peripheral nerves, require immediate therapy with the same strategies applied for the conventional plasma-cell dyscrasias.[35] A monoclonal gammopathy causing renal dysfunction—by direct antibody deposition or amyloidosis—is referred to as monoclonal gammopathy of renal significance.[36] Rising serum creatinine, dropping glomerular filtration rates, and increasing urinary–albumin excretion are all parameters that may signify renal damage and are assessed prospectively for high-risk MGUS patients. Although the N-terminal pro-brain natriuretic peptide is a very sensitive marker for amyloid involvement in the heart, the low specificity must be noted. These extra tests are included with the M-protein level, FLC levels, and FLC ratio when following patients with MGUS.[37]
In a retrospective review of 6,399 patients with newly diagnosed multiple myeloma, 44 patients were found to have a biclonal IgG or IgA MGUS. The overall response rate of the myeloma clone to induction therapy was 93%, compared with 64% for the separate-clone MGUS (P = .001).[38][Level of evidence C3] Many MGUS plasma cell clones were unresponsive to available myeloma therapy; this result highlights the need to lower expectations for response in situations in which an MGUS may require therapy because of end-organ damage.
Isolated Plasmacytoma of Bone
The patient has an isolated plasmacytoma of the bone if the following are found:
A solitary lytic lesion of plasma cells on skeletal survey in an otherwise asymptomatic patient.
A bone marrow examination from an uninvolved site contains less than 10% plasma cells.[39–41] The absence of plasma cells on flow cytometry of the bone marrow suggests a low (<10%) risk of recurrence after radiation therapy of the isolated bone plasmacytoma.[42]
MRI may reveal unsuspected bony lesions that were undetected on standard radiographs. MRI scans of the total spine and pelvis may identify other bony lesions.[43]
Extramedullary Plasmacytoma
A patient has extramedullary plasmacytoma if the following are found:
Isolated plasma-cell tumors of soft tissues, most commonly occurring in the tonsils, nasopharynx, or paranasal sinuses.
Negative findings on skeletal x-rays and bone marrow biopsy.[44–46]
Multiple Myeloma
Multiple myeloma is a systemic malignancy of plasma cells that typically involves multiple sites within the bone marrow and secretes all or part of a monoclonal antibody.
Prognosis
Multiple myeloma is highly treatable but rarely curable. The median survival in the prechemotherapy era was about 7 months. After the introduction of chemotherapy, prognosis improved significantly with a median survival of 24 to 30 months and a 10-year survival rate of 3%. Even further improvements in prognosis have occurred because of the introduction of newer biological therapies and better salvage options, with median survivals now exceeding 10 years.[47] Patients with plasma cell leukemia or with soft tissue plasmacytomas (often with plasmablastic morphology) in association with multiple myeloma have poor outcomes.[21,48] Racial disparities because of socioeconomic factors, genetics, differences in risk factor exposure, and structural racism are under evaluation.[49]
Multiple myeloma is potentially curable when it presents as a solitary plasmacytoma of bone or as an extramedullary plasmacytoma. For more information, see the sections on Isolated Plasmacytoma of Bone and Extramedullary Plasmacytoma.
Amyloidosis Associated With Plasma Cell Neoplasms
Multiple myeloma and other plasma cell neoplasms may cause a condition called amyloidosis. Primary amyloidosis can result in severe organ dysfunction, especially in the kidney, heart, or peripheral nerves.[50] Clinical symptoms and signs include:
Fatigue.
Purpura.
Enlarged tongue.
Diarrhea.
Edema.
Lower-extremity paresthesia.
Accurate diagnosis of amyloidosis requires histological evidence of amyloid deposits and characterization of the amyloidogenic protein using immunoelectron microscopy.[51] In one series of 745 consecutive patients, 20% of patients with nonamyloid light chain amyloidosis (usually transthyretin) had an innocent monoclonal gammopathy, indicating the significant risk of misdiagnosis.[51]
Elevated serum levels of cardiac troponins, amino-terminal fragment brain-type natriuretic peptide, and serum FLC are poor prognostic factors.[52,53] Proposed staging systems for primary systemic amyloidosis based on these serum levels require independent and prospective confirmation.[52,54] An increase in levels of serum FLC over many years can precede the clinical diagnosis of amyloid light chain amyloidosis.[55] Amyloidosis associated with an IgM monoclonal gammopathy is a rare, but distinct, clinical entity with more frequent neuropathy and adenopathy and less cardiac involvement.[56]
POEMS Syndrome
POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) syndrome is a rare paraneoplastic condition associated with a plasma cell dyscrasia of early or late stage. The acronym describes a constellation of findings often marked by polyneuropathy, organomegaly (usually splenomegaly), endocrinopathy, monoclonal plasma cell dyscrasia, and skin changes.[57] Both sclerotic or lytic bone lesions and lymphadenopathy (with possible Castleman histology) may be identified. Anecdotal reports suggest remissions have been achieved using myeloma-directed therapy.[58–62]
References
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Kyle RA, Rajkumar SV: Monoclonal gammopathy of undetermined significance and smouldering multiple myeloma: emphasis on risk factors for progression. Br J Haematol 139 (5): 730-43, 2007. [PUBMED Abstract]
Knowling MA, Harwood AR, Bergsagel DE: Comparison of extramedullary plasmacytomas with solitary and multiple plasma cell tumors of bone. J Clin Oncol 1 (4): 255-62, 1983. [PUBMED Abstract]
Zandecki M, Facon T, Preudhomme C, et al.: Significance of circulating plasma cells in multiple myeloma. Leuk Lymphoma 14 (5-6): 491-6, 1994. [PUBMED Abstract]
Billadeau D, Van Ness B, Kimlinger T, et al.: Clonal circulating cells are common in plasma cell proliferative disorders: a comparison of monoclonal gammopathy of undetermined significance, smoldering multiple myeloma, and active myeloma. Blood 88 (1): 289-96, 1996. [PUBMED Abstract]
He Y, Wheatley K, Clark O, et al.: Early versus deferred treatment for early stage multiple myeloma. Cochrane Database Syst Rev (1): CD004023, 2003. [PUBMED Abstract]
Kyle RA, Remstein ED, Therneau TM, et al.: Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med 356 (25): 2582-90, 2007. [PUBMED Abstract]
Vaxman I, Gertz MA: How I approach smoldering multiple myeloma. Blood 140 (8): 828-838, 2022. [PUBMED Abstract]
Riches PG, Sheldon J, Smith AM, et al.: Overestimation of monoclonal immunoglobulin by immunochemical methods. Ann Clin Biochem 28 ( Pt 3): 253-9, 1991. [PUBMED Abstract]
Dispenzieri A, Kyle R, Merlini G, et al.: International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia 23 (2): 215-24, 2009. [PUBMED Abstract]
Larsen JT, Kumar SK, Dispenzieri A, et al.: Serum free light chain ratio as a biomarker for high-risk smoldering multiple myeloma. Leukemia 27 (4): 941-6, 2013. [PUBMED Abstract]
Horger M, Kanz L, Denecke B, et al.: The benefit of using whole-body, low-dose, nonenhanced, multidetector computed tomography for follow-up and therapy response monitoring in patients with multiple myeloma. Cancer 109 (8): 1617-26, 2007. [PUBMED Abstract]
Walker R, Barlogie B, Haessler J, et al.: Magnetic resonance imaging in multiple myeloma: diagnostic and clinical implications. J Clin Oncol 25 (9): 1121-8, 2007. [PUBMED Abstract]
Kyle RA, Durie BG, Rajkumar SV, et al.: Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management. Leukemia 24 (6): 1121-7, 2010. [PUBMED Abstract]
Moreau P, Attal M, Caillot D, et al.: Prospective Evaluation of Magnetic Resonance Imaging and [18F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients With Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J Clin Oncol 35 (25): 2911-2918, 2017. [PUBMED Abstract]
Zamagni E, Tacchetti P, Cavo M: Imaging in multiple myeloma: How? When? Blood 133 (7): 644-651, 2019. [PUBMED Abstract]
Gertz MA, Li CY, Shirahama T, et al.: Utility of subcutaneous fat aspiration for the diagnosis of systemic amyloidosis (immunoglobulin light chain). Arch Intern Med 148 (4): 929-33, 1988. [PUBMED Abstract]
Greipp PR: Advances in the diagnosis and management of myeloma. Semin Hematol 29 (3 Suppl 2): 24-45, 1992. [PUBMED Abstract]
Durie BG, Stock-Novack D, Salmon SE, et al.: Prognostic value of pretreatment serum beta 2 microglobulin in myeloma: a Southwest Oncology Group Study. Blood 75 (4): 823-30, 1990. [PUBMED Abstract]
Garcés JJ, Cedena MT, Puig N, et al.: Circulating Tumor Cells for the Staging of Patients With Newly Diagnosed Transplant-Eligible Multiple Myeloma. J Clin Oncol 40 (27): 3151-3161, 2022. [PUBMED Abstract]
Pagano L, Valentini CG, De Stefano V, et al.: Primary plasma cell leukemia: a retrospective multicenter study of 73 patients. Ann Oncol 22 (7): 1628-35, 2011. [PUBMED Abstract]
Royer B, Minvielle S, Diouf M, et al.: Bortezomib, Doxorubicin, Cyclophosphamide, Dexamethasone Induction Followed by Stem Cell Transplantation for Primary Plasma Cell Leukemia: A Prospective Phase II Study of the Intergroupe Francophone du Myélome. J Clin Oncol 34 (18): 2125-32, 2016. [PUBMED Abstract]
Kyle RA, Therneau TM, Rajkumar SV, et al.: Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med 354 (13): 1362-9, 2006. [PUBMED Abstract]
International Myeloma Working Group: Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol 121 (5): 749-57, 2003. [PUBMED Abstract]
Bird J, Behrens J, Westin J, et al.: UK Myeloma Forum (UKMF) and Nordic Myeloma Study Group (NMSG): guidelines for the investigation of newly detected M-proteins and the management of monoclonal gammopathy of undetermined significance (MGUS). Br J Haematol 147 (1): 22-42, 2009. [PUBMED Abstract]
Attal M, Harousseau JL, Stoppa AM, et al.: A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Français du Myélome. N Engl J Med 335 (2): 91-7, 1996. [PUBMED Abstract]
Kyle RA, Therneau TM, Rajkumar SV, et al.: A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 346 (8): 564-9, 2002. [PUBMED Abstract]
Weiss BM, Abadie J, Verma P, et al.: A monoclonal gammopathy precedes multiple myeloma in most patients. Blood 113 (22): 5418-22, 2009. [PUBMED Abstract]
Landgren O, Kyle RA, Pfeiffer RM, et al.: Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: a prospective study. Blood 113 (22): 5412-7, 2009. [PUBMED Abstract]
Bladé J, Rosiñol L, Cibeira MT: Are all myelomas preceded by MGUS? Blood 113 (22): 5370, 2009. [PUBMED Abstract]
Rajkumar SV, Kyle RA, Therneau TM, et al.: Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance. Blood 106 (3): 812-7, 2005. [PUBMED Abstract]
Turesson I, Kovalchik SA, Pfeiffer RM, et al.: Monoclonal gammopathy of undetermined significance and risk of lymphoid and myeloid malignancies: 728 cases followed up to 30 years in Sweden. Blood 123 (3): 338-45, 2014. [PUBMED Abstract]
Kyle RA, Larson DR, Therneau TM, et al.: Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance. N Engl J Med 378 (3): 241-249, 2018. [PUBMED Abstract]
Dhodapkar MV, Sexton R, Waheed S, et al.: Clinical, genomic, and imaging predictors of myeloma progression from asymptomatic monoclonal gammopathies (SWOG S0120). Blood 123 (1): 78-85, 2014. [PUBMED Abstract]
Fermand JP, Bridoux F, Dispenzieri A, et al.: Monoclonal gammopathy of clinical significance: a novel concept with therapeutic implications. Blood 132 (14): 1478-1485, 2018. [PUBMED Abstract]
Leung N, Bridoux F, Nasr SH: Monoclonal Gammopathy of Renal Significance. N Engl J Med 384 (20): 1931-1941, 2021. [PUBMED Abstract]
Merlini G: Determining the significance of MGUS. Blood 123 (3): 305-7, 2014. [PUBMED Abstract]
Campbell JP, Heaney JLJ, Pandya S, et al.: Response comparison of multiple myeloma and monoclonal gammopathy of undetermined significance to the same anti-myeloma therapy: a retrospective cohort study. Lancet Haematol 4 (12): e584-e594, 2017. [PUBMED Abstract]
Ozsahin M, Tsang RW, Poortmans P, et al.: Outcomes and patterns of failure in solitary plasmacytoma: a multicenter Rare Cancer Network study of 258 patients. Int J Radiat Oncol Biol Phys 64 (1): 210-7, 2006. [PUBMED Abstract]
Dimopoulos MA, Moulopoulos LA, Maniatis A, et al.: Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood 96 (6): 2037-44, 2000. [PUBMED Abstract]
Dimopoulos MA, Hamilos G: Solitary bone plasmacytoma and extramedullary plasmacytoma. Curr Treat Options Oncol 3 (3): 255-9, 2002. [PUBMED Abstract]
Paiva B, Chandia M, Vidriales MB, et al.: Multiparameter flow cytometry for staging of solitary bone plasmacytoma: new criteria for risk of progression to myeloma. Blood 124 (8): 1300-3, 2014. [PUBMED Abstract]
Liebross RH, Ha CS, Cox JD, et al.: Solitary bone plasmacytoma: outcome and prognostic factors following radiotherapy. Int J Radiat Oncol Biol Phys 41 (5): 1063-7, 1998. [PUBMED Abstract]
Tournier-Rangeard L, Lapeyre M, Graff-Caillaud P, et al.: Radiotherapy for solitary extramedullary plasmacytoma in the head-and-neck region: A dose greater than 45 Gy to the target volume improves the local control. Int J Radiat Oncol Biol Phys 64 (4): 1013-7, 2006. [PUBMED Abstract]
Michalaki VJ, Hall J, Henk JM, et al.: Definitive radiotherapy for extramedullary plasmacytomas of the head and neck. Br J Radiol 76 (910): 738-41, 2003. [PUBMED Abstract]
Alexiou C, Kau RJ, Dietzfelbinger H, et al.: Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer 85 (11): 2305-14, 1999. [PUBMED Abstract]
Joseph NS, Kaufman JL, Dhodapkar MV, et al.: Long-Term Follow-Up Results of Lenalidomide, Bortezomib, and Dexamethasone Induction Therapy and Risk-Adapted Maintenance Approach in Newly Diagnosed Multiple Myeloma. J Clin Oncol 38 (17): 1928-1937, 2020. [PUBMED Abstract]
Bladé J, Fernández de Larrea C, Rosiñol L, et al.: Soft-tissue plasmacytomas in multiple myeloma: incidence, mechanisms of extramedullary spread, and treatment approach. J Clin Oncol 29 (28): 3805-12, 2011. [PUBMED Abstract]
Marinac CR, Ghobrial IM, Birmann BM, et al.: Dissecting racial disparities in multiple myeloma. Blood Cancer J 10 (2): 19, 2020. [PUBMED Abstract]
Gertz MA, Dispenzieri A: Systemic Amyloidosis Recognition, Prognosis, and Therapy: A Systematic Review. JAMA 324 (1): 79-89, 2020. [PUBMED Abstract]
Fernández de Larrea C, Verga L, Morbini P, et al.: A practical approach to the diagnosis of systemic amyloidoses. Blood 125 (14): 2239-44, 2015. [PUBMED Abstract]
Kumar S, Dispenzieri A, Lacy MQ, et al.: Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements. J Clin Oncol 30 (9): 989-95, 2012. [PUBMED Abstract]
Pinney JH, Lachmann HJ, Bansi L, et al.: Outcome in renal Al amyloidosis after chemotherapy. J Clin Oncol 29 (6): 674-81, 2011. [PUBMED Abstract]
Lilleness B, Ruberg FL, Mussinelli R, et al.: Development and validation of a survival staging system incorporating BNP in patients with light chain amyloidosis. Blood 133 (3): 215-223, 2019. [PUBMED Abstract]
Weiss BM, Hebreo J, Cordaro DV, et al.: Increased serum free light chains precede the presentation of immunoglobulin light chain amyloidosis. J Clin Oncol 32 (25): 2699-704, 2014. [PUBMED Abstract]
Sachchithanantham S, Roussel M, Palladini G, et al.: European Collaborative Study Defining Clinical Profile Outcomes and Novel Prognostic Criteria in Monoclonal Immunoglobulin M-Related Light Chain Amyloidosis. J Clin Oncol 34 (17): 2037-45, 2016. [PUBMED Abstract]
Dispenzieri A: POEMS syndrome: 2011 update on diagnosis, risk-stratification, and management. Am J Hematol 86 (7): 591-601, 2011. [PUBMED Abstract]
Humeniuk MS, Gertz MA, Lacy MQ, et al.: Outcomes of patients with POEMS syndrome treated initially with radiation. Blood 122 (1): 68-73, 2013. [PUBMED Abstract]
Li J, Zhang W, Jiao L, et al.: Combination of melphalan and dexamethasone for patients with newly diagnosed POEMS syndrome. Blood 117 (24): 6445-9, 2011. [PUBMED Abstract]
Royer B, Merlusca L, Abraham J, et al.: Efficacy of lenalidomide in POEMS syndrome: a retrospective study of 20 patients. Am J Hematol 88 (3): 207-12, 2013. [PUBMED Abstract]
Misawa S, Sato Y, Katayama K, et al.: Safety and efficacy of thalidomide in patients with POEMS syndrome: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol 15 (11): 1129-37, 2016. [PUBMED Abstract]
Zhao H, Huang XF, Gao XM, et al.: What is the best first-line treatment for POEMS syndrome: autologous transplantation, melphalan and dexamethasone, or lenalidomide and dexamethasone? Leukemia 33 (4): 1023-1029, 2019. [PUBMED Abstract]
Stage Information for Plasma Cell Neoplasms
No generally accepted staging system exists for monoclonal gammopathy of undetermined significance, isolated plasmacytoma of bone, or extramedullary plasmacytoma. Of the plasma cell neoplasms, a staging system exists only for multiple myeloma.
Multiple Myeloma
Multiple myeloma is staged by estimating the myeloma tumor cell mass based on the amount of monoclonal (or myeloma) protein (M protein) in the serum and/or urine, along with various clinical parameters, such as hemoglobin and serum calcium concentrations, the number of lytic bone lesions, and the presence or absence of renal failure. Impaired renal function worsens prognosis regardless of stage.[1]
The stage of the disease at presentation is a strong determinant of survival, but it has little influence on the choice of therapy because almost all patients, except for rare patients with solitary bone tumors or extramedullary plasmacytomas, have generalized disease.
International staging system
The International Myeloma Working Group (IMWG) studied 11,171 patients, 2,901 of whom received high-dose therapy and 8,270 of whom received only standard-dose therapy.[2] The IMWG evaluated 4,445 patients to create a Revised International Staging System (R-ISS) incorporating lactate dehydrogenase levels and interphase fluorescence in situ hybridization (I-FISH) results.[3]
An International Staging System (ISS) was derived and is shown below in Table 2.[2]
Table 2. The International Staging System (ISS) for Multiple Myeloma
Stage
Criteria
Median Survival (mo)
I-FISH = interphase fluorescence in situ hybridization; LDH = lactate dehydrogenase; R-ISS = Revised International Staging System.
I
Beta-2-microglobulin <3.5 mg/L and albumin ≥3.5 g/dL
Not reached
II
Not R-ISS I or III
83
III
Beta-2-microglobulin ≥5.5 mg/L and either high LDH or high-risk chromosomal abnormalities by I-FISH (defined as presence of del(17p) and/or translocation t(4;14) and/or translocation t(14;16))
43
Genetic factors and risk groups
Newer clinical investigations are stratifying patients with multiple myeloma into so-called good-risk, intermediate-risk, and high-risk groups, based on genetic aberrations detected by I-FISH.[4–6] (See Table 3 below.) This stratification, based on cytogenetic findings, has been derived from retrospective analyses and requires prospective validation.[4] Bone marrow samples are sent for cytogenetic and FISH analysis.[6] Plasma cell leukemia (>2%–5% circulating plasma cells) has a particularly poor prognosis.[7–13] The otherwise favorable prognosis of hyperploidy is trumped by coexistent adverse cytogenetics.[14]
Table 3. Risk Groups for Multiple Myeloma
Risk Group
Cytogenetic Findings
Disease Characteristics
Median Survival (y)
FISH = fluorescence in situ hybridization; Ig = immunoglobulin.
Good risk
Has any of the following cytogenetic findings:
These patients most often have disease that expresses IgG kappa monoclonal gammopathies, and lytic bone lesions.
1q gain (3 copies), 1 q amp (4 copies, ultra-high risk), monoallelic del (1p32),[17] biallelic del (1p32)[17]
Plasma cell leukemia
References
Royal V, Leung N, Troyanov S, et al.: Clinicopathologic predictors of renal outcomes in light chain cast nephropathy: a multicenter retrospective study. Blood 135 (21): 1833-1846, 2020. [PUBMED Abstract]
Greipp PR, San Miguel J, Durie BG, et al.: International staging system for multiple myeloma. J Clin Oncol 23 (15): 3412-20, 2005. [PUBMED Abstract]
Palumbo A, Avet-Loiseau H, Oliva S, et al.: Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol 33 (26): 2863-9, 2015. [PUBMED Abstract]
Kumar SK, Mikhael JR, Buadi FK, et al.: Management of newly diagnosed symptomatic multiple myeloma: updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) consensus guidelines. Mayo Clin Proc 84 (12): 1095-110, 2009. [PUBMED Abstract]
Avet-Loiseau H, Attal M, Campion L, et al.: Long-term analysis of the IFM 99 trials for myeloma: cytogenetic abnormalities [t(4;14), del(17p), 1q gains] play a major role in defining long-term survival. J Clin Oncol 30 (16): 1949-52, 2012. [PUBMED Abstract]
Sonneveld P, Avet-Loiseau H, Lonial S, et al.: Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group. Blood 127 (24): 2955-62, 2016. [PUBMED Abstract]
Ramsingh G, Mehan P, Luo J, et al.: Primary plasma cell leukemia: a Surveillance, Epidemiology, and End Results database analysis between 1973 and 2004. Cancer 115 (24): 5734-9, 2009. [PUBMED Abstract]
Fernández de Larrea C, Kyle RA, Durie BG, et al.: Plasma cell leukemia: consensus statement on diagnostic requirements, response criteria and treatment recommendations by the International Myeloma Working Group. Leukemia 27 (4): 780-91, 2013. [PUBMED Abstract]
Granell M, Calvo X, Garcia-Guiñón A, et al.: Prognostic impact of circulating plasma cells in patients with multiple myeloma: implications for plasma cell leukemia definition. Haematologica 102 (6): 1099-1104, 2017. [PUBMED Abstract]
Mina R, Joseph NS, Kaufman JL, et al.: Survival outcomes of patients with primary plasma cell leukemia (pPCL) treated with novel agents. Cancer 125 (3): 416-423, 2019. [PUBMED Abstract]
Royer B, Minvielle S, Diouf M, et al.: Bortezomib, Doxorubicin, Cyclophosphamide, Dexamethasone Induction Followed by Stem Cell Transplantation for Primary Plasma Cell Leukemia: A Prospective Phase II Study of the Intergroupe Francophone du Myélome. J Clin Oncol 34 (18): 2125-32, 2016. [PUBMED Abstract]
Gonsalves WI, Rajkumar SV, Go RS, et al.: Trends in survival of patients with primary plasma cell leukemia: a population-based analysis. Blood 124 (6): 907-12, 2014. [PUBMED Abstract]
Jelinek T, Bezdekova R, Zihala D, et al.: More Than 2% of Circulating Tumor Plasma Cells Defines Plasma Cell Leukemia-Like Multiple Myeloma. J Clin Oncol 41 (7): 1383-1392, 2023. [PUBMED Abstract]
Pawlyn C, Melchor L, Murison A, et al.: Coexistent hyperdiploidy does not abrogate poor prognosis in myeloma with adverse cytogenetics and may precede IGH translocations. Blood 125 (5): 831-40, 2015. [PUBMED Abstract]
Davies FE, Pawlyn C, Usmani SZ, et al.: Perspectives on the Risk-Stratified Treatment of Multiple Myeloma. Blood Cancer Discov 3 (4): 273-284, 2022. [PUBMED Abstract]
Khot A: Del(1p32): prime time in (ultra) high-risk myeloma. Blood 141 (11): 1241-1243, 2023. [PUBMED Abstract]
Schavgoulidze A, Talbot A, Perrot A, et al.: Biallelic deletion of 1p32 defines ultra-high-risk myeloma, but monoallelic del(1p32) remains a strong prognostic factor. Blood 141 (11): 1308-1315, 2023. [PUBMED Abstract]
Treatment Option Overview for Plasma Cell Neoplasms
The major challenge in treating plasma cell neoplasms is separating the stable asymptomatic patients who do not require immediate treatment from patients with progressive symptomatic myeloma who may need to be treated immediately.[1–3] Monoclonal gammopathy of undetermined significance or smoldering myeloma must be distinguished from progressive myeloma.
Asymptomatic patients with multiple myeloma who have no lytic bone lesions and normal renal function may be initially observed safely outside the context of a clinical trial.[1,4,5] Increasing anemia is the most reliable indicator of progression.[5] The following criteria represent the new definition for smoldering myeloma:[3]
Serum monoclonal protein immunoglobulin (Ig) G or IgA of at least 30 g/L or urinary monoclonal protein of at least 500 mg per 24 hours.
Clonal bone marrow plasma cells 10% to 60% (>60% represents overt myeloma).
Absence of amyloidosis or myeloma-defining events as follows:
Hypercalcemia greater than 1 mg/dL higher than reference range.
Creatinine greater than 2 mg/dL or creatinine clearance less than 40 mL/min.
Anemia with hemoglobin less than 10.0 g/dL.
Bone lesions (one or more) on skeletal radiography, computed tomography (CT) or positron emission tomography (PET)-CT.
Clonal plasma cell percentage in marrow at 60% or more.
Involved:uninvolved serum free light chain (FLC) ratio of 100 or more.
More than one focal lesion of at least 5 mm on magnetic resonance imaging (MRI) of the spine.
The International Myeloma Working Group (IMWG) 2/20/20 rule measures four adverse risk factors for patients with smoldering myeloma. The presence of three or four of the following adverse factors predicts a greater than 50% chance of progression to myeloma within 2 years:[6]
Serum monoclonal (or myeloma) protein (M protein) greater than 2 g/dL.
Involved:uninvolved serum FLC ratio of more than 20.
Bone marrow plasma cell infiltration of more than 20%.
t(4;14), t(14;16), 1q gain, or del13q/monosomy 13 chromosomal abnormality.
Clinical trials evaluating smoldering myeloma need to exclude patients at high risk of progression to myeloma because those patients should consider induction therapy for symptomatic patients. For more information, see the Symptomatic Plasma Cell Neoplasms section.
In a prospective randomized trial of 390 patients with smoldering myeloma, patients were eligible if the marrow plasmacytosis was 10% to 49% and one of the following criteria was met:
M protein of at least 3 g/dL.
Immunoparesis of two Ig classes.
Involved:uninvolved serum FLC ratio of 8 to 99.
IgA monoclonal protein.
Marrow plasmacytosis of 50% to 59%.
These patients received daratumumab (the anti-CD38 monoclonal antibody) or no therapy.[7]
With a median follow-up of 65.2 months, the 5-year progression-free survival rate was 63.1% for patients in the daratumumab arm and 40.8% for patients in the watchful waiting arm (hazard ratio [HR], 0.49; 95% confidence interval [CI], 0.36–0.67; P < .0001).[7][Level of evidence B1]
The median time to progression was 44.1 months for patients in the daratumumab arm and 17.8 months for patients in the watchful waiting arm (HR, 0.51; 95% CI, 0.40–0.66; P < .0001).
The 5-year overall survival (OS) rate was 93% for patients in the daratumumab arm and 86% for patients in the watchful waiting arm (HR, 0.52; 95% CI, 0.27–0.98).
Three quality-of-life assessments showed no difference between the arms.
Summary: This trial did not show a significant improvement in OS or quality of life. However, the significant and clinically relevant delay in progression may particularly benefit older, less fit patients with myeloma. Early use of daratumumab did not result in a shortened OS after the subsequent initiation of full-dose induction therapy.
Symptomatic Plasma Cell Neoplasms
Patients with symptomatic advanced disease require treatment.
Treatment most often is directed at reducing the tumor cell burden and reversing any complications of disease, such as renal failure, infection, hyperviscosity, or hypercalcemia, with appropriate medical management. The IMWG has published new criteria for identifying patients with active myeloma who require therapy:[3]
Amyloidosis.
Hypercalcemia greater than 1 mg/dL higher than reference range.
Creatinine greater than 2 mg/dL or creatinine clearance less than 40 mL/min. Myeloma can cause renal dysfunction via hypercalcemia, amyloidosis, or light chain deposition disease.[8]
Anemia with hemoglobin less than 10.0 g/dL.
Bone lesions (one or more) on skeletal radiography, whole-body MRI or spine and pelvis MRI, or PET-CT scans.[9]
Clonal plasma cell percentage in marrow at 60% or more.
Involved:uninvolved serum FLC ratio of 100 or more.
More than one focal lesion of at least 5 mm on skeletal bone survey, or if negative, total-body MRI, or MRI of the spine and pelvis, or PET-CT scan.
Response criteria have been developed for patients on clinical trials by the IMWG.[10] A very good partial response (VGPR) is defined as a reduction of 90% or more in the serum monoclonal protein and a 24-hour urine monoclonal protein of less than 100 mg. Although not incorporated in the IMWG criteria, many trials report near complete response when patients have less than 5% bone marrow plasma cells and unmeasurable serum monoclonal proteins but still have positive serum and/or urine immunofixation. Note that these near complete response patients are incorporated into the VGPR group by the IMWG. Patients who achieve a complete response by IMWG criteria (with a negative immunofixation along with the clear marrow and unmeasurable serum monoclonal proteins) are often said to have attained a stringent complete response if their free kappa/lambda light–chain levels and ratio return to reference ranges. The clinical utility of these various categories must be validated in clinical trials.
Therapy options for patients with symptomatic myeloma include:
Induction therapies.
Consolidation therapies, which are less applicable for patients of advanced age.
Infection prevention, which includes vaccination, antimicrobial prophylaxis, and immunoglobulin replacement (in a small subset of patients), per consensus guidelines from the IMWG.[11]
References
He Y, Wheatley K, Clark O, et al.: Early versus deferred treatment for early stage multiple myeloma. Cochrane Database Syst Rev (1): CD004023, 2003. [PUBMED Abstract]
Kyle RA, Remstein ED, Therneau TM, et al.: Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med 356 (25): 2582-90, 2007. [PUBMED Abstract]
Rajkumar SV, Dimopoulos MA, Palumbo A, et al.: International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 15 (12): e538-48, 2014. [PUBMED Abstract]
Riccardi A, Mora O, Tinelli C, et al.: Long-term survival of stage I multiple myeloma given chemotherapy just after diagnosis or at progression of the disease: a multicentre randomized study. Cooperative Group of Study and Treatment of Multiple Myeloma. Br J Cancer 82 (7): 1254-60, 2000. [PUBMED Abstract]
Bladé J, Dimopoulos M, Rosiñol L, et al.: Smoldering (asymptomatic) multiple myeloma: current diagnostic criteria, new predictors of outcome, and follow-up recommendations. J Clin Oncol 28 (4): 690-7, 2010. [PUBMED Abstract]
Mateos MV, Kumar S, Dimopoulos MA, et al.: International Myeloma Working Group risk stratification model for smoldering multiple myeloma (SMM). Blood Cancer J 10 (10): 102, 2020. [PUBMED Abstract]
Dimopoulos MA, Voorhees PM, Schjesvold F, et al.: Daratumumab or Active Monitoring for High-Risk Smoldering Multiple Myeloma. N Engl J Med 392 (18): 1777-1788, 2025. [PUBMED Abstract]
Sayed RH, Wechalekar AD, Gilbertson JA, et al.: Natural history and outcome of light chain deposition disease. Blood 126 (26): 2805-10, 2015. [PUBMED Abstract]
Dimopoulos MA, Hillengass J, Usmani S, et al.: Role of magnetic resonance imaging in the management of patients with multiple myeloma: a consensus statement. J Clin Oncol 33 (6): 657-64, 2015. [PUBMED Abstract]
Durie BG, Harousseau JL, Miguel JS, et al.: International uniform response criteria for multiple myeloma. Leukemia 20 (9): 1467-73, 2006. [PUBMED Abstract]
Raje NS, Anaissie E, Kumar SK, et al.: Consensus guidelines and recommendations for infection prevention in multiple myeloma: a report from the International Myeloma Working Group. Lancet Haematol 9 (2): e143-e161, 2022. [PUBMED Abstract]
Treatment of Amyloidosis Associated With Plasma Cell Neoplasms
Treatment Options for Amyloidosis Associated With Plasma Cell Neoplasms
Treatment depends on assessing the extent of systemic damage from the amyloidosis and the underlying plasma cell dyscrasia.[1,2] A rising and elevated level of N-terminal pro-brain natriuretic peptide (NT-proBNP) may predict impending cardiac failure in cases of cardiac amyloidosis, and early treatment should be considered for these patients.[3]
Treatment options for amyloidosis associated with plasma cell neoplasms include:
As is true for all plasma cell dyscrasias, responses have been reported for patients treated with all the same regimens active in multiple myeloma.[4–12] Lower doses of lenalidomide or pomalidomide must be used in patients with renal dysfunction.[13] Patients with amyloidosis respond to treatment with daratumumab, with or without other active agents. Daratumumab is usually combined with other agents used for myeloma.[14–20] Rapid responses to induction therapy may result in improvement of renal or cardiac function.[21,22]
Evidence (chemotherapy):
A prospective trial (NCT03201965) included 388 previously untreated patients with immunoglobulin light-chain amyloidosis (excluding symptomatic myeloma). Patients were randomly assigned to receive bortezomib, cyclophosphamide, and dexamethasone with or without subcutaneous daratumumab.[23]
With a median follow-up of 11.4 months, the hematologic complete response rate was 53% for patients in the daratumumab group and 18.1% for patients in the control group (relative risk, 2.9; 95% confidence interval [CI], 2.1–4.1; P < .001). A landmark analysis at 6 months was also performed.[23][Level of evidence B3]
Survival free from organ deterioration, hematologic progression, or death favored the daratumumab arm (hazard ratio, 0.58; 95% CI, 0.36–0.93; P = .02).
The cardiac and renal responses were doubled for patients in the daratumumab group, but no statistical analysis was provided.
Daratumumab combined with bortezomib, cyclophosphamide, and dexamethasone is considered a standard regimen for previously untreated patients who are eligible to receive this regimen. When using daratumumab induction therapy, the fluorescence in situ hybridization–detected cytogenetic abnormality of t(11;14) no longer confers an adverse prognostic impact. However, the presence of 1q gain continues to be associated with a lower response rate and hematologic event-free survival during treatment of amyloid light chain amyloidosis.[24]
Stem cell rescue
A prospective randomized study of 100 patients with immunoglobulin light-chain amyloidosis compared melphalan plus high-dose dexamethasone with high-dose melphalan plus autologous stem cell rescue.[25] After a median follow-up of 3 years, median overall survival (OS) favored the nontransplant arm (56.9 months vs. 22.2 months; P = .04).[25][Level of evidence A1] The 24% transplant-related mortality in this series and others reflects the difficulties involved with high-dose chemotherapy in older patients with organ dysfunction.[25–30] Between 2007 and 2012, the International Blood and Marrow Transplant Research Program identified 800 patients with amyloidosis who underwent autologous stem cell transplant (SCT); the 5-year OS rate was 77% and the transplant-related mortality rate was 5%, suggesting better selection of patients for transplant.[31][Level of evidence C1] Similarly, in a retrospective review of 672 consecutive patients with amyloidosis who underwent autologous SCT over 20 years, the treatment-related mortality rate declined to 2.4% between 2010 and 2016, compared with rates of 8.6% between 2003 and 2009 and 14.5% between 1996 and 2002.[32][Level of evidence C2] A randomized trial confirming the benefit of autologous SCT is not anticipated.[3,33]
An anecdotal series described full-intensity and reduced-intensity allogeneic SCT.[34]
Monoclonal antibody targeting of amyloid deposits
The monoclonal antibody anselamimab binds to immunoglobulin-associated amyloid in an effort to promote phagocytosis and clearance of the amyloid deposits.
In a phase I study (NCT02245867), 27 patients with deep hematologic responses to myeloma therapy, but persistent organ involvement, received anselamimab.[35]
Fifteen of 24 patients (63%) manifested cardiac, renal, hepatic, gastrointestinal, or soft tissue response by serum biomarkers (such as NT-proBNP), renal function, cardiac function, or imaging studies.
This treatment is not approved by the U.S. Food and Drug Administration and is under clinical evaluation.[35][Level of evidence C3]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Gertz MA, Dispenzieri A: Systemic Amyloidosis Recognition, Prognosis, and Therapy: A Systematic Review. JAMA 324 (1): 79-89, 2020. [PUBMED Abstract]
Palladini G, Merlini G: How I treat AL amyloidosis. Blood 139 (19): 2918-2930, 2022. [PUBMED Abstract]
Kumar SK, Hayman SR, Buadi FK, et al.: Lenalidomide, cyclophosphamide, and dexamethasone (CRd) for light-chain amyloidosis: long-term results from a phase 2 trial. Blood 119 (21): 4860-7, 2012. [PUBMED Abstract]
Venner CP, Lane T, Foard D, et al.: Cyclophosphamide, bortezomib, and dexamethasone therapy in AL amyloidosis is associated with high clonal response rates and prolonged progression-free survival. Blood 119 (19): 4387-90, 2012. [PUBMED Abstract]
Wechalekar AD, Schonland SO, Kastritis E, et al.: A European collaborative study of treatment outcomes in 346 patients with cardiac stage III AL amyloidosis. Blood 121 (17): 3420-7, 2013. [PUBMED Abstract]
Sanchorawala V, Shelton AC, Lo S, et al.: Pomalidomide and dexamethasone in the treatment of AL amyloidosis: results of a phase 1 and 2 trial. Blood 128 (8): 1059-62, 2016. [PUBMED Abstract]
Palladini G, Milani P, Foli A, et al.: Presentation and outcome with second-line treatment in AL amyloidosis previously sensitive to nontransplant therapies. Blood 131 (5): 525-532, 2018. [PUBMED Abstract]
Manwani R, Cohen O, Sharpley F, et al.: A prospective observational study of 915 patients with systemic AL amyloidosis treated with upfront bortezomib. Blood 134 (25): 2271-2280, 2019. [PUBMED Abstract]
Kastritis E, Leleu X, Arnulf B, et al.: Bortezomib, Melphalan, and Dexamethasone for Light-Chain Amyloidosis. J Clin Oncol 38 (28): 3252-3260, 2020. [PUBMED Abstract]
Lentzsch S, Lagos GG, Comenzo RL, et al.: Bendamustine With Dexamethasone in Relapsed/Refractory Systemic Light-Chain Amyloidosis: Results of a Phase II Study. J Clin Oncol 38 (13): 1455-1462, 2020. [PUBMED Abstract]
Dispenzieri A, Kastritis E, Wechalekar AD, et al.: A randomized phase 3 study of ixazomib-dexamethasone versus physician’s choice in relapsed or refractory AL amyloidosis. Leukemia 36 (1): 225-235, 2022. [PUBMED Abstract]
Mikhael J, Manola J, Dueck AC, et al.: Lenalidomide and dexamethasone in patients with relapsed multiple myeloma and impaired renal function: PrE1003, a PrECOG study. Blood Cancer J 8 (9): 86, 2018. [PUBMED Abstract]
Palladini G, Kastritis E, Maurer MS, et al.: Daratumumab plus CyBorD for patients with newly diagnosed AL amyloidosis: safety run-in results of ANDROMEDA. Blood 136 (1): 71-80, 2020. [PUBMED Abstract]
Sanchorawala V, Sarosiek S, Schulman A, et al.: Safety, tolerability, and response rates of daratumumab in relapsed AL amyloidosis: results of a phase 2 study. Blood 135 (18): 1541-1547, 2020. [PUBMED Abstract]
Nooka AK, Kaufman JL, Hofmeister CC, et al.: Daratumumab in multiple myeloma. Cancer 125 (14): 2364-2382, 2019. [PUBMED Abstract]
Dispenzieri A: AL patients don’t dare go without dara. Blood 135 (18): 1509-1510, 2020. [PUBMED Abstract]
Roussel M, Merlini G, Chevret S, et al.: A prospective phase 2 trial of daratumumab in patients with previously treated systemic light-chain amyloidosis. Blood 135 (18): 1531-1540, 2020. [PUBMED Abstract]
Kimmich CR, Terzer T, Benner A, et al.: Daratumumab for systemic AL amyloidosis: prognostic factors and adverse outcome with nephrotic-range albuminuria. Blood 135 (18): 1517-1530, 2020. [PUBMED Abstract]
Royal V, Leung N, Troyanov S, et al.: Clinicopathologic predictors of renal outcomes in light chain cast nephropathy: a multicenter retrospective study. Blood 135 (21): 1833-1846, 2020. [PUBMED Abstract]
Basset M, Milani P, Foli A, et al.: Early cardiac response is possible in stage IIIb cardiac AL amyloidosis and is associated with prolonged survival. Blood 140 (18): 1964-1971, 2022. [PUBMED Abstract]
Muchtar E, Dispenzieri A, Wisniowski B, et al.: Graded Cardiac Response Criteria for Patients With Systemic Light Chain Amyloidosis. J Clin Oncol 41 (7): 1393-1403, 2023. [PUBMED Abstract]
Kastritis E, Palladini G, Minnema MC, et al.: Daratumumab-Based Treatment for Immunoglobulin Light-Chain Amyloidosis. N Engl J Med 385 (1): 46-58, 2021. [PUBMED Abstract]
Chakraborty R, Zanwar S, Hegenbart U, et al.: Prognostic impact of cytogenetic abnormalities detected by FISH in AL amyloidosis with daratumumab-based frontline therapy. Blood 144 (25): 2613-2624, 2024. [PUBMED Abstract]
Jaccard A, Moreau P, Leblond V, et al.: High-dose melphalan versus melphalan plus dexamethasone for AL amyloidosis. N Engl J Med 357 (11): 1083-93, 2007. [PUBMED Abstract]
Dispenzieri A, Kyle RA, Lacy MQ, et al.: Superior survival in primary systemic amyloidosis patients undergoing peripheral blood stem cell transplantation: a case-control study. Blood 103 (10): 3960-3, 2004. [PUBMED Abstract]
Skinner M, Sanchorawala V, Seldin DC, et al.: High-dose melphalan and autologous stem-cell transplantation in patients with AL amyloidosis: an 8-year study. Ann Intern Med 140 (2): 85-93, 2004. [PUBMED Abstract]
Leung N, Leung TR, Cha SS, et al.: Excessive fluid accumulation during stem cell mobilization: a novel prognostic factor of first-year survival after stem cell transplantation in AL amyloidosis patients. Blood 106 (10): 3353-7, 2005. [PUBMED Abstract]
Madan S, Kumar SK, Dispenzieri A, et al.: High-dose melphalan and peripheral blood stem cell transplantation for light-chain amyloidosis with cardiac involvement. Blood 119 (5): 1117-22, 2012. [PUBMED Abstract]
Cibeira MT, Sanchorawala V, Seldin DC, et al.: Outcome of AL amyloidosis after high-dose melphalan and autologous stem cell transplantation: long-term results in a series of 421 patients. Blood 118 (16): 4346-52, 2011. [PUBMED Abstract]
D’Souza A, Dispenzieri A, Wirk B, et al.: Improved Outcomes After Autologous Hematopoietic Cell Transplantation for Light Chain Amyloidosis: A Center for International Blood and Marrow Transplant Research Study. J Clin Oncol 33 (32): 3741-9, 2015. [PUBMED Abstract]
Sidiqi MH, Aljama MA, Buadi FK, et al.: Stem Cell Transplantation for Light Chain Amyloidosis: Decreased Early Mortality Over Time. J Clin Oncol 36 (13): 1323-1329, 2018. [PUBMED Abstract]
Mehta J, Gerta MA, Dispenzieri A: High-dose therapy for amyloidosis: the end of the beginning? Blood 103 (10): 3612-3, 2004.
Schönland SO, Lokhorst H, Buzyn A, et al.: Allogeneic and syngeneic hematopoietic cell transplantation in patients with amyloid light-chain amyloidosis: a report from the European Group for Blood and Marrow Transplantation. Blood 107 (6): 2578-84, 2006. [PUBMED Abstract]
Edwards CV, Rao N, Bhutani D, et al.: Phase 1a/b study of monoclonal antibody CAEL-101 (11-1F4) in patients with AL amyloidosis. Blood 138 (25): 2632-2641, 2021. [PUBMED Abstract]
Treatment of Monoclonal Gammopathy of Undetermined Significance
Treatment Options for Monoclonal Gammopathy of Undetermined Significance (MGUS)
Multiple myeloma, other plasma cell dyscrasia, or lymphoma will develop in 12% of patients by 10 years, 25% of patients by 20 years, and 30% of patients by 25 years.
All patients with MGUS are generally observed to detect increases in monoclonal (M) protein levels and development of a plasma cell dyscrasia. Higher levels of initial M protein levels may correlate with increased risk of progression to multiple myeloma.[1,2] In a large retrospective report, the risk of progression at 20 years was 14% for an initial M protein level of 0.5 g/dL or less, 25% for a level of 1.5 g/dL, 41% for a level of 2.0 g/dL, 49% for a level of 2.5 g/dL, and 64% for a level of 3.0 g/dL.[1]
Treatment is delayed until the disease progresses to the stage that symptoms or signs appear.
Patients with MGUS or smoldering myeloma do not respond more frequently, achieve longer remissions, or have improved survival if chemotherapy is started early while they are still asymptomatic as opposed to waiting for progression before treatment is initiated.[3–6] Newer therapies have not been proven to prevent or delay the progression of MGUS to a plasma cell dyscrasia.[2]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Kyle RA, Therneau TM, Rajkumar SV, et al.: A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 346 (8): 564-9, 2002. [PUBMED Abstract]
Bird J, Behrens J, Westin J, et al.: UK Myeloma Forum (UKMF) and Nordic Myeloma Study Group (NMSG): guidelines for the investigation of newly detected M-proteins and the management of monoclonal gammopathy of undetermined significance (MGUS). Br J Haematol 147 (1): 22-42, 2009. [PUBMED Abstract]
Bladé J, Dimopoulos M, Rosiñol L, et al.: Smoldering (asymptomatic) multiple myeloma: current diagnostic criteria, new predictors of outcome, and follow-up recommendations. J Clin Oncol 28 (4): 690-7, 2010. [PUBMED Abstract]
He Y, Wheatley K, Clark O, et al.: Early versus deferred treatment for early stage multiple myeloma. Cochrane Database Syst Rev (1): CD004023, 2003. [PUBMED Abstract]
Riccardi A, Mora O, Tinelli C, et al.: Long-term survival of stage I multiple myeloma given chemotherapy just after diagnosis or at progression of the disease: a multicentre randomized study. Cooperative Group of Study and Treatment of Multiple Myeloma. Br J Cancer 82 (7): 1254-60, 2000. [PUBMED Abstract]
Kyle RA, Remstein ED, Therneau TM, et al.: Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med 356 (25): 2582-90, 2007. [PUBMED Abstract]
Treatment of Waldenström Macroglobulinemia (Lymphoplasmacytic Lymphoma)
Chemotherapy (if monoclonal [or myeloma] protein [M protein] increases and other evidence of symptomatic multiple myeloma occurs).
Radiation therapy
About 25% of patients have serum and/or urine M protein present. Generally, this disappears after adequate radiation therapy to the lytic lesion.
The survival rate of patients with isolated plasmacytoma of bone treated with radiation therapy to the lesion is greater than 50% at 10 years, which is more favorable than the survival rate of patients with disseminated multiple myeloma.[1]
Chemotherapy
Most patients eventually develop disseminated disease and require chemotherapy. Almost 50% of patients do so within 2 years of diagnosis.[2,3] However, patients with serum paraprotein or Bence Jones protein, who have complete disappearance of these proteins after radiation therapy, may remain free of disease for prolonged periods.[2,4] Patients with a negative flow cytometry on bone marrow examination for plasma cell infiltration are also unlikely to relapse.[5] Patients with progression to multiple myeloma often have good responses to chemotherapy, with a median survival of 63 months after progression.[2,4]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Tsang RW, Gospodarowicz MK, Pintilie M, et al.: Solitary plasmacytoma treated with radiotherapy: impact of tumor size on outcome. Int J Radiat Oncol Biol Phys 50 (1): 113-20, 2001. [PUBMED Abstract]
Liebross RH, Ha CS, Cox JD, et al.: Solitary bone plasmacytoma: outcome and prognostic factors following radiotherapy. Int J Radiat Oncol Biol Phys 41 (5): 1063-7, 1998. [PUBMED Abstract]
Dimopoulos MA, Moulopoulos LA, Maniatis A, et al.: Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood 96 (6): 2037-44, 2000. [PUBMED Abstract]
Dimopoulos MA, Goldstein J, Fuller L, et al.: Curability of solitary bone plasmacytoma. J Clin Oncol 10 (4): 587-90, 1992. [PUBMED Abstract]
Paiva B, Chandia M, Vidriales MB, et al.: Multiparameter flow cytometry for staging of solitary bone plasmacytoma: new criteria for risk of progression to myeloma. Blood 124 (8): 1300-3, 2014. [PUBMED Abstract]
Treatment of Extramedullary Plasmacytoma
Treatment Options for Extramedullary Plasmacytoma
Treatment options for extramedullary plasmacytoma include:
Radiation therapy to the isolated lesion with fields that cover the regional lymph nodes, if possible.[1,2]
In some cases, surgical resection may be considered, but it is usually followed by radiation therapy.[2]
If the presence of monoclonal (or myeloma) protein (M protein) persists or reappears, the patient may need further radiation therapy. In some patients, the plasmacytoma may shrink, but not disappear, and the M protein persists. Close follow-up is generally warranted for these patients. Surgery is often performed if the plasmacytoma is in a site where it can be removed easily (e.g., in the tonsil); the M protein may disappear from the blood or urine. In other cases, persistence or an increasing M protein may herald progression to multiple myeloma.
Chemotherapy is required if the disease progresses and causes symptoms.
Patients with isolated plasma cell tumors of soft tissues, most commonly occurring in the tonsils, nasopharynx, or paranasal sinuses, may need to have skeletal x-rays and bone marrow biopsy (both of which are most often negative) and evaluation for M protein in serum and urine.[1–4]
About 25% of patients have serum and/or urine M protein; this frequently disappears after adequate radiation.
Extramedullary plasmacytoma is a highly curable disease. Progression-free survival rates range from 70% to 87% at 10 to 14 years after treatment with radiation therapy (with or without previous resection).[1,2,5]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Tsang RW, Gospodarowicz MK, Pintilie M, et al.: Solitary plasmacytoma treated with radiotherapy: impact of tumor size on outcome. Int J Radiat Oncol Biol Phys 50 (1): 113-20, 2001. [PUBMED Abstract]
Alexiou C, Kau RJ, Dietzfelbinger H, et al.: Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer 85 (11): 2305-14, 1999. [PUBMED Abstract]
Meis JM, Butler JJ, Osborne BM, et al.: Solitary plasmacytomas of bone and extramedullary plasmacytomas. A clinicopathologic and immunohistochemical study. Cancer 59 (8): 1475-85, 1987. [PUBMED Abstract]
Soesan M, Paccagnella A, Chiarion-Sileni V, et al.: Extramedullary plasmacytoma: clinical behaviour and response to treatment. Ann Oncol 3 (1): 51-7, 1992. [PUBMED Abstract]
Strojan P, Soba E, Lamovec J, et al.: Extramedullary plasmacytoma: clinical and histopathologic study. Int J Radiat Oncol Biol Phys 53 (3): 692-701, 2002. [PUBMED Abstract]
Treatment of Multiple Myeloma
Initial Evaluation
The initial approach to the patient is to evaluate the following parameters:
Detection and quantification of a monoclonal (or myeloma) protein (M protein) in the serum or urine, and possible immunoparesis (suppression of the other uninvolved immunoglobulins [Ig]).[1]
Detection of more than 10% of plasma cells on a bone marrow examination, along with flow cytometry, cytogenetics, and fluorescence in situ hybridization testing.
Detection of lytic bone lesions or generalized osteoporosis in skeletal x-rays, or whole-body or spinal and pelvic magnetic resonance imaging (MRI) scans, or focal bone lesions on positron emission tomography-computed tomography (CT) scan.[2,3]
Presence of soft tissue plasmacytomas.
Serum albumin and beta-2-microglobulin levels.
Detection of free kappa and free lambda serum Ig light chain, with calculation of the serum free light chain ratio.[1,4]
Presence of hypercalcemia.
Detection of renal dysfunction attributable to the plasma cell dyscrasia (induced by gammopathy or amyloidosis).
Presence of anemia.
Presence of circulating plasma cells.
Presence of hyperviscosity. Asymptomatic patients usually respond to myeloma therapy; plasma exchange is indicated with hemorrhagic or central nervous system manifestations.[5]
Treatment selection is influenced by the age and general health of the patient, previous therapy, and the presence of disease complications.[6]
Therapeutic Overview
Despite the introduction of many new therapeutic agents over the past two decades, there is still no confirmed curative approach.
Newly diagnosed patients who require therapy fall into two categories: (1) patients in good or well-controlled health (previously referred to as the fit, transplant-eligible patient) or (2) the less-fit patient with significant comorbidities or advanced age (previously referred to as not transplant eligible). Comorbidities and performance status are important determinants to help decide about fitness of patients at all ages, especially those between the ages of 70 years and 80 years. Nomograms exist for geriatric patients to define life expectancy independent of the myeloma diagnosis.[7] Age, organ dysfunction, and risk of cardiovascular and thrombotic complications influence the choice of induction therapies. These factors are also important when considering consolidation therapies, such as chimeric antigen receptor T-cell therapy, bispecific antibody therapy, and autologous stem cell transplant (SCT) consolidation. Most patients also receive a bisphosphonate or RANKL inhibitor to prevent skeletal-related complications.[8,9]
The International Myeloma Working Group has issued guidance for the diagnosis and management of patients with renal impairment.[10]
Fit patients in good or well-controlled health
Patients in good or well-controlled health may receive induction chemotherapy with a four-drug (quadruplet) or three-drug (triplet) approach that includes bortezomib in the absence of a clinical trial. The most commonly used regimens include:
CyBorD: cyclophosphamide + bortezomib + dexamethasone.[19,20] This regimen is preferred in the presence of significant renal dysfunction (creatinine clearance less than 45 cc/min). If the renal function recovers rapidly, some clinicians switch to VRd.
After 4 to 8 months of therapy, patients with disease response may undergo autologous SCT consolidation.[16,21] The previously standard autologous SCT consolidation has been questioned because a large, prospective, randomized trial failed to demonstrate an overall survival (OS) benefit.[22] Maintenance therapy is then implemented until the time of relapse.[23–25] At relapse, subsequent therapies are given sequentially by using previously successful drugs (if the interval of time since previous exposure is >1 year) or newer drugs not previously tried.
Less-fit patients with significant comorbidities or advanced age (aged ≥80 years)
The less-fit patient may receive induction chemotherapy with a triplet or quadruplet regimen (as described for the patient in good or well-controlled health, but with dosage adjustments) including the CD38-directed monoclonal antibodies daratumumab or isatuximab, or with a doublet regimen including daratumumab or isatuximab, which might be better tolerated.[26] Therapy is continued until maximal response, and then maintenance therapy is given until relapse.[27] At relapse, subsequent therapies are given sequentially (as described for the patient in good or well-controlled health).
High risk versus standard risk
Patients with newly diagnosed or relapsing myeloma can be identified as having standard-risk or high-risk disease. This determination is made based on cytogenetics, genetic aberrations detected by fluorescence in situ hybridization, and possibly the genetic expression profile analyses that are in the process of standardization.[28] Plasma cell leukemia at presentation, or as a leukemic evolution of refractory myeloma, is a particularly high-risk, poor-prognosis entity.[29–33] Plasma cell leukemia with an ultra-high poor prognosis is defined by the presence of more than 2% circulating tumor plasma cells by flow cytometry.[34] Higher-risk patients are candidates for clinical trials using newer agents upfront or newer combination therapies currently used for relapsed disease at the discretion of the clinician.[35–37] Beyond induction therapy, high-risk disease can warrant more aggressive strategies, such as tandem transplant or consideration of allogeneic SCT. More intensive maintenance therapies may also be given for high-risk disease; instead of using lenalidomide alone, lenalidomide plus bortezomib has been chosen based on prior trials using thalidomide.[38] These more aggressive strategies have been implemented because of poor responsiveness to standard regimens and the worse prognosis of high-risk patients. Ultimately, prospective randomized trials are needed to establish improved outcomes with these newer approaches for high-risk patients.
Measurable Residual Disease
The assessment of measurable residual disease (MRD) in the bone marrow is mandatory for the assessment of efficacy in clinical trials.[39–42] Does MRD testing outside of the trial setting yield meaningful clinical improvement in patient outcomes by informing selection or duration of therapy? Achievement of MRD negativity after induction therapy (with or without consolidation therapy) is associated with improved progression-free survival (PFS) and improved OS.[43–52] While MRD negativity may be useful for the design of clinical trials, there are no data suggesting that this interim marker improves outcomes by altering subsequent therapy. Similarly, there are no data to suggest that sustained MRD negativity can allow deintensification or discontinuation of maintenance therapy.[53,54] Using peripheral blood to assess for MRD appears feasible with next-generation flow and mass spectroscopy. This approach is less-invasive than using bone marrow.[55]
Induction Therapy
Patients with myeloma who are symptomatic or require therapy because of progression or adverse laboratory findings require induction therapy. Ideally, induction therapy should reduce tumor burden, provide symptomatic relief, and prevent further end-organ damage.
Fit patients in good or well-controlled health
Two prospective randomized trials evaluated induction therapy with the D-VRd regimen (which includes daratumumab, an anti-CD38 monoclonal antibody) in fit patients in good or well-controlled health. Another prospective randomized trial evaluated I-VRd (which includes isatuximab, another anti-CD38 monoclonal antibody) as an alternative induction therapy.
A prospective trial included 709 transplant-eligible patients with newly diagnosed myeloma. Patients were randomly assigned to receive either D-VRd or VRd. All patients received an autologous SCT and subsequent lenalidomide maintenance therapy.[56]
With a median follow-up of 47.5 months, the 4-year PFS rate was 84.3% in the D-VRd group and 67.7% in the VRd group (hazard ratio [HR], 0.42; 95% confidence interval [CI], 0.30–0.59; P < .001).[56][Level of evidence B1]
The complete response rate was 87.9% in the D-VRd group and 70.1% in the VRd group (P < .001). The percentage of patients who achieved MRD-negative status favored D-VRd (75.2% vs. 47.5%; P < .001).
The most common grade 3 or 4 adverse event was neutropenia, which occurred in 62% of patients who received D-VRd and 51% of patients who received VRd.
The phase II GRIFFIN trial (NCT02874742) enrolled 207 patients with newly diagnosed transplant-eligible multiple myeloma. Patients were randomly assigned to receive induction therapy with either D-VRd or VRd. Patients then received an autologous SCT, two more cycles of the induction regimen, and 2 years of maintenance therapy with Dara-R (daratumumab and lenalidomide) or lenalidomide alone depending on the original randomization.[57]
With a median follow-up of 49.6 months, the percentage of patients with a stringent complete response was 67% in the D-VRd group and 48% in the VRd group (odds ratio [OR], 2.18; 95% CI, 1.22–3.89; P = .0079).[57][Level of evidence B3]
The 4-year PFS rate was 87.2% in the D-VRd group and 70.0% in the VRd group (HR, 0.45; 95% CI, 0.21–0.95; P = .032).[57][Level of evidence B3]
The median OS was not reached in either group (HR, 0.90; 95% CI, 0.31–2.56; P = .84).
A Markov model using MRD status to predict PFS suggested improved quality of life and lower cost over 10 years with the use of daratumumab in the first-line setting.[58]
A prospective trial, reported in abstract form, included 662 transplant-eligible patients with newly diagnosed myeloma. Patients were randomly assigned to receive either I-VRd or VRd. All patients received an autologous SCT and subsequent lenalidomide maintenance therapy.[13]
With a median follow-up of 47.0 months, the 3-year PFS rate was 83% in the I-VRd group and 75% in the VRd group (HR, 0.70; 95% CI, 0.52–0.94; P = .02).[13][Level of evidence B1]
Isatuximab is given intravenously (IV), unlike daratumumab, which is given subcutaneously.
A more intensive regimen of induction therapy, consolidation therapy, and maintenance therapy was investigated in patients with high-risk cytogenetic abnormalities.
In the multicenter phase II OPTIMUM trial (NCT03188172), 412 newly diagnosed patients were screened to identify 103 patients with ultra–high-risk (UHR) myeloma or plasma cell leukemia.[59] UHR myeloma was defined by the presence of at least two specified genetic risk markers (t(4;14), t(14;16), t(14;20), del (1p), 1q gain, and del 17p)) and/or SKY92 gene expression risk signature. All patients were treated with D-CVRd induction for six cycles (or until maximum response), autologous SCT consolidation, and D-VRd consolidation followed by Dara-R maintenance.[60]
With a median follow-up of 41.2 months, the 30-month PFS rate was 77% (95% CI, 69%–81%) for patients who received the study treatment versus 40% (95% CI, 31%–49%) for an historical control group who received KCRD (carfilzomib, cyclophosphamide, lenalidomide, and dexamethasone).[59][Level of evidence C2] The 30-month OS rate was 84% (95% CI, 76%–91%) for patients who received the OPTIMUM regimen and 74% (95% CI, 66%–82%) for the historical control KCRD regimen.[59][Level of evidence C1]
The study design did not prove that D-CVRd is the preferred regimen for patients with UHR myeloma, but it is a feasible regimen for further randomized trials in this patient population.
In transplant-eligible patients, alkylators such as melphalan are avoided upfront to prevent stem cell toxicity with subsequent risks for cytopenias, secondary malignancies, or poor stem cell harvesting.[61] Bortezomib is given subcutaneously, which helps to avoid the neuropathies that were much more severe with IV administration.[62–64] Bortezomib is also preferred for patients with renal impairment.[65] Patients receiving a bortezomib-containing regimen need prophylaxis for herpes zoster (usually with valacyclovir or acyclovir). Lenalidomide is given orally and can cause an increased risk of deep venous thrombosis (DVT) or pulmonary embolism, requiring additional prophylactic medication.[66,67] Because lenalidomide is metabolized erratically in patients with renal failure, clinicians may choose the CyBorD regimen,[19,20] but this selection is empiric and not based on randomized trial results. For patients without extra risk factors for DVT, aspirin (81 mg daily) suffices, but stronger anticoagulants should be considered for patients with multiple risk factors who receive lenalidomide (or other similar immunomodulating agents such as pomalidomide or thalidomide). Lower doses of lenalidomide must be used for patients with renal dysfunction.[68]
Less-fit patients with significant comorbidities or advanced age (aged ≥80 years)
Triplet or quadruplet therapies such as VRd and CyBorD with daratumumab or isatuximab can be used in patients with adequate fitness and minimal comorbidities. When triplets are deemed too difficult, doublets with Vd (bortezomib plus dexamethasone) or Rd (lenalidomide plus dexamethasone) can be used, or even a triplet such as VMP (bortezomib, melphalan, and prednisone).[15,26] Therapeutic options have changed with the advent of daratumumab and isatuximab, the CD38-directed monoclonal antibodies.
