Screening Tests to Detect Colorectal Cancer and Polyps
What is colorectal cancer?
Colorectal cancer (cancer that develops in the colon and/or the rectum) is a disease in which abnormal cells in the colon or rectum divide uncontrollably, ultimately forming a malignant tumor.
Parts of the colon. Drawing of the front of the abdomen that shows the four sections of the colon: the ascending colon, the transverse colon, the descending colon, and the sigmoid colon. Also shown are the small intestine, the cecum, and the rectum. The cecum, colon, rectum, and anal canal make up the large intestine. The cecum, ascending colon, and transverse colon make up the upper, or proximal, colon; the descending colon and sigmoid colon make up the lower, or distal, colon.
Most colorectal cancers begin as an abnormal growth, or lesion, in the tissue that lines the inner surface of the colon or rectum. Lesions may appear as raised polyps, or, less commonly, they may appear flat or slightly indented. Raised polyps may be attached to the inner surface of the colon or rectum with a stalk (pedunculated polyps), or they may grow along the surface without a stalk (sessile polyps).
Colorectal polyps are common in people older than 50 years of age, and most do not become cancer. However, a certain type of polyp known as an adenoma is more likely to become a cancer.
Colorectal cancer is the third most common type of non-skin cancer in both men (after prostate cancer and lung cancer) and women (after breast cancer and lung cancer). It is the second leading cause of cancer death in the United States after lung cancer. In 2024, an estimated 152,810 people in the United States will be diagnosed with colorectal cancer and 53,010 people will die from it (1).
Who is at risk for colorectal cancer?
Increasing age is a major risk factor for colorectal cancer. In the United States, colorectal cancer is most frequently diagnosed in adults aged 65 to 74 years. From 2017 through 2021, the colorectal cancer incidence rates were 8.6, 69.8, and 156.9 per 100,000 people for those younger than 50 years, those aged 50 to 64 years, and those 65 years and older, respectively.
Several other factors are known to be associated with smaller increases in risk. These include moderate to heavy alcohol use, obesity, physical inactivity, and cigarette smoking.
Expert medical groups, including the US Preventive Services Task Force (USPSTF) (2), strongly recommend screening for colorectal cancer. Although some details of the recommendations vary, most groups now generally recommend that people at average risk of colorectal cancer get screened at regular intervals beginning at age 45 (2–6).
The expert medical groups generally recommend that screening continue to age 75; for those aged 76 to 85 years, the decision to screen is based on the individual’s life expectancy, health conditions, and prior screening results.
What methods are used to screen people for colorectal cancer?
Several different screening tests are available that can help doctors find colorectal cancer before symptoms begin, when it may be more treatable. Some of these tests also allow adenomas and polyps to be found and removed before they become cancer. That is, some types of colorectal cancer screening may allow for cancer prevention in addition to early detection.
Stool tests. Both polyps and colorectal cancers can bleed, and stool tests check for tiny amounts of blood in feces (stool) that cannot be seen visually. (Hidden blood in stool—also called occult blood–may also indicate the presence of conditions that are not cancer, such as hemorrhoids.) With these tests, stool samples are collected by the patient using a kit, and the samples are sent to a laboratory for testing. People who have a positive finding with these tests are advised to have a colonoscopy.
The US Food and Drug Administration (FDA) has approved several types of stool tests to screen for colorectal cancer, including:
Guaiac fecal occult blood test (gFOBT). gFOBT uses a chemical to detect heme, a component of the blood protein hemoglobin. Because gFOBT can also detect heme in some foods (for example, red meat), people must avoid certain foods before having this test. If gFOBT is the only type of colorectal cancer screening test performed, experts generally recommend testing every year or two (3).
Fecal immunochemical test (FIT or iFOBT). FIT uses antibodies to detect hemoglobin protein specifically (5, 6). Dietary restrictions are typically not required for FIT. If FIT is the only type of colorectal cancer screening test performed, experts generally recommend testing every year or two (3).
Multitarget stool DNA testing (sDNA-FIT). sDNA-FIT (Cologuard) detects hemoglobin, along with certain DNA biomarkers. The DNA comes from cells in the lining of the colon and rectum that are shed and collect in stool as it passes through the large intestine and rectum. Experts generally suggest sDNA-FIT testing at least every 3 years (2).
Direct visualization tests. There are three direct visualization tests used for colorectal cancer screening. All involve pumping air into the colon through a tube inserted through the anus into the rectum to expand the colon so the doctor can see the lining more clearly. Of these three tests, colonoscopy is the most common direct visualization test in the United States.
Colonoscopy. In this test, the rectum and entire colon are examined using a colonoscope, a flexible lighted tube with a lens for viewing and a tool for removing tissue, which is inserted through the anus into the rectum. During colonoscopy, any abnormal growths in the entire colon and the rectum can be removed. The preparation for colonoscopy requires a thorough cleansing of the entire colon before the test. Most patients receive some form of sedation during the test.
Experts recommend screening colonoscopy every 10 years for people at average risk.
Virtual colonoscopy, also called computed tomographic (CT) colonography, is a screening method that uses special x-ray equipment (a CT scanner) to produce a series of pictures of the colon and the rectum from outside the body. A computer then assembles these pictures into detailed images that can show polyps and other abnormalities. As with standard colonoscopy, a thorough cleansing of the colon is necessary before this test. Virtual colonoscopy is much less invasive than standard colonoscopy (other than the pumping of air into the colon), but if polyps or other abnormal growths are found during a virtual colonoscopy a standard colonoscopy must usually be performed to remove them.
Because virtual colonoscopy also produces images of areas outside the colon and rectum it can lead to the unintentional discovery of medical findings in these areas that require additional follow-up procedures. Virtual colonoscopy may also miss small polyps (7). However, many small polyps may not be likely to become cancer and so taking them out may not be of benefit. Experts recommend screening with virtual colonoscopy every 5 years.
Sigmoidoscopy. In this test, the rectum and sigmoid colon are examined using a sigmoidoscope, a flexible lighted tube with a lens for viewing and a tool for removing tissue, which is inserted through the anus into the rectum and sigmoid colon. During sigmoidoscopy, abnormal growths in the rectum and sigmoid colon can be removed for analysis (biopsied). The lower colon must be cleared of stool before sigmoidoscopy, but the preparation is not very extensive. People are not usually sedated for this test.
Experts generally recommend screening sigmoidoscopy every 5 or 10 years for people at average risk (3). People who are screened with sigmoidoscopy may also be tested every few years with FIT.
Blood-based tests. A test for a molecular biomarker (methylated SEPT9) shed by colorectal cancer cells into the bloodstream, called Epi proColon 2.0, is FDA approved to be used to screen adults 50 years or older at average risk for colorectal cancer who have been offered and have a history of not completing colorectal cancer screening using a stool test or a direct visualization test.
Another blood-based test for colorectal cancer (Shield) is approved for screening adults ages 45 and older who are at average risk for the disease. It analyzes plasma DNA for certain changes, including the presence of harmful gene variants.
Blood-based tests have not yet been incorporated into clinical guidelines for first-line colorectal cancer screening.
Other methods. Several other tests to screen for colorectal cancer are sometimes used, although these are not generally recommended by expert groups.
Double-contrast barium enema (DCBE). This test is another method of visualizing the colon from outside the body. In DCBE, a series of x-ray images of the entire colon and rectum is taken after the patient is given an enema with a barium solution. The barium helps to outline the colon and the rectum on the images. DCBE is rarely used for colorectal cancer screening; however, it may be used for people who cannot undergo standard colonoscopy—for example, because they are at particular risk for complications.
Single-specimen gFOBT done in a doctor’s office. Doctors sometimes perform gFOBT on a stool sample collected during a digital rectal examination as part of a routine physical examination. However, this approach is not an effective way to screen for colorectal cancer (8).
How can people and their health care providers decide which colorectal cancer screening test(s) to use?
Different tests have different advantages and disadvantages, and people should talk with their health care provider about which test is best for them.
An individual’s decision about which test to have may depend on:
the person’s age, medical history, family history, and general health
potential harms of the test (more invasive tests have more potential harms than less invasive tests)
the preparation required for the test
whether sedation may be needed for the test
the follow-up care needed after the test
the convenience of the test
the cost of the test and the availability of insurance coverage
The table below summarizes key features of the different colorectal screening tests that people may want to consider when choosing a test.
Does health insurance pay for colorectal cancer screening?
Colorectal cancer screening is a preventive service that the Health Insurance Marketplace and many other health insurance plans are required to cover. Medicare covers several colorectal cancer screening tests for its beneficiaries. However, Medicare and some insurance companies currently do not pay for the costs of virtual colonoscopy. Specific information about Medicare benefits for colorectal cancer screening is available on the Medicare website.
A colonoscopy to follow up on a screening test with a positive result, such as an abnormal stool test or even a lesion detected on a screening colonoscopy, is considered a diagnostic exam and may or may not be covered (or not covered as fully as a screening colonoscopy). Some insurers consider a screening colonoscopy that reveals a polyp that must be removed to be a diagnostic exam and charge accordingly. People should check with their health insurance provider before their test to determine their colorectal cancer screening coverage and what their out-of-pocket expenses may be if the test finds an abnormality that needs to be followed up.
What happens if a colorectal cancer screening test finds an abnormality?
If an abnormality is found during a standard colonoscopy it will be removed (polypectomy) or a biopsy performed, and the cells will be examined to see if cancer is present. If an abnormality is found during a sigmoidoscopy, polypectomy or biopsy may or may not be performed, and a follow-up colonoscopy may be recommended. If a different screening test finds an abnormality, a colonoscopy will be needed to examine the colon directly.
What new tests are being developed for colorectal cancer screening?
Researchers are studying new blood markers to detect colorectal cancer early. For example, tumors release into the blood small fragments of RNA called microRNAs packaged into tiny sac-like structures called exosomes. Exosome-packaged microRNAs have shown promise for early detection of pancreatic cancer and may also be useful for early detection of colorectal cancer (10, 11).
Another approach being tested is whether artificial intelligence (AI)–based technology called computer-aided detection (CAD) can improve the interpretation of colonoscopy imaging by experienced doctors. Several clinical trials have found that the addition of CAD increased the detection of small polyps that are unlikely to become cancer but not of advanced adenomas. However, these studies used relatively primitive AI-based CADs. Newer AI technologies may improve the detection of advanced adenomas by CAD.
Researchers are continuing to improve the sensitivity of stool-based screening for detecting advanced adenomatous polyps, which can potentially become colorectal cancer, by testing for the presence of other (non-DNA) types of biomarkers. For example, a multitarget stool RNA (mt-sRNA) test (ColoSense) that detects occult hemoglobin (with FIT), along with levels of eight colorectal cancer–associated RNA markers was approved in 2024 for colorectal cancer screening. (This test is not yet commercially available, and experts have not yet recommended a screening interval for it.)
Researchers have also found that measuring three protein biomarkers in stool—hemoglobin, calprotectin, and serpin family F member 2—improved the ability of FIT to detect advanced lesions (including colorectal cancer) without reducing its specificity (12).
Capsule colonoscopy (also called capsule endoscopy) is a technique that continues to be explored to improve visualization of the colon. A person swallows a pill-like capsule that contains a tiny wireless camera. The camera takes pictures of the inside of the digestive tract and sends them to a small recorder that is worn on the patient’s waist or shoulder. The pictures are then viewed on a computer by the doctor to check for signs of disease. The capsule passes out of the body during a bowel movement. Cleansing of the colon is still necessary before this test. This method is currently approved for patients with an incomplete colonoscopy and for detection of colon polyps in patients with evidence of lower GI bleeding but not as a stand-alone screening test for people at average risk.
Some gastrointestinal stromal tumors (GISTs) grow slowly over time and may never cause a problem for a patient, while others can grow and spread very quickly. They are most common in the stomach and small intestine but may be found anywhere in or near the GI tract. Some scientists believe that GISTs begin in cells called interstitial cells of Cajal (ICC), in the wall of the GI tract.
EnlargeGastrointestinal stromal tumors (GISTs) may be found anywhere in or near the gastrointestinal tract.
Genetic factors can increase the risk of having a gastrointestinal stromal tumor.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk.
The genes in cells carry the hereditary information received from a person’s parents. The risk of GIST is increased in people who have inherited a mutation (change) in a certain gene. In rare cases, GISTs can be found in several members of the same family.
GIST may be part of a geneticsyndrome, but this is rare. A genetic syndrome is a set of symptoms or conditions that occur together and is usually caused by abnormal genes. The following genetic syndromes have been linked to GIST:
Tests that examine the GI tract are used to diagnose gastrointestinal stromal tumors.
The following tests and procedures may be used:
Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Endoscopic ultrasound and biopsy: Endoscopy and ultrasound are used to make an image of the upper GI tract and a biopsy is done. An endoscope (a thin, tube-like instrument with a light and a lens for viewing) is inserted through the mouth and into the esophagus, stomach, and first part of the small intestine. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography. Guided by the sonogram, the doctor removes tissue using a thin, hollow needle. A pathologist views the tissue under a microscope to look for cancer cells.
If cancer is found, the following tests may be done to study the cancer cells:
Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient’s tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
Mitotic rate: A measure of how fast the cancer cells are dividing and growing. The mitotic rate is found by counting the number of cells dividing in a certain amount of cancer tissue.
Very small GISTs are common.
Sometimes GISTs are smaller than the eraser on top of a pencil. Tumors may be found during a procedure that is done for another reason, such as an x-ray or surgery. Some of these small tumors will not grow and cause signs or symptoms or spread to the abdomen or other parts of the body. Doctors do not agree on whether these small tumors should be removed or whether they should be watched to see if they begin to grow.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
How quickly the cancer cells are growing and dividing.
The size of the tumor.
Where the tumor is in the body.
Whether the tumor can be completely removed by surgery.
Whether the tumor has spread to other parts of the body.
Stages of Gastrointestinal Stromal Tumors
Key Points
After a gastrointestinal stromal tumor has been diagnosed, tests are done to find out if cancer cells have spread within the gastrointestinal tract or to other parts of the body.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
The results of diagnostic and staging tests are used to plan treatment.
After a gastrointestinal stromal tumor has been diagnosed, tests are done to find out if cancer cells have spread within the gastrointestinal tract or to other parts of the body.
The process used to find out if cancer has spread within the gastrointestinal (GI) tract or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. The following tests and procedures may be used in the staging process:
PET scan (positron emission tomography scan): A procedure to find malignanttumorcells in the body. A small amount of radioactiveglucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
There are three ways that cancer spreads in the body.
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of tumor as the primary tumor. For example, if a gastrointestinal stromal tumor (GIST) spreads to the liver, the tumor cells in the liver are actually GIST cells. The disease is metastatic GIST, not liver cancer.
Many cancer deaths are caused when cancer moves from the original tumor and spreads to other tissues and organs. This is called metastatic cancer. This animation shows how cancer cells travel from the place in the body where they first formed to other parts of the body.
The results of diagnostic and staging tests are used to plan treatment.
For many cancers it is important to know the stage of the cancer in order to plan treatment. However, the treatment of GIST is not based on the stage of the cancer. Treatment is based on whether the tumor can be removed by surgery and if the tumor has spread to other parts of the abdomen or to distant parts of the body.
Treatment is based on whether the tumor is:
Resectable: These tumors can be removed by surgery .
Unresectable: These tumors cannot be completely removed by surgery.
Metastatic and recurrent: Metastatic tumors have spread to other parts of the body. Recurrent tumors have recurred (come back) after treatment. Recurrent GISTs may come back in the gastrointestinal tract or in other parts of the body. They are usually found in the abdomen, peritoneum, and/or liver.
Refractory: These tumors have not gotten better with treatment.
Treatment Option Overview
Key Points
There are different types of treatment for patients with gastrointestinal stromal tumors.
Four types of standard treatment are used:
Surgery
Targeted therapy
Watchful waiting
Supportive care
New types of treatment are being tested in clinical trials.
Treatment for gastrointestinal stromal tumors may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with gastrointestinal stromal tumors.
Different types of treatments are available for patients with gastrointestinal stromal tumors (GISTs). Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Four types of standard treatment are used:
Surgery
If the GIST has not spread and is in a place where surgery can be safely done, the tumor and some of the tissue around it may be removed. Sometimes surgery is done using a laparoscope (a thin, lighted tube) to see inside the body. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope is inserted into one of the incisions. Instruments may be inserted through the same incision or through other incisions to remove organs or tissues.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do.
Tyrosine kinase inhibitors (TKIs) are targeted therapy drugs that block signals needed for tumors to grow. TKIs may be used to treat GISTs that cannot be removed by surgery or to shrink GISTs so they become small enough to be removed by surgery. Imatinib mesylate and sunitinib are two TKIs used to treat GISTs. TKIs are sometimes given for as long as the tumor does not grow and serious side effects do not occur.
If a GIST gets worse during treatment or there are side effects, supportive care is usually given. The goal of supportive care is to prevent or treat the symptoms of a disease, side effects caused by treatment, and psychological, social, and spiritual problems related to a disease or its treatment. Supportive care helps improve the quality of life of patients who have a serious or life-threatening disease. Radiation therapy is sometimes given as supportive care to relieve pain in patients with large tumors that have spread.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for gastrointestinal stromal tumors may cause side effects.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Follow-up for GISTs that were removed by surgery may include CT scan of the liver and pelvis or watchful waiting. For GISTs that are treated with tyrosine kinase inhibitors, follow-up tests, such as CT, MRI, or PET scans, may be done to check how well the targeted therapy is working.
Treatment of Resectable Gastrointestinal Stromal Tumors
UnresectableGISTs cannot be completely removed by surgery because they are too large or in a place where there would be too much damage to nearby organs if the tumor is removed. Treatment is usually a clinical trial of targeted therapy with imatinib mesylate to shrink the tumor, followed by surgery to remove as much of the tumor as possible.
Treatment of Metastatic and Recurrent Gastrointestinal Stromal Tumors
Targeted therapy with sunitinib, if the tumor begins to grow during imatinib mesylate therapy or if the side effects are too bad.
Surgery to remove tumors that have been treated with targeted therapy and are shrinking, stable (not changing), or that have slightly increased in size. Targeted therapy may continue after surgery.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of adult gastrointestinal stromal tumors. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Gastrointestinal Stromal Tumors Treatment (Adult). Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/soft-tissue-sarcoma/patient/gist-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389367]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Colon cancer is a type of cancer that forms in the tissues of the colon.
Health history affects the risk of developing colon cancer.
Signs of colon cancer include blood in the stool or a change in bowel habits.
Tests that examine the colon and rectum are used to diagnose colon cancer.
After colon cancer has been diagnosed, imaging tests are done to find out if cancer cells have spread within the colon or to other parts of the body.
Some people decide to get a second opinion.
Certain factors affect prognosis (chance of recovery) and treatment options.
Colon cancer is a type of cancer that forms in the tissues of the colon.
The colon is part of the body’s digestive system. The digestive system takes in nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps pass waste material out of the body. The digestive system is made up of the esophagus, stomach, and the small and large intestines. The colon (large bowel) is the main part of the large intestine and is about 5 feet long. Together, the rectum and anal canal make up the last part of the large intestine and are about 6 to 8 inches long. The anal canal ends at the anus (the opening of the large intestine to the outside of the body).
EnlargeAnatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Health history affects the risk of developing colon cancer.
Colorectal cancer is caused by certain changes to the way colorectal cells function, especially how they grow and divide into new cells. There are many risk factors for colorectal cancer, but many do not directly cause cancer. Instead, they increase the chance of DNA damage in cells that may lead to colorectal cancer. To learn more about how cancer develops, see What Is Cancer?
A risk factor is anything that increases the chance of getting a disease. Some risk factors for colorectal cancer, like smoking, can be changed. However, risk factors also include things you cannot change, like your genetics, getting older, and your family history. Learning about risk factors for colorectal cancer can help you make changes that might lower your risk of getting it.
having a personal history of high-risk adenomas (colorectal polyps that are 1 centimeter or larger in size or that have cells that look abnormal under a microscope)
Older age is a main risk factor for most cancers. The chance of getting cancer increases as you get older.
Having one or more of these risk factors does not mean that you will get colorectal cancer. Many people with risk factors never develop colorectal cancer, while others with no known risk factors do. Talk with your doctor if you think you might be at increased risk.
EnlargePolyps in the colon. Some polyps have a stalk and others do not. Inset shows a photo of a polyp with a stalk.
Signs of colon cancer include blood in the stool or a change in bowel habits.
These and other signs and symptoms may be caused by colon cancer or by other conditions. Check with your doctor if you have:
blood (either bright red or very dark) in the stool
Digital rectal exam (DRE) is an exam of the rectum. The doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel for lumps or anything else that seems unusual.
Fecal occult blood test (FOBT) is a test to check stool (solid waste) for blood that can only be seen with a microscope. A small sample of stool is placed on a special card or in a special container and returned to the doctor or laboratory for testing. Blood in the stool may be a sign of polyps (small pieces of bulging tissue), cancer, or other conditions.
There are two types of FOBTs:
Guaiac FOBT: The sample of stool on the special card is tested with a chemical. If there is blood in the stool, the special card changes color. EnlargeA guaiac fecal occult blood test (FOBT) checks for occult (hidden) blood in the stool. Small samples of stool are placed on a special card and returned to a doctor or laboratory for testing.
Immunochemical FOBT: A liquid is added to the stool sample. This mixture is injected into a machine that contains antibodies that can detect blood in the stool. If there is blood in the stool, a line appears in a window in the machine. This test is also called fecal immunochemical test or FIT. EnlargeA fecal immunochemical test (FIT) checks for occult (hidden) blood in the stool. A small sample of stool is placed in a special collection tube or on special cards and returned to a doctor or laboratory for testing.
Sigmoidoscopy is a procedure to look inside the rectum and sigmoid (lower) colon for polyps (small pieces of bulging tissue), abnormal areas, or cancer. A sigmoidoscope is inserted through the rectum into the sigmoid colon. A sigmoidoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer. EnlargeSigmoidoscopy. A thin, lighted tube is inserted through the anus and rectum and into the lower part of the colon to look for abnormal areas.
Colonoscopy is a procedure that uses a colonoscope to look inside the rectum and colon for polyps (small pieces of bulging tissue), abnormal areas, or cancer. A colonoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer. EnlargeColonoscopy. A thin, lighted tube is inserted through the anus and rectum and into the colon to look for abnormal areas.
Virtual colonoscopy is a procedure that uses a series of x-rays called computed tomography to make a series of pictures of the colon. A computer puts the pictures together to create detailed images that may show polyps and anything else that seems unusual on the inside surface of the colon. This test is also called colonography or CT colonography.
Biopsy is the removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. Tumor tissue that is removed during the biopsy may be checked to see if the patient is likely to have the genemutation that causes Lynch syndrome (also known as hereditary nonpolyposis colorectal cancer). This may help to plan treatment. Learn about the type of information that can be found in a pathologist’s report about the cells or tissue removed during a biopsy at Pathology Reports.
DNA stool test checks DNA in stool cells for genetic changes that may be a sign of colorectal cancer.
After colon cancer has been diagnosed, imaging tests are done to find out if cancer cells have spread within the colon or to other parts of the body.
The process used to find out whether cancer has spread within the colon or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
CT scan (CAT scan) uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body, such as the abdomen, pelvis, or chest. The pictures are taken from different angles and are used to create 3-D views of tissues and organs. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
MRI (magnetic resonance imaging) uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the colon. A substance called gadolinium is injected into the patient through a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
PET scan (positron emission tomography scan) uses a small amount of sugar (also called radioactive glucose) that is injected into a vein. The PET scanner rotates around the body and makes a picture of where the sugar is being used in the body. Cancer cells show up brighter in the picture because they are more active and take up more sugar than normal cells do.
Chest x-ray is a type of radiation that can go through the body and make pictures of the organs and bones inside the chest.
Surgery is a procedure to remove the tumor and see how far it has spread through the colon.
Carcinoembryonic antigen (CEA) assay is a test that measures the level of CEA in the blood. CEA is released into the bloodstream from both cancer cells and normal cells. When found in higher than normal amounts, it can be a sign of colon cancer or other conditions.
Some people decide to get a second opinion.
You may want to get a second opinion to confirm your colon cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans. They may agree with the first doctor, suggest changes or another treatment approach, or provide more information about your cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on:
the stage of the cancer (whether it affects the inner lining of the colon only, or has spread to lymph nodes, nearby organs, or other places in the body)
whether the cancer is related to certain genetic changes in stool cells
whether the tumor has spread into or through the colon wall
whether the colon is blocked or has a hole in it
whether all of the tumor can be removed by surgery
the patient’s general health
whether the cancer has just been diagnosed or has recurred (come back)
Stages of Colon Cancer
Key Points
The following stages are used for colon cancer:
Stage 0 (carcinoma in situ)
Stage I (also called stage 1) colon cancer
Stage II (also called stage 2) colon cancer
Stage III (also called stage 3) colon cancer
Stage IV (also called stage 4) colon cancer
Colon cancer can recur (come back) after it has been treated.
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. It is important to know the stage of the colon cancer to plan the best treatment.
There are several staging systems for cancer that describe the extent of the cancer. Colon cancer staging usually uses the TNM staging system. The cancer may be described by this staging system in your pathology report. Based on the TNM results, a stage (I, II, III, or IV, also written as 1, 2, 3, or 4) is assigned to your cancer. When talking to you about your diagnosis, your doctor may describe the cancer as one of these stages.
EnlargeStage 0 (colon carcinoma in situ). Abnormal cells are shown in the mucosa of the colon wall.
In stage 0 colon cancer, abnormal cells are found in the mucosa (innermost layer) of the colon wall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage I (also called stage 1) colon cancer
EnlargeStage I colon cancer. Cancer has spread from the mucosa of the colon wall to the submucosa or to the muscle layer.
In stage I colon cancer, cancer has formed in the mucosa (innermost layer) of the colon wall and has spread to the submucosa (layer of tissue next to the mucosa) or to the muscle layer of the colon wall.
Stage II (also called stage 2) colon cancer
EnlargeStage II colon cancer. In stage IIA, cancer has spread through the muscle layer of the colon wall to the serosa. In stage IIB, cancer has spread through the serosa but has not spread to nearby organs. In stage IIC, cancer has spread through the serosa to nearby organs.
Stage II colon cancer is divided into stages IIA, IIB, and IIC.
Stage IIA: Cancer has spread through the muscle layer of the colon wall to the serosa (outermost layer) of the colon wall.
Stage IIB: Cancer has spread through the serosa (outermost layer) of the colon wall to the tissue that lines the organs in the abdomen (visceral peritoneum).
Stage IIC: Cancer has spread through the serosa (outermost layer) of the colon wall to nearby organs.
Stage III (also called stage 3) colon cancer
Stage III colon cancer is divided into stages IIIA, IIIB, and IIIC.
EnlargeStage IIIA colon cancer. Cancer has spread through the mucosa of the colon wall to the submucosa and may have spread to the muscle layer, and has spread to one to three nearby lymph nodes or tissues near the lymph nodes. OR, cancer has spread through the mucosa to the submucosa and four to six nearby lymph nodes.
In stage IIIA, cancer has spread:
through the mucosa (innermost layer) of the colon wall to the submucosa (layer of tissue next to the mucosa) or to the muscle layer of the colon wall. Cancer has spread to one to three nearby lymph nodes, or cancer cells have formed in tissue near the lymph nodes; or
through the mucosa (innermost layer) of the colon wall to the submucosa (layer of tissue next to the mucosa). Cancer has spread to four to six nearby lymph nodes.
EnlargeStage IIIB colon cancer. Cancer has spread through the muscle layer of the colon wall to the serosa or has spread through the serosa but not to nearby organs; cancer has spread to one to three nearby lymph nodes or to tissues near the lymph nodes. OR, cancer has spread to the muscle layer or to the serosa, and to four to six nearby lymph nodes. OR, cancer has spread through the mucosa to the submucosa and may have spread to the muscle layer; cancer has spread to seven or more nearby lymph nodes.
In stage IIIB, cancer has spread:
through the muscle layer of the colon wall to the serosa (outermost layer) of the colon wall or has spread through the serosa to the tissue that lines the organs in the abdomen (visceral peritoneum). Cancer has spread to one to three nearby lymph nodes, or cancer cells have formed in tissue near the lymph nodes; or
to the muscle layer or to the serosa (outermost layer) of the colon wall. Cancer has spread to four to six nearby lymph nodes; or
through the mucosa (innermost layer) of the colon wall to the submucosa (layer of tissue next to the mucosa) or to the muscle layer of the colon wall. Cancer has spread to seven or more nearby lymph nodes.
EnlargeStage IIIC colon cancer. Cancer has spread through the serosa of the colon wall but not to nearby organs; cancer has spread to four to six nearby lymph nodes. OR, cancer has spread through the muscle layer to the serosa or has spread through the serosa but not to nearby organs; cancer has spread to seven or more nearby lymph nodes. OR, cancer has spread through the serosa to nearby organs and to one or more nearby lymph nodes or to tissues near the lymph nodes.
In stage IIIC, cancer has spread:
through the serosa (outermost layer) of the colon wall to the tissue that lines the organs in the abdomen (visceral peritoneum). Cancer has spread to four to six nearby lymph nodes; or
through the muscle layer of the colon wall to the serosa (outermost layer) of the colon wall or has spread through the serosa to the tissue that lines the organs in the abdomen (visceral peritoneum). Cancer has spread to seven or more nearby lymph nodes; or
through the serosa (outermost layer) of the colon wall to nearby organs. Cancer has spread to one or more nearby lymph nodes, or cancer cells have formed in tissue near the lymph nodes.
Stage IV (also called stage 4) colon cancer
EnlargeStage IV colon cancer. The cancer has spread through the blood and lymph nodes to other parts of the body, such as the lung, liver, abdominal wall, or ovary (in females).
Stage IV colon cancer is divided into stages IVA, IVB, and IVC.
Stage IVA: Cancer has spread to one area or organ that is not near the colon, such as the liver, lung, ovary, or a distant lymph node.
Stage IVB: Cancer has spread to more than one area or organ that is not near the colon, such as the liver, lung, ovary, or a distant lymph node.
Stage IVC: Cancer has spread to the tissue that lines the wall of the abdomen and may have spread to other areas or organs.
Stage IV colon cancer is also called metastatic colon cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if colon cancer spreads to the liver, the cancer cells in the liver are actually colon cancer cells. The disease is called metastatic colon cancer, not liver cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
Colon cancer can recur (come back) after it has been treated.
Recurrent colon cancer is cancer that has come back after it has been treated. If colon cancer comes back, it may come back in the colon or in other parts of the body, such as the liver, lungs, or both. Tests will be done to help determine where the cancer has returned. The type of treatment for recurrent colon cancer will depend on where it has come back.
There are different types of treatment for people with colon cancer.
The following types of treatment are used:
Surgery
Chemotherapy
Radiation therapy
Targeted therapy
Immunotherapy
New types of treatment are being tested in clinical trials.
Treatment for colon cancer may cause side effects.
Follow-up care may be needed.
There are different types of treatment for people with colon cancer.
Different types of treatments are available for colon cancer. You and your cancer care team will work together to decide your treatment plan, which may include more than one type of treatment. Many factors will be considered, such as the stage of the cancer, your overall health, and your preferences. Your plan will include information about your cancer, the goals of treatment, your treatment options and the possible side effects, and the expected length of treatment.
Talking with your cancer care team before treatment begins about what to expect will be helpful. You’ll want to learn what you need to do before treatment begins, how you’ll feel while going through it, and what kind of help you will need. To learn more, visit Questions to Ask Your Doctor About Treatment.
The following types of treatment are used:
Surgery
Surgery is the most common treatment for all stages of colon cancer. The cancer is removed using one of the following types of surgery:
Polypectomy: If the cancer is found in a polyp (a small piece of bulging tissue), the polyp is often removed during a colonoscopy.
Local excision: If the cancer is found at a very early stage, the doctor may remove it without cutting through the abdominal wall. Instead, the doctor may put a tube with a cutting tool through the rectum into the colon and cut the cancer out. This is called a local excision.
Resection of the colon with anastomosis: If the cancer is larger, the doctor will perform a partial colectomy (removing the cancer and a small amount of healthy tissue around it). The doctor may then perform an anastomosis (sewing the healthy parts of the colon together). The doctor will also usually remove lymph nodes near the colon and examine them under a microscope to see whether they contain cancer. EnlargeResection of the colon with anastomosis. Part of the colon containing the cancer and nearby healthy tissue is removed, and then the cut ends of the colon are joined.
Resection of the colon with colostomy: If the doctor is not able to sew the two ends of the colon back together, a stoma (opening) is made on the outside of the body for waste to pass through. This procedure is called a colostomy. A bag is placed around the stoma to collect the waste. Sometimes the colostomy is needed only until the lower colon has healed, and then it can be reversed. If the doctor needs to remove the entire lower colon, however, the colostomy may be permanent. EnlargeColon cancer surgery with colostomy. Part of the colon containing the cancer and nearby healthy tissue is removed, a stoma is created, and a colostomy bag is attached to the stoma.
Radiofrequency ablation: The use of a special probe with tiny electrodes that kill cancer cells. Sometimes, the probe is inserted directly through the skin, and only local anesthesia is needed. In other cases, the probe is inserted through an incision in the abdomen. This is done in the hospital with general anesthesia.
Cryosurgery: A treatment that uses an instrument to freeze and destroy abnormal tissue. This type of treatment is also called cryotherapy. Learn more about Cryosurgery to Treat Cancer.
Radiation therapy and/or chemotherapy may be given before surgery to shrink the tumor, make it easier to remove the cancer, and help with bowel control after surgery. Treatment given before surgery is called neoadjuvant therapy. After all the cancer that can be seen at the time of the surgery is removed, some patients may be given radiation therapy and/or chemotherapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
If the cancer has spread to the liver and cannot be removed by surgery, a total hepatectomy and liver transplant after chemotherapy may be done. Total hepatectomy and liver transplant is the removal of the entire liver by surgery, followed by a transplant of a healthy liver from a donor.
Chemotherapy
Chemotherapy (also called chemo) uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing.