A prospective randomized trial, reported in abstract form, included 395 patients with newly diagnosed myeloma who were aged 70 years or older or ineligible for autologous SCT with medical comorbidities. Patients received D-VRd or VRd.[69]
With a median follow-up of 58.7 months, the 2-year MRD negativity (10-6) was 32.0% for patients who received D-VRd and 15.7% for patients who received VRd (HR, 0.40; 95% CI, 0.24–0.64; P = .001).[69][Level of evidence B3]
A prospective randomized trial (NCT03319667) was conducted in 446 patients with newly diagnosed myeloma who were ineligible for transplant. Patients were randomly assigned in a 3:2 ratio to receive either I-VRd or VRd alone.[14]
With a median follow-up of 59.7 months, the 5-year PFS rate was 63.2% for patients who received I-VRd versus 45.2% for patients who received VRd alone (HR, 0.60; 98.5% CI, 0.41–0.88; P < .001).[14][Level of evidence B1]
Isatuximab is given IV, unlike daratumumab, which is given subcutaneously (with significantly less side effects than the IV formulation).
Serious adverse events were similar in the two groups.
In a prospective randomized trial (NCT02252172) of 737 patients with newly diagnosed myeloma who were ineligible for transplant, daratumumab plus lenalidomide and dexamethasone was compared with Rd alone.[70]
With a median follow-up of 56.2 months, the 60-month OS rate was 66.3% (95% CI, 60.8%–71.3%) for patients who received daratumumab and 53.1% (95% CI, 47.2%–58.6%) for patients who received Rd alone (HR, 0.68; 95% CI, 0.53–0.86; P = .0013).[70][Level of evidence A1]
With a median follow-up of 56.2 months, the 60-month PFS rate was 52.5% for patients who received daratumumab (95% CI, 46.7%−58.0%) and 28.7% for patients who received Rd alone (95% CI, 23.1%−34.6%) (HR, 0.53; 95% CI, 0.43−0.66; P < .0001).[70]
Results for the percentage of patients falling below the threshold for MRD (<1 tumor cell per 105 white cells) favored the daratumumab combination, 24.2% versus 7.3% (P < .001).
The daratumumab combination resulted in significant and sustained reductions of pain scores and improved quality of life in the EuroQOL 5-dimensional descriptive visual system.[71][Level of evidence A3]
In a prospective randomized trial of 706 patients with newly diagnosed myeloma who were ineligible for transplant, daratumumab plus VMP was compared with VMP alone.[72]
With a median follow-up of 40.1 months, the 3-year OS rate favored the daratumumab combination group at 78% (95% CI, 73.2%−83.0%) versus 67.9% in the VMP-alone group (95% CI, 62.6%−72.6%) (HR, 0.60; 95% CI, 0.46−0.80; P = .003).[72][Level of evidence A1]
With a median follow-up of 40.1 months, the 3-year PFS rate favored the daratumumab combination group at 50.7% (95% CI, 45.1%−55.9%) versus 18.5% in the VMP-alone group (95% CI, 14.4%−23.1%) (HR, 0.42; 95% CI, 0.34−0.51; P < .0001).[72][Level of evidence B1]
In the daratumumab combination group, 22.3% of patients were MRD negative (at a threshold of one tumor cell per 105 white cells); in the VMP-alone group, 6.2% of patients were MRD negative (P < .001).
Immunological reaction to the initial dose of daratumumab can be modulated by splitting the first infusion over 2 days or using the subcutaneous version (this dosing schedule is not approved by the U.S. Food and Drug Administration).
In a prospective randomized trial (NCT04751877), 270 patients with newly diagnosed myeloma who were transplant ineligible and aged 65 to 79 years received either I-VRd or isatuximab plus Rd.[73]
With a median follow-up of 23.5 months, the MRD negativity rates (at 10-5) at 18 months were 53% for the I-VRd group and 26% for the isatuximab-Rd group (OR, 3.16; 95% CI, 1.89–5.28; P < .0001).[73][Level of evidence B3]
Isatuximab is given IV, unlike daratumumab, which is given subcutaneously (with significantly less side effects than the IV formulation).
Serious adverse events were similar in the two groups.
In a prospective randomized trial, 955 patients with newly diagnosed multiple myeloma who were ineligible for transplant received either carfilzomib plus melphalan and prednisone or VMP.[74]
With a median follow-up of 23 months, there was no difference in median PFS (22.3 vs. 22.1 months; HR, 0.91; 95% CI, 0.75−1.10; P = .159) or in median OS (HR, 1.1; 95% CI, 0.82−1.4).[74][Level of evidence A1]
In a prospective trial, 1,087 patients with standard-risk or intermediate-risk myeloma who deferred transplant for induction therapy were randomly assigned to receive carfilzomib plus lenalidomide and dexamethasone or bortezomib plus lenalidomide and dexamethasone.[75]
With a median follow-up of 26 months, there was no difference in median PFS (34.6 vs. 34.4 months; HR, 1.04; 95% CI, 0.83−1.31; P = .742) or in median OS (HR, 0.98; 95% CI, 0.71−1.36; P = .923).[75][Level of evidence A1]
Many other phase II and phase III trials, published in preliminary abstract form, show results similar to the trial that combined daratumumab with melphalan and prednisone, and used daratumumab with other triplets and doublets in both previously untreated and previously treated patients.[76,77] Further follow-up is required to establish OS benefits. Mature OS data are required to better assess the cost-effectiveness of daratumumab in the first-line setting.[78]
Consolidation Therapy
Autologous bone marrow or peripheral stem cell transplant
Evidence (autologous bone marrow or peripheral SCT):
The failure of conventional therapy to cure myeloma has led investigators to test the effectiveness of much higher doses of drugs such as melphalan. The development of techniques for harvesting hematopoietic stem cells, from marrow aspirates or the peripheral blood of the patient, and infusing these cells to promote hematopoietic recovery made it possible for investigators to test very large doses of chemotherapy.
Based on the experience of treating thousands of patients in this way, it is possible to draw a few conclusions:
The risk of early death caused by treatment-related toxic effects has been reduced to less than 3% in highly selected populations.[79]
Extensive prior chemotherapy, especially with alkylating agents, compromises marrow hemopoiesis and may make the harvesting of adequate numbers of hematopoietic stem cells impossible.[61]
Younger patients in good health tolerate high-dose therapy better than older patients with a poor performance status.[80–82] However, fit patients older than 70 to 75 years can receive autologous SCT consolidation.[83,84]
Single autologous bone marrow or peripheral stem cell transplant
Evidence (single autologous bone marrow or peripheral SCT):
While some prospective randomized trials showed improved survival for patients who received autologous peripheral stem cell or bone marrow transplant after induction chemotherapy compared with chemotherapy alone,[25,85–87][Level of evidence A1] other trials have not shown any survival advantage.[88–93][Level of evidence A1]
In a prospective randomized trial (NCT01208662), 722 patients aged 65 years or younger with newly diagnosed multiple myeloma received either VRd for three cycles followed by autologous SCT consolidation and two more cycles of VRd or VRd alone for eight cycles. Both groups received maintenance lenalidomide given continuously in the absence of disease relapse or unacceptable side effects.[94] At relapse, patients who received VRd only (without autologous SCT) were re-induced and offered transplant if they were still responding.
With a median follow-up of 76.0 months, the median PFS was shorter for patients in the nontransplant arm (42.0 months) than for patients in the transplant arm (67.5 months) (HR, 1.53; 95% CI, 1.23–1.91; P < .001).[94][Level of evidence B1]
The 5-year OS rate was not significantly different: 79.2% for patients in the nontransplant arm versus 80.7% for patients in the transplant arm (HR, 1.10; 95% CI, 0.73–1.65; P > 0.99).
Rates of grade 3 or 4 hematologic adverse events were significantly higher in the transplant arm (41.9%) than in the nontransplant arm (26.1%) (P < .001). Acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) were only reported in the transplant arm (10 cases).
Only 28% of patients who received VRd originally received autologous SCT at any time after the end of study treatment.
Three meta-analyses of almost 3,000 patients showed no survival advantage.[22,95,96][Level of evidence A1]
A meta-analysis was performed for all randomized clinical trials conducted between 2000 and 2021 that compared up-front autologous SCT with standard-dose therapy/consolidation. A total of 3,307 citations were screened: six trials were selected for PFS analysis and four trials were selected for OS analysis (2,959 patients).[97]
With a median follow-up of 3.1 to 7.8 years, patients with high-risk cytogenetics (t(4;14), t(14;16), and/or del(17p)) had a significant OS benefit from autologous SCT versus standard-dose therapy (HR, 0.66; 95% CI, 0.45–0.97; P = .03).[97][Level of evidence A2] No survival benefit was seen for patients with standard-risk cytogenetics.
Patients with high-risk disease (approximately 20% of the total) showed a significant PFS benefit from autologous SCT versus standard-dose therapy (HR, 0.52; 95% CI, 0.33–0.83). Patients with standard-risk disease also showed a PFS benefit from autologous SCT (HR, 0.65; 95% CI, 0.56–0.76).[97]
Even the trials suggesting improved survival showed no signs of a slowing in the relapse rate or a plateau to suggest that any of these patients had been cured.[25,85–87,98] The role of autologous SCT has changed, from a mandated standard consolidation for those patients healthy enough to undergo it toward a therapeutic option, like any other, that offers approximately 2 years of increased PFS on average with defined toxicities. Incorporating, eliminating, delaying, or even replacing autologous SCT in the future (perhaps with chimeric antigen receptor T cells or bispecific antibodies) will be the subject of ongoing and upcoming clinical trials. Subgroups of patients may have a particular benefit from autologous SCT. Patients with a t(11;14) translocation may show differential benefit, as found in a retrospective review of 3,538 total patients in a dataset from the Center of International Blood and Marrow Transplant Research.[99] One meta-analysis of only four randomized clinical trials suggested an OS benefit for up-front autologous SCT in patients with high-risk cytogenetics.[97]
Tandem autologous bone marrow or peripheral stem cell transplant followed by autologous or allogeneic transplant
Another approach to high-dose therapy has been the use of two sequential infusions of high-dose therapy with stem cell support (tandem transplants).[100–104]
Evidence (tandem autologous bone marrow or peripheral SCT):
A meta-analysis of six randomized clinical trials enrolling 1,803 patients compared single autologous hematopoietic cell transplant with tandem autologous hematopoietic cell transplant.
There was no difference in OS (HR, 0.94; 95% CI, 0.77–1.14) or in event-free survival (EFS) (HR, 0.86; 95% CI, 0.70–1.05).[105][Level of evidence A2]
A prospective randomized trial of 758 patients who completed induction therapy in less than 12 months compared autologous SCT plus lenalidomide maintenance, tandem autologous SCT, and autologous SCT plus VRd maintenance.[106]
There was no difference in 38-month PFS (53.9%−58.5%) and OS (81.8%−85.4%) rates among these three randomized groups.[106][Level of evidence A1]
Five different groups have compared single or tandem autologous transplants with one autologous transplant followed by a reduced-intensity conditioning allograft from a HLA-identical sibling; treatment assignment was based on the presence or absence of an HLA-identical sibling. The results have been discordant for survival in these nonrandomized trials.[107–110][Level of evidence C1]
Six clinical trials compared the outcomes of patients receiving tandem autologous transplant with those of patients receiving a reduced-intensity allogeneic SCT after autologous transplant. Patients were assigned to the latter treatments based on the availability of an HLA-matched donor. Two meta-analyses of these data showed that although the complete remission rate was higher in patients undergoing reduced-intensity allogeneic SCT, OS was comparable because of an increased incidence of nonrelapse mortality with allogeneic transplant.[111,112][Level of evidence A1]
A Cochrane review of 14 controlled studies found none of the trials helpful for contemporary treatment decisions regarding single versus tandem transplants.[113] None of the trials used bortezomib or lenalidomide, and the sharp decrease in compliance with a second transplant complicated sample-size calculations for sufficient statistical power.
Allogeneic bone marrow or peripheral stem cell transplant
Evidence (allogeneic bone marrow or peripheral SCT):
Many patients are not young enough or healthy enough to undergo these intensive approaches. A definite graft-versus-myeloma effect has been demonstrated, including regression of myeloma relapses after the infusion of donor lymphocytes.[114]
Favorable prognostic features included:
Low tumor burden.
Responsive disease before transplant.
Application of transplant after first-line therapy.
Myeloablative allogeneic SCT has significant toxic effects (15%–40% mortality), but the possibility of a potent and possibly curative graft-versus-myeloma effect in a minority of patients may offset the high transplant-related mortality.[114–116] In one anecdotal series of 60 patients who underwent allogeneic SCT, six of the patients relapsed between 6 and 12 years, suggesting that late relapses still occur with this type of consolidation.[117]
The lower transplant-related mortality from nonmyeloablative approaches has been accompanied by a greater risk of relapse.[116] Since the introduction of lenalidomide and bortezomib, a trial exploring donor versus no donor comparison of autologous SCT versus autologous SCT and nonmyeloablative allogeneic SCT in 260 untreated patients showed no difference in PFS or OS.[118][Level of evidence C1] This result contrasted with two older trials (before introduction of lenalidomide and bortezomib), which suggested improvement of PFS and OS with a sibling donor.[109,119][Level of evidence C1]
Six clinical trials compared the outcomes of patients receiving tandem autologous transplant with those of patients receiving a reduced-intensity autologous SCT after autologous transplant. Patients were assigned to the latter treatments based on the availability of an HLA-matched donor. Two meta-analyses of these data showed that although the complete remission rate was higher in patients undergoing reduced-intensity autologous SCT, OS was comparable because of an increased incidence of nonrelapse mortality with allogeneic transplant.[111,112][Level of evidence A1] Anecdotal long-term survivals have been reported for patients with therapy-related MDS, AML, acute lymphoblastic leukemia, or chronic myelomonocytic leukemia treated with allogeneic SCT.[120]
Salvage autologous bone marrow or peripheral stem cell transplant after relapse from first transplant
After relapsing more than 24 months after autologous SCT, 174 patients received reinduction therapy and were then randomly assigned to receive either high-dose melphalan and salvage autologous SCT or oral weekly cyclophosphamide.[121] With a median follow-up of 52 months, the median OS was superior for salvage autologous SCT: 67 months (95% CI, 55–not estimable) versus 52 months (42–60) (HR, 0.56; 0.35–0.90; P = .017).[121,122][Level of evidence A1]
In a retrospective review of 233 patients with refractory myeloma or relapsed and refractory myeloma who underwent a salvage autologous SCT, 81% of patients achieved a partial response (PR) or better.[123][Level of evidence C3]
Maintenance Therapy
Myeloma patients who respond to treatment show a progressive fall in the M protein until a plateau is reached; subsequent treatment with conventional doses does not result in any further improvement. This has led investigators to question how long treatment should be continued. No clinical trial has directly compared a consolidation approach with a maintenance approach to assess which is better in prolonging remission and, ultimately, survival.[124] Most clinical trials employ one or both.[125,126] Maintenance trials with glucocorticosteroids [127,128] and with interferon [129] showed very minor improvements in remission duration and survival but with toxicities that outweighed the benefits. The efficacy and tolerability of thalidomide, lenalidomide, bortezomib, and ixazomib in the induction and relapse settings has made these agents attractive options in maintenance trials.[124]
Maintenance therapy (lenalidomide, ixazomib, and daratumumab alone or in combination)
Evidence (maintenance therapy [lenalidomide, ixazomib, and daratumumab alone or in combination]):
The prospective randomized AURIGA trial (NCT03901963) included 200 patients with newly diagnosed multiple myeloma who achieved a very good or better partial response, were MRD-positive on bone marrow (10-5), and who had not received daratumumab (or isatuximab) anti-CD38 therapy during induction therapy.[130] Patients were randomly assigned to receive either Dara-R or lenalidomide alone.
At a median follow-up of 32.3 months, the 30-month PFS rate was 82.7% for patients who received Dara-R and 66.4% for patients who received lenalidomide alone (HR, 0.53; 95% CI, 0.29–0.97; P = .036).[130][Level of evidence B1]
The MRD-negative (10-6) conversion rate was 23.2% for patients who received Dara-R and 5.0% for patients who received lenalidomide alone (OR, 5.97; 95% CI, 2.15–16.58; P = .0002).
Grade 3 or 4 cytopenias occurred in 54.2% of patients who received Dara-R versus 46.9% of patients who received lenalidomide alone. Infections occurred in 18.8% of patients who received Dara-R versus 13.3% of patients who received lenalidomide alone.
A prospective randomized trial of 460 patients with newly diagnosed multiple myeloma who had completed induction therapy and autologous SCT compared lenalidomide maintenance with placebo.[131]
With a median follow-up of 91 months, the median OS for the lenalidomide maintenance group was 113.8 months (95% CI, 100.4−not reached) versus 84.1 months for the placebo group (range, 73.8−106.0 months; HR, 0.61; 95% CI, 0.46−0.80; P = .0004).[131][Level of evidence A1]
This translated to a 5-year OS rate of 76% (95% CI, 70%−81%) for the lenalidomide group versus 64% (95% CI, 58%−70%) for the placebo group.
A prospective randomized trial evaluated lenalidomide maintenance in 1,917 patients newly diagnosed with or without transplant.[132]
With a median follow-up of 31 months, lenalidomide showed improved median PFS, 39 months (95% CI, 36−42) versus 20 months (range, 18−22) (HR, 0.46; 95% CI, 0.41−0.53; P < .0001), but lenalidomide failed to significantly improve the 3-year OS rate, 78.6% (95% CI, 75.6%−81.6%) versus 75.8% (72.4%−79.2%) (HR, 0.87; 95% CI, 0.73−1.05; P = .15).[132][Level of evidence B1]
A meta-analysis included 1,208 patients with newly diagnosed disease who underwent an autologous SCT.[133]
With a median follow-up of 79.5 months, OS was not reached for the lenalidomide maintenance group versus 86 months for the placebo or observation group (HR, 0.75; 95% CI, 0.63‒0.90; P = .001).[133][Level of evidence A2]
A meta-analysis of 7,730 patients in randomized clinical trials investigated lenalidomide or thalidomide maintenance in patients with newly diagnosed myeloma, with or without transplant.[134]
The immunomodulatory maintenance therapy significantly improved PFS (HR, 0.62; 95% CI, 0.57−0.67; P < .001), but failed to significantly improve OS (HR, 0.93; 95% CI, 0.85−1.01; P = .082).[134][Level of evidence B1]
A meta-analysis of 5,073 patients in randomized clinical trials investigated maintenance therapy in patients with newly diagnosed myeloma.[135]
Lenalidomide (with or without prednisone) significantly improved PFS (HR, 0.47; 95% CI, 0.39−0.55), but also failed to significantly improve OS (HR, 0.76; 95% CI, 0.51−1.16).[135][Level of evidence B1]
A prospective randomized trial of lenalidomide maintenance versus no maintenance after induction with melphalan and prednisone or melphalan, prednisone, and lenalidomide included patients aged 65 years and older who were not eligible for transplant.[27]
The results showed a 66% reduction in the rate of progression (HR, 0.34; P < .001), which translated to an EFS of 31 months versus 14 months in favor of maintenance lenalidomide.[27][Level of evidence B1]
A prospective randomized trial (CASSIOPEIA [NCT02541383]) evaluated daratumumab maintenance versus no maintenance for patients with newly diagnosed myeloma. Patients had already received bortezomib, thalidomide, and dexamethasone with or without daratumumab as induction before autologous SCT.[136]
With a median follow-up of 35.4 months after maintenance randomization, the median PFS was not reached in the daratumumab arm and was 46.7 months (40.0–not evaluable) with observation only (HR, 0.53; 95% CI, 0.42–0.68; P < .0001).[136][Level of evidence B1]
A prospective randomized trial evaluated ixazomib maintenance versus no maintenance for patients with newly diagnosed myeloma who were not undergoing autologous SCT after induction therapy.[137]
With a median follow-up of 41 months, the median PFS favored ixazomib maintenance at 17.4 months versus 9.4 months (HR, 0.66; 95% CI, 0.54–0.80; P < .001).[137][Level of evidence B1]
A prospective trial (NCT02659293) evaluated maintenance therapy in patients with newly diagnosed melanoma who had received induction therapy and autologous SCT. Patients were randomly assigned to receive maintenance therapy with either 3 years of carfilzomib, lenalidomide, and dexamethasone or lenalidomide alone.[138]
With a median follow-up of 33.8 months, the median PFS was 59.1 months for patients who received the triplet maintenance therapy and 41.4 months for patients who received lenalidomide alone (HR, 0.51; 95% CI, 0.31–0.86; P = .012).[138][Level of evidence B1]
All the trials and meta-analyses of lenalidomide maintenance showed a significant improvement in PFS, while OS was improved in one trial and one meta-analysis, both after autologous SCT. All of these trials showed an increase in myelodysplasia or acute leukemia from 3% to 7% for lenalidomide, consistent with other studies of lenalidomide. This increased risk is mostly seen in patients with previous exposure to alkylating agents. Doses of 5 mg to 15 mg a day have been used either continuously or with 1 week off every month.
One prospective trial found improved benefit in PFS for Dara-R compared with lenalidomide alone in a population that had undergone transplant and was naïve to anti-CD38 therapy.[130] One trial establishing the D-VRd regimen for newly diagnosed patients included Dara-R maintenance (for 2 to 3 years or longer) in the D-VRd induction arm.[57] The incremental impact of Dara-R maintenance therapy in patients who received daratumumab induction therapy has not been established. It is also unclear if patients with MRD-negative (10-5) disease after induction therapy and transplant would benefit similarly since they were also not studied.[139]
Among 556 patients in the Myeloma XI trial (NCT01554852), those with del(1p), del(17p), and t(4;14) had a median PFS of 57.3 months with lenalidomide maintenance and 10.9 months with observation.[140] For patients unable to receive lenalidomide maintenance, ixazomib is a reasonable alternative. Although maintenance therapy with carfilzomib, lenalidomide, and dexamethasone resulted in improved PFS when compared with lenalidomide alone, the preliminary toxicity and efficacy results must mature before implementing this regimen.[138]
In a prospective randomized trial of 656 newly diagnosed patients with at least a PR after standard induction therapy followed by autologous SCT, ixazomib (the oral proteasome inhibitor) was compared with placebo.[141]
With a median follow-up of 31 months, the ixazomib maintenance improved medial PFS, 26.5 months (95% CI, 23.7−33.8) versus 21.3 months (95% CI, 18.0−24.7) (HR, 0.72; 95% CI, 0.58−0.89; P = .0023).[141][Level of evidence B1] There was no increase in second malignancies with the proteasome inhibitor (3% for both groups).
In 511 previously untreated patients not eligible for transplant and aged 65 years or older, a randomized comparison of bortezomib, melphalan, prednisone, thalidomide and subsequent maintenance using bortezomib plus thalidomide versus VMP (with no maintenance) showed superiority of the arm with thalidomide and bortezomib during induction and maintenance.
With a median follow-up of 47 months, the 3-year PFS rate was 55% versus 33% (P < .01), and the 5-year OS rate was 59% versus 46% (P = .04).[142][Level of evidence A1]
Because of trial design, it is unclear whether the improved results were caused by the addition of thalidomide during the induction or by the use of maintenance therapy with bortezomib and thalidomide.
Summary: After autologous SCT, patients are offered lenalidomide maintenance therapy based on the consistent PFS and occasional OS benefits previously described. But short-term and long-term toxicities, and financial toxicities, may prevent implementation.[143,144] High-risk patients, especially those with del(17p) or t(14;16), may require bortezomib maintenance (with or without lenalidomide), but this approach is not evidence-based and confirmatory clinical trials are required.[145,146]
Management and Prevention of Myeloma Bone Disease
Myeloma bone disease is a consequence of increased osteoclastic activity, and agents that inhibit osteoclasts are an important component of myeloma therapy.[9] The bisphosphonates pamidronate and zoledronate are used most often, via IV infusion, but the RANKL monoclonal antibody inhibitor denosumab, given subcutaneously, is also effective, especially when renal dysfunction precludes the use of bisphosphonates.[8,9]
Zoledronate (bisphosphonate)
Evidence (zoledronate):
A prospective randomized trial of 1,970 patients compared IV zoledronate with oral clodronate in newly diagnosed patients receiving induction chemotherapy with or without consolidation.[147]
With a median follow-up of 3.7 years, zoledronate improved median OS from 44.5 months to 50.0 months (HR, 0.84; 95% CI, 0.74–0.96; P = .0118).[147][Level of evidence A1]
In this trial, both bisphosphonates were continued until time of relapse. As expected, skeletal-related events were also reduced in the zoledronate group (27% vs. 35%; P = .004).[148,149]
The improvement of median OS with zoledronate was confirmed in a Cochrane network meta-analysis.[150][Level of evidence A2] This meta-analysis also showed that 6 to 15 patients need treatment with bisphosphonates to prevent one skeletal-related event.
A clinical trial of zoledronate given once a month compared with zoledronate given every 12 weeks showed noninferiority for the 12-week regimen in 1,822 patients with bone metastases from breast cancer, prostate cancer, or multiple myeloma.[151] However, this study included only 278 patients with myeloma, and evaluation of this subgroup was insufficiently powered to establish noninferiority for the 12-week regimen. Nonetheless, this trial is used as justification for implementing a 12-week schedule at the start of therapy or as soon as maximal response has been reached.
Bisphosphonates are associated with infrequent long-term complications (in 3%–5% of patients), including osteonecrosis of the jaw and avascular necrosis of the hip.[152,153] For more information about osteonecrosis of the jaw, see Oral Complications of Cancer Therapies. These side effects must be balanced against the potential benefits of bisphosphonates when bone metastases are evident.[154] Bisphosphonates are usually given IV on a monthly basis for 2 years and then extended at the same schedule or at a reduced schedule (i.e., once every 3–4 months), if there is evidence of active myeloma bone disease.[155,156] On the aforementioned randomized trial,[148] which showed OS advantage, patients received bisphosphonates monthly until time of relapse.
Pamidronate (bisphosphonate)
Evidence (pamidronate):
A randomized, double-blind study of patients with stage III myeloma showed that monthly IV pamidronate significantly reduced pathological fractures, bone pain, spinal cord compression, and the need for bone radiation therapy (38% skeletal-related events were reported in the treatment group vs. 51% in the placebo group after 21 months of therapy; P = .015).[157][Level of evidence B1] For more information about bisphosphonate therapy, see the Pharmacological Therapies for Pain Control section in Cancer Pain.
A double-blind, randomized, controlled trial of 504 patients with newly diagnosed multiple myeloma compared 30 mg of pamidronate to 90 mg of pamidronate. The study found that there was no difference in skeletal-related events, but there was less osteonecrosis (2 events vs. 8 events) seen in the low-dose group.[158][Level of evidence B3]
A randomized comparison of pamidronate versus zoledronic acid in 518 patients with multiple myeloma showed equivalent efficacy in regard to skeletal-related complications (both were given for 2 years).[159][Level of evidence B1]
Denosumab (RANKL inhibitor)
Evidence (denosumab):
In a prospective randomized double-blind trial, 1,718 patients with newly diagnosed myeloma and at least one documented lytic bone lesion received either zoledronate or denosumab.[8]
The study met its primary end point of noninferiority for denosumab compared with zoledronate (HR, 0.98; 95% CI, 0.85‒1.14; P = .01 for noninferiority).[8]
Denosumab is significantly more expensive than the bisphosphonates, which are available in generic form.
Unlike bisphosphonates, the reversible mechanism of action for denosumab may result in rebound fractures if it is discontinued, although this theoretical concern for patients with myeloma may be mitigated by continuous maintenance therapy.[160]
Radiation therapy for bone lesions
Lytic lesions of the spine generally require radiation if any of the following are true:
They are associated with an extramedullary (paraspinal) plasmacytoma.
A painful destruction of a vertebral body occurred.
CT or MRI scans present evidence of spinal cord compression.[161]
Back pain caused by osteoporosis and small compression fractures of the vertebrae responds best to chemotherapy.
Extensive radiation of the spine or long bones for diffuse osteoporosis may lead to prolonged suppression of hemopoiesis and is rarely indicated.[162]
Bisphosphonates are useful for slowing or reversing the osteopenia that is common in patients with myeloma.[157]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Dimopoulos MA, Hillengass J, Usmani S, et al.: Role of magnetic resonance imaging in the management of patients with multiple myeloma: a consensus statement. J Clin Oncol 33 (6): 657-64, 2015. [PUBMED Abstract]
Moreau P, Attal M, Caillot D, et al.: Prospective Evaluation of Magnetic Resonance Imaging and [18F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients With Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J Clin Oncol 35 (25): 2911-2918, 2017. [PUBMED Abstract]
Dispenzieri A, Kyle R, Merlini G, et al.: International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia 23 (2): 215-24, 2009. [PUBMED Abstract]
Raab MS, Podar K, Breitkreutz I, et al.: Multiple myeloma. Lancet 374 (9686): 324-39, 2009. [PUBMED Abstract]
Yourman LC, Lee SJ, Schonberg MA, et al.: Prognostic indices for older adults: a systematic review. JAMA 307 (2): 182-92, 2012. [PUBMED Abstract]
Raje N, Terpos E, Willenbacher W, et al.: Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: an international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol 19 (3): 370-381, 2018. [PUBMED Abstract]
Anderson K, Ismaila N, Flynn PJ, et al.: Role of Bone-Modifying Agents in Multiple Myeloma: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol 36 (8): 812-818, 2018. [PUBMED Abstract]
Dimopoulos MA, Sonneveld P, Leung N, et al.: International Myeloma Working Group Recommendations for the Diagnosis and Management of Myeloma-Related Renal Impairment. J Clin Oncol 34 (13): 1544-57, 2016. [PUBMED Abstract]
Voorhees PM, Kaufman JL, Laubach J, et al.: Daratumumab, lenalidomide, bortezomib, and dexamethasone for transplant-eligible newly diagnosed multiple myeloma: the GRIFFIN trial. Blood 136 (8): 936-945, 2020. [PUBMED Abstract]
Voorhees PM, Rodriguez C, Reeves B, et al.: Daratumumab plus RVd for newly diagnosed multiple myeloma: final analysis of the safety run-in cohort of GRIFFIN. Blood Adv 5 (4): 1092-1096, 2021. [PUBMED Abstract]
Goldschmidt H, Bertsch U, Pozek E, et al.: Isatuximab, lenalidomide, bortezomib and dexamethasone induction therapy for transplant-eligible patients with newly diagnosed multiple myeloma: final progression-free survival analysis of part 1 of an open-label, multicenter, randomized, phase 3 trial (GMMG-HD7). [Abstract] Blood 144 (Suppl 1): A-769, 2024.
Facon T, Dimopoulos MA, Leleu XP, et al.: Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 391 (17): 1597-1609, 2024. [PUBMED Abstract]
San Miguel JF, Schlag R, Khuageva NK, et al.: Persistent overall survival benefit and no increased risk of second malignancies with bortezomib-melphalan-prednisone versus melphalan-prednisone in patients with previously untreated multiple myeloma. J Clin Oncol 31 (4): 448-55, 2013. [PUBMED Abstract]
Attal M, Lauwers-Cances V, Hulin C, et al.: Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N Engl J Med 376 (14): 1311-1320, 2017. [PUBMED Abstract]
Rosiñol L, Oriol A, Rios R, et al.: Bortezomib, lenalidomide, and dexamethasone as induction therapy prior to autologous transplant in multiple myeloma. Blood 134 (16): 1337-1345, 2019. [PUBMED Abstract]
Piechotta V, Jakob T, Langer P, et al.: Multiple drug combinations of bortezomib, lenalidomide, and thalidomide for first-line treatment in adults with transplant-ineligible multiple myeloma: a network meta-analysis. Cochrane Database Syst Rev 2019 (11): , 2019. [PUBMED Abstract]
Reece DE, Rodriguez GP, Chen C, et al.: Phase I-II trial of bortezomib plus oral cyclophosphamide and prednisone in relapsed and refractory multiple myeloma. J Clin Oncol 26 (29): 4777-83, 2008. [PUBMED Abstract]
Knop S, Liebisch H, Wandt H, et al.: Bortezomib, IV cyclophosphamide, and dexamethasone (VelCD) as induction therapy in newly diagnosed multiple myeloma: results of an interim analysis of the German DSMM Xia trial. [Abstract] J Clin Oncol 27 (Suppl 15): A-8516, 2009.
Barlogie B, Attal M, Crowley J, et al.: Long-term follow-up of autotransplantation trials for multiple myeloma: update of protocols conducted by the intergroupe francophone du myelome, southwest oncology group, and university of arkansas for medical sciences. J Clin Oncol 28 (7): 1209-14, 2010. [PUBMED Abstract]
Koreth J, Cutler CS, Djulbegovic B, et al.: High-dose therapy with single autologous transplantation versus chemotherapy for newly diagnosed multiple myeloma: A systematic review and meta-analysis of randomized controlled trials. Biol Blood Marrow Transplant 13 (2): 183-96, 2007. [PUBMED Abstract]
McCarthy PL, Owzar K, Hofmeister CC, et al.: Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med 366 (19): 1770-81, 2012. [PUBMED Abstract]
Attal M, Lauwers-Cances V, Marit G, et al.: Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med 366 (19): 1782-91, 2012. [PUBMED Abstract]
Palumbo A, Cavallo F, Gay F, et al.: Autologous transplantation and maintenance therapy in multiple myeloma. N Engl J Med 371 (10): 895-905, 2014. [PUBMED Abstract]
Facon T, Dimopoulos MA, Dispenzieri A, et al.: Final analysis of survival outcomes in the phase 3 FIRST trial of up-front treatment for multiple myeloma. Blood 131 (3): 301-310, 2018. [PUBMED Abstract]
Palumbo A, Hajek R, Delforge M, et al.: Continuous lenalidomide treatment for newly diagnosed multiple myeloma. N Engl J Med 366 (19): 1759-69, 2012. [PUBMED Abstract]
Sonneveld P, Avet-Loiseau H, Lonial S, et al.: Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group. Blood 127 (24): 2955-62, 2016. [PUBMED Abstract]
Mina R, Joseph NS, Kaufman JL, et al.: Survival outcomes of patients with primary plasma cell leukemia (pPCL) treated with novel agents. Cancer 125 (3): 416-423, 2019. [PUBMED Abstract]
Fernández de Larrea C, Kyle RA, Durie BG, et al.: Plasma cell leukemia: consensus statement on diagnostic requirements, response criteria and treatment recommendations by the International Myeloma Working Group. Leukemia 27 (4): 780-91, 2013. [PUBMED Abstract]
Granell M, Calvo X, Garcia-Guiñón A, et al.: Prognostic impact of circulating plasma cells in patients with multiple myeloma: implications for plasma cell leukemia definition. Haematologica 102 (6): 1099-1104, 2017. [PUBMED Abstract]
Royer B, Minvielle S, Diouf M, et al.: Bortezomib, Doxorubicin, Cyclophosphamide, Dexamethasone Induction Followed by Stem Cell Transplantation for Primary Plasma Cell Leukemia: A Prospective Phase II Study of the Intergroupe Francophone du Myélome. J Clin Oncol 34 (18): 2125-32, 2016. [PUBMED Abstract]
Gonsalves WI, Rajkumar SV, Go RS, et al.: Trends in survival of patients with primary plasma cell leukemia: a population-based analysis. Blood 124 (6): 907-12, 2014. [PUBMED Abstract]
Jelinek T, Bezdekova R, Zihala D, et al.: More Than 2% of Circulating Tumor Plasma Cells Defines Plasma Cell Leukemia-Like Multiple Myeloma. J Clin Oncol 41 (7): 1383-1392, 2023. [PUBMED Abstract]
Landgren O, Hultcrantz M, Diamond B, et al.: Safety and Effectiveness of Weekly Carfilzomib, Lenalidomide, Dexamethasone, and Daratumumab Combination Therapy for Patients With Newly Diagnosed Multiple Myeloma: The MANHATTAN Nonrandomized Clinical Trial. JAMA Oncol 7 (6): 862-868, 2021. [PUBMED Abstract]
Corre J, Munshi NC, Avet-Loiseau H: Risk factors in multiple myeloma: is it time for a revision? Blood 137 (1): 16-19, 2021. [PUBMED Abstract]
Al Hadidi S, Yellapragada S: Treatment Options for Relapsed and Refractory Multiple Myeloma: A Luxury or a Challenge? JAMA Oncol 7 (10): 1449-1450, 2021. [PUBMED Abstract]
Mateos MV, Oriol A, Martínez-López J, et al.: Maintenance therapy with bortezomib plus thalidomide or bortezomib plus prednisone in elderly multiple myeloma patients included in the GEM2005MAS65 trial. Blood 120 (13): 2581-8, 2012. [PUBMED Abstract]
Kumar S, Paiva B, Anderson KC, et al.: International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol 17 (8): e328-e346, 2016. [PUBMED Abstract]
Lahuerta JJ, Paiva B, Vidriales MB, et al.: Depth of Response in Multiple Myeloma: A Pooled Analysis of Three PETHEMA/GEM Clinical Trials. J Clin Oncol 35 (25): 2900-2910, 2017. [PUBMED Abstract]
Gambella M, Omedé P, Spada S, et al.: Minimal residual disease by flow cytometry and allelic-specific oligonucleotide real-time quantitative polymerase chain reaction in patients with myeloma receiving lenalidomide maintenance: A pooled analysis. Cancer 125 (5): 750-760, 2019. [PUBMED Abstract]
Paiva B, Puig N, Cedena MT, et al.: Measurable Residual Disease by Next-Generation Flow Cytometry in Multiple Myeloma. J Clin Oncol 38 (8): 784-792, 2020. [PUBMED Abstract]
Munshi NC, Avet-Loiseau H, Rawstron AC, et al.: Association of Minimal Residual Disease With Superior Survival Outcomes in Patients With Multiple Myeloma: A Meta-analysis. JAMA Oncol 3 (1): 28-35, 2017. [PUBMED Abstract]
Gormley NJ, Farrell AT, Pazdur R: Minimal Residual Disease as a Potential Surrogate End Point-Lingering Questions. JAMA Oncol 3 (1): 18-20, 2017. [PUBMED Abstract]
Perrot A, Lauwers-Cances V, Corre J, et al.: Minimal residual disease negativity using deep sequencing is a major prognostic factor in multiple myeloma. Blood 132 (23): 2456-2464, 2018. [PUBMED Abstract]
San-Miguel J, Avet-Loiseau H, Paiva B, et al.: Sustained minimal residual disease negativity in newly diagnosed multiple myeloma and the impact of daratumumab in MAIA and ALCYONE. Blood 139 (4): 492-501, 2022. [PUBMED Abstract]
Avet-Loiseau H, San-Miguel J, Casneuf T, et al.: Evaluation of Sustained Minimal Residual Disease Negativity With Daratumumab-Combination Regimens in Relapsed and/or Refractory Multiple Myeloma: Analysis of POLLUX and CASTOR. J Clin Oncol 39 (10): 1139-1149, 2021. [PUBMED Abstract]
de Tute RM, Pawlyn C, Cairns DA, et al.: Minimal Residual Disease After Autologous Stem-Cell Transplant for Patients With Myeloma: Prognostic Significance and the Impact of Lenalidomide Maintenance and Molecular Risk. J Clin Oncol 40 (25): 2889-2900, 2022. [PUBMED Abstract]
Paiva B, Manrique I, Dimopoulos MA, et al.: MRD dynamics during maintenance for improved prognostication of 1280 patients with myeloma in the TOURMALINE-MM3 and -MM4 trials. Blood 141 (6): 579-591, 2023. [PUBMED Abstract]
Goicoechea I, Puig N, Cedena MT, et al.: Deep MRD profiling defines outcome and unveils different modes of treatment resistance in standard- and high-risk myeloma. Blood 137 (1): 49-60, 2021. [PUBMED Abstract]
Cavo M, San-Miguel J, Usmani SZ, et al.: Prognostic value of minimal residual disease negativity in myeloma: combined analysis of POLLUX, CASTOR, ALCYONE, and MAIA. Blood 139 (6): 835-844, 2022. [PUBMED Abstract]
Pasquini MC, Wallace PK, Logan B, et al.: Minimal Residual Disease Status in Multiple Myeloma 1 Year After Autologous Hematopoietic Cell Transplantation and Lenalidomide Maintenance Are Associated With Long-Term Overall Survival. J Clin Oncol 42 (23): 2757-2768, 2024. [PUBMED Abstract]
Costa LJ, Chhabra S, Medvedova E, et al.: Daratumumab, Carfilzomib, Lenalidomide, and Dexamethasone With Minimal Residual Disease Response-Adapted Therapy in Newly Diagnosed Multiple Myeloma. J Clin Oncol 40 (25): 2901-2912, 2022. [PUBMED Abstract]
Lasa M, Notarfranchi L, Agullo C, et al.: Minimally Invasive Assessment of Peripheral Residual Disease During Maintenance or Observation in Transplant-Eligible Patients With Multiple Myeloma. J Clin Oncol 43 (2): 125-132, 2025. [PUBMED Abstract]
Sonneveld P, Dimopoulos MA, Boccadoro M, et al.: Daratumumab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 390 (4): 301-313, 2024. [PUBMED Abstract]
Voorhees PM, Sborov DW, Laubach J, et al.: Addition of daratumumab to lenalidomide, bortezomib, and dexamethasone for transplantation-eligible patients with newly diagnosed multiple myeloma (GRIFFIN): final analysis of an open-label, randomised, phase 2 trial. Lancet Haematol 10 (10): e825-e837, 2023. [PUBMED Abstract]
Yamamoto C, Minakata D, Koyama S, et al.: Daratumumab in first-line therapy is cost-effective in transplant-eligible patients with newly diagnosed myeloma. Blood 140 (6): 594-607, 2022. [PUBMED Abstract]
Kaiser MF, Hall A, Walker K, et al.: Daratumumab, Cyclophosphamide, Bortezomib, Lenalidomide, and Dexamethasone as Induction and Extended Consolidation Improves Outcome in Ultra-High-Risk Multiple Myeloma. J Clin Oncol 41 (23): 3945-3955, 2023. [PUBMED Abstract]
Brown S, Sherratt D, Hinsley S, et al.: MUKnine OPTIMUM protocol: a screening study to identify high-risk patients with multiple myeloma suitable for novel treatment approaches combined with a phase II study evaluating optimised combination of biological therapy in newly diagnosed high-risk multiple myeloma and plasma cell leukaemia. BMJ Open 11 (3): e046225, 2021. [PUBMED Abstract]
Goldschmidt H, Hegenbart U, Wallmeier M, et al.: Factors influencing collection of peripheral blood progenitor cells following high-dose cyclophosphamide and granulocyte colony-stimulating factor in patients with multiple myeloma. Br J Haematol 98 (3): 736-44, 1997. [PUBMED Abstract]
Mateos MV, Richardson PG, Schlag R, et al.: Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol 28 (13): 2259-66, 2010. [PUBMED Abstract]
Richardson PG, Sonneveld P, Schuster M, et al.: Extended follow-up of a phase 3 trial in relapsed multiple myeloma: final time-to-event results of the APEX trial. Blood 110 (10): 3557-60, 2007. [PUBMED Abstract]
Richardson PG, Briemberg H, Jagannath S, et al.: Frequency, characteristics, and reversibility of peripheral neuropathy during treatment of advanced multiple myeloma with bortezomib. J Clin Oncol 24 (19): 3113-20, 2006. [PUBMED Abstract]
San-Miguel JF, Richardson PG, Sonneveld P, et al.: Efficacy and safety of bortezomib in patients with renal impairment: results from the APEX phase 3 study. Leukemia 22 (4): 842-9, 2008. [PUBMED Abstract]
Rajkumar SV, Jacobus S, Callander NS, et al.: Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial. Lancet Oncol 11 (1): 29-37, 2010. [PUBMED Abstract]
Bradbury CA, Craig Z, Cook G, et al.: Thrombosis in patients with myeloma treated in the Myeloma IX and Myeloma XI phase 3 randomized controlled trials. Blood 136 (9): 1091-1104, 2020. [PUBMED Abstract]
Mikhael J, Manola J, Dueck AC, et al.: Lenalidomide and dexamethasone in patients with relapsed multiple myeloma and impaired renal function: PrE1003, a PrECOG study. Blood Cancer J 8 (9): 86, 2018. [PUBMED Abstract]
Zweegman S, Facon T, Hungria V, et al.: Phase 3 randomized study of daratumumab (DARA) + bortezomib, lenalidomide and dexamethasone (VRd) versus alone in patients with transplant-ineligible newly diagnosed multiple myeloma or for whom transplant is not planned as initial therapy: analysis of minimal residual disease in the Cepheus trial. [Abstract] Blood 144 (Suppl 1): A-362, 2024.
Facon T, Kumar SK, Plesner T, et al.: Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol 22 (11): 1582-1596, 2021. [PUBMED Abstract]
Perrot A, Facon T, Plesner T, et al.: Health-Related Quality of Life in Transplant-Ineligible Patients With Newly Diagnosed Multiple Myeloma: Findings From the Phase III MAIA Trial. J Clin Oncol 39 (3): 227-237, 2021. [PUBMED Abstract]
Mateos MV, Cavo M, Blade J, et al.: Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet 395 (10218): 132-141, 2020. [PUBMED Abstract]
Leleu X, Hulin C, Lambert J, et al.: Isatuximab, lenalidomide, dexamethasone and bortezomib in transplant-ineligible multiple myeloma: the randomized phase 3 BENEFIT trial. Nat Med 30 (8): 2235-2241, 2024. [PUBMED Abstract]
Facon T, Lee JH, Moreau P, et al.: Carfilzomib or bortezomib with melphalan-prednisone for transplant-ineligible patients with newly diagnosed multiple myeloma. Blood 133 (18): 1953-1963, 2019. [PUBMED Abstract]
Kumar SK, Jacobus SJ, Cohen AD, et al.: Carfilzomib or bortezomib in combination with lenalidomide and dexamethasone for patients with newly diagnosed multiple myeloma without intention for immediate autologous stem-cell transplantation (ENDURANCE): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol 21 (10): 1317-1330, 2020. [PUBMED Abstract]
Sonneveld P, Chanan-Khan A, Weisel K, et al.: Overall Survival With Daratumumab, Bortezomib, and Dexamethasone in Previously Treated Multiple Myeloma (CASTOR): A Randomized, Open-Label, Phase III Trial. J Clin Oncol 41 (8): 1600-1609, 2023. [PUBMED Abstract]
Dimopoulos MA, Oriol A, Nahi H, et al.: Daratumumab, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 375 (14): 1319-1331, 2016. [PUBMED Abstract]
Patel KK, Giri S, Parker TL, et al.: Cost-Effectiveness of First-Line Versus Second-Line Use of Daratumumab in Older, Transplant-Ineligible Patients With Multiple Myeloma. J Clin Oncol 39 (10): 1119-1128, 2021. [PUBMED Abstract]
Siegel DS, Desikan KR, Mehta J, et al.: Age is not a prognostic variable with autotransplants for multiple myeloma. Blood 93 (1): 51-4, 1999. [PUBMED Abstract]
Badros A, Barlogie B, Siegel E, et al.: Autologous stem cell transplantation in elderly multiple myeloma patients over the age of 70 years. Br J Haematol 114 (3): 600-7, 2001. [PUBMED Abstract]
Lenhoff S, Hjorth M, Westin J, et al.: Impact of age on survival after intensive therapy for multiple myeloma: a population-based study by the Nordic Myeloma Study Group. Br J Haematol 133 (4): 389-96, 2006. [PUBMED Abstract]
Munshi PN, Vesole D, Jurczyszyn A, et al.: Age no bar: A CIBMTR analysis of elderly patients undergoing autologous hematopoietic cell transplantation for multiple myeloma. Cancer 126 (23): 5077-5087, 2020. [PUBMED Abstract]
Munshi PN, Vesole DH, St Martin A, et al.: Outcomes of upfront autologous hematopoietic cell transplantation in patients with multiple myeloma who are 75 years old or older. Cancer 127 (22): 4233-4239, 2021. [PUBMED Abstract]
Attal M, Harousseau JL, Stoppa AM, et al.: A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Français du Myélome. N Engl J Med 335 (2): 91-7, 1996. [PUBMED Abstract]
Child JA, Morgan GJ, Davies FE, et al.: High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med 348 (19): 1875-83, 2003. [PUBMED Abstract]
Palumbo A, Bringhen S, Petrucci MT, et al.: Intermediate-dose melphalan improves survival of myeloma patients aged 50 to 70: results of a randomized controlled trial. Blood 104 (10): 3052-7, 2004. [PUBMED Abstract]
Segeren CM, Sonneveld P, van der Holt B, et al.: Overall and event-free survival are not improved by the use of myeloablative therapy following intensified chemotherapy in previously untreated patients with multiple myeloma: a prospective randomized phase 3 study. Blood 101 (6): 2144-51, 2003. [PUBMED Abstract]
Fermand JP, Katsahian S, Divine M, et al.: High-dose therapy and autologous blood stem-cell transplantation compared with conventional treatment in myeloma patients aged 55 to 65 years: long-term results of a randomized control trial from the Group Myelome-Autogreffe. J Clin Oncol 23 (36): 9227-33, 2005. [PUBMED Abstract]
Bladé J, Rosiñol L, Sureda A, et al.: High-dose therapy intensification compared with continued standard chemotherapy in multiple myeloma patients responding to the initial chemotherapy: long-term results from a prospective randomized trial from the Spanish cooperative group PETHEMA. Blood 106 (12): 3755-9, 2005. [PUBMED Abstract]
Barlogie B, Kyle RA, Anderson KC, et al.: Standard chemotherapy compared with high-dose chemoradiotherapy for multiple myeloma: final results of phase III US Intergroup Trial S9321. J Clin Oncol 24 (6): 929-36, 2006. [PUBMED Abstract]
Cook G, Williams C, Brown JM, et al.: High-dose chemotherapy plus autologous stem-cell transplantation as consolidation therapy in patients with relapsed multiple myeloma after previous autologous stem-cell transplantation (NCRI Myeloma X Relapse [Intensive trial]): a randomised, open-label, phase 3 trial. Lancet Oncol 15 (8): 874-85, 2014. [PUBMED Abstract]
Gay F, Oliva S, Petrucci MT, et al.: Chemotherapy plus lenalidomide versus autologous transplantation, followed by lenalidomide plus prednisone versus lenalidomide maintenance, in patients with multiple myeloma: a randomised, multicentre, phase 3 trial. Lancet Oncol 16 (16): 1617-29, 2015. [PUBMED Abstract]
Richardson PG, Jacobus SJ, Weller EA, et al.: Triplet Therapy, Transplantation, and Maintenance until Progression in Myeloma. N Engl J Med 387 (2): 132-147, 2022. [PUBMED Abstract]
Lévy V, Katsahian S, Fermand JP, et al.: A meta-analysis on data from 575 patients with multiple myeloma randomly assigned to either high-dose therapy or conventional therapy. Medicine (Baltimore) 84 (4): 250-60, 2005. [PUBMED Abstract]
Dhakal B, Szabo A, Chhabra S, et al.: Autologous Transplantation for Newly Diagnosed Multiple Myeloma in the Era of Novel Agent Induction: A Systematic Review and Meta-analysis. JAMA Oncol 4 (3): 343-350, 2018. [PUBMED Abstract]
Chakraborty R, Siddiqi R, Willson G, et al.: Impact of autologous transplantation on survival in patients with newly diagnosed multiple myeloma who have high-risk cytogenetics: A meta-analysis of randomized controlled trials. Cancer 128 (12): 2288-2297, 2022. [PUBMED Abstract]
Pineda-Roman M, Barlogie B, Anaissie E, et al.: High-dose melphalan-based autotransplants for multiple myeloma: the Arkansas experience since 1989 in 3077 patients. Cancer 112 (8): 1754-64, 2008. [PUBMED Abstract]
Badar T, Hari P, Dávila O, et al.: African Americans with translocation t(11;14) have superior survival after autologous hematopoietic cell transplantation for multiple myeloma in comparison with Whites in the United States. Cancer 127 (1): 82-92, 2021. [PUBMED Abstract]
Barlogie B, Tricot GJ, van Rhee F, et al.: Long-term outcome results of the first tandem autotransplant trial for multiple myeloma. Br J Haematol 135 (2): 158-64, 2006. [PUBMED Abstract]
Barlogie B, Tricot G, Rasmussen E, et al.: Total therapy 2 without thalidomide in comparison with total therapy 1: role of intensified induction and posttransplantation consolidation therapies. Blood 107 (7): 2633-8, 2006. [PUBMED Abstract]
Barlogie B, Zangari M, Bolejack V, et al.: Superior 12-year survival after at least 4-year continuous remission with tandem transplantations for multiple myeloma. Clin Lymphoma Myeloma 6 (6): 469-74, 2006. [PUBMED Abstract]
Bruno B, Rotta M, Patriarca F, et al.: Nonmyeloablative allografting for newly diagnosed multiple myeloma: the experience of the Gruppo Italiano Trapianti di Midollo. Blood 113 (14): 3375-82, 2009. [PUBMED Abstract]
Rotta M, Storer BE, Sahebi F, et al.: Long-term outcome of patients with multiple myeloma after autologous hematopoietic cell transplantation and nonmyeloablative allografting. Blood 113 (14): 3383-91, 2009. [PUBMED Abstract]
Kumar A, Kharfan-Dabaja MA, Glasmacher A, et al.: Tandem versus single autologous hematopoietic cell transplantation for the treatment of multiple myeloma: a systematic review and meta-analysis. J Natl Cancer Inst 101 (2): 100-6, 2009. [PUBMED Abstract]
Stadtmauer EA, Pasquini MC, Blackwell B, et al.: Autologous Transplantation, Consolidation, and Maintenance Therapy in Multiple Myeloma: Results of the BMT CTN 0702 Trial. J Clin Oncol 37 (7): 589-597, 2019. [PUBMED Abstract]
Moreau P, Garban F, Attal M, et al.: Long-term follow-up results of IFM99-03 and IFM99-04 trials comparing nonmyeloablative allotransplantation with autologous transplantation in high-risk de novo multiple myeloma. Blood 112 (9): 3914-5, 2008. [PUBMED Abstract]
Bruno B, Rotta M, Patriarca F, et al.: A comparison of allografting with autografting for newly diagnosed myeloma. N Engl J Med 356 (11): 1110-20, 2007. [PUBMED Abstract]
Gahrton G, Iacobelli S, Björkstrand B, et al.: Autologous/reduced-intensity allogeneic stem cell transplantation vs autologous transplantation in multiple myeloma: long-term results of the EBMT-NMAM2000 study. Blood 121 (25): 5055-63, 2013. [PUBMED Abstract]
Rosiñol L, Pérez-Simón JA, Sureda A, et al.: A prospective PETHEMA study of tandem autologous transplantation versus autograft followed by reduced-intensity conditioning allogeneic transplantation in newly diagnosed multiple myeloma. Blood 112 (9): 3591-3, 2008. [PUBMED Abstract]
Armeson KE, Hill EG, Costa LJ: Tandem autologous vs autologous plus reduced intensity allogeneic transplantation in the upfront management of multiple myeloma: meta-analysis of trials with biological assignment. Bone Marrow Transplant 48 (4): 562-7, 2013. [PUBMED Abstract]
Kharfan-Dabaja MA, Hamadani M, Reljic T, et al.: Comparative efficacy of tandem autologous versus autologous followed by allogeneic hematopoietic cell transplantation in patients with newly diagnosed multiple myeloma: a systematic review and meta-analysis of randomized controlled trials. J Hematol Oncol 6: 2, 2013. [PUBMED Abstract]
Naumann-Winter F, Greb A, Borchmann P, et al.: First-line tandem high-dose chemotherapy and autologous stem cell transplantation versus single high-dose chemotherapy and autologous stem cell transplantation in multiple myeloma, a systematic review of controlled studies. Cochrane Database Syst Rev 10: CD004626, 2012. [PUBMED Abstract]
Reynolds C, Ratanatharathorn V, Adams P, et al.: Allogeneic stem cell transplantation reduces disease progression compared to autologous transplantation in patients with multiple myeloma. Bone Marrow Transplant 27 (8): 801-7, 2001. [PUBMED Abstract]
Arora M, McGlave PB, Burns LJ, et al.: Results of autologous and allogeneic hematopoietic cell transplant therapy for multiple myeloma. Bone Marrow Transplant 35 (12): 1133-40, 2005. [PUBMED Abstract]
Lokhorst H, Einsele H, Vesole D, et al.: International Myeloma Working Group consensus statement regarding the current status of allogeneic stem-cell transplantation for multiple myeloma. J Clin Oncol 28 (29): 4521-30, 2010. [PUBMED Abstract]
Sahebi F, Shen Y, Thomas SH, et al.: Late relapses following reduced intensity allogeneic transplantation in patients with multiple myeloma: a long-term follow-up study. Br J Haematol 160 (2): 199-206, 2013. [PUBMED Abstract]
Lokhorst HM, van der Holt B, Cornelissen JJ, et al.: Donor versus no-donor comparison of newly diagnosed myeloma patients included in the HOVON-50 multiple myeloma study. Blood 119 (26): 6219-25; quiz 6399, 2012. [PUBMED Abstract]
Giaccone L, Storer B, Patriarca F, et al.: Long-term follow-up of a comparison of nonmyeloablative allografting with autografting for newly diagnosed myeloma. Blood 117 (24): 6721-7, 2011. [PUBMED Abstract]
Vasudevan Nampoothiri R, Pasic I, Law AD, et al.: Allogeneic hematopoietic stem cell transplantation in patients with therapy-related hematologic malignancies developing after multiple myeloma. Eur J Haematol 108 (5): 430-436, 2022. [PUBMED Abstract]
Cook G, Ashcroft AJ, Cairns DA, et al.: The effect of salvage autologous stem-cell transplantation on overall survival in patients with relapsed multiple myeloma (final results from BSBMT/UKMF Myeloma X Relapse [Intensive]): a randomised, open-label, phase 3 trial. Lancet Haematol 3 (7): e340-51, 2016. [PUBMED Abstract]
Ahmedzai SH, Snowden JA, Ashcroft AJ, et al.: Patient-Reported Outcome Results From the Open-Label, Randomized Phase III Myeloma X Trial Evaluating Salvage Autologous Stem-Cell Transplantation in Relapsed Multiple Myeloma. J Clin Oncol 37 (19): 1617-1628, 2019. [PUBMED Abstract]
Veltri LW, Milton DR, Delgado R, et al.: Outcome of autologous hematopoietic stem cell transplantation in refractory multiple myeloma. Cancer 123 (18): 3568-3575, 2017. [PUBMED Abstract]
Ludwig H, Durie BG, McCarthy P, et al.: IMWG consensus on maintenance therapy in multiple myeloma. Blood 119 (13): 3003-15, 2012. [PUBMED Abstract]
Benboubker L, Dimopoulos MA, Dispenzieri A, et al.: Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med 371 (10): 906-17, 2014. [PUBMED Abstract]
Palumbo A, Gay F, Cavallo F, et al.: Continuous Therapy Versus Fixed Duration of Therapy in Patients With Newly Diagnosed Multiple Myeloma. J Clin Oncol 33 (30): 3459-66, 2015. [PUBMED Abstract]
Shustik C, Belch A, Robinson S, et al.: A randomised comparison of melphalan with prednisone or dexamethasone as induction therapy and dexamethasone or observation as maintenance therapy in multiple myeloma: NCIC CTG MY.7. Br J Haematol 136 (2): 203-11, 2007. [PUBMED Abstract]
Berenson JR, Crowley JJ, Grogan TM, et al.: Maintenance therapy with alternate-day prednisone improves survival in multiple myeloma patients. Blood 99 (9): 3163-8, 2002. [PUBMED Abstract]
The Myeloma Trialists’ Collaborative Group: Interferon as therapy for multiple myeloma: an individual patient data overview of 24 randomized trials and 4012 patients. Br J Haematol 113 (4): 1020-34, 2001. [PUBMED Abstract]
Badros A, Foster L, Anderson LD, et al.: Daratumumab with lenalidomide as maintenance after transplant in newly diagnosed multiple myeloma: the AURIGA study. Blood 145 (3): 300-310, 2025. [PUBMED Abstract]
Holstein SA, Jung SH, Richardson PG, et al.: Updated analysis of CALGB (Alliance) 100104 assessing lenalidomide versus placebo maintenance after single autologous stem-cell transplantation for multiple myeloma: a randomised, double-blind, phase 3 trial. Lancet Haematol 4 (9): e431-e442, 2017. [PUBMED Abstract]
Jackson GH, Davies FE, Pawlyn C, et al.: Lenalidomide maintenance versus observation for patients with newly diagnosed multiple myeloma (Myeloma XI): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 20 (1): 57-73, 2019. [PUBMED Abstract]
McCarthy PL, Holstein SA, Petrucci MT, et al.: Lenalidomide Maintenance After Autologous Stem-Cell Transplantation in Newly Diagnosed Multiple Myeloma: A Meta-Analysis. J Clin Oncol 35 (29): 3279-3289, 2017. [PUBMED Abstract]
Wang Y, Yang F, Shen Y, et al.: Maintenance Therapy With Immunomodulatory Drugs in Multiple Myeloma: A Meta-Analysis and Systematic Review. J Natl Cancer Inst 108 (3): , 2016. [PUBMED Abstract]
Gay F, Jackson G, Rosiñol L, et al.: Maintenance Treatment and Survival in Patients With Myeloma: A Systematic Review and Network Meta-analysis. JAMA Oncol 4 (10): 1389-1397, 2018. [PUBMED Abstract]
Moreau P, Hulin C, Perrot A, et al.: Maintenance with daratumumab or observation following treatment with bortezomib, thalidomide, and dexamethasone with or without daratumumab and autologous stem-cell transplant in patients with newly diagnosed multiple myeloma (CASSIOPEIA): an open-label, randomised, phase 3 trial. Lancet Oncol 22 (10): 1378-1390, 2021. [PUBMED Abstract]
Dimopoulos MA, Špička I, Quach H, et al.: Ixazomib as Postinduction Maintenance for Patients With Newly Diagnosed Multiple Myeloma Not Undergoing Autologous Stem Cell Transplantation: The Phase III TOURMALINE-MM4 Trial. J Clin Oncol 38 (34): 4030-4041, 2020. [PUBMED Abstract]
Dytfeld D, Wróbel T, Jamroziak K, et al.: Carfilzomib, lenalidomide, and dexamethasone or lenalidomide alone as maintenance therapy after autologous stem-cell transplantation in patients with multiple myeloma (ATLAS): interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol 24 (2): 139-150, 2023. [PUBMED Abstract]
Touzeau C, Perrot A: Daratumumab for maintenance in myeloma. Blood 145 (3): 251-252, 2025. [PUBMED Abstract]
Panopoulou A, Cairns DA, Holroyd A, et al.: Optimizing the value of lenalidomide maintenance by extended genetic profiling: an analysis of 556 patients in the Myeloma XI trial. Blood 141 (14): 1666-1674, 2023. [PUBMED Abstract]
Palumbo A, Bringhen S, Rossi D, et al.: Overall survival benefit for bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. [Abstract] Blood 120 (21): A-200, 2012.
Olszewski AJ, Dusetzina SB, Eaton CB, et al.: Subsidies for Oral Chemotherapy and Use of Immunomodulatory Drugs Among Medicare Beneficiaries With Myeloma. J Clin Oncol 35 (29): 3306-3314, 2017. [PUBMED Abstract]
Olszewski AJ, Dusetzina SB, Trivedi AN, et al.: Prescription Drug Coverage and Outcomes of Myeloma Therapy Among Medicare Beneficiaries. J Clin Oncol 36 (28): 2879-2886, 2018. [PUBMED Abstract]
van de Donk NWCJ, Yong K: Oral proteasome inhibitor maintenance for multiple myeloma. Lancet 393 (10168): 204-205, 2019. [PUBMED Abstract]
Morgan GJ, Davies FE, Gregory WM, et al.: First-line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma (MRC Myeloma IX): a randomised controlled trial. Lancet 376 (9757): 1989-99, 2010. [PUBMED Abstract]
Morgan GJ, Child JA, Gregory WM, et al.: Effects of zoledronic acid versus clodronic acid on skeletal morbidity in patients with newly diagnosed multiple myeloma (MRC Myeloma IX): secondary outcomes from a randomised controlled trial. Lancet Oncol 12 (8): 743-52, 2011. [PUBMED Abstract]
Morgan GJ, Davies FE, Gregory WM, et al.: Effects of induction and maintenance plus long-term bisphosphonates on bone disease in patients with multiple myeloma: the Medical Research Council Myeloma IX Trial. Blood 119 (23): 5374-83, 2012. [PUBMED Abstract]
Himelstein AL, Foster JC, Khatcheressian JL, et al.: Effect of Longer-Interval vs Standard Dosing of Zoledronic Acid on Skeletal Events in Patients With Bone Metastases: A Randomized Clinical Trial. JAMA 317 (1): 48-58, 2017. [PUBMED Abstract]
Badros A, Weikel D, Salama A, et al.: Osteonecrosis of the jaw in multiple myeloma patients: clinical features and risk factors. J Clin Oncol 24 (6): 945-52, 2006. [PUBMED Abstract]
Kademani D, Koka S, Lacy MQ, et al.: Primary surgical therapy for osteonecrosis of the jaw secondary to bisphosphonate therapy. Mayo Clin Proc 81 (8): 1100-3, 2006. [PUBMED Abstract]
Lacy MQ, Dispenzieri A, Gertz MA, et al.: Mayo clinic consensus statement for the use of bisphosphonates in multiple myeloma. Mayo Clin Proc 81 (8): 1047-53, 2006. [PUBMED Abstract]
Jakubowiak AJ, Kendall T, Al-Zoubi A, et al.: Phase II trial of combination therapy with bortezomib, pegylated liposomal doxorubicin, and dexamethasone in patients with newly diagnosed myeloma. J Clin Oncol 27 (30): 5015-22, 2009. [PUBMED Abstract]
Terpos E, Sezer O, Croucher PI, et al.: The use of bisphosphonates in multiple myeloma: recommendations of an expert panel on behalf of the European Myeloma Network. Ann Oncol 20 (8): 1303-17, 2009. [PUBMED Abstract]
Berenson JR, Lichtenstein A, Porter L, et al.: Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. Myeloma Aredia Study Group. J Clin Oncol 16 (2): 593-602, 1998. [PUBMED Abstract]
Gimsing P, Carlson K, Turesson I, et al.: Effect of pamidronate 30 mg versus 90 mg on physical function in patients with newly diagnosed multiple myeloma (Nordic Myeloma Study Group): a double-blind, randomised controlled trial. Lancet Oncol 11 (10): 973-82, 2010. [PUBMED Abstract]
Rosen LS, Gordon D, Kaminski M, et al.: Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial. Cancer 98 (8): 1735-44, 2003. [PUBMED Abstract]
Chakraborty R, Majhail NS, Anwer F: Denosumab vs Zoledronic Acid for Bone-Targeted Therapy in Multiple Myeloma: What Are the Unanswered Questions? JAMA Oncol 5 (8): 1095-1096, 2019. [PUBMED Abstract]
Rades D, Hoskin PJ, Stalpers LJ, et al.: Short-course radiotherapy is not optimal for spinal cord compression due to myeloma. Int J Radiat Oncol Biol Phys 64 (5): 1452-7, 2006. [PUBMED Abstract]
Catell D, Kogen Z, Donahue B, et al.: Multiple myeloma of an extremity: must the entire bone be treated? Int J Radiat Oncol Biol Phys 40 (1): 117-9, 1998. [PUBMED Abstract]
Treatment of Relapsed or Refractory Multiple Myeloma
Treatment Options for Relapsed or Refractory Multiple Myeloma
Relapses occur for almost all patients after induction therapy, consolidation with autologous stem cell transplant (SCT), and maintenance therapy. During initial therapy, some patients have poor disease response, or their disease progresses. The general strategy is to give new therapies sequentially as required. In fit patients, reinduction therapy with response may be consolidated with an autologous SCT or allogeneic SCT in some cases. Sometimes, when relapse occurs 1 year or more after initial therapy, the same drugs can be administered a second time.
A subgroup of patients who do not achieve a response to induction chemotherapy have stable disease and a survival prognosis that is as good as that for responding patients.[1,2] When the stable nature of the disease becomes established, these patients can discontinue therapy until the myeloma begins to progress again. Other patients with primary refractory myeloma and progressive disease require a change in therapy. For more information, see the Treatment of Multiple Myeloma section.
For patients with disease response to initial therapy, the myeloma growth rate, as measured by the monoclonal (or myeloma) protein-doubling time, increases progressively with each subsequent relapse, and remission durations become shorter and shorter. Marrow function becomes increasingly compromised as patients develop pancytopenia and enter a refractory phase; occasionally, the myeloma cells dedifferentiate and extramedullary plasmacytomas develop. The myeloma cells may still be sensitive to chemotherapy, but the regrowth rate during relapse is so rapid that progressive improvement is not observed.
Combinations of drugs or single agents may be given sequentially as required. The goal is to avoid symptoms and adverse consequences of relapsing disease. However, the onset of therapy may be delayed because of slow disease progression and good performance status.
Treatment options for relapsed or refractory multiple myeloma include:
Daratumumab is a monoclonal antibody targeting CD38 that can be given on its own but is usually given in combination with other drugs. Although it is given as an infusion, the subcutaneous formulation has equivalent efficacy and fewer adverse events.[3]
Evidence (daratumumab):
In the prospective CASTOR trial (NCT02136134), 498 previously treated patients were randomly assigned to receive either daratumumab, bortezomib, and dexamethasone (DVd) or bortezomib and dexamethasone (Vd).[4]
With a median follow-up of 72.6 months, the median overall survival (OS) was 49.6 months for patients in the DVd group and 38.5 months for patients in the Vd group (hazard ratio [HR], 0.74; 95% confidence interval [CI], 0.59–0.92; P = .0075).[4][Level of evidence A1]
In the prospective POLLUX trial (NCT02076009), 569 previously treated patients were randomly assigned to receive either daratumumab, lenalidomide, and dexamethasone (DRd) or lenalidomide and dexamethasone (Rd).[5,6]
With a median follow-up of 79.7 months, the median OS was 67.6 months for patients in the DRd group and 51.8 months for patients in the Rd group (HR, 0.73; 95% CI, 0.58–0.91; P = .0044).[6][Level of evidence A1]
In a prospective trial (NCT03158688), 466 previously treated patients were randomly assigned in a 2:1 ratio to receive either daratumumab, carfilzomib, and dexamethasone or carfilzomib and dexamethasone.[7]
With a median follow-up of 27.8 months, the median progression-free survival (PFS) was 28.6 months (95% CI, 25.6–29.5) in the daratumumab group and 15.2 months (11.1–19.9) in the control arm (log-rank P < .0001).[8][Level of evidence B1]
In a prospective randomized trial, 1,304 previously treated patients received either daratumumab plus pomalidomide and dexamethasone (DPd) or pomalidomide and dexamethasone (Pd) alone.[9]
With a median follow-up of 16.9 months, the median PFS was 12.4 months (95% CI, 8.3–19.3) for patients who received DPd and 6.9 months (95% CI, 5.5–9.3) for patients who received Pd (HR, 0.63; 95% CI, 0.47–0.85; P = .0018).[9][Level of evidence B1]
Several phase I and phase II trials evaluated daratumumab as a single agent for relapsed or refractory multiple myeloma.[10–12]
With a median follow-up of 12 to 17 months, the overall response rate was 31% and 36%, with minimal response or stable disease in about 40% of patients.[10–12][Level of evidence C3]
In every prospective randomized trial to date, adding daratumumab to other active myeloma combination therapies improved responses and PFS when compared with the combination therapies alone.
Elotuzumab
Elotuzumab is a monoclonal antibody directed at SLAMF7 (signaling lymphocytic activation molecule F7).
Evidence (elotuzumab):
A prospective trial (ELOQUENT-3 [NCT02654132]) included 117 patients with relapsed or refractory disease after both lenalidomide and a proteasome inhibitor. Patients were randomly assigned to receive either elotuzumab, pomalidomide, and dexamethasone (EPd) or Pd.[13]
With a median follow-up of 45 months, the median OS was 29.8 months (22.9–45.7) for patients who received EPd compared with 17.4 months (13.8–27.7) for patients who received Pd (HR, 0.59; 95% CI, 0.37–0.93; P = .0217).[13][Level of evidence A1]
In a prospective randomized trial (ELOQUENT-2 [NCT01239797]) of 646 patients with relapsed or refractory myeloma, elotuzumab was combined with lenalidomide and dexamethasone and compared with Rd alone.[14][Level of evidence A1]
With a median follow-up of 70.6 months, the 5-year PFS rate was 17% in the elotuzumab group and 11% in the Rd group (HR, 0.73; 95% CI, 0.60–0.89; P = .0014). The 5-year OS rate was 40% in the elotuzumab group and 33% in the Rd group (HR, 0.82; 95.4% CI, 0.68–1.00; P = .0408).[14]
Isatuximab
Isatuximab is a monoclonal antibody directed against CD38.
Evidence (isatuximab):
In a prospective randomized trial of 387 patients with relapsed or refractory disease, Pd was given with or without isatuximab.[15]
With a median follow-up of 35.3 months, the median OS was 24.6 months (95% CI, 20.3–31.3) for patients who received isatuximab plus PD and 17.7 months (95% CI, 14.4–26.2) for patients who received Pd alone (HR, 0.76; 95% CI, 0.57–1.01; 2-sided P = .056).
Similarly, the median PFS was 17.5 months (95% CI, 14.9–19.2) for the isatuximab group and 12.9 months (95% CI, 10.1–16.6) for the Pd group (HR, 0.76; 95% CI, 0.58–0.99; P = .020).[15][Level of evidence B1]
In a prospective randomized trial of 302 patients with relapsed or refractory disease, the combination of carfilzomib and dexamethasone was given with or without isatuximab.
With a median follow-up of 20.7 months, the 2-year PFS rate was 68.9% (95% CI, 60.7%–75.8%) for patients who received isatuximab group and 45.7% (95% CI, 35.2%–55.6%) for patients who received carfilzomib and dexamethasone alone (HR, 0.53; 99% CI, 0.32–0.89; 2-sided P = .0014).[16][Level of evidence B1]
There are no data comparing isatuximab with daratumumab, both of which target CD38. There are no data proving that isatuximab has efficacy in patients with disease that is resistant to daratumumab.
Proteasome inhibitors
Bortezomib
Bortezomib is the first-in-class proteasome inhibitor that is given subcutaneously on a weekly basis for 3 of every 4 weeks; the subcutaneous route is preferred to the intravenous (IV) route because it causes significantly less neuropathy and no loss of responsiveness.[17–19] Bortezomib is metabolized and cleared by the liver, and it appears to be active and well tolerated in patients with renal impairment.[20,21] More than 6 months after completion of bortezomib induction therapy, bortezomib can be given again with a 40% overall response rate, according to a meta-analysis of 23 phase II studies.[22][Level of evidence C3]
Evidence (bortezomib):
A prospective randomized study of 669 patients with relapsed myeloma compared bortezomib given by IV with high-dose oral dexamethasone.[23]
With a median follow-up of 22 months, the median OS was 29.8 months for bortezomib versus 23.7 months for dexamethasone (HR, 0.77; P = .027) even though the trial allowed crossover after relapse.[23][Level of evidence A1]
A prospective randomized trial (NCT00103506) of 646 previously treated patients compared bortezomib plus pegylated liposomal doxorubicin with bortezomib alone.[24]
With a median follow-up of 7.0 months, 1-year OS rates were better in patients who received the combination (82% vs. 75%; P = .05).[24][Level of evidence A1]
A prospective randomized trial of 260 newly diagnosed patients aged 65 years and older compared bortezomib, melphalan, and prednisone (VMP) with bortezomib, thalidomide, and prednisone (VTP).[25]
With a median follow-up of 72 months, the median OS favored the VMP arm, 63 months versus 43 months for the VTP group (HR, 0.67; 95% CI, 0.49–0.91; P = .01).[25][Level of evidence A1]
Carfilzomib
Carfilzomib is a second-generation proteasome inhibitor that is given by IV (unlike the subcutaneous route for bortezomib). Most studies have used twice-weekly administration, but once-weekly administration appears at least equally efficacious and safe.[26]
Evidence (carfilzomib):
A prospective randomized trial included 578 patients with relapsed or refractory myeloma.[26]
The median PFS of patients who received carfilzomib once a week was significantly better (11.2 months; 95% CI, 8.6‒13.0) than twice a week (7.6 months; 95% CI, 5.8‒9.2) (HR, 0.69; 95% CI, 0.54‒0.83; P = .0029).[26][Level of evidence B1]
In a prospective randomized trial of 792 patients with relapsed or refractory myeloma, the combination of carfilzomib, lenalidomide, and dexamethasone was compared with Rd.[27]
With a median follow-up of 67.1 months, median OS in the carfilzomib arm was 48.3 months (95% CI, 42.4‒52.8) versus 40.4 months (95% CI, 33.6‒44.4) (HR, 0.79; 95% CI, 0.67‒0.95; one-sided P = .009).[27][Level of evidence A1]
In a preplanned subgroup analysis, patients with high-risk cytogenetics (i.e., t(4;14), t(14;16), del(17p)) also had improved PFS with the triplet regimen (23 months vs. 14 months; HR, 0.70; 95% CI, 0.43−1.16; one-sided P = .083). Response rates were also improved, but the carfilzomib combination did not abrogate the worse prognosis.[28][Level of evidence B3]
A prospective randomized study (NCT01568866) of 929 patients compared carfilzomib and dexamethasone with bortezomib and dexamethasone.[29]
With a median follow-up of 37 months, the median OS was 47.6 months (95% CI, 42.5–not evaluable) for the carfilzomib combination compared with 40.0 months (95% CI, 32.6–42.3) for the bortezomib combination (HR, 0.79; 95% CI, 0.65–0.96; P = .020).[29][Level of evidence A1]
Cardiovascular adverse events such as heart failure, chest pain, and acute coronary syndrome (grade 3 or higher) occurred in 25% of patients, especially in the first 3 months of therapy.[30,31]
A systematic review and meta-analysis demonstrated that renal adverse events occurred in 21% of patients of patients who received carfilzomib, and 8.3% had grade 3 to 5 toxicities. Acute kidney injury was the most common renal toxicity.[32]
Ixazomib
Ixazomib is a second-generation proteasome inhibitor that is given orally on a weekly basis for 3 of every 4 weeks.
Evidence (ixazomib):
In a prospective randomized trial involving 722 patients with relapsed or refractory myeloma, ixazomib combined with lenalidomide and dexamethasone was compared with a placebo combined with lenalidomide and dexamethasone.[33,34]
With a median follow-up of 2 years, the median PFS was 20.6 months in the ixazomib group versus 14.7 months for the placebo group (HR, 0.66; 95% CI, 0.47–0.93; P = .016).[33][Level of evidence B1]
Improved PFS was also seen for high-risk patients (defined by fluorescence in situ hybridization and cytogenetics).[34][Level of evidence B1]
No grade 3 or 4 neuropathy was seen in any patient treated with ixazomib.
With a median follow-up of 85 months, there was little difference in the median OS at 53.6 months for the ixazomib group and 51.6 months for the placebo group (HR, 0.939; P = .49).[35][Level of evidence B1 based on PFS, as noted above]
A prospective randomized trial (NCT01850524) included 705 patients with newly diagnosed, transplant-eligible multiple myeloma. The study compared ixazomib combined with lenalidomide and dexamethasone with a placebo combined with lenalidomide and dexamethasone.[36]
With a median follow-up of 53.3 to 55.8 months for each arm, the median PFS was 35.3 months in the ixazomib group versus 21.8 months in the placebo group (HR, 0.830; 95% CI, 0.676–1.018; P = .073).[36][Level of evidence B1] This difference did not meet statistical significance for PFS.
A prospective randomized trial of patients with relapsed myeloma undergoing a second autologous SCT compared consolidation and maintenance therapy with ixazomib versus observation alone.[37]
With a median follow-up of 27 months, the median PFS was 20 months in the consolidation and maintenance therapy group and 13 months in the observation group (HR, 0.55; 95% CI, 0.39–0.78; P = .0006).[37][Level of evidence B1]
CAR T-cell therapy
CAR T-cell therapy is a cellular therapy for refractory and/or multiply relapsed myeloma. This therapy consists of autologous anti-BCMA transduced T cells. This therapy has shown a 50% to 65% complete remission rate and a median PFS of 18 to 20 months in patients from highly selected nonrandomized series.[38–40][Level of evidence C3] Based on the durable responses in these nonrandomized series, the U.S. Food and Drug Administration (FDA) approved the BCMA-directed CAR T-cell products idecabtagene vicleucel (ide-cel) and ciltacabtagene autoleucel (cilta-cel) for patients with relapsed or refractory disease. A review of the management of moderate-to-severe immune-related adverse events suggests immediate use of corticosteroids and supportive hospital care.[41] Other molecular targets and expanded clinical approaches are being investigated.[42][Level of evidence C3]
Ciltacabtagene autoleucel
Evidence (cilta-cel):
A prospective randomized trial (NCT04181827) included 419 patients with relapsed myeloma after one to three prior lines of treatment who also had lenalidomide-refractory disease. Patients received either CAR T-cell therapy with cilta-cel or the standard of care at the discretion of physicians.[43]
With a median follow-up of 15.9 months, the 12-month PFS rate was 75.9% (95% CI, 69.4%–81.1%) in the cilta-cel group and 48.6% (95% CI, 41.5%–55.3%) in the standard-of-care group (HR, 0.26; 95% CI, 0.18–0.38; P < .001).[43][Level of evidence B1]
No difference in OS was reported. Grade 3 or higher cytokine-release syndrome occurred in 1.1% of patients in the CAR T-cell therapy group, and no patients had grade 3 or higher neurotoxicity.
Two patients developed a T-cell lymphoma on the skin at 5 and 16 months after cilta-cell infusion, and the T cells had detectable CAR transgenic expression and integration.[44] Both patients attained a complete response with lymphoma-directed therapy.
A quality-of-life evaluation showed significant improvement in global health status and visual analogue scale responses for patients who received cilta-cel.[45][Level of evidence A3]
Based on this trial, the FDA approved cilta-cel for patients with (1) relapsed or refractory myeloma after at least one line of therapy including a proteosome inhibitor (such as bortezomib) and an immunomodulatory agent (such as lenalidomide) AND (2) lenalidomide-refractory disease.
Idecabtagene vicleucel (ide-cel)
Evidence (ide-cel):
A prospective randomized trial (NCT03651128) included 386 patients with relapsed or refractory myeloma after two to four prior lines of treatment who also had lenalidomide-refractory disease. Patients received either CAR T-cell therapy with ide-cel or one of five standard alternative regimens.[46,47]
With a median follow-up of 30.9 months, the median PFS was 13.8 months in the ide-cel group versus 4.4 months in the standard-regimen group (HR, 0.49; 95% CI, 0.38–0.63; P < .0001).[47][Level of evidence B1]
The overall and complete response rates were higher in patients who received ide-cel (71% and 39%, respectively) than in patients who received the standard regimens (42% and 5%, respectively).
Grade 3 or 4 adverse events occurred in 93% of patients who received ide-cel and 75% who received a standard regimen. Ide-cel was associated with cytokine-release syndrome in 88% of patients (grade 3 or higher in 5% of patients) and with neurological symptoms in 15% of patients (grade 3 or higher in 3% of patients).
Based on this trial, the FDA approved ide-cel for patients with (1) relapsed or refractory myeloma after at least two lines of therapy AND (2) lenalidomide-refractory disease.
Bispecific antibody therapy
Bispecific antibodies target both CD3, which is on the surface of T cells, and either BCMA or GPRC5D (G protein–coupled receptor family C group 5 member D), both of which concentrate on the surface of myeloma cells.[48,49]
Teclistamab
Teclistamab is a T-cell-redirecting bispecific antibody.
Evidence (teclistamab):
In a phase I/II study (NCT03145181 and NCT04557098), teclistamab was given to 165 patients with relapsed or refractory myeloma who received at last four prior systemic treatments.[50]
With a median follow-up of 14.1 months, the overall response rate was 63.0%, with a complete response rate of 39.4%. The median PFS was 11.3 months (95% CI, 8.8–17.1).[50][Level of evidence C3]
Side effects included cytokine release syndrome in 72% of patients (grade 3 or 4 in only one patient) and hematologic toxicity (grade 3 or 4) in 61% of patients, including febrile neutropenia (44.8%).
Of the 165 patients, 40 patients who had received prior anti-BCMA therapy (an antibody-drug conjugate or CAR T-cell therapy) were assessed at a median follow-up of 28.0 months.[51] The overall response rate was 52.5%. A total of 47.5% of patients had a very good partial response or better, and 30.0% of patients had a complete response or better. The median duration of response was 14.8 months.[51][Level of evidence C3]
Patients receiving teclistamab can be given replacement immunoglobulin G IV or subcutaneously every 2 to 4 weeks to reduce the risk of infection.[52] Replacement of immunoglobulin G may be applicable for patients receiving other bispecific antibodies.
Talquetamab
Talquetamab is a T-cell-redirecting bispecific antibody that targets GPRC5D, a receptor highly expressed on plasma cells, along with CD3.
Evidence (talquetamab):
In a phase II study, talquetamab was given to 232 patients with relapsed or refractory myeloma who had received at least four prior systemic treatments.[53]
At a median follow-up of 11.7 months, the overall response rate was 73.6% (95% CI, 63%–82.4%). Approximately 85% of responders were still in remission by 9 months.[53,54][Level of evidence C3]
Cytokine release syndrome occurred in up to 89% patients and was grade 1 or 2 in all but one case. Skin-related events and dysgeusia occurred in 60% to 70% of patients.
Elranatamab
Elranatamab is a T-cell directing bispecific antibody targeting BCMA and CD3.
Evidence (elranatamab):
Elranatamab was given to 187 patients with relapsed or refractory myeloma who received at least four prior lines of therapy.[55]
With a median follow-up of 14.7 months, the objective response rate was 61% (95% CI, 51.8%–69.6%), and 35% of patients achieved a complete response. The 15-month PFS rate was 50.9% (95% CI, 40.9%–60.0%).[55][Level of evidence C3]
Summary: Patients with myeloma who have received one to four prior lines of therapy, are refractory to proteosome inhibitors and immunomodulatory agents, and are also experiencing a slow relapse are often referred for CAR T-cell therapy. This is because delays in production of the CAR T-cell agent are less problematic, and because time receiving therapy is fixed and short-term, allowing a long duration therapy-free time after a response.[49] Patients who experience a quick relapse may benefit from an “off-the-shelf” bispecific antibody that results in similar response rates and durability of response, but this approach comes with the downside of required continual therapy.[49] The choice of bispecific antibody cannot be made based on any clinical evidence because of the lack of comparative trials. In heavily pretreated patients, bispecific antibodies impair humoral immunity, but this can be ameliorated using IV or subcutaneous immunoglobulin and antimicrobial prophylaxis.[49] Current logic supports using products with different targets sequentially.
Immunomodulatory agents
Pomalidomide
Pomalidomide is a third-generation immunomodulatory agent. Pomalidomide is associated with some myelosuppression and an increased incidence of thromboembolic events, as noted with lenalidomide and thalidomide (requiring thromboprophylaxis with aspirin at least), but very little peripheral neuropathy compared with other agents.
Evidence (pomalidomide):
A prospective trial (ELOQUENT-3 [NCT02654132]) included 117 patients who had relapsed or refractory disease after both lenalidomide and a proteasome inhibitor. Patients were randomly assigned to receive either EPd or Pd.[13]
With a median follow-up of 45 months, the median OS was 29.8 months (95% CI, 22.9–45.7) for patients who received EPd compared with 17.4 months (95% CI, 13.8–27.7) for patients who received Pd (HR, 0.59; 95% CI, 0.37–0.93; P = .0217).[13][Level of evidence A1]
In a prospective trial of 559 patients with relapsed or refractory myeloma and previous treatment with lenalidomide, patients were randomly assigned to receive either pomalidomide plus bortezomib and dexamethasone or Vd.[56]
With a median follow-up of 15.9 months, the median PFS was 11.2 months (95% CI, 9.7−13.7) in the pomalidomide combination group and 7.1 months (95% CI, 5.9−8.9) in the Vd group (HR, 0.61; 95% CI, 0.49−0.77; P < .001).[56][Level of evidence B1]
For 302 patients with relapsed or refractory disease, Pd (40 mg weekly) was compared with a higher-dose dexamethasone regimen (40 mg daily for 4 days every 8 days).[57]
With a median follow-up of 10.0 months, the PFS was superior for the pomalidomide arm, at 4.0 months versus 1.9 months (HR, 0.48; 95% CI, 0.39–0.60; P < .0001)[57][Level of evidence B1]
Lenalidomide
Lenalidomide is a second-generation immunomodulatory agent. Lenalidomide is associated with increased incidence of thromboembolic events, as noted with pomalidomide and thalidomide (requiring thromboprophylaxis with aspirin at least), myelosuppression (more than pomalidomide), and neuropathy (less than thalidomide, but more than pomalidomide).[58–62]
A meta-analysis of 3,254 patients from seven randomized trials showed that lenalidomide was associated with an increased risk of hematologic second primary malignancies (3.1% in patients who received lenalidomide vs. 1.4% in those who did not; HR, 3.8; 95% CI, 1.15–12.62; P = .029).[63] This risk was confined to the combination of lenalidomide and melphalan (HR, 4.86; 95% CI, 2.79–8.46; P = .0001) but was not higher for lenalidomide with either cyclophosphamide or dexamethasone.[63] A retrospective review of almost 4,000 patients with relapsed or refractory disease who received lenalidomide in 11 clinical trials suggested an increased incidence of nonmelanoma skin cancers.[64]
As a result of predominant renal clearance, lenalidomide doses need to be reduced for patients with impaired renal function (creatinine clearance, 30–50: 10 mg every day; creatinine clearance, <30: 15 mg every other day; dialysis, 15 mg on day after dialysis).[65] Uncontrolled trials have added clarithromycin (500 mg twice a day) to lenalidomide and dexamethasone, with reports of increased response rates.[66] Controlled studies are required to establish the value of this approach.
Evidence (lenalidomide):
Two prospective randomized and placebo-controlled studies of 351 and 353 patients with relapsed myeloma compared lenalidomide plus high-dose dexamethasone versus high-dose dexamethasone alone.[67,68]
With a median follow-up of 16 to 26 months, the median OS was 29.6 months or more (not reached in one trial) versus 20.2 months to 20.6 months in the control group (HR, 0.66; 95% CI, 0.45‒0.96; P = .03 in one study [67] and P < .001 in the other study).[68][Level of evidence A1]
A prospective randomized study of 1,623 patients with transplant-ineligible, previously untreated myeloma compared lenalidomide and dexamethasone given until disease progression with a 72-week induction regimen with melphalan, prednisone, and thalidomide (MPT) for 72 weeks.[59]
With a median follow-up of 46 months, there was improved OS for the lenalidomide group, with 4-year OS rates of 52% versus 38% (HR, 0.72; 95% CI, 0.54–0.96; P = .02).[59][Level of evidence A1]
Thalidomide
Thalidomide is a first-generation immunomodulatory agent that is not often used because of its sedative and constipating effects, its significant and potentially debilitating neuropathy, and its thrombogenic effect (thromboprophylaxis is required).[69,70] Very little myelosuppression is seen with this agent.
Late in the disease course, when all other options have failed, thalidomide can be employed, sometimes with durable responses.[71] By using a low dose (50 mg by mouth every day), significant sedation, constipation, and neuropathy may be avoided. Thromboprophylaxis with aspirin, warfarin, or low-molecular-weight heparin is required; the choice of therapy depends on preexisting risk factors.[62]
Evidence (thalidomide):
A meta-analysis of 1,685 previously untreated patients considered six prospective randomized trials comparing thalidomide, melphalan, and prednisone versus melphalan and prednisone alone.[72]
The addition of thalidomide improved median OS from 32.7 months to 39.3 months (HR, 0.83; 95% CI, 0.73–0.94; P = .004).[72][Level of evidence A1]
BCMA-targeting antibody-drug conjugates
Belantamab mafodotin
Belantamab mafodotin is an antibody-drug conjugate composed of an anti-BCMA monoclonal antibody attached to monomethyl auristatin, which inhibits microtubule formation. In 2020, the FDA approved this antibody-drug conjugate for patients with relapsed or refractory myeloma. However, this approval was withdrawn in 2023 based on findings from a prospective randomized trial in 325 patients with relapsed or refractory myeloma, which compared belantamab mafodotin with pomalidomide plus dexamethasone and showed no significant difference in median PFS.[73][Level of evidence B1] Since then, the results of several European clinical trials may revive interest in seeking FDA approval in the United States.
Evidence (belantamab mafodotin):
A prospective randomized trial (NCT04246047) included 494 patients with relapsed or refractory myeloma. Patients received either belantamab mafodotin plus Vd or DVd.[74,75]
With a median follow-up of 28.2 months, the 3-year OS rate was 74% for the belantamab-Vd group and 60% for the DVd group (HR, 0.58; 95% CI, 0.43–0.79; P = .00023).[75][Level of evidence A1]
The median PFS was 36.6 months for the belantamab mafodotin-Vd group and 13.4 months for the DVd group (HR, 0.41; 95% CI, 0.31–0.53; P < .001).[74][Level of evidence B1]
Belantamab mafodotin is known to cause ocular toxicity (mostly in the cornea) which was noted in 79% of patients who received the drug in this trial. Monthly corneal examinations allowed for dose modification, and 98% of patients regained normal vision from 20/50 or worse.
A prospective randomized trial (NCT04484623) included 302 patients with relapsed or refractory myeloma. Patients received either belantamab mafodotin plus Pd (BPd) or PVd (pomalidomide, bortezomib, and dexamethasone).[76]
With a median follow-up of 21.8 months, the 1-year PFS rate was 71% for the BPd group and 51% for the PVd group (HR, 0.52; 95% CI, 0.37–0.73; P < .001).[76][Level of evidence B1]
Belantamab mafodotin is known to cause ocular toxicity (usually in the cornea). Grade 3 or 4 ocular toxicity occurred in 43% of patients who received the drug in this trial (all-grades toxicity occurred in 89% of patients). Monthly corneal examinations allowed for dose modification, and 9% of patients in the BPd group required early treatment discontinuation.
Summary: The use of BCMA-targeted therapy in the second- or third-line of therapy appears better than the usual standard of care. FDA approval may occur after review of these European trials. The use of belantamab mafodotin may affect the subsequent efficacy of other BCMA-directed therapies that have already been approved by the FDA, including the CAR T-cell therapies, cilta-cel and ide-cel, and the bispecific BCMA T-cell enhancers, teclistamab and elranatamab. Clinical trials must establish the correct sequencing of BCMA-directed therapies. In the meantime, belantamab mafodotin has not been approved by the FDA.
Cyclophosphamide (+ bortezomib + dexamethasone in the CyBorD regimen).[81,82]
Pegylated liposomal doxorubicin (in a modified VAD regimen) [83,84] or combined with bortezomib and dexamethasone.[85]
Evidence (chemotherapy):
A meta-analysis of prospective randomized trials compared melphalan and prednisone with combinations of other cytotoxic agents. No differences were noted in PFS or OS.[78][Level of evidence A1]
The VAD regimen has shown activity in previously untreated patients and in relapsed patients, with response rates ranging from 60% to 80%.[79,80][Level of evidence C3] Because of logistics problems delivering a 96-hour infusion of doxorubicin, substitution with pegylated liposomal doxorubicin provides comparable response rates.[83,84]
Chemotherapy alone has been used to obtain a clinical remission after exhausting most of the new regimens, allowing improvement in performance status that may permit subsequent use of clinical trials investigating alternative therapies.
Selinexor
Selinexor is a selective inhibitor of nuclear export compounds that blocks exportin 1 (which activates tumor suppressor proteins), inhibits nuclear factor κB, and reduces oncoprotein mRNA translation.
Selinexor (evidence):
A prospective randomized trial included 402 patients with relapsed or refractory disease. Patients received either selinexor plus bortezomib and dexamethasone (SVd) or Vd.[86]
With a median follow-up of 13.2 months (SVd) or 16.5 months (Vd), the median PFS was 13.9 months (95% CI, 11.7–not evaluable) for patients who received SVd and 9.5 months (95% CI, 8.1–10.8) for patients who received Vd (HR, 0.70; 95% CI, 0.53–0.93; P = .0075).[86][Level of evidence B1]
Patients who received the selinexor combination had more thrombocytopenia (39% vs. 17%) and fatigue (13% vs. 1%).
In a phase IIB multicenter study, 122 patients with multiply resistant myeloma refractory to a proteasome inhibitor, an immunomodulatory agent, and daratumumab received oral selinexor and dexamethasone.[87] High-risk cytogenetics were present in 53% of patients. Patients had received a median of seven previous regimens.
A partial response or better was observed in 26% of patients (95% CI, 19%−35%), with a median duration of response of 4.4 months. The median PFS was 3.7 months; median OS was 8.6 months.[87][Level of evidence C3]
In a phase II study of 42 patients with relapsed or refractory disease, patients received SVd.[88]
A partial response or better was observed in 63% of patients, with a median PFS of 9.0 months.[88][Level of evidence C3]
Selinexor has significant side effects, including nausea, vomiting, fatigue, diarrhea, weight loss, poor appetite, and cytopenias. A descriptive retrospective study of 437 patients enrolled in clinical trials focused on aggressive medical support for these side effects.[89]
Venetoclax
Venetoclax is a selective BCL-2 inhibitor that induces apoptosis in myeloma cells, particularly in those with t(11;14), which expresses high levels of bcl2.
Evidence (venetoclax):
In a phase I study of 66 heavily pretreated patients with relapsed or refractory myeloma, 30 patients harbored a t(11;14) translocation.[90]
Among all 66 patients, the overall response rate was 21%, and 15% of patients achieved very good partial response or better. For those with t(11;14), the overall response rate was 40%, with 27% achieving a very good partial response or better.[90][Level of evidence C3]
In a prospective trial (BELLINI [NCT02755597]), 291 patients with relapsed or refractory myeloma were randomly assigned to receive venetoclax plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone.[91]
With a median follow-up of 18.7 months, the median PFS was 22.4 months for patients on the venetoclax arm versus 11.5 months for patients on the placebo arm (HR, 0.63; 95% CI, 0.44–0.90; P = .01).
OS favored the placebo arm because of treatment-related sepsis (HR, 2.03; 95% CI, 1.04–3.95; P = .034).[91][Level of evidence A1]
A prespecified analysis of 35 patients with t(11;14) translocation (20 patients who received venetoclax and 15 patients who received placebo) resulted in the median PFS not being reached for patients on the venetoclax arm versus 9.5 months for patients on the placebo arm (HR, 0.11; 95% CI, 0.02–0.56; P = .004).[91][Level of evidence B1]
BRAF/MEK inhibitors
Although activating BRAF variants are rarely found in patients with newly diagnosed myeloma, these variants appear in multiple-relapsing disease. Twelve such patients with a BRAF V600E variant who received encorafenib and binimetinib had an overall response rate of 83.3%, a median PFS of 5.6 months, and an OS rate of 55% at 24 months.[92][Level of evidence C3]
Corticosteroids
Dexamethasone dosage has been evaluated in two prospective randomized trials.
A prospective randomized study (ECOG-E4A03) of 445 previously untreated patients with myeloma compared lenalidomide and high-dose dexamethasone (40 mg on days 1–4, 9–12, and 17–20, every 28 days) with lenalidomide and low-dose dexamethasone (40 mg on days 1, 8, 15, and 22, every 28 days).[58]
With a median follow-up of 36 months, the 2-year OS rate favored the low-dose dexamethasone arm (87% vs. 75%; P = .006), despite no difference in PFS.[58][Level of evidence A1]
The increased deaths on the high-dose dexamethasone arm were attributed to cardiopulmonary toxicity.
Deep venous thromboses (DVTs) were also more frequent in the high-dose arm (25% vs. 9%). Patients in the low-dose dexamethasone arm with lenalidomide experienced less than 5% DVT with aspirin alone.
A prospective randomized trial of melphalan and prednisone versus melphalan and high-dose dexamethasone showed no difference in PFS or OS, but there was an increase in infection in the high-dose dexamethasone arm.[93]
A retrospective review of 541 patients in pooled myeloma studies from the Southwest Oncology Group found frequent dosage reductions of dexamethasone because of toxicity. These dose reductions did not appear to impact PFS or OS.[94][Level of evidence C3]
Summary: Although prospective randomized trials are needed to clarify the role of corticosteroids or their dose, it is doubtful that those studies will ever be performed.
Based on these trials, all ongoing trials and regimens use the low-dose dexamethasone schedule in combination with other therapeutic agents: 40 mg dexamethasone (oral or IV) weekly in fit patients, or 20 mg (oral or IV) in less-fit patients at higher risk for complications.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Riccardi A, Mora O, Tinelli C, et al.: Response to first-line chemotherapy and long-term survival in patients with multiple myeloma: results of the MM87 prospective randomised protocol. Eur J Cancer 39 (1): 31-7, 2003. [PUBMED Abstract]
Durie BG, Jacobson J, Barlogie B, et al.: Magnitude of response with myeloma frontline therapy does not predict outcome: importance of time to progression in southwest oncology group chemotherapy trials. J Clin Oncol 22 (10): 1857-63, 2004. [PUBMED Abstract]
Usmani SZ, Nahi H, Mateos MV, et al.: Subcutaneous delivery of daratumumab in relapsed or refractory multiple myeloma. Blood 134 (8): 668-677, 2019. [PUBMED Abstract]
Sonneveld P, Chanan-Khan A, Weisel K, et al.: Overall Survival With Daratumumab, Bortezomib, and Dexamethasone in Previously Treated Multiple Myeloma (CASTOR): A Randomized, Open-Label, Phase III Trial. J Clin Oncol 41 (8): 1600-1609, 2023. [PUBMED Abstract]
Dimopoulos MA, Oriol A, Nahi H, et al.: Daratumumab, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 375 (14): 1319-1331, 2016. [PUBMED Abstract]
Dimopoulos MA, Oriol A, Nahi H, et al.: Overall Survival With Daratumumab, Lenalidomide, and Dexamethasone in Previously Treated Multiple Myeloma (POLLUX): A Randomized, Open-Label, Phase III Trial. J Clin Oncol 41 (8): 1590-1599, 2023. [PUBMED Abstract]
Usmani SZ, Quach H, Mateos MV, et al.: Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): updated outcomes from a randomised, multicentre, open-label, phase 3 study. Lancet Oncol 23 (1): 65-76, 2022. [PUBMED Abstract]
Dimopoulos M, Quach H, Mateos MV, et al.: Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): results from a randomised, multicentre, open-label, phase 3 study. Lancet 396 (10245): 186-197, 2020. [PUBMED Abstract]
Dimopoulos MA, Terpos E, Boccadoro M, et al.: Daratumumab plus pomalidomide and dexamethasone versus pomalidomide and dexamethasone alone in previously treated multiple myeloma (APOLLO): an open-label, randomised, phase 3 trial. Lancet Oncol 22 (6): 801-812, 2021. [PUBMED Abstract]
Usmani SZ, Weiss BM, Plesner T, et al.: Clinical efficacy of daratumumab monotherapy in patients with heavily pretreated relapsed or refractory multiple myeloma. Blood 128 (1): 37-44, 2016. [PUBMED Abstract]
Lokhorst HM, Plesner T, Laubach JP, et al.: Targeting CD38 with Daratumumab Monotherapy in Multiple Myeloma. N Engl J Med 373 (13): 1207-19, 2015. [PUBMED Abstract]
Plesner T, Arkenau HT, Gimsing P, et al.: Phase 1/2 study of daratumumab, lenalidomide, and dexamethasone for relapsed multiple myeloma. Blood 128 (14): 1821-1828, 2016. [PUBMED Abstract]
Dimopoulos MA, Dytfeld D, Grosicki S, et al.: Elotuzumab Plus Pomalidomide and Dexamethasone for Relapsed/Refractory Multiple Myeloma: Final Overall Survival Analysis From the Randomized Phase II ELOQUENT-3 Trial. J Clin Oncol 41 (3): 568-578, 2023. [PUBMED Abstract]
Dimopoulos MA, Lonial S, White D, et al.: Elotuzumab, lenalidomide, and dexamethasone in RRMM: final overall survival results from the phase 3 randomized ELOQUENT-2 study. Blood Cancer J 10 (9): 91, 2020. [PUBMED Abstract]
Richardson PG, Perrot A, San-Miguel J, et al.: Isatuximab plus pomalidomide and low-dose dexamethasone versus pomalidomide and low-dose dexamethasone in patients with relapsed and refractory multiple myeloma (ICARIA-MM): follow-up analysis of a randomised, phase 3 study. Lancet Oncol 23 (3): 416-427, 2022. [PUBMED Abstract]
Moreau P, Dimopoulos MA, Mikhael J, et al.: Isatuximab, carfilzomib, and dexamethasone in relapsed multiple myeloma (IKEMA): a multicentre, open-label, randomised phase 3 trial. Lancet 397 (10292): 2361-2371, 2021. [PUBMED Abstract]
Bringhen S, Larocca A, Rossi D, et al.: Efficacy and safety of once-weekly bortezomib in multiple myeloma patients. Blood 116 (23): 4745-53, 2010. [PUBMED Abstract]
Mateos MV, Oriol A, Martínez-López J, et al.: Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial. Lancet Oncol 11 (10): 934-41, 2010. [PUBMED Abstract]
Moreau P, Pylypenko H, Grosicki S, et al.: Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma: a randomised, phase 3, non-inferiority study. Lancet Oncol 12 (5): 431-40, 2011. [PUBMED Abstract]
San-Miguel JF, Richardson PG, Sonneveld P, et al.: Efficacy and safety of bortezomib in patients with renal impairment: results from the APEX phase 3 study. Leukemia 22 (4): 842-9, 2008. [PUBMED Abstract]
Dimopoulos MA, Terpos E, Chanan-Khan A, et al.: Renal impairment in patients with multiple myeloma: a consensus statement on behalf of the International Myeloma Working Group. J Clin Oncol 28 (33): 4976-84, 2010. [PUBMED Abstract]
Knopf KB, Duh MS, Lafeuille MH, et al.: Meta-analysis of the efficacy and safety of bortezomib re-treatment in patients with multiple myeloma. Clin Lymphoma Myeloma Leuk 14 (5): 380-8, 2014. [PUBMED Abstract]
Richardson PG, Sonneveld P, Schuster M, et al.: Extended follow-up of a phase 3 trial in relapsed multiple myeloma: final time-to-event results of the APEX trial. Blood 110 (10): 3557-60, 2007. [PUBMED Abstract]
Orlowski RZ, Nagler A, Sonneveld P, et al.: Randomized phase III study of pegylated liposomal doxorubicin plus bortezomib compared with bortezomib alone in relapsed or refractory multiple myeloma: combination therapy improves time to progression. J Clin Oncol 25 (25): 3892-901, 2007. [PUBMED Abstract]
Mateos MV, Oriol A, Martínez-López J, et al.: GEM2005 trial update comparing VMP/VTP as induction in elderly multiple myeloma patients: do we still need alkylators? Blood 124 (12): 1887-93, 2014. [PUBMED Abstract]
Moreau P, Mateos MV, Berenson JR, et al.: Once weekly versus twice weekly carfilzomib dosing in patients with relapsed and refractory multiple myeloma (A.R.R.O.W.): interim analysis results of a randomised, phase 3 study. Lancet Oncol 19 (7): 953-964, 2018. [PUBMED Abstract]
Siegel DS, Dimopoulos MA, Ludwig H, et al.: Improvement in Overall Survival With Carfilzomib, Lenalidomide, and Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma. J Clin Oncol 36 (8): 728-734, 2018. [PUBMED Abstract]
Avet-Loiseau H, Fonseca R, Siegel D, et al.: Carfilzomib significantly improves the progression-free survival of high-risk patients in multiple myeloma. Blood 128 (9): 1174-80, 2016. [PUBMED Abstract]
Dimopoulos MA, Goldschmidt H, Niesvizky R, et al.: Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): an interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol 18 (10): 1327-1337, 2017. [PUBMED Abstract]
Cornell RF, Ky B, Weiss BM, et al.: Prospective Study of Cardiac Events During Proteasome Inhibitor Therapy for Relapsed Multiple Myeloma. J Clin Oncol 37 (22): 1946-1955, 2019. [PUBMED Abstract]
Waxman AJ, Clasen S, Hwang WT, et al.: Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol 4 (3): e174519, 2018. [PUBMED Abstract]
Ball S, Behera TR, Anwer F, et al.: Risk of kidney toxicity with carfilzomib in multiple myeloma: a meta-analysis of randomized controlled trials. Ann Hematol 99 (6): 1265-1271, 2020. [PUBMED Abstract]
Moreau P, Masszi T, Grzasko N, et al.: Oral Ixazomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 374 (17): 1621-34, 2016. [PUBMED Abstract]
Richardson PG, Kumar SK, Masszi T, et al.: Final Overall Survival Analysis of the TOURMALINE-MM1 Phase III Trial of Ixazomib, Lenalidomide, and Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma. J Clin Oncol 39 (22): 2430-2442, 2021. [PUBMED Abstract]
Facon T, Venner CP, Bahlis NJ, et al.: Oral ixazomib, lenalidomide, and dexamethasone for transplant-ineligible patients with newly diagnosed multiple myeloma. Blood 137 (26): 3616-3628, 2021. [PUBMED Abstract]
Cook G, Ashcroft AJ, Senior E, et al.: Ixazomib as consolidation and maintenance versus observation in patients with relapsed multiple myeloma eligible for salvage autologous stem-cell transplantation (Myeloma XII [ACCoRD]): interim analysis of a multicentre, open-label, randomised, phase 3 trial. Lancet Haematol 11 (11): e816-e829, 2024. [PUBMED Abstract]
Wang Y, Cao J, Gu W, et al.: Long-Term Follow-Up of Combination of B-Cell Maturation Antigen and CD19 Chimeric Antigen Receptor T Cells in Multiple Myeloma. J Clin Oncol 40 (20): 2246-2256, 2022. [PUBMED Abstract]
Munshi NC, Anderson LD, Shah N, et al.: Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N Engl J Med 384 (8): 705-716, 2021. [PUBMED Abstract]
Martin T, Usmani SZ, Berdeja JG, et al.: Ciltacabtagene Autoleucel, an Anti-B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. J Clin Oncol 41 (6): 1265-1274, 2023. [PUBMED Abstract]
Santomasso BD, Nastoupil LJ, Adkins S, et al.: Management of Immune-Related Adverse Events in Patients Treated With Chimeric Antigen Receptor T-Cell Therapy: ASCO Guideline. J Clin Oncol 39 (35): 3978-3992, 2021. [PUBMED Abstract]
Mailankody S, Devlin SM, Landa J, et al.: GPRC5D-Targeted CAR T Cells for Myeloma. N Engl J Med 387 (13): 1196-1206, 2022. [PUBMED Abstract]
San-Miguel J, Dhakal B, Yong K, et al.: Cilta-cel or Standard Care in Lenalidomide-Refractory Multiple Myeloma. N Engl J Med 389 (4): 335-347, 2023. [PUBMED Abstract]
Harrison SJ, Touzeau C, Kint N, et al.: CAR+ T-Cell Lymphoma after Cilta-cel Therapy for Relapsed or Refractory Myeloma. N Engl J Med 392 (7): 677-685, 2025. [PUBMED Abstract]
Mina R, Mylin AK, Yokoyama H, et al.: Patient-reported outcomes following ciltacabtagene autoleucel or standard of care in patients with lenalidomide-refractory multiple myeloma (CARTITUDE-4): results from a randomised, open-label, phase 3 trial. Lancet Haematol 12 (1): e45-e56, 2025. [PUBMED Abstract]
Rodriguez-Otero P, Ailawadhi S, Arnulf B, et al.: Ide-cel or Standard Regimens in Relapsed and Refractory Multiple Myeloma. N Engl J Med 388 (11): 1002-1014, 2023. [PUBMED Abstract]
Ailawadhi S, Arnulf B, Patel K, et al.: Ide-cel vs standard regimens in triple-class-exposed relapsed and refractory multiple myeloma: updated KarMMa-3 analyses. Blood 144 (23): 2389-2401, 2024. [PUBMED Abstract]
Moreau P, Touzeau C: T-cell-redirecting bispecific antibodies in multiple myeloma: a revolution? Blood 139 (26): 3681-3687, 2022. [PUBMED Abstract]
Holstein SA, Grant SJ, Wildes TM: Chimeric Antigen Receptor T-Cell and Bispecific Antibody Therapy in Multiple Myeloma: Moving Into the Future. J Clin Oncol 41 (27): 4416-4429, 2023. [PUBMED Abstract]
Moreau P, Garfall AL, van de Donk NWCJ, et al.: Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med 387 (6): 495-505, 2022. [PUBMED Abstract]
Touzeau C, Krishnan AY, Moreau P, et al.: Efficacy and safety of teclistamab in patients with relapsed/refractory multiple myeloma after BCMA-targeting therapies. Blood 144 (23): 2375-2388, 2024. [PUBMED Abstract]
Cheruvalath H, Clennon A, Shrestha A, et al.: Effects of intravenous immunoglobulin supplementation (IVIG) on infections in recipients of teclistamab therapy for multiple myeloma (MM): a multi-institutional study. [Abstract] Blood 144 (Suppl 1): A-256, 2024.
Chari A, Minnema MC, Berdeja JG, et al.: Talquetamab, a T-Cell-Redirecting GPRC5D Bispecific Antibody for Multiple Myeloma. N Engl J Med 387 (24): 2232-2244, 2022. [PUBMED Abstract]
U.S. Food and Drug Administration: FDA grants accelerated approval to talquetamab-tgvs for relapsed or refractory multiple myeloma. U.S. Food and Drug Administration, 2023. Available online. Last accessed April 23, 2025.
Lesokhin AM, Tomasson MH, Arnulf B, et al.: Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med 29 (9): 2259-2267, 2023. [PUBMED Abstract]
Richardson PG, Oriol A, Beksac M, et al.: Pomalidomide, bortezomib, and dexamethasone for patients with relapsed or refractory multiple myeloma previously treated with lenalidomide (OPTIMISMM): a randomised, open-label, phase 3 trial. Lancet Oncol 20 (6): 781-794, 2019. [PUBMED Abstract]
San Miguel J, Weisel K, Moreau P, et al.: Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol 14 (11): 1055-66, 2013. [PUBMED Abstract]
Rajkumar SV, Jacobus S, Callander NS, et al.: Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial. Lancet Oncol 11 (1): 29-37, 2010. [PUBMED Abstract]
Hulin C, Belch A, Shustik C, et al.: Updated Outcomes and Impact of Age With Lenalidomide and Low-Dose Dexamethasone or Melphalan, Prednisone, and Thalidomide in the Randomized, Phase III FIRST Trial. J Clin Oncol 34 (30): 3609-3617, 2016. [PUBMED Abstract]
Zangari M, Tricot G, Polavaram L, et al.: Survival effect of venous thromboembolism in patients with multiple myeloma treated with lenalidomide and high-dose dexamethasone. J Clin Oncol 28 (1): 132-5, 2010. [PUBMED Abstract]
Larocca A, Cavallo F, Bringhen S, et al.: Aspirin or enoxaparin thromboprophylaxis for patients with newly diagnosed multiple myeloma treated with lenalidomide. Blood 119 (4): 933-9; quiz 1093, 2012. [PUBMED Abstract]
Bradbury CA, Craig Z, Cook G, et al.: Thrombosis in patients with myeloma treated in the Myeloma IX and Myeloma XI phase 3 randomized controlled trials. Blood 136 (9): 1091-1104, 2020. [PUBMED Abstract]
Palumbo A, Bringhen S, Kumar SK, et al.: Second primary malignancies with lenalidomide therapy for newly diagnosed myeloma: a meta-analysis of individual patient data. Lancet Oncol 15 (3): 333-42, 2014. [PUBMED Abstract]
Dimopoulos MA, Richardson PG, Brandenburg N, et al.: A review of second primary malignancy in patients with relapsed or refractory multiple myeloma treated with lenalidomide. Blood 119 (12): 2764-7, 2012. [PUBMED Abstract]
Dimopoulos MA, Christoulas D, Roussou M, et al.: Lenalidomide and dexamethasone for the treatment of refractory/relapsed multiple myeloma: dosing of lenalidomide according to renal function and effect on renal impairment. Eur J Haematol 85 (1): 1-5, 2010. [PUBMED Abstract]
Rossi A, Mark T, Jayabalan D, et al.: BiRd (clarithromycin, lenalidomide, dexamethasone): an update on long-term lenalidomide therapy in previously untreated patients with multiple myeloma. Blood 121 (11): 1982-5, 2013. [PUBMED Abstract]
Dimopoulos M, Spencer A, Attal M, et al.: Lenalidomide plus dexamethasone for relapsed or refractory multiple myeloma. N Engl J Med 357 (21): 2123-32, 2007. [PUBMED Abstract]
Weber DM, Chen C, Niesvizky R, et al.: Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med 357 (21): 2133-42, 2007. [PUBMED Abstract]
Palumbo A, Cavo M, Bringhen S, et al.: Aspirin, warfarin, or enoxaparin thromboprophylaxis in patients with multiple myeloma treated with thalidomide: a phase III, open-label, randomized trial. J Clin Oncol 29 (8): 986-93, 2011. [PUBMED Abstract]
Delforge M, Bladé J, Dimopoulos MA, et al.: Treatment-related peripheral neuropathy in multiple myeloma: the challenge continues. Lancet Oncol 11 (11): 1086-95, 2010. [PUBMED Abstract]
Palumbo A, Facon T, Sonneveld P, et al.: Thalidomide for treatment of multiple myeloma: 10 years later. Blood 111 (8): 3968-77, 2008. [PUBMED Abstract]
Fayers PM, Palumbo A, Hulin C, et al.: Thalidomide for previously untreated elderly patients with multiple myeloma: meta-analysis of 1685 individual patient data from 6 randomized clinical trials. Blood 118 (5): 1239-47, 2011. [PUBMED Abstract]
Dimopoulos MA, Hungria VTM, Radinoff A, et al.: Efficacy and safety of single-agent belantamab mafodotin versus pomalidomide plus low-dose dexamethasone in patients with relapsed or refractory multiple myeloma (DREAMM-3): a phase 3, open-label, randomised study. Lancet Haematol 10 (10): e801-e812, 2023. [PUBMED Abstract]
Hungria V, Robak P, Hus M, et al.: Belantamab Mafodotin, Bortezomib, and Dexamethasone for Multiple Myeloma. N Engl J Med 391 (5): 393-407, 2024. [PUBMED Abstract]
Hungria V, Robak P, Hus M, et al.: Belantamab mafodotin, bortezomib, and dexamethasone vs daratumumab, bortezomib, and dexamethasone in relapsed/refractory multiple myeloma: overall survival analysis and updated efficacy outcomes of the phase 3 Dreamm-7 trial. [Abstract] Blood 144 (Suppl 1): A-772, 2024.
Dimopoulos MA, Beksac M, Pour L, et al.: Belantamab Mafodotin, Pomalidomide, and Dexamethasone in Multiple Myeloma. N Engl J Med 391 (5): 408-421, 2024. [PUBMED Abstract]
Gregory WM, Richards MA, Malpas JS: Combination chemotherapy versus melphalan and prednisolone in the treatment of multiple myeloma: an overview of published trials. J Clin Oncol 10 (2): 334-42, 1992. [PUBMED Abstract]
Combination chemotherapy versus melphalan plus prednisone as treatment for multiple myeloma: an overview of 6,633 patients from 27 randomized trials. Myeloma Trialists’ Collaborative Group. J Clin Oncol 16 (12): 3832-42, 1998. [PUBMED Abstract]
Segeren CM, Sonneveld P, van der Holt B, et al.: Vincristine, doxorubicin and dexamethasone (VAD) administered as rapid intravenous infusion for first-line treatment in untreated multiple myeloma. Br J Haematol 105 (1): 127-30, 1999. [PUBMED Abstract]
Anderson H, Scarffe JH, Ranson M, et al.: VAD chemotherapy as remission induction for multiple myeloma. Br J Cancer 71 (2): 326-30, 1995. [PUBMED Abstract]
Reece DE, Rodriguez GP, Chen C, et al.: Phase I-II trial of bortezomib plus oral cyclophosphamide and prednisone in relapsed and refractory multiple myeloma. J Clin Oncol 26 (29): 4777-83, 2008. [PUBMED Abstract]
Knop S, Liebisch H, Wandt H, et al.: Bortezomib, IV cyclophosphamide, and dexamethasone (VelCD) as induction therapy in newly diagnosed multiple myeloma: results of an interim analysis of the German DSMM Xia trial. [Abstract] J Clin Oncol 27 (Suppl 15): A-8516, 2009.
Dimopoulos MA, Pouli A, Zervas K, et al.: Prospective randomized comparison of vincristine, doxorubicin and dexamethasone (VAD) administered as intravenous bolus injection and VAD with liposomal doxorubicin as first-line treatment in multiple myeloma. Ann Oncol 14 (7): 1039-44, 2003. [PUBMED Abstract]
Rifkin RM, Gregory SA, Mohrbacher A, et al.: Pegylated liposomal doxorubicin, vincristine, and dexamethasone provide significant reduction in toxicity compared with doxorubicin, vincristine, and dexamethasone in patients with newly diagnosed multiple myeloma: a Phase III multicenter randomized trial. Cancer 106 (4): 848-58, 2006. [PUBMED Abstract]
Jakubowiak AJ, Kendall T, Al-Zoubi A, et al.: Phase II trial of combination therapy with bortezomib, pegylated liposomal doxorubicin, and dexamethasone in patients with newly diagnosed myeloma. J Clin Oncol 27 (30): 5015-22, 2009. [PUBMED Abstract]
Grosicki S, Simonova M, Spicka I, et al.: Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, phase 3 trial. Lancet 396 (10262): 1563-1573, 2020. [PUBMED Abstract]
Chari A, Vogl DT, Gavriatopoulou M, et al.: Oral Selinexor-Dexamethasone for Triple-Class Refractory Multiple Myeloma. N Engl J Med 381 (8): 727-738, 2019. [PUBMED Abstract]
Bahlis NJ, Sutherland H, White D, et al.: Selinexor plus low-dose bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma. Blood 132 (24): 2546-2554, 2018. [PUBMED Abstract]
Gavriatopoulou M, Chari A, Chen C, et al.: Integrated safety profile of selinexor in multiple myeloma: experience from 437 patients enrolled in clinical trials. Leukemia 34 (9): 2430-2440, 2020. [PUBMED Abstract]
Kumar S, Kaufman JL, Gasparetto C, et al.: Efficacy of venetoclax as targeted therapy for relapsed/refractory t(11;14) multiple myeloma. Blood 130 (22): 2401-2409, 2017. [PUBMED Abstract]
Kumar SK, Harrison SJ, Cavo M, et al.: Venetoclax or placebo in combination with bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma (BELLINI): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol 21 (12): 1630-1642, 2020. [PUBMED Abstract]
Giesen N, Chatterjee M, Scheid C, et al.: A phase 2 clinical trial of combined BRAF/MEK inhibition for BRAFV600E-mutated multiple myeloma. Blood 141 (14): 1685-1690, 2023. [PUBMED Abstract]
Shustik C, Belch A, Robinson S, et al.: A randomised comparison of melphalan with prednisone or dexamethasone as induction therapy and dexamethasone or observation as maintenance therapy in multiple myeloma: NCIC CTG MY.7. Br J Haematol 136 (2): 203-11, 2007. [PUBMED Abstract]
Banerjee R, Sexton R, Cowan AJ, et al.: Dexamethasone dose intensity does not impact outcomes in newly diagnosed multiple myeloma: a secondary SWOG analysis. Blood 145 (1): 75-84, 2025. [PUBMED Abstract]
Key References for Plasma Cell Neoplasms (Including Multiple Myeloma)
These references have been identified by members of the PDQ Adult Treatment Editorial Board as significant in the field of plasma cell neoplasms and multiple myeloma treatment. This list is provided to inform users of important studies that have helped shape the current understanding of and treatment options for plasma cell neoplasms and multiple myeloma. Listed after each reference are the sections within this summary where the reference is cited.
Facon T, Kumar SK, Plesner T, et al.: Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol 22 (11): 1582-1596, 2021. [PUBMED Abstract]
Moreau P, Masszi T, Grzasko N, et al.: Oral Ixazomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med 374 (17): 1621-34, 2016. [PUBMED Abstract]
Morgan GJ, Davies FE, Gregory WM, et al.: First-line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma (MRC Myeloma IX): a randomised controlled trial. Lancet 376 (9757): 1989-99, 2010. [PUBMED Abstract]
Palumbo A, Avet-Loiseau H, Oliva S, et al.: Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol 33 (26): 2863-9, 2015. [PUBMED Abstract]
Rajkumar SV, Dimopoulos MA, Palumbo A, et al.: International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 15 (12): e538-48, 2014. [PUBMED Abstract]
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Added text to state that when daratumumab is used for induction therapy, the fluorescence in situ hybridization–detected cytogenetic abnormality of t(11;14) no longer confers an adverse prognostic impact. However, the presence of 1q gain continues to be associated with a lower response rate and hematologic event-free survival during treatment of amyloid light chain amyloidosis (cited Chakraborty et al. as reference 24).
Added text to state that using peripheral blood to assess for measurable residual disease (MRD) appears feasible with next-generation flow and mass spectroscopy. This approach is less invasive than using bone marrow (cited Lasa et al. as reference 55).
Added text about a prospective randomized trial of 200 patients with newly diagnosed multiple myeloma who achieved a very good or better partial response, were MRD-positive on bone marrow, and who had not received daratumumab (or isatuximab) anti-CD38 therapy during induction. Patients were randomly assigned to receive either daratumumab and lenalidomide (Dara-R) or lenalidomide alone (cited Badros et al. as reference 130 and level of evidence B1).
Added text to state that one prospective trial found improved progression-free survival (PFS) for Dara-R compared with lenalidomide alone in a population that had undergone transplant and was naïve to anti-CD38 therapy. One trial establishing the daratumumab, bortezomib, lenalidomide, and dexamethasone (D-VRd) regimen for newly diagnosed patients included Dara-R maintenance in the D-VRd induction arm. The incremental impact of Dara-R maintenance therapy in patients who received daratumumab induction therapy has not been established. It is also unclear if patients with MRD-negative disease after induction therapy and transplant would benefit similarly since they were also not studied (cited Touzeau et al. as reference 139).
Revised text about the results of a prospective randomized trial that included 419 patients with relapsed myeloma after one to three prior lines of treatment who also had lenalidomide-refractory disease. Patients received either ciltacabtagene autoleucel or the standard of care at the discretion of physicians (cited Harrison et al. as reference 44, and Mina et al. as reference 45, level of evidence A3).
Added text about a retrospective review of 541 patients in pooled myeloma studies from the Southwest Oncology Group. The review found frequent dosage reductions of dexamethasone because of toxicity. These dose reductions did not appear to impact PFS or overall survival (cited Banerjee et al. as reference 94 and level of evidence C3). Also added text to state that although prospective randomized trials are needed to clarify the role of corticosteroids or their dose, it is doubtful that those studies will ever be performed.