Systemic chemotherapy is when chemotherapy drugs are taken by mouth or injected into a vein or muscle. When given this way, the drugs enter the bloodstream and can reach cancer cells throughout the body. Systemic chemotherapy used to treat colon cancer includes:
Combinations of these drugs may be used. Other chemotherapy drugs not listed here may also be used.
Chemotherapy may also be combined with other kinds of drugs. For example, it might be combined with the targeted therapy drug bevacizumab, cetuximab, or panitumumab.
Regional chemotherapy for colon cancer is when drugs are placed directly into the hepatic artery (the main artery that supplies blood to the liver) in a procedure called chemoembolization. Chemoembolization of the hepatic artery may be used to treat cancer that has spread to the liver. This is done by blocking the hepatic artery and injecting anticancer drugs between the blockage and the liver. The liver’s arteries then carry the drugs into the liver. Only a small amount of the drug reaches other parts of the body. The blockage may be temporary or permanent, depending on what is used to block the artery. The liver continues to receive some blood from the hepatic portal vein, which carries blood from the stomach and intestine.
The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Radiation therapy uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. Colon cancer is sometimes treated with two types of radiation therapy used to treat colon cancer:
External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. Internal radiation therapy may be used to treat colon cancer that has spread to the liver.
Targeted therapy uses drugs or other substances to identify and attack specific cancer cells. Your doctor may suggest biomarker tests to help predict your response to certain targeted therapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Targeted therapies used to treat colon cancer include:
Immunotherapy helps a person’s immune system fight cancer. Your doctor may suggest biomarker tests to help predict your response to certain immunotherapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Immunotherapy drugs used to treat colon cancer include:
New types of treatment are being tested in clinical trials.
For some people, joining a clinical trial may be an option. There are different types of clinical trials for people with cancer. For example, a treatment trial tests new treatments or new ways of using current treatments. Supportive care and palliative care trials look at ways to improve quality of life, especially for those who have side effects from cancer and its treatment.
You can use the clinical trial search to find NCI-supported cancer clinical trials accepting participants. The search allows you to filter trials based on the type of cancer, your age, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
After treatment for colon cancer, a blood test to measure amounts of carcinoembryonic antigen (a substance in the blood that may be increased when cancer is present) may be done to see if the cancer has come back.
Treatment of Stage 0 (carcinoma in situ)
Treatment of stage 0 may include the following types of surgery:
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of colon cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Colon Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/patient/colon-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389319]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Cancer of the colon is a highly treatable and often curable disease when localized to the bowel. Surgery is the primary form of treatment and results in cure in approximately 50% of patients. However, recurrence following surgery is a major problem and is often the ultimate cause of death.
Incidence and Mortality
Worldwide, colorectal cancer is the third most common form of cancer. In 2022, there were an estimated 1.93 million new cases of colorectal cancer and 903,859 deaths.[1]
Estimated new cases and deaths from colon and rectal cancer in the United States in 2025:[2]
New cases of colon cancer: 107,320.
New cases of rectal cancer: 46,950.
Deaths: 52,900 (colon and rectal cancers combined).
Screening for colon cancer should be a part of routine care for all adults aged 50 years and older, especially for those with first-degree relatives with colorectal cancer. This recommendation is based on the frequency of the disease, ability to identify high-risk groups, slow growth of primary lesions, better survival of patients with early-stage lesions, and relative simplicity and accuracy of screening tests. For more information, see Colorectal Cancer Screening.
Prognostic Factors
The prognosis of patients with colon cancer is clearly related to:
The degree of penetration of the tumor through the bowel wall.
The presence or absence of nodal involvement.
The presence or absence of distant metastases.
These three characteristics form the basis for all staging systems developed for this disease.
Other prognostic factors for colon cancer include:
Bowel obstruction and bowel perforation are indicators of poor prognosis.[14]
Elevated pretreatment serum levels of carcinoembryonic antigen (CEA) have a negative prognostic significance.[15]
Many other prognostic markers have been evaluated retrospectively for patients with colon cancer, though most, including allelic loss of chromosome 18q or thymidylate synthase expression, have not been prospectively validated.[16–25] Microsatellite instability, also associated with HNPCC, has been associated with improved survival independent of tumor stage in a population-based series of 607 patients younger than 50 years with colorectal cancer.[26] Patients with HNPCC reportedly have better prognoses in stage-stratified survival analysis than patients with sporadic colorectal cancer, but the retrospective nature of the studies and possibility of selection factors make this observation difficult to interpret.[27]
Treatment decisions depend on factors such as physician and patient preferences and the stage of the disease, rather than the age of the patient.[28–30]
Racial differences in overall survival (OS) after adjuvant therapy have been observed, without differences in disease-free survival, suggesting that comorbid conditions play a role in survival outcome in different patient populations.[31]
Follow-Up and Survivorship
Limited data and no high-level evidence are available to guide patients and physicians about surveillance and management of patients after surgical resection and adjuvant therapy. The American Society of Clinical Oncology and the National Comprehensive Cancer Network recommend specific surveillance and follow-up strategies.[32,33]
Following treatment of colon cancer, periodic evaluations may lead to the earlier identification and management of recurrent disease.[34–37] This monitoring has limited effect on overall mortality, as few localized, potentially curable metastases are found in patients with recurrent colon cancer. To date, no large-scale randomized trials have documented an OS benefit for standard, postoperative monitoring programs.[38–42]
CEA is a serum glycoprotein frequently used in the management of patients with colon cancer. A review of the use of this tumor marker suggests:[43]
A CEA level is not a valuable screening test for colorectal cancer because of the large number of false-positive and false-negative reports.
Postoperative CEA testing should be restricted to patients who would be candidates for resection of liver or lung metastases.
Routine use of CEA levels alone for monitoring response to treatment is not recommended.
The optimal regimen and frequency of follow-up examinations are not well defined because the impact on patient survival is not clear and the quality of data is poor.[40–42]
Factors Associated With Recurrence
Diet and exercise
Although cohort studies have suggested that a diet or exercise regimen may improve outcomes, no prospective randomized trials have confirmed these findings. The cohort studies contained multiple opportunities for unintended bias, and caution is needed when using the data from them.
Two prospective observational studies were performed with patients enrolled in the Cancer and Leukemia Group B CALGB-89803 trial (NCT00003835), an adjuvant chemotherapy trial for patients with stage III colon cancer.[44,45] In this trial, patients in the lowest quintile of the Western dietary pattern, compared with those patients in the highest quintile, experienced an adjusted hazard ratio (HR) for disease-free survival of 3.25 (95% confidence interval [CI], 2.04–5.19; P < .001) and an OS of 2.32 (95% CI, 1.36–3.96; P < .001). Additionally, stage III colon cancer patients in the highest quintile of dietary glycemic load experienced an adjusted HR for OS of 1.76 (95% CI, 1.22–2.54; P < .001), compared with those in the lowest quintile. Subsequently, in the Cancer Prevention Study II Nutrition Cohort, among 2,315 participants diagnosed with colorectal cancer, the degree of red and processed meat intake before diagnosis was associated with a higher risk of death (relative risk [RR], 1.29; 95% CI, 1.05–1.59; P = .03), but red meat consumption after diagnosis was not associated with overall mortality.[46][Level of evidence C1]
A meta-analysis of seven prospective cohort studies evaluating physical activity before and after a diagnosis of colorectal cancer demonstrated that patients who participated in any amount of physical activity before diagnosis had an RR of 0.75 (95% CI, 0.65–0.87; P < .001) for colorectal cancer-specific mortality, compared with patients who did not participate in any physical activity.[47] Patients who participated in a high amount of physical activity (vs. a low amount) before diagnosis had an RR of 0.70 (95% CI, 0.56–0.87; P = .002). Patients who participated in any physical activity (compared with no activity) after diagnosis had an RR of 0.74 (95% CI, 0.58–0.95; P = .02) for colorectal cancer-specific mortality. Those who participated in a high amount of physical activity (vs. a low amount) after diagnosis had an RR of 0.65 (95% CI, 0.47–0.92; P = .01).[47][Level of evidence C1]
Aspirin
A prospective cohort study examined the use of aspirin after a colorectal cancer diagnosis.[48] Regular users of aspirin after a diagnosis of colorectal cancer experienced an HRcolon cancer–specific mortality of 0.71 (95% CI, 0.53–0.95) and an HRoverall mortality of 0.79 (95% CI, 0.65–0.97).[48][Level of evidence C1] One study evaluated 964 patients with rectal or colon cancer from the Nurse’s Health Study and the Health Professionals Follow-up Study.[49] Among patients with colorectal cancer and PI3K variants, regular use of aspirin was associated with an HRdeath from any cause of 0.54 (95% CI, 0.31–0.94; P = .01)[49][Level of evidence C1]
References
Bray F, Laversanne M, Sung H, et al.: Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 74 (3): 229-263, 2024. [PUBMED Abstract]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Imperiale TF, Juluri R, Sherer EA, et al.: A risk index for advanced neoplasia on the second surveillance colonoscopy in patients with previous adenomatous polyps. Gastrointest Endosc 80 (3): 471-8, 2014. [PUBMED Abstract]
Singh H, Nugent Z, Demers A, et al.: Risk of colorectal cancer after diagnosis of endometrial cancer: a population-based study. J Clin Oncol 31 (16): 2010-5, 2013. [PUBMED Abstract]
Srinivasan R, Yang YX, Rubin SC, et al.: Risk of colorectal cancer in women with a prior diagnosis of gynecologic malignancy. J Clin Gastroenterol 41 (3): 291-6, 2007. [PUBMED Abstract]
Mork ME, You YN, Ying J, et al.: High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults With Colorectal Cancer. J Clin Oncol 33 (31): 3544-9, 2015. [PUBMED Abstract]
Laukoetter MG, Mennigen R, Hannig CM, et al.: Intestinal cancer risk in Crohn’s disease: a meta-analysis. J Gastrointest Surg 15 (4): 576-83, 2011. [PUBMED Abstract]
Fedirko V, Tramacere I, Bagnardi V, et al.: Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol 22 (9): 1958-72, 2011. [PUBMED Abstract]
Liang PS, Chen TY, Giovannucci E: Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer 124 (10): 2406-15, 2009. [PUBMED Abstract]
Laiyemo AO, Doubeni C, Pinsky PF, et al.: Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities. J Natl Cancer Inst 102 (8): 538-46, 2010. [PUBMED Abstract]
Lansdorp-Vogelaar I, Kuntz KM, Knudsen AB, et al.: Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol Biomarkers Prev 21 (5): 728-36, 2012. [PUBMED Abstract]
Ma Y, Yang Y, Wang F, et al.: Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One 8 (1): e53916, 2013. [PUBMED Abstract]
Steinberg SM, Barkin JS, Kaplan RS, et al.: Prognostic indicators of colon tumors. The Gastrointestinal Tumor Study Group experience. Cancer 57 (9): 1866-70, 1986. [PUBMED Abstract]
Filella X, Molina R, Grau JJ, et al.: Prognostic value of CA 19.9 levels in colorectal cancer. Ann Surg 216 (1): 55-9, 1992. [PUBMED Abstract]
McLeod HL, Murray GI: Tumour markers of prognosis in colorectal cancer. Br J Cancer 79 (2): 191-203, 1999. [PUBMED Abstract]
Jen J, Kim H, Piantadosi S, et al.: Allelic loss of chromosome 18q and prognosis in colorectal cancer. N Engl J Med 331 (4): 213-21, 1994. [PUBMED Abstract]
Lanza G, Matteuzzi M, Gafá R, et al.: Chromosome 18q allelic loss and prognosis in stage II and III colon cancer. Int J Cancer 79 (4): 390-5, 1998. [PUBMED Abstract]
Griffin MR, Bergstralh EJ, Coffey RJ, et al.: Predictors of survival after curative resection of carcinoma of the colon and rectum. Cancer 60 (9): 2318-24, 1987. [PUBMED Abstract]
Johnston PG, Fisher ER, Rockette HE, et al.: The role of thymidylate synthase expression in prognosis and outcome of adjuvant chemotherapy in patients with rectal cancer. J Clin Oncol 12 (12): 2640-7, 1994. [PUBMED Abstract]
Shibata D, Reale MA, Lavin P, et al.: The DCC protein and prognosis in colorectal cancer. N Engl J Med 335 (23): 1727-32, 1996. [PUBMED Abstract]
Bauer KD, Lincoln ST, Vera-Roman JM, et al.: Prognostic implications of proliferative activity and DNA aneuploidy in colonic adenocarcinomas. Lab Invest 57 (3): 329-35, 1987. [PUBMED Abstract]
Bauer KD, Bagwell CB, Giaretti W, et al.: Consensus review of the clinical utility of DNA flow cytometry in colorectal cancer. Cytometry 14 (5): 486-91, 1993. [PUBMED Abstract]
Sun XF, Carstensen JM, Zhang H, et al.: Prognostic significance of cytoplasmic p53 oncoprotein in colorectal adenocarcinoma. Lancet 340 (8832): 1369-73, 1992. [PUBMED Abstract]
Roth JA: p53 prognostication: paradigm or paradox? Clin Cancer Res 5 (11): 3345, 1999. [PUBMED Abstract]
Gryfe R, Kim H, Hsieh ET, et al.: Tumor microsatellite instability and clinical outcome in young patients with colorectal cancer. N Engl J Med 342 (2): 69-77, 2000. [PUBMED Abstract]
Watson P, Lin KM, Rodriguez-Bigas MA, et al.: Colorectal carcinoma survival among hereditary nonpolyposis colorectal carcinoma family members. Cancer 83 (2): 259-66, 1998. [PUBMED Abstract]
Iwashyna TJ, Lamont EB: Effectiveness of adjuvant fluorouracil in clinical practice: a population-based cohort study of elderly patients with stage III colon cancer. J Clin Oncol 20 (19): 3992-8, 2002. [PUBMED Abstract]
Chiara S, Nobile MT, Vincenti M, et al.: Advanced colorectal cancer in the elderly: results of consecutive trials with 5-fluorouracil-based chemotherapy. Cancer Chemother Pharmacol 42 (4): 336-40, 1998. [PUBMED Abstract]
Popescu RA, Norman A, Ross PJ, et al.: Adjuvant or palliative chemotherapy for colorectal cancer in patients 70 years or older. J Clin Oncol 17 (8): 2412-8, 1999. [PUBMED Abstract]
Dignam JJ, Colangelo L, Tian W, et al.: Outcomes among African-Americans and Caucasians in colon cancer adjuvant therapy trials: findings from the National Surgical Adjuvant Breast and Bowel Project. J Natl Cancer Inst 91 (22): 1933-40, 1999. [PUBMED Abstract]
Meyerhardt JA, Mangu PB, Flynn PJ, et al.: Follow-up care, surveillance protocol, and secondary prevention measures for survivors of colorectal cancer: American Society of Clinical Oncology clinical practice guideline endorsement. J Clin Oncol 31 (35): 4465-70, 2013. [PUBMED Abstract]
Benson AB, Bekaii-Saab T, Chan E, et al.: Localized colon cancer, version 3.2013: featured updates to the NCCN Guidelines. J Natl Compr Canc Netw 11 (5): 519-28, 2013. [PUBMED Abstract]
Martin EW, Minton JP, Carey LC: CEA-directed second-look surgery in the asymptomatic patient after primary resection of colorectal carcinoma. Ann Surg 202 (3): 310-7, 1985. [PUBMED Abstract]
Bruinvels DJ, Stiggelbout AM, Kievit J, et al.: Follow-up of patients with colorectal cancer. A meta-analysis. Ann Surg 219 (2): 174-82, 1994. [PUBMED Abstract]
Lautenbach E, Forde KA, Neugut AI: Benefits of colonoscopic surveillance after curative resection of colorectal cancer. Ann Surg 220 (2): 206-11, 1994. [PUBMED Abstract]
Khoury DA, Opelka FG, Beck DE, et al.: Colon surveillance after colorectal cancer surgery. Dis Colon Rectum 39 (3): 252-6, 1996. [PUBMED Abstract]
Safi F, Link KH, Beger HG: Is follow-up of colorectal cancer patients worthwhile? Dis Colon Rectum 36 (7): 636-43; discussion 643-4, 1993. [PUBMED Abstract]
Moertel CG, Fleming TR, Macdonald JS, et al.: An evaluation of the carcinoembryonic antigen (CEA) test for monitoring patients with resected colon cancer. JAMA 270 (8): 943-7, 1993. [PUBMED Abstract]
Rosen M, Chan L, Beart RW, et al.: Follow-up of colorectal cancer: a meta-analysis. Dis Colon Rectum 41 (9): 1116-26, 1998. [PUBMED Abstract]
Desch CE, Benson AB, Smith TJ, et al.: Recommended colorectal cancer surveillance guidelines by the American Society of Clinical Oncology. J Clin Oncol 17 (4): 1312, 1999. [PUBMED Abstract]
Benson AB, Desch CE, Flynn PJ, et al.: 2000 update of American Society of Clinical Oncology colorectal cancer surveillance guidelines. J Clin Oncol 18 (20): 3586-8, 2000. [PUBMED Abstract]
Clinical practice guidelines for the use of tumor markers in breast and colorectal cancer. Adopted on May 17, 1996 by the American Society of Clinical Oncology. J Clin Oncol 14 (10): 2843-77, 1996. [PUBMED Abstract]
Meyerhardt JA, Niedzwiecki D, Hollis D, et al.: Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer. JAMA 298 (7): 754-64, 2007. [PUBMED Abstract]
Meyerhardt JA, Sato K, Niedzwiecki D, et al.: Dietary glycemic load and cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Natl Cancer Inst 104 (22): 1702-11, 2012. [PUBMED Abstract]
McCullough ML, Gapstur SM, Shah R, et al.: Association between red and processed meat intake and mortality among colorectal cancer survivors. J Clin Oncol 31 (22): 2773-82, 2013. [PUBMED Abstract]
Je Y, Jeon JY, Giovannucci EL, et al.: Association between physical activity and mortality in colorectal cancer: a meta-analysis of prospective cohort studies. Int J Cancer 133 (8): 1905-13, 2013. [PUBMED Abstract]
Chan AT, Ogino S, Fuchs CS: Aspirin use and survival after diagnosis of colorectal cancer. JAMA 302 (6): 649-58, 2009. [PUBMED Abstract]
Liao X, Lochhead P, Nishihara R, et al.: Aspirin use, tumor PIK3CA mutation, and colorectal-cancer survival. N Engl J Med 367 (17): 1596-606, 2012. [PUBMED Abstract]
Cellular Classification of Colon Cancer
Histological types of colon cancer include:
Adenocarcinoma (most colon cancers).
Mucinous (colloid) adenocarcinoma.
Signet ring adenocarcinoma.
Scirrhous tumors.
Neuroendocrine.[1] Tumors with neuroendocrine differentiation typically have a poorer prognosis than pure adenocarcinoma variants.
References
Saclarides TJ, Szeluga D, Staren ED: Neuroendocrine cancers of the colon and rectum. Results of a ten-year experience. Dis Colon Rectum 37 (7): 635-42, 1994. [PUBMED Abstract]
Stage Information for Colon Cancer
Treatment decisions can be made with reference to the TNM (tumor, node, metastasis) classification [1] rather than to the older Dukes or the Modified Astler-Coller classification schema.
The AJCC and a National Cancer Institute–sponsored panel recommended that at least 12 lymph nodes be examined in patients with colon and rectal cancer to confirm the absence of nodal involvement by tumor.[1–3] This recommendation takes into consideration that the number of lymph nodes examined is a reflection of the aggressiveness of lymphovascular mesenteric dissection at the time of surgical resection and the pathological identification of nodes in the specimen. Retrospective studies demonstrated that the number of lymph nodes examined in colon and rectal surgery may be associated with patient outcome.[4–7]
AJCC Stage Groupings and TNM Definitions
The AJCC has designated staging by TNM classification to define colon cancer.[1] The same classification is used for both clinical and pathological staging.[1]
Table 1. Definitions of TNM Stage 0a
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
0
Tis, N0, M0
Tis = Carcinoma in situ, intramucosal carcinoma (involvement of lamina propria with no extension through muscularis mucosae).
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 2. Definitions of TNM Stage Ia
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
I
T1, T2, N0, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 3. Definitions of TNM Stages IIA, IIB, and IICa
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
IIA
T3, N0, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIB
T4a, N0, M0
T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N0 = No regional lymph node metastasis.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIC
T4b, N0, M0
T4b = Tumor directly invades or adheres to adjacent organs or structures.
N0 = No regional lymph node metastasis.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 4. Definitions of TNM Stages IIIA, IIIB, and IIICa
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
IIIA
T1, N2a, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T1–2, N1/N1c, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
T2 = Tumor invades the muscularis propria.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIIB
T1–T2, N2b, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T2–T3, N2a, M0
T2 = Tumor invades the muscularis propria.
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T3–T4a, N1/N1c, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIIC
T3–T4a, N2b, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T4a, N2a, M0
T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T4b, N1–N2, M0
T4b = Tumor directly invades or adheres to adjacent organs or structures.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1a = One regional lymph node is positive.
–N1b = Two or three regional lymph nodes are positive.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
N2 = Four or more regional nodes are positive.
–N2a = Four to six regional lymph nodes are positive.
–N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 5. Definitions of TNM Stages IVA, IVB, and IVCa
Stage
TNMb,c
Definition
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
bDirect invasion in T4 includes invasion of other organs or other segments of the colorectum as a result of direct extension through the serosa, as confirmed on microscopic examination (e.g., invasion of the sigmoid colon by a carcinoma of the cecum) or, for cancers in a retroperitoneal or subperitoneal location, direct invasion of other organs or structures by virtue of extension beyond the muscularis propria (i.e., respectively, a tumor on the posterior wall of the descending colon invading the left kidney or lateral abdominal wall; or a mid or distal rectal cancer with invasion of prostate, seminal vesicles, cervix, or vagina).
cTumor that is adherent to other organs or structures, grossly, is classified cT4b. However, if no tumor is present in the adhesion, microscopically, the classification should be pT1-4a depending on the anatomical depth of wall invasion. The V and L classification should be used to identify the presence or absence of vascular or lymphatic invasion whereas the PN prognostic factor should be used for perineural invasion.
Tis = Carcinoma in situ, intramucosal carcinoma (involvement of lamina propria with no extension through muscularis mucosae).
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
T2 = Tumor invades the muscularis propria.
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
–T4b = Tumor directly invades or adheres to adjacent organs or structures.
NX = Regional lymph nodes cannot be assessed.
N0 = No regional lymph node metastasis.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1a = One regional lymph node is positive.
–N1b = Two or three regional lymph nodes are positive.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
N2 = Four or more regional nodes are positive.
–N2a = Four to six regional lymph nodes are positive.
–N2b = Seven or more regional lymph nodes are positive.
M1a = Metastasis to one site or organ is identified without peritoneal metastasis.
IVB
Any T, Any N, M1b
Any T = See T descriptions above in Any T, Any N, M1a TNM stage group.
Any N = See N descriptions above in Any T, Any N1, M1a TNM stage group.
M1b = Metastasis to two or more sites or organs is identified without peritoneal metastasis.
IVC
Any T, Any N, M1c
Any T = See T descriptions above in Any T, Any N, M1a TNM stage group.
Any N = See N descriptions above in Any T, Any N1, M1a TNM stage group.
M1c = Metastasis to the peritoneal surface is identified alone or with other site or organ metastases.
References
Jessup J, Benson A, Chen V: Colon and Rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp 251–74.
Compton CC, Greene FL: The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin 54 (6): 295-308, 2004 Nov-Dec. [PUBMED Abstract]
Nelson H, Petrelli N, Carlin A, et al.: Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst 93 (8): 583-96, 2001. [PUBMED Abstract]
Swanson RS, Compton CC, Stewart AK, et al.: The prognosis of T3N0 colon cancer is dependent on the number of lymph nodes examined. Ann Surg Oncol 10 (1): 65-71, 2003 Jan-Feb. [PUBMED Abstract]
Le Voyer TE, Sigurdson ER, Hanlon AL, et al.: Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol 21 (15): 2912-9, 2003. [PUBMED Abstract]
Prandi M, Lionetto R, Bini A, et al.: Prognostic evaluation of stage B colon cancer patients is improved by an adequate lymphadenectomy: results of a secondary analysis of a large scale adjuvant trial. Ann Surg 235 (4): 458-63, 2002. [PUBMED Abstract]
Tepper JE, O’Connell MJ, Niedzwiecki D, et al.: Impact of number of nodes retrieved on outcome in patients with rectal cancer. J Clin Oncol 19 (1): 157-63, 2001. [PUBMED Abstract]
Standard treatment for patients with colon cancer has been open surgical resection of the primary and regional lymph nodes for localized disease.
The role of laparoscopic techniques [1–4] in the treatment of colon cancer has been examined in two studies.
Evidence (laparoscopic techniques):
A multicenter, prospective, randomized, noninferiority trial (NCCTG-934653 [NCT00002575]) compared laparoscopic-assisted colectomy (LAC) with open colectomy in 872 patients.
At a median follow-up of 4.4 years, 3-year recurrence rates (16% LAC vs. 18% open colectomy; hazard ratio [HR] for recurrence, 0.86; 95% confidence interval [CI], 0.63–1.17; P = .32) and 3-year overall survival (OS) rates (86% LAC vs. 85% open colectomy; HRdeath in LAC, 0.91; 95% CI, 0.68–1.21; P = .51) were similar in both groups for all stages of disease evaluated. Tumor recurrence in surgical incisions was less than 1% for both groups.[5][Level of evidence A1]
Decreased hospital stay (5 days LAC vs. 6 days open colectomy, P < .001) and decreased use of analgesics were reported in the LAC group. A 21% conversion rate from LAC to open procedure was shown.
This study excluded patients with locally advanced disease, transverse colon and rectal tumor locations, and perforated lesions. Each of the 66 surgeons participating in the trial had performed at least 20 LACs and were accredited for study participation after independent videotape review assured appropriate oncologic and surgical principles were maintained.[5] The quality-of-life component of this trial was published separately and minimal short-term quality-of-life benefits with LAC were reported.[6][Level of evidence A3]
One small, single-institution randomized study of 219 patients showed that the LAC procedure was independently associated with reduced tumor recurrence on multivariate analysis.[7][Level of evidence A1]
Surgery is curative in 25% to 40% of highly selected patients who develop resectable metastases in the liver and lung. Improved surgical techniques and advances in preoperative imaging have allowed for better patient selection for resection.
Adjuvant Chemotherapy
The potential value of adjuvant chemotherapy for patients with stage II colon cancer is controversial. Pooled analyses and meta-analyses have suggested a 2% to 4% improvement in OS for patients treated with adjuvant fluorouracil (5-FU)–based therapy compared with observation.[8–10] For more information, see the Treatment of Stage II Colon Cancer section.
Before 2000, 5-FU was the only useful cytotoxic chemotherapy in the adjuvant setting for patients with stage III colon cancer. Since 2000, capecitabine has been established as an equivalent alternative to 5-FU and leucovorin (5-FU/LV). The addition of oxaliplatin to 5-FU/LV has been shown to improve OS compared with 5-FU/LV alone. For more information, see the Treatment of Stage III Colon Cancer section.
Chemotherapy regimens
Table 7 describes the chemotherapy regimens used to treat colon cancer.
Table 7. Drug Combinations Used to Treat Colon Cancer
Regimen Name
Drug Combination
Dose
5-FU = fluorouracil; AIO = Arbeitsgemeinschaft Internistische Onkologie; bid = twice a day; IV = intravenous; LV = leucovorin.
AIO or German AIO
Folic acid, 5-FU, and irinotecan
Irinotecan (100 mg/m2) and LV (500 mg/m2) administered as 2-hour infusions on d 1, followed by 5-FU (2,000 mg/m2) IV bolus administered via ambulatory pump weekly over 24 h, 4 times a y (52 wk).
CAPOX
Capecitabine and oxaliplatin
Capecitabine (1,000 mg/m2) bid on d 1–14, plus oxaliplatin (70 mg/m2) on d 1 and 8 every 3 wk.
Douillard
Folic acid, 5-FU, and irinotecan
Irinotecan (180 mg/m2) administered as a 2-h infusion on d 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2.
FOLFIRI
LV, 5-FU, and irinotecan
Irinotecan (180 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus administered on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk.
FOLFOX-4
Oxaliplatin, LV, and 5-FU
Oxaliplatin (85 mg/m2) administered as a 2-h infusion on d 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2.
FOLFOX-6
Oxaliplatin, LV, and 5-FU
Oxaliplatin (85–100 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk.
FOLFOXIRI
Irinotecan, oxaliplatin, LV, 5-FU
Irinotecan (165 mg/m2) administered as a 60-min infusion, then concomitant infusion of oxaliplatin (85 mg/m2) and LV (200 mg/m2) over 120 min, followed by 5-FU (3,200 mg/m2) administered as a 48-h continuous infusion.
FUFOX
5-FU, LV, and oxaliplatin
Oxaliplatin (50 mg/m2) plus LV (500 mg/m2) plus 5-FU (2,000 mg/m2) administered as a 22-h continuous infusion on d 1, 8, 22, and 29 every 36 d.
FUOX
5-FU plus oxaliplatin
5-FU (2,250 mg/m2) administered as a continuous infusion over 48 h on d 1, 8, 15, 22, 29, and 36 plus oxaliplatin (85 mg/m2) on d 1, 15, and 29 every 6 wk.
IFL (or Saltz)
Irinotecan, 5-FU, and LV
Irinotecan (125 mg/m2) plus 5-FU (500 mg/m2) IV bolus and LV (20 mg/m2) IV bolus administered weekly for 4 out of 6 wk.
XELOX
Capecitabine plus oxaliplatin
Oral capecitabine (1,000 mg/m2) administered bid for 14 d plus oxaliplatin (130 mg/m2) on d 1 every 3 wk.
Capecitabine and fluorouracil dosing
The DPYD gene encodes an enzyme that catabolizes pyrimidines and fluoropyrimidines, like capecitabine and fluorouracil. An estimated 1% to 2% of the population has germline pathogenic variants in DPYD, which lead to reduced DPD protein function and an accumulation of pyrimidines and fluoropyrimidines in the body.[11,12] Patients with the DPYD*2A variant who receive fluoropyrimidines may experience severe, life-threatening toxicities that are sometimes fatal. Many other DPYD variants have been identified, with a range of clinical effects.[11–13] Fluoropyrimidine avoidance or a dose reduction of 50% may be recommended based on the patient’s DPYD genotype and number of functioning DPYD alleles.[14–16] DPYD genetic testing costs less than $200, but insurance coverage varies due to a lack of national guidelines.[17] In addition, testing may delay therapy by 2 weeks, which would not be advisable in urgent situations. This controversial issue requires further evaluation.[18]
Adjuvant Radiation Therapy
While combined modality therapy with chemotherapy and radiation therapy has a significant role in the management of patients with rectal cancer (below the peritoneal reflection), the role of adjuvant radiation therapy for patients with colon cancer (above the peritoneal reflection) is not well defined. Patterns-of-care analyses and single-institution retrospective reviews suggest a role for radiation therapy in certain high-risk subsets of colon cancer patients (e.g., T4, tumor location in immobile sites, local perforation, obstruction, and residual disease postresection).[19–24]
Evidence (adjuvant radiation therapy):
A phase III, randomized, intergroup study evaluated the benefit of adding radiation therapy to surgery and chemotherapy with 5-FU-levamisole in selected patients with high-risk colon cancer (e.g., T4; or T3, N1–N2 ascending and/or descending colon).[25]
This clinical trial closed early secondary to inadequate patient accrual. An analysis of 222 enrolled patients (the original goal was 700 patients) demonstrated no relapse or OS benefit for the group that received radiation therapy, although the sample size and statistical power were inadequate to exclude benefit.
Adjuvant radiation therapy has no current standard role in the management of patients with colon cancer following curative resection, although it may have a role for patients with residual disease.