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about treatment of plasma cell neoplasms (including multiple myeloma). It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewer for Plasma Cell Neoplasms (Including Multiple Myeloma) Treatment is:
Eric J. Seifter, MD (Johns Hopkins University)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Plasma Cell Neoplasms (Including Multiple Myeloma) Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/myeloma/hp/myeloma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389362]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Hairy cell leukemia is an indolent, low-grade, B-cell lymphoid malignancy. It is rare, with only 1,200 to 1,300 new cases annually in the United States.[1]
Clinical Presentation
Hairy cell leukemia usually presents with:
Splenomegaly.
Varying degrees of leukopenia (occasionally leukocytosis).
Pancytopenia.
Monocytopenia.
Bone marrow infiltration by atypical cells with prominent cytoplasmic projections (i.e., hairy cells).
Lymphadenopathy is absent, except with multiply recurrent progressive disease.
Diagnostic Evaluation
The following tests and procedures may be used to diagnose hairy cell leukemia:
Flow cytometry.
Bone marrow aspiration and biopsy.
Immunophenotyping.
Cytogenetic analysis.
BRAF gene testing.
Computed tomography scan.
The bone marrow is usually fibrotic and is not easily aspirated. It has circulating B cells with cytoplasmic projections (hairy appearance). Although a bone marrow biopsy may be required to enroll in a clinical trial, the hairy cell leukemia diagnosis can usually be made by flow cytometry.
In addition to the B-cell antigens CD19, CD20 (very high levels), and CD22, the cells coexpress CD11c, CD25, and CD103. The BRAF V600E pathogenic variant is a hairy cell leukemia–defining genetic feature that can aid in diagnosis.[2,3]
There is a variation of hairy cell leukemia (HCL-v) which accounts for 10% of cases. HCL-v is distinguished clinically by an elevated white blood cell count (15–50 × 109/L) and aberrant markers, including variable (instead of bright) CD103 and the absence of CD23, CD25, CD12, and CD43.[4,5] HCL-v cells also lack BRAF variants. Patients with HCL-v have more aggressive clinical courses, reduced responses to purine nucleoside analogue-based therapy, and shorter durations of response.[5]
The depth of a complete remission can be evaluated with measurable residual disease (MRD) by testing for a BRAF variant or an immunoglobulin heavy chain gene rearrangement. However, the usefulness of altering therapeutic choices with MRD remains unclear and requires further evaluation.[6]
References
Falini B, Tiacci E: Hairy-Cell Leukemia. N Engl J Med 391 (14): 1328-1341, 2024. [PUBMED Abstract]
Tiacci E, Schiavoni G, Forconi F, et al.: Simple genetic diagnosis of hairy cell leukemia by sensitive detection of the BRAF-V600E mutation. Blood 119 (1): 192-5, 2012. [PUBMED Abstract]
Naik RR, Saven A: My treatment approach to hairy cell leukemia. Mayo Clin Proc 87 (1): 67-76, 2012. [PUBMED Abstract]
Jones G, Parry-Jones N, Wilkins B, et al.: Revised guidelines for the diagnosis and management of hairy cell leukaemia and hairy cell leukaemia variant*. Br J Haematol 156 (2): 186-95, 2012. [PUBMED Abstract]
Troussard X, Grever MR: The revised guidelines for the diagnosis and management of hairy cell leukaemia and the hairy cell leukaemia variant. Br J Haematol 193 (1): 11-14, 2021. [PUBMED Abstract]
Ravandi F, Kreitman RJ, Tiacci E, et al.: Consensus opinion from an international group of experts on measurable residual disease in hairy cell leukemia. Blood Cancer J 12 (12): 165, 2022. [PUBMED Abstract]
Stage Information for Hairy Cell Leukemia
There is no generally accepted staging system used in the prognosis and treatment of hairy cell leukemia.
Treatment of Hairy Cell Leukemia
Hairy cell leukemia is highly treatable but rarely cured. Because it is easily controlled, many patients have prolonged survival with the use of sequential therapies. The decision to treat is based on signs of disease progression, including any of the following factors:
Cytopenias (especially if symptomatic).
Increasing splenomegaly.
The presence of other, usually infectious, complications.
If the patient is asymptomatic and if blood counts are maintained in an acceptable range, therapy may not be needed.[1]
Treatment Options for Hairy Cell Leukemia
Prior to the COVID-19 (SARS-CoV-2) pandemic, the standard initial therapy for patients with hairy cell leukemia was infusion of cladribine daily for 5 days, given with or without eight weekly doses of rituximab.[2–4] However, treatment with a purine analogue–based regimen led to significant and prolonged neutropenia and impairment of T-cell function, which were both problematic during the pandemic in fighting viral infection and establishing vaccination-induced immunity.
Other options for initial standard therapy, instead of cladribine or pentostatin, may offer less toxicity in terms of infection and long-term risk of secondary malignancies. However, these options may provide less durable response.
The Hairy Cell Leukemia Foundation convened a virtual meeting of 39 experts from around the world to amend the 2017 consensus recommendations.[5] The adapted treatment guidelines, published in 2021, are based primarily on anecdotal experience and expert opinion, as controlled trials for this indolent leukemia cannot be completed expeditiously given the low incidence of this disease.[6][Level of evidence C3] The adapted treatment guidelines are summarized below.
Consider watchful waiting when feasible; asymptomatic patients with noncritical levels of pancytopenia can be monitored closely.
Cladribine, with or without rituximab,[4] remains the standard of care. However, due to the risk of serious and prolonged immunosuppression, nonchemotherapy treatment options may be preferable for older, frail patients with higher risk of infection (or for those who have active infections).
BRAF inhibitors such as vemurafenib, dabrafenib, or encorafenib are nonchemotherapeutic options that can be combined with rituximab or obinutuzumab.[7–10] Most patients with hairy cell leukemia have BRAF pathogenic variants, but this should be verified by flow cytometry. Despite extensive experience with vemurafenib for patients with relapsed disease, the U.S. Food and Drug Administration (FDA) has not approved oral vemurafenib for patients with hairy cell leukemia.
Consider using rituximab alone intravenously (IV) for 4 to 8 weeks or in combination with a BRAF inhibitor.[11] Anti-CD20 monoclonal antibodies can impair future vaccine response, but they do not affect immunity from prior vaccination.
In patients with relapsed disease, the previously mentioned options are available, along with ibrutinib (the Bruton tyrosine kinase inhibitor).[12]
Treatment options for hairy cell leukemia include:
Cladribine may be given with or without rituximab to treat hairy cell leukemia.
Evidence (cladribine with or without rituximab):
In a phase II study, 68 patients with previously untreated hairy cell leukemia were randomly assigned to receive cladribine (0.15 mg/kg IV) on days 1 to 5, with eight weekly doses of rituximab either concurrently (starting on day 1) or delayed (starting after 6 months of cladribine treatment) if still positive with measurable residual disease (MRD) testing.[4][Level of evidence C3]
With a median follow-up of 96 months, 94% of patients who received concurrent therapy were MRD-free, compared with 12% of patients who received delayed therapy.
Although patients who underwent concurrent therapy had more need for platelet transfusions, they demonstrated higher neutrophil and platelet counts after 1 month.
A retrospective case series reported a median progression-free survival (PFS) of 67 months in patients with relapsed disease who received a purine nucleoside analogue (usually cladribine) plus rituximab.[13][Level of evidence C2]
A retrospective case series of nine patients with a histologic variation of hairy cell leukemia (HCL-v) reported an 88% complete response rate and 3-year PFS rate of 42% (95% confidence interval [CI], 1%–84%) after treatment with a purine nucleoside analogue (usually cladribine) plus rituximab.[14][Level of evidence C2]
Cladribine was given by daily subcutaneous injections or by daily 2-hour IV infusions for 5 to 7 days.[5,15–17][Level of evidence C3] Purine analogues should be avoided in cases of active infection or moderate to severe hepatic or renal impairment.
The complete response rate was 50% to 80%.
The overall response rate was 85% to 95%.
A National Cancer Institute group C protocol of 979 patients treated with cladribine reported lower response rates (i.e., 50% complete remission rate, 37% partial remission rate) compared with other studies.[18] Responses were durable in patients treated with a short course of cladribine, and patients who had a relapse often responded to re-treatment with cladribine.[2,13,19]
A retrospective review included 83 patients, aged 40 years and younger.[2]
The median time to first relapse was 54 months for all responders, and the median overall survival (OS) was 21 years from diagnosis.
Cladribine may cause fever and immunosuppression; documented infection was found in 33% of treated patients.
In a retrospective study of patients with cladribine-associated neutropenic fever, filgrastim (G-CSF) did not reduce the percentage of febrile patients, number of febrile days, or frequency of hospital admissions to receive antibiotics.[3]
BRAF inhibitors (vemurafenib or dabrafenib) with or without rituximab or trametinib
BRAF V600E pathogenic variants are found in almost 100% of patients with classic-form hairy cell leukemia and almost never found in patients with other B-cell lymphomas and leukemias, including HCL-v.[20][Level of evidence C3] Vemurafenib or other BRAF inhibitors such as dabrafenib can be given with rituximab or obinutuzumab.[10,21] The FDA has not approved BRAF inhibitors for hairy cell leukemia, but they can be used off-label in clinical practice.[22]
Evidence (vemurafenib with or without rituximab):
Several multicenter studies evaluated vemurafenib, given orally alone for 4 months or orally for 2 months with rituximab infused in eight doses over 18 weeks, in patients with relapsed or refractory hairy cell leukemia.[7,8,10,23][Level of evidence C3]
After a median follow-up of 23 to 40 months, for the 86 patients treated with vemurafenib alone, the following was reported in two studies:[7,8,23][Level of evidence C3]
The overall response rate was 86% to 98%.
The complete response rate was 33% to 38%.
The median treatment-free survival was 18 to 25 months.
Retreatment at relapse resulted in an 86% response rate, and the median relapse-free survival was 12.7 months in one of the trials, with a 40-month median follow-up.[23][Level of evidence C2]
After a median follow-up of 37 months, for the 30 patients treated with vemurafenib plus rituximab, the following was reported:[10][Level of evidence C3]
The complete response rate was 87%.
The PFS rate was 78% at 37 months.
In patients who had a complete response, 65% had no MRD.
Evidence (dabrafenib plus trametinib):
In a phase II trial of patients with relapsed or refractory disease, 55 patients received dabrafenib and trametinib orally until their disease progressed, they experienced unacceptable toxicity, or death occurred.[24]
With a median follow-up of 43.2 months, the overall response rate was 89.0% (95% CI, 77.8%–95.9%), the complete response rate was 65.5%, the 2-year PFS rate was 94.5%, and the 2-year OS rate was 95.5%.[24][Level of evidence C1]
Rituximab
Rituximab can induce durable remissions (with minimal toxic effects), but rarely complete remissions, in patients with multiple relapses or refractory disease after treatment with a purine analogue or interferon.[11,22,25][Level of evidence C3]
Pentostatin
Pentostatin given IV every other week for 3 to 6 months produced a 50% to 76% complete response rate and an 80% to 87% overall response rate.[26] Complete remissions were of substantial duration. Purine analogues should be avoided in cases of active infection or moderate to severe hepatic or renal impairment.
Evidence (pentostatin):
Two trials reported results on the 9-year median follow-up of patients treated with pentostatin.[27,28]
The relapse-free survival rates ranged from 56% to 67%.
Side effects included fever, immunosuppression, cytopenias, and renal dysfunction.
A randomized trial compared pentostatin to recombinant interferon alfa-2a.[26]
Pentostatin demonstrated higher response rates and more durable responses.
Ibrutinib
Ibrutinib, a tyrosine kinase inhibitor, has been studied in the treatment of hairy cell leukemia.
Evidence (ibrutinib):
In a phase II study, 37 patients with refractory hairy cell leukemia were treated with ibrutinib. The median follow-up was 42 months.[29][Level of evidence C3]
The response rate was 54%.
The estimated 36-month PFS rate was 73%.
The OS rate was 85%.
Re-treatment with cladribine or pentostatin
Patients with hairy cell leukemia who have a relapse after the first course of cladribine or pentostatin often respond well to re-treatment with the same or another purine analogue, especially if relapse occurs after several years.[13][Level of evidence C3]
Bendamustine with rituximab
Evidence (bendamustine with rituximab):
A phase II study evaluated 12 patients with relapsed or refractory disease, three of whom were negative for BRAF variants. Patients received the combination of bendamustine and rituximab.[30]
The overall response rate was 100%, and the complete remission rate was 50%.[30][Level of evidence C3]
Splenectomy
Splenectomy plays a decreasing role in treating hairy cell leukemia because effective alternatives are available. Splenectomy will partially or completely normalize the peripheral blood in most patients with hairy cell leukemia.[31] After a splenectomy, there is usually little or no change in the bone marrow, and virtually all patients have progressive disease within 12 to 18 months.
Interferon
Interferon alfa is no longer available because production has been halted.[32] According to the Hairy Cell Leukemia Foundation, ropeginterferon alfa-2b-njft is the best available preparation, but it is not FDA approved for hairy cell leukemia.
Interferon is useful when treating hairy cell leukemia during pregnancy because it does not involve cytotoxic agents.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Troussard X, Maître E, Cornet E: Hairy cell leukemia 2022: Update on diagnosis, risk-stratification, and treatment. Am J Hematol 97 (2): 226-236, 2022. [PUBMED Abstract]
Rosenberg JD, Burian C, Waalen J, et al.: Clinical characteristics and long-term outcome of young hairy cell leukemia patients treated with cladribine: a single-institution series. Blood 123 (2): 177-83, 2014. [PUBMED Abstract]
Saven A, Burian C, Adusumalli J, et al.: Filgrastim for cladribine-induced neutropenic fever in patients with hairy cell leukemia. Blood 93 (8): 2471-7, 1999. [PUBMED Abstract]
Chihara D, Arons E, Stetler-Stevenson M, et al.: Randomized Phase II Study of First-Line Cladribine With Concurrent or Delayed Rituximab in Patients With Hairy Cell Leukemia. J Clin Oncol 38 (14): 1527-1538, 2020. [PUBMED Abstract]
Grever MR, Abdel-Wahab O, Andritsos LA, et al.: Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood 129 (5): 553-560, 2017. [PUBMED Abstract]
Grever M, Andritsos L, Banerji V, et al.: Hairy cell leukemia and COVID-19 adaptation of treatment guidelines. Leukemia 35 (7): 1864-1872, 2021. [PUBMED Abstract]
Tiacci E, Park JH, De Carolis L, et al.: Targeting Mutant BRAF in Relapsed or Refractory Hairy-Cell Leukemia. N Engl J Med 373 (18): 1733-47, 2015. [PUBMED Abstract]
Dietrich S, Pircher A, Endris V, et al.: BRAF inhibition in hairy cell leukemia with low-dose vemurafenib. Blood 127 (23): 2847-55, 2016. [PUBMED Abstract]
Falini B, Tiacci E: New treatment options in hairy cell leukemia with focus on BRAF inhibitors. Hematol Oncol 37 (Suppl 1): 30-37, 2019. [PUBMED Abstract]
Tiacci E, De Carolis L, Simonetti E, et al.: Vemurafenib plus Rituximab in Refractory or Relapsed Hairy-Cell Leukemia. N Engl J Med 384 (19): 1810-1823, 2021. [PUBMED Abstract]
Angelopoulou MK, Pangalis GA, Sachanas S, et al.: Outcome and toxicity in relapsed hairy cell leukemia patients treated with rituximab. Leuk Lymphoma 49 (9): 1817-20, 2008. [PUBMED Abstract]
Jones J, Andritsos L, Kreitman RJ: Efficacy and safety of the Bruton tyrosine kinase inhibitor ibrutinib in patients with hairy cell leukemia: stage 1 results of a phase 2 study. [Abstract] Blood 128 (22): A-1215, 2016.
Hu R, Wei W, Mian A, et al.: Treatment outcomes with purine nucleoside analog alone or with rituximab for hairy cell leukemia at first relapse. Eur J Haematol 108 (5): 379-382, 2022. [PUBMED Abstract]
Wang Y, Wang T, Yu Y, et al.: Purine nucleoside analogs plus rituximab are an effective treatment choice for hairy cell leukemia-variant. Ann Hematol 101 (6): 1201-1210, 2022. [PUBMED Abstract]
Pagano L, Criscuolo M, Broccoli A, et al.: Long-term follow-up of cladribine treatment in hairy cell leukemia: 30-year experience in a multicentric Italian study. Blood Cancer J 12 (7): 109, 2022. [PUBMED Abstract]
Zenhäusern R, Schmitz SF, Solenthaler M, et al.: Randomized trial of daily versus weekly administration of 2-chlorodeoxyadenosine in patients with hairy cell leukemia: a multicenter phase III trial (SAKK 32/98). Leuk Lymphoma 50 (9): 1501-11, 2009. [PUBMED Abstract]
Hermel DJ, Cheng B, Bhangoo MS, et al.: Long-term outcomes of elderly hairy cell leukemia patients treated with cladribine. Ann Hematol 101 (5): 1089-1096, 2022. [PUBMED Abstract]
Cheson BD, Sorensen JM, Vena DA, et al.: Treatment of hairy cell leukemia with 2-chlorodeoxyadenosine via the Group C protocol mechanism of the National Cancer Institute: a report of 979 patients. J Clin Oncol 16 (9): 3007-15, 1998. [PUBMED Abstract]
Else M, Dearden CE, Catovsky D: Long-term follow-up after purine analogue therapy in hairy cell leukaemia. Best Pract Res Clin Haematol 28 (4): 217-29, 2015. [PUBMED Abstract]
Pettirossi V, Santi A, Imperi E, et al.: BRAF inhibitors reverse the unique molecular signature and phenotype of hairy cell leukemia and exert potent antileukemic activity. Blood 125 (8): 1207-16, 2015. [PUBMED Abstract]
Park JH, Devlin S, Durham BH, et al.: Vemurafenib and Obinutuzumab as Frontline Therapy for Hairy Cell Leukemia. NEJM Evid 2 (10): EVIDoa2300074, 2023. [PUBMED Abstract]
Falini B, De Carolis L, Tiacci E: How I treat refractory/relapsed hairy cell leukemia with BRAF inhibitors. Blood 139 (15): 2294-2305, 2022. [PUBMED Abstract]
Handa S, Lee JO, Derkach A, et al.: Long-term outcomes in patients with relapsed or refractory hairy cell leukemia treated with vemurafenib monotherapy. Blood 140 (25): 2663-2671, 2022. [PUBMED Abstract]
Kreitman RJ, Moreau P, Ravandi F, et al.: Dabrafenib plus trametinib in patients with relapsed/refractory BRAF V600E mutation-positive hairy cell leukemia. Blood 141 (9): 996-1006, 2023. [PUBMED Abstract]
Thomas DA, O’Brien S, Bueso-Ramos C, et al.: Rituximab in relapsed or refractory hairy cell leukemia. Blood 102 (12): 3906-11, 2003. [PUBMED Abstract]
Grever M, Kopecky K, Foucar MK, et al.: Randomized comparison of pentostatin versus interferon alfa-2a in previously untreated patients with hairy cell leukemia: an intergroup study. J Clin Oncol 13 (4): 974-82, 1995. [PUBMED Abstract]
Johnston JB, Eisenhauer E, Wainman N, et al.: Long-term outcome following treatment of hairy cell leukemia with pentostatin (Nipent): a National Cancer Institute of Canada study. Semin Oncol 27 (2 Suppl 5): 32-6, 2000. [PUBMED Abstract]
Flinn IW, Kopecky KJ, Foucar MK, et al.: Long-term follow-up of remission duration, mortality, and second malignancies in hairy cell leukemia patients treated with pentostatin. Blood 96 (9): 2981-6, 2000. [PUBMED Abstract]
Rogers KA, Andritsos LA, Wei L, et al.: Phase 2 study of ibrutinib in classic and variant hairy cell leukemia. Blood 137 (25): 3473-3483, 2021. [PUBMED Abstract]
Burotto M, Stetler-Stevenson M, Arons E, et al.: Bendamustine and rituximab in relapsed and refractory hairy cell leukemia. Clin Cancer Res 19 (22): 6313-21, 2013. [PUBMED Abstract]
Golomb HM, Vardiman JW: Response to splenectomy in 65 patients with hairy cell leukemia: an evaluation of spleen weight and bone marrow involvement. Blood 61 (2): 349-52, 1983. [PUBMED Abstract]
Assanto GM, Riemma C, Malaspina F, et al.: The current role of interferon in hairy cell leukaemia: clinical and molecular aspects. Br J Haematol 194 (1): 78-82, 2021. [PUBMED Abstract]
Latest Updates to This Summary (02/21/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Revised text to state that cladribine, with or without rituximab, remains the standard of care. However, due to the risk of serious and prolonged immunosuppression, nonchemotherapy treatment options may be preferable for older, frail patients with higher risks of infection (or for those who have active infections). BRAF inhibitors such as vemurafenib, dabrafenib, or encorafenib are nonchemotherapeutic options that can be combined with rituximab or obinutuzumab.
Revised the list of treatment options for hairy cell leukemia to include interferon.
Revised text to state that vemurafenib or other BRAF inhibitors such as dabrafenib can be given with rituximab or obinutuzumab (cited Park et al. as reference 21).
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of hairy cell leukemia. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewer for Hairy Cell Leukemia Treatment is:
Eric J. Seifter, MD (Johns Hopkins University)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Hairy Cell Leukemia Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/leukemia/hp/hairy-cell-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389184]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Estimated new cases and deaths from chronic lymphocytic leukemia (CLL) in the United States in 2025:[1]
New cases: 23,690.
Deaths: 4,460.
Anatomy
CLL is a disorder of morphologically mature, but immunologically less mature lymphocytes. It is manifested by progressive accumulation of these cells in the blood, bone marrow, and lymphatic tissues.[2]
EnlargeBlood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
Clinical Presentation
The clinical course of this disease progresses from an indolent lymphocytosis without other evident disease to one of generalized lymphatic enlargement with concomitant pancytopenia. Complications of pancytopenia, including hemorrhage and infection, represent a major cause of death in these patients.[3] Immunological aberrations, including Coombs-positive hemolytic anemia, immune thrombocytopenia, and depressed immunoglobulin levels, may all complicate the management of CLL.[4]
Diagnostic Evaluation and Differential Diagnosis
Tests and procedures used to diagnose CLL include the following:[5]
History and physical examination (including bidimensional diameters of the largest palpable lymph nodes in the cervical, axillary, and inguinal nodal sites and dimensions of the liver and spleen below their respective costal margins as assessed by palpation).
Complete blood count with differential and chemistry panel (including creatinine, bilirubin, transaminases, and alkaline phosphatase). Other blood tests may include lactate dehydrogenase and beta-2-microglobulin. With suspicion of autoimmune hemolytic anemia, testing for reticulocyte count, indirect bilirubin, serum haptoglobin, antiglobulin (direct Coombs), and cold agglutinin may be helpful.
Flow cytometry (for immunophenotyping).
Fluorescence in situ hybridization (FISH) (for del(11q), del(13q), del(17p), trisomy 12, and t(11;14)).
TP53 variant analysis.
IGH variant analysis.
Serum immunoglobulin levels.
Hepatitis B and C and HIV tests.
Computed tomography (CT) is usually not required in the absence of peripheral adenopathy; extensive adenopathy on examination should prompt investigation of retroperitoneal adenopathy.
Bone marrow aspiration and biopsy is usually not required.
In this disorder, lymphocyte counts in the blood are usually greater than or equal to 5,000/mm3 with a characteristic immunophenotype (CD5- and CD23-positive B cells).[6,7] As assays have become more sensitive for detecting monoclonal B-CLL–like cells in peripheral blood, researchers have detected a monoclonal B-cell lymphocytosis in 3% of adults older than 40 years and in 6% of adults older than 60 years.[8] Such early detection and diagnosis may falsely suggest improved survival for the group and may unnecessarily worry or result in therapy for some patients who would have remained undiagnosed in their lifetime, a circumstance known as overdiagnosis or pseudodisease.[9,10]
Confusion with other diseases may be avoided by determination of cell surface markers. CLL lymphocytes coexpress the B-cell antigens CD19 and CD20 along with the T-cell antigen CD5.[11] This coexpression occurs in only one other disease entity, mantle cell lymphoma. CLL B cells express relatively low levels of surface-membrane immunoglobulin (compared with normal peripheral blood B cells) and a single light chain (kappa or lambda).[12] CLL is diagnosed by an absolute increase in lymphocytosis and/or bone marrow infiltration coupled with the characteristic features of morphology and immunophenotype, which confirm the characteristic clonal population. In a database analysis, for up to 77 months before diagnosis, almost all patients with a CLL diagnosis had prediagnostic B-cell clones that were identified in peripheral blood (when available).[7,13]
About 1% of morphological CLL cases express T-cell markers (CD4 and CD7) and have clonal rearrangements of their T-cell receptor genes. These patients have a higher frequency of skin lesions, more variable lymphocyte shape, and shorter median survival (13 months) with minimal responses to chemotherapy and B-cell receptor inhibitors.[14]
The differential diagnosis must exclude the following:
Monoclonal B-cell lymphocytosis (MBL). MBL, the precursor to CLL, is defined as a clonal B-cell population circulating in peripheral blood with fewer than 5 × 109/L B cells and no signs of lymphadenopathy or splenomegaly.[15] Most cases have the immunophenotype of CLL. The incidence of MBL in the general population is 5% to 12% and increases with age.[16] In families with two or more cases of CLL, MBL has a prevalence of 13% to 18%. Low-count MBL (≤0.5 × 109/L B cells) rarely progresses to overt CLL, but higher levels can progress to symptomatic CLL at a rate of less than 2% per year, even for familial cases.[15,17] In two selected series of more than 900 patients monitored prospectively for a median of 5 to 7 years, overt CLL requiring chemotherapy occurred in 7% of patients.[8,18] A screening study using the Mayo Clinic Biobank identified 1,712 patients with MBL from 10,139 screened samples.[19] Low-count MBL was found in 95% of these patients. With a median follow-up of 10.0 years, only 0.58% of patients progressed to a lymphoid malignancy.[19]
Waldenström macroglobulinemia. Waldenström macroglobulinemia has a natural history and therapeutic options similar to CLL, with the exception of hyperviscosity syndrome associated with macroglobulinemia as a result of elevated immunoglobulin M. For more information, see Indolent B-Cell Non-Hodgkin Lymphoma Treatment.
Large granular lymphocyte (LGL) leukemia. LGL leukemia is characterized by lymphocytosis with a natural killer (NK) cell immunophenotype (CD2, CD16, and CD56) or a T-cell immunophenotype (CD2, CD3, and CD8).[20–22] These patients often have neutropenia and a history of rheumatoid arthritis. The natural history is indolent, often marked by anemia and splenomegaly. This condition appears to fit into the clinical spectrum of Felty syndrome.[23] A characteristic genetic finding in almost 50% of the patients with T-cell LGL involves pathogenic variants in the STAT3 gene.[24] Symptomatic patients with cytopenias typically manifest CD8-positive T cells with alpha/beta surface receptors plus a STAT3 variant, CD8-positive T cells with T gamma/delta surface receptors, or a mutated NK/T-cell phenotype.[25,26] Conversely, asymptomatic patients have wild-type STAT3 CD8-positive T cells, CD4-positive T cells, and wild-type NK cells.[25] Therapy includes low doses of oral cyclophosphamide or methotrexate, cyclosporine, and treatment of the bacterial infections acquired during severe neutropenia.[20,22,27,28]
For information on prolymphocytic leukemia, which was previously covered in this summary, see the Treatment of T-Cell Prolymphocytic Leukemia section in Peripheral T-Cell Non-Hodgkin Lymphoma Treatment.
Prognostic Factors
Prognostic markers help stratify patients in clinical trials, assess the need for therapy, and select the type of therapy.[2,29,30] Prognostic factors that may help predict clinical outcome include cytogenetic subgroup, immunoglobulin mutational status, and CD38 immunophenotype.[2,31–39]
Prognostic markers include the following:
IGH pathogenic variant.[32–34,39,40] The finding of significant numbers of variants in this region is associated with a median survival in excess of 20 to 25 years. The absence of variants is associated with a median survival of 8 to 10 years.
FISH test results. FISH chromosomal abnormalities were associated with prognosis in retrospective and prospective studies, and clonal evolution has been seen over time.[31,41–43] The following chromosomal abnormalities have been reported:
del(13q) is a favorable prognostic marker (median overall survival [OS], 17 years in one prospective study).[43]
Trisomy 12 and del(11) have a less favorable prognosis (median OS, 9–11 years in one prospective study).[43]
del(17p) is associated with TP53 pathogenic variants, poor response rates, and short duration of response to the standard therapeutic options.[39] del(17p) is associated with the most unfavorable prognosis (median OS, 7 years in one prospective trial).[43–45]
The combination of abnormal cytogenetics, such as del(11q) or del(17p) deletion (suggesting a worse prognosis), with zeta-chain-associated protein 70 kDa negativity (suggesting a better prognosis) in the same patients resulted in a poor prognosis.[38]
These findings emphasize the need for prospective studies of combinations of these prognostic markers.[46]
Other prognostic factors include the following:
Anemia and thrombocytopenia. These are important adverse prognostic variables, but only if due to extensive marrow involvement by CLL. Autoimmune hemolytic anemia and immune thrombocytopenic purpura do not confer a worse prognosis.
Age. CLL occurs primarily in middle-aged and older adults, with worse prognosis in successive decades of life.[42]
Positron emission tomography (PET)-CT scan results. This test should only be used in the context of recurrent fever, soaking night sweats, weight loss (>10% baseline weight in 6 months), or rapidly growing lymph nodes, because these findings might herald histological transformation to a diffuse large B-cell lymphoma (DLBCL) (so-called Richter transformation). Of 432 patients retrospectively reviewed, 209 patients had a maximum standardized uptake value (SUVmax) of 5 or higher.[49] Eighty percent of these patients had histologically aggressive CLL or Richter syndrome, and both of these entities had equally worse prognoses. When the SUVmax was 10 or higher, the 5-year OS rate was only 30%.[49]
Lymphocyte doubling time. Doubling of the white blood cell count in less than 1 year implies a worse prognosis.[50]
Beta-2-microglobulin. Higher levels imply a worse prognosis.[51]
Richter transformation. In 2% to 10% of patients, CLL will transform into a more aggressive lymphoma, termed Richter transformation.[52] This is usually a DLBCL of the more aggressive activated B-cell subtype. The prognosis is similar to de novo presentations of DLBCL when the CLL has never required therapy or when there is no clonal connection between the CLL and DLBCL (identified if they harbor different clonal light chains or if sequencing can be accomplished at the VDJ [variable, diversity, joining] recombination sites in the immunoglobulin heavy chain variable region).[52] However, the prognosis is poor (median survival, 6–14 months) for most patients with Richter transformation to DLBCL when there has been prior therapy for CLL with chemoimmunotherapy,[53], Bruton tyrosine kinase (BTK) inhibitors, and/or venetoclax.[54] There is no standard therapeutic approach for patients with poor prognoses. Therapies under clinical evaluation include chimeric antigen receptor (CAR) T-cell therapy, T-cell engaging bispecific antibodies, and non-covalent BTK inhibitors.[52,55] Allogeneic stem cell transplant consolidation is often recommended if induction therapy achieves a response.[52] In rare cases of Richter transformation from CLL to Hodgkin lymphoma, the prognosis appears the same for age-matched patients with de novo disease.[56,57]
Clearance of measurable residual disease (MRD). The improvements in response rates from more intensive regimens have maximized the clearance of MRD. In one prospective trial of 493 patients, clearance of MRD was an independent predictor of OS by multivariate analysis.[58] The surrogate end point of clearance of residual disease, while prognostic,[58,59] did not show improved survival in a randomized prospective trial. The necessary study would include patients who fail to completely clear the marrow with induction therapy and randomly assign them to further alternative treatment versus the same treatment later at relapse, looking at OS as the primary end point.[29,60]
CD38 immunophenotype.[33,61] CD38 positivity (>30%) correlates with a worse prognosis, but there is a 30% false-positive rate and a 50% false-negative rate using IGH mutational status as the gold standard for prognosis.
Other malignancies. Patients with CLL are also at increased risk of developing other malignancies, even before therapy.[62] A population-based analysis of almost 2 million cancer patients in the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program database was performed. The findings suggested that cancer-specific survival for patients with preexisting CLL who subsequently developed colorectal and breast cancer was significantly lower (hazard ratio [HR], 1.46; P < .001 for colorectal cancer and HR, 1.41; P = .005 for breast cancer) than cancer-specific survival for patients with colorectal and breast cancer who did not have antecedent CLL, after adjusting for age, sex, race, and disease stage, and excluding CLL-related deaths.[63]
An international prognostic index for CLL (CLL-IPI) identified four prognostic subgroups based on IGH mutational status, clinical stage, age (≤65 years vs. >65 years), and TP53 status (no abnormalities vs. del(17p), TP53 variant, or both).[64] A scoring system to predict time to first treatment for early-stage CLL identified three adverse risk factors: unmutated IGH, absolute lymphocyte count higher than 15 × 109/L, and palpable lymph nodes.[65] Any new prognostic model, and even the commonly used CLL-IPI, may be outdated because of the use of highly effective frontline therapies, including BCL2 inhibitors and BTK inhibitors.[66] Revalidation of these prognostic models will be required.
Follow-Up After Treatment
CT scans have a very limited role in monitoring patients after completion of treatment. CT scan or ultrasonography results determined the decision to treat for relapse in only 2 of 176 patients in three prospective trials for the German CLL Study Group.[67]
References
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Burger JA: Treatment of Chronic Lymphocytic Leukemia. N Engl J Med 383 (5): 460-473, 2020. [PUBMED Abstract]
Anaissie EJ, Kontoyiannis DP, O’Brien S, et al.: Infections in patients with chronic lymphocytic leukemia treated with fludarabine. Ann Intern Med 129 (7): 559-66, 1998. [PUBMED Abstract]
Mauro FR, Foa R, Cerretti R, et al.: Autoimmune hemolytic anemia in chronic lymphocytic leukemia: clinical, therapeutic, and prognostic features. Blood 95 (9): 2786-92, 2000. [PUBMED Abstract]
Hallek M, Cheson BD, Catovsky D, et al.: iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 131 (25): 2745-2760, 2018. [PUBMED Abstract]
Hallek M, Cheson BD, Catovsky D, et al.: Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood 111 (12): 5446-56, 2008. [PUBMED Abstract]
Shanafelt TD, Kay NE, Jenkins G, et al.: B-cell count and survival: differentiating chronic lymphocytic leukemia from monoclonal B-cell lymphocytosis based on clinical outcome. Blood 113 (18): 4188-96, 2009. [PUBMED Abstract]
Rawstron AC, Bennett FL, O’Connor SJ, et al.: Monoclonal B-cell lymphocytosis and chronic lymphocytic leukemia. N Engl J Med 359 (6): 575-83, 2008. [PUBMED Abstract]
Dighiero G: Monoclonal B-cell lymphocytosis–a frequent premalignant condition. N Engl J Med 359 (6): 638-40, 2008. [PUBMED Abstract]
Fazi C, Scarfò L, Pecciarini L, et al.: General population low-count CLL-like MBL persists over time without clinical progression, although carrying the same cytogenetic abnormalities of CLL. Blood 118 (25): 6618-25, 2011. [PUBMED Abstract]
DiGiuseppe JA, Borowitz MJ: Clinical utility of flow cytometry in the chronic lymphoid leukemias. Semin Oncol 25 (1): 6-10, 1998. [PUBMED Abstract]
Rozman C, Montserrat E: Chronic lymphocytic leukemia. N Engl J Med 333 (16): 1052-7, 1995. [PUBMED Abstract]
Landgren O, Albitar M, Ma W, et al.: B-cell clones as early markers for chronic lymphocytic leukemia. N Engl J Med 360 (7): 659-67, 2009. [PUBMED Abstract]
Hoyer JD, Ross CW, Li CY, et al.: True T-cell chronic lymphocytic leukemia: a morphologic and immunophenotypic study of 25 cases. Blood 86 (3): 1163-9, 1995. [PUBMED Abstract]
Shim YK, Rachel JM, Ghia P, et al.: Monoclonal B-cell lymphocytosis in healthy blood donors: an unexpectedly common finding. Blood 123 (9): 1319-26, 2014. [PUBMED Abstract]
Slager SL, Lanasa MC, Marti GE, et al.: Natural history of monoclonal B-cell lymphocytosis among relatives in CLL families. Blood 137 (15): 2046-2056, 2021. [PUBMED Abstract]
Shanafelt TD, Kay NE, Rabe KG, et al.: Brief report: natural history of individuals with clinically recognized monoclonal B-cell lymphocytosis compared with patients with Rai 0 chronic lymphocytic leukemia. J Clin Oncol 27 (24): 3959-63, 2009. [PUBMED Abstract]
Slager SL, Parikh SA, Achenbach SJ, et al.: Progression and survival of MBL: a screening study of 10 139 individuals. Blood 140 (15): 1702-1709, 2022. [PUBMED Abstract]
Semenzato G, Zambello R, Starkebaum G, et al.: The lymphoproliferative disease of granular lymphocytes: updated criteria for diagnosis. Blood 89 (1): 256-60, 1997. [PUBMED Abstract]
Lamy T, Loughran TP: How I treat LGL leukemia. Blood 117 (10): 2764-74, 2011. [PUBMED Abstract]
Bowman SJ, Sivakumaran M, Snowden N, et al.: The large granular lymphocyte syndrome with rheumatoid arthritis. Immunogenetic evidence for a broader definition of Felty’s syndrome. Arthritis Rheum 37 (9): 1326-30, 1994. [PUBMED Abstract]
Koskela HL, Eldfors S, Ellonen P, et al.: Somatic STAT3 mutations in large granular lymphocytic leukemia. N Engl J Med 366 (20): 1905-13, 2012. [PUBMED Abstract]
Cheon H, Xing JC, Moosic KB, et al.: Genomic landscape of TCRαβ and TCRγδ T-large granular lymphocyte leukemia. Blood 139 (20): 3058-3072, 2022. [PUBMED Abstract]
Barilà G, Grassi A, Cheon H, et al.: Tγδ LGLL identifies a subset with more symptomatic disease: analysis of an international cohort of 137 patients. Blood 141 (9): 1036-1046, 2023. [PUBMED Abstract]
Loughran TP, Kidd PG, Starkebaum G: Treatment of large granular lymphocyte leukemia with oral low-dose methotrexate. Blood 84 (7): 2164-70, 1994. [PUBMED Abstract]
Dhodapkar MV, Li CY, Lust JA, et al.: Clinical spectrum of clonal proliferations of T-large granular lymphocytes: a T-cell clonopathy of undetermined significance? Blood 84 (5): 1620-7, 1994. [PUBMED Abstract]
Developments in the treatment of lymphoproliferative disorders: rising to the new challenges of CLL therapy. A report of a symposium presented during the 48th American Society of Hematology Annual Meeting and Exposition, December 8, 2006, Orlando, Florida. Clin Adv Hematol Oncol 5 (3 Suppl 5): 1-14; quiz 15-6, 2007. [PUBMED Abstract]
Pflug N, Bahlo J, Shanafelt TD, et al.: Development of a comprehensive prognostic index for patients with chronic lymphocytic leukemia. Blood 124 (1): 49-62, 2014. [PUBMED Abstract]
Döhner H, Stilgenbauer S, Benner A, et al.: Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med 343 (26): 1910-6, 2000. [PUBMED Abstract]
Hamblin TJ, Davis Z, Gardiner A, et al.: Unmutated Ig V(H) genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood 94 (6): 1848-54, 1999. [PUBMED Abstract]
Damle RN, Wasil T, Fais F, et al.: Ig V gene mutation status and CD38 expression as novel prognostic indicators in chronic lymphocytic leukemia. Blood 94 (6): 1840-7, 1999. [PUBMED Abstract]
Rosenwald A, Alizadeh AA, Widhopf G, et al.: Relation of gene expression phenotype to immunoglobulin mutation genotype in B cell chronic lymphocytic leukemia. J Exp Med 194 (11): 1639-47, 2001. [PUBMED Abstract]
Klein U, Tu Y, Stolovitzky GA, et al.: Gene expression profiling of B cell chronic lymphocytic leukemia reveals a homogeneous phenotype related to memory B cells. J Exp Med 194 (11): 1625-38, 2001. [PUBMED Abstract]
Orchard JA, Ibbotson RE, Davis Z, et al.: ZAP-70 expression and prognosis in chronic lymphocytic leukaemia. Lancet 363 (9403): 105-11, 2004. [PUBMED Abstract]
Rassenti LZ, Huynh L, Toy TL, et al.: ZAP-70 compared with immunoglobulin heavy-chain gene mutation status as a predictor of disease progression in chronic lymphocytic leukemia. N Engl J Med 351 (9): 893-901, 2004. [PUBMED Abstract]
Kröber A, Bloehdorn J, Hafner S, et al.: Additional genetic high-risk features such as 11q deletion, 17p deletion, and V3-21 usage characterize discordance of ZAP-70 and VH mutation status in chronic lymphocytic leukemia. J Clin Oncol 24 (6): 969-75, 2006. [PUBMED Abstract]
Byrd JC, Gribben JG, Peterson BL, et al.: Select high-risk genetic features predict earlier progression following chemoimmunotherapy with fludarabine and rituximab in chronic lymphocytic leukemia: justification for risk-adapted therapy. J Clin Oncol 24 (3): 437-43, 2006. [PUBMED Abstract]
Kharfan-Dabaja MA, Chavez JC, Khorfan KA, et al.: Clinical and therapeutic implications of the mutational status of IgVH in patients with chronic lymphocytic leukemia. Cancer 113 (5): 897-906, 2008. [PUBMED Abstract]
Kröber A, Seiler T, Benner A, et al.: V(H) mutation status, CD38 expression level, genomic aberrations, and survival in chronic lymphocytic leukemia. Blood 100 (4): 1410-6, 2002. [PUBMED Abstract]
Catovsky D, Fooks J, Richards S: Prognostic factors in chronic lymphocytic leukaemia: the importance of age, sex and response to treatment in survival. A report from the MRC CLL 1 trial. MRC Working Party on Leukaemia in Adults. Br J Haematol 72 (2): 141-9, 1989. [PUBMED Abstract]
Shanafelt TD, Witzig TE, Fink SR, et al.: Prospective evaluation of clonal evolution during long-term follow-up of patients with untreated early-stage chronic lymphocytic leukemia. J Clin Oncol 24 (28): 4634-41, 2006. [PUBMED Abstract]
Grever MR, Lucas DM, Dewald GW, et al.: Comprehensive assessment of genetic and molecular features predicting outcome in patients with chronic lymphocytic leukemia: results from the US Intergroup Phase III Trial E2997. J Clin Oncol 25 (7): 799-804, 2007. [PUBMED Abstract]
Catovsky D, Richards S, Matutes E, et al.: Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet 370 (9583): 230-9, 2007. [PUBMED Abstract]
Binet JL, Caligaris-Cappio F, Catovsky D, et al.: Perspectives on the use of new diagnostic tools in the treatment of chronic lymphocytic leukemia. Blood 107 (3): 859-61, 2006. [PUBMED Abstract]
Rai KR, Sawitsky A, Cronkite EP, et al.: Clinical staging of chronic lymphocytic leukemia. Blood 46 (2): 219-34, 1975. [PUBMED Abstract]
Binet JL, Auquier A, Dighiero G, et al.: A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer 48 (1): 198-206, 1981. [PUBMED Abstract]
Falchi L, Keating MJ, Marom EM, et al.: Correlation between FDG/PET, histology, characteristics, and survival in 332 patients with chronic lymphoid leukemia. Blood 123 (18): 2783-90, 2014. [PUBMED Abstract]
Montserrat E, Sanchez-Bisono J, Viñolas N, et al.: Lymphocyte doubling time in chronic lymphocytic leukaemia: analysis of its prognostic significance. Br J Haematol 62 (3): 567-75, 1986. [PUBMED Abstract]
Di Giovanni S, Valentini G, Carducci P, et al.: Beta-2-microglobulin is a reliable tumor marker in chronic lymphocytic leukemia. Acta Haematol 81 (4): 181-5, 1989. [PUBMED Abstract]
Parikh SA, Kay NE, Shanafelt TD: How we treat Richter syndrome. Blood 123 (11): 1647-57, 2014. [PUBMED Abstract]
Rossi D, Spina V, Deambrogi C, et al.: The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation. Blood 117 (12): 3391-401, 2011. [PUBMED Abstract]
Kittai AS, Huang Y, Miller S, et al.: Outcomes of patients with Richter transformation without prior chemoimmunotherapy for CLL/SLL: an international multicenter retrospective study. [Abstract] Blood 142 (Suppl 1): A-497, 2023.
Kittai AS, Bond D, Huang Y, et al.: Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy for Richter Transformation: An International, Multicenter, Retrospective Study. J Clin Oncol 42 (17): 2071-2079, 2024. [PUBMED Abstract]
Al-Sawaf O, Robrecht S, Bahlo J, et al.: Richter transformation in chronic lymphocytic leukemia (CLL)-a pooled analysis of German CLL Study Group (GCLLSG) front line treatment trials. Leukemia 35 (1): 169-176, 2021. [PUBMED Abstract]
Stephens DM, Boucher K, Kander E, et al.: Hodgkin lymphoma arising in patients with chronic lymphocytic leukemia: outcomes from a large multi-center collaboration. Haematologica 106 (11): 2845-2852, 2021. [PUBMED Abstract]
Böttcher S, Ritgen M, Fischer K, et al.: Minimal residual disease quantification is an independent predictor of progression-free and overall survival in chronic lymphocytic leukemia: a multivariate analysis from the randomized GCLLSG CLL8 trial. J Clin Oncol 30 (9): 980-8, 2012. [PUBMED Abstract]
Strati P, Keating MJ, O’Brien SM, et al.: Eradication of bone marrow minimal residual disease may prompt early treatment discontinuation in CLL. Blood 123 (24): 3727-32, 2014. [PUBMED Abstract]
Montserrat E, Moreno C, Esteve J, et al.: How I treat refractory CLL. Blood 107 (4): 1276-83, 2006. [PUBMED Abstract]
Ghia P, Guida G, Stella S, et al.: The pattern of CD38 expression defines a distinct subset of chronic lymphocytic leukemia (CLL) patients at risk of disease progression. Blood 101 (4): 1262-9, 2003. [PUBMED Abstract]
Tsimberidou AM, Wen S, McLaughlin P, et al.: Other malignancies in chronic lymphocytic leukemia/small lymphocytic lymphoma. J Clin Oncol 27 (6): 904-10, 2009. [PUBMED Abstract]
Solomon BM, Rabe KG, Slager SL, et al.: Overall and cancer-specific survival of patients with breast, colon, kidney, and lung cancers with and without chronic lymphocytic leukemia: a SEER population-based study. J Clin Oncol 31 (7): 930-7, 2013. [PUBMED Abstract]
International CLL-IPI working group: An international prognostic index for patients with chronic lymphocytic leukaemia (CLL-IPI): a meta-analysis of individual patient data. Lancet Oncol 17 (6): 779-90, 2016. [PUBMED Abstract]
Condoluci A, Terzi di Bergamo L, Langerbeins P, et al.: International prognostic score for asymptomatic early-stage chronic lymphocytic leukemia. Blood 135 (21): 1859-1869, 2020. [PUBMED Abstract]
Kreuzberger N, Damen JA, Trivella M, et al.: Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: a systematic review and meta-analysis. Cochrane Database Syst Rev 7: CD012022, 2020. [PUBMED Abstract]
Eichhorst BF, Fischer K, Fink AM, et al.: Limited clinical relevance of imaging techniques in the follow-up of patients with advanced chronic lymphocytic leukemia: results of a meta-analysis. Blood 117 (6): 1817-21, 2011. [PUBMED Abstract]
Stage Information for Chronic Lymphocytic Leukemia
Chronic lymphocytic leukemia (CLL) does not have a standard staging system. The Rai staging system (Table 1) and the Binet classification (Table 2) are presented below.[1,2] A National Cancer Institute (NCI)-sponsored working group has formulated standardized guidelines for criteria related to eligibility, response, and toxic effects to be used in future clinical trials in CLL.[3]
Rai Staging System
Table 1. Rai Staging System
Stage
Stage Criteria
Stage 0
Absolute lymphocytosis (>15,000/mm3) without adenopathy, hepatosplenomegaly, anemia, or thrombocytopenia.
Stage I
Absolute lymphocytosis with lymphadenopathy without hepatosplenomegaly, anemia, or thrombocytopenia.
Stage II
Absolute lymphocytosis with either hepatomegaly or splenomegaly with or without lymphadenopathy.
Stage III
Absolute lymphocytosis and anemia (hemoglobin <11 g/dL) with or without lymphadenopathy, hepatomegaly, or splenomegaly.
Stage IV
Absolute lymphocytosis and thrombocytopenia (<100,000/mm3) with or without lymphadenopathy, hepatomegaly, splenomegaly, or anemia.
Binet Classification
Table 2. Binet Classification System
Stage
Stage Criteria
aLymphoid areas include cervical, axillary, inguinal, and splenic.
Clinical stage Aa
No anemia or thrombocytopenia and fewer than three areas of lymphoid involvement (Rai stages 0, I, and II).
Clinical stage Ba
No anemia or thrombocytopenia with three or more areas of lymphoid involvement (Rai stages I and II).
Clinical stage C
Anemia and/or thrombocytopenia regardless of the number of areas of lymphoid enlargement (Rai stages III and IV).
The Binet classification integrates the number of disease-involved nodal groups with bone marrow failure. Its major benefit derives from the recognition of a predominantly splenic form of the disease, which may have a better prognosis than was recognized in the Rai staging, and from the recognition that the presence of anemia or thrombocytopenia has a similar prognosis and does not merit a separate stage. Neither system separates immune from nonimmune causes of cytopenia. Patients with thrombocytopenia, anemia, or both, which is caused by extensive marrow infiltration and impaired production (Rai III/IV, Binet C), have a poorer prognosis than patients with immune cytopenias.[4]
The International Workshop on CLL has recommended integrating the Rai and Binet systems as follows: A(0), A(I), A(II); B(I), B(II); and C(III), C(IV).[5] The NCI-sponsored working group has published guidelines for the diagnosis and treatment of CLL in both clinical trial and general practice settings.[3] Use of these systems allows comparison of clinical results and establishment of therapeutic guidelines.
References
Rai KR, Sawitsky A, Cronkite EP, et al.: Clinical staging of chronic lymphocytic leukemia. Blood 46 (2): 219-34, 1975. [PUBMED Abstract]
Binet JL, Auquier A, Dighiero G, et al.: A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer 48 (1): 198-206, 1981. [PUBMED Abstract]
Hallek M, Cheson BD, Catovsky D, et al.: Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood 111 (12): 5446-56, 2008. [PUBMED Abstract]
Moreno C, Hodgson K, Ferrer G, et al.: Autoimmune cytopenia in chronic lymphocytic leukemia: prevalence, clinical associations, and prognostic significance. Blood 116 (23): 4771-6, 2010. [PUBMED Abstract]
Chronic lymphocytic leukemia: recommendations for diagnosis, staging, and response criteria. International Workshop on Chronic Lymphocytic Leukemia. Ann Intern Med 110 (3): 236-8, 1989. [PUBMED Abstract]
Selection of Therapy for Chronic Lymphocytic Leukemia
Treatment of patients with chronic lymphocytic leukemia (CLL) must be individualized based on the clinical behavior of the disease.[1] Because this disease is generally not curable, occurs in an older population, and often progresses slowly, it is most often treated in a conservative fashion.[2]
In older trials with data collected from the 1970s through the 1990s, the median survival for all patients ranged from 8 to 12 years.[3,4] However, with the introduction of the B-cell receptor inhibitors and targeting of BCL2, the median survival for all patients has not been reached with over 10 years of follow-up.
Treatment of patients with CLL ranges from observation with treatment of infectious, hemorrhagic, or immunological complications to a variety of therapeutic options administered as single agents or combination therapy. In asymptomatic patients, treatment may be deferred until the disease progresses and symptoms occur.[3] Because the rate of progression may vary from patient to patient, with long periods of stability and sometimes spontaneous regressions, frequent and careful observation is required to monitor the clinical course.[5] Although even asymptomatic patients with del(17p) on fluorescence in situ hybridization (FISH) analysis (or those with a TP53 pathogenic variant) may be followed with watchful waiting, frequent monitoring may be required to avert rapid progression. A meta-analysis of randomized trials showed no survival benefit for immediate versus delayed therapy for patients with early-stage disease.[6][Level of evidence A1] For patients with progressing CLL, treatment will not be curative in most cases. Selected patients treated with allogeneic stem cell transplant have achieved prolonged disease-free survival (DFS), sometimes exceeding 20 years.[7–11] Prolonged DFS was also noted in young patients (<60 years) with IGH hypermutation who received the FCR regimen (fludarabine, cyclophosphamide, and rituximab).[12–14]
The following clinical factors may be helpful in predicting progression of disease:[2]
IGH pathogenic variant.
Chromosomal abnormalities found by FISH or cytogenetic analysis.
Beta-2-microglobulin.
Lymphocyte doubling time.
The International Workshop on Chronic Lymphocytic Leukemia defines symptomatic or progressive CLL as having the following signs and symptoms:[15]
Evidence of progressive marrow failure—the development or worsening of anemia and/or thrombocytopenia (in some patients, platelet counts <100 × 109/L may remain stable over a long period; this does not automatically require therapeutic intervention). Cutoff levels of hemoglobin less than 10 g/dL or platelet counts less than 50 × 109/L are generally regarded as an indication for treatment.
Massive (i.e., ≥6 cm below the left costal margin), progressive, or symptomatic splenomegaly.
Massive lymph nodes (i.e., ≥10 cm in longest diameter), progressive, or symptomatic lymphadenopathy.
Progressive lymphocytosis with an increase of 50% or more over a 2-month period, or lymphocyte-doubling time (LDT) less than 6 months. LDT can be obtained by linear regression extrapolation of absolute lymphocyte counts obtained at intervals of 2 weeks over an observation period of 2 to 3 months; patients with initial blood lymphocyte counts less than 30 × 109/L may require a longer observation period to determine the LDT. Factors contributing to lymphocytosis other than CLL (e.g., infections or steroid administration) should be excluded.
Autoimmune complications, including anemia or thrombocytopenia that respond poorly to corticosteroids.
Symptomatic or functional extranodal involvement (e.g., skin, kidney, lung, or spine). Disease-related symptoms defined as any of the following:
Unintentional weight loss of 10% or more within the previous 6 months.
Significant fatigue (i.e., Eastern Cooperative Oncology Group performance scale 2 or worse, cannot work, or unable to perform usual activities).
Fevers of 100.5°F or 38.0°C or higher for 2 or more weeks without evidence of infection.
Night sweats for at least 1 month without evidence of infection.
Considerations for the Selection of Therapy
The following general principles may provide a sequencing for available therapeutic options:
Despite many therapeutic options, asymptomatic or minimally affected patients with CLL are often offered observation outside the context of a clinical trial. Therapy often begins when patients develop profound cytopenias, or when symptoms, such as enlarging bulky lymphadenopathy or debilitating symptoms, substantially impact their quality of life.
Because nontransplant curative therapy has not been found, the initial goal of therapy is to maximize efficacy (with improvement of overall survival), while introducing the least overall short- and long-term toxicity.
The U.S. Food and Drug Administration approved the biological agents ibrutinib, acalabrutinib, and venetoclax for first-line use in newly diagnosed patients with CLL who require therapy.[16] In patients with poor prognostic factors (especially those with del(17p) or TP53 pathogenic variants), ibrutinib, acalabrutinib, or venetoclax should be considered.[17]
Standard chemotherapeutic agents, such as fludarabine, bendamustine, cyclophosphamide, and chlorambucil, induce DNA damage that can manifest as more aggressive and refractory phenotypes upon relapse and can induce secondary malignancies. Yet, prolonged DFS (over 10 years) can be seen with the use of the FCR regimen in younger patients (<60 years) with IGH hypermutation.[12–14]
Avoiding alkylating agents and purine analogues also prevents prolonged cytopenias and the recurrent, long-lasting, and sometimes fatal infections seen after therapy with these agents.
Avoiding chemotherapeutic agents up-front, when possible, is a new paradigm of sequencing therapy for CLL.
Older patients with comorbidities may better tolerate the newer biological agents (such as ibrutinib or venetoclax), monoclonal antibody therapy alone (such as high-dose rituximab), or dose modification of standard chemotherapeutic agents combined with rituximab. For older patients (>65 years), the combination of rituximab plus bendamustine (BR regimen) resulted in fewer adverse events and better outcomes than the FCR regimen.[18]
Adverse Sequelae of the Disease and Therapy
Infectious complications in advanced disease are in part a consequence of the hypogammaglobulinemia and the inability to mount a humoral defense against bacterial or viral agents. Herpes zoster represents a frequent viral infection in these patients, but infections with Pneumocystis carinii and Candida albicans may also occur. The early recognition of infections and the institution of appropriate therapy are critical to the long-term survival of these patients. A randomized study of intravenous immunoglobulin (400 mg/kg every 3 weeks for 1 year) in patients with CLL and hypogammaglobulinemia produced significantly fewer bacterial infections and a significant delay in onset of first infection during the study period.[19] There was, however, no effect on survival. Routine chronic administration of intravenous immunoglobulin is expensive, and the long-term benefit (>1 year) is unproven.[20,21]
Patients with CLL who required hospitalization for COVID-19 prior to the induction of vaccines fared poorly regardless of stage in two retrospective reports.[22,23] One of the studies noted a protective effect from Bruton tyrosine kinase (BTK) inhibitors (usually ibrutinib),[23] but this was not seen in the other report.[22] With enhanced testing and the advent of multiple therapeutic strategies to prevent and treat COVID-19, the case fatality rate for patients with CLL dropped from 35% in early 2020 to 11% in late 2020 and early 2021 (P < .001).[22] For patients requiring hospitalization, the case fatality rate dropped from 40% to 20% (P = .003).
Autoimmune hemolytic anemia and/or thrombocytopenia can occur in patients with any stage of CLL.[24] Initial therapy involves corticosteroids with or without alkylating agents (fludarabine can worsen the hemolytic anemia). It is often necessary to control the autoimmune destruction with corticosteroids, if possible, before administering marrow-suppressive chemotherapy because it may be difficult for a patient to successfully receive a red blood cell or platelet transfusion. Alternate therapies include high-dose immune globulin, rituximab, cyclosporine, azathioprine, splenectomy, and low-dose radiation therapy to the spleen.[3,25] Tumor lysis syndrome is an uncommon complication (presenting in 1 of 300 patients) of chemotherapy for patients with bulky disease.[26]
Second malignancies and treatment-induced acute leukemias may also occur in a small percentage of patients.[27] Transformation of CLL to diffuse large B-cell lymphoma (DLBCL, known as Richter syndrome) occurs in 2% to 10% of patients. Risk factors for transformation include unmutated IGH, TP53 or NOTCH1 pathogenic variants, CDKN2A/B loss, and a complex karyotype.[28] Up to 60% to 70% of patients develop a DLBCL clonally related to the CLL, and these patients have a significantly worse prognosis than patients with de novo DLBCL.[29–31] Patients with a clonally unrelated DLBCL have a much better prognosis, which is similar to de novo DLBCL.[29] However, there is limited availability for real-life sequencing of the immunoglobulin heavy chains in the original CLL sample to compare with the transformed sample. Characteristic molecular signatures may serve as an alternate way to assess prognosis.[32] Up to 20% to 40% of patients with clonally related Richter syndrome are disease free for more than 5 years after aggressive combination chemotherapy, typically R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) or Pola-R-CHP (polatuzumab, rituximab, cyclophosphamide, doxorubicin, and prednisone), often followed by autologous or allogeneic stem cell transplant.[33–35] For more information, see Aggressive B-Cell Non-Hodgkin Lymphoma Treatment. In two retrospective reports, CLL with transformation to Hodgkin lymphoma had the same prognosis as de novo presentations of Hodgkin lymphoma at an equivalent age.[36,37][Level of evidence C3]
The BTK inhibitors increased the risk of bleeding requiring hospitalization (3-year risk for patients who received ibrutinib, 8.8% [95% confidence interval (CI), 6.5%–11.7%]) and atrial fibrillation (3-year incidence for patients who received ibrutinib, 22.7% [95% CI, 19.0%–26.6%]).[38] A randomized trial with a median follow-up of 41 months showed less atrial fibrillation for patients with CLL who received acalabrutinib compared with ibrutinib (9.4% vs. 16%; P = .02).[39]
Gribben JG, O’Brien S: Update on therapy of chronic lymphocytic leukemia. J Clin Oncol 29 (5): 544-50, 2011. [PUBMED Abstract]
Rozman C, Montserrat E: Chronic lymphocytic leukemia. N Engl J Med 333 (16): 1052-7, 1995. [PUBMED Abstract]
Wierda WG, O’Brien S, Wang X, et al.: Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood 109 (11): 4679-85, 2007. [PUBMED Abstract]
Del Giudice I, Chiaretti S, Tavolaro S, et al.: Spontaneous regression of chronic lymphocytic leukemia: clinical and biologic features of 9 cases. Blood 114 (3): 638-46, 2009. [PUBMED Abstract]
Chemotherapeutic options in chronic lymphocytic leukemia: a meta-analysis of the randomized trials. CLL Trialists’ Collaborative Group. J Natl Cancer Inst 91 (10): 861-8, 1999. [PUBMED Abstract]
Ritgen M, Stilgenbauer S, von Neuhoff N, et al.: Graft-versus-leukemia activity may overcome therapeutic resistance of chronic lymphocytic leukemia with unmutated immunoglobulin variable heavy-chain gene status: implications of minimal residual disease measurement with quantitative PCR. Blood 104 (8): 2600-2, 2004. [PUBMED Abstract]
Moreno C, Villamor N, Colomer D, et al.: Allogeneic stem-cell transplantation may overcome the adverse prognosis of unmutated VH gene in patients with chronic lymphocytic leukemia. J Clin Oncol 23 (15): 3433-8, 2005. [PUBMED Abstract]
Khouri IF, Keating MJ, Saliba RM, et al.: Long-term follow-up of patients with CLL treated with allogeneic hematopoietic transplantation. Cytotherapy 4 (3): 217-21, 2002. [PUBMED Abstract]
Doney KC, Chauncey T, Appelbaum FR, et al.: Allogeneic related donor hematopoietic stem cell transplantation for treatment of chronic lymphocytic leukemia. Bone Marrow Transplant 29 (10): 817-23, 2002. [PUBMED Abstract]
Pavletic SZ, Khouri IF, Haagenson M, et al.: Unrelated donor marrow transplantation for B-cell chronic lymphocytic leukemia after using myeloablative conditioning: results from the Center for International Blood and Marrow Transplant research. J Clin Oncol 23 (24): 5788-94, 2005. [PUBMED Abstract]
Thompson PA, Tam CS, O’Brien SM, et al.: Fludarabine, cyclophosphamide, and rituximab treatment achieves long-term disease-free survival in IGHV-mutated chronic lymphocytic leukemia. Blood 127 (3): 303-9, 2016. [PUBMED Abstract]
Fischer K, Bahlo J, Fink AM, et al.: Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: updated results of the CLL8 trial. Blood 127 (2): 208-15, 2016. [PUBMED Abstract]
Rossi D, Terzi-di-Bergamo L, De Paoli L, et al.: Molecular prediction of durable remission after first-line fludarabine-cyclophosphamide-rituximab in chronic lymphocytic leukemia. Blood 126 (16): 1921-4, 2015. [PUBMED Abstract]
Hallek M, Cheson BD, Catovsky D, et al.: iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 131 (25): 2745-2760, 2018. [PUBMED Abstract]
Burger JA, Tedeschi A, Barr PM, et al.: Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. N Engl J Med 373 (25): 2425-37, 2015. [PUBMED Abstract]
Cramer P, Tausch E, von Tresckow J, et al.: Durable remissions following combined targeted therapy in patients with CLL harboring TP53 deletions and/or mutations. Blood 138 (19): 1805-1816, 2021. [PUBMED Abstract]
Eichhorst B, Fink AM, Bahlo J, et al.: First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol 17 (7): 928-942, 2016. [PUBMED Abstract]
Intravenous immunoglobulin for the prevention of infection in chronic lymphocytic leukemia. A randomized, controlled clinical trial. Cooperative Group for the Study of Immunoglobulin in Chronic Lymphocytic Leukemia. N Engl J Med 319 (14): 902-7, 1988. [PUBMED Abstract]
Griffiths H, Brennan V, Lea J, et al.: Crossover study of immunoglobulin replacement therapy in patients with low-grade B-cell tumors. Blood 73 (2): 366-8, 1989. [PUBMED Abstract]
Weeks JC, Tierney MR, Weinstein MC: Cost effectiveness of prophylactic intravenous immune globulin in chronic lymphocytic leukemia. N Engl J Med 325 (2): 81-6, 1991. [PUBMED Abstract]
Mato AR, Roeker LE, Lamanna N, et al.: Outcomes of COVID-19 in patients with CLL: a multicenter international experience. Blood 136 (10): 1134-1143, 2020. [PUBMED Abstract]
Scarfò L, Chatzikonstantinou T, Rigolin GM, et al.: COVID-19 severity and mortality in patients with chronic lymphocytic leukemia: a joint study by ERIC, the European Research Initiative on CLL, and CLL Campus. Leukemia 34 (9): 2354-2363, 2020. [PUBMED Abstract]
Mauro FR, Foa R, Cerretti R, et al.: Autoimmune hemolytic anemia in chronic lymphocytic leukemia: clinical, therapeutic, and prognostic features. Blood 95 (9): 2786-92, 2000. [PUBMED Abstract]
Kaufman M, Limaye SA, Driscoll N, et al.: A combination of rituximab, cyclophosphamide and dexamethasone effectively treats immune cytopenias of chronic lymphocytic leukemia. Leuk Lymphoma 50 (6): 892-9, 2009. [PUBMED Abstract]
Cheson BD, Frame JN, Vena D, et al.: Tumor lysis syndrome: an uncommon complication of fludarabine therapy of chronic lymphocytic leukemia. J Clin Oncol 16 (7): 2313-20, 1998. [PUBMED Abstract]
Maddocks-Christianson K, Slager SL, Zent CS, et al.: Risk factors for development of a second lymphoid malignancy in patients with chronic lymphocytic leukaemia. Br J Haematol 139 (3): 398-404, 2007. [PUBMED Abstract]
Visentin A, Bonaldi L, Rigolin GM, et al.: The complex karyotype landscape in chronic lymphocytic leukemia allows the refinement of the risk of Richter syndrome transformation. Haematologica 107 (4): 868-876, 2022. [PUBMED Abstract]
Rossi D, Spina V, Deambrogi C, et al.: The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation. Blood 117 (12): 3391-401, 2011. [PUBMED Abstract]
Chigrinova E, Rinaldi A, Kwee I, et al.: Two main genetic pathways lead to the transformation of chronic lymphocytic leukemia to Richter syndrome. Blood 122 (15): 2673-82, 2013. [PUBMED Abstract]
Parry EM, Leshchiner I, Guièze R, et al.: Evolutionary history of transformation from chronic lymphocytic leukemia to Richter syndrome. Nat Med 29 (1): 158-169, 2023. [PUBMED Abstract]
Parry EM, Ten Hacken E, Wu CJ: Richter syndrome: novel insights into the biology of transformation. Blood 142 (1): 11-22, 2023. [PUBMED Abstract]
Robertson LE, Pugh W, O’Brien S, et al.: Richter’s syndrome: a report on 39 patients. J Clin Oncol 11 (10): 1985-9, 1993. [PUBMED Abstract]
Jain N, Keating M, Thompson P, et al.: Ibrutinib and Venetoclax for First-Line Treatment of CLL. N Engl J Med 380 (22): 2095-2103, 2019. [PUBMED Abstract]
Ben-Dali Y, Hleuhel MH, da Cunha-Bang C, et al.: Richter’s transformation in patients with chronic lymphocytic leukaemia: a Nationwide Epidemiological Study. Leuk Lymphoma 61 (6): 1435-1444, 2020. [PUBMED Abstract]
Stephens DM, Boucher K, Kander E, et al.: Hodgkin lymphoma arising in patients with chronic lymphocytic leukemia: outcomes from a large multi-center collaboration. Haematologica 106 (11): 2845-2852, 2021. [PUBMED Abstract]
Al-Sawaf O, Robrecht S, Bahlo J, et al.: Richter transformation in chronic lymphocytic leukemia (CLL)-a pooled analysis of German CLL Study Group (GCLLSG) front line treatment trials. Leukemia 35 (1): 169-176, 2021. [PUBMED Abstract]
Abdel-Qadir H, Sabrie N, Leong D, et al.: Cardiovascular Risk Associated With Ibrutinib Use in Chronic Lymphocytic Leukemia: A Population-Based Cohort Study. J Clin Oncol 39 (31): 3453-3462, 2021. [PUBMED Abstract]
Byrd JC, Hillmen P, Ghia P, et al.: Acalabrutinib Versus Ibrutinib in Previously Treated Chronic Lymphocytic Leukemia: Results of the First Randomized Phase III Trial. J Clin Oncol 39 (31): 3441-3452, 2021. [PUBMED Abstract]
Treatment of Asymptomatic Chronic Lymphocytic Leukemia
Treatment Options for Asymptomatic Chronic Lymphocytic Leukemia (CLL)
Observation
Because of its indolent nature, chemotherapy is not indicated for asymptomatic or minimally affected patients with CLL, and observation is the generally accepted approach.[1] Because the rate of progression may vary, with long periods of stability and sometimes spontaneous regressions, frequent and careful observation is required to monitor the clinical course. One nomogram to predict time-to-first treatment relies on the number of lymph node sites, size of cervical lymph nodes, lactate dehydrogenase level, the IGH mutational status, and the presence of del(11q) or del(17p) established by fluorescence in situ hybridization analysis.[2] Spontaneous regression, manifested by a sustained reduction of the malignant clone without therapy, occurs in less than 5% of patients. These patients almost exclusively have hypermutation of IGH.[3]
Evidence (observation):
The French Cooperative Group on Chronic Lymphocytic Leukemia randomly assigned 1,535 patients with previously untreated stage A disease to receive either chlorambucil or no immediate treatment.[4]
The results showed no survival advantage for immediate treatment with chlorambucil.[4][Level of evidence A1]
A meta-analysis evaluated six trials of patients with early-stage CLL that involved immediate versus deferred therapy with chlorambucil (including the aforementioned trial by the French Cooperative Group).[5]
The results showed no difference in overall survival at 10 years.[5][Level of evidence A1]
Despite many therapeutic options, observation should be considered for asymptomatic or minimally affected patients, even in the context of adverse prognostic findings. Therapy begins when patients develop profound cytopenias or when symptoms adversely impact quality of life.
There are no clinical trial results that confirm that immediate treatment of asymptomatic or minimally affected patients with the B-cell receptor inhibitors or BCL2 inhibitors is superior to observation.
Clinical trials will need to establish improved outcomes using the newer biological therapies in asymptomatic patients before observation or watchful waiting is discontinued.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Casper JT: Prognostic features of early chronic lymphocytic leukaemia. International Workshop on CLL. Lancet 2 (8669): 968-9, 1989.
Molica S, Giannarelli D, Gentile M, et al.: External validation on a prospective basis of a nomogram for predicting the time to first treatment in patients with chronic lymphocytic leukemia. Cancer 119 (6): 1177-85, 2013. [PUBMED Abstract]
Kwok M, Oldreive C, Rawstron AC, et al.: Integrative analysis of spontaneous CLL regression highlights genetic and microenvironmental interdependency in CLL. Blood 135 (6): 411-428, 2020. [PUBMED Abstract]
Dighiero G, Maloum K, Desablens B, et al.: Chlorambucil in indolent chronic lymphocytic leukemia. French Cooperative Group on Chronic Lymphocytic Leukemia. N Engl J Med 338 (21): 1506-14, 1998. [PUBMED Abstract]
Chemotherapeutic options in chronic lymphocytic leukemia: a meta-analysis of the randomized trials. CLL Trialists’ Collaborative Group. J Natl Cancer Inst 91 (10): 861-8, 1999. [PUBMED Abstract]
Treatment of Symptomatic or Progressive Chronic Lymphocytic Leukemia
Treatment Options for Symptomatic or Progressive Chronic Lymphocytic Leukemia (CLL)
The following regimens are considered first-line treatment approaches for patients with CLL who are experiencing symptomatic progression:
R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) (only if Richter syndrome with histological progression is suspected clinically).
Several large prospective clinical trials have compared these approaches. A chemotherapy-free approach for first-line therapy is usually preferred for most patients, but it is mandatory for patients with del(17p) or TP53-altered disease.[1–5]
BTK inhibitors
Ibrutinib versus zanubrutinib
Evidence (ibrutinib vs. zanubrutinib):
A prospective randomized trial of 652 patients with relapsed or refractory CLL compared ibrutinib and zanubrutinib.[6]
With a median follow-up of 29.6 months, the 2-year progression-free survival (PFS) rate was 78.4% in the zanubrutinib group and 65.9% in the ibrutinib group (hazard ratio [HR], 0.65; 95% confidence interval [CI], 0.49–0.86; P = .002).[6][Level of evidence B1]
Cardiac disorders leading to treatment discontinuation occurred in 1 patient (0.3%) in the zanubrutinib group and 14 patients (4.3%) in the ibrutinib group. Six deaths caused by cardiac events were all in patients who received ibrutinib.
Ibrutinib versus acalabrutinib
Evidence (ibrutinib vs. acalabrutinib):
A prospective randomized trial of 533 previously untreated patients compared the BTK inhibitors acalabrutinib and ibrutinib.[7]
With a median follow-up of 41 months, acalabrutinib was noninferior to ibrutinib, with a median PFS of 38.4 months for patients in both arms of the trial (HR, 1.00; 95% CI, 0.79–1.27).[7][Level of evidence B1]
The incidence of atrial fibrillation of any grade was lower for patients who received acalabrutinib than for patients who received ibrutinib (9.4% vs. 16.0%, P = .02). In this trial, the incidence of diarrhea and headaches was significantly higher in patients who received acalabrutinib (P < .05), while musculoskeletal pain was higher in patients who received ibrutinib (P = .0229).[8]
Ventricular arrhythmias and sudden death events appear to be a side effect of all the BTK inhibitors. For acalabrutinib, these events occur with a relative risk of 8.2 over age-matched controls.[9]
Ibrutinib versus ibrutinib plus rituximab versus BR
Evidence (ibrutinib vs. ibrutinib plus rituximab vs. BR):
A prospective trial included 547 previously untreated patients aged 65 years or older. Patients were randomly assigned to receive BR, ibrutinib alone, or ibrutinib plus rituximab.[10]
With a median follow-up of 38 months, the 2-year PFS rate was 74% for patients who received BR. The rates were significantly higher for patients who received ibrutinib alone (87%; HR, 0.39; 95% CI, 0.25–0.58) or ibrutinib plus rituximab (88%; HR, 0.38; 95% CI, 0.25–0.59; P < .001).[10][Level of evidence B1]
There was no difference in PFS between the two ibrutinib groups (HR, 1.00; 95% CI, 0.62–1.62; P = .49) and no difference in overall survival (OS) between each of the groups.
Ibrutinib versus rituximab plus ibrutinib
Evidence (ibrutinib vs. rituximab plus ibrutinib):
A prospective randomized trial included 208 patients who were previously untreated or had relapsed disease. Patients received rituximab plus ibrutinib or ibrutinib alone.[11]
With a median follow-up of 36 months, there was no difference in PFS (86%; HR, 1.04; 95% CI, 0.49−2.20; P = .91).[11][Level of evidence B1]
Ibrutinib versus FCR
Ibrutinib is a selective irreversible inhibitor of BTK, a signaling molecule located upstream in the B-cell receptor-signaling cascade.
Evidence (ibrutinib vs. FCR):
ECOG-E1912 (NCT02048813) was a prospective randomized trial that compared ibrutinib and rituximab with FCR. A total of 529 patients previously untreated for CLL were randomly assigned in a 2:1 ratio to receive either ibrutinib and rituximab followed by ibrutinib maintenance (354 patients) or six cycles of FCR (175 patients).[12,13]
With a median follow-up of 5.8 years, the 5-year OS rate favored the ibrutinib arm (95% vs. 89%) (HR, 0.47; 95% CI, 0.25–0.89; P = .018).[13][Level of evidence A1]
In 281 patients without IGH pathogenic variants, the 5-year PFS rate favored ibrutinib plus rituximab versus FCR (75% vs. 33%) (HR, 0.27; 95% CI, 0.18−0.41; P < .0001). In 114 patients with IGH pathogenic variants, the 5-year PFS rate was also significantly different, at 83% for the ibrutinib arm and 68% for the FCR arm (HR, 0.27; 95% CI, 0.11−0.62; P = .001).[12–14]
Although undetectable measurable residual disease (MRD) was less than 10% between 12 and 36 months follow-up, patients with detectable MRD did not have significantly worse PFS (P = .14 at 12 months, P = .90 at 24 months, and P = .53 at 36 months).[15]
Zanubrutinib versus BR
Evidence (zanubrutinib vs. BR):
A prospective randomized trial included 590 previously untreated patients aged 65 years or older. Patients were randomly assigned to receive zanubrutinib or BR.[16]
With a median follow-up of 26.2 months, the 2-year PFS rate was 85.5% (95% CI, 80.1%–89.6%) for patients who received zanubrutinib and 69.5% (95% CI, 62.4%–75.5%) for patients who received BR (HR, 0.42; 95% CI, 0.28–0.63; P < .0001).[16][Level of evidence B1]
Acalabrutinib plus obinutuzumab versus acalabrutinib versus chlorambucil plus obinutuzumab
Acalabrutinib is a highly selective covalent irreversible BTK inhibitor, designed to minimize the gastrointestinal toxicities and risk of atrial fibrillation seen with ibrutinib.
Evidence (acalabrutinib plus obinutuzumab vs. acalabrutinib vs. chlorambucil plus obinutuzumab):
The prospective ELEVATE TN trial (NCT02475681) included 535 previously untreated patients aged 65 years or older with comorbidities (e.g., creatinine clearance <70 mL/min). Patients were randomly assigned to one of three arms: acalabrutinib plus obinutuzumab, acalabrutinib alone, or chlorambucil plus obinutuzumab.[17]
With a median follow-up of 28 months, the 24-month PFS rates were 93% for acalabrutinib plus obinutuzumab (HR, 0.10; 95% CI, 0.06−0.17; P < .0001), 87% for acalabrutinib alone (HR, 0.20; 95% CI, 0.13−0.30; P < .0001), and 47% for chlorambucil plus obinutuzumab.[17][Level of evidence B1]
There was a small but significant difference in the PFS rates between the two acalabrutinib groups (93% vs. 87% at 24 months), which favored the combination (HR, 0.49; 95% CI, 0.26−0.95).[17]
Venetoclax with initial use of obinutuzumab and rituximab
Venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab
Evidence (venetoclax plus obinutuzumab vs. chlorambucil plus obinutuzumab):
The prospective CLL14 trial (NCT02242942) included 432 previously untreated patients with significant medical comorbidities (6 or higher on the Cumulative Illness Rating Scale; median age, 72 years). Patients were randomly assigned to receive either venetoclax (a highly selective inhibitor of BCL2) plus obinutuzumab (the human anti-CD20 monoclonal antibody) or chlorambucil plus obinutuzumab.[18]
With a median follow-up of 76.4 months, the median PFS rate was 76.2 months for venetoclax plus obinutuzumab, compared with 36.4 months for chlorambucil plus obinutuzumab (HR, 0.40; 95% CI, 0.31–0.52; P < .0001).[18][Level of evidence B1]
The 6-year OS rate was 78.7% for venetoclax plus obinutuzumab and 69.2% for chlorambucil plus obinutuzumab (HR, 0.69; 95% CI, 0.48–1.01; P = .052).
Venetoclax plus rituximab (VenR) versus BR
Evidence (VenR vs. BR):
The prospective MURANO trial (NCT02005471) included 389 patients with relapsed or refractory CLL. Patients were randomly assigned to receive either VenR (venetoclax for 2 years plus rituximab for the first 6 months) or 6 months of BR.
With a median follow-up of 24 months, the 2-year PFS rate was 84.9% for VenR and 36.3% for BR (HR, 0.17; 95% CI, 0.11–0.25; P < .001).[19,20] An update with a 48-month median follow-up, reported in abstract form, showed a 4-year OS rate of 85.3% for VenR and 66.8% for BR (HR, 0.41; 95% CI, 0.26−0.65; P < .0001).[21][Level of evidence A1]
With a median follow-up of 59.2 months, the 5-year OS rate was 82.1% (95% CI, 76.4%–87.8%) for patients who received VenR and 62.2% (95% CI, 54.8%–69.6%) for patients who received BR (P < .0001).[22][Level of evidence A1] The median time to next treatment was 57.8 months (95% CI, 55.1–not estimable) for VenR.
For the 43% of patients assigned to VenR who achieved undetectable MRD at the end of treatment, the median time to MRD conversion was 19.4 months. The median time from MRD conversion to overt clinical progressive disease was another 25.2 months.[22]
Bendamustine and rituximab
BR versus FCR
Evidence (BR vs. FCR):
The German CLL Study Group compared BR versus FCR as first-line therapy in patients with CLL who required therapy.[23]
With a median follow-up of 37.1 months, the median PFS was better for patients who received FCR (55.2 months vs. 41.7 months) (HR, 1.64; 90% CI, 1.31–2.06; P = .001), but there was no difference in the OS rate at 3 years (91% vs. 92%, not significant).[23][Level of evidence B1]
In patients older than 65 years, there was no difference in PFS between the two arms, but more infections occurred with FCR than with BR (grade 3 to 5 infection, 47% vs. 27%).
Fludarabine, cyclophosphamide, and rituximab (FCR)
FCR
FCR is used for patients with an IGH hypermutation.
Evidence (FCR):
Several trials used FCR for appropriate patients with IGH pathogenic variants who required therapy.
The PFS rate exceeded 60% at more than 10 years.[24–26][Level of evidence C2] Nonetheless, late relapses were seen beyond 10 years.
BTK inhibitor plus venetoclax
BTK inhibitor (ibrutinib or acalabrutinib) plus venetoclax
Evidence (BTK inhibitor [ibrutinib or acalabrutinib] plus venetoclax):
A prospective randomized trial included 523 patients with previously untreated CLL. Patients received either ibrutinib plus venetoclax for up to 6 years or FCR for six cycles.[27] This comparison was embedded in a larger three-arm randomization that also included ibrutinib alone for up to 6 years; the statistics were thought too preliminary to analyze the ibrutinib-alone group versus the other arms.
With a median follow-up of 43.7 months, the 3-year OS rate was 98.0% (95% CI, 95.2%–99.2%) in the ibrutinib-plus-venetoclax group and 93.0% (95% CI, 88.9%–95.6%) in the FCR group (HR, 0.31; 95% CI, 0.15–0.67).[27][Level of evidence A1]
The 3-year OS benefit favored ibrutinib plus venetoclax (HR, 0.23; 95% CI, 0.06–0.81) for patients without IGH pathogenic variants, but not for those with IGH pathogenic variants (HR, 0.61; 95% CI, 0.20–1.82).
The 3-year PFS rate was 97.2% (95% CI, 94.1%–98.6%) in the ibrutinib-plus-venetoclax group and 76.8% (95% CI, 70.8%–81.7%) in the FCR group (HR, 0.13; 95% CI, 0.07–0.24; P < .001).
MRD negativity was a requirement for stopping therapy with venetoclax and ibrutinib after 2 years. This trial did not randomly assign patients to either continued therapy or cessation of therapy based on MRD status. The utility and value of MRD could not be determined from this trial due to its design.
A prospective randomized trial (GLOW [NCT03462719]) included 211 patients with previously untreated CLL. Patients were aged 65 and older or aged 18 to 64 with comorbidities and an Eastern Cooperative Oncology Group performance status of 0 to 2. Patients were randomly assigned to receive either fixed-duration ibrutinib and venetoclax (15 months total) or chlorambucil and obinutuzumab (6 months total).[28]
With a median follow-up of 46 months, the 42-month PFS rate was 74.6% in the ibrutinib-plus-venetoclax group and 24.8% in the chlorambucil-plus-obinutuzumab group (HR, 0.214; 95% CI, 0.138–0.334; P < .0001).[28][Level of evidence B1]
Ibrutinib was given for 3 months prior to the combination of venetoclax with ibrutinib to avoid tumor lysis syndrome.
At 3 months after the end of therapy, 40.6% of patients who received ibrutinib and venetoclax achieved undetectable MRD (<10-5 by next-generation sequencing) in the bone marrow, and 43.4% of patients achieved undetectable MRD in the peripheral blood.[28] However, the PFS rate exceeded 90% at 12 months after the end of therapy regardless of if the MRD was detectable or not.
A prospective trial included 867 patients with previously untreated CLL. Patients were randomly assigned to one of three treatment regimens: (1) AV (acalabrutinib and venetoclax), (2) AVO (acalabrutinib, venetoclax, and obinutuzumab), or (3) either BR or FCR (at the discretion of the investigator).[29]
With a median follow-up of 41 months, the 3-year OS rate was 94.1% for patients who received AV and 85.9% for patients who received BR or FCR (HR, 0.33; 95% CI, 0.18–0.56; P < .0001). However, the 3-year OS rate was 87.7% for patients who received AVO compared with 85.9% for patients who received BR or FCR (HR, 0.76; 95% CI, 0.49–1.18; P = nonsignificant).[29][Level of evidence A1]
The 3-year PFS rate was 76.5% for patients who received AV, 83.1% for patients who received AVO, and 66.5% for patients who received BR or FCR. The PFS for patients who received AV versus those who received BR or FCR had an HR of 0.65 (95% CI, 0.49–0.87; P = .004). The PFS for patients who received AVO versus those who received BR or FCR had an HR of 0.42 (95% CI, 0.30–0.59; P < .001).
Although treatment with AVO resulted in a better PFS than AV, there were increased infectious deaths with AVO, especially from COVID-19 (SARS-CoV-2). These deaths accounted for a nonsignificant difference in OS rates between patients who received AVO (87.7%) and patients who received BR or FCR (85.9%).
A phase II trial included 80 previously untreated patients who were aged 65 or older or had high-risk disease. Patients were treated with ibrutinib for 3 months followed by combined ibrutinib plus venetoclax for a total of 24 months.[30]
With a median follow-up of 38.5 months, the 2-year response rate was 82%, the 3-year PFS rate was 93% (95% CI, 88%–99%), and the 3-year OS rate was 96%.[30][Level of evidence C1]
The toxicity of the combination is similar to either agent alone and avoids the tumor lysis syndrome seen when starting with venetoclax.
High rates of undetectable MRD (<10-4 by 8-color flow cytometry) in the peripheral blood (75%) and bone marrow (72%) is unprecedented. The clinical significance of this finding awaits prospective randomized trials to establish clinical outcomes versus either drug alone. This combination has also been tested in the relapsed/refractory setting.[31]
A phase II trial included 159 previously untreated patients aged 70 years or older. Patients received 3 cycles of ibrutinib alone followed by 12 cycles of ibrutinib plus venetoclax.[32]
With a median follow-up of 27.9 months, the complete response rate was 55% (95% CI, 48%–63%), the undetectable MRD rate was 77% (95% CI, 70%–83%) for blood and 60% (95% CI, 52%–67%) for bone marrow, the 2-year PFS rate was 95% (95% CI, 90%–97%), and the 2-year OS rate was 98% (95% CI, 94%–99%).[32][Level of evidence C1]
The toxicity of the ibrutinib-venetoclax combination was similar to either agent alone, and the ibrutinib-alone lead-in avoided tumor lysis syndrome.
A phase II trial included 41 previously untreated patients who received ibrutinib plus venetoclax and obinutuzumab. Patients with undetectable MRD at cycle 16 could opt to discontinue treatment if they had a complete response.[33]
With a median follow-up of 38.4 months, the 3-year PFS rate was 79.9% and the 3-year OS rate was 92.6%.[33][Level of evidence C1]
In summary, these trials establish the use of venetoclax with obinutuzumab or rituximab, or the use of ibrutinib, acalabrutinib, or zanubrutinib as first-line therapy in patients with previously untreated CLL. A lower rate of atrial fibrillation occurs with acalabrutinib or zanubrutinib than with ibrutinib.[6,7,34,35] Unlike ibrutinib or acalabrutinib, which are given continuously until relapse, venetoclax may be stopped after 12 months, with durable maintenance of remission. Venetoclax, ibrutinib, acalabrutinib, or zanubrutinib can be readministered with success, if needed.[35,36] These targeting drugs are also effective for patients with TP53 pathogenic variants.[37] Different regimens of these drugs, as standalone agents or in combinations, with or without obinutuzumab, need to be evaluated in prospective randomized trials. Several provocative phase II and III trials with these combinations have resulted in unprecedented rates of MRD-negative disease which appear more durable;[30,38–41] whether this results in any clinical advantage to a more sequential approach requires prospective randomized trials. The National Comprehensive Cancer Network has listed the combination of venetoclax and ibrutinib as a first-line treatment option for patients with previously untreated CLL.[42] The considerable financial toxicity of these combinations mandates verification of superior efficacy. These trials further establish the rationale for a chemotherapy-free approach for first-line therapy for CLL instead of the previous standard of BR and FCR (which proved more efficacious than chlorambucil regimens). Patients at the highest risk of relapse have multiple poor prognostic factors, including TP53 pathogenic variants, elevated lactate dehydrogenase, elevated beta-2 microglobulin, and prior treatment.[43] These highest risk patients should consider clinical trials.
MRD Testing Outside the Context of a Clinical Trial
Undetectable MRD (≤1 × 10-4 CLL cells in peripheral blood or bone marrow aspirates) can be confirmed by flow cytometry or next-generation sequencing. The attainment of undetectable MRD represents an even more stringent complete remission that was prognostic for improved PFS and OS in multiple studies.[22,44–46]The use of time-limited therapy with venetoclax, or the investigational combination of venetoclax and a BTK inhibitor, has produced complete responses, and even undetectable MRD, in most patients.[22,44,47]
Testing for undetectable MRD has become a standard parameter for defining responses in all modern clinical trials for CLL. Undetectable MRD has prognostic value but its status as a predictive marker is uncertain. The potential value of MRD testing in routine clinical practice depends on whether it can be used for clinical decision making such as stopping, changing, or continuing treatment. High-level evidence for this intervention would require a prospective randomized clinical trial in which MRD was used as a predictive biomarker for a group attaining an OS advantage compared with a control group disregarding MRD status. Such evidence has not been attained. Similar to outcomes in follicular lymphoma and other indolent lymphoid neoplasms, improved PFS in patients with CLL does not directly predict OS.
A phase II trial used a combination of venetoclax and ibrutinib in patients with undetectable MRD after 1 year of therapy. Patients were randomly assigned to receive either ibrutinib maintenance therapy or treatment cessation.[47] All MRD-positive patients continued to receive ibrutinib. With a median follow-up of 34.4 months, the 1-year PFS rates were 98% for patients with undetectable MRD who ceased therapy, 96% for patients with undetectable MRD who received continued ibrutinib, and 97% for MRD-positive patients who received continued ibrutinib. All patients did well at 12 months. Knowledge of MRD status to guide discontinuation of therapy did not affect the outcome.[47]
Another phase II trial included 70 previously untreated patients who received 1 year of venetoclax plus obinutuzumab. Patients were randomly assigned to receive another year of venetoclax irrespective of MRD status, or another year of venetoclax only if they were MRD-positive. With a median follow-up of 35.2 months, the MRD rates were identical for both randomized groups, suggesting no improved efficacy with this approach, although increased adverse events were reported with an extra year of venetoclax.[48]
Before MRD is used outside the context of a clinical trial, conclusive evidence is required to establish that MRD is a predictive biomarker that can guide clinical decisions.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Byrd JC, Furman RR, Coutre SE, et al.: Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med 369 (1): 32-42, 2013. [PUBMED Abstract]
O’Brien S, Furman RR, Coutre S, et al.: Single-agent ibrutinib in treatment-naïve and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood 131 (17): 1910-1919, 2018. [PUBMED Abstract]
O’Brien S, Jones JA, Coutre SE, et al.: Ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia with 17p deletion (RESONATE-17): a phase 2, open-label, multicentre study. Lancet Oncol 17 (10): 1409-1418, 2016. [PUBMED Abstract]
Stilgenbauer S, Eichhorst B, Schetelig J, et al.: Venetoclax in relapsed or refractory chronic lymphocytic leukaemia with 17p deletion: a multicentre, open-label, phase 2 study. Lancet Oncol 17 (6): 768-78, 2016. [PUBMED Abstract]
Stilgenbauer S, Eichhorst B, Schetelig J, et al.: Venetoclax for Patients With Chronic Lymphocytic Leukemia With 17p Deletion: Results From the Full Population of a Phase II Pivotal Trial. J Clin Oncol 36 (19): 1973-1980, 2018. [PUBMED Abstract]
Brown JR, Eichhorst B, Hillmen P, et al.: Zanubrutinib or Ibrutinib in Relapsed or Refractory Chronic Lymphocytic Leukemia. N Engl J Med 388 (4): 319-332, 2023. [PUBMED Abstract]
Byrd JC, Hillmen P, Ghia P, et al.: Acalabrutinib Versus Ibrutinib in Previously Treated Chronic Lymphocytic Leukemia: Results of the First Randomized Phase III Trial. J Clin Oncol 39 (31): 3441-3452, 2021. [PUBMED Abstract]
Seymour JF, Byrd JC, Ghia P, et al.: Detailed safety profile of acalabrutinib vs ibrutinib in previously treated chronic lymphocytic leukemia in the ELEVATE-RR trial. Blood 142 (8): 687-699, 2023. [PUBMED Abstract]
Bhat SA, Gambril J, Azali L, et al.: Ventricular arrhythmias and sudden death events following acalabrutinib initiation. Blood 140 (20): 2142-2145, 2022. [PUBMED Abstract]
Woyach JA, Ruppert AS, Heerema NA, et al.: Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. N Engl J Med 379 (26): 2517-2528, 2018. [PUBMED Abstract]
Burger JA, Sivina M, Jain N, et al.: Randomized trial of ibrutinib vs ibrutinib plus rituximab in patients with chronic lymphocytic leukemia. Blood 133 (10): 1011-1019, 2019. [PUBMED Abstract]
Shanafelt TD, Wang XV, Kay NE, et al.: Ibrutinib-Rituximab or Chemoimmunotherapy for Chronic Lymphocytic Leukemia. N Engl J Med 381 (5): 432-443, 2019. [PUBMED Abstract]
Shanafelt TD, Wang XV, Hanson CA, et al.: Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: updated results of the E1912 trial. Blood 140 (2): 112-120, 2022. [PUBMED Abstract]
Shanafelt TD, Wang V, Kay NE, et al.: Ibrutinib and rituximab provides superior clinical outcome compared to FCR in younger patients with chronic lymphocytic leukemia (CLL): extended follow-up from the E1912 trial. [Abstract] Blood 134 (Suppl 1): A-33, 2019.
Wang XV, Hanson CA, Tschumper RC, et al.: Measurable residual disease does not preclude prolonged progression-free survival in CLL treated with ibrutinib. Blood 138 (26): 2810-2827, 2021. [PUBMED Abstract]
Tam CS, Brown JR, Kahl BS, et al.: Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Lancet Oncol 23 (8): 1031-1043, 2022. [PUBMED Abstract]
Sharman JP, Egyed M, Jurczak W, et al.: Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial. Lancet 395 (10232): 1278-1291, 2020. [PUBMED Abstract]
Al-Sawaf O, Robrecht S, Zhang C, et al.: Venetoclax-obinutuzumab for previously untreated chronic lymphocytic leukemia: 6-year results of the randomized phase 3 CLL14 study. Blood 144 (18): 1924-1935, 2024. [PUBMED Abstract]
Seymour JF, Kipps TJ, Eichhorst B, et al.: Venetoclax-Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukemia. N Engl J Med 378 (12): 1107-1120, 2018. [PUBMED Abstract]
Kater AP, Seymour JF, Hillmen P, et al.: Fixed Duration of Venetoclax-Rituximab in Relapsed/Refractory Chronic Lymphocytic Leukemia Eradicates Minimal Residual Disease and Prolongs Survival: Post-Treatment Follow-Up of the MURANO Phase III Study. J Clin Oncol 37 (4): 269-277, 2019. [PUBMED Abstract]
Seymour JF, Kipps TJ, Eichhorst BF, et al.: Four-year analysis of Murano study confirms sustained benefit of time-limited venetoclax-rituximab (VenR) in relapsed/refractory (R/R) chronic lymphocytic leukemia (CLL). [Abstract] Blood 134 (Suppl 1): A-355, 2019.
Seymour JF, Kipps TJ, Eichhorst BF, et al.: Enduring undetectable MRD and updated outcomes in relapsed/refractory CLL after fixed-duration venetoclax-rituximab. Blood 140 (8): 839-850, 2022. [PUBMED Abstract]
Eichhorst B, Fink AM, Bahlo J, et al.: First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol 17 (7): 928-942, 2016. [PUBMED Abstract]
Thompson PA, Tam CS, O’Brien SM, et al.: Fludarabine, cyclophosphamide, and rituximab treatment achieves long-term disease-free survival in IGHV-mutated chronic lymphocytic leukemia. Blood 127 (3): 303-9, 2016. [PUBMED Abstract]
Fischer K, Bahlo J, Fink AM, et al.: Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: updated results of the CLL8 trial. Blood 127 (2): 208-15, 2016. [PUBMED Abstract]
Rossi D, Terzi-di-Bergamo L, De Paoli L, et al.: Molecular prediction of durable remission after first-line fludarabine-cyclophosphamide-rituximab in chronic lymphocytic leukemia. Blood 126 (16): 1921-4, 2015. [PUBMED Abstract]
Munir T, Cairns DA, Bloor A, et al.: Chronic Lymphocytic Leukemia Therapy Guided by Measurable Residual Disease. N Engl J Med 390 (4): 326-337, 2024. [PUBMED Abstract]
Niemann CU, Munir T, Moreno C, et al.: Fixed-duration ibrutinib-venetoclax versus chlorambucil-obinutuzumab in previously untreated chronic lymphocytic leukaemia (GLOW): 4-year follow-up from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 24 (12): 1423-1433, 2023. [PUBMED Abstract]
Brown JR, Seymour JF, Jurczak W, et al.: Fixed-Duration Acalabrutinib Combinations in Untreated Chronic Lymphocytic Leukemia. N Engl J Med 392 (8): 748-762, 2025. [PUBMED Abstract]
Wierda WG, Allan JN, Siddiqi T, et al.: Ibrutinib Plus Venetoclax for First-Line Treatment of Chronic Lymphocytic Leukemia: Primary Analysis Results From the Minimal Residual Disease Cohort of the Randomized Phase II CAPTIVATE Study. J Clin Oncol 39 (34): 3853-3865, 2021. [PUBMED Abstract]
Hillmen P, Rawstron AC, Brock K, et al.: Ibrutinib Plus Venetoclax in Relapsed/Refractory Chronic Lymphocytic Leukemia: The CLARITY Study. J Clin Oncol 37 (30): 2722-2729, 2019. [PUBMED Abstract]
Tam CS, Allan JN, Siddiqi T, et al.: Fixed-duration ibrutinib plus venetoclax for first-line treatment of CLL: primary analysis of the CAPTIVATE FD cohort. Blood 139 (22): 3278-3289, 2022. [PUBMED Abstract]
Huber H, Tausch E, Schneider C, et al.: Final analysis of the CLL2-GIVe trial: obinutuzumab, ibrutinib, and venetoclax for untreated CLL with del(17p)/TP53mut. Blood 142 (11): 961-972, 2023. [PUBMED Abstract]
Hillmen P, Eichhorst B, Brown JR, et al.: Zanubrutinib Versus Ibrutinib in Relapsed/Refractory Chronic Lymphocytic Leukemia and Small Lymphocytic Lymphoma: Interim Analysis of a Randomized Phase III Trial. J Clin Oncol 41 (5): 1035-1045, 2023. [PUBMED Abstract]
Shadman M, Flinn IW, Levy MY, et al.: Zanubrutinib in patients with previously treated B-cell malignancies intolerant of previous Bruton tyrosine kinase inhibitors in the USA: a phase 2, open-label, single-arm study. Lancet Haematol 10 (1): e35-e45, 2023. [PUBMED Abstract]
Ma S, Seymour JF, Brander DM, et al.: Efficacy of venetoclax plus rituximab for relapsed CLL: 5-year follow-up of continuous or limited- duration therapy. Blood 138 (10): 836-846, 2021. [PUBMED Abstract]
Allan JN, Shanafelt T, Wiestner A, et al.: Long-term efficacy of first-line ibrutinib treatment for chronic lymphocytic leukaemia in patients with TP53 aberrations: a pooled analysis from four clinical trials. Br J Haematol 196 (4): 947-953, 2022. [PUBMED Abstract]
Jain N, Keating M, Thompson P, et al.: Ibrutinib and Venetoclax for First-Line Treatment of CLL. N Engl J Med 380 (22): 2095-2103, 2019. [PUBMED Abstract]
Rogers KA, Huang Y, Ruppert AS, et al.: Phase II Study of Combination Obinutuzumab, Ibrutinib, and Venetoclax in Treatment-Naïve and Relapsed or Refractory Chronic Lymphocytic Leukemia. J Clin Oncol 38 (31): 3626-3637, 2020. [PUBMED Abstract]
Soumerai JD, Mato AR, Dogan A, et al.: Zanubrutinib, obinutuzumab, and venetoclax with minimal residual disease-driven discontinuation in previously untreated patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: a multicentre, single-arm, phase 2 trial. Lancet Haematol 8 (12): e879-e890, 2021. [PUBMED Abstract]
Huber H, Edenhofer S, von Tresckow J, et al.: Obinutuzumab (GA-101), ibrutinib, and venetoclax (GIVe) frontline treatment for high-risk chronic lymphocytic leukemia. Blood 139 (9): 1318-1329, 2022. [PUBMED Abstract]
Wierda WG, Brown J, Abramson JS, et al.: Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 22 (3): 175-204, 2024. [PUBMED Abstract]
Ahn IE, Tian X, Ipe D, et al.: Prediction of Outcome in Patients With Chronic Lymphocytic Leukemia Treated With Ibrutinib: Development and Validation of a Four-Factor Prognostic Model. J Clin Oncol 39 (6): 576-585, 2021. [PUBMED Abstract]
Kovacs G, Robrecht S, Fink AM, et al.: Minimal Residual Disease Assessment Improves Prediction of Outcome in Patients With Chronic Lymphocytic Leukemia (CLL) Who Achieve Partial Response: Comprehensive Analysis of Two Phase III Studies of the German CLL Study Group. J Clin Oncol 34 (31): 3758-3765, 2016. [PUBMED Abstract]
Al-Sawaf O, Zhang C, Lu T, et al.: Minimal Residual Disease Dynamics after Venetoclax-Obinutuzumab Treatment: Extended Off-Treatment Follow-up From the Randomized CLL14 Study. J Clin Oncol 39 (36): 4049-4060, 2021. [PUBMED Abstract]
Thompson PA, Srivastava J, Peterson C, et al.: Minimal residual disease undetectable by next-generation sequencing predicts improved outcome in CLL after chemoimmunotherapy. Blood 134 (22): 1951-1959, 2019. [PUBMED Abstract]
Kater AP, Levin MD, Dubois J, et al.: Minimal residual disease-guided stop and start of venetoclax plus ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia (HOVON141/VISION): primary analysis of an open-label, randomised, phase 2 trial. Lancet Oncol 23 (6): 818-828, 2022. [PUBMED Abstract]
Kersting S, Dubois J, Nasserinejad K, et al.: Venetoclax consolidation after fixed-duration venetoclax plus obinutuzumab for previously untreated chronic lymphocytic leukaemia (HOVON 139/GiVe): primary endpoint analysis of a multicentre, open-label, randomised, parallel-group, phase 2 trial. Lancet Haematol 9 (3): e190-e199, 2022. [PUBMED Abstract]
Treatment of Recurrent or Refractory Chronic Lymphocytic Leukemia
Treatment Options for Recurrent or Refractory Chronic Lymphocytic Leukemia (CLL)
The same regimens considered for first-line therapy for patients with CLL can be readministered in a sequential fashion. These regimens are described in more detail under first-line therapy. For more information, see the Treatment of Symptomatic or Progressive CLL section.
Bruton tyrosine kinase (BTK) inhibitors (acalabrutinib, zanubrutinib, or ibrutinib).
Venetoclax with initial use of obinutuzumab or rituximab.
Bendamustine and rituximab (BR).
Fludarabine, cyclophosphamide, and rituximab (FCR).
BTK inhibitor (ibrutinib or acalabrutinib) plus venetoclax.
R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) (only if Richter syndrome with histological progression is suspected clinically).
In the relapsed setting, venetoclax showed similar efficacy and safety even after previous therapy with ibrutinib or idelalisib (the phosphatidylinositol 3-kinase [PI3K] delta inhibitor).[1,2]
Similarly, in a trial reported in abstract form, ibrutinib and acalabrutinib showed similar efficacy and safety after previous therapy with venetoclax.[3] Sequencing these novel agents showed efficacy in the relapsed/refractory setting.[4,5]
Noncovalent BTK inhibitors
Unlike other BTK inhibitors (ibrutinib, acalabrutinib, and zanubrutinib), pirtobrutinib binds to BTK in a noncovalent manner.[6]
In a prospective phase I/II study, 317 patients with CLL/small lymphocytic leukemia received pirtobrutinib. A total of 247 of these patients had been treated previously with a covalent-binding BTK inhibitor.[7]
With a median follow-up of 19.4 months, the median progression-free survival (PFS) was 19.6 months (95% confidence interval [CI], 16.9–22.1) for all patients and 16.8 months (95% CI, 13.2–18.7) for the subgroup of patients with BTK inhibitor resistance, intolerance, or BTK C481 variants (a resistance variant for the covalent agents).[7][Level of evidence C3]
In this trial, 82 patients had a diagnosis of Richter transformation. Among those patients, the overall response rate was 50.0% (95% CI, 38.7%–61.3%), and the complete response rate was 13%.[8][Level of evidence C3]
Chimeric antigen receptor (CAR) T-cell therapy
Autologous T cells can be modified by viral vectors to incorporate antigen receptor specificity for the B-cell antigen CD19 and then infused into previously treated patients.[9] A dramatic response lasting 6 months has prompted larger trials of this concept. Ongoing clinical trials are testing the concept of T cells directed at CD19 with engineered CAR T cells.[10–12]
PI3K inhibitors
Idelalisib is an oral inhibitor of the delta isoform of PI3K, which is in the B-cell receptor-signaling cascade. This drug has been withdrawn from its U.S. Food and Drug Administration (FDA) indication due to toxicity and is no longer available. Duvelisib is an oral dual inhibitor of the delta and gamma isoforms of PI3K.[13]
In a prospective trial, 319 patients with relapsed and refractory CLL/small lymphocytic lymphoma were randomly assigned to receive duvelisib versus ofatumumab.[14]
With a median follow-up of 22.4 months, the median PFS was significantly higher for patients who received duvelisib, at 13.3 months, than for patients who received ofatumumab, at 9.9 months (hazard ratio [HR], 0.52; P < .0001).[14][Level of evidence B1]
Serious side effects include infections, pneumonitis, diarrhea or colitis, dermatitis, neutropenia, rash, fatigue, pyrexia, nausea, anemia, and transaminitis.
The FDA has approved duvelisib for third-line (or greater) use. However, follow-up data submitted to the FDA showed, with a median follow-up of 63 months, a median OS of 52.3 months (95% CI, 41.8–68.0) in the duvelisib group and 63.3 months (95% CI, 41.2–not estimable) in the ofatumumab group.[15]
Lenalidomide (with or without rituximab)
Lenalidomide is an oral immunomodulatory agent with response rates of more than 50%, with or without rituximab, for patients with previously treated and untreated disease.[16–22][Level of evidence C3] Prolonged, lower-dose approaches and attention to prevention of tumor lysis syndrome are suggested with this agent.[16,23] Combination therapy and long-term toxicities from using lenalidomide (such as increased myelodysplasia, as seen in myeloma patients) remain undefined for patients with CLL.
Bone marrow or peripheral blood stem cell transplant
In a prospective randomized trial, 241 previously untreated patients younger than 66 years with advanced-stage disease received induction therapy with a CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone)-based regimen followed by fludarabine.[24] Complete responders (105 patients) were randomly assigned to undergo autologous stem cell transplant (SCT) or observation, while the other 136 patients were randomly assigned to receive dexamethasone, high-dose cytarabine, and cisplatin reinduction followed by either autologous SCT or fludarabine plus cyclophosphamide (FC). Although the 3-year event-free survival (EFS) favored autologous SCT in complete responders, there was no difference in OS in any of the randomized comparisons.[24][Level of evidence B1] Autologous bone marrow/stem cell transplant is rarely employed for patients with relapsed CLL.
Patients with adverse prognostic factors are very likely to die from CLL. These patients are candidates for clinical trials that employ high-dose chemotherapy and immunotherapy with myeloablative or nonmyeloablative allogeneic peripheral blood SCT.[25–30] Although most patients who attain complete remission after autologous SCT eventually relapse, a survival plateau for allogeneic SCT suggests an additional graft-versus-leukemia effect.[30] A series (NCT00281983) of 90 patients with relapsed or refractory CLL who underwent allogeneic SCT reported a 6-year OS rate of 58% and a 6-year EFS rate of 38%, which included patients with the worst prognostic factors (such as a TP53 pathogenic variant).[31][Level of evidence C2]
Ofatumumab
Ofatumumab is a humanized anti-CD20 monoclonal antibody.
Evidence (ofatumumab alone and in combination with chlorambucil):
A prospective trial included 474 previously treated patients who attained partial or complete remission to second- or third-line chemotherapy. Patients were randomly assigned to 2 years of maintenance therapy with ofatumumab versus observation.[32]
With a median follow-up of 19 months, median PFS favored the ofatumumab maintenance arm, at 29.4 months versus 15.2 months (HR, 0.50; 95% CI, 0.38–0.66; P < .0001). There was no difference in OS.[32][Level of evidence B1]
A prospective randomized trial of 447 patients who were previously untreated compared ofatumumab plus chlorambucil with chlorambucil alone.[33]
With a median follow-up of 2 years, median PFS favored the ofatumumab plus chlorambucil arm, at 22.4 months versus 13.1 months (HR, 0.57; 95% CI, 0.45–0.72; P = .0001). There was no difference in OS.[33][Level of evidence B1]
Involved-field radiation therapy
Relatively low doses of radiation therapy can be administered for lymphadenopathy that causes problems due to size or encroachment on adjacent organs. Sometimes radiation therapy to one nodal area or the spleen will result in an abscopal effect (i.e., the shrinkage of lymph nodes in untreated sites).
Alemtuzumab, the monoclonal antibody directed at CD52, shows activity in the setting of chemotherapy-resistant disease or high-risk untreated patients with del(17p) or TP53 pathogenic variants.[34–36] As a single agent, the subcutaneous route of delivery is preferred to the intravenous route in patients because of the similar efficacy and decreased adverse effects, including less acute allergic reactions that were shown in some nonrandomized reports.[36–40]
In a combination regimen, subcutaneous alemtuzumab plus fludarabine (with or without cyclophosphamide) or intravenous alemtuzumab plus alkylating agents have resulted in excess infectious toxicities and death, with no compensatory improvement in efficacy in three phase II trials and one randomized trial.[41–43][Level of evidence C3]; [44][Level of evidence B1]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Jones JA, Mato AR, Wierda WG, et al.: Venetoclax for chronic lymphocytic leukaemia progressing after ibrutinib: an interim analysis of a multicentre, open-label, phase 2 trial. Lancet Oncol 19 (1): 65-75, 2018. [PUBMED Abstract]
Coutre S, Choi M, Furman RR, et al.: Venetoclax for patients with chronic lymphocytic leukemia who progressed during or after idelalisib therapy. Blood 131 (15): 1704-1711, 2018. [PUBMED Abstract]
Kater AP, Wu JQ, Kipps T, et al.: Venetoclax Plus Rituximab in Relapsed Chronic Lymphocytic Leukemia: 4-Year Results and Evaluation of Impact of Genomic Complexity and Gene Mutations From the MURANO Phase III Study. J Clin Oncol 38 (34): 4042-4054, 2020. [PUBMED Abstract]
Mato AR, Hill BT, Lamanna N, et al.: Optimal sequencing of ibrutinib, idelalisib, and venetoclax in chronic lymphocytic leukemia: results from a multicenter study of 683 patients. Ann Oncol 28 (5): 1050-1056, 2017. [PUBMED Abstract]
Kater AP, Arslan Ö, Demirkan F, et al.: Activity of venetoclax in patients with relapsed or refractory chronic lymphocytic leukaemia: analysis of the VENICE-1 multicentre, open-label, single-arm, phase 3b trial. Lancet Oncol 25 (4): 463-473, 2024. [PUBMED Abstract]
Thompson PA, Tam CS: Pirtobrutinib: a new hope for patients with BTK inhibitor-refractory lymphoproliferative disorders. Blood 141 (26): 3137-3142, 2023. [PUBMED Abstract]
Mato AR, Woyach JA, Brown JR, et al.: Pirtobrutinib after a Covalent BTK Inhibitor in Chronic Lymphocytic Leukemia. N Engl J Med 389 (1): 33-44, 2023. [PUBMED Abstract]
Wierda WG, Shah NN, Cheah CY, et al.: Pirtobrutinib, a highly selective, non-covalent (reversible) BTK inhibitor in patients with B-cell malignancies: analysis of the Richter transformation subgroup from the multicentre, open-label, phase 1/2 BRUIN study. Lancet Haematol 11 (9): e682-e692, 2024. [PUBMED Abstract]
Porter DL, Levine BL, Kalos M, et al.: Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med 365 (8): 725-33, 2011. [PUBMED Abstract]
Turtle CJ, Hay KA, Hanafi LA, et al.: Durable Molecular Remissions in Chronic Lymphocytic Leukemia Treated With CD19-Specific Chimeric Antigen Receptor-Modified T Cells After Failure of Ibrutinib. J Clin Oncol 35 (26): 3010-3020, 2017. [PUBMED Abstract]
Siddiqi T, Soumerai JD, Dorritie KA: Rapid undetectable MRD (uMRD) responses in patients with relapsed/refractory (R/R) chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) treated with lisocabtagene maraleucel (liso-cel), a CD19-directed CAR T cell product: updated results from Transcend CLL 004, a phase 1/2 study including patients with high-risk disease previously treated with ibrutinib. [Abstract] Blood 134 (Suppl 1): 503, 2019.
Frey NV, Gill S, Hexner EO, et al.: Long-Term Outcomes From a Randomized Dose Optimization Study of Chimeric Antigen Receptor Modified T Cells in Relapsed Chronic Lymphocytic Leukemia. J Clin Oncol 38 (25): 2862-2871, 2020. [PUBMED Abstract]
Patel K, Danilov AV, Pagel JM: Duvelisib for CLL/SLL and follicular non-Hodgkin lymphoma. Blood 134 (19): 1573-1577, 2019. [PUBMED Abstract]
Flinn IW, Hillmen P, Montillo M, et al.: The phase 3 DUO trial: duvelisib vs ofatumumab in relapsed and refractory CLL/SLL. Blood 132 (23): 2446-2455, 2018. [PUBMED Abstract]
U.S. Food and Drug Administration: FDA warns about possible increased risk of death and serious side effects with cancer drug Copiktra (duvelisib). Silver Spring, Md: U.S. Food and Drug Administration, 2022. Available online. Last accessed April 3, 2025.
Chen CI, Bergsagel PL, Paul H, et al.: Single-agent lenalidomide in the treatment of previously untreated chronic lymphocytic leukemia. J Clin Oncol 29 (9): 1175-81, 2011. [PUBMED Abstract]
Chanan-Khan A, Miller KC, Musial L, et al.: Clinical efficacy of lenalidomide in patients with relapsed or refractory chronic lymphocytic leukemia: results of a phase II study. J Clin Oncol 24 (34): 5343-9, 2006. [PUBMED Abstract]
Ferrajoli A, Lee BN, Schlette EJ, et al.: Lenalidomide induces complete and partial remissions in patients with relapsed and refractory chronic lymphocytic leukemia. Blood 111 (11): 5291-7, 2008. [PUBMED Abstract]
Strati P, Keating MJ, Wierda WG, et al.: Lenalidomide induces long-lasting responses in elderly patients with chronic lymphocytic leukemia. Blood 122 (5): 734-7, 2013. [PUBMED Abstract]
Wendtner CM, Hillmen P, Mahadevan D, et al.: Final results of a multicenter phase 1 study of lenalidomide in patients with relapsed or refractory chronic lymphocytic leukemia. Leuk Lymphoma 53 (3): 417-23, 2012. [PUBMED Abstract]
Badoux XC, Keating MJ, Wen S, et al.: Phase II study of lenalidomide and rituximab as salvage therapy for patients with relapsed or refractory chronic lymphocytic leukemia. J Clin Oncol 31 (5): 584-91, 2013. [PUBMED Abstract]
Takahashi K, Hu B, Wang F, et al.: Clinical implications of cancer gene mutations in patients with chronic lymphocytic leukemia treated with lenalidomide. Blood 131 (16): 1820-1832, 2018. [PUBMED Abstract]
Sutton L, Chevret S, Tournilhac O, et al.: Autologous stem cell transplantation as a first-line treatment strategy for chronic lymphocytic leukemia: a multicenter, randomized, controlled trial from the SFGM-TC and GFLLC. Blood 117 (23): 6109-19, 2011. [PUBMED Abstract]
Toze CL, Dalal CB, Nevill TJ, et al.: Allogeneic haematopoietic stem cell transplantation for chronic lymphocytic leukaemia: outcome in a 20-year cohort. Br J Haematol 158 (2): 174-85, 2012. [PUBMED Abstract]
Khouri IF, Saliba RM, Admirand J, et al.: Graft-versus-leukaemia effect after non-myeloablative haematopoietic transplantation can overcome the unfavourable expression of ZAP-70 in refractory chronic lymphocytic leukaemia. Br J Haematol 137 (4): 355-63, 2007. [PUBMED Abstract]
Sorror ML, Storer BE, Sandmaier BM, et al.: Five-year follow-up of patients with advanced chronic lymphocytic leukemia treated with allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning. J Clin Oncol 26 (30): 4912-20, 2008. [PUBMED Abstract]
Schetelig J, van Biezen A, Brand R, et al.: Allogeneic hematopoietic stem-cell transplantation for chronic lymphocytic leukemia with 17p deletion: a retrospective European Group for Blood and Marrow Transplantation analysis. J Clin Oncol 26 (31): 5094-100, 2008. [PUBMED Abstract]
Malhotra P, Hogan WJ, Litzow MR, et al.: Long-term outcome of allogeneic stem cell transplantation in chronic lymphocytic leukemia: analysis after a minimum follow-up of 5 years. Leuk Lymphoma 49 (9): 1724-30, 2008. [PUBMED Abstract]
Dreger P, Döhner H, Ritgen M, et al.: Allogeneic stem cell transplantation provides durable disease control in poor-risk chronic lymphocytic leukemia: long-term clinical and MRD results of the German CLL Study Group CLL3X trial. Blood 116 (14): 2438-47, 2010. [PUBMED Abstract]
Dreger P, Schnaiter A, Zenz T, et al.: TP53, SF3B1, and NOTCH1 mutations and outcome of allotransplantation for chronic lymphocytic leukemia: six-year follow-up of the GCLLSG CLL3X trial. Blood 121 (16): 3284-8, 2013. [PUBMED Abstract]
van Oers MH, Kuliczkowski K, Smolej L, et al.: Ofatumumab maintenance versus observation in relapsed chronic lymphocytic leukaemia (PROLONG): an open-label, multicentre, randomised phase 3 study. Lancet Oncol 16 (13): 1370-9, 2015. [PUBMED Abstract]
Hillmen P, Robak T, Janssens A, et al.: Chlorambucil plus ofatumumab versus chlorambucil alone in previously untreated patients with chronic lymphocytic leukaemia (COMPLEMENT 1): a randomised, multicentre, open-label phase 3 trial. Lancet 385 (9980): 1873-83, 2015. [PUBMED Abstract]
Moreton P, Kennedy B, Lucas G, et al.: Eradication of minimal residual disease in B-cell chronic lymphocytic leukemia after alemtuzumab therapy is associated with prolonged survival. J Clin Oncol 23 (13): 2971-9, 2005. [PUBMED Abstract]
Parikh SA, Keating MJ, O’Brien S, et al.: Frontline chemoimmunotherapy with fludarabine, cyclophosphamide, alemtuzumab, and rituximab for high-risk chronic lymphocytic leukemia. Blood 118 (8): 2062-8, 2011. [PUBMED Abstract]
Pettitt AR, Jackson R, Carruthers S, et al.: Alemtuzumab in combination with methylprednisolone is a highly effective induction regimen for patients with chronic lymphocytic leukemia and deletion of TP53: final results of the national cancer research institute CLL206 trial. J Clin Oncol 30 (14): 1647-55, 2012. [PUBMED Abstract]
Stilgenbauer S, Zenz T, Winkler D, et al.: Subcutaneous alemtuzumab in fludarabine-refractory chronic lymphocytic leukemia: clinical results and prognostic marker analyses from the CLL2H study of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol 27 (24): 3994-4001, 2009. [PUBMED Abstract]
Cortelezzi A, Pasquini MC, Gardellini A, et al.: Low-dose subcutaneous alemtuzumab in refractory chronic lymphocytic leukaemia (CLL): results of a prospective, single-arm multicentre study. Leukemia 23 (11): 2027-33, 2009. [PUBMED Abstract]
Osterborg A, Foà R, Bezares RF, et al.: Management guidelines for the use of alemtuzumab in chronic lymphocytic leukemia. Leukemia 23 (11): 1980-8, 2009. [PUBMED Abstract]
Gritti G, Reda G, Maura F, et al.: Low dose alemtuzumab in patients with fludarabine-refractory chronic lymphocytic leukemia. Leuk Lymphoma 53 (3): 424-9, 2012. [PUBMED Abstract]
Lin TS, Donohue KA, Byrd JC, et al.: Consolidation therapy with subcutaneous alemtuzumab after fludarabine and rituximab induction therapy for previously untreated chronic lymphocytic leukemia: final analysis of CALGB 10101. J Clin Oncol 28 (29): 4500-6, 2010. [PUBMED Abstract]
Badoux XC, Keating MJ, Wang X, et al.: Cyclophosphamide, fludarabine, alemtuzumab, and rituximab as salvage therapy for heavily pretreated patients with chronic lymphocytic leukemia. Blood 118 (8): 2085-93, 2011. [PUBMED Abstract]
Lepretre S, Aurran T, Mahé B, et al.: Excess mortality after treatment with fludarabine and cyclophosphamide in combination with alemtuzumab in previously untreated patients with chronic lymphocytic leukemia in a randomized phase 3 trial. Blood 119 (22): 5104-10, 2012. [PUBMED Abstract]
Geisler CH, van T’ Veer MB, Jurlander J, et al.: Frontline low-dose alemtuzumab with fludarabine and cyclophosphamide prolongs progression-free survival in high-risk CLL. Blood 123 (21): 3255-62, 2014. [PUBMED Abstract]
Key References for Chronic Lymphocytic Leukemia Treatment
These references have been identified by members of the PDQ Adult Treatment Editorial Board as significant in the field of chronic lymphocytic leukemia (CLL) treatment. This list is provided to inform users of important studies that have helped shape the current understanding of and treatment options for CLL. Listed after each reference are the sections within this summary where the reference is cited.
Seymour JF, Kipps TJ, Eichhorst BF, et al.: Four-year analysis of Murano study confirms sustained benefit of time-limited venetoclax-rituximab (VenR) in relapsed/refractory (R/R) chronic lymphocytic leukemia (CLL). [Abstract] Blood 134 (Suppl 1): A-355, 2019.
Shanafelt TD, Wang XV, Kay NE, et al.: Ibrutinib-Rituximab or Chemoimmunotherapy for Chronic Lymphocytic Leukemia. N Engl J Med 381 (5): 432-443, 2019. [PUBMED Abstract]
Shanafelt TD, Wang V, Kay NE, et al.: Ibrutinib and rituximab provides superior clinical outcome compared to FCR in younger patients with chronic lymphocytic leukemia (CLL): extended follow-up from the E1912 trial. [Abstract] Blood 134 (Suppl 1): A-33, 2019.
Al-Sawaf O, Zhang C, Tandon M, et al.: Venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab for previously untreated chronic lymphocytic leukaemia (CLL14): follow-up results from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncology 21 (9): 1188-1200, 2020. [PUBMED Abstract]
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Revised text about the results of a prospective trial that included 432 previously untreated patients with significant medical comorbidities. Patients were randomly assigned to receive either venetoclax plus obinutuzumab or chlorambucil plus obinutuzumab (cited Al-Sawaf et al. as reference 18).
Added text about a prospective trial that included 867 patients with previously untreated CLL. Patients were randomly assigned to one of three treatment regimens: (1) acalabrutinib and venetoclax, (2) acalabrutinib, venetoclax, and obinutuzumab, or (3) either bendamustine and rituximab or fludarabine, cyclophosphamide, and rituximab (at the discretion of the investigator) (cited Brown et al. as reference 29 and level of evidence A1).
Added text to state that the National Comprehensive Cancer Network has listed the combination of venetoclax and ibrutinib as a first-line treatment option for patients with previously untreated CLL (cited Wierda et al. as reference 42).
Revised text about the results of a prospective phase I/II study of pirtobrutinib in 317 patients with CLL/small lymphocytic leukemia (cited Wierda et al. as reference 8 and level of evidence C3).
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of chronic lymphocytic leukemia. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewer for Chronic Lymphocytic Leukemia Treatment is:
Eric J. Seifter, MD (Johns Hopkins University)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Chronic Lymphocytic Leukemia Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/leukemia/hp/cll-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389470]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Like Hodgkin lymphoma, NHL usually originates in lymphoid tissues and can spread to other organs. However, NHL is much less predictable than Hodgkin lymphoma and has a far greater tendency to spread to extranodal sites. The prognosis depends on the histological type, disease stage, and treatment.
Incidence and Mortality
Estimated new cases and deaths from all types of NHL in the United States in 2025:[2]
New cases: 80,350.
Deaths: 19,390.
B-cell lymphomas make up about 85% of NHL cases.[3]
Anatomy
NHL usually originates in lymphoid tissues.
EnlargeThe lymph system is part of the body’s immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, adenoids (not shown), thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph tissue is also found in many other parts of the body, including the small intestine.
Prognosis and Survival
NHL can be divided into two prognostic groups: indolent lymphomas and aggressive lymphomas.