References
Bokey EL, Moore JW, Chapuis PH, et al.: Morbidity and mortality following laparoscopic-assisted right hemicolectomy for cancer. Dis Colon Rectum 39 (10 Suppl): S24-8, 1996. [PUBMED Abstract]
Franklin ME, Rosenthal D, Abrego-Medina D, et al.: Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum 39 (10 Suppl): S35-46, 1996. [PUBMED Abstract]
Fleshman JW, Nelson H, Peters WR, et al.: Early results of laparoscopic surgery for colorectal cancer. Retrospective analysis of 372 patients treated by Clinical Outcomes of Surgical Therapy (COST) Study Group. Dis Colon Rectum 39 (10 Suppl): S53-8, 1996. [PUBMED Abstract]
Schwenk W, Böhm B, Müller JM: Postoperative pain and fatigue after laparoscopic or conventional colorectal resections. A prospective randomized trial. Surg Endosc 12 (9): 1131-6, 1998. [PUBMED Abstract]
Clinical Outcomes of Surgical Therapy Study Group: A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350 (20): 2050-9, 2004. [PUBMED Abstract]
Weeks JC, Nelson H, Gelber S, et al.: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287 (3): 321-8, 2002. [PUBMED Abstract]
Lacy AM, García-Valdecasas JC, Delgado S, et al.: Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 359 (9325): 2224-9, 2002. [PUBMED Abstract]
Efficacy of adjuvant fluorouracil and folinic acid in B2 colon cancer. International Multicentre Pooled Analysis of B2 Colon Cancer Trials (IMPACT B2) Investigators. J Clin Oncol 17 (5): 1356-63, 1999. [PUBMED Abstract]
Gill S, Loprinzi CL, Sargent DJ, et al.: Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: who benefits and by how much? J Clin Oncol 22 (10): 1797-806, 2004. [PUBMED Abstract]
Mamounas E, Wieand S, Wolmark N, et al.: Comparative efficacy of adjuvant chemotherapy in patients with Dukes’ B versus Dukes’ C colon cancer: results from four National Surgical Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04) J Clin Oncol 17 (5): 1349-55, 1999. [PUBMED Abstract]
Sharma BB, Rai K, Blunt H, et al.: Pathogenic DPYD Variants and Treatment-Related Mortality in Patients Receiving Fluoropyrimidine Chemotherapy: A Systematic Review and Meta-Analysis. Oncologist 26 (12): 1008-1016, 2021. [PUBMED Abstract]
Lam SW, Guchelaar HJ, Boven E: The role of pharmacogenetics in capecitabine efficacy and toxicity. Cancer Treat Rev 50: 9-22, 2016. [PUBMED Abstract]
Shakeel F, Fang F, Kwon JW, et al.: Patients carrying DPYD variant alleles have increased risk of severe toxicity and related treatment modifications during fluoropyrimidine chemotherapy. Pharmacogenomics 22 (3): 145-155, 2021. [PUBMED Abstract]
Amstutz U, Henricks LM, Offer SM, et al.: Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clin Pharmacol Ther 103 (2): 210-216, 2018. [PUBMED Abstract]
Henricks LM, Lunenburg CATC, de Man FM, et al.: DPYD genotype-guided dose individualisation of fluoropyrimidine therapy in patients with cancer: a prospective safety analysis. Lancet Oncol 19 (11): 1459-1467, 2018. [PUBMED Abstract]
Lau-Min KS, Varughese LA, Nelson MN, et al.: Preemptive pharmacogenetic testing to guide chemotherapy dosing in patients with gastrointestinal malignancies: a qualitative study of barriers to implementation. BMC Cancer 22 (1): 47, 2022. [PUBMED Abstract]
Brooks GA, Tapp S, Daly AT, et al.: Cost-effectiveness of DPYD Genotyping Prior to Fluoropyrimidine-based Adjuvant Chemotherapy for Colon Cancer. Clin Colorectal Cancer 21 (3): e189-e195, 2022. [PUBMED Abstract]
Baker SD, Bates SE, Brooks GA, et al.: DPYD Testing: Time to Put Patient Safety First. J Clin Oncol 41 (15): 2701-2705, 2023. [PUBMED Abstract]
Willett C, Tepper JE, Cohen A, et al.: Local failure following curative resection of colonic adenocarcinoma. Int J Radiat Oncol Biol Phys 10 (5): 645-51, 1984. [PUBMED Abstract]
Willett C, Tepper JE, Cohen A, et al.: Obstructive and perforative colonic carcinoma: patterns of failure. J Clin Oncol 3 (3): 379-84, 1985. [PUBMED Abstract]
Gunderson LL, Sosin H, Levitt S: Extrapelvic colon–areas of failure in a reoperation series: implications for adjuvant therapy. Int J Radiat Oncol Biol Phys 11 (4): 731-41, 1985. [PUBMED Abstract]
Willett CG, Goldberg S, Shellito PC, et al.: Does postoperative irradiation play a role in the adjuvant therapy of stage T4 colon cancer? Cancer J Sci Am 5 (4): 242-7, 1999 Jul-Aug. [PUBMED Abstract]
Schild SE, Gunderson LL, Haddock MG, et al.: The treatment of locally advanced colon cancer. Int J Radiat Oncol Biol Phys 37 (1): 51-8, 1997. [PUBMED Abstract]
Martenson JA, Willett CG, Sargent DJ, et al.: Phase III study of adjuvant chemotherapy and radiation therapy compared with chemotherapy alone in the surgical adjuvant treatment of colon cancer: results of intergroup protocol 0130. J Clin Oncol 22 (16): 3277-83, 2004. [PUBMED Abstract]
Treatment of Stage 0 Colon Cancer
Stage 0 colon cancer is the most superficial of all the lesions and is limited to the mucosa without invasion of the lamina propria. Because of its superficial nature, the surgical procedure may be limited.
Surgical options include local excision or simple polypectomy with clear margins, or colon resection for larger lesions not amenable to local excision.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Treatment of Stage I Colon Cancer
Because of its localized nature, stage I colon cancer has a high cure rate.
The role of laparoscopic techniques [1–4] in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) with open colectomy.
Three-year recurrence rates and 3-year overall survival rates were similar in the two groups. For more information, see the Primary Surgical Therapy section.
The quality-of-life component of this trial has been published and minimal short-term quality-of-life benefits with LAC were reported.[5][Level of evidence A3]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Bokey EL, Moore JW, Chapuis PH, et al.: Morbidity and mortality following laparoscopic-assisted right hemicolectomy for cancer. Dis Colon Rectum 39 (10 Suppl): S24-8, 1996. [PUBMED Abstract]
Franklin ME, Rosenthal D, Abrego-Medina D, et al.: Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum 39 (10 Suppl): S35-46, 1996. [PUBMED Abstract]
Fleshman JW, Nelson H, Peters WR, et al.: Early results of laparoscopic surgery for colorectal cancer. Retrospective analysis of 372 patients treated by Clinical Outcomes of Surgical Therapy (COST) Study Group. Dis Colon Rectum 39 (10 Suppl): S53-8, 1996. [PUBMED Abstract]
Schwenk W, Böhm B, Müller JM: Postoperative pain and fatigue after laparoscopic or conventional colorectal resections. A prospective randomized trial. Surg Endosc 12 (9): 1131-6, 1998. [PUBMED Abstract]
Weeks JC, Nelson H, Gelber S, et al.: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287 (3): 321-8, 2002. [PUBMED Abstract]
The role of laparoscopic techniques [1–4] in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) to open colectomy.
Three-year recurrence rates and 3-year overall survival (OS) rates were similar in the two groups. For more information, see the Primary Surgical Therapy section.
The quality-of-life component of this trial reported minimal short-term quality-of-life benefits with LAC.[4][Level of evidence A3]
Adjuvant chemotherapy
The potential value of adjuvant chemotherapy for patients with stage II colon cancer remains controversial. Although subgroups of patients with stage II colon cancer may be at higher-than-average risk for recurrence (including those with anatomical features such as tumor adherence to adjacent structures, perforation, and complete obstruction),[5–7] evidence is inconsistent that adjuvant fluorouracil (5-FU)–based chemotherapy is associated with an improved OS compared with surgery alone.[8]
Features in patients with stage II colon cancer that are associated with an increased risk of recurrence include:
Inadequate lymph node sampling.
T4 disease.
Involvement of the visceral peritoneum.
A poorly differentiated histology.
The decision to use adjuvant chemotherapy for patients with stage II colon cancer is complicated and requires thoughtful consideration by both patients and their physicians. Adjuvant therapy is not indicated for most patients unless they are entered into a clinical trial.
Evidence (adjuvant chemotherapy):
The GRECCR-03 (NCT00046995) and NCRI-QUASAR1 (NCT00005586) trials evaluated the use of systemic or regional chemotherapy or biological therapy. Following surgery, patients can be considered for entry into a carefully controlled clinical trial.
Investigators from the National Surgical Adjuvant Breast and Bowel Project have indicated that the reduction in risk of recurrence by adjuvant therapy in patients with stage II disease is of similar magnitude to the benefit seen in patients with stage III disease treated with adjuvant therapy, though an OS advantage has not been established.[9]
A meta-analysis of 1,000 stage II patients whose experience was amalgamated from a series of trials indicates a 2% advantage in disease-free survival at 5 years when adjuvant therapy–treated patients treated with 5-FU/leucovorin are compared with untreated controls.[10][Level of evidence B1]; [11]
The Cancer Care Ontario Practice Guideline Initiative Gastrointestinal Cancer Disease Site Group undertook a meta-analysis of the English language–published literature consisting of randomized trials in which adjuvant chemotherapy was compared with observation for patients with stage II colon cancer.
The mortality risk ratio was 0.87 (95% confidence interval, 0.75–1.01; P = .07).[12]
Based on these data, the American Society of Clinical Oncology issued a guideline stating “direct evidence from randomized controlled trials does not support the routine use of adjuvant chemotherapy for patients with stage II colon cancer.”[13]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Bokey EL, Moore JW, Chapuis PH, et al.: Morbidity and mortality following laparoscopic-assisted right hemicolectomy for cancer. Dis Colon Rectum 39 (10 Suppl): S24-8, 1996. [PUBMED Abstract]
Franklin ME, Rosenthal D, Abrego-Medina D, et al.: Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum 39 (10 Suppl): S35-46, 1996. [PUBMED Abstract]
Fleshman JW, Nelson H, Peters WR, et al.: Early results of laparoscopic surgery for colorectal cancer. Retrospective analysis of 372 patients treated by Clinical Outcomes of Surgical Therapy (COST) Study Group. Dis Colon Rectum 39 (10 Suppl): S53-8, 1996. [PUBMED Abstract]
Weeks JC, Nelson H, Gelber S, et al.: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287 (3): 321-8, 2002. [PUBMED Abstract]
Lanza G, Matteuzzi M, Gafá R, et al.: Chromosome 18q allelic loss and prognosis in stage II and III colon cancer. Int J Cancer 79 (4): 390-5, 1998. [PUBMED Abstract]
Jen J, Kim H, Piantadosi S, et al.: Allelic loss of chromosome 18q and prognosis in colorectal cancer. N Engl J Med 331 (4): 213-21, 1994. [PUBMED Abstract]
Merkel S, Wein A, Günther K, et al.: High-risk groups of patients with Stage II colon carcinoma. Cancer 92 (6): 1435-43, 2001. [PUBMED Abstract]
Moertel CG, Fleming TR, Macdonald JS, et al.: Intergroup study of fluorouracil plus levamisole as adjuvant therapy for stage II/Dukes’ B2 colon cancer. J Clin Oncol 13 (12): 2936-43, 1995. [PUBMED Abstract]
Mamounas E, Wieand S, Wolmark N, et al.: Comparative efficacy of adjuvant chemotherapy in patients with Dukes’ B versus Dukes’ C colon cancer: results from four National Surgical Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04) J Clin Oncol 17 (5): 1349-55, 1999. [PUBMED Abstract]
Efficacy of adjuvant fluorouracil and folinic acid in B2 colon cancer. International Multicentre Pooled Analysis of B2 Colon Cancer Trials (IMPACT B2) Investigators. J Clin Oncol 17 (5): 1356-63, 1999. [PUBMED Abstract]
Harrington DP: The tea leaves of small trials. J Clin Oncol 17 (5): 1336-8, 1999. [PUBMED Abstract]
Figueredo A, Charette ML, Maroun J, et al.: Adjuvant therapy for stage II colon cancer: a systematic review from the Cancer Care Ontario Program in evidence-based care’s gastrointestinal cancer disease site group. J Clin Oncol 22 (16): 3395-407, 2004. [PUBMED Abstract]
Benson AB, Schrag D, Somerfield MR, et al.: American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol 22 (16): 3408-19, 2004. [PUBMED Abstract]
Treatment of Stage III Colon Cancer
Stage III colon cancer denotes lymph node involvement. Studies have indicated that the number of lymph nodes involved affects prognosis; patients with one to three involved nodes have a significantly better survival than those with four or more involved nodes.
Clinical trials. Eligible patients can consider enrollment in carefully controlled clinical trials comparing various postoperative chemotherapy regimens.[1]
Surgery
Surgery for stage III colon cancer is wide surgical resection and anastomosis.
Evidence (laparoscopic techniques):
The role of laparoscopic techniques [2–5] in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) with open colectomy.
Three-year recurrence rates and 3-year overall survival (OS) rates were similar in the two groups. For more information, see the Primary Surgical Therapy section.
The quality-of-life component of this trial has been published and minimal short-term quality-of-life benefits with LAC were reported.[6][Level of evidence A3]
Adjuvant chemotherapy
Chemotherapy regimens before 2000
Before 2000, fluorouracil (5-FU) was the only useful cytotoxic chemotherapy in the adjuvant setting for patients with stage III colon cancer. Many of the early randomized studies of 5-FU in the adjuvant setting failed to show a significant improvement in survival for patients.[7–10] These trials employed 5-FU alone or 5-FU/semustine.
Evidence (5-FU alone and 5-FU/semustine):
The North Central Cancer Treatment Group conducted a randomized trial comparing surgical resection alone with postoperative levamisole or levamisole/5-FU.[11][Level of evidence A1]
A significant improvement in disease-free survival (DFS) was observed for patients with stage III colon cancer who received levamisole/5-FU, but OS benefits were of borderline statistical significance.
An absolute survival benefit of approximately 12% (49% vs. 37%) was seen in patients with stage III disease treated with levamisole/5-FU.
In a large confirmatory intergroup trial, levamisole/5-FU- prolonged DFS and OS in patients with stage III colon cancer compared with patients who received no treatment after surgery.[12][Level of evidence A1] Levamisole alone did not confer these benefits.
Subsequent studies tested the combination of 5-FU/leucovorin (5-FU/LV) in the adjuvant treatment of patients with resected carcinoma of the colon.
Results of multiple randomized trials that have enrolled more than 4,000 patients comparing adjuvant chemotherapy with 5-FU/LV to surgery or 5-FU/semustine/vincristine demonstrate a relative reduction in mortality of between 22% and 33% (3-year OS of 71%–78% increased to 75%–84%).[13–15]
The completed Intergroup trial 0089 (INT-0089 [NCT00201331]) randomly assigned 3,794 patients with high-risk stage II or stage III colon cancer to one of the following four treatment arms:[16]
The Mayo Clinic regimen administered for a total of six cycles.
The Roswell Park regimen administered for a total of four cycles.
The Mayo Clinic regimen administered with levamisole for six cycles.
The levamisole regimen administered for a total of 1 year.
Results:
Five-year OS ranged from 49% for the Mayo Clinic regimen with levamisole to 60% for the Mayo Clinic regimen, and there were no statistically significant differences among treatment arms.[16][Level of evidence A1]
A preliminary report in November 1997 demonstrated a statistically significant advantage for OS for the Mayo Clinic regimen with levamisole compared with the levamisole regimen. This difference became insignificant with longer follow-up.
Overall, grade 3 or greater toxicity occurred more frequently for the Mayo Clinic regimen and the Mayo Clinic regimen with levamisole. In addition, the Mayo Clinic regimen was significantly more toxic with levamisole than without levamisole.
The death rate for all four regimens ranged from 0.5% to 1%.
Because of its ease of use and its good toxicity profile, the Roswell Park regimen became the preferred adjuvant regimen used in the United States and was often the control arm in subsequent randomized studies.
In addition to INT-0089, multiple studies have refined the use of 5-FU/LV in the adjuvant setting and can be summarized as follows:
Levamisole is unnecessary when using leucovorin.[16]
Treatment that includes 6 to 8 months of 5-FU/LV is equivalent to 12 months of therapy.[17–19]
Treatment that includes 24 weeks of adjuvant 5-FU/LV is equivalent to 36 weeks of therapy.[20]
High-dose leucovorin is equivalent to low-dose leucovorin.[21]
A meta-analysis of seven trials revealed no significant difference in efficacy or toxicity among patients aged 70 years or younger compared with patients older than 70 years.[22]
An infusional de Gramont bolus and infusional 5-FU/LV schedule is safer than a bolus modified Mayo Clinic schedule of 5-FU/LV.[20]
Chemotherapy regimens after 2000
Capecitabine
Capecitabine is an oral fluoropyrimidine that undergoes a three-step enzymatic conversion to 5-FU with the last step occurring in the tumor cell. For patients with metastatic colon cancer, two studies have demonstrated the equivalence of capecitabine to 5-FU/LV.[23,24]
For patients with stage III colon cancer, capecitabine provides equivalent outcome to intravenous 5-FU/LV.
Evidence (capecitabine):
A multicenter European study compared capecitabine (1,250 mg/m2) administered twice daily for days 1 to 14, then given every 21 days for eight cycles against the Mayo Clinic schedule of 5-FU and low-dose LV for patients with stage III colon cancer.[25]
The study demonstrated that DFS at 3 years is equivalent for patients who received capecitabine or 5-FU/LV (hazard ratio [HR], 0.87; P < .001).[25][Level of evidence B1]
Hand-foot syndrome and hyperbilirubinemia were significantly more common for patients receiving capecitabine, but diarrhea, nausea or vomiting, stomatitis, alopecia, and neutropenia were significantly less common.
Of patients receiving capecitabine, 57% required a dose modification.
For patients with stage III colon cancer in whom treatment with 5-FU/LV is planned, capecitabine is an equivalent alternative.
Oxaliplatin
Oxaliplatin has significant activity when combined with 5-FU/LV in patients with metastatic colorectal cancer.
Evidence (oxaliplatin):
In the 2,246 patients with resected stage II or stage III colon cancer in the completed Multicenter International Study of Oxaliplatin/Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer study (MOSAIC [NCT00275210]), the toxic effects and efficacy of FOLFOX-4 (oxaliplatin/LV/5-FU) were compared with the same 5-FU/LV regimen without oxaliplatin administered for 6 months.[26] Based on results from the MOSAIC trial, adjuvant FOLFOX-4 demonstrated prolonged OS for patients with stage III colon cancer compared with patients receiving 5-FU/LV without oxaliplatin.[27]
The preliminary results of the study with 37 months of follow-up demonstrated a significant improvement in DFS at 3 years (77.8% vs. 72.9%; P = .01) in favor of FOLFOX-4. When initially reported, there was no difference in OS.[27][Level of evidence B1]
Further follow-up at 6 years demonstrated that the OS for all patients (both stage II and stage III) who entered the study was not significantly different (OS, 78.5% vs. 76.0%; HR, 0.84; 95% confidence interval [CI], 0.71–1.00). On subset analysis, the 6-year OS in patients with stage III colon cancer was 72.9% in the patients receiving FOLFOX-4 and 68.7% in the patients receiving 5-FU/LV (HR, 0.80; 95% CI, 0.65–0.97; P = .023).[27][Level of evidence A1]
Patients treated with FOLFOX-4 experienced more frequent toxic effects consisting mainly of neutropenia (41% >grade 3) and reversible peripheral sensorial neuropathy (12.4% >grade 3).
In a randomized phase III study (NSABP C-07 [NCT00004931]), 2,407 patients with stage II or stage III colon cancer were randomly assigned to adjuvant 5-FU/LV or fluorouracil-leucovorin-oxaliplatin (FLOX) (weekly 5-FU/LV with oxaliplatin administered on weeks 1, 3, and 5 of each 6-week cycle). DFS was the primary end point of the study.[28]
DFS was significantly longer in the treatment group who received FLOX, but OS was not significantly different. The DFS rate was 69.4% for patients who received FLOX and 64.2% for patients who received 5-FU/LV (HR, 0.82; 95% CI, 0.72–0.93; P = .0034).
The OS rate at 5 years was 80.2% for patients who received FLOX and 78.4% for patients who received 5-FU/LV (HR, 0.88; 95% CI, 0.75–1.02; P = .08).[28][Level of evidence B1]
Grade 3 and grade 4 diarrhea was experienced by 36.9% of patients who received FLOX, and grade 3 and grade 4 dehydration was experienced by 16.1% of patients who received FLOX.
Most physicians have adopted FOLFOX as the standard of care because of toxicity concerns with weekly FLOX. FOLFOX has become the reference standard for the next generation of clinical trials for patients with stage III colon cancer.[27]
Capecitabine and oxaliplatin
The combination of capecitabine and oxaliplatin (CAPOX) is an accepted standard therapy in patients with metastatic colorectal cancer.
Evidence (CAPOX):
CAPOX was evaluated in the adjuvant setting for patients with resected stage III colon cancer (capecitabine 1,000 mg/m2 bid on days 1 to 14 every 21 days and oxaliplatin 130 mg/m2 every 21 days for a total of 8 cycles).[29] A randomized phase III trial (NO16968 [NCT00069121]), randomly assigned 1,886 patients with stage III colon cancer to receive CAPOX or bolus 5FU-LV (Roswell Park or Mayo Clinic schedule).
The 7-year DFS rates were 63% for patients who received CAPOX and 56% for patients who received bolus 5-FU/LV (HR, 0.8; 95% CI, 0.69–0.93; P = .004).
The 7-year OS rates were 73% for patients who received CAPOX and 67% for patients who received a bolus 5-FU/LV (HR, 0.83; 95% CI, 0.70–0.99; P = .04).[29][Level of evidence A1]
Based on this trial, CAPOX has become an acceptable standard regimen for patients with stage III colon cancer.
Oxaliplatin length of therapy
Given the high rate of disabling neuropathy, the duration of oxaliplatin adjuvant therapy became an open question.
Evidence (length of therapy for oxaliplatin):
The International Duration Evaluation of Adjuvant Therapy (IDEA) collaboration consisted of six separate randomized trials with regimens of 6 months versus 3 months of adjuvant oxaliplatin-based chemotherapy. The IDEA study was a prospective, preplanned pooled analysis of these concurrently conducted studies to evaluate the noninferiority of adjuvant therapy of either FOLFOX or CAPOX administered for 3 months versus 6 months. Noninferiority could be claimed if the upper limit of the two-sided 95% CI of the HR did not exceed 1.12.[30]
From 2007 through 2015, 13,025 patients with stage III colon cancer were enrolled in six concurrent phase III trials. Of these patients, 12,834 patients met the criteria for intention-to-treat analysis. At a median follow-up of 41.8 months, noninferiority of 3 months versus 6 months was not confirmed in the modified intention-to-treat population (HR, 1.07; 95% CI, 1.00–1.15, P = .11 for noninferiority of 3 months).
The 3-year DFS rates were 74.6% in the 3-month group and 75.5% in the 6-month group.
Neurotoxicity of grade 2 or higher was lower in the 3-month group (16.6% for patients who received FOLFOX and 14.2% for patients who received CAPOX) than in the 6-month group (47.7% for patients who received FOLFOX and 44.9% for patients who received CAPOX). Moreover, all other toxicities were substantially lower with 3 months of treatment than with 6 months.
A subgroup analyses observed:
Among patients receiving FOLFOX, 6 months of therapy was superior to 3 months of therapy (HR, 1.16; 95% CI, 1.06–1.26; P = .001)
Among patients receiving CAPOX, 3 months of therapy was like 6 months of therapy (HRDFS, 0.95; 95% CI, 0.85–1.06) and met the prespecified margin for noninferiority.
Among patients with N1 tumors (<4 positive nodes), the HR was 1.07 (0.97–1.17), and among those patients with N2 tumors (≥4 positive nodes), the HR was 1.07 (0.96–1.19).
Among patients with T4 tumors, a therapy duration of 3 months was inferior to a duration of 6 months (HR, 1.16; 95% CI, 1.03–1.31).
Among patients with low-risk tumors (T1–3, N1), 3 months of therapy was noninferior to 6 months of therapy (HR, 1.01; 95% CI, 0.90–1.12) with a 3-year DFS rate of 83.1% for patients who received 3 months of therapy and 83.3% for patients who received 6 months of therapy.
Among patients with high-risk tumors (T4 or N2), 6 months of therapy was superior to 3 months of therapy (HR, 1.12; 95% CI, 1.03–1.23; P = .01).
The IDEA study has generated much debate regarding the optimal length of therapy. It is recommended that patients and doctors weigh the pros and cons of potential diminished efficacy of 3 months of therapy versus the definite increased risk of toxicity, particularly neuropathy. CAPOX appears to be slightly more active than FOLFOX in the adjuvant setting.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Rougier P, Nordlinger B: Large scale trial for adjuvant treatment in high risk resected colorectal cancers. Rationale to test the combination of loco-regional and systemic chemotherapy and to compare l-leucovorin + 5-FU to levamisole + 5-FU. Ann Oncol 4 (Suppl 2): 21-8, 1993. [PUBMED Abstract]
Bokey EL, Moore JW, Chapuis PH, et al.: Morbidity and mortality following laparoscopic-assisted right hemicolectomy for cancer. Dis Colon Rectum 39 (10 Suppl): S24-8, 1996. [PUBMED Abstract]
Franklin ME, Rosenthal D, Abrego-Medina D, et al.: Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum 39 (10 Suppl): S35-46, 1996. [PUBMED Abstract]
Fleshman JW, Nelson H, Peters WR, et al.: Early results of laparoscopic surgery for colorectal cancer. Retrospective analysis of 372 patients treated by Clinical Outcomes of Surgical Therapy (COST) Study Group. Dis Colon Rectum 39 (10 Suppl): S53-8, 1996. [PUBMED Abstract]
Schwenk W, Böhm B, Müller JM: Postoperative pain and fatigue after laparoscopic or conventional colorectal resections. A prospective randomized trial. Surg Endosc 12 (9): 1131-6, 1998. [PUBMED Abstract]
Weeks JC, Nelson H, Gelber S, et al.: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287 (3): 321-8, 2002. [PUBMED Abstract]
Panettiere FJ, Goodman PJ, Costanzi JJ, et al.: Adjuvant therapy in large bowel adenocarcinoma: long-term results of a Southwest Oncology Group Study. J Clin Oncol 6 (6): 947-54, 1988. [PUBMED Abstract]
Adjuvant therapy of colon cancer–results of a prospectively randomized trial. Gastrointestinal Tumor Study Group. N Engl J Med 310 (12): 737-43, 1984. [PUBMED Abstract]
Higgins GA, Amadeo JH, McElhinney J, et al.: Efficacy of prolonged intermittent therapy with combined 5-fluorouracil and methyl-CCNU following resection for carcinoma of the large bowel. A Veterans Administration Surgical Oncology Group report. Cancer 53 (1): 1-8, 1984. [PUBMED Abstract]
Buyse M, Zeleniuch-Jacquotte A, Chalmers TC: Adjuvant therapy of colorectal cancer. Why we still don’t know. JAMA 259 (24): 3571-8, 1988. [PUBMED Abstract]
Laurie JA, Moertel CG, Fleming TR, et al.: Surgical adjuvant therapy of large-bowel carcinoma: an evaluation of levamisole and the combination of levamisole and fluorouracil. The North Central Cancer Treatment Group and the Mayo Clinic. J Clin Oncol 7 (10): 1447-56, 1989. [PUBMED Abstract]
Moertel CG, Fleming TR, Macdonald JS, et al.: Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 322 (6): 352-8, 1990. [PUBMED Abstract]
Wolmark N, Rockette H, Fisher B, et al.: The benefit of leucovorin-modulated fluorouracil as postoperative adjuvant therapy for primary colon cancer: results from National Surgical Adjuvant Breast and Bowel Project protocol C-03. J Clin Oncol 11 (10): 1879-87, 1993. [PUBMED Abstract]
Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. International Multicentre Pooled Analysis of Colon Cancer Trials (IMPACT) investigators. Lancet 345 (8955): 939-44, 1995. [PUBMED Abstract]
O’Connell M, Mailliard J, Macdonald J, et al.: An intergroup trial of intensive course 5FU and low dose leucovorin as surgical adjuvant therapy for high risk colon cancer. [Abstract] Proceedings of the American Society of Clinical Oncology 12: A-552, 190, 1993.
Haller DG, Catalano PJ, Macdonald JS, et al.: Phase III study of fluorouracil, leucovorin, and levamisole in high-risk stage II and III colon cancer: final report of Intergroup 0089. J Clin Oncol 23 (34): 8671-8, 2005. [PUBMED Abstract]
Wolmark N, Bryant J, Smith R, et al.: Adjuvant 5-fluorouracil and leucovorin with or without interferon alfa-2a in colon carcinoma: National Surgical Adjuvant Breast and Bowel Project protocol C-05. J Natl Cancer Inst 90 (23): 1810-6, 1998. [PUBMED Abstract]
Wolmark N, Rockette H, Mamounas E, et al.: Clinical trial to assess the relative efficacy of fluorouracil and leucovorin, fluorouracil and levamisole, and fluorouracil, leucovorin, and levamisole in patients with Dukes’ B and C carcinoma of the colon: results from National Surgical Adjuvant Breast and Bowel Project C-04. J Clin Oncol 17 (11): 3553-9, 1999. [PUBMED Abstract]
Okuno SH, Woodhouse CL, Loprinzi CL, et al.: Phase III placebo-controlled clinical trial evaluation of glutamine for decreasing mucositis in patients receiving 5FU (fluorouracil)-base chemotherapy. [Abstract] Proceedings of the American Society of Clinical Oncology 17: A-256, 1998.
Andre T, Colin P, Louvet C, et al.: Semimonthly versus monthly regimen of fluorouracil and leucovorin administered for 24 or 36 weeks as adjuvant therapy in stage II and III colon cancer: results of a randomized trial. J Clin Oncol 21 (15): 2896-903, 2003. [PUBMED Abstract]
Comparison of flourouracil with additional levamisole, higher-dose folinic acid, or both, as adjuvant chemotherapy for colorectal cancer: a randomised trial. QUASAR Collaborative Group. Lancet 355 (9215): 1588-96, 2000. [PUBMED Abstract]
Sargent DJ, Goldberg RM, Jacobson SD, et al.: A pooled analysis of adjuvant chemotherapy for resected colon cancer in elderly patients. N Engl J Med 345 (15): 1091-7, 2001. [PUBMED Abstract]
Van Cutsem E, Twelves C, Cassidy J, et al.: Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol 19 (21): 4097-106, 2001. [PUBMED Abstract]
Hoff PM, Ansari R, Batist G, et al.: Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 19 (8): 2282-92, 2001. [PUBMED Abstract]
Twelves C, Wong A, Nowacki MP, et al.: Capecitabine as adjuvant treatment for stage III colon cancer. N Engl J Med 352 (26): 2696-704, 2005. [PUBMED Abstract]
André T, Boni C, Mounedji-Boudiaf L, et al.: Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 350 (23): 2343-51, 2004. [PUBMED Abstract]
André T, Boni C, Navarro M, et al.: Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 27 (19): 3109-16, 2009. [PUBMED Abstract]
Yothers G, O’Connell MJ, Allegra CJ, et al.: Oxaliplatin as adjuvant therapy for colon cancer: updated results of NSABP C-07 trial, including survival and subset analyses. J Clin Oncol 29 (28): 3768-74, 2011. [PUBMED Abstract]
Schmoll HJ, Tabernero J, Maroun J, et al.: Capecitabine Plus Oxaliplatin Compared With Fluorouracil/Folinic Acid As Adjuvant Therapy for Stage III Colon Cancer: Final Results of the NO16968 Randomized Controlled Phase III Trial. J Clin Oncol 33 (32): 3733-40, 2015. [PUBMED Abstract]
Grothey A, Sobrero AF, Shields AF, et al.: Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N Engl J Med 378 (13): 1177-1188, 2018. [PUBMED Abstract]
Treatment of Stage IV and Recurrent Colon Cancer
Stage IV colon cancer denotes distant metastatic disease. Treatment of recurrent colon cancer depends on the sites of recurrent disease demonstrable by physical examination and/or radiographic studies. In addition to standard radiographic procedures, radioimmunoscintography may add clinical information that may affect management.[1] Such approaches have not led to improvements in long-term outcome measures such as survival.
Treatment options for stage IV colon cancer, recurrent colon cancer, and liver metastases include:
Surgical resection of locally recurrent cancer.
Surgical resection and anastomosis or bypass of obstructing or bleeding primary lesions in selected metastatic cases.
Resection of liver metastases in selected metastatic patients (5-year cure rate for resection of solitary or combination metastases exceeds 20%) or ablation in selected patients.[2–11]
Resection of isolated pulmonary or ovarian metastases in selected patients.[12]
Palliative radiation therapy.
Palliative chemotherapy.
Targeted therapy.
Clinical trials comparing various new drugs, chemotherapy regimens, or biological therapies, alone or in combination.
Treatment Options for Liver Metastasis
Approximately 50% of colon cancer patients will be diagnosed with hepatic metastases, either at the time of initial presentation or because of disease recurrence. Although only a small proportion of patients with hepatic metastases are candidates for surgical resection, advances in tumor ablation techniques and in both regional and systemic chemotherapy administration provide for several treatment options. These include:
Hepatic metastasis may be considered to be resectable based on the following factors:[5,7,13–16]
Limited number of lesions.
Intrahepatic locations of lesions.
Lack of major vascular involvement.
Absent or limited extrahepatic disease.
Enough functional hepatic reserve.
For patients with resectable hepatic metastasis, a negative margin resection resulted in 5-year survival rates of 25% to 40% in mostly nonrandomized studies, such as the North Central Cancer Treatment Group trial (NCCTG-934653 [NCT00002575]).[5,7,13–16][Level of evidence C3] Improved surgical techniques and advances in preoperative imaging have improved patient selection for resection. In addition, multiple studies with multiagent chemotherapy have demonstrated that patients with metastatic disease isolated to the liver, which historically would be considered unresectable, can occasionally be made resectable after the administration of chemotherapy.[17]
For patients with unresectable liver metastases, excellent outcomes have been achieved with liver transplant. The optimal patient cohort for this therapy is still being determined, but in general, the goal is to achieve good initial systemic control with chemotherapy, followed by transplant. In one study of 91 patients, 11% underwent live donor liver transplant. At a median follow-up of 1.5 years after transplant, the recurrence-free survival rate was 62% and the overall survival (OS) rate was 100%.[18][Level of evidence C3]
In the TRANSMET study (NCT02597348), published in abstract form, 94 patients were randomly assigned to receive either chemotherapy and liver transplant (n = 47) or chemotherapy alone (n = 47). In an intent-to-treat analysis, the 5-year OS rate was 57% in the chemotherapy-and-liver transplant arm and 13% in the chemotherapy-alone arm. In a per-protocol analysis, the 5-year OS rate was 73% in the chemotherapy-and-liver transplant arm and 9% in the chemotherapy-alone arm.[19][Level of evidence A1]
Neoadjuvant chemotherapy for unresectable liver metastases
Patients with hepatic metastases that are deemed unresectable will occasionally become candidates for resection if they have a good response to chemotherapy. These patients have 5-year survival rates similar to patients who initially had resectable disease.[17] There is no consensus on the best regimen to use to convert unresectable isolated liver metastases to resectable liver metastases.
Local ablation
Radiofrequency ablation has emerged as a safe technique (2% major morbidity and <1% mortality rate) that may provide for long-term tumor control.[20–26] Radiofrequency ablation and cryosurgical ablation [27–30] remain options for patients with tumors that cannot be resected and for patients who are not candidates for liver resection.
Other local ablative techniques that have been used to manage liver metastases include embolization and interstitial radiation therapy.[31,32] Patients with limited pulmonary metastases, and patients with both pulmonary and hepatic metastases, may also be considered for surgical resection, with 5-year survival possible in highly-selected patients.[12,33,34]
Adjuvant or neoadjuvant chemotherapy for resectable liver metastases
The role of adjuvant chemotherapy after potentially curative resection of liver metastases is uncertain.