Indolent NHL has a relatively good prognosis, with a median survival as long as 20 years, but it is usually not curable in advanced clinical stages.[4]
Aggressive NHL has a worse prognosis in the short term, but a significant number of these patients can be cured with intensive combination chemotherapy regimens. Patients who present with, or convert to, aggressive forms of NHL may have sustained complete remissions with combination chemotherapy regimens or aggressive consolidation with marrow or stem cell support.[5,6]
In general, with modern treatment of patients with NHL, the 5-year overall survival rate is over 60%. More than 70% of patients with aggressive NHL can be cured. Most relapses occur in the first 2 years after therapy. The risk of late relapse is higher in patients who manifest both indolent and aggressive histologies.[7]
Late Effects of Treatment of NHL
Late effects of treatment of non-Hodgkin lymphoma (NHL) have been observed. Impaired fertility may occur after exposure to alkylating agents.[8] For as many as three decades after diagnosis, patients are at a significantly elevated risk of developing second primary cancers, especially the following:[9–12]
Lung cancer.
Brain cancer.
Kidney cancer.
Bladder cancer.
Melanoma.
Hodgkin lymphoma.
Acute nonlymphocytic leukemia.
Left ventricular dysfunction was a significant late effect in long-term survivors of high-grade NHL who received more than 200 mg/m² of doxorubicin.[8,13]
Myelodysplastic syndrome and acute myelogenous leukemia are late complications of myeloablative therapy with autologous bone marrow or peripheral blood stem cell support, as well as conventional chemotherapy-containing alkylating agents.[10,14–21] Most of these patients show clonal hematopoiesis even before the transplant, suggesting that the hematologic injury usually occurs during induction or reinduction chemotherapy.[16,22,23] A series of 605 patients who received autologous bone marrow transplant (BMT) with cyclophosphamide and total-body radiation therapy (as conditioning) were followed for a median of 10 years. The incidence of a second malignancy was 21%, and 10% of those malignancies were solid tumors.[24]
A study of young women who received autologous BMT reported successful pregnancies with children born free of congenital abnormalities.[25] Late-occurring venous thromboembolism can occur after allogeneic or autologous BMT.[26]
Some patients have osteopenia or osteoporosis at the start of therapy; bone density may worsen after therapy for lymphoma.[27]
Long-term impaired immune health was evaluated in a retrospective cohort study of 21,690 survivors of diffuse large B-cell lymphoma from the California Cancer Registry. Elevated incidence rate ratios were found up to 10 years later for pneumonia (10.8-fold), meningitis (5.3-fold), immunoglobulin deficiency (17.6-fold), and autoimmune cytopenias (12-fold).[28] Similarly, there are impaired humoral responses to COVID-19 virus vaccination in patients with lymphoma who receive B-cell–directed therapies.[29,30]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
American Cancer Society: Types of B-cell Lymphoma. American Cancer Society, 2019. Available online. Last accessed February 7, 2025.
Tan D, Horning SJ, Hoppe RT, et al.: Improvements in observed and relative survival in follicular grade 1-2 lymphoma during 4 decades: the Stanford University experience. Blood 122 (6): 981-7, 2013. [PUBMED Abstract]
Bastion Y, Sebban C, Berger F, et al.: Incidence, predictive factors, and outcome of lymphoma transformation in follicular lymphoma patients. J Clin Oncol 15 (4): 1587-94, 1997. [PUBMED Abstract]
Yuen AR, Kamel OW, Halpern J, et al.: Long-term survival after histologic transformation of low-grade follicular lymphoma. J Clin Oncol 13 (7): 1726-33, 1995. [PUBMED Abstract]
Cabanillas F, Velasquez WS, Hagemeister FB, et al.: Clinical, biologic, and histologic features of late relapses in diffuse large cell lymphoma. Blood 79 (4): 1024-8, 1992. [PUBMED Abstract]
Haddy TB, Adde MA, McCalla J, et al.: Late effects in long-term survivors of high-grade non-Hodgkin’s lymphomas. J Clin Oncol 16 (6): 2070-9, 1998. [PUBMED Abstract]
Travis LB, Curtis RE, Glimelius B, et al.: Second cancers among long-term survivors of non-Hodgkin’s lymphoma. J Natl Cancer Inst 85 (23): 1932-7, 1993. [PUBMED Abstract]
Mudie NY, Swerdlow AJ, Higgins CD, et al.: Risk of second malignancy after non-Hodgkin’s lymphoma: a British Cohort Study. J Clin Oncol 24 (10): 1568-74, 2006. [PUBMED Abstract]
Hemminki K, Lenner P, Sundquist J, et al.: Risk of subsequent solid tumors after non-Hodgkin’s lymphoma: effect of diagnostic age and time since diagnosis. J Clin Oncol 26 (11): 1850-7, 2008. [PUBMED Abstract]
Major A, Smith DE, Ghosh D, et al.: Risk and subtypes of secondary primary malignancies in diffuse large B-cell lymphoma survivors change over time based on stage at diagnosis. Cancer 126 (1): 189-201, 2020. [PUBMED Abstract]
Moser EC, Noordijk EM, van Leeuwen FE, et al.: Long-term risk of cardiovascular disease after treatment for aggressive non-Hodgkin lymphoma. Blood 107 (7): 2912-9, 2006. [PUBMED Abstract]
Darrington DL, Vose JM, Anderson JR, et al.: Incidence and characterization of secondary myelodysplastic syndrome and acute myelogenous leukemia following high-dose chemoradiotherapy and autologous stem-cell transplantation for lymphoid malignancies. J Clin Oncol 12 (12): 2527-34, 1994. [PUBMED Abstract]
Stone RM, Neuberg D, Soiffer R, et al.: Myelodysplastic syndrome as a late complication following autologous bone marrow transplantation for non-Hodgkin’s lymphoma. J Clin Oncol 12 (12): 2535-42, 1994. [PUBMED Abstract]
Armitage JO, Carbone PP, Connors JM, et al.: Treatment-related myelodysplasia and acute leukemia in non-Hodgkin’s lymphoma patients. J Clin Oncol 21 (5): 897-906, 2003. [PUBMED Abstract]
André M, Mounier N, Leleu X, et al.: Second cancers and late toxicities after treatment of aggressive non-Hodgkin lymphoma with the ACVBP regimen: a GELA cohort study on 2837 patients. Blood 103 (4): 1222-8, 2004. [PUBMED Abstract]
Oddou S, Vey N, Viens P, et al.: Second neoplasms following high-dose chemotherapy and autologous stem cell transplantation for malignant lymphomas: a report of six cases in a cohort of 171 patients from a single institution. Leuk Lymphoma 31 (1-2): 187-94, 1998. [PUBMED Abstract]
Lenz G, Dreyling M, Schiegnitz E, et al.: Moderate increase of secondary hematologic malignancies after myeloablative radiochemotherapy and autologous stem-cell transplantation in patients with indolent lymphoma: results of a prospective randomized trial of the German Low Grade Lymphoma Study Group. J Clin Oncol 22 (24): 4926-33, 2004. [PUBMED Abstract]
McLaughlin P, Estey E, Glassman A, et al.: Myelodysplasia and acute myeloid leukemia following therapy for indolent lymphoma with fludarabine, mitoxantrone, and dexamethasone (FND) plus rituximab and interferon alpha. Blood 105 (12): 4573-5, 2005. [PUBMED Abstract]
Morton LM, Curtis RE, Linet MS, et al.: Second malignancy risks after non-Hodgkin’s lymphoma and chronic lymphocytic leukemia: differences by lymphoma subtype. J Clin Oncol 28 (33): 4935-44, 2010. [PUBMED Abstract]
Mach-Pascual S, Legare RD, Lu D, et al.: Predictive value of clonality assays in patients with non-Hodgkin’s lymphoma undergoing autologous bone marrow transplant: a single institution study. Blood 91 (12): 4496-503, 1998. [PUBMED Abstract]
Lillington DM, Micallef IN, Carpenter E, et al.: Detection of chromosome abnormalities pre-high-dose treatment in patients developing therapy-related myelodysplasia and secondary acute myelogenous leukemia after treatment for non-Hodgkin’s lymphoma. J Clin Oncol 19 (9): 2472-81, 2001. [PUBMED Abstract]
Brown JR, Yeckes H, Friedberg JW, et al.: Increasing incidence of late second malignancies after conditioning with cyclophosphamide and total-body irradiation and autologous bone marrow transplantation for non-Hodgkin’s lymphoma. J Clin Oncol 23 (10): 2208-14, 2005. [PUBMED Abstract]
Jackson GH, Wood A, Taylor PR, et al.: Early high dose chemotherapy intensification with autologous bone marrow transplantation in lymphoma associated with retention of fertility and normal pregnancies in females. Scotland and Newcastle Lymphoma Group, UK. Leuk Lymphoma 28 (1-2): 127-32, 1997. [PUBMED Abstract]
Gangaraju R, Chen Y, Hageman L, et al.: Risk of venous thromboembolism in patients with non-Hodgkin lymphoma surviving blood or marrow transplantation. Cancer 125 (24): 4498-4508, 2019. [PUBMED Abstract]
Westin JR, Thompson MA, Cataldo VD, et al.: Zoledronic acid for prevention of bone loss in patients receiving primary therapy for lymphomas: a prospective, randomized controlled phase III trial. Clin Lymphoma Myeloma Leuk 13 (2): 99-105, 2013. [PUBMED Abstract]
Shree T, Li Q, Glaser SL, et al.: Impaired Immune Health in Survivors of Diffuse Large B-Cell Lymphoma. J Clin Oncol 38 (15): 1664-1675, 2020. [PUBMED Abstract]
Ghione P, Gu JJ, Attwood K, et al.: Impaired humoral responses to COVID-19 vaccination in patients with lymphoma receiving B-cell-directed therapies. Blood 138 (9): 811-814, 2021. [PUBMED Abstract]
Terpos E, Trougakos IP, Gavriatopoulou M, et al.: Low neutralizing antibody responses against SARS-CoV-2 in older patients with myeloma after the first BNT162b2 vaccine dose. Blood 137 (26): 3674-3676, 2021. [PUBMED Abstract]
Cellular Classification of B-Cell Non-Hodgkin Lymphoma
A pathologist should be consulted before a biopsy because some studies require special preparation of tissue (e.g., frozen tissue). Knowledge of cell surface markers and immunoglobulin and T-cell receptor gene rearrangements may help with diagnostic and therapeutic decisions. The clonal excess of light-chain immunoglobulin may differentiate malignant cells from reactive cells. Because the prognosis and the approach to treatment are influenced by histopathology, outside biopsy specimens should be carefully reviewed by a hematopathologist who is experienced in diagnosing lymphomas. Although lymph node biopsies are recommended whenever possible, sometimes immunophenotypic data are sufficient for diagnosis of lymphoma when fine-needle aspiration cytology or core needle biopsy is preferred.[1,2]
Historical Classification Systems
Historically, uniform treatment of patients with non-Hodgkin lymphoma (NHL) has been hampered by the lack of a uniform classification system. In 1982, results of a consensus study were published as the Working Formulation.[3] The Working Formulation combined results from six major classification systems into one classification. This allowed comparison of studies from different institutions and countries. The Rappaport classification, which also follows, is no longer in common use.
Table 1. Historical Classification Systems for Non-Hodgkin Lymphoma (NHL)
A. Small lymphocytic, consistent with chronic lymphocytic leukemia
Diffuse lymphocytic, well-differentiated
B. Follicular, predominantly small-cleaved cell
Nodular lymphocytic, poorly differentiated
C. Follicular, mixed small-cleaved, and large cell
Nodular mixed, lymphocytic, and histiocytic
Intermediate grade
D. Follicular, predominantly large cell
Nodular histiocytic
E. Diffuse small-cleaved cell
Diffuse lymphocytic, poorly differentiated
F. Diffuse mixed, small and large cell
Diffuse mixed, lymphocytic, and histiocytic
G. Diffuse, large cell, cleaved, or noncleaved cell
Diffuse histiocytic
High grade
H. Immunoblastic, large cell
Diffuse histiocytic
I. Lymphoblastic, convoluted, or nonconvoluted cell
Diffuse lymphoblastic
J. Small noncleaved-cell, Burkitt, or non-Burkitt
Diffuse undifferentiated Burkitt or non-Burkitt
Current Classification Systems
As the histopathological diagnosis of NHL has become more sophisticated with the use of immunologic and genetic techniques, a number of new pathological entities have been described.[4] In addition, the understanding and treatment of many of the previously described pathological subtypes have changed. As a result, the Working Formulation has become outdated and less useful to clinicians and pathologists. European and American pathologists have proposed a new classification, the Revised European American Lymphoma (REAL) classification.[5–8] Since 1995, members of the European and American Hematopathology societies have been collaborating on a new World Health Organization (WHO) classification, which represents an updated version of the REAL system.[9,10]
Updated REAL/WHO classification
The World Health Organization (WHO) modification of the Revised European American Lymphoma (REAL) classification recognizes three major categories of lymphoid malignancies based on morphology and cell lineage: B-cell neoplasms, T-cell/natural killer (NK)-cell neoplasms, and Hodgkin lymphoma (HL). Both lymphomas and lymphoid leukemias are included in this classification because both solid and circulating phases are present in many lymphoid neoplasms and distinction between them is artificial. For example, B-cell chronic lymphocytic leukemia (CLL) and B-cell small lymphocytic lymphoma are simply different manifestations of the same neoplasm, as are lymphoblastic lymphomas and acute lymphocytic leukemias. Within the B-cell and T-cell categories, two subdivisions are recognized: precursor neoplasms, which correspond to the earliest stages of differentiation, and more mature differentiated neoplasms.[9,10]
Zeppa P, Marino G, Troncone G, et al.: Fine-needle cytology and flow cytometry immunophenotyping and subclassification of non-Hodgkin lymphoma: a critical review of 307 cases with technical suggestions. Cancer 102 (1): 55-65, 2004. [PUBMED Abstract]
Young NA, Al-Saleem T: Diagnosis of lymphoma by fine-needle aspiration cytology using the revised European-American classification of lymphoid neoplasms. Cancer 87 (6): 325-45, 1999. [PUBMED Abstract]
National Cancer Institute sponsored study of classifications of non-Hodgkin’s lymphomas: summary and description of a working formulation for clinical usage. The Non-Hodgkin’s Lymphoma Pathologic Classification Project. Cancer 49 (10): 2112-35, 1982. [PUBMED Abstract]
Pugh WC: Is the working formulation adequate for the classification of the low grade lymphomas? Leuk Lymphoma 10 (Suppl 1): 1-8, 1993.
Harris NL, Jaffe ES, Stein H, et al.: A revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group. Blood 84 (5): 1361-92, 1994. [PUBMED Abstract]
Pittaluga S, Bijnens L, Teodorovic I, et al.: Clinical analysis of 670 cases in two trials of the European Organization for the Research and Treatment of Cancer Lymphoma Cooperative Group subtyped according to the Revised European-American Classification of Lymphoid Neoplasms: a comparison with the Working Formulation. Blood 87 (10): 4358-67, 1996. [PUBMED Abstract]
Armitage JO, Weisenburger DD: New approach to classifying non-Hodgkin’s lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin’s Lymphoma Classification Project. J Clin Oncol 16 (8): 2780-95, 1998. [PUBMED Abstract]
A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. The Non-Hodgkin’s Lymphoma Classification Project. Blood 89 (11): 3909-18, 1997. [PUBMED Abstract]
Pileri SA, Milani M, Fraternali-Orcioni G, et al.: From the R.E.A.L. Classification to the upcoming WHO scheme: a step toward universal categorization of lymphoma entities? Ann Oncol 9 (6): 607-12, 1998. [PUBMED Abstract]
Society for Hematopathology Program: Society for Hematopathology Program. Am J Surg Pathol 21 (1): 114-121, 1997.
Stage Information for Aggressive B-Cell Non-Hodgkin Lymphoma
Stage is important in selecting a treatment for patients with non-Hodgkin lymphoma (NHL). Chest and abdominal computed tomography (CT) scans are usually part of the staging evaluation for all patients with lymphoma. The staging system for NHL is similar to the staging system used for Hodgkin lymphoma (HL).
It is common for patients with NHL to have involvement of the following sites:
Noncontiguous lymph nodes.
Waldeyer ring.
Epitrochlear nodes.
Gastrointestinal tract.
Extranodal presentations. (A single extranodal site is occasionally the only site of involvement in patients with diffuse lymphoma.)
Bone marrow.
Liver (especially common in patients with low-grade lymphomas).
Cytological examination of cerebrospinal fluid may be positive in patients with aggressive NHL. Involvement of hilar and mediastinal lymph nodes is less common than in HL. Mediastinal adenopathy, however, is a prominent feature of lymphoblastic lymphoma and primary mediastinal B-cell lymphoma, entities primarily found in young adults.
Most patients with NHL present with advanced (stage III or stage IV) disease often identified by CT scans or biopsies of the bone marrow and other accessible sites of involvement. In a retrospective review of over 32,000 cases of lymphoma in France, up to 40% of diagnoses were made by core needle biopsy, and 60% were made by excisional biopsy.[1] After expert review, core needle biopsy provided a definite diagnosis in 92.3% of cases; excisional biopsy provided a definite diagnosis in 98.1% of cases (P < .0001). Laparoscopic biopsy or laparotomy is not required for staging but rarely may be necessary to establish a diagnosis or histological type.[2]
Positron emission tomography (PET) with fluorine F 18-fludeoxyglucose can be used for initial staging. It can also be used for follow-up after therapy as a supplement to CT scanning.[3] Multiple studies have demonstrated that interim PET scans after two to four cycles of therapy do not provide reliable prognostic information. A large cooperative group trial (ECOG-E344 [NCT00274924]) reported problems with interobserver reproducibility. Two prospective trials and one meta-analysis showed no differences in outcomes between PET-negative and PET-positive/biopsy-negative patients.[4–7]
In a retrospective study of 130 patients with diffuse large B-cell lymphoma, PET scanning identified all clinically important marrow involvement from lymphoma, and bone marrow biopsy did not upstage any patient’s lymphoma.[8] A retrospective study of 580 patients with follicular lymphoma from seven National Cancer Institute–sponsored trials showed no improvement in assessing response to therapy when bone marrow biopsy was added to radiological imaging.[9] The workup of NHL should include bone marrow biopsy when management would change (e.g., determining limited stage vs. advanced stage) or when evaluating cytopenias.
For patients with follicular lymphoma, a positive PET result after therapy has a worse prognosis; however, it is unclear whether a positive PET result is predictive when further or different therapy is implemented.[10]
Staging Subclassification System
Lugano classification
The American Joint Committee on Cancer (AJCC) has adopted the Lugano classification to evaluate and stage lymphoma.[11] The Lugano classification system replaces the Ann Arbor classification system, which was adopted in 1971 at the Ann Arbor Conference,[12] with some modifications 18 years later from the Cotswolds meeting.[13,14]
Table 2. Lugano Classification for Hodgkin and Non-Hodgkin Lymphomaa
Stage
Stage Description
Illustration
CSF = cerebrospinal fluid; CT = computed tomography; DLBCL = diffuse large B-cell lymphoma; NHL = non-Hodgkin lymphoma.
aHodgkin and Non-Hodgkin Lymphomas. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 937–58.
bStage II bulky may be considered either early or advanced stage based on lymphoma histology and prognostic factors.
cThe definition of disease bulk varies according to lymphoma histology. In the Lugano classification, bulk ln Hodgkin lymphoma is defined as a mass greater than one-third of the thoracic diameter on CT of the chest or a mass >10 cm. For NHL, the recommended definitions of bulk vary by lymphoma histology. In follicular lymphoma, 6 cm has been suggested based on the Follicular Lymphoma International Prognostic Index-2 and its validation. In DLBCL, cutoffs ranging from 5 cm to 10 cm have been used, although 10 cm is recommended.
Limited stage
I
Involvement of a single lymphatic site (i.e., nodal region, Waldeyer’s ring, thymus, or spleen).
Diffuse or disseminated involvement of one or more extralymphatic organs, with or without associated lymph node involvement; or noncontiguous extralymphatic organ involvement in conjunction with nodal stage II disease; or any extralymphatic organ involvement in nodal stage III disease. Stage IV includes any involvement of the CSF, bone marrow, liver, or multiple lung lesions (other than by direct extension in stage IIE disease).
Note: Hodgkin lymphoma uses A or B designation with stage group. A/B is no longer used in NHL.
Occasionally, specialized staging systems are used. The physician should be aware of the system used in a specific report.
The E designation is used when extranodal lymphoid malignancies arise in tissues separate from, but near, the major lymphatic aggregates. Stage IV refers to disease that is diffusely spread throughout an extranodal site, such as the liver. If pathological proof of involvement of one or more extralymphatic sites has been documented, the symbol for the site of involvement, followed by a plus sign (+), is listed.
Table 3. Notation to Identify Specific Sites
N = nodes
H = liver
L = lung
M = bone marrow
S = spleen
P = pleura
O = bone
D = skin
Current practice assigns a clinical stage based on the findings of the clinical evaluation and a pathological stage based on the findings from invasive procedures beyond the initial biopsy.
For example, on percutaneous biopsy, a patient with inguinal adenopathy and a positive lymphangiogram without systemic symptoms might have involvement of the liver and bone marrow. The precise stage of such a patient would be clinical stage IIA, pathological stage IVA(H+)(M+).
Several other factors that are not included in the above staging system are important for the staging and prognosis of patients with NHL. These factors include the following:
Age.
Performance status (PS).
Tumor size.
Lactate dehydrogenase (LDH) values.
The number of extranodal sites.
The National Comprehensive Cancer Network International Prognostic Index (IPI) for aggressive NHL (diffuse large cell lymphoma) identifies the following five significant risk factors prognostic of overall survival (OS) and their associated risk scores:[15]
Age.
<40 years: 0.
41–60 years: 1.
61–75 years: 2.
>75 years: 3.
Stage III/IV: 1.
Performance status (PS) 2/3/4: 1.
Serum lactate dehydrogenase (LDH).
Normalized: 0.
>1x–3x: 1.
>3x: 2.
Number of extranodal sites ≥2: 1.
Risk scores:
Low (0 or 1): 5-year OS rate, 96%; progression-free survival (PFS) rate, 91%.
Low intermediate (2 or 3): 5-year OS rate, 82%; PFS rate, 74%.
High intermediate (4 or 5): 5-year OS rate, 64%; PFS rate, 51%.
High (>6): 5-year OS rate, 33%; PFS rate, 30%.
Age-adjusted and stage-adjusted modifications of this IPI are used for younger patients with localized disease.[16] Shorter intervals of time between diagnosis and treatment appear to be a surrogate for poor prognostic biological factors.[17]
The BCL2 gene and rearrangement of the MYC gene or dual overexpression of the MYC gene, or both, confer a particularly poor prognosis.[18,19] Patients at high risk of relapse may benefit from consolidation therapy or other approaches under clinical evaluation.[20] Molecular profiles of gene expression using DNA microarrays may help to stratify patients in the future for therapies directed at specific targets and to better predict survival after standard chemotherapy.[21]
References
Syrykh C, Chaouat C, Poullot E, et al.: Lymph node excisions provide more precise lymphoma diagnoses than core biopsies: a French Lymphopath network survey. Blood 140 (24): 2573-2583, 2022. [PUBMED Abstract]
Mann GB, Conlon KC, LaQuaglia M, et al.: Emerging role of laparoscopy in the diagnosis of lymphoma. J Clin Oncol 16 (5): 1909-15, 1998. [PUBMED Abstract]
Barrington SF, Mikhaeel NG, Kostakoglu L, et al.: Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J Clin Oncol 32 (27): 3048-58, 2014. [PUBMED Abstract]
Horning SJ, Juweid ME, Schöder H, et al.: Interim positron emission tomography scans in diffuse large B-cell lymphoma: an independent expert nuclear medicine evaluation of the Eastern Cooperative Oncology Group E3404 study. Blood 115 (4): 775-7; quiz 918, 2010. [PUBMED Abstract]
Moskowitz CH, Schöder H, Teruya-Feldstein J, et al.: Risk-adapted dose-dense immunochemotherapy determined by interim FDG-PET in Advanced-stage diffuse large B-Cell lymphoma. J Clin Oncol 28 (11): 1896-903, 2010. [PUBMED Abstract]
Pregno P, Chiappella A, Bellò M, et al.: Interim 18-FDG-PET/CT failed to predict the outcome in diffuse large B-cell lymphoma patients treated at the diagnosis with rituximab-CHOP. Blood 119 (9): 2066-73, 2012. [PUBMED Abstract]
Sun N, Zhao J, Qiao W, et al.: Predictive value of interim PET/CT in DLBCL treated with R-CHOP: meta-analysis. Biomed Res Int 2015: 648572, 2015. [PUBMED Abstract]
Khan AB, Barrington SF, Mikhaeel NG, et al.: PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood 122 (1): 61-7, 2013. [PUBMED Abstract]
Rutherford SC, Yin J, Pederson L, et al.: Relevance of Bone Marrow Biopsies for Response Assessment in US National Cancer Institute National Clinical Trials Network Follicular Lymphoma Clinical Trials. J Clin Oncol 41 (2): 336-342, 2023. [PUBMED Abstract]
Pyo J, Won Kim K, Jacene HA, et al.: End-therapy positron emission tomography for treatment response assessment in follicular lymphoma: a systematic review and meta-analysis. Clin Cancer Res 19 (23): 6566-77, 2013. [PUBMED Abstract]
Hodgkin and non-Hodgkin lymphoma. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp. 937–58.
Carbone PP, Kaplan HS, Musshoff K, et al.: Report of the Committee on Hodgkin’s Disease Staging Classification. Cancer Res 31 (11): 1860-1, 1971. [PUBMED Abstract]
Lister TA, Crowther D, Sutcliffe SB, et al.: Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin’s disease: Cotswolds meeting. J Clin Oncol 7 (11): 1630-6, 1989. [PUBMED Abstract]
National Cancer Institute sponsored study of classifications of non-Hodgkin’s lymphomas: summary and description of a working formulation for clinical usage. The Non-Hodgkin’s Lymphoma Pathologic Classification Project. Cancer 49 (10): 2112-35, 1982. [PUBMED Abstract]
Zhou Z, Sehn LH, Rademaker AW, et al.: An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 123 (6): 837-42, 2014. [PUBMED Abstract]
Møller MB, Christensen BE, Pedersen NT: Prognosis of localized diffuse large B-cell lymphoma in younger patients. Cancer 98 (3): 516-21, 2003. [PUBMED Abstract]
Maurer MJ, Ghesquières H, Link BK, et al.: Diagnosis-to-Treatment Interval Is an Important Clinical Factor in Newly Diagnosed Diffuse Large B-Cell Lymphoma and Has Implication for Bias in Clinical Trials. J Clin Oncol 36 (16): 1603-1610, 2018. [PUBMED Abstract]
Scott DW, King RL, Staiger AM, et al.: High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with diffuse large B-cell lymphoma morphology. Blood 131 (18): 2060-2064, 2018. [PUBMED Abstract]
Horn H, Ziepert M, Becher C, et al.: MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 121 (12): 2253-63, 2013. [PUBMED Abstract]
A predictive model for aggressive non-Hodgkin’s lymphoma. The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. N Engl J Med 329 (14): 987-94, 1993. [PUBMED Abstract]
Sha C, Barrans S, Cucco F, et al.: Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J Clin Oncol 37 (3): 202-212, 2019. [PUBMED Abstract]
Aggressive B-Cell Non-Hodgkin Lymphoma
Aggressive B-cell non-Hodgkin lymphoma (NHL) includes the following subtypes:
Diffuse large B-cell lymphoma.
Primary mediastinal large B-cell lymphoma.
Intravascular large B-cell lymphoma (intravascular lymphomatosis).
Diffuse large B-cell lymphoma (DLBCL) is the most common type of NHL and makes up 30% of newly diagnosed cases.[1] Most patients present with rapidly enlarging masses, often with both local and systemic symptoms (designated B symptoms with fever, recurrent night sweats, or weight loss). For more information about weight loss, see Nutrition in Cancer Care.
Some cases of large B-cell lymphoma have a prominent background of reactive T cells and histiocytes, and is so-called T-cell/histiocyte-rich large B-cell lymphoma. This subtype of large cell lymphoma has frequent liver, spleen, and bone marrow involvement; however, the outcome is equivalent to that of similarly staged patients with DLBCL.[2–4] At diagnosis, some patients with DLBCL have a concomitant indolent small B-cell component. While overall survival (OS) appears similar to de novo DLBCL after multidrug chemotherapy, there is a higher risk of indolent relapse.[5]
Prognosis
For most patients, localized disease can be cured with combined-modality therapy or combination chemotherapy alone, typically R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).[6] Among patients with advanced-stage disease, 50% are cured with doxorubicin-based combination chemotherapy and rituximab, typically Pola-R-CHP (polatuzumab, rituximab, cyclophosphamide, doxorubicin, and prednisone) or R-CHOP.[7–10]
The BCL2 gene and rearrangement of the MYC gene or dual overexpression of the MYC gene, or both, confer a particularly poor prognosis.[11–13] Dose-intensive therapies, infusional therapies, and stem cell transplant (SCT) consolidation are being explored in this high-risk group.[14–17]
In a retrospective review of 117 patients with relapsed or refractory DLBCL who underwent autologous SCT, the 4-year OS rate was 25% for patients with double-hit lymphomas (rearrangement of BCL2 and MYC), 61% for patients with double-expressor lymphomas (no rearrangement, but increased expression of BCL2 and MYC), and 70% for patients without these features.[18]
Molecular profiles of gene expression using DNA microarrays may help to stratify patients in the future for therapies directed at specific targets and to better predict survival after standard chemotherapy.[19] For example, true ALK-positive large B-cell lymphomas are extremely rare, and they do not respond well to conventional R-CHOP therapy. Anecdotal responses to ALK inhibitors like lorlatinib or alectinib have been reported.[20][Level of evidence C3] Coexpression of CD20 and CD30 may define a subgroup of patients with DLBCL with a unique molecular signature and a more favorable prognosis. Patients in this subgroup may be treated with an anti-CD30–specific therapy, such as brentuximab vedotin.[21] Patients with DLBCL who are event-free after 2 years have a subsequent OS equivalent to that of the age- and sex-matched general population.[22]
Patients at high risk for central nervous system (CNS) relapse may be candidates for prophylaxis. For more information, see the CNS Prophylaxis section in the Treatment of Aggressive, Noncontiguous Stage II/III/IV B-Cell Non-Hodgkin Lymphoma section.
Primary Mediastinal Large B-Cell Lymphoma
Primary mediastinal (thymic) large B-cell lymphoma (PMBCL) is a subset of DLBCL with molecular characteristics that are most similar to nodular-sclerosing Hodgkin lymphoma (HL).[23] Mediastinal lymphomas with features intermediate between primary mediastinal B-cell lymphoma and nodular-sclerosing HL are called mediastinal gray-zone lymphomas.[24,25] Patients are usually female and young (median age, 30–40 years). Patients present with a locally invasive anterior mediastinal mass that may cause respiratory symptoms or superior vena cava syndrome.
Prognosis and therapy are the same as for other comparably staged patients with DLBCL. Uncontrolled phase II studies using dose-adjusted R-EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin plus rituximab) or R-CHOP showed high cure rates while avoiding any mediastinal radiation.[25–31][Level of evidence C1] These results suggest that patients who receive R-CHOP–based regimens may avoid the serious long-term complications of radiation therapy when given with chemotherapy. Posttreatment fluorine F 18-fludeoxyglucose (18F-FDG) positron emission tomography–computed tomography (PET-CT) scans are controversial. It remains unclear if PET scans can reliably identify patients who can undergo or omit radiation therapy consolidation.[26,32–34]
A retrospective review of 109 patients with PMBCL showed that 63% had a negative end-of-treatment PET-CT (EOT-PET-CT) (Deauville score 1–3).[35] No radiation therapy was offered and the 5-year time-to-progression rate (similar to disease-free survival, but restricted to lymphoma relapse) was 90% (95% confidence interval [CI], 74%–95%), and the 5-year OS rate was 97% (95% CI, 88%–99%).[35][Level of evidence C3] Patients with a positive EOT-PET-CT received radiation therapy consolidation. It is unclear from this study whether those patients might have done just as well without radiation therapy. Clinicians may monitor patients with Deauville 4 scores on EOT-PET-CT scans for improvement over time, as an alternative to giving radiation therapy. However, this approach has not been studied in a clinical trial.
Because PMBCL is characterized by high expression of programmed death-ligand 1 and variable expression of CD30, a phase II study evaluated nivolumab plus brentuximab vedotin in 30 patients with relapsed disease. With a median follow-up of 11.1 months, the objective response rate was 73% (95% CI, 54%−88%).[36][Level of evidence C3] Similarly, a phase II trial of pembrolizumab in 53 patients with relapsed or refractory disease showed an objective response rate of 41.5%. With a median follow-up of 48.7 months, the 4-year progression-free survival (PFS) rate was 33.0% and the 4-year OS rate was 45.3%.[37][Level of evidence C3] Among the 11 patients who achieved a complete response, all remained in complete response at the time of the final analysis.
Among those who had received two prior lines of therapy, more than one-half of patients who received chimeric antigen receptor (CAR) T-cell therapy with lisocabtagene maraleucel had a disease response.[38][Level of evidence C3]
Intravascular Large B-Cell Lymphoma (Intravascular Lymphomatosis)
Intravascular lymphomatosis is characterized by large cell lymphoma confined to the intravascular lumen. The brain, kidneys, lungs, and skin are the organs most likely to be affected by intravascular lymphomatosis.
With the use of aggressive R-CHOP–based combination chemotherapy, as is used in DLBCL, the prognosis is similar to that of conventional stage IV DLBCL.[39–41]
Follicular Lymphoma (Grade 3b)
Prognosis
The natural history of follicular large cell lymphoma remains controversial.[42] While there is agreement about the significant number of long-term disease-free survivors with early-stage disease, the potential for cure in patients with advanced disease (stage III or stage IV) remains uncertain. Some groups report a continuous relapse rate similar to the other follicular lymphomas (a pattern of indolent lymphoma).[43] Other investigators report a plateau in freedom from progression at levels expected for an aggressive lymphoma (40% at 10 years).[44,45] This discrepancy may be caused by variations in histological classification between institutions and the rarity of patients with follicular large cell lymphoma. A retrospective review of 252 patients, all treated with anthracycline-containing combination chemotherapy, showed that patients with more than 50% diffuse components on biopsy had a worse OS than other patients with follicular large cell lymphoma.[46]
Therapeutic approaches
Treatment of follicular large cell lymphoma is more similar to the treatment of aggressive NHL than it is to the treatment of indolent NHL. In support of this approach, treatment with high-dose chemotherapy and autologous hematopoietic peripheral SCT shows the same curative potential in patients with follicular large cell lymphoma who relapse as it does in patients with diffuse large cell lymphoma who relapse.[47][Level of evidence C1]
Among patients who had received two prior lines of therapy, more than one-half who received CAR T-cell therapy with lisocabtagene maraleucel had a disease response.[38][Level of evidence C3]
Burkitt Lymphoma/Diffuse Small Noncleaved-Cell Lymphoma
Burkitt lymphoma/diffuse small noncleaved-cell lymphoma typically involves younger patients and represents the most common type of pediatric NHL.[48] These types of aggressive extranodal B-cell lymphomas are characterized by translocation and deregulation of the MYC gene on chromosome 8.[49] A subgroup of patients with dual translocation of MYC and BCL2 appear to have an extremely poor outcome despite aggressive therapy (median OS, 5 months).[50][Level of evidence C1]
In some patients with larger B cells, there is morphological overlap with DLBCL. These Burkitt-like large cell lymphomas show MYC deregulation, extremely high proliferation rates, and a gene-expression profile as expected for classic Burkitt lymphoma.[51–53] Endemic cases, usually from Africa, involve the facial bones or jaws of children, mostly containing Epstein-Barr virus (EBV) genomes. Sporadic cases usually involve the gastrointestinal system, ovaries, or kidneys. Patients present with rapidly growing masses and a very high lactate dehydrogenase (LDH) level but are potentially curable with intensive doxorubicin-based combination chemotherapy.
Therapeutic approaches
Treatment of Burkitt lymphoma/diffuse small noncleaved-cell lymphoma involves aggressive multidrug regimens in combination with rituximab, similar to those used for the advanced-stage aggressive lymphomas (DLBCL).[54–57] Aggressive combination chemotherapy, which is modeled after that used in childhood Burkitt lymphoma, has been successful for adult patients with more than 60% of advanced-stage patients free of disease at 5 years.[58–61] Adverse prognostic factors include bulky abdominal disease and a high serum LDH level. Patients with Burkitt lymphoma have a 20% to 30% lifetime risk of CNS involvement. Prophylaxis with intrathecal chemotherapy is required as part of induction therapy.[62] Patients with HIV-associated Burkitt lymphoma also benefit from less-toxic modification of the aggressive multidrug regimens in combination with rituximab.[63][Level of evidence C3] For more information, see Primary Central Nervous System Lymphoma Treatment and AIDS-Related Lymphoma Treatment.
B-Cell Lymphoblastic Lymphoma
B-cell lymphoblastic lymphoma (precursor T-cell) is a very aggressive form of NHL. Treatment is usually modeled after that for acute lymphoblastic leukemia. Intensive combination chemotherapy with or without bone marrow transplant is the standard treatment for this aggressive histological type of NHL.[64–66] Radiation therapy is sometimes given to areas of bulky tumor masses. Because these forms of NHL tend to progress quickly, combination chemotherapy is instituted rapidly once the diagnosis is confirmed. Careful review of the pathological specimens, bone marrow aspirate, biopsy specimen, cerebrospinal fluid cytology, and lymphocyte marker constitute the most important aspects of the pretreatment staging workup. For more information, see Acute Lymphoblastic Leukemia Treatment.
Primary Effusion Lymphoma
Primary effusion lymphoma presents exclusively or mainly in the pleural, pericardial, or abdominal cavities in the absence of an identifiable tumor mass.[67] Patients are usually HIV seropositive, and the tumor usually contains Kaposi sarcoma–associated herpes virus/human herpes virus 8.[68]
Prognosis
The prognosis of primary effusion lymphoma is extremely poor.
Therapeutic approaches
Therapy is usually modeled after the treatment of comparably staged diffuse large cell lymphomas.
Plasmablastic Lymphoma
Plasmablastic lymphoma is most often seen in patients with HIV infection and is characterized by CD20-negative large B cells with plasmacytic features. This type of lymphoma has a very aggressive clinical course, including poor responses and short remissions with standard chemotherapy.[69] Anecdotal reports suggest using aggressive chemotherapy for Burkitt or lymphoblastic lymphoma, followed by SCT consolidation in responding patients, when feasible.[69–71]
Patients who undergo a transplant of the heart, lung, liver, kidney, or pancreas usually require lifelong immunosuppression. This may result in posttransplant lymphoproliferative disorder (PTLD) in 1% to 3% of recipients, which appears as an aggressive lymphoma.[72] Pathologists can distinguish a polyclonal B-cell hyperplasia from a monoclonal B-cell lymphoma; both are almost always associated with EBV.[73]
Prognosis
Poor performance status, grafted organ involvement, high International Prognostic Index, elevated LDH, and multiple sites of disease are poor prognostic factors for PTLD.[74,75]
Therapeutic options
In some cases, withdrawal of immunosuppression results in eradication of the lymphoma.[76,77] When this is unsuccessful or not feasible, a course of rituximab may be considered because it has shown durable remissions in approximately 60% of patients and a favorable toxicity profile.[76,78,79] If these measures fail, doxorubicin-based combination chemotherapy (R-CHOP) is recommended, although some patients can avoid cytotoxic therapy.[79,80] Localized presentations can be controlled with surgery or radiation therapy alone. These localized mass lesions, which may grow over a period of months, are often phenotypically polyclonal and tend to occur within weeks or a few months after transplant.[73] Multifocal, rapidly progressive disease occurs late after transplant (>1 year) and is usually phenotypically monoclonal and associated with EBV.[81] These patients may have durable remissions using standard chemotherapy regimens for aggressive lymphoma.[81–83] Instances of EBV-negative PTLD occur even later (median, 5 years posttransplant) and have a worse prognosis; R-CHOP can be given directly in this circumstance.[84] A sustained clinical response in patients with chemotherapy-refractory disease was attained using an immunotoxin (anti-CD22 B-cell surface antigen antibody linked with ricin, a plant toxin).[85] An anti-interleukin-6 monoclonal antibody is also under clinical evaluation.[86]
Lymphomatoid Granulomatosis
Lymphomatoid granulomatosis is an EBV-positive large B-cell lymphoma with a predominant T-cell background.[87,88] The histology shows association with angioinvasion and vasculitis, usually manifesting as pulmonary lesions or paranasal sinus involvement.
Patients are managed like others with diffuse large cell lymphoma and require doxorubicin-based combination chemotherapy.
References
Sehn LH, Salles G: Diffuse Large B-Cell Lymphoma. N Engl J Med 384 (9): 842-858, 2021. [PUBMED Abstract]
Delabie J, Vandenberghe E, Kennes C, et al.: Histiocyte-rich B-cell lymphoma. A distinct clinicopathologic entity possibly related to lymphocyte predominant Hodgkin’s disease, paragranuloma subtype. Am J Surg Pathol 16 (1): 37-48, 1992. [PUBMED Abstract]
Achten R, Verhoef G, Vanuytsel L, et al.: T-cell/histiocyte-rich large B-cell lymphoma: a distinct clinicopathologic entity. J Clin Oncol 20 (5): 1269-77, 2002. [PUBMED Abstract]
Bouabdallah R, Mounier N, Guettier C, et al.: T-cell/histiocyte-rich large B-cell lymphomas and classical diffuse large B-cell lymphomas have similar outcome after chemotherapy: a matched-control analysis. J Clin Oncol 21 (7): 1271-7, 2003. [PUBMED Abstract]
Ghesquières H, Berger F, Felman P, et al.: Clinicopathologic characteristics and outcome of diffuse large B-cell lymphomas presenting with an associated low-grade component at diagnosis. J Clin Oncol 24 (33): 5234-41, 2006. [PUBMED Abstract]
Miller TP, Dahlberg S, Cassady JR, et al.: Chemotherapy alone compared with chemotherapy plus radiotherapy for localized intermediate- and high-grade non-Hodgkin’s lymphoma. N Engl J Med 339 (1): 21-6, 1998. [PUBMED Abstract]
Coiffier B, Lepage E, Briere J, et al.: CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med 346 (4): 235-42, 2002. [PUBMED Abstract]
Habermann TM, Weller EA, Morrison VA, et al.: Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol 24 (19): 3121-7, 2006. [PUBMED Abstract]
Tilly H, Morschhauser F, Sehn LH, et al.: Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N Engl J Med 386 (4): 351-363, 2022. [PUBMED Abstract]
Scott DW, King RL, Staiger AM, et al.: High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with diffuse large B-cell lymphoma morphology. Blood 131 (18): 2060-2064, 2018. [PUBMED Abstract]
Horn H, Ziepert M, Becher C, et al.: MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 121 (12): 2253-63, 2013. [PUBMED Abstract]
Staiger AM, Ziepert M, Horn H, et al.: Clinical Impact of the Cell-of-Origin Classification and the MYC/ BCL2 Dual Expresser Status in Diffuse Large B-Cell Lymphoma Treated Within Prospective Clinical Trials of the German High-Grade Non-Hodgkin’s Lymphoma Study Group. J Clin Oncol 35 (22): 2515-2526, 2017. [PUBMED Abstract]
Howlett C, Snedecor SJ, Landsburg DJ, et al.: Front-line, dose-escalated immunochemotherapy is associated with a significant progression-free survival advantage in patients with double-hit lymphomas: a systematic review and meta-analysis. Br J Haematol 170 (4): 504-14, 2015. [PUBMED Abstract]
Sesques P, Johnson NA: Approach to the diagnosis and treatment of high-grade B-cell lymphomas with MYC and BCL2 and/or BCL6 rearrangements. Blood 129 (3): 280-288, 2017. [PUBMED Abstract]
Landsburg DJ, Falkiewicz MK, Maly J, et al.: Outcomes of Patients With Double-Hit Lymphoma Who Achieve First Complete Remission. J Clin Oncol 35 (20): 2260-2267, 2017. [PUBMED Abstract]
Canellos GP: CHOP may have been part of the beginning but certainly not the end: issues in risk-related therapy of large-cell lymphoma. J Clin Oncol 15 (5): 1713-6, 1997. [PUBMED Abstract]
Herrera AF, Mei M, Low L, et al.: Relapsed or Refractory Double-Expressor and Double-Hit Lymphomas Have Inferior Progression-Free Survival After Autologous Stem-Cell Transplantation. J Clin Oncol 35 (1): 24-31, 2017. [PUBMED Abstract]
Sha C, Barrans S, Cucco F, et al.: Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J Clin Oncol 37 (3): 202-212, 2019. [PUBMED Abstract]
Soumerai JD, Rosenthal A, Harkins S, et al.: Next-generation ALK inhibitors are highly active in ALK-positive large B-cell lymphoma. Blood 140 (16): 1822-1826, 2022. [PUBMED Abstract]
Hu S, Xu-Monette ZY, Balasubramanyam A, et al.: CD30 expression defines a novel subgroup of diffuse large B-cell lymphoma with favorable prognosis and distinct gene expression signature: a report from the International DLBCL Rituximab-CHOP Consortium Program Study. Blood 121 (14): 2715-24, 2013. [PUBMED Abstract]
Maurer MJ, Ghesquières H, Jais JP, et al.: Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J Clin Oncol 32 (10): 1066-73, 2014. [PUBMED Abstract]
Savage KJ: Primary mediastinal large B-cell lymphoma. Blood 140 (9): 955-970, 2022. [PUBMED Abstract]
van Besien K, Kelta M, Bahaguna P: Primary mediastinal B-cell lymphoma: a review of pathology and management. J Clin Oncol 19 (6): 1855-64, 2001. [PUBMED Abstract]
Dunleavy K, Wilson WH: Primary mediastinal B-cell lymphoma and mediastinal gray zone lymphoma: do they require a unique therapeutic approach? Blood 125 (1): 33-9, 2015. [PUBMED Abstract]
Dunleavy K, Pittaluga S, Maeda LS, et al.: Dose-adjusted EPOCH-rituximab therapy in primary mediastinal B-cell lymphoma. N Engl J Med 368 (15): 1408-16, 2013. [PUBMED Abstract]
Savage KJ, Yenson PR, Shenkier T, et al.: The outcome of primary mediastinal large B-cell lymphoma in the R-CHOP treatment era. [Abstract] Blood 120 (21): A-303, 2012.
Vassilakopoulos TP, Pangalis GA, Katsigiannis A, et al.: Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone with or without radiotherapy in primary mediastinal large B-cell lymphoma: the emerging standard of care. Oncologist 17 (2): 239-49, 2012. [PUBMED Abstract]
Rieger M, Osterborg A, Pettengell R, et al.: Primary mediastinal B-cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: results of the Mabthera International Trial Group study. Ann Oncol 22 (3): 664-70, 2011. [PUBMED Abstract]
Gleeson M, Hawkes EA, Cunningham D, et al.: Rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) in the management of primary mediastinal B-cell lymphoma: a subgroup analysis of the UK NCRI R-CHOP 14 versus 21 trial. Br J Haematol 175 (4): 668-672, 2016. [PUBMED Abstract]
Held G, Thurner L, Poeschel V, et al.: Role of radiotherapy and dose-densification of R-CHOP in primary mediastinal B-cell lymphoma: A subgroup analysis of the unfolder trial of the German Lymphoma Alliance (GLA). [Abstract] J Clin Oncol 38 (Suppl 15): A-8041, 2021.
Martelli M, Ceriani L, Zucca E, et al.: [18F]fluorodeoxyglucose positron emission tomography predicts survival after chemoimmunotherapy for primary mediastinal large B-cell lymphoma: results of the International Extranodal Lymphoma Study Group IELSG-26 Study. J Clin Oncol 32 (17): 1769-75, 2014. [PUBMED Abstract]
Zinzani PL, Broccoli A, Casadei B, et al.: The role of rituximab and positron emission tomography in the treatment of primary mediastinal large B-cell lymphoma: experience on 74 patients. Hematol Oncol 33 (4): 145-50, 2015. [PUBMED Abstract]
Ceriani L, Martelli M, Conconi A, et al.: Prognostic models for primary mediastinal (thymic) B-cell lymphoma derived from 18-FDG PET/CT quantitative parameters in the International Extranodal Lymphoma Study Group (IELSG) 26 study. Br J Haematol 178 (4): 588-591, 2017. [PUBMED Abstract]
Hayden AR, Tonseth P, Lee DG, et al.: Outcome of primary mediastinal large B-cell lymphoma using R-CHOP: impact of a PET-adapted approach. Blood 136 (24): 2803-2811, 2020. [PUBMED Abstract]
Zinzani PL, Santoro A, Gritti G, et al.: Nivolumab Combined With Brentuximab Vedotin for Relapsed/Refractory Primary Mediastinal Large B-Cell Lymphoma: Efficacy and Safety From the Phase II CheckMate 436 Study. J Clin Oncol 37 (33): 3081-3089, 2019. [PUBMED Abstract]
Zinzani PL, Thieblemont C, Melnichenko V, et al.: Pembrolizumab in relapsed or refractory primary mediastinal large B-cell lymphoma: final analysis of KEYNOTE-170. Blood 142 (2): 141-145, 2023. [PUBMED Abstract]
Abramson JS, Palomba ML, Gordon LI, et al.: Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet 396 (10254): 839-852, 2020. [PUBMED Abstract]
Shimada K, Matsue K, Yamamoto K, et al.: Retrospective analysis of intravascular large B-cell lymphoma treated with rituximab-containing chemotherapy as reported by the IVL study group in Japan. J Clin Oncol 26 (19): 3189-95, 2008. [PUBMED Abstract]
Ponzoni M, Ferreri AJ, Campo E, et al.: Definition, diagnosis, and management of intravascular large B-cell lymphoma: proposals and perspectives from an international consensus meeting. J Clin Oncol 25 (21): 3168-73, 2007. [PUBMED Abstract]
Shimada K, Yamaguchi M, Atsuta Y, et al.: Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone combined with high-dose methotrexate plus intrathecal chemotherapy for newly diagnosed intravascular large B-cell lymphoma (PRIMEUR-IVL): a multicentre, single-arm, phase 2 trial. Lancet Oncol 21 (4): 593-602, 2020. [PUBMED Abstract]
Longo DL: What’s the deal with follicular lymphomas? J Clin Oncol 11 (2): 202-8, 1993. [PUBMED Abstract]
Anderson JR, Vose JM, Bierman PJ, et al.: Clinical features and prognosis of follicular large-cell lymphoma: a report from the Nebraska Lymphoma Study Group. J Clin Oncol 11 (2): 218-24, 1993. [PUBMED Abstract]
Bartlett NL, Rizeq M, Dorfman RF, et al.: Follicular large-cell lymphoma: intermediate or low grade? J Clin Oncol 12 (7): 1349-57, 1994. [PUBMED Abstract]
Wendum D, Sebban C, Gaulard P, et al.: Follicular large-cell lymphoma treated with intensive chemotherapy: an analysis of 89 cases included in the LNH87 trial and comparison with the outcome of diffuse large B-cell lymphoma. Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol 15 (4): 1654-63, 1997. [PUBMED Abstract]
Hans CP, Weisenburger DD, Vose JM, et al.: A significant diffuse component predicts for inferior survival in grade 3 follicular lymphoma, but cytologic subtypes do not predict survival. Blood 101 (6): 2363-7, 2003. [PUBMED Abstract]
Vose JM, Bierman PJ, Lynch JC, et al.: Effect of follicularity on autologous transplantation for large-cell non-Hodgkin’s lymphoma. J Clin Oncol 16 (3): 844-9, 1998. [PUBMED Abstract]
Blum KA, Lozanski G, Byrd JC: Adult Burkitt leukemia and lymphoma. Blood 104 (10): 3009-20, 2004. [PUBMED Abstract]
Onciu M, Schlette E, Zhou Y, et al.: Secondary chromosomal abnormalities predict outcome in pediatric and adult high-stage Burkitt lymphoma. Cancer 107 (5): 1084-92, 2006. [PUBMED Abstract]
Macpherson N, Lesack D, Klasa R, et al.: Small noncleaved, non-Burkitt’s (Burkit-Like) lymphoma: cytogenetics predict outcome and reflect clinical presentation. J Clin Oncol 17 (5): 1558-67, 1999. [PUBMED Abstract]
Dave SS, Fu K, Wright GW, et al.: Molecular diagnosis of Burkitt’s lymphoma. N Engl J Med 354 (23): 2431-42, 2006. [PUBMED Abstract]
Hummel M, Bentink S, Berger H, et al.: A biologic definition of Burkitt’s lymphoma from transcriptional and genomic profiling. N Engl J Med 354 (23): 2419-30, 2006. [PUBMED Abstract]
Salaverria I, Siebert R: The gray zone between Burkitt’s lymphoma and diffuse large B-cell lymphoma from a genetics perspective. J Clin Oncol 29 (14): 1835-43, 2011. [PUBMED Abstract]
Thomas DA, Faderl S, O’Brien S, et al.: Chemoimmunotherapy with hyper-CVAD plus rituximab for the treatment of adult Burkitt and Burkitt-type lymphoma or acute lymphoblastic leukemia. Cancer 106 (7): 1569-80, 2006. [PUBMED Abstract]
Dunleavy K, Pittaluga S, Shovlin M, et al.: Low-intensity therapy in adults with Burkitt’s lymphoma. N Engl J Med 369 (20): 1915-25, 2013. [PUBMED Abstract]
Hoelzer D, Walewski J, Döhner H, et al.: Improved outcome of adult Burkitt lymphoma/leukemia with rituximab and chemotherapy: report of a large prospective multicenter trial. Blood 124 (26): 3870-9, 2014. [PUBMED Abstract]
Ribrag V, Koscielny S, Bosq J, et al.: Rituximab and dose-dense chemotherapy for adults with Burkitt’s lymphoma: a randomised, controlled, open-label, phase 3 trial. Lancet 387 (10036): 2402-11, 2016. [PUBMED Abstract]
Magrath I, Adde M, Shad A, et al.: Adults and children with small non-cleaved-cell lymphoma have a similar excellent outcome when treated with the same chemotherapy regimen. J Clin Oncol 14 (3): 925-34, 1996. [PUBMED Abstract]
Hoelzer D, Ludwig WD, Thiel E, et al.: Improved outcome in adult B-cell acute lymphoblastic leukemia. Blood 87 (2): 495-508, 1996. [PUBMED Abstract]
Lee EJ, Petroni GR, Schiffer CA, et al.: Brief-duration high-intensity chemotherapy for patients with small noncleaved-cell lymphoma or FAB L3 acute lymphocytic leukemia: results of cancer and leukemia group B study 9251. J Clin Oncol 19 (20): 4014-22, 2001. [PUBMED Abstract]
Mead GM, Sydes MR, Walewski J, et al.: An international evaluation of CODOX-M and CODOX-M alternating with IVAC in adult Burkitt’s lymphoma: results of United Kingdom Lymphoma Group LY06 study. Ann Oncol 13 (8): 1264-74, 2002. [PUBMED Abstract]
Rizzieri DA, Johnson JL, Niedzwiecki D, et al.: Intensive chemotherapy with and without cranial radiation for Burkitt leukemia and lymphoma: final results of Cancer and Leukemia Group B Study 9251. Cancer 100 (7): 1438-48, 2004. [PUBMED Abstract]
Noy A, Lee JY, Cesarman E, et al.: AMC 048: modified CODOX-M/IVAC-rituximab is safe and effective for HIV-associated Burkitt lymphoma. Blood 126 (2): 160-6, 2015. [PUBMED Abstract]
Verdonck LF, Dekker AW, de Gast GC, et al.: Autologous bone marrow transplantation for adult poor-risk lymphoblastic lymphoma in first remission. J Clin Oncol 10 (4): 644-6, 1992. [PUBMED Abstract]
Thomas DA, O’Brien S, Cortes J, et al.: Outcome with the hyper-CVAD regimens in lymphoblastic lymphoma. Blood 104 (6): 1624-30, 2004. [PUBMED Abstract]
Sweetenham JW, Santini G, Qian W, et al.: High-dose therapy and autologous stem-cell transplantation versus conventional-dose consolidation/maintenance therapy as postremission therapy for adult patients with lymphoblastic lymphoma: results of a randomized trial of the European Group for Blood and Marrow Transplantation and the United Kingdom Lymphoma Group. J Clin Oncol 19 (11): 2927-36, 2001. [PUBMED Abstract]
Nador RG, Cesarman E, Chadburn A, et al.: Primary effusion lymphoma: a distinct clinicopathologic entity associated with the Kaposi’s sarcoma-associated herpes virus. Blood 88 (2): 645-56, 1996. [PUBMED Abstract]
Shimada K, Hayakawa F, Kiyoi H: Biology and management of primary effusion lymphoma. Blood 132 (18): 1879-1888, 2018. [PUBMED Abstract]
Castillo JJ, Bibas M, Miranda RN: The biology and treatment of plasmablastic lymphoma. Blood 125 (15): 2323-30, 2015. [PUBMED Abstract]
Al-Malki MM, Castillo JJ, Sloan JM, et al.: Hematopoietic cell transplantation for plasmablastic lymphoma: a review. Biol Blood Marrow Transplant 20 (12): 1877-84, 2014. [PUBMED Abstract]
Cattaneo C, Re A, Ungari M, et al.: Plasmablastic lymphoma among human immunodeficiency virus-positive patients: results of a single center’s experience. Leuk Lymphoma 56 (1): 267-9, 2015. [PUBMED Abstract]
Morrison VA, Dunn DL, Manivel JC, et al.: Clinical characteristics of post-transplant lymphoproliferative disorders. Am J Med 97 (1): 14-24, 1994. [PUBMED Abstract]
Knowles DM, Cesarman E, Chadburn A, et al.: Correlative morphologic and molecular genetic analysis demonstrates three distinct categories of posttransplantation lymphoproliferative disorders. Blood 85 (2): 552-65, 1995. [PUBMED Abstract]
Leblond V, Dhedin N, Mamzer Bruneel MF, et al.: Identification of prognostic factors in 61 patients with posttransplantation lymphoproliferative disorders. J Clin Oncol 19 (3): 772-8, 2001. [PUBMED Abstract]
Ghobrial IM, Habermann TM, Maurer MJ, et al.: Prognostic analysis for survival in adult solid organ transplant recipients with post-transplantation lymphoproliferative disorders. J Clin Oncol 23 (30): 7574-82, 2005. [PUBMED Abstract]
Evens AM, David KA, Helenowski I, et al.: Multicenter analysis of 80 solid organ transplantation recipients with post-transplantation lymphoproliferative disease: outcomes and prognostic factors in the modern era. J Clin Oncol 28 (6): 1038-46, 2010. [PUBMED Abstract]
Dierickx D, Tousseyn T, Gheysens O: How I treat posttransplant lymphoproliferative disorders. Blood 126 (20): 2274-83, 2015. [PUBMED Abstract]
Kuehnle I, Huls MH, Liu Z, et al.: CD20 monoclonal antibody (rituximab) for therapy of Epstein-Barr virus lymphoma after hemopoietic stem-cell transplantation. Blood 95 (4): 1502-5, 2000. [PUBMED Abstract]
Trappe RU, Dierickx D, Zimmermann H, et al.: Response to Rituximab Induction Is a Predictive Marker in B-Cell Post-Transplant Lymphoproliferative Disorder and Allows Successful Stratification Into Rituximab or R-CHOP Consolidation in an International, Prospective, Multicenter Phase II Trial. J Clin Oncol 35 (5): 536-543, 2017. [PUBMED Abstract]
Leblond V, Sutton L, Dorent R, et al.: Lymphoproliferative disorders after organ transplantation: a report of 24 cases observed in a single center. J Clin Oncol 13 (4): 961-8, 1995. [PUBMED Abstract]
Mamzer-Bruneel MF, Lomé C, Morelon E, et al.: Durable remission after aggressive chemotherapy for very late post-kidney transplant lymphoproliferation: A report of 16 cases observed in a single center. J Clin Oncol 18 (21): 3622-32, 2000. [PUBMED Abstract]
Swinnen LJ: Durable remission after aggressive chemotherapy for post-cardiac transplant lymphoproliferation. Leuk Lymphoma 28 (1-2): 89-101, 1997. [PUBMED Abstract]
McCarthy M, Ramage J, McNair A, et al.: The clinical diversity and role of chemotherapy in lymphoproliferative disorder in liver transplant recipients. J Hepatol 27 (6): 1015-21, 1997. [PUBMED Abstract]
Leblond V, Davi F, Charlotte F, et al.: Posttransplant lymphoproliferative disorders not associated with Epstein-Barr virus: a distinct entity? J Clin Oncol 16 (6): 2052-9, 1998. [PUBMED Abstract]
Senderowicz AM, Vitetta E, Headlee D, et al.: Complete sustained response of a refractory, post-transplantation, large B-cell lymphoma to an anti-CD22 immunotoxin. Ann Intern Med 126 (11): 882-5, 1997. [PUBMED Abstract]
Haddad E, Paczesny S, Leblond V, et al.: Treatment of B-lymphoproliferative disorder with a monoclonal anti-interleukin-6 antibody in 12 patients: a multicenter phase 1-2 clinical trial. Blood 97 (6): 1590-7, 2001. [PUBMED Abstract]
Guinee D, Jaffe E, Kingma D, et al.: Pulmonary lymphomatoid granulomatosis. Evidence for a proliferation of Epstein-Barr virus infected B-lymphocytes with a prominent T-cell component and vasculitis. Am J Surg Pathol 18 (8): 753-64, 1994. [PUBMED Abstract]
Myers JL, Kurtin PJ, Katzenstein AL, et al.: Lymphomatoid granulomatosis. Evidence of immunophenotypic diversity and relationship to Epstein-Barr virus infection. Am J Surg Pathol 19 (11): 1300-12, 1995. [PUBMED Abstract]
Other Lymphoproliferative and Related Disorders
Castleman Disease
A biopsy of localized or multifocal collections of lymph nodes may lead to a diagnosis of Castleman disease (CD). Strictly speaking, this uncommon diagnosis is not a lymphoma or even a malignancy. Yet, many patients with CD may be seen and treated by hematologists or oncologists.
Localized or unicentric CD is usually asymptomatic and occurs in the mediastinum, which is the most common presentation for CD.[1] Watchful waiting, surgery, or radiation therapy can be used to treat this indolent form. Multicentric CD (30% of CD patients) presents with lymphadenopathy in multiple sites; symptoms such as fever, night sweats, weight loss, and fatigue; and laboratory abnormalities such as anemia, low albumin level, elevated C-reactive protein level, and high fibrinogen level.[1] Multicentric CD (MCD) is subdivided into human herpes virus-8–associated MCD (usually with HIV or severe immunocompromise) or idiopathic MCD. Cytopenias and cytokine storm are attributed to interleukin-6 (IL-6) overproduction. MCD is a feature seen in POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin abnormalities) syndrome [2] and TAFRO (thrombocytopenia, anasarca, fever, reticulin fibrosis, and organomegaly) syndrome.[3,4] Therapy with siltuximab (an anti–IL-6 monoclonal antibody), rituximab (an anti-CD20 monoclonal antibody), or chemotherapeutic agents has been presented in anecdotal nonrandomized series.[5–8]
True Histiocytic Lymphoma
True histiocytic lymphomas are very rare tumors that show histiocytic differentiation and express histiocytic markers in the absence of B-cell or T-cell lineage-specific immunologic markers.[9,10] Care must be taken with immunophenotypic tests to exclude anaplastic large cell lymphoma or hemophagocytic syndromes caused by viral infections, especially Epstein-Barr virus.
Therapeutic options
Therapy is modeled after the treatment of comparably staged diffuse large cell lymphomas, but the optimal approach remains to be defined.