Evidence (adjuvant or neoadjuvant chemotherapy for resectable liver metastases):
In the era before the use of FOLFOX (leucovorin calcium [LV], fluorouracil [5-FU], and oxaliplatin) and FOLFIRI (5-FU/LV/irinotecan), two trials attempted to randomly assign patients after resection of liver metastases to 5-FU/LV or observation, but both studies were closed early because of poor accrual.
The FFCD-9902 trial (NCT00304135) randomly assigned 173 patients (200 patients were planned) to postoperative 5-FU/LV, which is the Mayo Clinic regimen, or observation.[35]
The 5-year disease-free survival (DFS) rate was 33.5% for patients in the chemotherapy group and 26.7% for patients in the control group (Cox multivariate analysis: odds ratio (OR) for recurrence or death, 0.66; 95% confidence interval [CI], 0.46–0.96; P = .028). The 5-year OS rate was not significantly different between the groups (chemotherapy group, 51.1% vs. the control group, 41.1%; ORdeath, 0.73; 95% CI, 0.48–1.10; P = .13).
The European Organisation for Research and Treatment of Cancer/National Cancer Institute of Canada/Gruppo Interdisciplinare Valutazione Interventi in Oncologia (EORTC/NCIC/GIVIO) International trial attempted a similar random assignment of patients after surgical resection of liver metastases. The study closed because of poor accrual, and a combined analysis of the study and the FFCD-9902 study was done instead. In the combined analysis, 278 patients (138 of whom received chemotherapy; 14 of whom received surgery alone) were included.[36]
The median progression-free survival (PFS) was 27.9 months in the chemotherapy arm and 18.8 months in the surgery alone arm (hazard ratio [HR], 1.32; 95% CI, 1.00–1.76; P = .058).
The median OS was 62.2 months in the chemotherapy arm compared with 47.3 months in the surgery-alone arm (HR, 1.32; 95% CI, 0.95–1.82; P = .095).
In the era of multiagent chemotherapy, two subsequent studies evaluated its role in the adjuvant setting following resection of liver metastases from colorectal cancer.
A phase III study randomly assigned 306 patients to 5-FU/LV or FOLFIRI after a resection of liver metastases.[37]
There was no difference in DFS (21.6 months for 5-FU/LV vs. 24.7 months for FOLFIRI; HR, 0.89; log-rank P = .44) or OS (HR, 1.09; 95% CI, 0.72–1.64).
The EORTC-40983 trial (NCT00006479) randomly assigned 364 patients with up to four resectable liver metastases to perioperative FOLFOX (six cycles presurgery and six cycles postsurgery) or surgery alone.[38]
The PFS rate was 28.1% (95.66% CI, 21.3%–35.5%) for the surgery-alone group and 35.4% (28.1%–42.7%; HR, 0.79; 0.62–1.02; P = .058) for the perioperative chemotherapy group. There was no difference in OS. Subsequent post hoc analysis demonstrated that the difference in PFS in truly eligible patients rose 8.1% (from 28.1% [21.2%–36.6%] to 36.2% [28.7%–43.8%]; HR, 0.77 [0.60–1.00]; P = .041). In patients who underwent resection of liver metastases, the difference in PFS rose 9.2% (from 33.2% [25.3%–41.2%] to 42.4% [34.0%–50.5%]; HR, 0.73 [0.55–0.97]; P = .025).
Reversible postoperative complications occurred more often after chemotherapy than after surgery (40 [25%] of the 159 complications vs. 27 [16%] of the 170 complications; P = .04). After surgery, there were two deaths in the surgery-alone group and one in the perioperative chemotherapy group.
There is no high-level evidence to demonstrate that perioperative or postoperative chemotherapy improves OS for patients undergoing resection of liver metastases. Nevertheless, on the basis of post hoc subset analyses of the EORTC study, some physicians feel perioperative or postoperative therapy is reasonable in this setting.
Intra-arterial chemotherapy after liver resection
Hepatic intra-arterial chemotherapy with floxuridine for liver metastases has produced higher overall response rates but no consistent improvement in survival when compared with systemic chemotherapy.[2,39–43] A meta-analysis of the randomized studies, which were all done in the era when only fluoropyrimidines were available for systemic therapy, did not demonstrate a survival advantage.[44]
Evidence (intra-arterial chemotherapy after liver resection):
Two trials evaluated hepatic arterial floxuridine in the adjuvant setting after liver resection.
A trial of hepatic arterial floxuridine and dexamethasone plus systemic 5-FU/LV compared with systemic 5-FU/LV alone showed improved 2-year PFS rates (57% vs. 42%, P = .07) and OS rates (86% vs. 72%, P = .03) for patients in the combined therapy arm but did not show a significant statistical difference in median survival compared with systemic 5-FU therapy alone.[45][Level of evidence A1]
The median survival in the combined therapy arm was 72.2 months versus 59.3 months in the monotherapy arm (P = .21).
A second trial preoperatively randomly assigned 109 patients who had one to three potentially resectable colorectal hepatic metastases to either no further therapy or postoperative hepatic arterial floxuridine plus systemic 5-FU.[46] Of those randomly assigned patients, 27% were deemed ineligible at the time of surgery, which left only 75 patients evaluable for recurrence and survival.
While liver cancer recurrence was decreased, median or 4-year survival was not significantly different between the patient groups.
Further studies are required to evaluate this treatment approach and to determine whether more effective systemic combination chemotherapy alone may provide similar results compared with hepatic intra-arterial therapy plus systemic treatment.
Several studies show increased local toxic effects with hepatic infusional therapy, including liver function abnormalities and fatal biliary sclerosis.
Treatment Options for Stage IV and Recurrent Colon Cancer
Treatment of patients with recurrent or advanced colon cancer depends on the location of the disease.
For patients with locally recurrent and/or liver-only and/or lung-only metastatic disease, surgical resection, if feasible, is the only potentially curative treatment.
Systemic therapy
The following drugs are used alone and in combination with other drugs for patients with metastatic colorectal cancer:
When 5-FU was the only active chemotherapy drug, trials in patients with locally advanced, unresectable, or metastatic disease demonstrated partial responses and prolongation of the time-to-progression (TTP) of disease,[47,48] and improved survival and quality of life for patients who received chemotherapy versus best supportive care.[49–51] Several trials have analyzed the activity and toxic effects of various 5-FU/LV regimens using different doses and administration schedules and showed essentially equivalent results with a median survival time in the 12-month range.[52]
Capecitabine
Before the advent of multiagent chemotherapy, two randomized studies demonstrated that capecitabine was associated with equivalent efficacy when compared with the Mayo Clinic regimen of 5-FU/LV.[53,54][Level of evidence A1]
Irinotecan
Three randomized studies demonstrated improved response rates, PFS, and OS when irinotecan or oxaliplatin was combined with 5-FU/LV.[55–57]
Evidence (irinotecan):
An intergroup study (NCCTG-N9741 [NCT00003594]) compared irinotecan/5-FU/LV (IFL) with oxaliplatin/LV/5-FU (FOLFOX-4) in first-line treatment for patients with metastatic colorectal cancer.
Patients assigned to FOLFOX-4 experienced an improved PFS (median, 6.9 months vs. 8.7 months; P = .014; HR, 0.74; 95% CI, 0.61–0.89) and OS (15.0 months vs. 19.5 months, P = .001; HR, 0.66; 95% CI, 0.54–0.82) compared with patients randomly assigned to IFL.
Subsequently, two studies compared FOLFOX with FOLFIRI, and patients were allowed to cross over upon progression on first-line therapy, respectively.[58,59][Level of evidence B1]
PFS and OS were identical between the treatment arms in both studies.
The Bolus, Infusional, or Capecitabine with Camptosar-Celecoxib (BICC-C [NCT00094965]) trial evaluated several different irinotecan-based regimens in patients with previously untreated metastatic colorectal cancer, including FOLFIRI, irinotecan plus bolus 5-FU/LV (mIFL), and capecitabine/irinotecan (CAPIRI).[60][Level of evidence A1]
The study randomly assigned 430 patients and was closed early because of poor accrual.
The patients who received FOLFIRI had a better PFS than the patients who received either mIFL (7.6 months vs. 5.9 months, P = .004) or CAPIRI (7.6 months vs. 5.8 months, P = .015).
Patients who received CAPIRI had the highest grade 3 or higher rates of nausea, vomiting, diarrhea, dehydration, and hand-foot syndrome.
Since the publication of these studies, the use of either FOLFOX or FOLFIRI is considered acceptable for first-line treatment of patients with metastatic colorectal cancer.
When using an irinotecan-based regimen as first-line treatment of metastatic colorectal cancer, FOLFIRI is preferred.[60][Level of evidence B1]
Oxaliplatin
Randomized phase III trials have addressed the equivalence of substituting capecitabine for infusional 5-FU. Two phase III studies have evaluated 5-FU/oxaliplatin (FUOX) versus capecitabine/oxaliplatin (CAPOX).[61,62]
Evidence (oxaliplatin):
The AIO Colorectal Study Group randomly assigned 474 patients to either 5-FU/LV/oxaliplatin (FUFOX) or CAPOX.
The median PFS was 7.1 months for the CAPOX arm and 8.0 months for the FUFOX arm (HR, 1.17; 95% CI, 0.96–1.43; P = .117), and the HR was in the prespecified equivalence range.
The Spanish Grupo de Tratamiento de los Tumores Digestivos randomly assigned 348 patients to CAPOX or FUOX.[61][Level of evidence B1]
The TTP was 8.9 months versus 9.5 months (P = .153) and met the prespecified range for noninferiority.
When using an oxaliplatin-based regimen as first-line treatment of metastatic colorectal cancer, a CAPOX regimen is not inferior to a FUOX regimen.
Before the availability of cetuximab, panitumumab, bevacizumab, and ziv-aflibercept as second-line therapy, second-line chemotherapy with irinotecan in patients treated with 5-FU/LV as first-line therapy demonstrated improved OS when compared with either infusional 5-FU or supportive care.[63–66]
Similarly, a phase III trial randomly assigned patients who progressed on irinotecan and 5-FU/LV to bolus and infusional 5-FU/LV (LV5FU2), single-agent oxaliplatin, or FOLFOX-4. The median TTP for FOLFOX-4 versus LV5FU2 was 4.6 months versus 2.7 months (stratified log-rank test, 2-sided P < .001).[67][Level of evidence B1]
Bevacizumab
Bevacizumab is a partially humanized monoclonal antibody that binds to VEGF. Bevacizumab can reasonably be added to either FOLFIRI or FOLFOX for patients undergoing first-line treatment of metastatic colorectal cancer.
Evidence (bevacizumab):
After bevacizumab was approved, the BICC-C trial was amended, and an additional 117 patients were randomly assigned to receive FOLFIRI/bevacizumab or mIFL/bevacizumab.
Although the primary end point of PFS was not significantly different, patients who received FOLFIRI/bevacizumab had a significantly better OS (not yet reached with a median follow-up of 22.6 months vs. 19.2 months, P = .007).
Patients with previously untreated metastatic colorectal cancer were randomly assigned to either IFL or IFL/bevacizumab.[68][Level of evidence A1]
The patients randomly assigned to IFL/bevacizumab experienced a significantly better PFS (10.6 months in the IFL/bevacizumab arm compared with 6.2 months in the IFL/placebo arm; HRdisease progression, 0.54; P < .001) and OS (20.3 months in the IFL/ bevacizumab arm compared with 15.6 months in the IFL/placebo arm; HRdeath , 0.66; P < .001).[68]
Despite the lack of direct data, in standard practice, bevacizumab was added to FOLFOX as a standard first-line regimen based on the results of the NCCTG-N9741 trial.[69] Subsequently, in a randomized phase III study, patients with untreated, stage IV, colorectal cancer were randomly assigned in a 2 × 2 factorial design to CAPOX versus FOLFOX-4, then to bevacizumab versus placebo. PFS was the primary end point.
In this trial, 1,401 patients were randomly assigned, and the median PFS was 9.4 months for patients who received bevacizumab and 8.0 months for the patients who received placebo (HR, 0.83; 97.5% CI, 0.72–0.95; P = .0023).[70][Level of evidence B1]
The median OS was 21.3 months for patients who received bevacizumab and 19.9 months for patients who received placebo (HR, 0.89; 97.5% CI, 0.76–1.03; P = .077).
The median PFS (intention-to-treat analysis) was 8.0 months in the pooled CAPOX-containing arms versus 8.5 months in the FOLFOX-4-containing arms (HR, 1.04; 97.5% CI, 0.93–1.16), with the upper limit of the 97.5% CI being below the predefined noninferiority margin of 1.23.[70,71]
The effect of bevacizumab on OS is likely to be less than what was seen in the original Hurwitz study.[68]
Investigators from the Eastern Cooperative Oncology Group randomly assigned patients who had progressed on 5-FU/leucovorin and irinotecan to either FOLFOX or FOLFOX /bevacizumab.
Patients randomly assigned to FOLFOX/bevacizumab experienced a statistically significant improvement in PFS (7.43 months vs. 4.7 months, HR, 0.61; P < .0001) and OS (12.9 months vs. 10.8 months, HR, 0.75; P = .0011).[72][Level of evidence A1]
Based on these studies, bevacizumab can reasonably be added to either FOLFIRI or FOLFOX for patients undergoing first-line treatment of metastatic colorectal cancer. A major question was whether the use of bevacizumab after first-line therapy was warranted when bevacizumab was used as a component of first-line therapy. At the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting, data were presented from a randomized, controlled trial.[73] In the trial, 820 patients with metastatic colorectal cancer, after progressing on first-line chemotherapy that included bevacizumab, were randomly assigned to chemotherapy without bevacizumab or chemotherapy with bevacizumab. Patients who received bevacizumab experienced an improved OS compared with the patients who did not receive bevacizumab. The median OS was 11.2 months for patients who received bevacizumab/chemotherapy and 9.8 months for patients who received chemotherapy without bevacizumab (HR, 0.81; 95% CI, 0.69–0.94; unstratified log-rank test, P = .0062). The median PFS was 5.7 months for patients who received bevacizumab/chemotherapy and 4.1 months for those who received chemotherapy without bevacizumab (HR, 0.68; 95% CI, 0.59–0.78; unstratified log-rank test, P < .0001).[73][Level of evidence A1]
FOLFOXIRI
Evidence (FOLFOXIRI):
The combination of FOLFOXIRI with bevacizumab was compared with FOLFIRI with bevacizumab in a randomized, phase III study of 508 patients with untreated metastatic colorectal cancer.[74][Level of evidence B1]
The median PFS was 12.1 months in the FOLFOXIRI group, compared with 9.7 months in the FOLFIRI group (HRprogression, 0.75; 95% CI, 0.62–0.90; P = .003). OS was not significantly different between the groups (31.0 vs. 25.8 months; HRdeath, 0.79; 95% CI, 0.63–1.00; P = .054).
Patients who received FOLFOXIRI had significantly more grade 3 and 4 toxicities, including neutropenia, stomatitis, and peripheral neuropathy.
Cetuximab
Cetuximab is a partially humanized monoclonal antibody against EGFR. Because cetuximab affects tyrosine kinase signaling at the surface of the cell membrane, tumors with activating variants of the pathway downstream of the EGFR, such as KRAS variants, are not sensitive to its effects. The addition of cetuximab to multiagent chemotherapy improves survival in patients with colon cancers that lack a KRAS variant (i.e., KRAS wild type). Importantly, patients with KRAS-altered tumors may experience worse outcome when cetuximab is added to multiagent chemotherapy regimens containing bevacizumab.
Evidence (cetuximab):
For patients who had disease progression while receiving irinotecan-containing regimens, a randomized phase II study was performed using either cetuximab or irinotecan and cetuximab.[75][Level of evidence C3]
The median TTP for patients who received cetuximab was 1.5 months, compared with the median TTP of 4.2 months for patients who received irinotecan/cetuximab.[75][Level of evidence B1]
Based on this study, cetuximab was approved for use in patients with metastatic colorectal cancer refractory to 5-FU and irinotecan.
The Crystal Study (EMR 62202-013 [NCT00154102]) randomly assigned 1,198 patients with stage IV colorectal cancer to FOLFIRI with or without cetuximab.[76][Level of evidence B1]
The addition of cetuximab was associated with an improved PFS (HR, 0.85; 95% CI, 0.72–0.99; stratified log-rank P = .048) but not OS.
Retrospective studies of patients with metastatic colorectal cancer have suggested that responses to anti-EGFR antibody therapy are confined to patients with tumors that harbor wild types of KRAS (i.e., lack activating variants at codon 12 or 13 of the KRAS gene).
A subset analysis evaluating efficacy in relation to KRAS status was done in patients enrolled in the Crystal Study. There was a significant interaction for KRAS variant status and treatment for tumor response (P = .03) but not for PFS (P = .07). Among patients with KRAS wild-type tumors, the HR favored the FOLFIRI/cetuximab group (HR, 0.68; 95% CI, 0.50–0.94).
In a randomized trial, patients with metastatic colorectal cancer received capecitabine/oxaliplatin/bevacizumab with or without cetuximab.[77][Level of evidence B1]
The median PFS was 9.4 months in the group who received cetuximab and 10.7 months in the group who did not receive cetuximab (P = .01).
In a subset analysis, patients with tumors with KRAS variants who received cetuximab had significantly decreased PFS compared with patients with wild-type KRAS tumors who received cetuximab (8.1 months vs. 10.5 months; P = .04).
Among patients with KRAS-altered tumors, PFS was significantly shorter in those who received cetuximab than those did not receive cetuximab (8.1 months vs. 12.5 months; P = .003). OS was also significantly shorter (17.2 months vs. 24.9 months, respectively; P = .03).
The Medical Research Council (MRC) COIN trial (NCT00182715) sought to determine if adding cetuximab to combination chemotherapy with a fluoropyrimidine and oxaliplatin in first-line treatment for patients with KRAS wild-type tumors was beneficial.[78,79] In addition, the MRC sought to evaluate the effect of intermittent chemotherapy versus continuous chemotherapy. The 1,630 patients were randomly assigned to three treatment groups:
Arm A: fluoropyrimidine/oxaliplatin.
Arm B: fluoropyrimidine/oxaliplatin/cetuximab.
Arm C: intermittent fluoropyrimidine/oxaliplatin.
The comparisons between arms A and B and arms A and C were analyzed and published separately.[78,79]
In patients with KRAS wild-type tumors (arm A, n = 367; arm B, n = 362), OS did not differ between treatment groups (median survival, 17.9 months [interquartile range (IQR) 10.3–29.2] in the control group vs. 17.0 months [IQR, 9.4–30.1] in the cetuximab group; HR, 1.04; 95% CI, 0.87–1.23; P = .67). Similarly, there was no effect on PFS (8.6 months [IQR, 5.0–12.5] in the control group versus 8.6 months [IQR, 5.1–13.8] in the cetuximab group; HR, 0.96; 95% CI, 0.82–1.12; P = .60).[78,79][Level of evidence A1]
The reasons for lack of benefit in adding cetuximab are unclear. Subset analyses suggest that the use of capecitabine was associated with an inferior outcome, and the use of second-line therapy was less frequent in patients treated with cetuximab.
There was no difference between the continuously treated patients (arm A) and the intermittently treated patients (arm C). Median survival in the intent-to-treat population (n = 815 in both groups) was 15.8 months (IQR, 9.4–26.1) in arm A and 14.4 months (IQR, 8.0–24.7) in arm C (HR, 1.084; 80% CI, 1.008–1.165). In the per-protocol population, which included only those patients who were free from progression at 12 weeks and randomly assigned to continue treatment or go on a chemotherapy holiday (arm A, n = 467; arm C, n = 511), median survival was 19.6 months (IQR, 13.0–28.1) in arm A and 18.0 months (IQR, 12.1–29.3) in arm C (HR, 1.087; 95% CI, 0.986–1.198).
The upper limits of CIs for HRs in both analyses were greater than the predefined noninferiority boundary. While intermittent chemotherapy was not deemed noninferior, there appeared to be clinically insignificant differences in patient outcomes.
The OPUS study sought to evaluate the effect of adding cetuximab to first-line treatment with a FOLFOX regimen in an open-label, randomized, multicenter, phase II study of patients with EGFR-expressing metastatic colorectal cancer.[80]
In the trial, 344 patients were randomly assigned to receive FOLFOX-4 alone or FOLFOX-4/cetuximab. There was no statistically significant difference in response rate or PFS.
On subset analysis, patients with KRAS wild-type tumors were analyzed separately. In the KRAS wild-type tumor population, there was a statistically significant improvement in response rate (61% vs. 37%, P = .011) and PFS (7.7 months vs. 7.2 months, P = .0163).
On subset analysis among patients with KRAS-altered tumors, those who received FOLFOX-4/cetuximab had a statistically significant worse PFS than patients who received FOLFOX-4 alone (5.5 months vs. 8.6 months; P = .0192).[80][Level of evidence B1]
Ziv-aflibercept
Ziv-aflibercept is an anti-VEGF molecule and has been evaluated as a component of second-line therapy in patients with metastatic colorectal cancer.
Evidence (ziv-aflibercept):
In one trial, 1,226 patients were randomly assigned to receive ziv-aflibercept (4 mg/kg intravenously [IV]) or placebo every 2 weeks in combination with FOLFIRI.[81][Level of evidence A2]
Patients who received ziv-aflibercept/FOLFIRI had significantly improved OS rates, with median survival times of 13.50 months compared with patients who received placebo/FOLFIRI, with median survival times of 12.06 months (HR, 0.817; 95.34% CI, 0.713–0.937; P = .0032).
Patients who received ziv-aflibercept/FOLFIRI also had significantly improved PFS rates, with median PFS rates of 6.90 months compared with patients who received placebo/FOLFIRI, with median PFS rates of 4.67 months (HR, 0.758; 95% CI, 0.661–0.869; P < .0001).
Based on these results, the use of ziv-aflibercept/FOLFIRI is an acceptable second-line regimen for patients previously treated with FOLFOX-based chemotherapy. Whether to continue bevacizumab or initiate ziv-aflibercept in second-line therapy has not been addressed yet in any clinical trial, and there are no data available.
Ramucirumab
Ramucirumab is a fully humanized monoclonal antibody that binds to vascular endothelial growth factor receptor-2.
Evidence (ramucirumab):
In the randomized, unblinded, phase III RAISE study (NCT01183780), 1,072 patients with stage IV colorectal cancer who had progressed on first-line chemotherapy were randomly assigned to FOLFIRI with or without ramucirumab (8 mg/kg).[82][Level of evidence A1]
Patients assigned to FOLFIRI/ramucirumab had a significant improvement in median OS (13.3 months vs. 11.7 months; HR, 0.84; P = .0219) and PFS (5.7 months vs. 4.5 months; HR, 0.793; P = .0005).
Grade 3 adverse events were more common in the ramucirumab group, including grade 3 neutropenia.
Based on these data, FOLFIRI/ramucirumab is an acceptable second-line regimen for patients previously treated with FOLFOX/bevacizumab. Whether to continue bevacizumab in second-line chemotherapy or use ramucirumab in second-line chemotherapy has not yet been addressed in a clinical trial.
Panitumumab
Panitumumab is a fully humanized antibody against the EGFR. The U.S. Food and Drug Administration (FDA) approved panitumumab for patients with metastatic colorectal cancer refractory to chemotherapy.[83] In clinical trials, panitumumab demonstrated efficacy as a single agent or in combination therapy, which was consistent with the effects on PFS and OS with cetuximab. There appears to be a consistent class effect.
Evidence (panitumumab):
In a phase III trial, patients with chemotherapy-refractory colorectal cancer were randomly assigned to panitumumab or best supportive care.[83][Level of evidence B1]
Patients who received panitumumab experienced an improved PFS (8 weeks vs. 7.3 weeks; HR, 0.54; 95% CI, 0.44–0.66; P < .0001).
There was no difference in OS, which was thought to be the result of 76% of patients on best supportive care crossing over to panitumumab.
In the Panitumumab Randomized Trial in Combination With Chemotherapy for Metastatic Colorectal Cancer to Determine Efficacy (PRIME) study [NCT00364013], 1,183 patients were randomly assigned to FOLFOX-4 with or without panitumumab as first-line therapy for metastatic colorectal cancer. The study was amended to enlarge the sample size to address patients with the KRAS wild-type tumors and patients with KRAS-altered tumors separately.[84][Level of evidence B1]
For patients with KRAS wild-type tumors, a statistically significant improvement in PFS was observed in those who received panitumumab/FOLFOX-4 compared with those who received only FOLFOX-4 (HR, 0.80; 95% CI, 0.66–0.97; stratified log-rank P = .02).
The median PFS was 9.6 months (95% CI, 9.2–11.1) for patients who received panitumumab/FOLFOX-4 and 8.0 months (95% CI, 7.5–9.3) for patients who received FOLFOX-4. OS was not significantly different between the groups (HR, 0.83; 95% CI, 0.67–1.02; P = .072).
For patients with KRAS-altered tumors, there was worse PFS with the addition of panitumumab (HR, 1.29; 95% CI, 1.04–1.62; stratified log-rank P = .02).
The median PFS was 7.3 months (95% CI, 6.3–8.0) for panitumumab/FOLFOX-4 and 8.8 months (95% CI, 7.7–9.4) for FOLFOX-4 alone.
Subsequently, a retrospective analysis evaluated patients with wild-type KRAS exon 2 status for other KRAS and BRAF variants.[85][Level of evidence C1]
Of the 620 patients who were initially identified as not having a variant in exon 2 of KRAS, 108 patients (17%) were found to have additional RAS variants and 53 patients (8%) were found to have BRAF variants. In a retrospective analysis, patients without any RAS or BRAF variants had a longer PFS (10.8 months vs. 9.2 months, P = .002) and OS (28.3 months vs. 20.9 months, P = .02) when assigned to the FOLFOX-4/panitumumab arm than the patients assigned to the FOLFOX-4 arm.
Similarly, the addition of panitumumab to a regimen of FOLFOX/bevacizumab resulted in a worse PFS and worse toxicity compared with a regimen of FOLFOX/bevacizumab alone in patients not selected for KRAS variant in metastatic colon cancer (11.4 months vs. 10.0 months, HR, 1.27; 95% CI, 1.06–1.52).[86][Level of evidence B1]
In another study (NCT00339183), patients with metastatic colorectal cancer who had already received a fluoropyrimidine regimen were randomly assigned to either FOLFIRI or FOLFIRI/panitumumab.[87][Level of evidence B1]
In a post hoc analysis, patients with KRAS wild-type tumors experienced a statistically significant PFS advantage (HR, 0.73; 95% CI, 0.59–0.90; stratified log-rank P = .004).
The median PFS was 5.9 months (95% CI, 5.5–6.7) for panitumumab/FOLFIRI and 3.9 months (95% CI, 3.7–5.3) for FOLFIRI alone.
OS was not significantly different. Patients with KRAS-altered tumors experienced no benefit from the addition of panitumumab.
Anti-EGFR antibody versus anti-VEGF antibody with first-line chemotherapy
In the management of patients with stage IV colorectal cancer, it is unknown whether patients with KRAS wild-type cancer should receive an anti-EGFR antibody with chemotherapy or an anti-VEGF antibody with chemotherapy. Two studies attempted to answer this question.[88,89]
Evidence (anti-EGFR antibody vs. anti-VEGF antibody with first-line chemotherapy)
The FIRE-3 study (NCT00433927) randomly assigned 592 patients with KRAS exon 2 wild-type tumors who were previously untreated to FOLFIRI/cetuximab (297 patients) or FOLFIRI/bevacizumab (295 patients). The primary end point of the study was objective response rate.[88][Level of evidence A1]
The objective response rate was not significantly different between the groups (objective response rate, 62.0%; 95% CI, 56.2%–67.5% vs. objective response rate, 58.0%; 95% CI, 52.1%–63.7%; OR, 1.18; 95% CI, 0.85–1.64; P = .18).
The median PFS was 10.0 months (95% CI, 8.8–10.8) in the cetuximab group and 10.3 months (95% CI, 9.8–11.3) in the bevacizumab group (HR, 1.06; 95% CI, 0.88–1.26; P = .55).
The median OS was 28.7 months (95% CI, 24.0–36.6) in the cetuximab group compared with 25.0 months (22.7–27.6) in the bevacizumab group (HR, 0.77; 95% CI, 0.62–0.96; P = .017).
In a post hoc analysis of patients with expanded RAS wild-type tumors (sequencing for mutational hot spots within KRAS and NRAS genes, including exon 2 codons 12 and 13; exon 3 codons 59 and 61; and exon 4 codons 117 and 146), the median OS was 33.1 months (95% CI, 24.5–39.4) in the cetuximab group compared with 25.0 months (95% CI, 23.0–28.1) in the bevacizumab group (HR, 0.70; 95% CI, 0.54–0.90; P = .0059).[90]
Of note, only 52% of patients assigned to the bevacizumab arm subsequently received cetuximab or panitumumab.[91]
The Cancer and Leukemia Group B Intergroup study 80405 (NCT00265850) was presented at the ASCO meeting in 2014. This study randomly assigned 2,334 previously untreated patients with KRAS wild-type cancer to chemotherapy (FOLFOX or FOLFIRI) plus bevacizumab or chemotherapy/cetuximab. OS was the primary end point.[89][Level of evidence B1]
There was no statistically significant difference in OS among the patients assigned to bevacizumab or cetuximab (for OS differences, chemotherapy/bevacizumab = 29.04 [25.66–31.21] months vs. chemotherapy/cetuximab = 29.93 [27.56–31.21] months; HR, 0.92 [0.78–1.09]; P = .34).
Based on these two studies, no apparent significant difference is evident about starting treatment with chemotherapy/bevacizumab or chemotherapy/cetuximab in patients with KRAS wild-type metastatic colorectal cancer. However, in patients with KRAS wild-type cancer, administration of an anti-EGFR antibody during management improves OS.
Trifluridine-tipiracil
Trifluridine-tipiracil (Lonsurf; also called TAS-102) is an orally administered combination of a thymidine-based nucleic acid analogue, trifluridine, and a thymidine phosphorylase inhibitor, tipiracil hydrochloride. Trifluridine, in its triphosphate form, inhibits thymidylate synthase; therefore, trifluridine, in this form, has an antitumor effect. Tipiracil hydrochloride is a potent inhibitor of thymidine phosphorylase, which actively degrades trifluridine. The combination of trifluridine and tipiracil allows for adequate plasma levels of trifluridine.
Evidence (trifluridine-tipiracil):
A phase III, double-blind study (RECOURSE [NCT01607957]) randomly assigned 800 stage IV colorectal cancer patients whose cancer had been refractory to two previous therapies. Patients were required to have received 5-FU, oxaliplatin, irinotecan, bevacizumab and, if the patients had KRAS wild-type cancer, cetuximab or panitumumab. Patients were randomly assigned in a 2:1 ratio to receive best supportive care plus trifluridine-tipiracil (n = 534) or placebo (n = 266). The median age of patients was 63 years, and most patients (60%–63%) received four or more previous lines of therapy. All patients had formerly received fluoropyrimidine, irinotecan, oxaliplatin, and bevacizumab, and 52% of them had received an EGFR inhibitor. Approximately 20% of the patients had received previous treatment with regorafenib.[92][Level of evidence A1]
Trifluridine-tipiracil was administered at 35 mg/m2 twice daily with meals for 5 days, with 2 days of rest for 2 weeks, followed by a 14-day rest period.
The primary end point of the study was OS. The median OS for patients with metastatic colorectal cancer who received trifluridine-tipiracil was 7.1 months compared with 5.3 months for those who received a placebo (HR, 0.68; P < .0001).
The median PFS time in the trifluridine-tipiracil arm was 2 months versus 1.7 months with a placebo (HR, 0.48; P < .0001).
Secondary end points focused on PFS, overall response rate, and disease control rate.
The overall response rate was 1.6% with trifluridine-tipiracil, which consisted of a complete response in one patient and partial responses in other patients. The overall response rate with a placebo was 0.4% (P = .29).
The FDA approved trifluridine-tipiracil for the treatment of patients with metastatic colorectal cancer, based on the results of the RECOURSE trial.
Evidence (combination of trifluridine-tipiracil and bevacizumab):
A phase III, international, multi-institutional trial (SUNLIGHT [NCT04737187]) included 492 patients with stage IV colorectal cancer whose cancer was refractory to up to two prior chemotherapy regimens. Patients were required to have received 5-FU, oxaliplatin, irinotecan, an anti-VEGF monoclonal antibody, or an anti-EGFR monoclonal antibody (for patients with RAS wild-type disease). Patients were randomly assigned 1:1 to receive either trifluridine-tipiracil monotherapy (n = 246) or trifluridine-tipiracil combined with bevacizumab (n = 246). The median patient age was 62 years for the combination arm, and 64 years for the monotherapy arm and most patients (93% and 91%) had received two prior lines of therapy. Over 98% of patients in both arms had received 5-FU, irinotecan, and oxaliplatin, and over 93% of patients with RAS wild-type variants in both arms had received anti-EGFR monoclonal antibody therapy. The median follow-up was 14.2 months. Trifluridine-tipiracil was given at 35 mg/m2 twice daily on days 1 to 5 and 8 to 12 of a 28-day cycle. Bevacizumab was given on days 1 and 15 of each cycle at 5 mg/kg. The primary end point of the study was OS.[93]
The median OS was 10.8 months for patients who received trifluridine-tipiracil and bevacizumab and 7.5 months for patients who received trifluridine-tipiracil monotherapy (HR, 0.61; 95% CI, 0.49–0.77; P < .001).[93][Level of evidence A1]
OS was significant across subgroups, including patients with RAS variants and wild-type variants, patients with microsatellite instability-high (MSI-H) and microsatellite stability (MSS) cancers, and both for patients previously treated with bevacizumab and bevacizumab-naïve patients.