References
van Rhee F, Voorhees P, Dispenzieri A, et al.: International, evidence-based consensus treatment guidelines for idiopathic multicentric Castleman disease. Blood 132 (20): 2115-2124, 2018. [PUBMED Abstract]
Dispenzieri A: POEMS Syndrome: 2019 Update on diagnosis, risk-stratification, and management. Am J Hematol 94 (7): 812-827, 2019. [PUBMED Abstract]
Zhang Y, Suo SS, Yang HJ, et al.: Clinical features and treatment of 7 Chinese TAFRO syndromes from 96 de novo Castleman diseases: a 10-year retrospective study. J Cancer Res Clin Oncol 146 (2): 357-365, 2020. [PUBMED Abstract]
Fujimoto S, Sakai T, Kawabata H, et al.: Is TAFRO syndrome a subtype of idiopathic multicentric Castleman disease? Am J Hematol 94 (9): 975-983, 2019. [PUBMED Abstract]
Tonialini L, Bonfichi M, Ferrero S, et al.: Siltuximab in relapsed/refractory multicentric Castleman disease: Experience of the Italian NPP program. Hematol Oncol 36 (4): 689-692, 2018. [PUBMED Abstract]
Dong Y, Zhang L, Nong L, et al.: Effectiveness of rituximab-containing treatment regimens in idiopathic multicentric Castleman disease. Ann Hematol 97 (9): 1641-1647, 2018. [PUBMED Abstract]
Zhang L, Zhao AL, Duan MH, et al.: Phase 2 study using oral thalidomide-cyclophosphamide-prednisone for idiopathic multicentric Castleman disease. Blood 133 (16): 1720-1728, 2019. [PUBMED Abstract]
van Rhee F, Wong RS, Munshi N, et al.: Siltuximab for multicentric Castleman’s disease: a randomised, double-blind, placebo-controlled trial. Lancet Oncol 15 (9): 966-74, 2014. [PUBMED Abstract]
Soslow RA, Davis RE, Warnke RA, et al.: True histiocytic lymphoma following therapy for lymphoblastic neoplasms. Blood 87 (12): 5207-12, 1996. [PUBMED Abstract]
Kamel OW, Gocke CD, Kell DL, et al.: True histiocytic lymphoma: a study of 12 cases based on current definition. Leuk Lymphoma 18 (1-2): 81-6, 1995. [PUBMED Abstract]
Treatment Option Overview for Aggressive B-Cell Non-Hodgkin Lymphoma
Treatment of aggressive non-Hodgkin lymphoma (NHL) depends on the histological type and stage. Many of the improvements in survival have been made because of clinical trials that have attempted to improve conventional or standard therapy.
In asymptomatic patients with indolent forms of advanced NHL, treatment may be deferred until the patient becomes symptomatic as the disease progresses. When treatment is deferred, the clinical course of patients with indolent NHL varies; frequent and careful observation is required so that effective treatment can be initiated when the clinical course of the disease accelerates. Some patients have a prolonged indolent course, but others have disease that rapidly evolves into more aggressive types of NHL that require immediate treatment.
Radiation techniques differ somewhat from those used in the treatment of Hodgkin lymphoma. The dose of radiation therapy usually varies from 25 Gy to 50 Gy and is dependent on factors that include the histological type of lymphoma, the patient’s stage and overall condition, the goal of treatment (curative or palliative), the proximity of sensitive surrounding organs, and whether the patient is being treated with radiation therapy alone or in combination with chemotherapy. Given the patterns of disease presentations and relapse, treatment may need to include unusual sites such as Waldeyer ring, epitrochlear nodes, or mesenteric nodes. The associated morbidity of the treatment must be considered carefully. Most patients who receive radiation are treated on only one side of the diaphragm. Localized presentations of extranodal NHL may be treated with involved-field techniques with significant (>50%) success.
In situations where mediastinal radiation therapy would encompass the left side of the heart or would increase breast cancer risk in young female patients, proton therapy may be considered to reduce radiation dose to organs at risk.[1] For more information, see the Superior Vena Cava Syndrome section in Cardiopulmonary Syndromes.
Table 4. Treatment Options for Aggressive B-Cell Non-Hodgkin Lymphoma (NHL)
Stage
Treatment Options
BMT = bone marrow transplant; CAR = chimeric antigen receptor; CNS = central nervous system; IF-XRT = involved-field radiation therapy; Pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-ACVBP = rituximab, doxorubicin, cyclophosphamide, vindesine, bleomycin, prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; SCT = stem cell transplant.
Aggressive Stage I and Aggressive, Contiguous Stage II B-cell NHL
Even though existing treatments cure a significant fraction of patients with lymphoma, numerous clinical trials that explore treatment improvements are in progress. If possible, patients can participate in these studies. Standardized guidelines for response assessment have been suggested for use in clinical trials.[2]
Several retrospective reviews suggest that routine surveillance scans offer little to no value in patients with diffuse-large B-cell lymphoma (DLBCL) who have attained a clinical complete remission after induction therapy. Prognostic value is also difficult to identify for an interim positron emission tomography-computed tomography scan during induction therapy for DLBCL.[3–6]
Aggressive lymphomas are increasingly seen in patients with HIV. Treatment of these patients requires special consideration. For more information, see AIDS-Related Lymphoma Treatment
In addition to screening for HIV among patients with aggressive lymphomas, active hepatitis B or hepatitis C can be assessed before treatment with rituximab and/or chemotherapy.[7,8] Patients with detectable hepatitis B virus (HBV) benefit from prophylaxis with entecavir in the context of rituximab therapy.[9,10] Patients with a resolved HBV infection (defined as hepatitis B surface antigen-negative but hepatitis B core antibody-positive) are at risk of reactivation of HBV and require monitoring of HBV DNA. In a retrospective study of 326 patients, prophylactic nucleoside analogue therapy lowered HBV reactivation from 10.8% to 2.1%.[11] Similarly, prophylaxis for herpes zoster with acyclovir or valacyclovir and prophylaxis for Pneumocystis with trimethoprim/sulfamethoxazole or dapsone are usually given to patients receiving rituximab with or without combination chemotherapy. Long-term impaired immune health was evaluated in a retrospective cohort study of 21,690 survivors of DLBCL from the California Cancer Registry. Elevated incidence rate ratios were found up to 10 years later for pneumonia (10.8-fold), meningitis (5.3-fold), immunoglobulin deficiency (17.6-fold), and autoimmune cytopenias (12-fold).[12]
Among 2,508 patients in a Danish registry, the incidence of doxorubicin-induced congestive heart failure increased for 115 NHL survivors with a history of cardiac disease (hazard ratio [HR], 2.71; 95% confidence interval [CI], 1.15−6.36) and/or multiple cardiovascular risk factors (HR, 2.86; 95% CI, 1.56−5.23).[13]
Dabaja BS, Hoppe BS, Plastaras JP, et al.: Proton therapy for adults with mediastinal lymphomas: the International Lymphoma Radiation Oncology Group guidelines. Blood 132 (16): 1635-1646, 2018. [PUBMED Abstract]
Cheson BD, Horning SJ, Coiffier B, et al.: Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol 17 (4): 1244, 1999. [PUBMED Abstract]
Mamot C, Klingbiel D, Hitz F, et al.: Final Results of a Prospective Evaluation of the Predictive Value of Interim Positron Emission Tomography in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP-14 (SAKK 38/07). J Clin Oncol 33 (23): 2523-9, 2015. [PUBMED Abstract]
Thompson CA, Ghesquieres H, Maurer MJ, et al.: Utility of routine post-therapy surveillance imaging in diffuse large B-cell lymphoma. J Clin Oncol 32 (31): 3506-12, 2014. [PUBMED Abstract]
El-Galaly TC, Jakobsen LH, Hutchings M, et al.: Routine Imaging for Diffuse Large B-Cell Lymphoma in First Complete Remission Does Not Improve Post-Treatment Survival: A Danish-Swedish Population-Based Study. J Clin Oncol 33 (34): 3993-8, 2015. [PUBMED Abstract]
Huntington SF, Svoboda J, Doshi JA: Cost-effectiveness analysis of routine surveillance imaging of patients with diffuse large B-cell lymphoma in first remission. J Clin Oncol 33 (13): 1467-74, 2015. [PUBMED Abstract]
Niitsu N, Hagiwara Y, Tanae K, et al.: Prospective analysis of hepatitis B virus reactivation in patients with diffuse large B-cell lymphoma after rituximab combination chemotherapy. J Clin Oncol 28 (34): 5097-100, 2010. [PUBMED Abstract]
Dong HJ, Ni LN, Sheng GF, et al.: Risk of hepatitis B virus (HBV) reactivation in non-Hodgkin lymphoma patients receiving rituximab-chemotherapy: a meta-analysis. J Clin Virol 57 (3): 209-14, 2013. [PUBMED Abstract]
Huang YH, Hsiao LT, Hong YC, et al.: Randomized controlled trial of entecavir prophylaxis for rituximab-associated hepatitis B virus reactivation in patients with lymphoma and resolved hepatitis B. J Clin Oncol 31 (22): 2765-72, 2013. [PUBMED Abstract]
Li H, Zhang HM, Chen LF, et al.: Prophylactic lamivudine to improve the outcome of HBsAg-positive lymphoma patients during chemotherapy: a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol 39 (1): 80-92, 2015. [PUBMED Abstract]
Kusumoto S, Arcaini L, Hong X, et al.: Risk of HBV reactivation in patients with B-cell lymphomas receiving obinutuzumab or rituximab immunochemotherapy. Blood 133 (2): 137-146, 2019. [PUBMED Abstract]
Shree T, Li Q, Glaser SL, et al.: Impaired Immune Health in Survivors of Diffuse Large B-Cell Lymphoma. J Clin Oncol 38 (15): 1664-1675, 2020. [PUBMED Abstract]
Salz T, Zabor EC, de Nully Brown P, et al.: Preexisting Cardiovascular Risk and Subsequent Heart Failure Among Non-Hodgkin Lymphoma Survivors. J Clin Oncol 35 (34): 3837-3843, 2017. [PUBMED Abstract]
Treatment of Aggressive Stage I and Aggressive, Contiguous Stage II B-Cell Non-Hodgkin Lymphoma
Patients with aggressive stage I or aggressive, contiguous stage II diffuse large B-cell lymphoma (DLBCL) are candidates for combination chemotherapy with or without involved-field radiation therapy (IF-XRT).
Patients with a resolved hepatitis B virus (HBV) infection (defined as hepatitis B surface antigen-negative but hepatitis B core antibody-positive) are at risk of reactivation of HBV and require monitoring of HBV DNA. In a retrospective study of 326 patients, prophylactic nucleoside analogue therapy lowered HBV reactivation from 10.8% to 2.1%.[1]
Stage IE or IIE Gastric DLBCL
Four case series involving more than 100 patients with stage IE or IIE disease (with or without mucosa-associated lymphatic tissue) and with positive Helicobacter pylori infection. The series reported that more than 50% of patients attained a durable complete remission after appropriate antibiotic therapy to eradicate H. pylori.[2–5][Level of evidence C3]
Treatment Options for Aggressive Stage I and Aggressive, Contiguous Stage II B-Cell Non-Hodgkin Lymphoma
Treatment options for aggressive stage I and aggressive, contiguous stage II B-cell non-Hodgkin lymphoma include:
Rituximab has efficacy in advanced-stage disease. However, its use is only supported by retrospective comparisons in studies of R-CHOP with or without radiation therapy.[8][Level of evidence C2]
R-CHOP (four to six cycles).
R-CHOP (three to six cycles) + IF-XRT.
Evidence (R-CHOP with or without IF-XRT):
In a randomized prospective trial of 334 patients with nonbulky (≤7 cm) stage I or stage II DLBCL, after receiving four to six cycles of R-CHOP-14 (R-CHOP delivered every 2 weeks), patients were randomly assigned to undergo 40 Gy of radiation therapy or no radiation therapy.[9]
After a median follow-up of 64 months, the 5-year event-free survival rate (89%–92%; P = .18) and 5-year overall survival (OS) rate (92%–96%; P = .32) were the same.[9][Level of evidence A1]
Similar to the results of randomized studies of radiation therapy in the era before rituximab, radiation therapy can be deferred in patients with nonbulky early-stage disease. For patients unable to tolerate prolonged-course chemotherapy, three cycles of R-CHOP plus radiation therapy has produced equivalent results based on single-arm retrospective trials.[8]
In a randomized prospective trial (NCT00278421) of 592 patients younger than 60 years with nonbulky (<7.5 cm) stage I or stage II DLBCL, patients were randomly assigned to receive either four or six cycles of R-CHOP (with an extra two cycles of rituximab after four cycles).[10]
With a median follow-up of 66 months, the 3-year progression-free survival (PFS) rate was 96% (95% confidence interval [CI], 94%−99%) for patients who received four cycles of R-CHOP, which was 3% better (lower limit of one-sided 95% CI was zero) than the PFS rate for patients who received six cycles, establishing noninferiority for the four-cycle regimen.[10][Level of evidence B1]
A retrospective analysis at Memorial Sloan Kettering Cancer Center between 2001 and 2015 included 341 patients with stage I disease. The analysis found that 66% of patients had an extranodal presentation. After R-CHOP (or a similar regimen), with or without radiation therapy, the 5-year disease-free survival rate was 77%, and the 5-year OS rate was 94%.[11][Level of evidence C3] A multivariate analysis suggested that radiation therapy may improve outcomes for patients with extranodal disease that is positron emission tomography (PET)–positive at the end of therapy. This hypothesis needs confirmation in a prospective randomized trial.[11]
In summary, for patients with favorable prognosis, nonbulky (<7 cm), stage I or stage II DLBCL, four cycles of R-CHOP are sufficient. For patients with an unfavorable prognosis, six cycles of R-CHOP or three cycles of R-CHOP and 40 Gy of radiation therapy can be used. Early-stage patients with bulky disease (>7.5 cm) have not been studied in randomized trials; combined-modality therapy with R-CHOP for four to six cycles plus radiation therapy is usually chosen. Although a retrospective study suggested that patients with stage I extranodal disease and a positive PET scan at the end of therapy may benefit from radiation therapy, this hypothesis must be confirmed in a prospective randomized trial.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Kusumoto S, Arcaini L, Hong X, et al.: Risk of HBV reactivation in patients with B-cell lymphomas receiving obinutuzumab or rituximab immunochemotherapy. Blood 133 (2): 137-146, 2019. [PUBMED Abstract]
Morgner A, Miehlke S, Fischbach W, et al.: Complete remission of primary high-grade B-cell gastric lymphoma after cure of Helicobacter pylori infection. J Clin Oncol 19 (7): 2041-8, 2001. [PUBMED Abstract]
Chen LT, Lin JT, Shyu RY, et al.: Prospective study of Helicobacter pylori eradication therapy in stage I(E) high-grade mucosa-associated lymphoid tissue lymphoma of the stomach. J Clin Oncol 19 (22): 4245-51, 2001. [PUBMED Abstract]
Chen LT, Lin JT, Tai JJ, et al.: Long-term results of anti-Helicobacter pylori therapy in early-stage gastric high-grade transformed MALT lymphoma. J Natl Cancer Inst 97 (18): 1345-53, 2005. [PUBMED Abstract]
Kuo SH, Yeh KH, Wu MS, et al.: Helicobacter pylori eradication therapy is effective in the treatment of early-stage H pylori-positive gastric diffuse large B-cell lymphomas. Blood 119 (21): 4838-44; quiz 5057, 2012. [PUBMED Abstract]
Reyes F, Lepage E, Ganem G, et al.: ACVBP versus CHOP plus radiotherapy for localized aggressive lymphoma. N Engl J Med 352 (12): 1197-205, 2005. [PUBMED Abstract]
Ketterer N, Coiffier B, Thieblemont C, et al.: Phase III study of ACVBP versus ACVBP plus rituximab for patients with localized low-risk diffuse large B-cell lymphoma (LNH03-1B). Ann Oncol 24 (4): 1032-7, 2013. [PUBMED Abstract]
Persky DO, Unger JM, Spier CM, et al.: Phase II study of rituximab plus three cycles of CHOP and involved-field radiotherapy for patients with limited-stage aggressive B-cell lymphoma: Southwest Oncology Group study 0014. J Clin Oncol 26 (14): 2258-63, 2008. [PUBMED Abstract]
Lamy T, Damaj G, Soubeyran P, et al.: R-CHOP 14 with or without radiotherapy in nonbulky limited-stage diffuse large B-cell lymphoma. Blood 131 (2): 174-181, 2018. [PUBMED Abstract]
Poeschel V, Held G, Ziepert M, et al.: Four versus six cycles of CHOP chemotherapy in combination with six applications of rituximab in patients with aggressive B-cell lymphoma with favourable prognosis (FLYER): a randomised, phase 3, non-inferiority trial. Lancet 394 (10216): 2271-2281, 2019. [PUBMED Abstract]
Bobillo S, Joffe E, Lavery JA, et al.: Clinical characteristics and outcomes of extranodal stage I diffuse large B-cell lymphoma in the rituximab era. Blood 137 (1): 39-48, 2021. [PUBMED Abstract]
Treatment of Aggressive, Noncontiguous Stage II/III/IV B-Cell Non-Hodgkin Lymphoma
The treatment of choice for patients with advanced stages of aggressive non-Hodgkin lymphoma (NHL) is combination chemotherapy, either alone or supplemented by local-field radiation therapy.[1]
The following drug combinations are referred to in this section:
R-CHOP has been compared with Pola-R-CHP. Polatuzumab is an antibody-drug conjugate composed of an anti-CD79B monoclonal antibody attached to vedotin (monomethyl auristatin E), a microtubule inhibitor.
Evidence (Pola-R-CHP):
A prospective, randomized study (POLARIX [NCT03274492]) of 879 patients with previously untreated diffuse large B-cell lymphoma (DLBCL) and an IPI score of 2 or higher compared R-CHOP with Pola-R-CHP.[2] Polatuzumab vedotin was substituted for vincristine to mitigate neurological toxicity.
At a median follow-up of 28.2 months, the 2-year progression-free survival (PFS) rate was significantly higher in the Pola-R-CHP group than in the R-CHOP group: 76.7% (95% confidence interval [CI], 72.7%–80.0%) versus 70.2% (95% CI, 65.8%–74.6%) (hazard ratio [HR], 0.73; 95% CI, 0.57–0.95; P = .02).[2][Level of evidence B1]
The 2-year overall survival (OS) rate was 88.7% (95% CI, 85.7%–91.6%) for patients who received Pola-R-CHP and 88.6% (95% CI, 85.6%–91.6%) for patients who received R-CHOP (HR, 0.94; 95% CI, 0.65–1.37; P = .75).
A similar 7.7% improvement in 2-year PFS for Pola-R-CHP versus R-CHOP has been seen in an Asian subpopulation analysis from this trial.[3][Level of evidence C2]
The follow-up interval was too short to establish whether the 6% improvement in the PFS rate will plateau or improve after 2 years, and there is no evidence of OS advantage. Nonetheless, updated outcomes with a median follow-up over 3 years showed continued improvement of PFS, prompting the U.S. Food and Drug Administration (FDA) to approve Pola-R-CHP. Pola-R-CHP is the first regimen in over 20 years to be approved by the FDA as a therapy for patients with noncontiguous stage II, stage III, and stage IV disease. The new regimen is more than twice the cost of R-CHOP using acquisition prices in 2022, and polatuzumab may not be available worldwide.
The Pola-R-CHP regimen demonstrated substantial efficacy for patients with DLBCL non–germinal center B-cell (GCB)-origin tumors, predominantly those with the ABC (activated B-cell) subtype.[4] In the POLARIX trial, the HRPFS for Pola-R-CHP versus R-CHOP in patients with ABC-subtype tumors was 0.34 (95% CI, 0.13–0.85), and the HROS for those patients was 0.27 (95% CI, 0.06–1.26). In contrast, no such benefit was observed for patients with GCB-subtype tumors in this trial. For Pola-R-CHP, the HRPFS was 1.18 (95% CI, 0.75–1.84), and the HROS was 1.64 (95% CI, 0.87–3.07). This differential efficacy in favor of the non-GCB or ABC subtype was seen in five prospective phase I and II trials of the Pola-R-CHP regimen in patients with relapsed or refractory disease, with a combined analysis of data showing a level of significance P < .001.[4] Combining the data for a randomized phase II trial studying Pola-R-CHP in patients with relapsed or refractory disease with data from the POLARIX trial in patients with previously untreated disease, the HRdisease relapse/progression/death was 0.25 for patients with ABC-subtype tumors and 0.98 for patients with GCB-subtype tumors (P < .001).[4] The only exception to this observation is the clear benefit of Pola-R-CHP in GCB patients with double-hit variants (MYC gene and BCL2 gene). Given the increased rates of febrile neutropenia in patients who receive Pola-R-CHP and the significant financial toxicity, it is reasonable to consider R-CHOP as a standard regimen for patients with GCB-subtype DLBCL without a double-hit variant. However, assessing the GCB subtype using commercially available immunophenotyping is less accurate than using the molecular genetic signatures used in the POLARIX study. Some patients may miss the PFS benefit of polatuzumab. Some clinicians err on the side of using Pola-R-CHP for GCB subtype when patients have other high-risk features (e.g., CD5 positivity or involvement in two or more extranodal sites).
R-CHOP
The following studies established R-CHOP as a standard regimen for patients with newly diagnosed DLBCL and noncontiguous stage II, stage III, and stage IV disease for over 20 years.[5] Dose intensification of R-CHOP by a 14-day versus a 21-day cycle did not result in improved outcomes.[6] R-CHOP is the preferred regimen when polatuzumab is not available or affordable, or when contraindicated due to adverse side effects.
Evidence (R-CHOP):
R-CHOP showed improved event-free survival (EFS) and OS compared with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) alone in 399 patients older than 60 years with advanced-stage DLBCL (EFS rate, 57% vs. 38%; P = .002, and OS rate, 70% vs. 57%; P = .007 at 2 years).[7][Level of evidence A1] At a median follow-up of 10 years, the OS rate of patients who received R-CHOP was 44% compared with 28% for patients who received CHOP (P < .0001).[8]
Similarly, for 326 evaluable patients younger than 61 years, R-CHOP showed improved EFS and OS compared with CHOP alone (EFS rate, 79% vs. 59%, P = .001, and OS rate, 93% vs. 84%, P = .001 at 3 years).[9][Level of evidence A1]
A randomized study (DSHNHL-1999-1A [NCT00052936]) of 1,222 patients older than 60 years compared R-CHOP given every 2 weeks for six or eight cycles with CHOP given every 2 weeks for six or eight cycles.[10] With a median follow-up of 72 months, the EFS favored R-CHOP given every 2 weeks for six or eight cycles (6-year EFS rate, 74% vs. 56%; P < .0001). The OS favored R-CHOP for only six cycles because of increased toxicity in the eight-cycle arm (6-year OS rate, 90% vs. 80%; P = .0004).[10][Level of evidence A1] There was no comparison with standard R-CHOP or CHOP given every 3 weeks.
A trial (NCT00140595) of 380 patients younger than 60 years with DLBCL and an age-adjusted IPI score of 1 randomly assigned patients to receive ACVBP and R-ACVBP plus consolidation with methotrexate, ifosfamide, etoposide, and cytarabine versus CHOP and rituximab.[11] With a median follow-up of 44 months, 3-year OS rates favored R-ACVBP (92% vs. 84%; HR, 0.44; 95% CI, 0.28–0.81, P = .007).[11][Level of evidence A1] The significantly worse toxicities with R-ACVBP, the narrow target population (<60 years with either elevated lactate dehydrogenase [LDH] or stage III-stage IV disease, but not both), and the lack of a confirmatory trial may inhibit adoption of R-ACVBP as a new standard of care.[12]
There is no validated trial for interim positron emission tomography–based treatment intensification.[13] R-CHOP has curative potential, even in patients older than 80 years who are frail and require reduced dosage of R-CHOP components. In a retrospective review of 239 patients, the 5-year cause-specific survival rate was 48% (95% CI, 41%−55%).[14][Level of evidence C3]
Less than 10% of patients with DLBCL present with a concurrent indolent lymphoma at diagnosis, and these are predominantly of GCB phenotype. A retrospective review of 1,324 patients showed similar EFS (HR, 1.19) and OS (HR, 1.09).[15][Level of evidence C3] For 847 patients who were treated with R-CHOP and free of disease 24 months after therapy, the rate of indolent lymphoma relapse by 5 years was higher with a concurrent diagnosis of follicular lymphoma (7.4% vs. 2.1%, P < .01) and with a GCB phenotype (3.9% vs. 0.0% at 5 years, P = .02).[16]
Modifications to R-CHOP to achieve improved efficacy continue to be explored in clinical trials.
Radiation therapy consolidation to sites of bulky disease
After R-CHOP induction chemotherapy (or similar regimens), the addition of involved-field radiation therapy to sites of initial bulky disease (≥5–10 cm) or to extralymphatic sites remains controversial.[17–19] Increased risks, such as long-term toxicities (e.g., second malignancies), must be considered.
Bone marrow transplant (BMT) or stem cell transplant (SCT)
Several randomized prospective trials evaluated the role of autologous BMT or SCT consolidation versus chemotherapy alone in patients with diffuse large cell lymphoma in first remission.[20–27]; [28–30][Level of evidence A1] Although some of these trials demonstrated significant increases in EFS (by 10% to 20%) among patients who received high-dose therapy, significant differences in OS could not be demonstrated prospectively in any of the series.
Retrospective analyses of high-intermediate (two risk factors) or high-risk (more than three risk factors) patients as defined by IPI suggest improved survival with BMT in two of the trials.[21,27] These studies do not establish that high-dose consolidation is of value to patients with aggressive lymphoma who are truly at high risk of relapse, and they also demonstrate that EFS may be a poor surrogate for OS for these patients.[31]
Prognostic factors
The National Comprehensive Cancer Network International Prognostic Index (IPI) for aggressive NHL (diffuse large cell lymphoma) identifies the following five significant risk factors prognostic of overall survival (OS) and their associated risk scores:[32]
Age.
<40 years: 0.
41–60 years: 1.
61–75 years: 2.
>75 years: 3.
Stage III/IV: 1.
Performance status (PS) 2/3/4: 1.
Serum lactate dehydrogenase (LDH).
Normalized: 0.
>1x–3x: 1.
>3x: 2.
Number of extranodal sites ≥2: 1.
Risk scores:
Low (0 or 1): 5-year OS rate, 96%; progression-free survival (PFS) rate, 91%.
Low intermediate (2 or 3): 5-year OS rate, 82%; PFS rate, 74%.
High intermediate (4 or 5): 5-year OS rate, 64%; PFS rate, 51%.
High (>6): 5-year OS rate, 33%; PFS rate, 30%.
Age-adjusted and stage-adjusted modifications of this IPI are used for younger patients with localized disease.[33] Shorter intervals of time between diagnosis and treatment appear to be a surrogate for poor prognostic biological factors.[34]
The BCL2 gene and rearrangement of the MYC gene or dual overexpression of the MYC gene, or both, confer a particularly poor prognosis.[35–38] Patients at high risk of relapse may be considered for clinical trials.[39] Molecular profiles of gene expression using DNA microarrays may help to stratify patients in the future for therapies directed at specific targets and to better predict survival after standard chemotherapy.[40]
Treatment of Tumor Lysis Syndrome
Patients with bulky and extensive lymphadenopathy and elevations of serum uric acid and LDH are at increased risk of tumor lysis syndrome, resulting in metabolic derangements such as hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, and subsequent acute renal failure.[41] Treatment options include alkaline hydration, allopurinol, and rasburicase (a recombinant urate oxidase).[42]
Central Nervous System (CNS) Prophylaxis
The CNS-IPI tool predicts which patients have a CNS relapse risk exceeding 10%.[43,44] It was developed by the German Lymphoma Study Group and validated by the British Columbia Cancer Agency database. The presence of four to six of the CNS-IPI risk factors (age >60 years, performance status ≥2, elevated LDH, stage III or IV disease, >1 extranodal site, or involvement of the kidneys or adrenal glands) was used to define a high-risk group for CNS recurrence (a 12% risk of CNS involvement by 2 years).[44]
CNS prophylaxis (usually with four to six doses of intrathecal methotrexate) is often recommended for patients with testicular involvement.[45–47][Level of evidence C3] A retrospective analysis of the German RICOVER studies compared intrathecal methotrexate with no prophylaxis in patients with DLBCL. This study was completed during the R-CHOP treatment era. With the possible exception of patients with testicular involvement, the analysis showed that intrathecal methotrexate did not reduce the risk of CNS disease.[48][Level of evidence C3]
Some clinicians use high-dose intravenous (IV) methotrexate (usually four doses) as an alternative to intrathecal therapy because drug delivery is improved and patient morbidity is decreased.[43,49] Five retrospective studies and one network meta-analysis evaluating high-dose methotrexate alone in patients with high-risk DLBCL also showed no improvement in CNS relapse rate.[50–55][Level of evidence C3] Patients deemed at high risk for CNS relapse (e.g., patients with testicular, renal, or adrenal disease and three or more extranodal sites) may receive intrathecal methotrexate or high-dose IV methotrexate, but the lack of confirmatory randomized studies calls this standard into question and shows an urgent need for better therapeutics verified in clinical trials.[43,43] While there is insufficient evidence to support a significant benefit for CNS prophylaxis in most high-risk patients, the perceived risk of not treating for CNS relapse has often outweighed the lack of evidence for its efficacy.[43] Although patients with testicular involvement or kidney/adrenal involvement are considered an exception, there is only anecdotal benefit from intrathecal or high-dose IV methotrexate in reducing CNS recurrence.[45–47][Level of evidence C3]
In retrospective analyses, the addition of rituximab to CHOP-based regimens has significantly reduced the risk of CNS relapse.[48,56][Level of evidence C3] Patients with CNS dissemination at diagnosis or at relapse usually receive rituximab and high doses of methotrexate and/or cytarabine followed by autologous SCT, but this approach has not been assessed in randomized trials.[57,58][Level of evidence C3]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Tilly H, Morschhauser F, Sehn LH, et al.: Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N Engl J Med 386 (4): 351-363, 2022. [PUBMED Abstract]
Song Y, Tilly H, Rai S, et al.: Polatuzumab vedotin in previously untreated DLBCL: an Asia subpopulation analysis from the phase 3 POLARIX trial. Blood 141 (16): 1971-1981, 2023. [PUBMED Abstract]
Palmer AC, Kurtz DM, Alizadeh AA: Cell-of-Origin Subtypes and Therapeutic Benefit from Polatuzumab Vedotin. N Engl J Med 389 (8): 764-766, 2023. [PUBMED Abstract]
Cunningham D, Hawkes EA, Jack A, et al.: Rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone in patients with newly diagnosed diffuse large B-cell non-Hodgkin lymphoma: a phase 3 comparison of dose intensification with 14-day versus 21-day cycles. Lancet 381 (9880): 1817-26, 2013. [PUBMED Abstract]
Coiffier B, Lepage E, Briere J, et al.: CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med 346 (4): 235-42, 2002. [PUBMED Abstract]
Coiffier B, Thieblemont C, Van Den Neste E, et al.: Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood 116 (12): 2040-5, 2010. [PUBMED Abstract]
Pfreundschuh M, Trümper L, Osterborg A, et al.: CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol 7 (5): 379-91, 2006. [PUBMED Abstract]
Pfreundschuh M, Kuhnt E, Trümper L, et al.: CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol 12 (11): 1013-22, 2011. [PUBMED Abstract]
Récher C, Coiffier B, Haioun C, et al.: Intensified chemotherapy with ACVBP plus rituximab versus standard CHOP plus rituximab for the treatment of diffuse large B-cell lymphoma (LNH03-2B): an open-label randomised phase 3 trial. Lancet 378 (9806): 1858-67, 2011. [PUBMED Abstract]
Casasnovas RO, Ysebaert L, Thieblemont C, et al.: FDG-PET-driven consolidation strategy in diffuse large B-cell lymphoma: final results of a randomized phase 2 study. Blood 130 (11): 1315-1326, 2017. [PUBMED Abstract]
Dührsen U, Müller S, Hertenstein B, et al.: Positron Emission Tomography-Guided Therapy of Aggressive Non-Hodgkin Lymphomas (PETAL): A Multicenter, Randomized Phase III Trial. J Clin Oncol 36 (20): 2024-2034, 2018. [PUBMED Abstract]
Gobba S, Moccia AA, Gulden-Sala W, et al.: Outcome of patients older than 80 years with diffuse large B-cell lymphoma (DLBCL) treated with “standard” immunochemotherapy: A large retrospective study from 4 institutions. Hematol Oncol 36 (1): 84-92, 2018. [PUBMED Abstract]
Wang Y, Link BK, Witzig TE, et al.: Impact of concurrent indolent lymphoma on the clinical outcome of newly diagnosed diffuse large B-cell lymphoma. Blood 134 (16): 1289-1297, 2019. [PUBMED Abstract]
Wang Y, Farooq U, Link BK, et al.: Late Relapses in Patients With Diffuse Large B-Cell Lymphoma Treated With Immunochemotherapy. J Clin Oncol 37 (21): 1819-1827, 2019. [PUBMED Abstract]
Held G, Murawski N, Ziepert M, et al.: Role of radiotherapy to bulky disease in elderly patients with aggressive B-cell lymphoma. J Clin Oncol 32 (11): 1112-8, 2014. [PUBMED Abstract]
Kahl BS: Bulky aggressive B-cell lymphoma: to radiate or not to radiate–that is the question. J Clin Oncol 32 (11): 1097-8, 2014. [PUBMED Abstract]
Phan J, Mazloom A, Medeiros LJ, et al.: Benefit of consolidative radiation therapy in patients with diffuse large B-cell lymphoma treated with R-CHOP chemotherapy. J Clin Oncol 28 (27): 4170-6, 2010. [PUBMED Abstract]
Haioun C, Lepage E, Gisselbrecht C, et al.: Survival benefit of high-dose therapy in poor-risk aggressive non-Hodgkin’s lymphoma: final analysis of the prospective LNH87-2 protocol–a groupe d’Etude des lymphomes de l’Adulte study. J Clin Oncol 18 (16): 3025-30, 2000. [PUBMED Abstract]
Haioun C, Lepage E, Gisselbrecht C, et al.: Benefit of autologous bone marrow transplantation over sequential chemotherapy in poor-risk aggressive non-Hodgkin’s lymphoma: updated results of the prospective study LNH87-2. Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol 15 (3): 1131-7, 1997. [PUBMED Abstract]
Santini G, Salvagno L, Leoni P, et al.: VACOP-B versus VACOP-B plus autologous bone marrow transplantation for advanced diffuse non-Hodgkin’s lymphoma: results of a prospective randomized trial by the non-Hodgkin’s Lymphoma Cooperative Study Group. J Clin Oncol 16 (8): 2796-802, 1998. [PUBMED Abstract]
Gianni AM, Bregni M, Siena S, et al.: High-dose chemotherapy and autologous bone marrow transplantation compared with MACOP-B in aggressive B-cell lymphoma. N Engl J Med 336 (18): 1290-7, 1997. [PUBMED Abstract]
Kluin-Nelemans HC, Zagonel V, Anastasopoulou A, et al.: Standard chemotherapy with or without high-dose chemotherapy for aggressive non-Hodgkin’s lymphoma: randomized phase III EORTC study. J Natl Cancer Inst 93 (1): 22-30, 2001. [PUBMED Abstract]
Gisselbrecht C, Lepage E, Molina T, et al.: Shortened first-line high-dose chemotherapy for patients with poor-prognosis aggressive lymphoma. J Clin Oncol 20 (10): 2472-9, 2002. [PUBMED Abstract]
Martelli M, Gherlinzoni F, De Renzo A, et al.: Early autologous stem-cell transplantation versus conventional chemotherapy as front-line therapy in high-risk, aggressive non-Hodgkin’s lymphoma: an Italian multicenter randomized trial. J Clin Oncol 21 (7): 1255-62, 2003. [PUBMED Abstract]
Milpied N, Deconinck E, Gaillard F, et al.: Initial treatment of aggressive lymphoma with high-dose chemotherapy and autologous stem-cell support. N Engl J Med 350 (13): 1287-95, 2004. [PUBMED Abstract]
Betticher DC, Martinelli G, Radford JA, et al.: Sequential high dose chemotherapy as initial treatment for aggressive sub-types of non-Hodgkin lymphoma: results of the international randomized phase III trial (MISTRAL). Ann Oncol 17 (10): 1546-52, 2006. [PUBMED Abstract]
Stiff PJ, Unger JM, Cook JR, et al.: Autologous transplantation as consolidation for aggressive non-Hodgkin’s lymphoma. N Engl J Med 369 (18): 1681-90, 2013. [PUBMED Abstract]
Chiappella A, Martelli M, Angelucci E, et al.: Rituximab-dose-dense chemotherapy with or without high-dose chemotherapy plus autologous stem-cell transplantation in high-risk diffuse large B-cell lymphoma (DLCL04): final results of a multicentre, open-label, randomised, controlled, phase 3 study. Lancet Oncol 18 (8): 1076-1088, 2017. [PUBMED Abstract]
Shipp MA, Abeloff MD, Antman KH, et al.: International Consensus Conference on high-dose therapy with hematopoietic stem-cell transplantation in aggressive non-Hodgkin’s lymphomas: report of the jury. Ann Oncol 10 (1): 13-9, 1999. [PUBMED Abstract]
Zhou Z, Sehn LH, Rademaker AW, et al.: An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 123 (6): 837-42, 2014. [PUBMED Abstract]
Møller MB, Christensen BE, Pedersen NT: Prognosis of localized diffuse large B-cell lymphoma in younger patients. Cancer 98 (3): 516-21, 2003. [PUBMED Abstract]
Maurer MJ, Ghesquières H, Link BK, et al.: Diagnosis-to-Treatment Interval Is an Important Clinical Factor in Newly Diagnosed Diffuse Large B-Cell Lymphoma and Has Implication for Bias in Clinical Trials. J Clin Oncol 36 (16): 1603-1610, 2018. [PUBMED Abstract]
Cuccuini W, Briere J, Mounier N, et al.: MYC+ diffuse large B-cell lymphoma is not salvaged by classical R-ICE or R-DHAP followed by BEAM plus autologous stem cell transplantation. Blood 119 (20): 4619-24, 2012. [PUBMED Abstract]
Johnson NA, Slack GW, Savage KJ, et al.: Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol 30 (28): 3452-9, 2012. [PUBMED Abstract]
Green TM, Young KH, Visco C, et al.: Immunohistochemical double-hit score is a strong predictor of outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol 30 (28): 3460-7, 2012. [PUBMED Abstract]
Horn H, Ziepert M, Becher C, et al.: MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 121 (12): 2253-63, 2013. [PUBMED Abstract]
Canellos GP: CHOP may have been part of the beginning but certainly not the end: issues in risk-related therapy of large-cell lymphoma. J Clin Oncol 15 (5): 1713-6, 1997. [PUBMED Abstract]
Sha C, Barrans S, Cucco F, et al.: Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J Clin Oncol 37 (3): 202-212, 2019. [PUBMED Abstract]
Coiffier B, Altman A, Pui CH, et al.: Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol 26 (16): 2767-78, 2008. [PUBMED Abstract]
Cortes J, Moore JO, Maziarz RT, et al.: Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone–results of a multicenter phase III study. J Clin Oncol 28 (27): 4207-13, 2010. [PUBMED Abstract]
Eyre TA, Savage KJ, Cheah CY, et al.: CNS prophylaxis for diffuse large B-cell lymphoma. Lancet Oncol 23 (9): e416-e426, 2022. [PUBMED Abstract]
Schmitz N, Zeynalova S, Nickelsen M, et al.: CNS International Prognostic Index: A Risk Model for CNS Relapse in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP. J Clin Oncol 34 (26): 3150-6, 2016. [PUBMED Abstract]
Zucca E, Conconi A, Mughal TI, et al.: Patterns of outcome and prognostic factors in primary large-cell lymphoma of the testis in a survey by the International Extranodal Lymphoma Study Group. J Clin Oncol 21 (1): 20-7, 2003. [PUBMED Abstract]
Vitolo U, Chiappella A, Ferreri AJ, et al.: First-line treatment for primary testicular diffuse large B-cell lymphoma with rituximab-CHOP, CNS prophylaxis, and contralateral testis irradiation: final results of an international phase II trial. J Clin Oncol 29 (20): 2766-72, 2011. [PUBMED Abstract]
Boehme V, Schmitz N, Zeynalova S, et al.: CNS events in elderly patients with aggressive lymphoma treated with modern chemotherapy (CHOP-14) with or without rituximab: an analysis of patients treated in the RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Blood 113 (17): 3896-902, 2009. [PUBMED Abstract]
Glantz MJ, Cole BF, Recht L, et al.: High-dose intravenous methotrexate for patients with nonleukemic leptomeningeal cancer: is intrathecal chemotherapy necessary? J Clin Oncol 16 (4): 1561-7, 1998. [PUBMED Abstract]
Puckrin R, El Darsa H, Ghosh S, et al.: Ineffectiveness of high-dose methotrexate for prevention of CNS relapse in diffuse large B-cell lymphoma. Am J Hematol 96 (7): 764-771, 2021. [PUBMED Abstract]
Jeong H, Cho H, Kim H, et al.: Efficacy and safety of prophylactic high-dose MTX in high-risk DLBCL: a treatment intent-based analysis. Blood Adv 5 (8): 2142-2152, 2021. [PUBMED Abstract]
Orellana-Noia VM, Reed DR, McCook AA, et al.: Single-route CNS prophylaxis for aggressive non-Hodgkin lymphomas: real-world outcomes from 21 US academic institutions. Blood 139 (3): 413-423, 2022. [PUBMED Abstract]
Lewis KL, Jakobsen LH, Villa D, et al.: High-dose methotrexate is not associated with reduction in CNS relapse in patients with aggressive B-cell lymphoma: an international retrospective study of 2300 high-risk patients. [Abstract] Blood 138 (Suppl 1): A-181, 2021.
Wilson MR, Eyre TA, Kirkwood AA, et al.: Timing of high-dose methotrexate CNS prophylaxis in DLBCL: a multicenter international analysis of 1384 patients. Blood 139 (16): 2499-2511, 2022. [PUBMED Abstract]
Haddad PA, Hammoud D, Gallagher KM: Effective central nervous system (CNS) prophylaxis chemotherapy approach in high risk diffuse large B-cell lymphoma (DLBCL): a network meta-analysis. [Abstract] Blood 138 (Suppl 1): A-1461, 2021.
Villa D, Connors JM, Shenkier TN, et al.: Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: the impact of the addition of rituximab to CHOP chemotherapy. Ann Oncol 21 (5): 1046-52, 2010. [PUBMED Abstract]
Ferreri AJ, Donadoni G, Cabras MG, et al.: High Doses of Antimetabolites Followed by High-Dose Sequential Chemoimmunotherapy and Autologous Stem-Cell Transplantation in Patients With Systemic B-Cell Lymphoma and Secondary CNS Involvement: Final Results of a Multicenter Phase II Trial. J Clin Oncol 33 (33): 3903-10, 2015. [PUBMED Abstract]
Schmitz N, Wu HS: Advances in the Treatment of Secondary CNS Lymphoma. J Clin Oncol 33 (33): 3851-3, 2015. [PUBMED Abstract]
Treatment of Aggressive, Recurrent B-Cell Non-Hodgkin Lymphoma
Treatment Options for Aggressive, Recurrent B-Cell Non-Hodgkin Lymphoma
In a retrospective review of multiple international trials, 636 patients were identified as having refractory diffuse large B-cell lymphoma (DLBCL), which was defined as progression or stable disease during or just at completion of full-course chemotherapy or relapse within 1 year after autologous stem cell transplant (SCT).[1] With subsequent therapy, the objective response rate was 26%, complete response rate was 7%, median overall survival (OS) was 6.3 months, and only 20% of patients were alive at 2 years. Even with reinduction chemotherapy with planned autologous SCT, outcomes remain poor.[2]
Treatment options for aggressive, recurrent B-cell non-Hodgkin lymphoma include the following:
CAR T-cell therapy for primary refractory disease or relapse within 1 year (or relapse after autologous SCT)
Patients with DLBCL who relapse during or within 2 months of receiving R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) chemotherapy have primary refractory disease. Any patient with disease relapse within 1 year of R-CHOP chemotherapy or with primary refractory disease has a poor prognosis, even with reinduction using chemoimmunotherapy followed by autologous SCT.[1,2] Patients who received CAR T-cell therapy had a 40% to 50% 3-year progression-free survival (PFS) rate with a 40-month follow-up, a result equivalent retrospectively to autologous SCT in bone marrow registries.[3–6]
Three randomized trials compared chemoimmunotherapy followed by autologous SCT with CAR T-cell therapy with or without bridging chemoimmunotherapy for patients with high-risk relapsed disease, defined as primary refractory disease or relapse within 12 months of initial R-CHOP therapy.
Evidence (CAR T-cell therapy):
A prospective randomized trial included 359 patients with primary refractory disease or relapse within 12 months of initial R-CHOP chemotherapy. Patients received the CAR T-cell therapy axicabtagene ciloleucel (axi-cel) with only bridging steroids or second-line chemoimmunotherapy (usually R-ICE [rituximab, ifosfamide, etoposide, and carboplatin] or R-DHAP [rituximab, dexamethasone, high-dose cytarabine, and cisplatin]) followed by autologous SCT.[7,8]
With a median follow-up of 47.2 months, the median OS was not reached in the axi-cel cohort and was 31.1 months in the chemoimmunotherapy cohort. The estimated 4-year OS rate was 54.6% for patients who received axi-cel and 46.0% for patients who received chemoimmunotherapy (hazard ratio [HR]death, 0.73; 95% confidence interval [CI], 0.54–0.98; P = .03).[8][Level of evidence A1]
The median investigator-assessed PFS was 14.7 months in the axi-cel cohort and 3.7 months in the chemotherapy cohort (HR, 0.51; 95% CI, 0.38–0.67).
In the chemoimmunotherapy arm, 64% patients never received autologous SCT during the study because of inadequate response, progression, or death.[7]
Clinically meaningful and statistically significant differences in quality of life were obtained in the CAR T-cell arm at day 100 and day 150, compared with the standard of care.[7][Level of evidence A2]
Grade 3 or 4 cytokine release syndrome occurred in 6% of patients, and grade 3 or 4 neurotoxicity occurred in 21% of patients.
A prospective randomized trial included 184 patients with primary refractory disease or relapse within 12 months of initial R-CHOP chemotherapy. Patients received the CAR T-cell therapy lisocabtagene maraleucel (liso-cel), with 63% of patients receiving bridging therapy or second-line chemoimmunotherapy followed by autologous SCT.[9]
With a median follow-up of 17.5 months, the median PFS was not reached for patients who received liso-cel and was 6.2 months for patients who received chemoimmunotherapy followed by autologous SCT (HR, 0.40; P < .0001).[9][Level of evidence B1]
On the chemoimmunotherapy arm of the study, 53% of patients never received autologous SCT because of inadequate response, progression, or death.[9]
Grade 3 cytokine release syndrome occurred in 1% of patients, and grade 3 neurotoxicity occurred in 4% of patients. There were no grade 4 or 5 occurrences.
A prospective randomized trial included 322 patients with primary refractory disease or relapse within 12 months of initial R-CHOP chemotherapy. Patients received the CAR T-cell therapy tisagenlecleucel, with most patients receiving bridging therapy to achieve response, or second-line chemoimmunotherapy followed by autologous SCT.[10]
There was no difference in event-free survival (EFS) for patients in either arm (HR, 1.07; 95% CI, 0.82–1.40; P = .69).[10][Level of evidence B1]
In the CAR T-cell therapy arm, 48% of patients received two or more cycles of chemoimmunotherapy as part of bridging therapy. This approach to bridging therapy may have led to an unacceptable number of cases of progressive disease.
In summary:
For patients with high-risk relapsing DLBCL with primary refractory disease or relapse within 12 months of R-CHOP-based chemotherapy, axi-cel and liso-cel are superior induction regimens, compared with chemoimmunotherapy with regimens like R-ICE, R-DHAP, and R-GDP (rituximab, gemcitabine, dexamethasone, and cisplatin).
The interval until patients receive CAR T cells must be minimized, optimally by using only steroids, eliminating bridging chemoimmunotherapy, and infusing the CAR T-cell product as quickly as possible.
The preference for CAR T-cell therapy over chemoimmunotherapy followed by autologous SCT does not apply to patients who relapse more than 12 months after R-CHOP therapy.
The American Society of Clinical Oncology (ASCO) has compiled guidelines for the management of adverse events in patients treated with CAR T-cell therapy.[11]
Worse outcomes were reported when apheresis for CAR T-cell therapy occurred just after bendamustine therapy. In a retrospective multicenter review of 439 patients who were infused with CD-19–targeted CAR T cells, 80 patients had received prior bendamustine. With a median follow-up of 20.6 months after CAR T-cell infusion, the patients who had received prior bendamustine had a lower overall response rate (53% vs. 72%, P < .01), worse median PFS (3.1 vs. 6.2 months, P = .04), and worse median OS (4.6 vs. 23.5 months, P < .01).[12][Level of evidence C1]
BMT or SCT consolidation
BMT
BMT consolidation is a treatment option for patients with relapsed lymphoma.[13] Preliminary studies indicate that approximately 20% to 40% of patients will have a long-term disease-free status, but the precise percentage depends on patient selection and the specific treatment used. Preparative drug regimens have varied; some investigators also use total-body irradiation. Similar success has been achieved using autologous marrow, with or without marrow purging, and allogeneic marrow.[14–18]
Evidence (BMT):
In a prospective randomized study (EORTC-PARMA), 215 patients in first or second relapse of aggressive lymphoma, younger than 60 years, and with no bone marrow or central nervous system involvement, were given two cycles of intensive combination chemotherapy. The 109 patients who responded were randomly assigned to receive four more cycles of chemotherapy and involved-field radiation therapy (IF-XRT) versus autologous BMT followed by IF-XRT. With a 5-year median follow-up, the EFS rate was significantly improved with transplant (46% vs. 12%). The OS rate was also significantly better with transplant (53% vs. 32%).[19][Level of evidence A1] Salvage BMT was unsuccessful for patients on the nontransplant arm whose disease relapsed.
In general, patients who responded to initial therapy and who responded to conventional therapy for relapse before the BMT have had the best results.[20]
In a prospective trial, patients who relapsed late (>12 months after diagnosis) had better OS than patients who relapsed earlier (the 8-year survival rate was 29% vs. 13%, P = .001).[21][Level of evidence C1]
Peripheral SCT
Peripheral SCT has yielded results equivalent to standard autologous SCT.[22,23] Even patients who never experienced complete remission with conventional chemotherapy may have prolonged PFS (31% at 5 years) after high-dose chemotherapy and hematopoietic SCT if they retain chemosensitivity to reinduction therapy.[24][Level of evidence C2] Some patients who relapse after a previous autologous SCT can have durable remissions after myeloablative or nonmyeloablative allogeneic SCT.[25,26]; [27][Level of evidence C3] Reduced-intensity conditioning for allogeneic SCT typically involves fludarabine plus busulfan or fludarabine plus cyclophosphamide, with or without 2 Gy of total-body irradiation.[28]
Evidence (peripheral SCT):
In a randomized prospective trial, 396 patients with DLBCL in first relapse or who were refractory to first-line therapy received either R-ICE or R-DHAP followed by autologous SCT.[29]
In a randomized prospective trial, 619 patients with relapsed or refractory aggressive lymphoma received either R-DHAP or R-GDP followed by autologous SCT.[30]
At a median follow-up of 53 months, there was no difference in EFS or OS, but patients who received R-GDP reported less toxicity.[30][Level of evidence A3]
CAR T-cell therapy for relapse after autologous SCT
In the event of disease relapse after autologous SCT, many patients receive consolidation with CAR T-cell therapy.
Multiple trials describe patients with refractory large B-cell lymphoma who underwent an infusion of T cells that were engineered to express a CAR to target the CD19 antigen expressed on the malignant B cells using three different constructs: axi-cel, tisagenlecleucel, and liso-cel.[31–35] Each study reported a complete response rate of 50% to 60% and a 2-year OS rate of 40% to 50%, but the long-term durability of response has yet to be determined in these highly-selected patients.[31–33][Level of evidence C3] This therapy is an option for patients with otherwise refractory or resistant disease. These results have been verified off-study in two reports that included 397 patients treated after U.S. Food and Drug Administration (FDA) approval.[36,37][Level of evidence C3] The highest risk patients who respond adequately may receive a subsequent allogeneic SCT consolidation in some cases if eligible.
ASCO has compiled guidelines for the management of adverse events in patients treated with CAR T-cell therapy.[11]
Tafasitamab plus lenalidomide
Tafasitamab is a humanized anti-CD19 monoclonal antibody with a fucosylated Fc region to enhance antibody-dependent cellular cytotoxicity. Tafasitamab has been studied mostly in combination with lenalidomide.
Evidence (tafasitamab plus lenalidomide):
In a phase II study, 80 patients with SCT-ineligible relapsed or refractory DLBCL were treated with tafasitamab and lenalidomide. The study excluded patients with high-risk cytogenetics (MYC and BCL2 and/or BCL6 rearrangements) and those who had received more than four prior lines of therapy or prior CD19-directed therapy.[38]
The complete response rate was 43% and the objective response rate was 60%.
The FDA approved the combination of tafasitamab and lenalidomide for patients with relapsed or refractory DLBCL.[38][Level of evidence C3] It is unclear if using this CD19-directed therapy interferes with consolidation using CD19-CAR T cells.
Bispecific T-cell engagers
Bispecific T-cell engagers (BiTEs) bind to CD20 (or CD19) and to CD3 to direct T cells to eliminate malignant B cells.[39]
Epcoritamab
Epcoritamab is a CD20-directed BiTE. It is given subcutaneously every 28 days until disease progression or unacceptable toxicity with weekly step-up dosing during cycle 1.
Evidence (epcoritamab):
A phase I/II trial (NCT03625037) included 157 patients with relapsed or refractory DLBCL after two or more prior lines of therapy.[40]
With a median follow-up of 10.7 months, the overall response rate was 63.1% (95% CI, 55.0%–70.6%), and the complete response rate was 38.9% (95% CI, 31.2%–46.9%).[40][Level of evidence C3]
The median PFS was 4.4 months (95% CI, 3.0–7.9).
The median OS was not reached (95% CI, 11.3–not reached).
Cytokine release syndrome occurred in 49.7% of patients, and it was grade 3 or higher in 2.5% of patients. Immune effector cell–associated neurotoxicity syndrome (ICANS) occurred in 6.4% of patients, and it was grade 3 or higher in 0.6% of patients.
Results were not significantly different among 61 recipients of prior CD19-directed CAR T-cell therapy.
Glofitamab
Glofitamab is a CD20-directed BiTE with bivalency for CD20. It is given intravenously every 21 days for a maximum of 12 cycles with weekly step-up dosing during cycle 1.
Evidence (glofitamab):
A phase I/II trial included 155 patients with relapsed or refractory DLBCL after two or more prior lines of therapy.[39]
With a median follow up of 12.6 months, the overall response rate was 52% (95% CI, 43%–60%), and the complete response rate was 39% (95% CI, 32%–48%).[39][Level of evidence C3]
The median PFS was 4.9 months (95% CI, 3.4–8.1).
The estimated 12-month OS rate was 50% (95% CI, 41%–58%).
Cytokine release syndrome occurred in 63% of patients, and it was grade 3 or higher in 4% of patients. ICANS occurred in 8% of patients, and it was grade 3 or higher in 3% of patients.
Results were not significantly different among 52 recipients of prior CD19-directed CAR T-cell therapy.
Polatuzumab vedotin plus rituximab and bendamustine
Polatuzumab vedotin is a CD79b-directed monoclonal antibody conjugated to the cytotoxic agent vedotin (an antibody-drug conjugate).
Evidence (polatuzumab vedotin plus rituximab and bendamustine):
In a randomized, prospective trial, 80 patients with SCT-ineligible relapsed or refractory DLBCL were treated with either polatuzumab vedotin combined with bendamustine and rituximab (BR) or BR alone, with a primary end point of complete response.[41]
The complete response rate by positron emission tomography−computed tomography scan was 40% for the polatuzumab vedotin-BR combination, compared with 18% for BR alone (P = .026).[41]
Similarly, the median PFS was higher for patients who received the polatuzumab vedotin combination (9.5 months) than for the patients who received BR alone (3.7 months) (HR, 0.36; 95% CI, 0.21−0.63; P < .001); the OS was 12.4 months for patients who received the polatuzumab vedotin combination versus 4.7 months for the patients who received BR alone (HR, 0.42; 95% CI, 0.24−0.75; P = .002).[41][Level of evidence C1]
The FDA approved the combination of polatuzumab vedotin and BR for patients with relapsed or refractory DLBCL.
Loncastuximab tesirine
Loncastuximab tesirine is a CD19-directed antibody conjugated to a pyrrolobenzodiazepine dimer cytotoxin (an antibody-drug conjugate).[42]
Evidence (loncastuximab tesirine):
A phase I and subsequent phase II trial included 184 patients with SCT-ineligible relapsed or refractory DLBCL after two or more lines of therapy.