The median PFS was 5.6 months in the combination arm and 2.4 months in the trifluridine-tipiracil monotherapy arm (HR, 0.44; 95% CI, 0.36–0.54; P < .001).
Secondary end points focused on PFS, overall response rate, and safety.
The overall response rate was 6.1% for the combination arm and 1.2% for the monotherapy arm.
Adverse events leading to therapy discontinuation were observed in 12.6% of patients in both arms. Dose reductions occurred in 16.3% of patients in the combination group and 12.2% of patients in the trifluridine-tipiracil monotherapy group. The most common adverse event was neutropenia, with grade 3 or 4 neutropenia observed in 43% of patients in the combination arm and 32% of patients in the monotherapy arm.
The FDA approved the combination of trifluridine-tipiracil and bevacizumab for the treatment of patients with previously treated metastatic colorectal cancer based on the results of the SUNLIGHT trial.
Regorafenib
Regorafenib is an inhibitor of multiple tyrosine kinase pathways, including VEGF. In 2012, the FDA approved regorafenib for patients who had progressed on previous therapy.
Evidence (regorafenib):
The safety and effectiveness of regorafenib were evaluated in a single, clinical study of 760 patients with previously treated metastatic colorectal cancer. Patients were randomly assigned 2:1 to receive regorafenib or a placebo in addition to the best supportive care.[94,95]
Patients treated with regorafenib had a statistically significant improvement in OS (6.4 months in the regorafenib group vs. 5.0 months in the placebo group; HR, 0.77; 95% CI, 0.64–0.94; one-sided P = .0052).
With the improved OS from the combination of trifluridine-tipiracil and bevacizumab discussed above, regorafenib is now often considered a fourth-line or later option for treatment of patients with metastatic colorectal cancer.
Fruquintinib
Fruquintinib is an inhibitor of VEGF receptors 1, 2 and 3. In 2023, the FDA approved fruquintinib for adults with metastatic colorectal cancer who had previously received fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy and an anti-VEGF therapy. If patients had RAS wild-type disease and were medically appropriate, an anti-EGFR therapy was also required.
Evidence (fruquintinib):
The phase III, international, double-blind, placebo-controlled FRESCO-2 trial (NCT04322539) included 691 patients with metastatic colorectal adenocarcinoma who had received all standard approved cytotoxic and targeted therapies. Patients had disease progression during, or were intolerant of, trifluridine-tipiracil, regorafenib, or both. Patients had received a median of four lines of prior systemic therapy. Patients were randomly assigned in a 2:1 fashion to receive one of the following regimens:
Fruquintinib (5 mg orally once daily on days 1–21 of a 28-day cycle).
Placebo (orally once daily on days 1–21 of a 28-day cycle).
All patients received best supportive care. A total of 461 patients received fruquintinib, and 230 received placebo. The primary end point was OS.[96] The results were as follows:
The median OS was significantly longer in the fruquintinib group (7.4 months; 95% CI, 6.7–8.2) than in the placebo group (4.8 months; 95% CI, 4.0–5.8) (HR, 0.66; 95% CI, 0.55–0.80; P < .0001).[96][Level of evidence A1]
The median PFS was 3.7 months (95% CI, 3.5–3.8) in the fruquintinib group and 1.8 months (95% CI, 1.8–1.9) in the placebo group (HR, 0.26; 95% CI, 0.21–0.34; P < .001).
Subgroup analyses demonstrated the benefit of fruquintinib as opposed to placebo in most subgroups. Notably, this benefit was seen in patients with both RAS variants and RAS wild-type disease, patients with liver metastases, and patients pretreated with trifluridine-tipiracil with or without regorafenib.
The disease control rate was significantly longer in the fruquintinib group (56%) than in the placebo group (16%), with an adjusted difference of 39% (95% CI, 32.8%–46.0%; P < .0001).
Grade 3 or higher adverse events occurred in 65% of patients in the fruquintinib group. The most common adverse events were hypertension (14%), asthenia (8%), abnormal hepatic function (8%), dermatologic toxicity (7%), and hand-foot syndrome (6%). Grade 3 or higher adverse events occurred in 50% of patients in the placebo group. The most common were abnormal hepatic function (9%), infection (6%), and asthenia (4%).
Encorafenib with cetuximab in patients with BRAF V600E variants
BRAF V600E variants occur in about 10% of metastatic colorectal cancers and are an indicator of poor prognosis. Unlike in melanoma, BRAF inhibitor monotherapy has not shown a benefit in colorectal cancer, and multiple studies have evaluated concurrent targeting of the EGFR-MAPK pathway.
Evidence (encorafenib with cetuximab in patients with BRAF V600E variants):
Encorafenib (BRAF inhibitor), binimetinib (MEK inhibitor), and cetuximab (EGFR inhibitor): In the international, open-label, randomized, phase III BEACON trial, patients with metastatic colorectal cancer and BRAF V600E variants who previously received one or two treatment regimens were enrolled.[97] The trial randomly assigned 665 patients in a 1:1:1 ratio to receive one of the following:
Triplet therapy: encorafenib (300 mg PO daily), binimetinib (45 mg PO twice daily), and cetuximab (400 mg/m2 IV loading dose followed by 250 mg/m2 IV weekly) (n = 224).
Doublet therapy: encorafenib and cetuximab (as per triplet therapy dosing) (n = 220).
Control group: FOLFIRI or irinotecan (every 2 weeks) with cetuximab (400 mg/m2 IV loading dose followed by 250 mg/m2 IV weekly) (n = 221).
The primary end points were OS and objective response in the triplet-therapy group when compared with the control group.
The OS was 9.0 months in the triplet-therapy arm and 5.4 months in the control group (HR, 0.52; 95% CI, 0.39–0.70, P < .0001).[97][Level of evidence A1]
Grade 3 or higher side effects occurred in 58% of patients in the triplet-therapy arm, with 10% of patients experiencing diarrhea and 11% of patients experiencing anemia. Grade 3 or higher side effects occurred in 50% of patients in the doublet-therapy arm and 61% of patients in the control arm. Fourteen percent of patients who received the doublet regimen developed melanocytic nevi.
Updated data were presented in abstract form in 2020:[98]
The median OS was 9.3 months in both the triplet-therapy and doublet-therapy arms and 5.9 months in the control arm (HR, 0.60 for triplet therapy vs. control; 95% CI, 0.47–0.75; HR, 0.61 for doublet therapy vs. control; 95% CI, 0.48–0.77).
The objective response rate was 26.8% for patients who received triplet therapy (95% CI, 21.1%–33.1%) and 19.5% for patients who received doublet therapy (95% CI, 14.5%–25.4%).
Based on these data, the FDA approved the combination of encorafenib with cetuximab for patients with previously treated metastatic colon cancer and BRAF V600E variants.
Sotorasib with panitumumab for patients with KRAS G12C variants
KRAS G12C variants are found in approximately 4% of patients with colorectal cancer and are associated with poor prognosis.[99–102] Sotorasib and adagrasib are two of the first KRAS G12C–specific inhibitors to show benefit in patients with KRAS G12C–altered cancers.[103,104] Given that EGFR reactivation is a well-described resistance mechanism to KRAS G12C inhibition, sotorasib was combined with the anti-EGFR antibody panitumumab in patients with colorectal cancer and KRAS G12C variants.
The phase III, multicenter, open-label CodeBreaK 300 trial (NCT05198934) included patients with metastatic colorectal cancer and KRAS G12C variants who previously received treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.[103] The trial randomly assigned 160 patients 1:1:1 to receive one of the following:
Doublet therapy with sotorasib 960 mg once daily plus panitumumab (6 mg/kg IV every 2 weeks) (n = 53).
Doublet therapy with sotorasib 240 mg once daily plus panitumumab (6 mg/kg IV every 2 weeks) (n = 53).
Investigator’s choice standard-of-care therapy with trifluridine-tipiracil (35 mg/m2) or regorafenib (160 mg once daily) (control group).
The primary end point was PFS assessed by blinded independent central review according to RECIST 1.1. Secondary end points included OS and objective response rate.
The median PFS was 5.6 months (95% CI, 4.2–6.3) in the 960 mg-sotorasib/panitumumab group, 3.9 months (95% CI, 3.7–5.8) in the 240 mg-sotorasib/panitumumab group, and 2.2 months (95% CI, 1.9–3.9) in the standard-of-care group.[103][Level of evidence B1]
The HR for progression of disease or death was 0.49 (95% CI, 0.3–0.8; P = .006) for the 960 mg-sotorasib/panitumumab group and 0.58 (95% CI, 0.36–0.98; P = .03) for the 240 mg-sotorasib/panitumumab group.
The objective response rate was 26.4% (95% CI, 15.3%–40.3%) in the 960 mg-sotorasib/panitumumab group, 5.7% (95% CI, 1.2%–15.7%) in the 240 mg-sotorasib/panitumumab group, and 0% (95% CI, 0.0%–6.6%) in the standard-of-care group. OS data are still not mature. However, at data cutoff the HRs were 0.77 (95% CI, 0.4–1.45) for the 960 mg-sotorasib/panitumumab group and 0.91 (95% CI, 0.48–1.71) for the 240 mg-sotorasib/panitumumab group when compared with standard-of-care therapy.
Grade 3 or higher side effects occurred in 35.8% of patients who received 960 mg sotorasib/panitumumab, 30.2% of patients who received 240 mg sotorasib/panitumumab, and 43.1% of patients who received the standard of care. The most common adverse effects with combined sotorasib and panitumumab therapy were skin-related toxicities and hypomagnesemia.
Immunotherapy
Approximately 4% of patients with stage IV colorectal cancer have tumors that are mismatch repair deficient (dMMR) or microsatellite unstable/MSI-H. The MSI-H phenotype is associated with germline defects in the MLH1, MSH2, MSH6, and PMS2 genes and is the primary phenotype observed in tumors from patients with hereditary nonpolyposis colorectal cancer (HNPCC) or Lynch syndrome. Patients can also have the MSI-H phenotype because one of these genes was silenced via DNA methylation. Testing for microsatellite instability can be done with molecular genetic tests, which look for microsatellite instability in the tumor tissue, or with immunohistochemistry, which looks for the loss of mismatch repair proteins. MSI-H status has historically been prognostic of increased survival for patients with earlier-stage disease and since 2015, has also been found to predict tumor response to checkpoint inhibition.
The FDA approved pembrolizumab for patients with treatment-naïve, metastatic, dMMR/MSI-H colorectal cancer in 2020. Studies regarding first-line treatment with dual checkpoint inhibitors are ongoing. The FDA approved the anti-programmed cell death protein 1 (PD-1) antibodies pembrolizumab and nivolumab in 2017 for patients with microsatellite-unstable tumors who had previously received 5-FU, oxaliplatin, and irinotecan-based therapy. In 2018, the FDA granted accelerated approval for the combination of nivolumab with ipilimumab (a CTLA-4 inhibitor) to treat MSI-H colorectal cancers that progressed on prior 5-FU, oxaliplatin, and irinotecan-based therapies.
First-line immunotherapy
Pembrolizumab monotherapy
Evidence (pembrolizumab monotherapy):
In the phase III, open-label, international, randomized KEYNOTE-177 trial (NCT02563002), 307 patients with treatment-naïve MSI-H or dMMR metastatic colorectal cancer were randomly assigned in a 1:1 ratio to receive either pembrolizumab (200 mg every 3 weeks) or chemotherapy (FOLFIRI or modified FOLFOX-6 with or without bevacizumab or cetuximab).[105]
The median PFS was 16.5 months for patients who received pembrolizumab and 8.2 months for patients who received chemotherapy (HR, 0.60; 95% CI, 0.45–0.80; P = .0002).[105][Level of evidence A3]
The PFS in prespecified subgroups showed HRs that favored the pembrolizumab arm, except in patients with KRAS/NRAS variants.
The objective response rate was 43.8% in the pembrolizumab arm and 33.3% in the chemotherapy arm. The median duration of response was not reached in the pembrolizumab arm (range, 2.3–41.4 months) and was 10.6 months in the chemotherapy arm (range, 2.8–37.5 months).
Grade 3 or higher adverse events occurred in 56% of patients who received pembrolizumab (with 9% experiencing grade 3 or higher infusion-related adverse events), compared with 78% of patients who received chemotherapy.
A final review of OS, presented in abstract form, showed that median OS was not reached in the pembrolizumab arm and was 36.7 months in the chemotherapy arm (HR, 0.74; 95% CI, 0.53–1.03; P = .0359).[106]
Nivolumab and ipilimumab
Evidence (nivolumab and ipilimumab):
In a single-arm cohort of the phase II, multicenter CheckMate-142 study (NCT02060188) presented in abstract form, 45 treatment-naïve patients with MSI-H/dMMR metastatic colorectal cancer received nivolumab (3 mg/kg every 2 weeks) with ipilimumab (1 mg/kg every 6 weeks). The primary end point was objective response rate.[107]
The objective response rate was 69% among all enrolled patients and 80% for patients with KRAS variants (n = 10).[107][Level of evidence C2]
At a 2-year clinical follow-up, the median PFS and OS had not been reached.
In the CheckMate 8HW trial (NCT04008030), published in abstract form, 303 patients who had received various lines of treatment were randomly assigned to receive either nivolumab and ipilimumab (n = 202) or chemotherapy alone (n = 101). Some patients were also randomly assigned to receive nivolumab, but results from these patients were not presented in the abstract. Treatments were continued until disease progression or unacceptable toxicity (all arms), or for up to 2 years (nivolumab-ipilimumab arm). A total of 171 patients who received nivolumab and ipilimumab and 84 patients who received chemotherapy alone were centrally confirmed to have dMMR/MSI-H metastatic colorectal cancer.[108]
At a median follow-up of 31.5 months, the PFS was superior for patients who received nivolumab and ipilimumab compared with those who received chemotherapy alone (HR, 0.21; 97.91% CI, 0.13–0.35; P < .0001). Of note, in the chemotherapy arm, 67% of patients received subsequent immunotherapy.
Two grade 5 deaths occurred in the nivolumab-ipilimumab arm. Grade 3 to 4 events occurred in 23% of patients in the nivolumab-ipilimumab arm and 48% of patients in the chemotherapy-alone arm.
Second-line immunotherapy
Pembrolizumab monotherapy
Evidence (pembrolizumab monotherapy):
The FDA approval of pembrolizumab monotherapy was based on data from 149 patients with MSI-H or dMMR cancers enrolled across five uncontrolled, multicohort, multicenter, single-arm clinical trials. Ninety patients had colorectal cancer, and 59 patients were diagnosed with 1 of 14 other cancer types. Patients received either 200 mg of pembrolizumab every 3 weeks or 10 mg/kg of pembrolizumab every 2 weeks. Treatment continued until unacceptable toxicity or disease progression occurred. The major efficacy outcome measures were objective response rate (assessed by blinded independent central radiologists’ review in accordance with Response Evaluation Criteria in Solid Tumors [RECIST] 1.1) and response duration.
The objective response rate was 39.6% (95% CI, 31.7%–47.9%).
Responses lasted 6 months or longer for 78% of patients who responded to pembrolizumab. There were 11 complete responses and 48 partial responses.
The objective response rate was similar whether patients were diagnosed with colorectal cancer (36%) or a different cancer (46% across the 14 other cancer types).
Nivolumab monotherapy
Evidence (nivolumab monotherapy):
In the CheckMate-142 trial (NCT02060188), 74 patients with previously treated dMMR/MSI-H colorectal cancer were enrolled in an open-label, single-arm, phase II study to receive nivolumab (3 mg/kg every 2 weeks). The primary end point was objective response as per RECIST 1.1.[109]
The objective response rate was 31.1% (95% CI, 20.8%–42.9%).
Grade 3 to 4 treatment-related adverse events occurred in 21% of patients.
Nivolumab and ipilimumab
Evidence (nivolumab and ipilimumab):
CheckMate-142 (NCT02060188) was a multicenter, open-label, phase II trial with a cohort for patients with recurrent or metastatic dMMR and/or MSI-H colorectal cancer who had progressed on, were intolerant of, or declined at least one line of chemotherapy (including 5-FU and oxaliplatin and/or irinotecan). The trial enrolled 119 patients who received four doses of nivolumab (3 mg/kg) and ipilimumab (1 mg/kg) every 3 weeks (induction), then nivolumab (3 mg/kg IV) every 2 weeks (maintenance). The primary end point was objective response rate.[109]
The objective response rate was 55% (95% CI, 45.2%–63.8%).
Among patients experiencing a response, 83% had responses lasting more than 6 months.
Grade 3 to 4 treatment-related adverse events occurred in 32% of patients.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Serafini AN, Klein JL, Wolff BG, et al.: Radioimmunoscintigraphy of recurrent, metastatic, or occult colorectal cancer with technetium 99m-labeled totally human monoclonal antibody 88BV59: results of pivotal, phase III multicenter studies. J Clin Oncol 16 (5): 1777-87, 1998. [PUBMED Abstract]
Wagman LD, Kemeny MM, Leong L, et al.: A prospective, randomized evaluation of the treatment of colorectal cancer metastatic to the liver. J Clin Oncol 8 (11): 1885-93, 1990. [PUBMED Abstract]
Scheele J, Stangl R, Altendorf-Hofmann A: Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg 77 (11): 1241-6, 1990. [PUBMED Abstract]
Scheele J, Stangl R, Altendorf-Hofmann A, et al.: Indicators of prognosis after hepatic resection for colorectal secondaries. Surgery 110 (1): 13-29, 1991. [PUBMED Abstract]
Adson MA, van Heerden JA, Adson MH, et al.: Resection of hepatic metastases from colorectal cancer. Arch Surg 119 (6): 647-51, 1984. [PUBMED Abstract]
Coppa GF, Eng K, Ranson JH, et al.: Hepatic resection for metastatic colon and rectal cancer. An evaluation of preoperative and postoperative factors. Ann Surg 202 (2): 203-8, 1985. [PUBMED Abstract]
Gayowski TJ, Iwatsuki S, Madariaga JR, et al.: Experience in hepatic resection for metastatic colorectal cancer: analysis of clinical and pathologic risk factors. Surgery 116 (4): 703-10; discussion 710-1, 1994. [PUBMED Abstract]
Jaeck D, Bachellier P, Guiguet M, et al.: Long-term survival following resection of colorectal hepatic metastases. Association Française de Chirurgie. Br J Surg 84 (7): 977-80, 1997. [PUBMED Abstract]
Taylor M, Forster J, Langer B, et al.: A study of prognostic factors for hepatic resection for colorectal metastases. Am J Surg 173 (6): 467-71, 1997. [PUBMED Abstract]
Elias D, Cavalcanti A, Sabourin JC, et al.: Resection of liver metastases from colorectal cancer: the real impact of the surgical margin. Eur J Surg Oncol 24 (3): 174-9, 1998. [PUBMED Abstract]
Girard P, Ducreux M, Baldeyrou P, et al.: Surgery for lung metastases from colorectal cancer: analysis of prognostic factors. J Clin Oncol 14 (7): 2047-53, 1996. [PUBMED Abstract]
Hughes KS, Simon R, Songhorabodi S, et al.: Resection of the liver for colorectal carcinoma metastases: a multi-institutional study of patterns of recurrence. Surgery 100 (2): 278-84, 1986. [PUBMED Abstract]
Schlag P, Hohenberger P, Herfarth C: Resection of liver metastases in colorectal cancer–competitive analysis of treatment results in synchronous versus metachronous metastases. Eur J Surg Oncol 16 (4): 360-5, 1990. [PUBMED Abstract]
Rosen CB, Nagorney DM, Taswell HF, et al.: Perioperative blood transfusion and determinants of survival after liver resection for metastatic colorectal carcinoma. Ann Surg 216 (4): 493-504; discussion 504-5, 1992. [PUBMED Abstract]
Fong Y, Fortner J, Sun RL, et al.: Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg 230 (3): 309-18; discussion 318-21, 1999. [PUBMED Abstract]
Leonard GD, Brenner B, Kemeny NE: Neoadjuvant chemotherapy before liver resection for patients with unresectable liver metastases from colorectal carcinoma. J Clin Oncol 23 (9): 2038-48, 2005. [PUBMED Abstract]
Hernandez-Alejandro R, Ruffolo LI, Sasaki K, et al.: Recipient and Donor Outcomes After Living-Donor Liver Transplant for Unresectable Colorectal Liver Metastases. JAMA Surg 157 (6): 524-530, 2022. [PUBMED Abstract]
Adam R, Piedvache C, Chiche L, et al.: Chemotherapy and liver transplantation versus chemotherapy alone in patients with definitively unresectable colorectal liver metastases: A prospective multicentric randomized trial (TRANSMET). [Abstract] J Clin Oncol 46 (Suppl 16): A-3500, 2024.
Rossi S, Buscarini E, Garbagnati F, et al.: Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR Am J Roentgenol 170 (4): 1015-22, 1998. [PUBMED Abstract]
Solbiati L, Livraghi T, Goldberg SN, et al.: Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 221 (1): 159-66, 2001. [PUBMED Abstract]
Lencioni R, Goletti O, Armillotta N, et al.: Radio-frequency thermal ablation of liver metastases with a cooled-tip electrode needle: results of a pilot clinical trial. Eur Radiol 8 (7): 1205-11, 1998. [PUBMED Abstract]
Curley SA, Izzo F, Delrio P, et al.: Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg 230 (1): 1-8, 1999. [PUBMED Abstract]
Oshowo A, Gillams A, Harrison E, et al.: Comparison of resection and radiofrequency ablation for treatment of solitary colorectal liver metastases. Br J Surg 90 (10): 1240-3, 2003. [PUBMED Abstract]
Livraghi T, Solbiati L, Meloni F, et al.: Percutaneous radiofrequency ablation of liver metastases in potential candidates for resection: the “test-of-time approach”. Cancer 97 (12): 3027-35, 2003. [PUBMED Abstract]
Pawlik TM, Izzo F, Cohen DS, et al.: Combined resection and radiofrequency ablation for advanced hepatic malignancies: results in 172 patients. Ann Surg Oncol 10 (9): 1059-69, 2003. [PUBMED Abstract]
Jarnagin WR, Fong Y, Ky A, et al.: Liver resection for metastatic colorectal cancer: assessing the risk of occult irresectable disease. J Am Coll Surg 188 (1): 33-42, 1999. [PUBMED Abstract]
Ravikumar TS, Kaleya R, Kishinevsky A: Surgical ablative therapy of liver tumors. Cancer: Principles and Practice of Oncology Updates 14 (3): 1-12, 2000.
Seifert JK, Morris DL: Prognostic factors after cryotherapy for hepatic metastases from colorectal cancer. Ann Surg 228 (2): 201-8, 1998. [PUBMED Abstract]
Bageacu S, Kaczmarek D, Lacroix M, et al.: Cryosurgery for resectable and unresectable hepatic metastases from colorectal cancer. Eur J Surg Oncol 33 (5): 590-6, 2007. [PUBMED Abstract]
Thomas DS, Nauta RJ, Rodgers JE, et al.: Intraoperative high-dose rate interstitial irradiation of hepatic metastases from colorectal carcinoma. Results of a phase I-II trial. Cancer 71 (6): 1977-81, 1993. [PUBMED Abstract]
Ravikumar TS: Interstitial therapies for liver tumors. Surg Oncol Clin N Am 5 (2): 365-77, 1996. [PUBMED Abstract]
McAfee MK, Allen MS, Trastek VF, et al.: Colorectal lung metastases: results of surgical excision. Ann Thorac Surg 53 (5): 780-5; discussion 785-6, 1992. [PUBMED Abstract]
Headrick JR, Miller DL, Nagorney DM, et al.: Surgical treatment of hepatic and pulmonary metastases from colon cancer. Ann Thorac Surg 71 (3): 975-9; discussion 979-80, 2001. [PUBMED Abstract]
Portier G, Elias D, Bouche O, et al.: Multicenter randomized trial of adjuvant fluorouracil and folinic acid compared with surgery alone after resection of colorectal liver metastases: FFCD ACHBTH AURC 9002 trial. J Clin Oncol 24 (31): 4976-82, 2006. [PUBMED Abstract]
Mitry E, Fields AL, Bleiberg H, et al.: Adjuvant chemotherapy after potentially curative resection of metastases from colorectal cancer: a pooled analysis of two randomized trials. J Clin Oncol 26 (30): 4906-11, 2008. [PUBMED Abstract]
Ychou M, Hohenberger W, Thezenas S, et al.: A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer. Ann Oncol 20 (12): 1964-70, 2009. [PUBMED Abstract]
Nordlinger B, Sorbye H, Glimelius B, et al.: Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 371 (9617): 1007-16, 2008. [PUBMED Abstract]
Kemeny N, Daly J, Reichman B, et al.: Intrahepatic or systemic infusion of fluorodeoxyuridine in patients with liver metastases from colorectal carcinoma. A randomized trial. Ann Intern Med 107 (4): 459-65, 1987. [PUBMED Abstract]
Chang AE, Schneider PD, Sugarbaker PH, et al.: A prospective randomized trial of regional versus systemic continuous 5-fluorodeoxyuridine chemotherapy in the treatment of colorectal liver metastases. Ann Surg 206 (6): 685-93, 1987. [PUBMED Abstract]
Rougier P, Laplanche A, Huguier M, et al.: Hepatic arterial infusion of floxuridine in patients with liver metastases from colorectal carcinoma: long-term results of a prospective randomized trial. J Clin Oncol 10 (7): 1112-8, 1992. [PUBMED Abstract]
Kemeny N, Cohen A, Seiter K, et al.: Randomized trial of hepatic arterial floxuridine, mitomycin, and carmustine versus floxuridine alone in previously treated patients with liver metastases from colorectal cancer. J Clin Oncol 11 (2): 330-5, 1993. [PUBMED Abstract]
Reappraisal of hepatic arterial infusion in the treatment of nonresectable liver metastases from colorectal cancer. Meta-Analysis Group in Cancer. J Natl Cancer Inst 88 (5): 252-8, 1996. [PUBMED Abstract]
Mocellin S, Pilati P, Lise M, et al.: Meta-analysis of hepatic arterial infusion for unresectable liver metastases from colorectal cancer: the end of an era? J Clin Oncol 25 (35): 5649-54, 2007. [PUBMED Abstract]
Kemeny N, Huang Y, Cohen AM, et al.: Hepatic arterial infusion of chemotherapy after resection of hepatic metastases from colorectal cancer. N Engl J Med 341 (27): 2039-48, 1999. [PUBMED Abstract]
Kemeny MM, Adak S, Gray B, et al.: Combined-modality treatment for resectable metastatic colorectal carcinoma to the liver: surgical resection of hepatic metastases in combination with continuous infusion of chemotherapy–an intergroup study. J Clin Oncol 20 (6): 1499-505, 2002. [PUBMED Abstract]
Petrelli N, Herrera L, Rustum Y, et al.: A prospective randomized trial of 5-fluorouracil versus 5-fluorouracil and high-dose leucovorin versus 5-fluorouracil and methotrexate in previously untreated patients with advanced colorectal carcinoma. J Clin Oncol 5 (10): 1559-65, 1987. [PUBMED Abstract]
Petrelli N, Douglass HO, Herrera L, et al.: The modulation of fluorouracil with leucovorin in metastatic colorectal carcinoma: a prospective randomized phase III trial. Gastrointestinal Tumor Study Group. J Clin Oncol 7 (10): 1419-26, 1989. [PUBMED Abstract]
Scheithauer W, Rosen H, Kornek GV, et al.: Randomised comparison of combination chemotherapy plus supportive care with supportive care alone in patients with metastatic colorectal cancer. BMJ 306 (6880): 752-5, 1993. [PUBMED Abstract]
Expectancy or primary chemotherapy in patients with advanced asymptomatic colorectal cancer: a randomized trial. Nordic Gastrointestinal Tumor Adjuvant Therapy Group. J Clin Oncol 10 (6): 904-11, 1992. [PUBMED Abstract]
Buyse M, Thirion P, Carlson RW, et al.: Relation between tumour response to first-line chemotherapy and survival in advanced colorectal cancer: a meta-analysis. Meta-Analysis Group in Cancer. Lancet 356 (9227): 373-8, 2000. [PUBMED Abstract]
Leichman CG, Fleming TR, Muggia FM, et al.: Phase II study of fluorouracil and its modulation in advanced colorectal cancer: a Southwest Oncology Group study. J Clin Oncol 13 (6): 1303-11, 1995. [PUBMED Abstract]
Van Cutsem E, Twelves C, Cassidy J, et al.: Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol 19 (21): 4097-106, 2001. [PUBMED Abstract]
Hoff PM, Ansari R, Batist G, et al.: Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 19 (8): 2282-92, 2001. [PUBMED Abstract]
Saltz LB, Cox JV, Blanke C, et al.: Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med 343 (13): 905-14, 2000. [PUBMED Abstract]
de Gramont A, Figer A, Seymour M, et al.: Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 18 (16): 2938-47, 2000. [PUBMED Abstract]
Douillard JY, Cunningham D, Roth AD, et al.: Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet 355 (9209): 1041-7, 2000. [PUBMED Abstract]
Tournigand C, André T, Achille E, et al.: FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol 22 (2): 229-37, 2004. [PUBMED Abstract]
Colucci G, Gebbia V, Paoletti G, et al.: Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell’Italia Meridionale. J Clin Oncol 23 (22): 4866-75, 2005. [PUBMED Abstract]
Fuchs CS, Marshall J, Mitchell E, et al.: Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol 25 (30): 4779-86, 2007. [PUBMED Abstract]
Díaz-Rubio E, Tabernero J, Gómez-España A, et al.: Phase III study of capecitabine plus oxaliplatin compared with continuous-infusion fluorouracil plus oxaliplatin as first-line therapy in metastatic colorectal cancer: final report of the Spanish Cooperative Group for the Treatment of Digestive Tumors Trial. J Clin Oncol 25 (27): 4224-30, 2007. [PUBMED Abstract]
Porschen R, Arkenau HT, Kubicka S, et al.: Phase III study of capecitabine plus oxaliplatin compared with fluorouracil and leucovorin plus oxaliplatin in metastatic colorectal cancer: a final report of the AIO Colorectal Study Group. J Clin Oncol 25 (27): 4217-23, 2007. [PUBMED Abstract]
Rothenberg ML, Eckardt JR, Kuhn JG, et al.: Phase II trial of irinotecan in patients with progressive or rapidly recurrent colorectal cancer. J Clin Oncol 14 (4): 1128-35, 1996. [PUBMED Abstract]
Conti JA, Kemeny NE, Saltz LB, et al.: Irinotecan is an active agent in untreated patients with metastatic colorectal cancer. J Clin Oncol 14 (3): 709-15, 1996. [PUBMED Abstract]
Rougier P, Van Cutsem E, Bajetta E, et al.: Randomised trial of irinotecan versus fluorouracil by continuous infusion after fluorouracil failure in patients with metastatic colorectal cancer. Lancet 352 (9138): 1407-12, 1998. [PUBMED Abstract]
Cunningham D, Pyrhönen S, James RD, et al.: Randomised trial of irinotecan plus supportive care versus supportive care alone after fluorouracil failure for patients with metastatic colorectal cancer. Lancet 352 (9138): 1413-8, 1998. [PUBMED Abstract]
Rothenberg ML, Oza AM, Bigelow RH, et al.: Superiority of oxaliplatin and fluorouracil-leucovorin compared with either therapy alone in patients with progressive colorectal cancer after irinotecan and fluorouracil-leucovorin: interim results of a phase III trial. J Clin Oncol 21 (11): 2059-69, 2003. [PUBMED Abstract]
Hurwitz H, Fehrenbacher L, Novotny W, et al.: Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350 (23): 2335-42, 2004. [PUBMED Abstract]
Sanoff HK, Sargent DJ, Campbell ME, et al.: Five-year data and prognostic factor analysis of oxaliplatin and irinotecan combinations for advanced colorectal cancer: N9741. J Clin Oncol 26 (35): 5721-7, 2008. [PUBMED Abstract]
Saltz LB, Clarke S, Díaz-Rubio E, et al.: Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 26 (12): 2013-9, 2008. [PUBMED Abstract]
Cassidy J, Clarke S, Díaz-Rubio E, et al.: Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J Clin Oncol 26 (12): 2006-12, 2008. [PUBMED Abstract]
Giantonio BJ, Catalano PJ, Meropol NJ, et al.: High-dose bevacizumab improves survival when combined with FOLFOX4 in previously treated advanced colorectal cancer: results from the Eastern Cooperative Oncology Group (ECOG) study E3200. [Abstract] J Clin Oncol 23 (Suppl 16): A-2, 1s, 2005.
Arnold D, Andre T, Bennouna J, et al.: Bevacizumab (BEV) plus chemotherapy (CT) continued beyond first progression in patients with metastatic colorectal cancer (mCRC) previously treated with BEV plus CT: results of a randomized phase III intergroup study (TML study). [Abstract] J Clin Oncol 30 (Suppl 15): A-CRA3503, 2012.
Loupakis F, Cremolini C, Masi G, et al.: Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med 371 (17): 1609-18, 2014. [PUBMED Abstract]
Cunningham D, Humblet Y, Siena S, et al.: Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351 (4): 337-45, 2004. [PUBMED Abstract]
Van Cutsem E, Köhne CH, Hitre E, et al.: Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med 360 (14): 1408-17, 2009. [PUBMED Abstract]
Tol J, Koopman M, Cats A, et al.: Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl J Med 360 (6): 563-72, 2009. [PUBMED Abstract]
Maughan TS, Adams RA, Smith CG, et al.: Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 377 (9783): 2103-14, 2011. [PUBMED Abstract]
Adams RA, Meade AM, Seymour MT, et al.: Intermittent versus continuous oxaliplatin and fluoropyrimidine combination chemotherapy for first-line treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet Oncol 12 (7): 642-53, 2011. [PUBMED Abstract]
Bokemeyer C, Cutsem EV, Rougier P, et al.: Addition of cetuximab to chemotherapy as first-line treatment for KRAS wild-type metastatic colorectal cancer: pooled analysis of the CRYSTAL and OPUS randomised clinical trials. Eur J Cancer 48 (10): 1466-75, 2012. [PUBMED Abstract]
Van Cutsem E, Tabernero J, Lakomy R, et al.: Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol 30 (28): 3499-506, 2012. [PUBMED Abstract]
Tabernero J, Yoshino T, Cohn AL, et al.: Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol 16 (5): 499-508, 2015. [PUBMED Abstract]
Van Cutsem E, Peeters M, Siena S, et al.: Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 25 (13): 1658-64, 2007. [PUBMED Abstract]
Douillard JY, Siena S, Cassidy J, et al.: Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 28 (31): 4697-705, 2010. [PUBMED Abstract]
Douillard JY, Oliner KS, Siena S, et al.: Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 369 (11): 1023-34, 2013. [PUBMED Abstract]
Hecht JR, Mitchell E, Chidiac T, et al.: A randomized phase IIIB trial of chemotherapy, bevacizumab, and panitumumab compared with chemotherapy and bevacizumab alone for metastatic colorectal cancer. J Clin Oncol 27 (5): 672-80, 2009. [PUBMED Abstract]
Peeters M, Price TJ, Cervantes A, et al.: Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol 28 (31): 4706-13, 2010. [PUBMED Abstract]
Heinemann V, von Weikersthal LF, Decker T, et al.: FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol 15 (10): 1065-75, 2014. [PUBMED Abstract]
Venook AP, Niedzwiecki D, Lenz HJ, et al.: CALGB/SWOG 80405: Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC). [Abstract] J Clin Oncol 32 (Suppl 5): A-LBA3, 2014.
Stintzing S, Modest DP, Rossius L, et al.: FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): a post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol 17 (10): 1426-1434, 2016. [PUBMED Abstract]
Modest DP, Stintzing S, von Weikersthal LF, et al.: Impact of Subsequent Therapies on Outcome of the FIRE-3/AIO KRK0306 Trial: First-Line Therapy With FOLFIRI Plus Cetuximab or Bevacizumab in Patients With KRAS Wild-Type Tumors in Metastatic Colorectal Cancer. J Clin Oncol 33 (32): 3718-26, 2015. [PUBMED Abstract]
Mayer RJ, Van Cutsem E, Falcone A, et al.: Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med 372 (20): 1909-19, 2015. [PUBMED Abstract]
Prager GW, Taieb J, Fakih M, et al.: Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer. N Engl J Med 388 (18): 1657-1667, 2023. [PUBMED Abstract]
Grothey A, Sobrero AF, Siena S, et al.: Results of a phase III randomized, double-blind, placebo-controlled, multicenter trial (CORRECT) of regorafenib plus best supportive care (BSC) versus placebo plus BSC in patients (pts) with metastatic colorectal cancer (mCRC) who have progressed after standard therapies. [Abstract] J Clin Oncol 30 (Suppl 4): A-LBA385, 2012.
Grothey A, Van Cutsem E, Sobrero A, et al.: Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 381 (9863): 303-12, 2013. [PUBMED Abstract]
Dasari A, Lonardi S, Garcia-Carbonero R, et al.: Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet 402 (10395): 41-53, 2023. [PUBMED Abstract]
Kopetz S, Grothey A, Yaeger R, et al.: Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N Engl J Med 381 (17): 1632-1643, 2019. [PUBMED Abstract]
Kopetz S, Grothey A, Van Cutsem E, et al.: Encorafenib plus cetuximab with or without binimetinib for BRAF V600E metastatic colorectal cancer: updated survival results from a randomized, three-arm, phase III study versus choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). [Abstract] J Clin Oncol 38 (15) (suppl): A-4001, 2020. Available online. Last accessed January 30, 2025.
Fakih M, Tu H, Hsu H, et al.: Real-World Study of Characteristics and Treatment Outcomes Among Patients with KRAS p.G12C-Mutated or Other KRAS Mutated Metastatic Colorectal Cancer. Oncologist 27 (8): 663-674, 2022. [PUBMED Abstract]
Lee JK, Sivakumar S, Schrock AB, et al.: Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol 6 (1): 91, 2022. [PUBMED Abstract]
Neumann J, Zeindl-Eberhart E, Kirchner T, et al.: Frequency and type of KRAS mutations in routine diagnostic analysis of metastatic colorectal cancer. Pathol Res Pract 205 (12): 858-62, 2009. [PUBMED Abstract]
Henry JT, Coker O, Chowdhury S, et al.: Comprehensive Clinical and Molecular Characterization of KRAS G12C-Mutant Colorectal Cancer. JCO Precis Oncol 5: , 2021. [PUBMED Abstract]
Fakih MG, Salvatore L, Esaki T, et al.: Sotorasib plus Panitumumab in Refractory Colorectal Cancer with Mutated KRAS G12C. N Engl J Med 389 (23): 2125-2139, 2023. [PUBMED Abstract]
Yaeger R, Weiss J, Pelster MS, et al.: Adagrasib with or without Cetuximab in Colorectal Cancer with Mutated KRAS G12C. N Engl J Med 388 (1): 44-54, 2023. [PUBMED Abstract]
André T, Shiu KK, Kim TW, et al.: Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med 383 (23): 2207-2218, 2020. [PUBMED Abstract]
Andre T, Shiu K, Kim TW, et al.: Final overall survival for the phase III KN177 study: pembrolizumab versus chemotherapy in microsatellite instability-high/mismatch repair deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC). [Abstract] J Clin Oncol 39 (15) (suppl): A-3500, 2021. Available online. Last accessed January 30, 2025.
Lenz H, Lonardi S, Zagonel V, et al.: Subgroup analyses of patients (pts) with microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC) treated with nivolumab (NIVO) plus low-dose ipilimumab (IPI) as first-line (1L) therapy: two-year clinical update. [Abstract] J Clin Oncol 39 (3) (suppl): A-58, 2021. Available online. Last accessed January 30, 2025.
Lenz HJ, Lonardi S, Elez E, et al.: Nivolumab (NIVO) plus ipilimumab (IPI) vs chemotherapy (chemo) as first-line (1L) treatment for microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC): Expanded efficacy analysis from CheckMate 8HW. [Abstract] J Clin Oncol 42 (Suppl 16): A-3503, 2024.
Overman MJ, McDermott R, Leach JL, et al.: Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol 18 (9): 1182-1191, 2017. [PUBMED Abstract]
Latest Updates to This Summary (02/12/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Added text to state that, worldwide, colorectal cancer is the third most common form of cancer. In 2022, there were an estimated 1.93 million new cases of colorectal cancer and 903,859 deaths (cited Bray et al. as reference 1).
Updated statistics with estimated new cases and deaths for 2025 (cited American Cancer Society as reference 2).
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of colon cancer. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Colon Cancer Treatment are:
Amit Chowdhry, MD, PhD (University of Rochester Medical Center)
Leon Pappas, MD, PhD (Massachusetts General Hospital)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Colon Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/hp/colon-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389297]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
It is difficult to separate epidemiological considerations of rectal cancer from those of colon cancer because studies often consider colon and rectal cancer together (i.e., colorectal cancer).
Worldwide, colorectal cancer is the third most common form of cancer. In 2022, there were an estimated 1.93 million new cases of colorectal cancer and 903,859 deaths.[1]
Estimated new cases and deaths from rectal and colon cancer in the United States in 2025:[2]
New cases of rectal cancer: 46,950.
New cases of colon cancer: 107,320.
Deaths: 52,900 (rectal and colon cancers combined).
Colorectal cancer affects men and women almost equally. Among all racial groups in the United States, Black individuals have the highest sporadic colorectal cancer incidence and mortality rates.[3,4]
Anatomy
EnlargeAnatomy of the lower gastrointestinal (digestive) system.
The rectum is located within the pelvis, extending from the transitional mucosa of the anal dentate line to the sigmoid colon at the peritoneal reflection. By rigid sigmoidoscopy, the rectum measures between 10 cm and 15 cm from the anal verge.[5] The location of a rectal tumor is usually indicated by the distance between the anal verge, dentate line, or anorectal ring and the lower edge of the tumor, with measurements differing depending on the use of a rigid or flexible endoscope or digital examination.[6]
The distance of the tumor from the anal sphincter musculature has implications for the ability to perform sphincter-sparing surgery. The bony constraints of the pelvis limit surgical access to the rectum, which results in a lower likelihood of attaining widely negative margins and a higher risk of local recurrence.[5]
Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for colorectal cancer include the following:
Family history of colorectal cancer in a first-degree relative.[7]
Personal history of colorectal adenomas, colorectal cancer, or ovarian cancer.[8–10]
Hereditary conditions, including familial adenomatous polyposis (FAP) and Lynch syndrome (hereditary nonpolyposis colorectal cancer [HNPCC]).[11]
Personal history of long-standing chronic ulcerative colitis or Crohn colitis.[12]
Evidence supports screening for rectal cancer as a part of routine care for all adults aged 50 years and older, especially for those with first-degree relatives with colorectal cancer. Reasons include the following:
Incidence of the disease in adults 50 years and older.
Ability to identify high-risk groups.
Slow growth of primary lesions.
Better survival of patients with early-stage lesions.
Relative simplicity and accuracy of screening tests.
Similar to colon cancer, symptoms of rectal cancer may include:[18]
Rectal bleeding.
Change in bowel habits.
Abdominal pain.
Intestinal obstruction.
Change in appetite.
Weight loss.
Weakness.
With the exception of obstructive symptoms, these symptoms do not necessarily correlate with the stage of disease or signify a particular diagnosis.[19]
Diagnostic Evaluation
The initial clinical evaluation may include:
Physical exam and history.
Digital rectal exam.
Colonoscopy.
Biopsy.
Carcinoembryonic antigen (CEA) assay.
Immunohistochemistry.
DNA mismatch repair/microsatellite instability (MSI) testing.
Physical examination may reveal a palpable mass and bright blood in the rectum. Adenopathy, hepatomegaly, or pulmonary signs may be present with metastatic disease.[6] Laboratory examination may reveal iron-deficiency anemia and electrolyte and liver function abnormalities.
Prognostic Factors
The prognosis of patients with rectal cancer is related to several factors, including:[6,20–28]
Tumor adherence to or invasion of adjacent organs.[20]
Presence or absence of tumor involvement in the lymph nodes and the number of positive lymph nodes.[6,21–24]
Presence or absence of high-risk pathological features, including:[26,27,29]
Positive surgical margins.
Lymphovascular invasion.
Perineural invasion.
Poorly differentiated histology.
Circumferential resection margin (CRM) or depth of penetration of the tumor through the bowel wall.[6,25,30] Measured in millimeters, CRM is defined as the retroperitoneal or peritoneal adventitial soft-tissue margin closest to the deepest penetration of the tumor.
Presence of MSI that results from impaired DNA mismatch repair.
Only disease stage (designated by tumor [T], nodal status [N], and distant metastasis [M]) has been validated as a prognostic factor in multi-institutional prospective studies.[20–25] A major pooled analysis evaluating the impact of T and N stage and treatment on survival and relapse in patients with rectal cancer who are treated with adjuvant therapy confirmed these findings.[31]
Mismatch repair deficiency occurs in 5% to 10% of patients with rectal adenocarcinomas. Mismatch repair–deficient tumors do not respond well to chemotherapy applied in the neoadjuvant, adjuvant, or metastatic settings.[32–34] In a population-based series of 607 patients aged 50 years or younger at the time of diagnosis, MSI-related colorectal cancer was associated with improved survival that was independent of tumor stage. MSI is also associated with Lynch syndrome.[35] In addition, gene expression profiling is useful for predicting the response of rectal adenocarcinomas to preoperative chemoradiation therapy. It can also help determine the prognosis of stages II and III rectal cancer after neoadjuvant fluorouracil-based chemoradiation therapy.[36,37]
Racial and ethnic differences in overall survival (OS) after adjuvant therapy for rectal cancer have been observed, with shorter OS for Black patients than for White patients. Factors contributing to this disparity may include tumor position, type of surgical procedure, and presence of comorbid conditions.[38]
Follow-Up After Treatment
The primary goals of postoperative surveillance programs for rectal cancer are to:[39]
Assess the efficacy of initial therapy.
Detect new or metachronous malignancies.
Detect potentially curable recurrent or metastatic cancers.
Routine, periodic studies following treatment for rectal cancer may lead to earlier identification and management of recurrent disease.[39–43] A statistically significant survival benefit has been demonstrated for more intensive follow-up protocols in two clinical trials. A meta-analysis that combined these two trials with four others reported a statistically significant improvement in survival for patients who were intensively followed.[39,44,45]
Guidelines for surveillance after initial treatment with curative intent for colorectal cancer vary between leading U.S. and European oncology societies, and optimal surveillance strategies remain uncertain.[46,47] Large, well-designed, prospective, multi-institutional, randomized studies are required to establish an evidence-based consensus for follow-up evaluation.
Carcinoembryonic antigen (CEA)
Measurement of CEA, a serum glycoprotein, is frequently used in the management and follow-up of patients with rectal cancer. A review of the use of this tumor marker for rectal cancer suggests the following:[39]
Serum CEA testing is not a valuable screening tool for rectal cancer because of its low sensitivity and low specificity.
Postoperative CEA testing is typically restricted to patients who are potential candidates for further intervention, as follows:
Patients with stage II or III rectal cancer (every 2–3 months for at least 2 years after diagnosis).
Patients with rectal cancer who would be candidates for resection of liver metastases.
In one Dutch retrospective study of total mesorectal excision for the treatment of rectal cancer, investigators found that the preoperative serum CEA level was normal in most patients with rectal cancer, and yet, serum CEA levels rose by at least 50% in patients with recurrence. The authors concluded that serial, postoperative CEA testing cannot be discarded based on a normal preoperative serum CEA level in patients with rectal cancer.[48,49]
References
Bray F, Laversanne M, Sung H, et al.: Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 74 (3): 229-263, 2024. [PUBMED Abstract]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Albano JD, Ward E, Jemal A, et al.: Cancer mortality in the United States by education level and race. J Natl Cancer Inst 99 (18): 1384-94, 2007. [PUBMED Abstract]
Wolpin BM, Meyerhardt JA, Mamon HJ, et al.: Adjuvant treatment of colorectal cancer. CA Cancer J Clin 57 (3): 168-85, 2007 May-Jun. [PUBMED Abstract]
Libutti SK, Willett CG, Saltz LB: Cancer of the rectum. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Lippincott Williams & Wilkins, 2011, pp 1127-41.
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Imperiale TF, Juluri R, Sherer EA, et al.: A risk index for advanced neoplasia on the second surveillance colonoscopy in patients with previous adenomatous polyps. Gastrointest Endosc 80 (3): 471-8, 2014. [PUBMED Abstract]
Singh H, Nugent Z, Demers A, et al.: Risk of colorectal cancer after diagnosis of endometrial cancer: a population-based study. J Clin Oncol 31 (16): 2010-5, 2013. [PUBMED Abstract]
Srinivasan R, Yang YX, Rubin SC, et al.: Risk of colorectal cancer in women with a prior diagnosis of gynecologic malignancy. J Clin Gastroenterol 41 (3): 291-6, 2007. [PUBMED Abstract]
Mork ME, You YN, Ying J, et al.: High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults With Colorectal Cancer. J Clin Oncol 33 (31): 3544-9, 2015. [PUBMED Abstract]
Laukoetter MG, Mennigen R, Hannig CM, et al.: Intestinal cancer risk in Crohn’s disease: a meta-analysis. J Gastrointest Surg 15 (4): 576-83, 2011. [PUBMED Abstract]
Fedirko V, Tramacere I, Bagnardi V, et al.: Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol 22 (9): 1958-72, 2011. [PUBMED Abstract]
Liang PS, Chen TY, Giovannucci E: Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer 124 (10): 2406-15, 2009. [PUBMED Abstract]
Laiyemo AO, Doubeni C, Pinsky PF, et al.: Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities. J Natl Cancer Inst 102 (8): 538-46, 2010. [PUBMED Abstract]
Lansdorp-Vogelaar I, Kuntz KM, Knudsen AB, et al.: Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol Biomarkers Prev 21 (5): 728-36, 2012. [PUBMED Abstract]
Ma Y, Yang Y, Wang F, et al.: Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One 8 (1): e53916, 2013. [PUBMED Abstract]
Stein W, Farina A, Gaffney K, et al.: Characteristics of colon cancer at time of presentation. Fam Pract Res J 13 (4): 355-63, 1993. [PUBMED Abstract]
Majumdar SR, Fletcher RH, Evans AT: How does colorectal cancer present? Symptoms, duration, and clues to location. Am J Gastroenterol 94 (10): 3039-45, 1999. [PUBMED Abstract]
Compton CC, Greene FL: The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin 54 (6): 295-308, 2004 Nov-Dec. [PUBMED Abstract]
Swanson RS, Compton CC, Stewart AK, et al.: The prognosis of T3N0 colon cancer is dependent on the number of lymph nodes examined. Ann Surg Oncol 10 (1): 65-71, 2003 Jan-Feb. [PUBMED Abstract]
Le Voyer TE, Sigurdson ER, Hanlon AL, et al.: Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol 21 (15): 2912-9, 2003. [PUBMED Abstract]
Prandi M, Lionetto R, Bini A, et al.: Prognostic evaluation of stage B colon cancer patients is improved by an adequate lymphadenectomy: results of a secondary analysis of a large scale adjuvant trial. Ann Surg 235 (4): 458-63, 2002. [PUBMED Abstract]
Tepper JE, O’Connell MJ, Niedzwiecki D, et al.: Impact of number of nodes retrieved on outcome in patients with rectal cancer. J Clin Oncol 19 (1): 157-63, 2001. [PUBMED Abstract]
Balch GC, De Meo A, Guillem JG: Modern management of rectal cancer: a 2006 update. World J Gastroenterol 12 (20): 3186-95, 2006. [PUBMED Abstract]
Weiser MR, Landmann RG, Wong WD, et al.: Surgical salvage of recurrent rectal cancer after transanal excision. Dis Colon Rectum 48 (6): 1169-75, 2005. [PUBMED Abstract]
Fujita S, Nakanisi Y, Taniguchi H, et al.: Cancer invasion to Auerbach’s plexus is an important prognostic factor in patients with pT3-pT4 colorectal cancer. Dis Colon Rectum 50 (11): 1860-6, 2007. [PUBMED Abstract]
Griffin MR, Bergstralh EJ, Coffey RJ, et al.: Predictors of survival after curative resection of carcinoma of the colon and rectum. Cancer 60 (9): 2318-24, 1987. [PUBMED Abstract]
DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Lippincott Williams & Wilkins, 2011.
Wieder HA, Rosenberg R, Lordick F, et al.: Rectal cancer: MR imaging before neoadjuvant chemotherapy and radiation therapy for prediction of tumor-free circumferential resection margins and long-term survival. Radiology 243 (3): 744-51, 2007. [PUBMED Abstract]
Gunderson LL, Sargent DJ, Tepper JE, et al.: Impact of T and N stage and treatment on survival and relapse in adjuvant rectal cancer: a pooled analysis. J Clin Oncol 22 (10): 1785-96, 2004. [PUBMED Abstract]
Le DT, Uram JN, Wang H, et al.: PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 372 (26): 2509-20, 2015. [PUBMED Abstract]
Overman MJ, Lonardi S, Wong KYM, et al.: Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol 36 (8): 773-779, 2018. [PUBMED Abstract]
André T, Shiu KK, Kim TW, et al.: Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med 383 (23): 2207-2218, 2020. [PUBMED Abstract]
Gryfe R, Kim H, Hsieh ET, et al.: Tumor microsatellite instability and clinical outcome in young patients with colorectal cancer. N Engl J Med 342 (2): 69-77, 2000. [PUBMED Abstract]
Liersch T, Langer C, Ghadimi BM, et al.: Lymph node status and TS gene expression are prognostic markers in stage II/III rectal cancer after neoadjuvant fluorouracil-based chemoradiotherapy. J Clin Oncol 24 (25): 4062-8, 2006. [PUBMED Abstract]
Ghadimi BM, Grade M, Difilippantonio MJ, et al.: Effectiveness of gene expression profiling for response prediction of rectal adenocarcinomas to preoperative chemoradiotherapy. J Clin Oncol 23 (9): 1826-38, 2005. [PUBMED Abstract]
Dignam JJ, Ye Y, Colangelo L, et al.: Prognosis after rectal cancer in blacks and whites participating in adjuvant therapy randomized trials. J Clin Oncol 21 (3): 413-20, 2003. [PUBMED Abstract]
Abir F, Alva S, Longo WE, et al.: The postoperative surveillance of patients with colon cancer and rectal cancer. Am J Surg 192 (1): 100-8, 2006. [PUBMED Abstract]
Martin EW, Minton JP, Carey LC: CEA-directed second-look surgery in the asymptomatic patient after primary resection of colorectal carcinoma. Ann Surg 202 (3): 310-7, 1985. [PUBMED Abstract]
Bruinvels DJ, Stiggelbout AM, Kievit J, et al.: Follow-up of patients with colorectal cancer. A meta-analysis. Ann Surg 219 (2): 174-82, 1994. [PUBMED Abstract]
Lautenbach E, Forde KA, Neugut AI: Benefits of colonoscopic surveillance after curative resection of colorectal cancer. Ann Surg 220 (2): 206-11, 1994. [PUBMED Abstract]
Khoury DA, Opelka FG, Beck DE, et al.: Colon surveillance after colorectal cancer surgery. Dis Colon Rectum 39 (3): 252-6, 1996. [PUBMED Abstract]
Pietra N, Sarli L, Costi R, et al.: Role of follow-up in management of local recurrences of colorectal cancer: a prospective, randomized study. Dis Colon Rectum 41 (9): 1127-33, 1998. [PUBMED Abstract]
Secco GB, Fardelli R, Gianquinto D, et al.: Efficacy and cost of risk-adapted follow-up in patients after colorectal cancer surgery: a prospective, randomized and controlled trial. Eur J Surg Oncol 28 (4): 418-23, 2002. [PUBMED Abstract]
Pfister DG, Benson AB, Somerfield MR: Clinical practice. Surveillance strategies after curative treatment of colorectal cancer. N Engl J Med 350 (23): 2375-82, 2004. [PUBMED Abstract]
Li Destri G, Di Cataldo A, Puleo S: Colorectal cancer follow-up: useful or useless? Surg Oncol 15 (1): 1-12, 2006. [PUBMED Abstract]
Kapiteijn E, Kranenbarg EK, Steup WH, et al.: Total mesorectal excision (TME) with or without preoperative radiotherapy in the treatment of primary rectal cancer. Prospective randomised trial with standard operative and histopathological techniques. Dutch ColoRectal Cancer Group. Eur J Surg 165 (5): 410-20, 1999. [PUBMED Abstract]
Grossmann I, de Bock GH, Meershoek-Klein Kranenbarg WM, et al.: Carcinoembryonic antigen (CEA) measurement during follow-up for rectal carcinoma is useful even if normal levels exist before surgery. A retrospective study of CEA values in the TME trial. Eur J Surg Oncol 33 (2): 183-7, 2007. [PUBMED Abstract]
Cellular Classification and Pathology of Rectal Cancer
Adenocarcinomas account for most rectal tumors in the United States. Other histological types account for an estimated 2% to 5% of colorectal tumors.[1]
The World Health Organization classification of tumors of the colon and rectum includes:[2]
Kang H, O’Connell JB, Leonardi MJ, et al.: Rare tumors of the colon and rectum: a national review. Int J Colorectal Dis 22 (2): 183-9, 2007. [PUBMED Abstract]
Hamilton SR, Aaltonen LA: Pathology and Genetics of Tumours of the Digestive System. International Agency for Research on Cancer, 2000.
Stage Information for Rectal Cancer
Accurate staging provides crucial information about the location and size of the primary tumor in the rectum, and, if present, the size, number, and location of any metastases. Accurate initial staging can influence therapy by helping to determine the type of surgical intervention and the choice of neoadjuvant therapy to maximize the likelihood of resection with clear margins. In primary rectal cancer, pelvic imaging helps determine the following factors:[1–7]
The depth of tumor invasion.
The distance from the sphincter complex.
The potential for achieving negative circumferential (radial) margins.
The involvement of locoregional lymph nodes or adjacent organs.
Staging Evaluation
Clinical evaluation and staging procedures may include:
Digital-rectal examination (DRE): DRE and/or rectovaginal exam and rigid proctoscopy to determine if sphincter-saving surgery is possible.[1,2,5]
Colonoscopy: Complete colonoscopy to rule out cancers elsewhere in the bowel.[5]
Computed tomography (CT): Pan-body CT scan to rule out metastatic disease.[5]
Magnetic resonance imaging (MRI): MRI of the abdomen and pelvis to determine the depth of penetration and the potential for achieving negative circumferential (radial) margins and to identify locoregional nodal metastases and distant metastatic disease. MRI may be particularly helpful in determining sacral involvement in local recurrence.[1]
Endorectal ultrasound: Endorectal ultrasound with a rigid probe or a flexible scope for stenotic lesions to determine the depth of penetration and identify locoregional nodal metastases.[2,4]
Positron emission tomography (PET): PET to image distant metastatic disease.[1]
Carcinoembryonic antigen (CEA): Measurement of the serum CEA level for prognostic assessment and the determination of response to therapy.[6,7]
In the tumor (T) staging of rectal carcinoma, several studies indicate that the accuracy of endorectal ultrasound ranges from 80% to 95% compared with 65% to 75% for CT and 75% to 85% for MRI. The accuracy in determining metastatic nodal involvement by endorectal ultrasound is approximately 70% to 75% compared with 55% to 65% for CT and 60% to 70% for MRI.[2] In a meta-analysis of 84 studies, none of the three imaging modalities, including endorectal ultrasound, CT, and MRI, were significantly superior to the others in staging nodal (N) status.[8] Endorectal ultrasound using a rigid probe may be similarly accurate in T and N staging when compared with endorectal ultrasound using a flexible scope. However, a technically difficult endorectal ultrasound may give an inconclusive or inaccurate result for both T stage and N stage. In this case, further assessment by MRI or flexible endorectal ultrasound may be considered.[4,9]
In patients with rectal cancer, the circumferential resection margin is an important pathological staging parameter. Measured in millimeters, it is defined as the retroperitoneal or peritoneal adventitial soft-tissue margin closest to the deepest penetration of tumor.[10]
AJCC Stage Groupings and TNM Definitions
The AJCC has designated staging by TNM (tumor, node, metastasis) classification to define rectal cancer.[11] The same classification is used for both clinical and pathological staging.[11] Treatment decisions are made with reference to the TNM classification system, rather than the older Dukes or Modified Astler-Coller classification schema.
Cancers staged using this staging system include adenocarcinomas, high-grade neuroendocrine carcinomas, and squamous carcinomas of the colon and rectum. Cancers not staged using this staging system include these histopathological types of cancer: appendiceal carcinomas, anal carcinomas, well-differentiated neuroendocrine tumors (carcinoids).[11] For more information, see Anal Cancer Treatment and Gastrointestinal Neuroendocrine Tumors Treatment.
Lymph node status
The AJCC and a National Cancer Institute-sponsored panel suggested that at least 10 to 14 lymph nodes be examined in radical colon and rectum resections in patients who did not receive neoadjuvant therapy. In cases in which a tumor is resected for palliation or in patients who have received preoperative radiation therapy, fewer lymph nodes may be present.[10–12] This takes into consideration that the number of lymph nodes examined is a reflection of both the aggressiveness of lymphovascular mesenteric dissection at the time of surgical resection and the pathological identification of nodes in the specimen.
Retrospective studies, such as Intergroup trial INT-0089 (NCT00201331), have demonstrated that the number of lymph nodes examined during colon and rectal surgery may be associated with patient outcome.[13–16]
A new tumor-metastasis staging strategy for node-positive rectal cancer has been proposed.[17]
Table 1. Definitions of TNM Stage 0a
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
0
Tis, N0, M0
Tis = Carcinoma in situ, intramucosal carcinoma (involvement of lamina propria with no extension through muscularis mucosae).
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 2. Definitions of TNM Stage Ia
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
I
T1–T2, N0, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 3. Definitions of TNM Stages IIA, IIB, and IICa
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
IIA
T3, N0, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIB
T4a, N0, M0
T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N0 = No regional lymph node metastasis.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIC
T4b, N0, M0
T4b = Tumor directly invades or adheres to adjacent organs or structures.
N0 = No regional lymph node metastasis.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 4. Definitions of TNM Stages IIIA, IIIB, and IIICa
Stage
TNMb,c
Description
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
The explanations for superscripts b and c are at the end of Table 5.
IIIA
T1, N2a, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T1–2, N1/N1c, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
T2 = Tumor invades the muscularis propria.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIIB
T1–T2, N2b, M0
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T2–T3, N2a, M0
T2 = Tumor invades the muscularis propria.
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T3–T4a, N1/N1c, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
IIIC
T3–T4a, N2b, M0
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T4a, N2a, M0
T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
N2a = Four to six regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
T4b, N1–N2, M0
T4b = Tumor directly invades or adheres to adjacent organs or structures.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1a = One regional lymph node is positive.
–N1b = Two or three regional lymph nodes are positive.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
N2 = Four or more regional nodes are positive.
–N2a = Four to six regional lymph nodes are positive.
–N2b = Seven or more regional lymph nodes are positive.
M0 = No distant metastasis by imaging, etc.; no evidence of tumor in distant sites or organs. (This category is not assigned by pathologists.)
Table 5. Definitions of TNM Stages IVA, IVB, and IVCa
Stage
TNMb,c
Definition
Illustration
T = primary tumor; N = regional lymph nodes; M = distant metastasis.
aReprinted with permission from AJCC: Colon and rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp 251–74.
b Direct invasion in T4 includes invasion of other organs or other segments of the colorectum as a result of direct extension through the serosa, as confirmed on microscopic examination (e.g., invasion of the sigmoid colon by a carcinoma of the cecum) or, for cancers in a retroperitoneal or subperitoneal location, direct invasion of other organs or structures by virtue of extension beyond the muscularis propria (i.e., respectively, a tumor on the posterior wall of the descending colon invading the left kidney or lateral abdominal wall; or a mid or distal rectal cancer with invasion of prostate, seminal vesicles, cervix, or vagina).
cTumor that is adherent to other organs or structures, grossly, is classified cT4b. However, if no tumor is present in the adhesion, microscopically, the classification should be pT1-4a depending on the anatomical depth of wall invasion. The V and L classification should be used to identify the presence or absence of vascular or lymphatic invasion whereas the PN prognostic factor should be used for perineural invasion.
Tis = Carcinoma in situ, intramucosal carcinoma (involvement of lamina propria with no extension through muscularis mucosae).
T1 = Tumor invades the submucosa (through the muscularis mucosa but not into the muscularis propria).
T2 = Tumor invades the muscularis propria.
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4 = Tumor invades the visceral peritoneum or invades or adheres to adjacent organ or structure.
–T4a = Tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).
–T4b = Tumor directly invades or adheres to adjacent organs or structures.
NX = Regional lymph nodes cannot be assessed.
N0 = No regional lymph node metastasis.
N1 = One to three regional lymph nodes are positive (tumor in lymph nodes measuring ≥0.2 mm), or any number of tumor deposits are present and all identifiable lymph nodes are negative.
–N1a = One regional lymph node is positive.
–N1b = Two or three regional lymph nodes are positive.
–N1c = No regional lymph nodes are positive, but there are tumor deposits in the subserosa, mesentery, or nonperitonealized pericolic, or perirectal/mesorectal tissues.
N2 = Four or more regional nodes are positive.
–N2a = Four to six regional lymph nodes are positive.
–N2b = Seven or more regional lymph nodes are positive.
M1a = Metastasis to one site or organ is identified without peritoneal metastasis.
IVB
Any T, Any N, M1b
Any T = See T descriptions above in Any T, Any N, M1a TNM stage group.
Any N = See N descriptions above in Any T, Any N1, M1a TNM stage group.
M1b = Metastasis to two or more sites or organs is identified without peritoneal metastasis.
IVC
Any T, Any N, M1c
Any T = See T descriptions above in Any T, Any N, M1a TNM stage group.
Any N = See N descriptions above in Any T, Any N1, M1a TNM stage group.
M1c = Metastasis to the peritoneal surface is identified alone or with other site or organ metastases.
References
Schmidt CR, Gollub MJ, Weiser MR: Contemporary imaging for colorectal cancer. Surg Oncol Clin N Am 16 (2): 369-88, 2007. [PUBMED Abstract]
Siddiqui AA, Fayiga Y, Huerta S: The role of endoscopic ultrasound in the evaluation of rectal cancer. Int Semin Surg Oncol 3: 36, 2006. [PUBMED Abstract]
Søreide K: Molecular testing for microsatellite instability and DNA mismatch repair defects in hereditary and sporadic colorectal cancers–ready for prime time? Tumour Biol 28 (5): 290-300, 2007. [PUBMED Abstract]
Zammit M, Jenkins JT, Urie A, et al.: A technically difficult endorectal ultrasound is more likely to be inaccurate. Colorectal Dis 7 (5): 486-91, 2005. [PUBMED Abstract]
Libutti SK, Willett CG, Saltz LB: Cancer of the rectum. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Lippincott Williams & Wilkins, 2011, pp 1127-41.
Goldstein MJ, Mitchell EP: Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Invest 23 (4): 338-51, 2005. [PUBMED Abstract]
Das P, Skibber JM, Rodriguez-Bigas MA, et al.: Predictors of tumor response and downstaging in patients who receive preoperative chemoradiation for rectal cancer. Cancer 109 (9): 1750-5, 2007. [PUBMED Abstract]
Lahaye MJ, Engelen SM, Nelemans PJ, et al.: Imaging for predicting the risk factors–the circumferential resection margin and nodal disease–of local recurrence in rectal cancer: a meta-analysis. Semin Ultrasound CT MR 26 (4): 259-68, 2005. [PUBMED Abstract]
Balch GC, De Meo A, Guillem JG: Modern management of rectal cancer: a 2006 update. World J Gastroenterol 12 (20): 3186-95, 2006. [PUBMED Abstract]
Compton CC, Greene FL: The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin 54 (6): 295-308, 2004 Nov-Dec. [PUBMED Abstract]
Jessup J, Benson A, Chen V: Colon and Rectum. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp 251–74.