The overall response rate was 48.3% (95% CI, 39.9%–56.7%), and the complete response rate was 24%.[43,44][Level of evidence C3]
Rituximab plus lenalidomide
Evidence (rituximab plus lenalidomide):
In two phase II trials, 49 patients showed a 19% to 35% overall response rate to lenalidomide with rituximab.[45,46][Level of evidence C3]
Palliative radiation therapy
In general, patients with aggressive lymphoma who relapse with indolent histology will benefit from palliative therapy.[47] Palliation may be achieved with very low-dose (4 Gy) IF-XRT for patients with indolent and aggressive relapsed disease.[48]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Crump M, Neelapu SS, Farooq U, et al.: Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood 130 (16): 1800-1808, 2017. [PUBMED Abstract]
Ayers EC, Li S, Medeiros LJ, et al.: Outcomes in patients with aggressive B-cell non-Hodgkin lymphoma after intensive frontline treatment failure. Cancer 126 (2): 293-303, 2020. [PUBMED Abstract]
Schuster SJ, Tam CS, Borchmann P, et al.: Long-term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive B-cell lymphomas (JULIET): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol 22 (10): 1403-1415, 2021. [PUBMED Abstract]
Shah NN, Ahn KW, Litovich C, et al.: Is autologous transplant in relapsed DLBCL patients achieving only a PET+ PR appropriate in the CAR T-cell era? Blood 137 (10): 1416-1423, 2021. [PUBMED Abstract]
Shadman M, Pasquini M, Ahn KW, et al.: Autologous transplant vs chimeric antigen receptor T-cell therapy for relapsed DLBCL in partial remission. Blood 139 (9): 1330-1339, 2022. [PUBMED Abstract]
Cappell KM, Sherry RM, Yang JC, et al.: Long-Term Follow-Up of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy. J Clin Oncol 38 (32): 3805-3815, 2020. [PUBMED Abstract]
Locke FL, Miklos DB, Jacobson CA, et al.: Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N Engl J Med 386 (7): 640-654, 2022. [PUBMED Abstract]
Westin JR, Oluwole OO, Kersten MJ, et al.: Survival with Axicabtagene Ciloleucel in Large B-Cell Lymphoma. N Engl J Med 389 (2): 148-157, 2023. [PUBMED Abstract]
Abramson JS, Solomon SR, Arnason J, et al.: Lisocabtagene maraleucel as second-line therapy for large B-cell lymphoma: primary analysis of the phase 3 TRANSFORM study. Blood 141 (14): 1675-1684, 2023. [PUBMED Abstract]
Bishop MR, Dickinson M, Purtill D, et al.: Second-Line Tisagenlecleucel or Standard Care in Aggressive B-Cell Lymphoma. N Engl J Med 386 (7): 629-639, 2022. [PUBMED Abstract]
Santomasso BD, Nastoupil LJ, Adkins S, et al.: Management of Immune-Related Adverse Events in Patients Treated With Chimeric Antigen Receptor T-Cell Therapy: ASCO Guideline. J Clin Oncol 39 (35): 3978-3992, 2021. [PUBMED Abstract]
Iacoboni G, Navarro V, Martín-López AÁ, et al.: Recent Bendamustine Treatment Before Apheresis Has a Negative Impact on Outcomes in Patients With Large B-Cell Lymphoma Receiving Chimeric Antigen Receptor T-Cell Therapy. J Clin Oncol 42 (2): 205-217, 2024. [PUBMED Abstract]
Shipp MA, Abeloff MD, Antman KH, et al.: International Consensus Conference on high-dose therapy with hematopoietic stem-cell transplantation in aggressive non-Hodgkin’s lymphomas: report of the jury. Ann Oncol 10 (1): 13-9, 1999. [PUBMED Abstract]
Freedman AS, Takvorian T, Anderson KC, et al.: Autologous bone marrow transplantation in B-cell non-Hodgkin’s lymphoma: very low treatment-related mortality in 100 patients in sensitive relapse. J Clin Oncol 8 (5): 784-91, 1990. [PUBMED Abstract]
Phillips GL, Fay JW, Herzig RH, et al.: The treatment of progressive non-Hodgkin’s lymphoma with intensive chemoradiotherapy and autologous marrow transplantation. Blood 75 (4): 831-8, 1990. [PUBMED Abstract]
Chopra R, Goldstone AH, Pearce R, et al.: Autologous versus allogeneic bone marrow transplantation for non-Hodgkin’s lymphoma: a case-controlled analysis of the European Bone Marrow Transplant Group Registry data. J Clin Oncol 10 (11): 1690-5, 1992. [PUBMED Abstract]
Ratanatharathorn V, Uberti J, Karanes C, et al.: Prospective comparative trial of autologous versus allogeneic bone marrow transplantation in patients with non-Hodgkin’s lymphoma. Blood 84 (4): 1050-5, 1994. [PUBMED Abstract]
Mills W, Chopra R, McMillan A, et al.: BEAM chemotherapy and autologous bone marrow transplantation for patients with relapsed or refractory non-Hodgkin’s lymphoma. J Clin Oncol 13 (3): 588-95, 1995. [PUBMED Abstract]
Philip T, Guglielmi C, Hagenbeek A, et al.: Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N Engl J Med 333 (23): 1540-5, 1995. [PUBMED Abstract]
Vellenga E, van Putten WL, van ‘t Veer MB, et al.: Rituximab improves the treatment results of DHAP-VIM-DHAP and ASCT in relapsed/progressive aggressive CD20+ NHL: a prospective randomized HOVON trial. Blood 111 (2): 537-43, 2008. [PUBMED Abstract]
Guglielmi C, Gomez F, Philip T, et al.: Time to relapse has prognostic value in patients with aggressive lymphoma enrolled onto the Parma trial. J Clin Oncol 16 (10): 3264-9, 1998. [PUBMED Abstract]
Vose JM, Anderson JR, Kessinger A, et al.: High-dose chemotherapy and autologous hematopoietic stem-cell transplantation for aggressive non-Hodgkin’s lymphoma. J Clin Oncol 11 (10): 1846-51, 1993. [PUBMED Abstract]
Liberti G, Pearce R, Taghipour G, et al.: Comparison of peripheral blood stem-cell and autologous bone marrow transplantation for lymphoma patients: a case-controlled analysis of the EBMT Registry data. Lymphoma Working Party of the EBMT. Ann Oncol 5 (Suppl 2): 151-3, 1994. [PUBMED Abstract]
Vose JM, Zhang MJ, Rowlings PA, et al.: Autologous transplantation for diffuse aggressive non-Hodgkin’s lymphoma in patients never achieving remission: a report from the Autologous Blood and Marrow Transplant Registry. J Clin Oncol 19 (2): 406-13, 2001. [PUBMED Abstract]
van Kampen RJ, Canals C, Schouten HC, et al.: Allogeneic stem-cell transplantation as salvage therapy for patients with diffuse large B-cell non-Hodgkin’s lymphoma relapsing after an autologous stem-cell transplantation: an analysis of the European Group for Blood and Marrow Transplantation Registry. J Clin Oncol 29 (10): 1342-8, 2011. [PUBMED Abstract]
Freytes CO, Loberiza FR, Rizzo JD, et al.: Myeloablative allogeneic hematopoietic stem cell transplantation in patients who experience relapse after autologous stem cell transplantation for lymphoma: a report of the International Bone Marrow Transplant Registry. Blood 104 (12): 3797-803, 2004. [PUBMED Abstract]
Rezvani AR, Norasetthada L, Gooley T, et al.: Non-myeloablative allogeneic haematopoietic cell transplantation for relapsed diffuse large B-cell lymphoma: a multicentre experience. Br J Haematol 143 (3): 395-403, 2008. [PUBMED Abstract]
Ghosh N, Ahmed S, Ahn KW, et al.: Association of Reduced-Intensity Conditioning Regimens With Overall Survival Among Patients With Non-Hodgkin Lymphoma Undergoing Allogeneic Transplant. JAMA Oncol 6 (7): 1011-1018, 2020. [PUBMED Abstract]
Gisselbrecht C, Glass B, Mounier N, et al.: Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol 28 (27): 4184-90, 2010. [PUBMED Abstract]
Crump M, Kuruvilla J, Couban S, et al.: Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J Clin Oncol 32 (31): 3490-6, 2014. [PUBMED Abstract]
Neelapu SS, Locke FL, Bartlett NL, et al.: Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med 377 (26): 2531-2544, 2017. [PUBMED Abstract]
Schuster SJ, Bishop MR, Tam CS, et al.: Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med 380 (1): 45-56, 2019. [PUBMED Abstract]
Locke FL, Ghobadi A, Jacobson CA, et al.: Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol 20 (1): 31-42, 2019. [PUBMED Abstract]
Abramson JS, Palomba ML, Gordon LI, et al.: Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet 396 (10254): 839-852, 2020. [PUBMED Abstract]
Lin JK, Muffly LS, Spinner MA, et al.: Cost Effectiveness of Chimeric Antigen Receptor T-Cell Therapy in Multiply Relapsed or Refractory Adult Large B-Cell Lymphoma. J Clin Oncol 37 (24): 2105-2119, 2019. [PUBMED Abstract]
Jacobson CA, Hunter BD, Redd R, et al.: Axicabtagene Ciloleucel in the Non-Trial Setting: Outcomes and Correlates of Response, Resistance, and Toxicity. J Clin Oncol 38 (27): 3095-3106, 2020. [PUBMED Abstract]
Nastoupil LJ, Jain MD, Feng L, et al.: Standard-of-Care Axicabtagene Ciloleucel for Relapsed or Refractory Large B-Cell Lymphoma: Results From the US Lymphoma CAR T Consortium. J Clin Oncol 38 (27): 3119-3128, 2020. [PUBMED Abstract]
Salles G, Duell J, González Barca E, et al.: Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol 21 (7): 978-988, 2020. [PUBMED Abstract]
Dickinson MJ, Carlo-Stella C, Morschhauser F, et al.: Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med 387 (24): 2220-2231, 2022. [PUBMED Abstract]
Thieblemont C, Phillips T, Ghesquieres H, et al.: Epcoritamab, a Novel, Subcutaneous CD3xCD20 Bispecific T-Cell-Engaging Antibody, in Relapsed or Refractory Large B-Cell Lymphoma: Dose Expansion in a Phase I/II Trial. J Clin Oncol 41 (12): 2238-2247, 2023. [PUBMED Abstract]
Sehn LH, Herrera AF, Flowers CR, et al.: Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J Clin Oncol 38 (2): 155-165, 2020. [PUBMED Abstract]
Calabretta E, Hamadani M, Zinzani PL, et al.: The antibody-drug conjugate loncastuximab tesirine for the treatment of diffuse large B-cell lymphoma. Blood 140 (4): 303-308, 2022. [PUBMED Abstract]
Caimi PF, Ai W, Alderuccio JP, et al.: Loncastuximab tesirine in relapsed or refractory diffuse large B-cell lymphoma (LOTIS-2): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol 22 (6): 790-800, 2021. [PUBMED Abstract]
Hamadani M, Radford J, Carlo-Stella C, et al.: Final results of a phase 1 study of loncastuximab tesirine in relapsed/refractory B-cell non-Hodgkin lymphoma. Blood 137 (19): 2634-2645, 2021. [PUBMED Abstract]
Zinzani PL, Pellegrini C, Gandolfi L, et al.: Combination of lenalidomide and rituximab in elderly patients with relapsed or refractory diffuse large B-cell lymphoma: a phase 2 trial. Clin Lymphoma Myeloma Leuk 11 (6): 462-6, 2011. [PUBMED Abstract]
Wiernik PH, Lossos IS, Tuscano JM, et al.: Lenalidomide monotherapy in relapsed or refractory aggressive non-Hodgkin’s lymphoma. J Clin Oncol 26 (30): 4952-7, 2008. [PUBMED Abstract]
Lee AY, Connors JM, Klimo P, et al.: Late relapse in patients with diffuse large-cell lymphoma treated with MACOP-B. J Clin Oncol 15 (5): 1745-53, 1997. [PUBMED Abstract]
Haas RL, Poortmans P, de Jong D, et al.: Effective palliation by low dose local radiotherapy for recurrent and/or chemotherapy refractory non-follicular lymphoma patients. Eur J Cancer 41 (12): 1724-30, 2005. [PUBMED Abstract]
Treatment of B-Cell Lymphoblastic Lymphoma/B-Cell Acute Lymphoblastic Leukemia
Lymphoblastic lymphoma (LBL) is a very aggressive form of non-Hodgkin lymphoma, which occurs often but not exclusively in young patients. LBL is the lymphomatous manifestation of acute lymphoblastic leukemia (ALL). The treatment paradigms are based on trials for ALL because LBL and ALL are considered different manifestations of the same biological disease. LBL is commonly associated with large mediastinal masses and has a high tendency to spread to bone marrow and the central nervous system. For more information, see Acute Lymphoblastic Leukemia Treatment.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Treatment of Diffuse Small Noncleaved-Cell/Burkitt Lymphoma
Diffuse small noncleaved-cell/Burkitt lymphoma typically involves younger patients and represents the most common type of pediatric non-Hodgkin lymphoma.[1,2] High-grade B-cell lymphoma, not otherwise specified, includes lymphomas with Burkitt-like or blastoid morphology without double hit cytogenetics, and with germinal center B-cell phenotype.[3] Up to one-half of patients have a single MYC rearrangement. Optimal treatment is poorly defined because the diagnosis is rare. Burkitt lymphoma regimens with central nervous system (CNS) prophylaxis are usually chosen.[3]
Treatment Options for Diffuse Small Noncleaved-Cell/Burkitt Lymphoma
Treatment options for diffuse small noncleaved-cell/Burkitt lymphoma include the following:
Treatment for diffuse small noncleaved-cell/Burkitt lymphoma is usually an aggressive multidrug regimen similar to those used for advanced-stage aggressive lymphomas (such as diffuse large cell).[4–6] Adverse prognostic factors include age older than 40 years, high serum lactate dehydrogenase (>3 times normal), Eastern Cooperative Oncology Group performance status of 2 or greater, and CNS involvement.[2] A retrospective review of 641 adult patients with Burkitt lymphoma from 30 U.S. cancer centers found a 3-year progression-free survival (PFS) rate of 64%. Nineteen percent of patients had CNS involvement, 14% had primary refractory disease, and the treatment-related mortality rate was 10%.[2]
Evidence (aggressive multidrug regimens):
Aggressive combination chemotherapy modeled after that used in childhood Burkitt lymphoma has been successful for adult patients. More than 60% of advanced-stage patients were free of disease at 5 years.[6–9]
Rituximab has been incorporated into these aggressive combination chemotherapy regimens. A nonrandomized, single-arm, prospective, multicenter trial of 363 patients, aged 16 years to 85 years, showed a 5-year PFS rate of 71% and a 5-year overall survival rate of 80%.[5][Level of evidence C1]
CNS prophylaxis
Patients with diffuse small noncleaved-cell/Burkitt lymphoma have a 20% to 30% lifetime risk of CNS involvement. CNS prophylaxis with methotrexate is recommended for all patients and is usually given as four to six intrathecal injections.[10] For more information, see Acute Lymphoblastic Leukemia Treatment.
Evidence (CNS prophylaxis):
In a series of 41 patients treated with systemic and intrathecal chemotherapy, 44% of those who presented with CNS disease and 13% of those who relapsed with CNS involvement became long-term disease-free survivors.[11] CNS relapse patterns were similar whether or not patients received radiation therapy, but increased neurological deficits were noted among those who received radiation therapy.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Blum KA, Lozanski G, Byrd JC: Adult Burkitt leukemia and lymphoma. Blood 104 (10): 3009-20, 2004. [PUBMED Abstract]
Evens AM, Danilov A, Jagadeesh D, et al.: Burkitt lymphoma in the modern era: real-world outcomes and prognostication across 30 US cancer centers. Blood 137 (3): 374-386, 2021. [PUBMED Abstract]
Olszewski AJ, Kurt H, Evens AM: Defining and treating high-grade B-cell lymphoma, NOS. Blood 140 (9): 943-954, 2022. [PUBMED Abstract]
Thomas DA, Faderl S, O’Brien S, et al.: Chemoimmunotherapy with hyper-CVAD plus rituximab for the treatment of adult Burkitt and Burkitt-type lymphoma or acute lymphoblastic leukemia. Cancer 106 (7): 1569-80, 2006. [PUBMED Abstract]
Hoelzer D, Walewski J, Döhner H, et al.: Improved outcome of adult Burkitt lymphoma/leukemia with rituximab and chemotherapy: report of a large prospective multicenter trial. Blood 124 (26): 3870-9, 2014. [PUBMED Abstract]
Roschewski M, Dunleavy K, Abramson JS, et al.: Multicenter Study of Risk-Adapted Therapy With Dose-Adjusted EPOCH-R in Adults With Untreated Burkitt Lymphoma. J Clin Oncol 38 (22): 2519-2529, 2020. [PUBMED Abstract]
Magrath I, Adde M, Shad A, et al.: Adults and children with small non-cleaved-cell lymphoma have a similar excellent outcome when treated with the same chemotherapy regimen. J Clin Oncol 14 (3): 925-34, 1996. [PUBMED Abstract]
Hoelzer D, Ludwig WD, Thiel E, et al.: Improved outcome in adult B-cell acute lymphoblastic leukemia. Blood 87 (2): 495-508, 1996. [PUBMED Abstract]
Mead GM, Sydes MR, Walewski J, et al.: An international evaluation of CODOX-M and CODOX-M alternating with IVAC in adult Burkitt’s lymphoma: results of United Kingdom Lymphoma Group LY06 study. Ann Oncol 13 (8): 1264-74, 2002. [PUBMED Abstract]
Rizzieri DA, Johnson JL, Niedzwiecki D, et al.: Intensive chemotherapy with and without cranial radiation for Burkitt leukemia and lymphoma: final results of Cancer and Leukemia Group B Study 9251. Cancer 100 (7): 1438-48, 2004. [PUBMED Abstract]
Magrath IT, Haddy TB, Adde MA: Treatment of patients with high grade non-Hodgkin’s lymphomas and central nervous system involvement: is radiation an essential component of therapy? Leuk Lymphoma 21 (1-2): 99-105, 1996. [PUBMED Abstract]
Latest Updates to This Summary (05/12/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Editorial changes were made to this summary.
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of adult aggressive B-cell non-Hodgkin lymphoma. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Aggressive B-Cell Non-Hodgkin Lymphoma Treatment are:
Eric J. Seifter, MD (Johns Hopkins University)
Cole H. Sterling, MD (Johns Hopkins University)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Aggressive B-Cell Non-Hodgkin Lymphoma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/lymphoma/hp/aggressive-b-cell-lymphoma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 40203163]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Cancer cells that have absorbed a drug called a photosensitizer. When activated by light, the drug kills the cancer cells.
Credit: National Cancer Institute
What is photodynamic therapy?
Photodynamic therapy uses a drug that is activated by light, called a photosensitizer or photosensitizing agent, to kill cancer cells. The light can come from a laser or other source, such as LEDs. Photodynamic therapy is also called PDT.
Photodynamic therapy is most often used as a local treatment, which means it treats a specific part of the body.
Cancer and precancers treated with photodynamic therapy
The FDA has approved photodynamic therapy to treat:
non-small cell lung cancer when it blocks the airways
How photodynamic therapy treats cancer
When cells that have absorbed photosensitizers are exposed to a specific wavelength of light, the photosensitizer produces a form of oxygen, called an oxygen radical, that kills them.
Photodynamic therapy may also damage blood vessels in the tumor, which prevents it from receiving the blood it needs to keep growing. And, it may trigger the immune system to attack tumor cells, even in other areas of the body.
How photodynamic therapy is given
Photodynamic therapy is a two-step process. First, you will first receive a photosensitizer. The drug may be taken by mouth, spread on the skin, or given through an IV, depending on where the tumor is in the body. After 24 to 72 hours, most of the drug will have left normal cells but remain in cancer or precancer cells. Then your tumor will be exposed to the light source.
How the light is applied depends on where the tumor is. For skin tumors, the light is aimed right at the cancer. For tumors in the throat, airways, and lungs, your doctor will insert an endoscope down your throat. An endoscope is a thin, lighted tube that can help the doctor see inside the body. Once the endoscope is in place, the doctor threads a fiber optic cable that transmits light through it to reach the treatment areas.
One type of photodynamic therapy called extracorporeal photopheresis (ECP) is used to treat abnormal white blood cells that can cause skin symptoms in people with cutaneous T-cell lymphoma. In ECP, a machine collects your blood cells, treats them with a photosensitizer, exposes them to light, and then returns them to your body through a needle in a vein.
Most often, you will have photodynamic therapy as an outpatient, which means you go home after treatment and do not spend the night in the hospital. You may have photodynamic therapy by itself, or you may have it along with other cancer treatments.
Benefits of photodynamic therapy
Photodynamic therapy limits damage to healthy cells because the photosensitizers tend to build up in abnormal cells and the light is focused directly on them.
Photodynamic therapy does not cause scarring, which makes it good for people with skin cancers and precancers.
Drawbacks of photodynamic therapy
Photodynamic therapy can harm normal cells in the treatment area and cause side effects.
The light used in photodynamic therapy can’t pass through more than about 1/3-inch of tissue, or 1 centimeter. So, photodynamic therapy can only be used to treat tumors that are on or just under the skin or on the lining of internal organs or cavities.
Because the light can’t reach very far into large tumors, photodynamic therapy is less helpful in treating them.
Side effects of photodynamic therapy
Damage to normal cells is limited but photodynamic therapy can still cause burns, swelling, pain, and scarring in the treatment area. Other side effects may occur depending on the area that is treated, including:
cough
trouble swallowing
stomach pain
painful breathing
shortness of breath
skin problems, such as redness, stinging, swelling, or itching
A type of photosensitizer called porfimer sodium makes the skin and eyes sensitive to light for about 6 weeks. During this time, you should avoid direct sunlight and bright indoor light.
A small number of hospitals and cancer centers throughout the country have skilled doctors and the machines needed to perform photodynamic therapy. Talk with your doctor or contact hospitals and cancer centers in your area to find out if they are using this treatment.
Photodynamic therapy research
Researchers are looking for ways to expand photodynamic therapy to other cancers, including improving the equipment used and the delivery of the light.
Studies are underway to see if ECP may be used for other blood cancers and to help reduce rejection after stem cell transplants.
Researchers are also developing a new type of PDT called photoimmunotherapy, or PIT. In this treatment, a photosensitizer is combined with an immune protein that delivers the photosynthesizer to cancer cells. When light is applied, the photosynthesizer kills the cancer cells. This process also causes an immune response inside the tumor that can cause more cancer cells to die. Studies of PIT are going on with people with head and neck cancers. Other research is focused on finding photosensitizers that:
are more powerful
target cancer cells more precisely
are triggered by light that can go through tissue to treat deep or large tumors
Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin.
Different types of cancer start in the skin.
Having a fair complexion and being exposed to sunlight are risk factors for basal cell carcinoma and squamous cell carcinoma of the skin.
Basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis often appear as a change in the skin.
Tests or procedures that examine the skin are used to diagnose basal cell carcinoma and squamous cell carcinoma of the skin.
Certain factors affect prognosis (chance of recovery) and treatment options.
Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin.
The skin is the body’s largest organ. It protects against heat, sunlight, injury, and infection. Skin also helps control body temperature and stores water, fat, and vitamin D. The skin has several layers, but the two main layers are the epidermis (upper or outer layer) and the dermis (lower or inner layer). Skin cancer begins in the epidermis, which is made up of three kinds of cells:
Squamous cells: Thin, flat cells that form the top layer of the epidermis.
Basal cells: Round cells under the squamous cells.
Melanocytes: Cells that make melanin and are found in the lower part of the epidermis. Melanin is the pigment that gives skin its natural color. When skin is exposed to the sun, melanocytes make more pigment and cause the skin to darken.
EnlargeAnatomy of the skin showing the epidermis (including the squamous cell and basal cell layers), dermis, subcutaneous tissue, and other parts of the skin.
Skin cancer can occur anywhere on the body, but it is most common in skin that is often exposed to sunlight, such as the face, neck, and hands.
Melanoma is less common than basal cell carcinoma or squamous cell carcinoma. It is more likely to invade nearby tissues and spread to other parts of the body.
This summary is about basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis.
Having a fair complexion and being exposed to sunlight are risk factors for basal cell carcinoma and squamous cell carcinoma of the skin.
Anything that increases a person’s chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop skin cancer, and it will develop in people who don’t have any known risk factors. Talk with your doctor if you think you may be at risk.
Risk factors for basal cell carcinoma and squamous cell carcinoma of the skin include the following:
Being exposed to natural sunlight or artificial sunlight (such as from tanning beds) over long periods of time.
Having a fair complexion, which includes the following:
Fair skin that freckles and burns easily, does not tan, or tans poorly.
Blue, green, or other light-colored eyes.
Red or blond hair.
Although having a fair complexion is a risk factor for skin cancer, people of all skin colors can get skin cancer.
Older age is the main risk factor for most cancers. The chance of getting cancer increases as you get older.
Basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis often appear as a change in the skin.
Not all changes in the skin are a sign of basal cell carcinoma, squamous cell carcinoma of the skin, or actinic keratosis. Check with your doctor if you notice any changes in your skin.
Signs of basal cell carcinoma and squamous cell carcinoma of the skin include the following:
A sore that does not heal.
Areas of the skin that are:
Raised, smooth, shiny, and look pearly.
Firm and look like a scar, and may be white, yellow, or waxy.
Raised and red or reddish-brown.
Scaly, bleeding, or crusty.
Basal cell carcinoma and squamous cell carcinoma of the skin occur most often in areas of the skin exposed to the sun, such as the nose, ears, lower lip, or top of the hands.
Signs of actinic keratosis include the following:
A rough, red, pink, or brown, scaly patch on the skin that may be flat or raised.
Cracking or peeling of the lower lip that is not helped by lip balm or petroleum jelly.
Actinic keratosis occurs most commonly on the face or the top of the hands.
Tests or procedures that examine the skin are used to diagnose basal cell carcinoma and squamous cell carcinoma of the skin.
Skin exam: An exam of the skin for bumps or spots that look abnormal in color, size, shape, or texture.
Skin biopsy: All or part of the abnormal-looking growth is cut from the skin and viewed under a microscope by a pathologist to check for signs of cancer. There are four main types of skin biopsies:
Shave biopsy: A sterile razor blade is used to “shave-off” the abnormal-looking growth.
Punch biopsy: A special instrument called a punch or a trephine is used to remove a circle of tissue from the abnormal-looking growth. EnlargePunch biopsy. A sharp, hollow, circular instrument is used to remove a small, round piece of tissue from a lesion on the skin. The instrument is turned clockwise and counterclockwise to cut about 4 millimeters (mm) down to the layer of fatty tissue below the skin and remove the sample of tissue. Skin thickness is different on different parts of the body.
Treatment options for basal cell carcinoma and squamous cell carcinoma of the skin depend on the following:
The type of cancer.
The stage of the cancer, for squamous cell carcinoma.
The size of the tumor and what part of the body it affects.
The patient’s general health.
Stages of Skin Cancer
Key Points
After squamous cell cancer of the skin has been diagnosed, tests are done to find out if cancer cells have spread within the skin or to other parts of the body.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
Staging for basal cell carcinoma and squamous cell carcinoma of the skin depends on where the cancer formed.
The following stages are used for basal cell carcinoma and squamous cell carcinoma of the skin that is on the head or neck but not on the eyelid:
Stage 0 (Carcinoma in situ)
Stage I
Stage II
Stage III
Stage IV
The following stages are used for basal cell carcinoma and squamous cell carcinoma of the skin on the eyelid:
Stage 0 (Carcinoma in situ)
Stage I
Stage II
Stage III
Stage IV
Treatment depends on the type of skin cancer or other skin condition diagnosed:
Basal cell carcinoma
Squamous cell carcinoma
Actinic keratosis
After squamous cell cancer of the skin has been diagnosed, tests are done to find out if cancer cells have spread within the skin or to other parts of the body.
The process used to find out if cancer has spread within the skin or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment for squamous cell carcinoma of the skin.
Basal cell carcinoma of the skin rarely spreads to other parts of the body. Staging tests to check whether basal cell carcinoma of the skin has spread are usually not needed.
The following tests and procedures may be used in the staging process for squamous cell carcinoma of the skin:
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the head, neck, and chest, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
PET scan (positron emission tomography scan): A procedure to find malignanttumorcells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. Sometimes a PET scan and CT scan are done at the same time.
Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues, such as lymph nodes, or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later. An ultrasound exam of the regional lymph nodes may be done for basal cell carcinoma and squamous cell carcinoma of the skin.
Eye exam with dilatedpupil: An exam of the eye in which the pupil is dilated (opened wider) with medicated eye drops to allow the doctor to look through the lens and pupil to the retina and optic nerve. The inside of the eye, including the retina and the optic nerve, is examined with a light.
Lymph node biopsy: The removal of all or part of a lymph node. A pathologist views the lymph node tissue under a microscope to check for cancer cells. A lymph node biopsy may be done for squamous cell carcinoma of the skin.
There are three ways that cancer spreads in the body.
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if skin cancer spreads to the lung, the cancer cells in the lung are actually skin cancer cells. The disease is metastatic skin cancer, not lung cancer.
Many cancer deaths are caused when cancer moves from the original tumor and spreads to other tissues and organs. This is called metastatic cancer. This animation shows how cancer cells travel from the place in the body where they first formed to other parts of the body.
Staging for basal cell carcinoma and squamous cell carcinoma of the skin depends on where the cancer formed.
Staging for basal cell carcinoma and squamous cell carcinoma of the eyelid is different from staging for basal cell carcinoma and squamous cell carcinoma found on other areas of the head or neck. There is no staging system for basal cell carcinoma or squamous cell carcinoma that is not found on the head or neck.
Surgery to remove the primary tumor and abnormal lymph nodes is done so that tissue samples can be studied under a microscope. This is called pathologic staging and the findings are used for staging as described below. If staging is done before surgery to remove the tumor, it is called clinical staging. The clinical stage may be different from the pathologic stage.
The following stages are used for basal cell carcinoma and squamous cell carcinoma of the skin that is on the head or neck but not on the eyelid:
EnlargeNonmelanoma skin cancer of the head and neck (carcinoma in situ). Abnormal cells are found in the squamous cell or basal cell layer of the epidermis. These abnormal cells may become cancer and spread into nearby normal tissue.
EnlargeStage II nonmelanoma skin cancer of the head and neck. The tumor is larger than 2 centimeters but not larger than 4 centimeters.
Stage III
EnlargeStage III nonmelanoma skin cancer of the head and neck (1). The tumor is (a) larger than 4 centimeters; or cancer has spread to (b) tissue covering the nerves below the dermis; or (c) below the subcutaneous tissue; or (d) the bone and the bone has minor damage. Cancer may have spread to one lymph node on the same side of the body as the tumor and the node is 3 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph node (not shown).
or
EnlargeStage III nonmelanoma skin cancer of the head and neck (2). The tumor is 4 centimeters or smaller. Cancer has spread to one lymph node on the same side of the body as the tumor and the node is 3 centimeters or smaller.
the tumor is larger than 4 centimeters, or cancer has spread to tissue covering the nerves below the dermis, or has spread below the subcutaneous tissue, or has spread to the bone and the bone has minor damage. Cancer may have also spread to one lymph node on the same side of the body as the tumor and the node is 3 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph node; or
the tumor is 4 centimeters or smaller. Cancer has spread to one lymph node on the same side of the body as the tumor and the node is 3 centimeters or smaller.
Stage IV
EnlargeStage IV nonmelanoma skin cancer of the head and neck (1). The tumor is any size. Cancer may have spread to the bone and the bone has minor damage, or to tissue covering the nerves below the dermis, or below the subcutaneous tissue. Cancer has spread to: (a) one lymph node on the same side of the body as the tumor, the node is 3 centimeters or smaller, and cancer has spread through to the outside covering of the lymph node; or (b) one lymph node on the same side of the body as the tumor, the node is larger than 3 centimeters but not larger than 6 centimeters, and cancer has not spread through to the outside covering of the lymph node; or (c) more than one lymph node on the same side of the body as the tumor, the nodes are 6 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph nodes; or (d) one or more lymph nodes on the opposite side of the body as the tumor or on both sides of the body, the nodes are 6 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph nodes.
or
EnlargeStage IV nonmelanoma skin cancer of the head and neck (2). The tumor is any size and cancer has spread to: (a) one lymph node that is larger than 6 centimeters and cancer has not spread through to the outside covering of the lymph node; or (b) one lymph node on the same side of the body as the tumor, the affected node is larger than 3 centimeters, and cancer has spread through to the outside covering of the lymph node; or (c) one lymph node on the opposite side of the body as the tumor, the affected node is any size, and cancer has spread through to the outside covering of the lymph node; or (d) more than one lymph node on one or both sides of the body and cancer has spread through to the outside covering of the lymph nodes.
or
EnlargeStage IV nonmelanoma skin cancer of the head and neck (3). The tumor is any size and cancer has spread to bone marrow or to bone, including the base of the skull, and the bone has been damaged; or cancer has spread to other parts of the body, such as the lung.
the tumor is any size and cancer may have spread to the bone and the bone has minor damage, or to tissue covering the nerves below the dermis, or below the subcutaneous tissue. Cancer has spread to the lymph nodes as follows:
one lymph node on the same side of the body as the tumor, the affected node is 3 centimeters or smaller, and cancer has spread through to the outside covering of the lymph node; or
one lymph node on the same side of the body as the tumor, the affected node is larger than 3 centimeters but not larger than 6 centimeters, and cancer has not spread through to the outside covering of the lymph node; or
more than one lymph node on the same side of the body as the tumor, the affected nodes are 6 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph nodes; or
one or more lymph nodes on the opposite side of the body as the tumor or on both sides of the body, the affected nodes are 6 centimeters or smaller, and cancer has not spread through to the outside covering of the lymph nodes.
the tumor is any size and cancer may have spread to tissue covering the nerves below the dermis, or below the subcutaneous tissue, or to bone marrow or to bone, including the bottom of the skull. Also:
cancer has spread to one lymph node that is larger than 6 centimeters and cancer has not spread through to the outside covering of the lymph node; or
cancer has spread to one lymph node on the same side of the body as the tumor, the affected node is larger than 3 centimeters, and cancer has spread through to the outside covering of the lymph node; or
cancer has spread to one lymph node on the opposite side of the body as the tumor, the affected node is any size, and cancer has spread through to the outside covering of the lymph node; or
cancer has spread to more than one lymph node on one or both sides of the body and cancer has spread through to the outside covering of the lymph nodes.
the tumor is any size and cancer has spread to bone marrow or to bone, including the bottom of the skull, and the bone has been damaged. Cancer may have also spread to the lymph nodes; or
cancer has spread to other parts of the body, such as the lung.
The following stages are used for basal cell carcinoma and squamous cell carcinoma of the skin on the eyelid:
Stage 0 (Carcinoma in situ)
In stage 0, abnormalcells are found in the epidermis, usually in the basal cell layer. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage I
In stage I, cancer has formed. Stage I is divided into stages IA and IB.
Stage IA: The tumor is 10 millimeters or smaller and may have spread to the edge of the eyelid where the lashes are, to the connective tissue in the eyelid, or to the full thickness of the eyelid.
Stage IB: The tumor is larger than 10 millimeters but not larger than 20 millimeters and the tumor has not spread to the edge of the eyelid where the lashes are, or to the connective tissue in the eyelid.
the tumor is larger than 10 millimeters but not larger than 20 millimeters and has spread to the edge of the eyelid where the lashes are, to the connective tissue in the eyelid, or to the full thickness of the eyelid; or
the tumor is larger than 20 millimeters but not larger than 30 millimeters and may have spread to the edge of the eyelid where the lashes are, to the connective tissue in the eyelid, or to the full thickness of the eyelid.
In stage IIB, the tumor may be any size and has spread to the eye, eye socket, sinuses, tear ducts, or brain, or to the tissues that support the eye.
Stage IIIA: The tumor may be any size and may have spread to the edge of the eyelid where the lashes are, to the connective tissue in the eyelid, or to the full thickness of the eyelid, or to the eye, eye socket, sinuses, tear ducts, or brain, or to the tissues that support the eye. Cancer has spread to one lymph node on the same side of the body as the tumor and the node is 3 centimeters or smaller.
Stage IIIB: The tumor may be any size and may have spread to the edge of the eyelid where the lashes are, to the connective tissue in the eyelid, or to the full thickness of the eyelid, or to the eye, eye socket, sinuses, tear ducts, or brain, or to the tissues that support the eye. Cancer has spread to lymph nodes as follows:
one lymph node on the same side of the body as the tumor and the node is larger than 3 centimeters; or
more than one lymph node on the opposite side of the body as the tumor or on both sides of the body.
Stage IV
In stage IV, the tumor has spread to other parts of the body, such as the lung or liver.
Treatment depends on the type of skin cancer or other skin condition diagnosed:
Basal cell carcinoma
EnlargeBasal cell carcinoma. A skin cancer lesion that looks reddish brown and slightly raised (left panel) and a skin cancer lesion that looks like an open sore with a pearly rim (right panel).
Basal cell carcinoma is the most common type of skin cancer. It usually occurs on areas of the skin that have been in the sun, most often the nose. Often this cancer appears as a raised bump that looks smooth and pearly. A less common type looks like a scar or it is flat and firm and may be skin-colored, yellow, or waxy. Basal cell carcinoma may spread to tissues around the cancer, but it usually does not spread to other parts of the body.
Squamous cell carcinoma
EnlargeSquamous cell carcinoma. A skin cancer lesion on the face that looks raised and crusty (left panel) and a skin cancer lesion on the leg that looks pink and raised (right panel).
Squamous cell carcinoma occurs on areas of the skin that have been damaged by the sun, such as the ears, lower lip, and the back of the hands. Squamous cell carcinoma may also appear on areas of the skin that have been sunburned or exposed to chemicals or radiation. Often this cancer looks like a firm red bump. The tumor may feel scaly, bleed, or form a crust. Squamous cell tumors may spread to nearby lymph nodes. Squamous cell carcinoma that has not spread can usually be cured.
Actinic keratosis
Actinic keratosis is a skin condition that is not cancer, but sometimes changes into squamous cell carcinoma. One or more lesions may occur in areas that have been exposed to the sun, such as the face, the back of the hands, and the lower lip. It looks like rough, red, pink, or brown scaly patches on the skin that may be flat or raised, or as a cracked and peeling lower lip that is not helped by lip balm or petroleum jelly. Actinic keratosis may disappear without treatment.
Treatment Option Overview
Key Points
There are different types of treatment for patients with basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis.
The following types of treatment are used:
Surgery
Radiation therapy
Chemotherapy
Photodynamic therapy
Immunotherapy
Targeted therapy
Chemical peel
Other drug therapy
New types of treatment are being tested in clinical trials.
Treatment for skin cancer may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis.
Different types of treatment are available for patients with basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
The following types of treatment are used:
Surgery
One or more of the following surgical procedures may be used to treat basal cell carcinoma, squamous cell carcinoma of the skin, or actinic keratosis:
Simple excision: The tumor, along with some of the normal tissue around it, is cut from the skin.
Mohs micrographic surgery: The tumor is cut from the skin in thin layers. During the procedure, the edges of the tumor and each layer of tumor removed are viewed through a microscope to check for cancer cells. Layers continue to be removed until no more cancer cells are seen. This type of surgery removes as little normal tissue as possible. It is often used to remove skin cancer on the face, fingers, or genitals and skin cancer that does not have a clear border. EnlargeMohs surgery. A surgical procedure to remove skin cancer in several steps. First, a thin layer of cancerous tissue is removed. Then, a second thin layer of tissue is removed and viewed under a microscope to check for cancer cells. More layers are removed one at a time until the tissue viewed under a microscope shows no remaining cancer. This type of surgery is used to remove as little normal tissue as possible and is often used to remove skin cancer on the face.
Shave excision: The abnormal area is shaved off the surface of the skin with a small blade.
Curettage and electrodesiccation: The tumor is cut from the skin with a curette (a sharp, spoon-shaped tool). A needle-shaped electrode is then used to treat the area with an electric current that stops the bleeding and destroys cancer cells that remain around the edge of the wound. The process may be repeated one to three times during the surgery to remove all of the cancer. This type of treatment is also called electrosurgery.
Cryosurgery: A treatment that uses an instrument to freeze and destroy abnormal tissue, such as carcinoma in situ. This type of treatment is also called cryotherapy. EnlargeCryosurgery. An instrument with a nozzle is used to spray liquid nitrogen or liquid carbon dioxide to freeze and destroy abnormal tissue.
Laser surgery: A surgical procedure that uses a laser beam (a narrow beam of intense light) as a knife to make bloodless cuts in tissue or to remove a surface lesion such as a tumor.
Dermabrasion: Removal of the top layer of skin using a rotating wheel or small particles to rub away skin cells.
Simple excision, Mohs micrographic surgery, curettage and electrodesiccation, and cryosurgery are used to treat basal cell carcinoma and squamous cell carcinoma of the skin. Laser surgery is rarely used to treat basal cell carcinoma. Simple excision, shave excision, curettage and desiccation, dermabrasion, and laser surgery are used to treat actinic keratosis.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
External radiation therapy is used to treat basal cell carcinoma and squamous cell carcinoma of the skin.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing.
Chemotherapy for basal cell carcinoma, squamous cell carcinoma of the skin, and actinic keratosis is usually topical (applied to the skin in a cream or lotion). Topical fluorouracil (5-FU) is used to treat basal cell carcinoma.
Photodynamic therapy (PDT) is a cancer treatment that uses a drug and a certain type of light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein or put on the skin. The drug collects more in cancer cells than in normal cells. For skin cancer, laser light is shined onto the skin and the drug becomes active and kills the cancer cells. Photodynamic therapy causes little damage to healthy tissue.
Photodynamic therapy is also used to treat actinic keratoses.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer.
There are different types of immunotherapy used to treat skin cancer:
Immune checkpoint inhibitors block proteins called checkpoints that are made by some types of immune system cells, such as T cells, and some cancer cells. PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells.
Cemiplimab and pembrolizumab are types of PD-1 inhibitors used to treat squamous cell carcinoma of the skin that is locally advanced or has spread to other parts of the body.
EnlargeImmune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
Immunotherapy uses the body’s immune system to fight cancer. This animation explains one type of immunotherapy that uses immune checkpoint inhibitors to treat cancer.
Interferon (by injection) may be used to treat squamous cell carcinoma of the skin.
Topicalimiquimod therapy is an immune response modifier that may be used to treat some basal cell carcinomas and is applied to the skin as a cream.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells.
Signal transduction inhibitor therapy: This treatment block signals that are passed from one molecule to another inside a cell. Blocking these signals may kill cancer cells. Vismodegib and sonidegib are signal transduction inhibitors used to treat basal cell carcinoma.
A chemical peel is a procedure used to improve the way certain skin conditions look. A chemical solution is put on the skin to dissolve the top layers of skin cells. Chemical peels may be used to treat actinic keratosis. This type of treatment is also called chemabrasion and chemexfoliation.
Other drug therapy
Retinoids (drugs related to vitamin A) are sometimes used to treat squamous cell carcinoma of the skin. Diclofenac and ingenol are topical drugs used to treat actinic keratosis.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
If basal cell carcinoma and squamous cell carcinoma recur (come back), it is usually within 5 years of initial treatment. Talk to your doctor about how often you should have your skin checked for signs of cancer.
Treatment of recurrent basal cell carcinoma that is not metastatic may include the following:
Simple excision.
Mohs micrographic surgery.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of recurrent squamous cell carcinoma that is not metastatic may include the following:
Simple excision.
Mohs micrographic surgery.
Radiation therapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of skin cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Skin Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/skin/patient/skin-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389265]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
EnlargeBlood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
In mycosis fungoides, T-cell lymphocytes become cancerous and affect the skin. When these lymphocytes occur in the blood, they are called Sézary cells. In Sézary syndrome, cancerous T-cell lymphocytes affect the skin and large numbers of Sézary cells are found in the blood.
Mycosis fungoides and Sézary syndrome are types of cutaneous T-cell lymphoma.
Mycosis fungoides and Sézary syndrome are the two most common types of cutaneous T-cell lymphoma (a type of non-Hodgkin lymphoma). For information about other types of skin cancer or non-Hodgkin lymphoma, see the following PDQ summaries:
A sign of mycosis fungoides is a red rash on the skin.
Mycosis fungoides may go through the following phases:
Premycotic phase: A scaly, red rash in areas of the body that usually are not exposed to the sun. This rash does not cause symptoms and may last for months or years. It is hard to diagnose the rash as mycosis fungoides during this phase.
Plaque phase: Small raised bumps (papules) or hardened lesions on the skin, which may be reddened.
Tumor phase: Tumors form on the skin. These tumors may develop ulcers and the skin may get infected.
Check with your doctor if you have any of these signs.
In Sézary syndrome, cancerous T-cells are found in the blood.
Also, skin all over the body is reddened, itchy, peeling, and painful. There may also be patches, plaques, or tumors on the skin. It is not known if Sézary syndrome is an advanced form of mycosis fungoides or a separate disease.
Tests that examine the skin and blood are used to diagnose mycosis fungoides and Sézary syndrome.
The following tests and procedures may be used:
Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps, the number and type of skin lesions, or anything else that seems unusual. Pictures of the skin and a history of the patient’s health habits and past illnesses and treatments will also be taken.
The portion of the blood sample made up of red blood cells.
EnlargeComplete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions.
Sézary blood cell count: A procedure in which a sample of blood is viewed under a microscope to count the number of Sézary cells.
HIV test: A test to measure the level of HIV antibodies in a sample of blood. Antibodies are made by the body when it is invaded by a foreign substance. A high level of HIV antibodies may mean the body has been infected with HIV.
Skin biopsy: The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. The doctor may remove a growth from the skin, which will be examined by a pathologist. More than one skin biopsy may be needed to diagnose mycosis fungoides. Other tests that may be done on the cells or tissue sample include the following:
Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of lymphoma.
Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
T-cell receptor (TCR) gene rearrangement test: A laboratory test in which cells in a sample of blood or bone marrow are checked to see if there are certain changes in the genes that make receptors on T cells (white blood cells). Testing for these gene changes can tell whether large numbers of T cells with a certain T-cell receptor are being made.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
Mycosis fungoides and Sézary syndrome are hard to cure. Treatment is usually palliative, to relieve symptoms and improve the quality of life. Patients with earlystage disease may live many years.
Stages of Mycosis Fungoides (Including Sézary Syndrome)
Key Points
After mycosis fungoides and Sézary syndrome have been diagnosed, tests are done to find out if cancer cells have spread from the skin to other parts of the body.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
The following stages are used for mycosis fungoides and Sézary syndrome:
Stage I Mycosis Fungoides
Stage II Mycosis Fungoides
Stage III Mycosis Fungoides
Stage IV Mycosis Fungoides/Sézary Syndrome
Mycosis fungoides and Sézary syndrome can recur (come back) after they have been treated.
After mycosis fungoides and Sézary syndrome have been diagnosed, tests are done to find out if cancer cells have spread from the skin to other parts of the body.
The process used to find out if cancer has spread from the skin to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following procedures may be used in the staging process:
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the lymph nodes, chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
PET scan (positron emission tomography scan): A procedure to find malignanttumorcells in the body. A small amount of radioactiveglucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow and bone under a microscope to look for signs of cancer.
There are three ways that cancer spreads in the body.
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if mycosis fungoides spreads to the liver, the cancer cells in the liver are actually mycosis fungoides cells. The disease is metastatic mycosis fungoides, not liver cancer.
Many cancer deaths are caused when cancer moves from the original tumor and spreads to other tissues and organs. This is called metastatic cancer. This animation shows how cancer cells travel from the place in the body where they first formed to other parts of the body.
The following stages are used for mycosis fungoides and Sézary syndrome:
Stage I Mycosis Fungoides
Stage I is divided into stages IA and IB as follows:
There may be a low number of Sézary cells in the blood.
Stage IV Mycosis Fungoides/Sézary Syndrome
When there is a high number of Sézary cells in the blood, the disease is called Sézary syndrome.
Stage IV is divided into stages IVA1, IVA2, and IVB as follows:
Stage IVA1: Patches, papules, plaques, or tumors may cover any amount of the skin surface, and 80% or more of the skin surface may be reddened. The lymph nodes may be abnormal, but they are not cancerous. There is a high number of Sézary cells in the blood.
Stage IVA2: Patches, papules, plaques, or tumors may cover any amount of the skin surface, and 80% or more of the skin surface may be reddened. The lymph nodes are very abnormal, or cancer has formed in the lymph nodes. There may be a high number of Sézary cells in the blood.
Stage IVB: Cancer has spread to other organs in the body, such as the spleen or liver. Patches, papules, plaques, or tumors may cover any amount of the skin surface, and 80% or more of the skin surface may be reddened. The lymph nodes may be abnormal or cancerous. There may be a high number of Sézary cells in the blood.
Mycosis fungoides and Sézary syndrome can recur (come back) after they have been treated.
Mycosis fungoides and Sézary syndrome may come back in the skin or in other parts of the body, such as the spleen or liver.
Treatment Option Overview
Key Points
There are different types of treatment for patients with mycosis fungoides and cancer.
Seven types of standard treatment are used:
Photodynamic therapy
Radiation therapy
Chemotherapy
Other drug therapy
Immunotherapy
Targeted therapy
High-dose chemotherapy and radiation therapy with stem cell transplant
New types of treatment are being tested in clinical trials.
Immune checkpoint inhibitor therapy
Treatment for mycosis fungoides and Sézary syndrome may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with mycosis fungoides and cancer.
Different types of treatment are available for patients with mycosis fungoides and . Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Seven types of standard treatment are used:
Photodynamic therapy
Photodynamic therapy is a cancer treatment that uses a drug and a certain type of laser light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein. The drug collects more in cancer cells than in normal cells. For skin cancer, laser light is shined onto the skin and the drug becomes active and kills the cancer cells. Photodynamic therapy causes little damage to healthy tissue. Patients undergoing photodynamic therapy will need to limit the amount of time spent in sunlight. There are different types of photodynamic therapy:
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Sometimes, total skin electron beam (TSEB) radiation therapy is used to treat mycosis fungoides and Sézary syndrome. This is a type of external radiation treatment in which a radiation therapy machine aims electrons (tiny, invisible particles) at the skin covering the whole body . External radiation therapy may also be used as palliative therapy to relieve symptoms and improve quality of life.
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). Sometimes the chemotherapy is topical (put on the skin in a cream, lotion, or ointment).
Topical corticosteroids are used to relieve red, swollen, and inflamed skin. They are a type of steroid. Topical corticosteroids may be in a cream, lotion, or ointment.
Retinoids, such as bexarotene, are drugs related to vitamin A that can slow the growth of certain types of cancer cells. The retinoids may be taken by mouth or put on the skin.
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This cancer treatment is a type of biologic therapy.
Interferon: This treatment interferes with the division of mycosis fungoides and Sézary cells and can slow tumor growth.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do.
Monoclonal antibodies: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Types of monoclonal antibodies include:
Brentuximab vedotin, which contains a monoclonal antibody that binds to a protein, called CD30, found on some types of lymphoma cells. It also contains an anticancer drug that may help kill cancer cells.
Mogamulizumab, which contains a monoclonal antibody that binds to a protein, called CCR4, found on some types of lymphoma cells. It may block this protein and help the immune system kill cancer cells. It is used to treat mycosis fungoides and Sézary syndrome that came back or did not get better after treatment with at least one systemic therapy.
How do monoclonal antibodies work to treat cancer? This video shows how monoclonal antibodies, such as trastuzumab, pembrolizumab, and rituximab, block molecules cancer cells need to grow, flag cancer cells for destruction by the body’s immune system, or deliver harmful substances to cancer cells.
High-dose chemotherapy and radiation therapy with stem cell transplant
High doses of chemotherapy and sometimes radiation therapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy and radiation therapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body’s blood cells.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Immune checkpoint inhibitor therapy
Immune checkpoint inhibitortherapy: Immune checkpoint inhibitors block proteins called checkpoints that are made by some types of immune system cells, such as T cells, and some cancer cells. These checkpoints help keep immune responses from being too strong and sometimes can keep T cells from killing cancer cells. When these checkpoints are blocked, T cells can kill cancer cells better.
PD-1 and PD-L1 inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells. Pembrolizumab is a type of PD-1 inhibitor.
EnlargeImmune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
Immunotherapy uses the body’s immune system to fight cancer. This animation explains one type of immunotherapy that uses immune checkpoint inhibitors to treat cancer.
Information about clinical trials is available from the NCI website.
Treatment for mycosis fungoides and Sézary syndrome may cause side effects.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Treatment of Stage I and Stage II Mycosis Fungoides
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage III and Stage IV Mycosis Fungoides (Including Sézary Syndrome)
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment Recurrent Mycosis Fungoides (Including and Sézary Syndrome)
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Mycosis Fungoides Sézary Syndrome
For more information from the National Cancer Institute about mycosis fungoides and Sézary syndrome, see the following:
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of mycosis fungoides (including Sézary Syndrome). It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Mycosis Fungoides (Including Sézary Syndrome) Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/lymphoma/patient/mycosis-fungoides-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389317]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
EnlargeThe lymph system is part of the body’s immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, adenoids (not shown), thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph tissue is also found in many other parts of the body, including the small intestine.
Having a weakened immune system may increase the risk of developing primary CNS lymphoma.
Anything that increases a person’s chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop primary CNS lymphoma, and it will develop in people who don’t have any known risk factors. Talk with your doctor if you think you may be at risk.
Signs and symptoms of primary CNS lymphoma may include nausea and vomiting or seizures.
These and other signs and symptoms may be caused by primary CNS lymphoma or by other conditions. Check with your doctor if you have any of the following:
Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks a person’s mental status, coordination, ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
Eye exam with dilatedpupil: An exam of the eye in which the pupil is dilated (enlarged) with medicated eye drops to allow the doctor to look through the lens and pupil to the retina. The inside of the eye, including the retina and the optic nerve, is checked. Pictures may be taken over time to keep track of changes in the size of the tumor. There are several types of eye exams:
Ophthalmoscopy: An exam of the inside of the back of the eye to check the retina and optic nerve using a small magnifying lens and a light.
Slit-lamp biomicroscopy: An exam of the inside of the eye to check the retina, optic nerve, and other parts of the eye using a strong beam of light and a microscope.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. A substance called gadolinium is injected into the patient through a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. A higher than normal amount of protein or lower than normal amount of glucose may be a sign of a tumor. This procedure is also called an LP or spinal tap. EnlargeLumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing.
Stereotactic biopsy: A biopsy procedure that uses a computer and a 3-dimensional (3-D) scanning device to find a tumor site and guide the removal of tissue so it can be viewed under a microscope to check for signs of cancer.
The following tests may be done on the samples of tissue that are removed:
Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient’s tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
Cytogeneticanalysis: A laboratory test in which the chromosomes of cells in a sample of blood or bone marrow are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
FISH (fluorescence in situ hybridization): A laboratory test used to look at and count genes or chromosomes in cells and tissues. Pieces of DNA that contain fluorescent dyes are made in the laboratory and added to a sample of a patient’s cells or tissues. When these dyed pieces of DNA attach to certain genes or areas of chromosomes in the sample, they light up when viewed under a fluorescent microscope. The FISH test is used to help diagnose cancer and help plan treatment.
The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
The portion of the blood sample made up of red blood cells.
EnlargeComplete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions.
Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
HIV test: A test to measure the level of HIV antibodies in a sample of blood. Antibodies are made by the body when it is invaded by a foreign substance. A high level of HIV antibodies may mean the body has been infected with HIV.
Certain factors affect prognosis (chance of recovery) and treatment options.
Whether the tumor is in the central nervous system, eye, or both.
The level of certain substances in the blood and cerebrospinal fluid (CSF).
Treatment options depend on the following:
Whether the tumor is in the central nervous system, eye, or both.
The patient’s age and general health.
Whether the cancer has just been diagnosed or has recurred (come back).
Treatment of primary CNS lymphoma works best when the tumor has not spread outside the cerebrum (the largest part of the brain) and the patient is younger than 60 years, able to carry out most daily activities, and does not have AIDS or other diseases that weaken the immune system.
Staging Primary CNS Lymphoma
Key Points
After primary central nervous system (CNS) lymphoma has been diagnosed, tests are done to find out if cancer cells have spread within the brain and spinal cord or to the eye.
There is no standard staging system for primary CNS lymphoma.
Primary CNS lymphoma often recurs (comes back) after it has been treated.
After primary central nervous system (CNS) lymphoma has been diagnosed, tests are done to find out if cancer cells have spread within the brain and spinal cord or to the eye.
Primary CNS lymphoma usually does not spread beyond the central nervous system or the eye. The process used to find out if cancer has spread is called staging. There is no standard system for staging primary CNS lymphoma.
The following tests and procedures may be used to help plan treatment:
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
PET scan (positron emission tomography scan): A procedure to find malignanttumorcells in the body. A small amount of radioactiveglucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. A PET scan and CT scan may be done at the same time. This is called a PET-CT.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for signs of cancer. EnlargeBone marrow aspiration and biopsy. After a small area of skin is numbed, a long, hollow needle is inserted through the patient’s skin and hip bone into the bone marrow. A sample of bone marrow and a small piece of bone are removed for examination under a microscope.
There is no standard staging system for primary CNS lymphoma.
Primary CNS lymphoma often recurs (comes back) after it has been treated.
There are different types of treatment for patients with primary central nervous system (CNS) lymphoma.
The following types of treatments are used:
Radiation therapy
Chemotherapy
Steroid therapy
Targeted therapy
High-dose chemotherapy with stem cell transplant
Immunotherapy
New types of treatment are being tested in clinical trials.
Treatment for primary CNS lymphoma may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with primary central nervous system (CNS) lymphoma.
Different types of treatment are available for patients with primary CNS lymphoma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Surgery is not used to treat primary CNS lymphoma.
The following types of treatments are used:
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Because primary CNS lymphoma spreads throughout the brain, external radiation therapy is given to the whole brain. This is called whole-brain radiation therapy.
High-dose radiation therapy to the brain can damage healthy tissue and cause disorders that can affect thinking, learning, problem solving, reading, writing, speech, and memory. Clinical trials have tested the use of chemotherapy alone or before radiation therapy to reduce the damage to healthy brain tissue that occurs with the use of radiation therapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid (intrathecal chemotherapy), an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy).
The way the chemotherapy is given depends on where the tumor is in the CNS or eye. Primary CNS lymphoma may be treated with systemic chemotherapy, intrathecal chemotherapy, and/or intraventricular chemotherapy, in which anticancer drugs are placed into the ventricles (fluid-filled cavities) of the brain. If primary CNS lymphoma is found in the eye, anticancer drugs are injected directly into the vitreous humor (jelly-like substance) inside the eye.
EnlargeIntrathecal chemotherapy. Anticancer drugs are injected into the intrathecal space, which is the space that holds the cerebrospinal fluid (CSF, shown in blue). There are two different ways to do this. One way, shown in the top part of the figure, is to inject the drugs into an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). The other way, shown in the bottom part of the figure, is to inject the drugs directly into the CSF in the lower part of the spinal column, after a small area on the lower back is numbed.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells.
Monoclonal antibodies: Monoclonal antibodies are immune systemproteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Rituximab and nivolumab are types of monoclonal antibodies used to treat newly diagnosed or recurrent primary CNS lymphoma.
How do monoclonal antibodies work to treat cancer? This video shows how monoclonal antibodies, such as trastuzumab, pembrolizumab, and rituximab, block molecules cancer cells need to grow, flag cancer cells for destruction by the body’s immune system, or deliver harmful substances to cancer cells.
Tyrosine kinase inhibitors: These small-molecule drugs go through the cell membrane and work inside cancer cells to block signals that cancer cells need to grow and divide. Ibrutinib is a type of tyrosine kinase inhibitor used to treat newly diagnosed or recurrent primary CNS lymphoma.
High-dose chemotherapy with stem cell transplant
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body’s blood cells.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer.
CAR T-cell therapy: This treatment changes the patient’s T cells (a type of immune system cell) so they will attack certain proteins on the surface of cancer cells. T cells are taken from the patient, and special receptors are added to their surface in the laboratory. The changed cells are called chimeric antigen receptor (CAR) T cells. The CAR T cells are grown in the laboratory and given to the patient by infusion. The CAR T cells multiply in the patient’s blood and attack cancer cells. EnlargeCAR T-cell therapy. A type of treatment in which a patient’s T cells (a type of immune cell) are changed in the laboratory so they will bind to cancer cells and kill them. Blood from a vein in the patient’s arm flows through a tube to an apheresis machine (not shown), which removes the white blood cells, including the T cells, and sends the rest of the blood back to the patient. Then, the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. Millions of the CAR T cells are grown in the laboratory and then given to the patient by infusion. The CAR T cells are able to bind to an antigen on the cancer cells and kill them.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for primary CNS lymphoma may cause side effects.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
A clinical trial of high-dose chemotherapy followed by whole-brain radiation therapy, stem cell transplant, and/or targeted therapy.
A clinical trial of chemotherapy with or without stem cell transplant.
A clinical trial of targeted therapy (rituximab and ibrutinib) and chemotherapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of primary CNS lymphoma. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Primary CNS Lymphoma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/lymphoma/patient/primary-cns-lymphoma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389274]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.

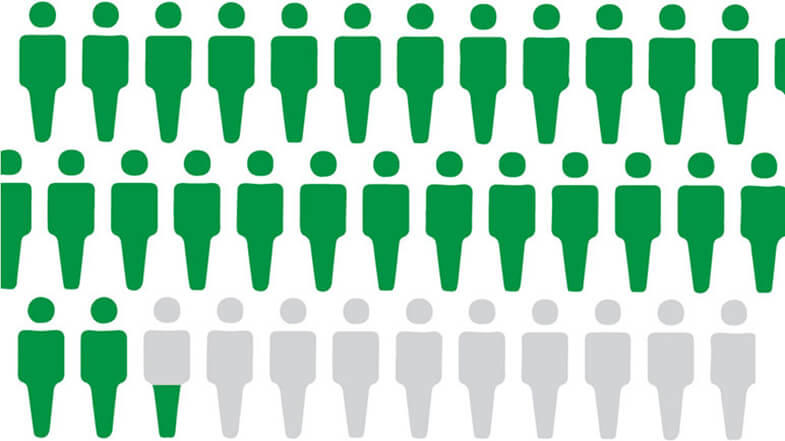
, and antibodies. Also shown is red marrow inside bone, where plasma cells are made.")

: Drawing of stem cells being collected from a donor's bloodstream using an apheresis machine. Blood is removed from a vein in the donor's arm and flows through the machine where the stem cells are removed. The rest of the blood is then returned to the donor through a vein in their other arm. (Panel 2): Drawing of a health care provider giving a patient an infusion of chemotherapy through a catheter in the patient's chest. The chemotherapy is given to kill cancer cells and prepare the patient's body for the donor stem cells. (Panel 3): Drawing of a patient receiving an infusion of the donor stem cells through a catheter in the chest.")
 being made in the laboratory; the gene for CAR is inserted into the T cells and then millions of CAR T cells are grown. Drawing also shows the CAR T cells being given to the patient by infusion and binding to antigens on the cancer cells and killing them.")
. A lymphoid stem cell becomes a lymphoblast and then becomes a B-lymphocyte, T-lymphocyte, or natural killer cell.")
. There are also two pullouts: one showing a close up of the inside structure of a lymph node and the attached artery, vein, and lymph vessels with arrows showing how the lymph (clear, watery fluid) moves into and out of the lymph node, and another showing a close up of bone marrow with blood cells.")




 the top left panel shows cancer in the liver; (b) the top right panel shows cancer in the left lung and in two groups of lymph nodes below the diaphragm; (c) the bottom left panel shows cancer in the left lung and in a group of lymph nodes above the diaphragm and below the diaphragm; and (d) the bottom right panel shows cancer in both lungs, the liver, and the bone marrow (pullout). Also shown is primary cancer in the lymph nodes and a pullout of the brain with cerebrospinal fluid (in blue).")
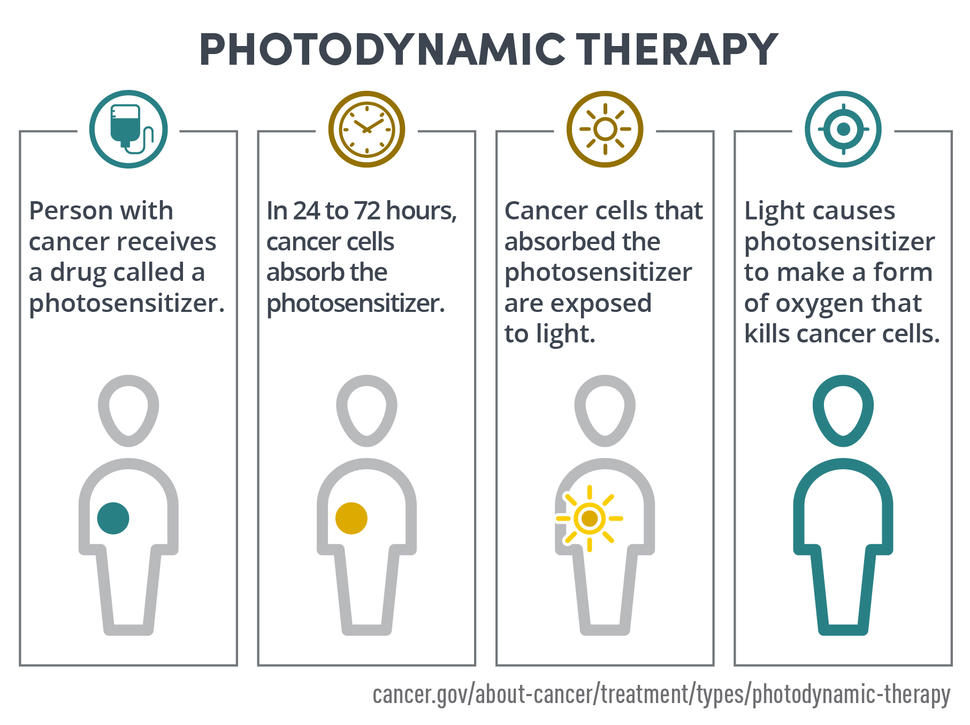
, dermis, and subcutaneous tissue. Also shown are the hair shafts, hair follicles, oil glands, lymph vessels, nerves, fatty tissue, veins, arteries, and sweat glands.")
 down to the layer of fatty tissue below the skin.")
; drawing shows abnormal squamous cells and basal cells in the epidermis. Also shown are the dermis and the subcutaneous tissue below the dermis. There are two insets: the inset on the left shows a close up of normal and abnormal squamous cells; the inset on the right shows a close up of normal and abnormal basal cells.")
. An inset shows that the tumor is 2 centimeters or smaller and that 2 centimeters is about the size of a peanut. Also shown are the dermis (the inner layer of the skin) and the subcutaneous tissue below the dermis.")

; drawing shows (a) an inset showing that the tumor is larger than 4 centimeters and that 4 centimeters is about the size of a walnut. Also shown is cancer spreading through the epidermis to (b) tissue covering the nerves below the dermis; (c) below the subcutaneous tissue; and (d) bone.")
; drawing shows a primary tumor on the face and cancer in one lymph node on the same side of the body as the tumor. The top inset shows that the tumor is 4 centimeters or smaller and that 4 centimeters is about the size of a walnut. The bottom inset shows that the lymph node with cancer is 3 centimeters or smaller and that 3 centimeters is about the size of a grape.")
; drawing shows a primary tumor on the face and cancer that has spread to: (a) one lymph node on the same side of the body as the tumor, the node is 3 centimeters or smaller, and cancer has spread through to the outside covering of the lymph node; (b) one lymph node on the same side of the body as the tumor and the node is larger than 3 centimeters but not larger than 6 centimeters; (c) more than one lymph node on the same side of the body as the tumor and the nodes are 6 centimeters or smaller; and (d) one or more lymph nodes on the opposite or both sides of the body as the tumor and the nodes are 6 centimeters or smaller. Also shown is a 10-centimeter ruler and a 4-inch ruler.")
; drawing shows a primary skin tumor on the face and cancer that has spread to: (a) one lymph node that is larger than 6 centimeters; (b) one lymph node on the same side of the body as the tumor, the affected node is larger than 3 centimeters, and cancer has spread through to the outside covering of the lymph node; (c) one lymph node on the opposite side of the body as the tumor, the affected node is any size, and cancer has spread through to the outside covering of the lymph node; and (d) more than one lymph node on one or both sides of the body and cancer has spread through to the outside covering of the lymph nodes. Also shown is a 10-centimeter ruler and a 4-inch ruler.")
; drawing shows a primary skin tumor on the face and other parts of the body where nonmelanoma skin cancer may spread, including the base of the skull, the lung, the bone, and the bone marrow. An inset shows cancer cells spreading through the blood and lymph system to another part of the body where metastatic cancer has formed.")
 and the back of a person’s ear with a skin cancer lesion that looks like an open sore with a pearly rim (right panel).")
 and a person’s leg with a skin cancer lesion that looks pink and raised (right panel).")
 and the dermis (inner layer of the skin). A visible lesion is shown on the skin’s surface. Four numbered blocks show the removal of thin layers of the skin one at a time until all the cancer is removed.")

 to PD-1 (on the T cell), which keeps T cells from killing tumor cells in the body. Also shown are a tumor cell antigen and T cell receptor. The panel on the right shows immune checkpoint inhibitors (anti-PD-L1 and anti-PD-1) blocking the binding of PD-L1 to PD-1, which allows the T cells to kill tumor cells.")
; left panel shows blood being drawn from a vein on the inside of the elbow using a tube attached to a syringe; right panel shows a laboratory test tube with blood cells separated into layers: plasma, white blood cells, platelets, and red blood cells.")
 being inserted into the lower back. Inset shows a close-up of the spinal needle inserted into the cerebrospinal fluid (CSF) in the lower part of the spinal column.")
 in the brain and spinal cord, and an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). Top section shows a syringe and needle injecting anticancer drugs into the Ommaya reservoir. Bottom section shows a syringe and needle injecting anticancer drugs directly into the cerebrospinal fluid in the lower part of the spinal column.")