Nelson H, Petrelli N, Carlin A, et al.: Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst 93 (8): 583-96, 2001. [PUBMED Abstract]
Swanson RS, Compton CC, Stewart AK, et al.: The prognosis of T3N0 colon cancer is dependent on the number of lymph nodes examined. Ann Surg Oncol 10 (1): 65-71, 2003 Jan-Feb. [PUBMED Abstract]
Le Voyer TE, Sigurdson ER, Hanlon AL, et al.: Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol 21 (15): 2912-9, 2003. [PUBMED Abstract]
Prandi M, Lionetto R, Bini A, et al.: Prognostic evaluation of stage B colon cancer patients is improved by an adequate lymphadenectomy: results of a secondary analysis of a large scale adjuvant trial. Ann Surg 235 (4): 458-63, 2002. [PUBMED Abstract]
Tepper JE, O’Connell MJ, Niedzwiecki D, et al.: Impact of number of nodes retrieved on outcome in patients with rectal cancer. J Clin Oncol 19 (1): 157-63, 2001. [PUBMED Abstract]
Greene FL, Stewart AK, Norton HJ: New tumor-node-metastasis staging strategy for node-positive (stage III) rectal cancer: an analysis. J Clin Oncol 22 (10): 1778-84, 2004. [PUBMED Abstract]
Treatment Option Overview for Rectal Cancer
The management of rectal cancer varies somewhat from that of colon cancer because of the increased risk of local recurrence and a poorer overall prognosis. Differences include surgical technique, the use of radiation therapy, and the method of chemotherapy administration. In addition to determining the intent of rectal cancer surgery (i.e., curative or palliative), it is important to consider therapeutic issues related to the maintenance or restoration of normal anal sphincter, genitourinary function, and sexual function.[1,2]
The approach to the management of rectal cancer is multimodal and involves a multidisciplinary team of cancer specialists with expertise in gastroenterology, medical oncology, surgical oncology, radiation oncology, and radiology.
Among patients with rectal adenocarcinomas, 5% to 10% of the tumors have mismatch repair deficiency or high microsatellite instability. Immune checkpoint inhibitors are efficacious as a first-line therapy for metastatic colorectal cancers, with overall response rates of 30% to 60%.[3–5] These responses proved durable, and prolonged overall survival (OS) was demonstrated in these settings.
Evidence (immunotherapy):
A phase II trial (NCT04165772) studied dostarlimab, an anti-programmed death-1 (PD-1) monoclonal antibody, in 12 patients with locally advanced, mismatch repair–deficient, stage II or stage III rectal adenocarcinoma.[6]
All 12 patients had clinical complete responses of 100% (95% confidence interval [CI], 74%–100%) after a median follow-up of 12 months. Patients’ cancers did not recur when the follow-up period ranged from 6 to 25 months. At the time of follow-up, chemoradiation therapy and surgery had been avoided.[6][Level of evidence C3]
Before this approach becomes a new standard, more patients need to be evaluated. A longer follow-up period is required to ensure durability and assess the need for future surgery or chemoradiation therapy.
Primary Surgical Therapy
The primary treatment for patients with rectal cancer is surgical resection of the primary tumor. The surgical approach to treatment varies according to:
Tumor location.
Stage of disease.
Presence or absence of high-risk features (i.e., positive margins, lymphovascular invasion, perineural invasion, and poorly differentiated histology).
Transanal local excision and transanal endoscopic microsurgery for select clinically staged T1/T2, N0 rectal cancers.
Total mesorectal excision with autonomic nerve preservation techniques via low-anterior resection.
Total mesorectal excision via abdominoperineal resection for patients who are not candidates for sphincter-preservation, leaving patients with a permanent end-colostomy.
Polypectomy alone may be used in certain instances (T1) in which polyps with invasive cancer can be completely resected with clear margins and have favorable histological features.[8,9]
Local excision of clinical T1 tumors is an acceptable surgical technique for appropriately selected patients. For all other tumors, a mesorectal excision is the treatment of choice. Very select patients with T2 tumors may be candidates for local excision. Local failure rates in the range of 4% to 8% after rectal resection with appropriate mesorectal excision (total mesorectal excision for low/middle rectal tumors and mesorectal excision at least 5 cm below the tumor for high rectal tumors) have been reported.[10–14]
For patients with advanced cancers of the mid- to upper rectum, low-anterior resection followed by the creation of a colorectal anastomosis may be the treatment of choice. For locally advanced rectal cancers for which radical resection is indicated, however, total mesorectal excision with autonomic nerve preservation techniques via low-anterior resection is preferable to abdominoperineal resection.[1,2]
The low incidence of local relapse after meticulous mesorectal excision has led some investigators to question the routine use of adjuvant radiation therapy. Because of an increased tendency for first failure in locoregional sites only, the impact of perioperative radiation therapy is greater in rectal cancer than in colon cancer.[15]
Chemoradiation Therapy
Preoperative chemoradiation therapy
Neoadjuvant therapy for rectal cancer, using preoperative chemoradiation therapy, is the preferred treatment option for patients with stages II and III disease. However, postoperative chemoradiation therapy for patients with stage II or III rectal cancer remains an acceptable option.[16][Level of evidence A1] Total neoadjuvant therapy (chemotherapy followed by [chemo]radiation or [chemo]radiation followed by chemotherapy) is also an option.
Preoperative chemoradiation therapy has become the standard of care for patients with clinically staged T3–T4 or node-positive disease (stages II/III), based on the results of several studies:
Multiple phase II and III studies examined the benefits of preoperative chemoradiation therapy, which include:[16]
Tumor regression and downstaging of the tumor.
Improved tumor resectability.
Higher rate of local control.
Improved toxicity profile of chemoradiation therapy.
Higher rate of sphincter preservation.
Complete pathological response rates of 10% to 25% may be achieved with preoperative chemoradiation therapy.[19–26] However, preoperative radiation therapy is associated with increased complications compared with surgery alone. Some patients with cancers at a lower risk of local recurrence might be adequately treated with surgery and adjuvant chemotherapy.[27–30] For more information about these studies, see the Preoperative chemoradiation therapy section in the Treatment of Stages II and III Rectal Cancer section.
Postoperative chemoradiation therapy
Preoperative chemoradiation therapy is the current standard of care for stages II and III rectal cancer. However, before 1990, the following studies noted an increase in both disease-free survival (DFS) and OS with the use of postoperative combined-modality therapy:
The Gastrointestinal Tumor Study Group trial (GITSG-7175).
The Mayo/North Central Cancer Treatment Group trial (NCCTG-794751).
The National Surgical Adjuvant Breast and Bowel Project trial (NSABP-R-01).
Subsequent studies have attempted to increase the survival benefit by improving radiation sensitization and by identifying the optimal chemotherapeutic agents and delivery systems.
Fluorouracil (5-FU): The following studies examined optimal delivery methods for adjuvant 5-FU:
Acceptable postoperative chemoradiation therapy for patients with stage II or III rectal cancer not enrolled in clinical trials includes continuous-infusion 5-FU during 45 Gy to 55 Gy pelvic radiation and four cycles of adjuvant maintenance chemotherapy with bolus 5-FU with or without modulation with leucovorin (LV).
Findings from the NSABP-R-01 trial compared surgery alone with surgery followed by chemotherapy or radiation therapy.[33] Subsequently, the NSABP-R-02 study (NCT00410579), addressed whether adding postoperative radiation therapy to chemotherapy would enhance the survival advantage reported in R-01.[34][Level of evidence A1]
In the NSABP-R-02 study, the addition of radiation therapy significantly reduced local recurrence at 5 years (8% for chemotherapy and radiation vs. 13% for chemotherapy alone, P = .02) but failed to demonstrate a significant survival benefit. Radiation therapy appeared to improve survival among patients younger than 60 years and among patients who underwent abdominoperineal resection.
While this trial has initiated discussion in the oncologic community about the proper role of postoperative radiation therapy, omission of radiation therapy seems premature because of the serious complications of locoregional recurrence.
Chemotherapy regimens
Table 7 describes the chemotherapy regimens used to treat rectal cancer.
Table 7. Drug Combinations Used to Treat Rectal Cancer
Regimen Name
Drug Combination
Dose
5-FU = fluorouracil; AIO = Arbeitsgemeinschaft Internistische Onkologie; bid = twice a day; IV = intravenous; LV = leucovorin.
AIO or German AIO
LV, 5-FU, and irinotecan
Irinotecan (100 mg/m2) and LV (500 mg/m2) administered as 2-h infusions on d 1, followed by 5-FU (2,000 mg/m2) IV bolus administered via ambulatory pump weekly over 24 h, 4 times a y (52 wk).
CAPOX
Capecitabine and oxaliplatin
Capecitabine (1,000 mg/m2) bid on d 1–14, plus oxaliplatin (70 mg/m2) on d 1 and 8 every 3 wk.
Douillard
LV, 5-FU, and irinotecan
Irinotecan (180 mg/m2) administered as a 2-h infusion on d 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2.
FOLFIRI
LV, 5-FU, and irinotecan
Irinotecan (180 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus administered on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk.
FOLFOX4
Oxaliplatin, LV, and 5-FU
Oxaliplatin (85 mg/m2) administered as a 2-h infusion on day 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2.
FOLFOX6
Oxaliplatin, LV, and 5-FU
Oxaliplatin (85–100 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk.
FOLFOXIRI
Irinotecan, oxaliplatin, LV, 5-FU
Irinotecan (165 mg/m2) administered as a 60-min infusion, then concomitant infusion of oxaliplatin (85 mg/m2) and LV (200 mg/m2) over 120 min, followed by 5-FU (3,200 mg/m2) administered as a 48-h continuous infusion.
FUFOX
5-FU, LV, and oxaliplatin
Oxaliplatin (50 mg/m2) plus LV (500 mg/m2) plus 5-FU (2,000 mg/m2) administered as a 22-h continuous infusion on d 1, 8, 22, and 29 every 36 d.
FUOX
5-FU plus oxaliplatin
5-FU (2,250 mg/m2) administered as a continuous infusion over 48 h on d 1, 8, 15, 22, 29, and 36 plus oxaliplatin (85 mg/m2) on d 1, 15, and 29 every 6 wk.
IFL (or Saltz)
Irinotecan, 5-FU, and LV
Irinotecan (125 mg/m2) plus 5-FU (500 mg/m2) IV bolus and LV (20 mg/m2) IV bolus administered weekly for 4 out of 6 wk.
XELOX
Capecitabine plus oxaliplatin
Oral capecitabine (1,000 mg/m2) administered bid for 14 d plus oxaliplatin (130 mg/m2) on d 1 every 3 wk.
Total neoadjuvant therapy
Data support giving all radiation therapy and chemotherapy neoadjuvantly.
The RAPIDO trial (NCT01558921) randomly assigned 920 patients to receive either short-course radiation therapy followed by six cycles of CAPOX (capecitabine and oxaliplatin) or nine cycles of FOLFOX (LV, 5-FU, and oxaliplatin) followed by surgery, or long-course chemoradiation therapy followed by surgery with the option to add adjuvant chemotherapy. The primary end point was 3-year disease-related treatment failure (defined as first occurrence of locoregional failure, distant metastasis, new primary colorectal tumor, or treatment-related death). The 3-year disease-related treatment failure rate was 23.7% (95% CI, 19.8%–27.6%) in the short-course radiation therapy group and 30.4% (95% CI, 26.1%–34.6%) in the long-course chemoradiation therapy group (hazard ratio [HR], 0.75; 95% CI, 0.60–0.95; P = .019).[35][Level of evidence B1]
In the randomized, phase III, French UNICANCER-PRODIGE 23 study (NCT01804790), 461 patients were randomly assigned to receive either six cycles of FOLFIRINOX (LV, 5-FU, irinotecan, and oxaliplatin) followed by chemoradiation therapy (experimental group) or chemoradiation therapy (standard-of-care group). Patients in both groups underwent total mesorectal excision. This was not fully a total neoadjuvant therapy trial as both groups also received adjuvant chemotherapy with modified FOLFOX or capecitabine for 3 months (experimental group) or 6 months (standard-of-care group). The 3-year DFS rate was 76% (95% CI, 69%–81%) in the experimental group and 69% (95% CI, 62%–74%) in the standard-of-care group (stratified HR, 0.69; 95% CI, 0.49–0.97; P = .034).[36][Level of evidence B1]
The total neoadjuvant approach was studied in clinical trials because data showed that many patients do not receive all of the recommended chemotherapy when given after surgery. For example, in the OPRA trial (NCT02008656), which used a total neoadjuvant therapy approach, approximately 85% of patients received all of the recommended chemotherapy, an improvement in adherence over trials that used adjuvant chemotherapy. Another potential benefit of this approach is that it allows more patients to receive nonoperative management (also known as the watch-and-wait approach), which is described in more detail below. This approach may interest patients who would otherwise require an abdominoperineal resection, which results in the need for lifelong stoma.[37,38][Level of evidence B1]
Select patients with locally advanced rectal cancer may omit radiation therapy if they receive escalated chemotherapy, but they would still need a total mesorectal excision. In the PROSPECT trial (NCT01515787), 1,194 patients were randomly assigned to receive either neoadjuvant FOLFOX chemotherapy (with chemoradiation therapy only given if the primary tumor decreased in size by <20% or if FOLFOX was discontinued because of side effects) or standard neoadjuvant chemoradiation therapy. All patients then underwent surgery and had the option to receive adjuvant FOLFOX (four or six cycles for the neoadjuvant chemotherapy group and eight cycles for the neoadjuvant chemoradiation therapy group). The study population included patients with T2, node-positive; T3, N0; or T3, node-positive disease who were eligible for sphincter-sparing surgery (thus, excluding most patients with low-rectal tumors). This study found that the omission of radiation therapy was possible in select patients without compromising oncologic outcomes based on a noninferiority study design. It should be noted that in Europe, many patients with T3, N0 disease do not undergo any neoadjuvant therapy prior to resection. Omission of radiation is beneficial for patients desiring to preserve fertility.[39]
Total neoadjuvant therapy is currently the preferred approach for most patients with locally advanced rectal cancer without distant metastases.
Treatment toxicity
The acute side effects of pelvic radiation therapy for rectal cancer are mainly the result of gastrointestinal toxicity, are self-limiting, and usually resolve within 4 to 6 weeks of completing treatment.
Of greater concern is the potential for late morbidity after rectal cancer treatment. Patients who undergo aggressive surgical procedures for rectal cancer can have chronic symptoms, particularly if there is impairment of the anal sphincter.[40] Patients treated with radiation therapy appear to have increased chronic bowel dysfunction, anorectal sphincter dysfunction (if the sphincter was surgically preserved), and sexual dysfunction than do patients who undergo surgical resection alone.[28,41–46]
An analysis of patients treated with postoperative chemotherapy and radiation therapy suggests that these patients may have more chronic bowel dysfunction than do patients who undergo surgical resection alone.[47] A Cochrane review highlights the risks of increased surgical morbidity as well as late rectal and sexual function in association with radiation therapy.[40]
Improved radiation therapy planning and techniques may minimize these acute and late treatment-related complications. These techniques include:[48–52]
The use of high-energy radiation machines.
The use of multiple pelvic radiation fields.
Prone patient positioning.
Customized patient molds (belly boards) to exclude as much small bowel as possible from the radiation fields and immobilize patients during treatment.
Bladder distention during radiation therapy to exclude as much small bowel as possible from the radiation fields.
Visualization of the small bowel through oral contrast during treatment planning so that, when possible, the small bowel can be excluded from the radiation field.
The use of 3-dimensional or other advanced radiation planning techniques.
Long-course versus short-course radiation therapy
There are two approaches commonly used for radiation therapy:
Long-course chemoradiation therapy (generally to doses of 50.4–54 Gy), commonly given with concurrent capecitabine or 5-FU/LV.
Short-course radiation therapy (25 Gy in five fractions), generally given without chemotherapy.
In Europe, preoperative radiation therapy is commonly delivered alone in 1 week (5 Gy × five daily treatments) followed by surgery one week later, rather than the long-course chemoradiation therapy approach used in the United States. One reason for this difference is the concern in the United States for heightened late effects when high radiation doses per fraction are given.
A Polish study randomly assigned 316 patients to receive either preoperative long-course chemoradiation therapy (50.4 Gy in 28 daily fractions with 5-FU/LV) or short-course preoperative radiation therapy (25 Gy in five fractions).[46] Although the primary end point was sphincter preservation, late toxicity was not statistically significantly different between the two treatment approaches (7% for the long-course group vs. 10% for the short-course group). Of note, data on anal sphincter and sexual function were not reported, and toxicity was determined by the physician, not patient reported.
The choice of long-course versus short-course radiation therapy for rectal cancer is an area of active study, and it is not known which is superior. Generally, long-course chemoradiation therapy results in a higher biologically equivalent dose being delivered to the patient (along with chemosensitization, most commonly with capecitabine or 5-FU), which would theoretically result in improved local control. This is supported by the RAPIDO trial, where a higher local recurrence rate was seen in the patients who received short-course radiation therapy rather than those who received long-course chemoradiation therapy.[35]
Alternatively, short-course radiation therapy requires a shorter break from stronger systemic therapy. Therefore, if a patient is at a relatively higher risk of local recurrence than distant recurrence, long-course chemoradiation therapy may be preferred, but if the patient is at a higher risk of distant recurrence, short-course therapy may be preferred to allow a quicker return to chemotherapy. Many physicians also do not offer short-course chemoradiation therapy when a nonoperative management approach is used, as it has not been studied, and given the potentially lower local control rates due to the lower biologically equivalent dose as compared with long-course chemoradiation therapy. The optimal sequencing of radiation therapy and chemotherapy when given as a part of total neoadjuvant therapy is still being evaluated. There are also some clinical situations where short-course radiation therapy may not be preferred, such as when a rectal stent is present (which may result in greater rectal toxicity).
Capecitabine and fluorouracil dosing
The DPYD gene encodes an enzyme that catabolizes pyrimidines and fluoropyrimidines, like capecitabine and fluorouracil. An estimated 1% to 2% of the population has germline pathogenic variants in DPYD, which lead to reduced DPD protein function and an accumulation of pyrimidines and fluoropyrimidines in the body.[53,54] Patients with the DPYD*2A variant who receive fluoropyrimidines may experience severe, life-threatening toxicities that are sometimes fatal. Many other DPYD variants have been identified, with a range of clinical effects.[53–55] Fluoropyrimidine avoidance or a dose reduction of 50% may be recommended based on the patient’s DPYD genotype and number of functioning DPYD alleles.[56–58] DPYD genetic testing costs less than $200, but insurance coverage varies due to a lack of national guidelines.[59] In addition, testing may delay therapy by 2 weeks, which would not be advisable in urgent situations. This controversial issue requires further evaluation.[60]
References
Balch GC, De Meo A, Guillem JG: Modern management of rectal cancer: a 2006 update. World J Gastroenterol 12 (20): 3186-95, 2006. [PUBMED Abstract]
Baxter NN, Garcia-Aguilar J: Organ preservation for rectal cancer. J Clin Oncol 25 (8): 1014-20, 2007. [PUBMED Abstract]
Le DT, Uram JN, Wang H, et al.: PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 372 (26): 2509-20, 2015. [PUBMED Abstract]
Overman MJ, Lonardi S, Wong KYM, et al.: Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol 36 (8): 773-779, 2018. [PUBMED Abstract]
André T, Shiu KK, Kim TW, et al.: Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med 383 (23): 2207-2218, 2020. [PUBMED Abstract]
Cercek A, Lumish M, Sinopoli J, et al.: PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N Engl J Med 386 (25): 2363-2376, 2022. [PUBMED Abstract]
Guillem JG, Cohen AM: Current issues in colorectal cancer surgery. Semin Oncol 26 (5): 505-13, 1999. [PUBMED Abstract]
Seitz U, Bohnacker S, Seewald S, et al.: Is endoscopic polypectomy an adequate therapy for malignant colorectal adenomas? Presentation of 114 patients and review of the literature. Dis Colon Rectum 47 (11): 1789-96; discussion 1796-7, 2004. [PUBMED Abstract]
Enker WE, Thaler HT, Cranor ML, et al.: Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg 181 (4): 335-46, 1995. [PUBMED Abstract]
Zaheer S, Pemberton JH, Farouk R, et al.: Surgical treatment of adenocarcinoma of the rectum. Ann Surg 227 (6): 800-11, 1998. [PUBMED Abstract]
Heald RJ, Smedh RK, Kald A, et al.: Abdominoperineal excision of the rectum–an endangered operation. Norman Nigro Lectureship. Dis Colon Rectum 40 (7): 747-51, 1997. [PUBMED Abstract]
Lopez-Kostner F, Lavery IC, Hool GR, et al.: Total mesorectal excision is not necessary for cancers of the upper rectum. Surgery 124 (4): 612-7; discussion 617-8, 1998. [PUBMED Abstract]
Gunderson LL, Sosin H: Areas of failure found at reoperation (second or symptomatic look) following “curative surgery” for adenocarcinoma of the rectum. Clinicopathologic correlation and implications for adjuvant therapy. Cancer 34 (4): 1278-92, 1974. [PUBMED Abstract]
Sauer R, Becker H, Hohenberger W, et al.: Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351 (17): 1731-40, 2004. [PUBMED Abstract]
Sauer R, Liersch T, Merkel S, et al.: Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol 30 (16): 1926-33, 2012. [PUBMED Abstract]
Roh MS, Colangelo LH, O’Connell MJ, et al.: Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol 27 (31): 5124-30, 2009. [PUBMED Abstract]
Janjan NA, Khoo VS, Abbruzzese J, et al.: Tumor downstaging and sphincter preservation with preoperative chemoradiation in locally advanced rectal cancer: the M. D. Anderson Cancer Center experience. Int J Radiat Oncol Biol Phys 44 (5): 1027-38, 1999. [PUBMED Abstract]
Crane CH, Skibber JM, Birnbaum EH, et al.: The addition of continuous infusion 5-FU to preoperative radiation therapy increases tumor response, leading to increased sphincter preservation in locally advanced rectal cancer. Int J Radiat Oncol Biol Phys 57 (1): 84-9, 2003. [PUBMED Abstract]
Grann A, Minsky BD, Cohen AM, et al.: Preliminary results of preoperative 5-fluorouracil, low-dose leucovorin, and concurrent radiation therapy for clinically resectable T3 rectal cancer. Dis Colon Rectum 40 (5): 515-22, 1997. [PUBMED Abstract]
Rich TA, Skibber JM, Ajani JA, et al.: Preoperative infusional chemoradiation therapy for stage T3 rectal cancer. Int J Radiat Oncol Biol Phys 32 (4): 1025-9, 1995. [PUBMED Abstract]
Chari RS, Tyler DS, Anscher MS, et al.: Preoperative radiation and chemotherapy in the treatment of adenocarcinoma of the rectum. Ann Surg 221 (6): 778-86; discussion 786-7, 1995. [PUBMED Abstract]
Hyams DM, Mamounas EP, Petrelli N, et al.: A clinical trial to evaluate the worth of preoperative multimodality therapy in patients with operable carcinoma of the rectum: a progress report of National Surgical Breast and Bowel Project Protocol R-03. Dis Colon Rectum 40 (2): 131-9, 1997. [PUBMED Abstract]
Bosset JF, Magnin V, Maingon P, et al.: Preoperative radiochemotherapy in rectal cancer: long-term results of a phase II trial. Int J Radiat Oncol Biol Phys 46 (2): 323-7, 2000. [PUBMED Abstract]
Hiotis SP, Weber SM, Cohen AM, et al.: Assessing the predictive value of clinical complete response to neoadjuvant therapy for rectal cancer: an analysis of 488 patients. J Am Coll Surg 194 (2): 131-5; discussion 135-6, 2002. [PUBMED Abstract]
Lai LL, Fuller CD, Kachnic LA, et al.: Can pelvic radiotherapy be omitted in select patients with rectal cancer? Semin Oncol 33 (6 Suppl 11): S70-4, 2006. [PUBMED Abstract]
Peeters KC, van de Velde CJ, Leer JW, et al.: Late side effects of short-course preoperative radiotherapy combined with total mesorectal excision for rectal cancer: increased bowel dysfunction in irradiated patients–a Dutch colorectal cancer group study. J Clin Oncol 23 (25): 6199-206, 2005. [PUBMED Abstract]
Tepper JE, O’Connell M, Niedzwiecki D, et al.: Adjuvant therapy in rectal cancer: analysis of stage, sex, and local control–final report of intergroup 0114. J Clin Oncol 20 (7): 1744-50, 2002. [PUBMED Abstract]
Gunderson LL, Sargent DJ, Tepper JE, et al.: Impact of T and N stage and treatment on survival and relapse in adjuvant rectal cancer: a pooled analysis. J Clin Oncol 22 (10): 1785-96, 2004. [PUBMED Abstract]
O’Connell MJ, Martenson JA, Wieand HS, et al.: Improving adjuvant therapy for rectal cancer by combining protracted-infusion fluorouracil with radiation therapy after curative surgery. N Engl J Med 331 (8): 502-7, 1994. [PUBMED Abstract]
Smalley SR, Benedetti JK, Williamson SK, et al.: Phase III trial of fluorouracil-based chemotherapy regimens plus radiotherapy in postoperative adjuvant rectal cancer: GI INT 0144. J Clin Oncol 24 (22): 3542-7, 2006. [PUBMED Abstract]
Fisher B, Wolmark N, Rockette H, et al.: Postoperative adjuvant chemotherapy or radiation therapy for rectal cancer: results from NSABP protocol R-01. J Natl Cancer Inst 80 (1): 21-9, 1988. [PUBMED Abstract]
Wolmark N, Wieand HS, Hyams DM, et al.: Randomized trial of postoperative adjuvant chemotherapy with or without radiotherapy for carcinoma of the rectum: National Surgical Adjuvant Breast and Bowel Project Protocol R-02. J Natl Cancer Inst 92 (5): 388-96, 2000. [PUBMED Abstract]
Bahadoer RR, Dijkstra EA, van Etten B, et al.: Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. Lancet Oncol 22 (1): 29-42, 2021. [PUBMED Abstract]
Conroy T, Bosset JF, Etienne PL, et al.: Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 22 (5): 702-715, 2021. [PUBMED Abstract]
Verheij FS, Omer DM, Williams H, et al.: Long-Term Results of Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J Clin Oncol 42 (5): 500-506, 2024. [PUBMED Abstract]
Garcia-Aguilar J, Patil S, Gollub MJ, et al.: Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy. J Clin Oncol 40 (23): 2546-2556, 2022. [PUBMED Abstract]
Schrag D, Weiser M, Saltz L, et al.: Challenges and solutions in the design and execution of the PROSPECT Phase II/III neoadjuvant rectal cancer trial (NCCTG N1048/Alliance). Clin Trials 16 (2): 165-175, 2019. [PUBMED Abstract]
Wong RK, Tandan V, De Silva S, et al.: Pre-operative radiotherapy and curative surgery for the management of localized rectal carcinoma. Cochrane Database Syst Rev (2): CD002102, 2007. [PUBMED Abstract]
Randomised trial of surgery alone versus surgery followed by radiotherapy for mobile cancer of the rectum. Medical Research Council Rectal Cancer Working Party. Lancet 348 (9042): 1610-4, 1996. [PUBMED Abstract]
Initial report from a Swedish multicentre study examining the role of preoperative irradiation in the treatment of patients with resectable rectal carcinoma. Swedish Rectal Cancer Trial. Br J Surg 80 (10): 1333-6, 1993. [PUBMED Abstract]
Dahlberg M, Glimelius B, Graf W, et al.: Preoperative irradiation affects functional results after surgery for rectal cancer: results from a randomized study. Dis Colon Rectum 41 (5): 543-9; discussion 549-51, 1998. [PUBMED Abstract]
Birgisson H, Påhlman L, Gunnarsson U, et al.: Adverse effects of preoperative radiation therapy for rectal cancer: long-term follow-up of the Swedish Rectal Cancer Trial. J Clin Oncol 23 (34): 8697-705, 2005. [PUBMED Abstract]
Marijnen CA, van de Velde CJ, Putter H, et al.: Impact of short-term preoperative radiotherapy on health-related quality of life and sexual functioning in primary rectal cancer: report of a multicenter randomized trial. J Clin Oncol 23 (9): 1847-58, 2005. [PUBMED Abstract]
Bujko K, Nowacki MP, Nasierowska-Guttmejer A, et al.: Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg 93 (10): 1215-23, 2006. [PUBMED Abstract]
Kollmorgen CF, Meagher AP, Wolff BG, et al.: The long-term effect of adjuvant postoperative chemoradiotherapy for rectal carcinoma on bowel function. Ann Surg 220 (5): 676-82, 1994. [PUBMED Abstract]
Martling A, Holm T, Johansson H, et al.: The Stockholm II trial on preoperative radiotherapy in rectal carcinoma: long-term follow-up of a population-based study. Cancer 92 (4): 896-902, 2001. [PUBMED Abstract]
Dahlberg M, Glimelius B, Påhlman L: Improved survival and reduction in local failure rates after preoperative radiotherapy: evidence for the generalizability of the results of Swedish Rectal Cancer Trial. Ann Surg 229 (4): 493-7, 1999. [PUBMED Abstract]
Guerrero Urbano MT, Henrys AJ, Adams EJ, et al.: Intensity-modulated radiotherapy in patients with locally advanced rectal cancer reduces volume of bowel treated to high dose levels. Int J Radiat Oncol Biol Phys 65 (3): 907-16, 2006. [PUBMED Abstract]
Koelbl O, Richter S, Flentje M: Influence of patient positioning on dose-volume histogram and normal tissue complication probability for small bowel and bladder in patients receiving pelvic irradiation: a prospective study using a 3D planning system and a radiobiological model. Int J Radiat Oncol Biol Phys 45 (5): 1193-8, 1999. [PUBMED Abstract]
Gunderson LL, Russell AH, Llewellyn HJ, et al.: Treatment planning for colorectal cancer: radiation and surgical techniques and value of small-bowel films. Int J Radiat Oncol Biol Phys 11 (7): 1379-93, 1985. [PUBMED Abstract]
Sharma BB, Rai K, Blunt H, et al.: Pathogenic DPYD Variants and Treatment-Related Mortality in Patients Receiving Fluoropyrimidine Chemotherapy: A Systematic Review and Meta-Analysis. Oncologist 26 (12): 1008-1016, 2021. [PUBMED Abstract]
Lam SW, Guchelaar HJ, Boven E: The role of pharmacogenetics in capecitabine efficacy and toxicity. Cancer Treat Rev 50: 9-22, 2016. [PUBMED Abstract]
Shakeel F, Fang F, Kwon JW, et al.: Patients carrying DPYD variant alleles have increased risk of severe toxicity and related treatment modifications during fluoropyrimidine chemotherapy. Pharmacogenomics 22 (3): 145-155, 2021. [PUBMED Abstract]
Amstutz U, Henricks LM, Offer SM, et al.: Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clin Pharmacol Ther 103 (2): 210-216, 2018. [PUBMED Abstract]
Henricks LM, Lunenburg CATC, de Man FM, et al.: DPYD genotype-guided dose individualisation of fluoropyrimidine therapy in patients with cancer: a prospective safety analysis. Lancet Oncol 19 (11): 1459-1467, 2018. [PUBMED Abstract]
Lau-Min KS, Varughese LA, Nelson MN, et al.: Preemptive pharmacogenetic testing to guide chemotherapy dosing in patients with gastrointestinal malignancies: a qualitative study of barriers to implementation. BMC Cancer 22 (1): 47, 2022. [PUBMED Abstract]
Brooks GA, Tapp S, Daly AT, et al.: Cost-effectiveness of DPYD Genotyping Prior to Fluoropyrimidine-based Adjuvant Chemotherapy for Colon Cancer. Clin Colorectal Cancer 21 (3): e189-e195, 2022. [PUBMED Abstract]
Baker SD, Bates SE, Brooks GA, et al.: DPYD Testing: Time to Put Patient Safety First. J Clin Oncol 41 (15): 2701-2705, 2023. [PUBMED Abstract]
Treatment of Stage 0 Rectal Cancer
Treatment Options for Stage 0 Rectal Cancer
Stage 0 rectal cancer or carcinoma in situ is the most superficial of all rectal lesions and is limited to the mucosa without invasion of the lamina propria.
Treatment options for stage 0 rectal cancer include:
Local excision or simple polypectomy may be indicated for stage 0 rectal cancer tumors.[1] Because of its localized nature at presentation, stage 0 rectal cancer has a high cure rate. For large lesions not amenable to local excision, full-thickness rectal resection by the transanal or transcoccygeal route may be performed.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Bailey HR, Huval WV, Max E, et al.: Local excision of carcinoma of the rectum for cure. Surgery 111 (5): 555-61, 1992. [PUBMED Abstract]
Treatment of Stage I Rectal Cancer
Treatment Options for Stage I Rectal Cancer
Stage I tumors extend beneath the mucosa into the submucosa (T1) or into, but not through, the bowel muscle wall (T2). Because of its localized nature at presentation, stage I rectal cancer has a high cure rate.
Treatment options for stage I rectal cancer include:
There are three potential options for surgical resection in stage I rectal cancer:
Local excision. Local excision is restricted to tumors that are confined to the rectal wall and that do not, on rectal ultrasound or magnetic resonance imaging, involve the full thickness of the rectum (i.e., are not T3 tumors). The ideal candidate for local excision has a T1 tumor with well-to-moderate differentiation that occupies less than one-third of the circumference of the bowel wall. Local excision is associated with a higher risk of local and systemic failure and is applicable only to select patients with T2 tumors. Local transanal or other resection [1,2] with or without perioperative external-beam radiation therapy (EBRT) plus fluorouracil (5-FU) may be indicated.
Low-anterior resection. Wide surgical resection and anastomosis are options when an adequate low-anterior resection can be performed with sufficient distal rectum to allow a conventional anastomosis or coloanal anastomosis.
Abdominoperineal resection. Wide surgical resection with abdominoperineal resection is used for lesions too distal to permit low-anterior resection.
Patients with tumors that are pathologically T1 may not need postoperative therapy. Patients with tumors that are T2 or greater have lymph node involvement about 20% of the time. Patients may want to consider additional therapy, such as radiation therapy and chemotherapy, or wide surgical resection of the rectum.[3] Patients with poor histological features or positive margins after local excision may consider low-anterior resection or abdominoperineal resection and postoperative treatment as dictated by full surgical staging.
For patients with T1 and T2 tumors, no randomized trials are available to compare local excision with or without postoperative chemoradiation therapy to wide surgical resection (low-anterior resection and abdominoperineal resection).
Evidence (surgery):
Investigators with the Cancer and Leukemia Group B enrolled patients with T1 and T2 rectal adenocarcinomas that were within 10 cm of the dentate line and not more than 4 cm in diameter, and involving not more than 40% of the rectal circumference, onto a prospective protocol, CLB-8984. Patients with T1 tumors received no additional treatment after surgery, whereas patients with T2 tumors were treated with EBRT (54 Gy in 30 fractions, 5 days/week) and 5-FU (500 mg/m2 on days 1 through 2 and days 29 through 31 of radiation therapy).[4]
For patients with T1 tumors, at 48 months median follow-up, the 6-year failure-free survival (FFS) rate was 83%, and the overall survival (OS) rate was 87%.
For patients with T2 tumors, the 6-year FFS rate was 71%, and the OS rate was 85%.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Bailey HR, Huval WV, Max E, et al.: Local excision of carcinoma of the rectum for cure. Surgery 111 (5): 555-61, 1992. [PUBMED Abstract]
Benson R, Wong CS, Cummings BJ, et al.: Local excision and postoperative radiotherapy for distal rectal cancer. Int J Radiat Oncol Biol Phys 50 (5): 1309-16, 2001. [PUBMED Abstract]
Sitzler PJ, Seow-Choen F, Ho YH, et al.: Lymph node involvement and tumor depth in rectal cancers: an analysis of 805 patients. Dis Colon Rectum 40 (12): 1472-6, 1997. [PUBMED Abstract]
Steele GD, Herndon JE, Bleday R, et al.: Sphincter-sparing treatment for distal rectal adenocarcinoma. Ann Surg Oncol 6 (5): 433-41, 1999 Jul-Aug. [PUBMED Abstract]
Treatment of Stages II and III Rectal Cancer
Treatment Options for Stages II and III Rectal Cancer
Treatment options for stages II and III rectal cancer include:
Immunotherapy (for patients with mismatch repair deficiency or high microsatellite instability [MSI]).
Preoperative chemoradiation therapy
Preoperative chemoradiation therapy has become the standard of care for patients with clinically staged T3 or T4 or node-positive disease, based on the results of several studies. The results of one study affirm neoadjuvant FOLFOX (leucovorin [LV], fluorouracil [5-FU], and oxaliplatin) as an alternative to chemoradiation therapy for select patients with lower-risk disease.[1]
Evidence (preoperative chemoradiation therapy):
The German Rectal Cancer Study Group (CAO/ARO/AIO-94 [Working Group of Surgical Oncology/Working Group of Radiation Oncology/Working Group of Medical Oncology of the Germany Cancer Society]) randomly assigned 823 patients with ultrasound-staged T3 or T4 or lymph node-positive rectal cancer to either preoperative chemoradiation therapy or postoperative chemoradiation therapy (50.4 Gy in 28 daily fractions to the tumor and pelvic lymph nodes concurrent with infusional 5-FU 1,000 mg/m2 daily for 5 days during the first and fifth weeks of radiation therapy).[2][Level of evidence A1] All patients underwent total mesorectal excision and received four additional cycles of 5-FU–based chemotherapy.
The 5-year overall survival (OS) rates were 76% for preoperative chemoradiation therapy and 74% for postoperative chemoradiation therapy (P = .80). The 5-year cumulative incidence of local relapse was 6% for patients assigned to the preoperative chemoradiation therapy group and 13% for patients in the postoperative chemoradiation therapy group (P = .006).
Grade 3 or 4 acute toxic effects occurred in 27% of patients in the preoperative-treatment group and in 40% of patients in the postoperative-treatment group (P = .001). The corresponding rates of long-term toxic effects were 14% and 24%, respectively (P = .01).
The same number of patients underwent abdominoperineal resection in each arm. However, among the 194 patients with tumors that were determined by the surgeon before randomization to require an abdominoperineal excision, a statistically significant increase in sphincter preservation was achieved among patients who received preoperative chemoradiation therapy (P = .004). These results have now been updated with a median follow-up of 11 years.[3]
The 10-year OS was equivalent in both arms, (59.6% in the preoperative group vs. 59.9% in the postoperative group; P = .85). However, a local control benefit persists among patients treated with preoperative chemoradiation therapy compared with patients treated with postoperative chemoradiation therapy (10-year cumulative incidence of local relapse: 7.1% in the preoperative group vs. 10.1% in the postoperative group; P = .048). There were no significant differences detected for 10-year cumulative incidence of distant metastases or disease-free survival (DFS).[3]
Among the patients assigned to the postoperative chemoradiation therapy treatment arm, 18% actually had pathologically determined stage I disease and were overestimated by endorectal ultrasound to have T3 or T4 or N1 disease. A similar number of patients were possibly overtreated in the preoperative treatment group.
The NSABP R-03 trial (NCT00410579) similarly compared preoperative versus postoperative chemoradiation therapy for patients with clinically staged T3 or T4 or lymph node-positive rectal cancer. Chemotherapy consisted of 5-FU/LV with 45 Gy in 25 fractions with a 5.4 Gy boost. Although the intended sample size was 900 patients, the study with 267 patients closed early because of poor accrual.[4][Level of evidence A1]
With a median follow-up of 8.4 years, preoperative chemoradiation therapy was found to confer a significant improvement in 5-year DFS (64.7% vs. 53.4% for postoperative patients; P = .011).
Similar to the German Rectal Cancer Study, there was no significant difference in OS between treatment arms (74.5% for preoperative chemoradiation therapy vs. 65.6% for postoperative chemoradiation therapy; P =. 065).
Neoadjuvant chemotherapy with FOLFOX without preoperative chemoradiation therapy (for select patients with lower-risk disease)
Evidence (neoadjuvant chemotherapy with FOLFOX without preoperative chemoradiation therapy [for select patients with lower-risk disease]):
The PROSPECT trial (NCT01515787) included 1,194 patients with clinical T2, node-positive; T3, N0; or T3, node-positive rectal cancer who were candidates for sphincter-sparing surgery. A total of 1,128 patients were randomly assigned to receive either neoadjuvant FOLFOX (six cycles) or chemoradiation therapy.[1][Level of evidence B1]
Patients in the neoadjuvant FOLFOX group who had less than 20% clinical response upon restaging, or who were unable to tolerate at least five cycles of FOLFOX were selected to receive chemoradiation therapy. Neoadjuvant FOLFOX with only selective use of pelvic chemoradiation therapy was noninferior to up-front neoadjuvant pelvic chemoradiation therapy for DFS (hazard ratio [HR]disease recurrence or death, 0.92; 90.2% confidence interval [CI], 0.74–1.14; P = .005 for noninferiority).[1]
These results show that using six cycles of FOLFOX instead of neoadjuvant chemoradiation therapy is an acceptable option for this patient population, which is considered to represent potentially over one-half of all patients with locally advanced rectal cancer in the United States. Avoidance of chemoradiation therapy could potentially spare patients from long-term side effects, such as impairment in bowel, bladder and sexual function, increased risk of pelvic fractures and secondary malignancies, decreased bone marrow reserve, and fertility impacts.
Short-course preoperative radiation therapy followed by surgery and chemotherapy
The use of short-course radiation therapy before surgery has been a standard approach in parts of Europe and Australia.
The use of short-course radiation therapy was evaluated in a randomized study in the Swedish Rectal Cancer Trial (NCT00337545).[5][Level of evidence A1] In the trial, 1,168 patients younger than 80 years with stage I to stage III resectable rectal adenocarcinoma were randomly assigned to receive preoperative radiation therapy (25 Gy in five fractions) or to undergo immediate surgery. Patients did not receive adjuvant chemotherapy.
The 5-year OS rate was 58% in the radiation therapy group and 48% in the surgery group (P = .005).
The rate of local control was 11% in the radiation therapy group and 27% in the surgery group (P < .001).
Subsequently, the Polish Rectal Trial and the Trans-Tasman Radiation Oncology Group (TROG) compared short-course preoperative radiation therapy with the standard long-course preoperative chemoradiation therapy administered with 5-FU.
In the Polish Rectal Trial, 312 patients with clinical stage T3 or T4 rectal cancer were randomly assigned to receive preoperative radiation therapy (25 Gy in five fractions) followed by total mesorectal excision within 7 days, 6 months of adjuvant 5-FU/LV or preoperative chemoradiation therapy (50.4 Gy in 28 fractions with concurrent bolus 5-FU/LV), total mesorectal excision in 4 to 6 weeks after completion of radiation therapy, and 4 months of adjuvant 5-FU/LV.[6] The primary end point of the study was to detect a difference of at least 15% in sphincter preservation with a power of 80%.
The rates of sphincter preservation were 61.2% in the short-course group and 58% in the chemoradiation therapy group (P = .570).
The actuarial 4-year survival rate was 67.2% in the short-course group and 66.2% in the chemoradiation therapy group (HR, 1.01; 95% CI, 0.69–1.48; P = .960).
The HR for local recurrence in the short-course group compared with the chemoradiation therapy group was 0.65 (95% CI, 0.32–1.28; P = .210).
There was no difference in late toxicity between the short-course group and the chemoradiation therapy group.
In the TROG trial (TROG 01.04 [NCT00145769]), 326 patients with ultrasound-staged or magnetic resonance imaging (MRI)–staged T3, N0 to N2, M0 rectal adenocarcinoma within 12 cm from the anal verge were randomly assigned to receive short-course radiation therapy (25 Gy in five fractions) followed by surgery 3 to 7 days later or long-course chemoradiation therapy (50.4 Gy in 28 fractions with concurrent continuous infusional 5-FU) followed by surgery in 4 to 6 weeks. All patients received adjuvant chemotherapy (5-FU/LV) after surgery. The trial was designed to have 80% power to detect a 10% difference in local recurrence at 3 years with a two-sided test at the 5% level of significance.[7]
Cumulative incidence of local recurrence at 3 years was 7.5% for the short-course group and 4.4% for the long-course group (P = .24).
The OS rate at 5 years was 74% for the short-course group and 70% for the long-course group (HR, 1.12; 95% CI, 0.76–1.67; P = .62).
The Medical Research Council of the United Kingdom and the National Cancer Institute of Canada built on the short-course experience and conducted a randomized study (MRC CR07 and NCIC-CTG C016 [NCT00003422]) that compared short-course preoperative radiation therapy with selective postoperative chemoradiation therapy.[8] In the trial, 1,350 patients from 80 centers who had resectable rectal adenocarcinomas that were less than 15 cm from the anal verge were randomly assigned. Of note, pelvic MRI or ultrasound was not mandated. Patients randomly assigned to short-course radiation therapy received 25 Gy in five fractions followed by total mesorectal excision and then adjuvant chemotherapy according to the local center policy about nodal and margin status. Patients randomly assigned to selective postoperative chemoradiation therapy received immediate surgery followed by postoperative chemoradiation (45 Gy in 25 fractions with concurrent 5-FU) if their circumferential resection margin was 1 mm or smaller. Adjuvant chemotherapy for the group that received selective chemoradiation therapy was again given based on local standards regarding nodal and margin status.[8]
The risk of local recurrence at 3 years was 4.4% in the preoperative short-course group and 10.6% in the selective chemoradiation therapy group (HR, 0.39; 95% CI, 0.27–0.58; P < .0001).
OS did not differ between the groups.
Taken together, these studies demonstrate that short-course preoperative radiation therapy and long-course preoperative chemoradiation therapy are both reasonable treatment strategies for patients with stage II or III rectal adenocarcinoma.
Postoperative chemoradiation therapy
Progress in the development of postoperative treatment regimens relates to the integration of systemic chemotherapy and radiation therapy, as well as redefining the techniques for both modalities. The efficacy of postoperative radiation therapy and 5-FU-based chemotherapy for stages II and III rectal cancer was established by a series of prospective, randomized clinical trials, including:[9–11][Level of evidence A1]
Gastrointestinal Tumor Study Group (GITSG-7175).
Mayo/North Central Cancer Treatment Group (NCCTG-794751).
National Surgical Adjuvant Breast and Bowel Project (NSABP-R-01).
These studies demonstrated an increase in DFS interval and OS when radiation therapy was combined with chemotherapy after surgical resection. After the publication in 1990 of the results of these trials, experts at a National Cancer Institute-sponsored Consensus Development Conference recommended postoperative combined-modality treatment for patients with stages II and III rectal carcinoma.[12] Since that time, preoperative chemoradiation therapy has become the standard of care, although postoperative chemoradiation therapy is still an acceptable alternative. For more information, see the Preoperative chemoradiation therapy section.
Intergroup protocol 86-47-51 (MAYO-864751) compared continuous-infusion 5-FU (225 mg/m2/day throughout the entire course of radiation therapy) with bolus 5-FU (500 mg/m2/day for 3 consecutive days during the first and fifth weeks of radiation therapy).[13][Level of evidence A1]
A 10% improvement in OS was demonstrated with the use of continuous-infusion 5-FU.
A three-arm randomized trial determined whether continuous-infusion 5-FU given throughout the entire standard six-cycle course of adjuvant chemotherapy was more effective than continuous infusion 5-FU given only during pelvic radiation therapy. Median follow-up was 5.7 years.[14]
Arm 1 received bolus 5-FU in two 5-day cycles before (500 mg/m2/day) and after (450 mg/m2/day) radiation therapy, with protracted venous infusion 5-FU (225 mg/m2/day) during radiation therapy.
Arm 2 received continuous infusion 5-FU before (300 mg/m2/day for 42 days), after (300 mg/m2/day for 56 days), and during (225 mg/m2/day) radiation therapy.
Arm 3 received bolus 5-FU/LV in two 5-day cycles before (5-FU, 425 mg/m2/day; LV, 20 mg/m2/day) and after (5-FU, 380 mg/m2/day; LV, 20 mg/m2/day) radiation therapy, and bolus 5-FU/LV (5-FU, 400 mg/m2/day; LV, 20 mg/m2/day; days 1 to 4, every 28 days) during radiation therapy. Levamisole (150 mg/day) was administered in 3-day cycles every 14 days before and after radiation therapy.
No DFS, OS, or locoregional failure difference was detected (across all arms: 3-year DFS rate, 67%–69%; 3-year OS rate, 81%–83%; locoregional failure rate, 4.6%–8%).
Lethal toxicity was less than 1%, with grades 3 to 4 hematologic toxicity in 55% of patients in arm 1 and in 49% of the patients in arm 3, versus in 4% of patients in the continuous-infusion arm.[14][Level of evidence A1]
The final study results of Intergroup trial 0114 (INT-0114) showed no survival or local-control benefit with the addition of LV, levamisole, or both to 5-FU administered postoperatively for patients with stages II and III rectal cancers at a median follow-up of 7.4 years.[15][Level of evidence A1]
A pooled analysis of 3,791 patients enrolled in clinical trials demonstrated that, for patients with T3, N0 disease, the 5-year OS rate with surgery plus chemotherapy (OS, 84%) compared favorably with the survival rates of patients treated with surgery plus radiation therapy and bolus chemotherapy (OS rate, 76%) or surgery plus radiation therapy and protracted-infusion chemotherapy (OS rate, 80%).[16]
Surgery
Total mesorectal excision with either low anterior resection or abdominoperineal resection is usually performed for stages II and III rectal cancer before or after chemoradiation therapy.
Retrospective studies have demonstrated that some patients with pathological T3, N0 disease treated with surgery and no additional therapy have a very low risk of local and systemic recurrence.[17]
Primary chemoradiation therapy followed by intensive surveillance for complete clinical responders
Since the advent of preoperative chemoradiation therapy in rectal cancer, the standard approach has been to recommend definitive surgical resection by either abdominoperineal resection or laparoscopic-assisted resection. In most series, after long-course chemoradiation therapy, 10% to 20% of patients will have a complete clinical response in which there is no sign of persistent cancer by imaging, rectal exam, or direct visualization during sigmoidoscopy. It was a long-held belief that most patients who did not undergo surgery for personal or medical reasons would experience a local and/or systemic recurrence. However, it became clear that patients with a pathological complete response to preoperative chemoradiation therapy followed by definitive surgery had a better DFS than did patients who did not have a pathological clinical response.[18]
Several single-institution studies have challenged this standard of care by demonstrating that most patients with complete clinical response will be cured of rectal cancer without surgery and that many patients who experience a local recurrence can be treated with surgical resection (abdominoperineal resection or laparoscopic-assisted resection) at the time of their recurrence.[19–22] These institutional series were hampered by their small size and inherent selection bias.
Evidence (primary chemoradiation therapy followed by intensive surveillance for complete clinical responders):
Investigators in England performed the Oncological Outcomes after Clinical Complete Response in Patients with Rectal Cancer trial.[23] This was a propensity-score−matched cohort analysis. At a tertiary medical center in Manchester, 228 patients who chose watchful waiting from 2011 to 2013 after a complete clinical response to preoperative chemoradiation therapy were combined with 98 patients from a registry of three neighboring medical centers who chose watchful waiting after chemoradiation therapy beginning in 2005. A clinical complete response was considered in the absence of residual ulceration, stenosis, or mass within the rectum during digital rectal examination and endoscopic examination 8 weeks or more after completion of concurrent chemoradiation therapy. The only positive findings consistent with a complete clinical response during clinical or endoscopic examination were whitening of the mucosa and telangiectasia. Classification of complete clinical response required normal radiological imaging of the mesorectum and pelvis. Complete clinical responders (n = 129) were compared with a cohort of patients treated similarly who underwent surgery for complete resection (n = 228). Compared with all patients who underwent surgery, patients who chose watch and wait had tumors with an earlier T stage and N stage and that were less likely to be poorly differentiated.
After a median follow-up of 33 months, 44 (34%) of the 129 patients who chose watchful waiting had a local recurrence, and 36 patients had a salvage resection.
In the paired-cohort analysis, the 3-year non-regrowth DFS rate for all patients was 83% (95% CI, 76%–88%): 88% (95% CI, 75%–94%) for the watch-and-wait group and 78% (95% CI, 63%–87%) for the surgical resection group (log-rank P = .022).
The 3-year OS rate was 96% (95% CI, 88%–98%) in the watch-and-wait group versus 87% (95% CI, 77%–93%) for the surgical resection group (log-rank P = .015).
The 3-year colostomy-free survival rate was 74% (95% CI, 64%–82%) for the watch-and-wait group and 47% (95% CI, 37%–57%; log-rank P < .0001) for the surgical group.
Patients managed by watch and wait underwent a more intensive follow-up protocol consisting of outpatient digital rectal examination; MRI (every 4–6 months in the first 2 years); examination under anesthesia or endoscopy; computed tomography scan of the chest, abdomen, and pelvis; and at least two carcinoembryonic antigen measurements in the first 2 years. The optimal follow-up has not been determined.
For patients who have a complete clinical response to therapy, it is reasonable to consider a watch-and-wait approach with intensive surveillance instead of immediate surgical resection.
In the OPRA study (NCT02008656), 324 patients with stage II/III rectal cancer were randomly assigned to receive either induction chemotherapy followed by chemoradiation therapy or chemoradiation therapy followed by consolidation chemotherapy. Patients had the potential to omit surgery based on response assessment.[24,25]
The 5-year DFS rate was 71% (95% CI, 64%–79%) and the total mesorectal excision–free survival rate was 39% (95% CI, 32%–48%) in the patients who received induction chemotherapy followed by chemoradiation therapy. The 5-year DFS rate was 69% (95% CI, 62%–77%) and the total mesorectal excision–free survival rate was 54% (95% CI, 46%–62%) in the patients who received chemoradiation therapy followed by consolidation chemotherapy.[24][Level of evidence B1]
While the optimal surveillance regimen for patients undergoing nonoperative management is still under active study, the regimen in the OPRA trial involved periodic surveillance with digital rectal examination, sigmoidoscopy, and MRI. Digital rectal examination and flexible sigmoidoscopy were performed every 4 months for the first 2 years from the time of assessment of response, and every 6 months for the following 3 years. Rectal MRI was performed every 6 months for the first 2 years and yearly for the following 3 years. Patients could have additional assessments if clinically indicated.
The optimal follow-up for these patients has not been determined. For patients who have a complete clinical response to therapy, nonoperative management with intensive surveillance instead of immediate surgical resection is a standard-of-care approach.
Immunotherapy
Among patients with rectal adenocarcinomas, 5% to 10% of the tumors have mismatch repair deficiency or high MSI. Immune checkpoint inhibitors are efficacious as a first-line therapy for metastatic colorectal cancers, with overall response rates of 30% to 60%.[26–28] These responses proved durable, and prolonged OS was demonstrated in these settings.
Evidence (immunotherapy):
A phase II trial (NCT04165772) studied dostarlimab, an anti-programmed death-1 (PD-1) monoclonal antibody, in 12 patients with locally advanced, mismatch repair–deficient, stage II or stage III rectal adenocarcinoma.[29]
All 12 patients had clinical complete responses of 100% (95% CI, 74%–100%) after a median follow-up of 12 months. Patients’ cancers did not recur when the follow-up period ranged from 6 to 25 months. At the time of follow-up, chemoradiation therapy and surgery had been avoided.[29][Level of evidence C3]
Before this approach becomes a new standard, more patients need to be evaluated. A longer follow-up period is required to ensure durability and assess the need for future surgery or chemoradiation therapy.
Chemotherapy regimens
Many academic oncologists suggest that FOLFOX be considered the standard for adjuvant chemotherapy in rectal cancer. However, there are no data about rectal cancer to support this consideration. FOLFOX has become the standard arm in the latest Intergroup study evaluating adjuvant chemotherapy in rectal cancer. An Eastern Cooperative Oncology Group trial (ECOG-E5202 [NCT00217737]) randomly assigned patients with stage II or III rectal cancer who received preoperative or postoperative chemoradiation therapy to receive 6 months of FOLFOX with or without bevacizumab, but this trial closed because of poor accrual. No efficacy data are available.
Preoperative oxaliplatin with chemoradiation therapy
Oxaliplatin has also shown radiosensitizing properties in preclinical models.[30] Phase II studies that combined oxaliplatin with fluoropyrimidine-based chemoradiation therapy have reported pathological complete response rates ranging from 14% to 30%.[31–35] Data from multiple studies have demonstrated a correlation between rates of pathological complete response and end points including distant metastasis-free survival, DFS, and OS.[36–38]
There is no current role for off-trial use of concurrent oxaliplatin and radiation therapy in the treatment of patients with rectal cancer.
Evidence (preoperative oxaliplatin with chemoradiation therapy):
The ACCORD 12/0405-Prodige 2 trial (NCT00227747), which randomly assigned 598 patients with clinically staged T2 or T3 or resectable T4 rectal cancer accessible by digital rectal examination to either preoperative radiation therapy (45 Gy in 25 fractions over 5 weeks) with capecitabine (800 mg/m2 twice daily 5 of every 7 days) or to a higher dose of radiation (50 Gy in 25 fractions over 5 weeks) with the same dose of capecitabine and oxaliplatin (50 mg/m2 weekly). Total mesorectal excision was performed in 98% of both groups at a median interval of 6 weeks after chemoradiation therapy was completed.[39]
Pathological complete response was the primary end point (albeit never validated as a true surrogate of OS). A higher percentage of patients achieved a pathological complete response in the oxaliplatin-treated group (19.2% vs. 13.9%). However, the difference did not reach statistical significance (P = .09).
The rate of grade 3 or 4 toxicity was significantly higher in the oxaliplatin-treated group (25% vs. 11%; P < .001), and there was no difference in the rate of sphincter-sparing surgery (75% vs. 78%).
Similarly, the STAR-01 trial investigated the role of oxaliplatin combined with 5-FU chemoradiation therapy for locally advanced rectal cancer.[40][Level of evidence A1] This Italian study randomly assigned 747 patients with resectable, locally advanced, clinically staged T3 or T4 and/or clinical N1 to N2 adenocarcinoma of the mid- to low-rectum to receive either continuous-infusion 5-FU with radiation therapy or to receive the same regimen in combination with oxaliplatin (60 mg/m2). Although the primary end point was OS, a protocol-planned analysis of response to preoperative therapy has been preliminarily reported.
The rate of pathological complete response was equivalent at 16% in both arms (odds ratio, 0.98; 95% CI, 0.66–1.44; P = .904).
There was no difference noted in the rate of pathologically positive lymph nodes, tumor infiltration beyond the muscularis propria, or the rate of circumferential margin positivity.
An increase in grades 3 to 4 treatment-related acute toxicity was noted with the addition of oxaliplatin (24% vs. 8%; P <.001). Longer-term outcomes including OS have not yet been reported.
The NSABP-R-04 trial (NCT00058474) randomly assigned 1,608 patients with clinically staged T3 or T4 or clinical node-positive adenocarcinoma within 12 cm of the anal verge in a 2 × 2 factorial design to one of the following four treatment groups:
Intravenous (IV) continuous infusion 5-FU with radiation therapy.
Capecitabine with radiation therapy.
IV continuous infusion 5-FU plus weekly oxaliplatin with radiation therapy.
Capecitabine plus weekly oxaliplatin with radiation therapy.
The primary objective of this study is locoregional disease control.[41][Level of evidence B1] Preliminary results, reported in abstract form at the 2011 American Society of Clinical Oncology annual meeting, demonstrated the following results:
There was no significant difference in the rates of pathological complete response, sphincter-sparing surgery, or surgical downstaging between the 5-FU and capecitabine regimens or between the regimens with and without oxaliplatin.
Patients treated with oxaliplatin had significantly higher rates of grade 3 and grade 4 acute toxicity (15.4% vs. 6.6%; P < .001).
The German CAO/ARO/AIO-04 trial randomly assigned 1,236 patients with clinically staged T3 to T4 or clinical lymph node-positive adenocarcinoma within 12 cm from the anal verge to receive either concurrent chemoradiation therapy with 5-FU (week 1 and week 5) or concurrent chemoradiation therapy with 5-FU daily (250 mg/m2) and oxaliplatin (50 mg/m2).[42][Level of evidence B1]
In contrast to the previous studies, a significantly higher rate of pathological complete response was achieved in patients who received oxaliplatin (17% vs. 13%; P = .038).
There was no significant difference in rates of overall grades 3 and 4 toxicity; however, diarrhea and nausea and vomiting were more common among those treated with oxaliplatin.
The 5-FU schedules in this study differed between the two arms, which may have contributed to the difference in outcomes noted. Longer follow-up will be necessary to determine the effect on the primary end point of the study, DFS.
Postoperative oxaliplatin-containing regimens
Based on results of several studies, oxaliplatin as a radiation sensitizer does not appear to add any benefit in terms of primary tumor response, and it has been associated with increased acute treatment-related toxicity. The question of whether oxaliplatin should be added to adjuvant 5-FU/LV for postoperative management of stages II and III rectal cancer is an ongoing debate. There are no randomized phase III studies to support the use of oxaliplatin for the adjuvant treatment of rectal cancer. However, the addition of oxaliplatin to 5-FU/LV for the adjuvant treatment of colon cancer is now considered standard care.
Evidence (postoperative oxaliplatin):
In the randomized Multicenter International Study of Oxaliplatin/5-FU/LV in the Adjuvant Treatment of Colon Cancer (MOSAIC) study, the toxic effects and efficacy of FOLFOX4 (a 2-hour infusion of 200 mg/m2 LV, followed by a bolus of 400 mg/m2 5-FU, and then a 22-hour infusion of 600 mg/m2 5-FU on 2 consecutive days every 14 days for 12 cycles, plus a 2-hour infusion of 85 mg/m2 oxaliplatin on day 1, given simultaneously with LV) were compared with the same 5-FU/LV regimen without oxaliplatin when administered for 6 months. Each arm of the trial included 1,123 patients.[43]
Preliminary results of the study, with 37 months of follow-up, demonstrated a significant improvement in DFS at 3 years in favor of FOLFOX4 (77.8% vs. 72.9%; P = .01). When initially reported, there was no difference in OS.[44][Level of evidence B1]
Further follow-up at 6 years demonstrated that the OS for all patients (both stage II and stage III) who entered the study was not significantly different (OS rate, 78.5% FOLFOX4 vs. 76.0% 5-FU/LV group; HR, 0.84; 95% CI, 0.71–1.00).
On subset analysis, the 6-year OS rate in patients with stage III colon cancer was 72.9% in the patients who received FOLFOX4 and 68.9% in the patients who received 5-FU/LV (HR, 0.80; 95% CI, 0.65–0.97; P = .023).[44][Level of evidence A1]
Patients treated with FOLFOX4 experienced more frequent toxic effects, consisting mainly of neutropenia (41% > grade 3) and reversible peripheral sensory neuropathy (12.4% > grade 3).
The results of the completed NSABP-C-07 study confirmed and extended the results of the MOSAIC trial.[45] In NSABP C-07, 2,492 patients with stage II or III colon or rectal cancer were randomly assigned to receive either FLOX (2-hour IV infusion of 85 mg/m2 oxaliplatin on days 1, 15, and 29 of each 8-week treatment cycle, followed by a 2-hour IV infusion of 500 mg/m2 LV plus bolus 500 mg/m2 5-FU 1 hour after the start of the LV infusion on days 1, 8, 15, 22, 29, and 36, followed by a 2-week rest period, for a total of three cycles [24 weeks]) or the same chemotherapy without oxaliplatin (Roswell Park regimen).
The 3- and 4-year DFS rates were 71.8% and 67% for the Roswell Park regimen and 76.1% and 73.2% for FLOX, respectively.
The HR was 0.80 (95% CI, 0.69–0.93), a 20% risk reduction in favor of FLOX (P < .004).
It is unclear whether the results of these colon cancer trials can be applied to the management of patients with rectal cancer. There are no randomized phase III studies to support the routine practice of administering FOLFOX as adjuvant therapy to patients with rectal cancer.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Schrag D, Shi Q, Weiser MR, et al.: Preoperative Treatment of Locally Advanced Rectal Cancer. N Engl J Med 389 (4): 322-334, 2023. [PUBMED Abstract]
Sauer R, Becker H, Hohenberger W, et al.: Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351 (17): 1731-40, 2004. [PUBMED Abstract]
Sauer R, Liersch T, Merkel S, et al.: Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol 30 (16): 1926-33, 2012. [PUBMED Abstract]
Roh MS, Colangelo LH, O’Connell MJ, et al.: Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol 27 (31): 5124-30, 2009. [PUBMED Abstract]
Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med 336 (14): 980-7, 1997. [PUBMED Abstract]
Bujko K, Nowacki MP, Nasierowska-Guttmejer A, et al.: Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg 93 (10): 1215-23, 2006. [PUBMED Abstract]
Ngan SY, Burmeister B, Fisher RJ, et al.: Randomized trial of short-course radiotherapy versus long-course chemoradiation comparing rates of local recurrence in patients with T3 rectal cancer: Trans-Tasman Radiation Oncology Group trial 01.04. J Clin Oncol 30 (31): 3827-33, 2012. [PUBMED Abstract]
Sebag-Montefiore D, Stephens RJ, Steele R, et al.: Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet 373 (9666): 811-20, 2009. [PUBMED Abstract]
Thomas PR, Lindblad AS: Adjuvant postoperative radiotherapy and chemotherapy in rectal carcinoma: a review of the Gastrointestinal Tumor Study Group experience. Radiother Oncol 13 (4): 245-52, 1988. [PUBMED Abstract]
Krook JE, Moertel CG, Gunderson LL, et al.: Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 324 (11): 709-15, 1991. [PUBMED Abstract]
Fisher B, Wolmark N, Rockette H, et al.: Postoperative adjuvant chemotherapy or radiation therapy for rectal cancer: results from NSABP protocol R-01. J Natl Cancer Inst 80 (1): 21-9, 1988. [PUBMED Abstract]
NIH consensus conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA 264 (11): 1444-50, 1990. [PUBMED Abstract]
O’Connell MJ, Martenson JA, Wieand HS, et al.: Improving adjuvant therapy for rectal cancer by combining protracted-infusion fluorouracil with radiation therapy after curative surgery. N Engl J Med 331 (8): 502-7, 1994. [PUBMED Abstract]
Smalley SR, Benedetti JK, Williamson SK, et al.: Phase III trial of fluorouracil-based chemotherapy regimens plus radiotherapy in postoperative adjuvant rectal cancer: GI INT 0144. J Clin Oncol 24 (22): 3542-7, 2006. [PUBMED Abstract]
Tepper JE, O’Connell M, Niedzwiecki D, et al.: Adjuvant therapy in rectal cancer: analysis of stage, sex, and local control–final report of intergroup 0114. J Clin Oncol 20 (7): 1744-50, 2002. [PUBMED Abstract]
Gunderson LL, Sargent DJ, Tepper JE, et al.: Impact of T and N stage and treatment on survival and relapse in adjuvant rectal cancer: a pooled analysis. J Clin Oncol 22 (10): 1785-96, 2004. [PUBMED Abstract]
Willett CG, Badizadegan K, Ancukiewicz M, et al.: Prognostic factors in stage T3N0 rectal cancer: do all patients require postoperative pelvic irradiation and chemotherapy? Dis Colon Rectum 42 (2): 167-73, 1999. [PUBMED Abstract]
Maas M, Nelemans PJ, Valentini V, et al.: Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol 11 (9): 835-44, 2010. [PUBMED Abstract]
Maas M, Beets-Tan RG, Lambregts DM, et al.: Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J Clin Oncol 29 (35): 4633-40, 2011. [PUBMED Abstract]
Lambregts DM, Maas M, Bakers FC, et al.: Long-term follow-up features on rectal MRI during a wait-and-see approach after a clinical complete response in patients with rectal cancer treated with chemoradiotherapy. Dis Colon Rectum 54 (12): 1521-8, 2011. [PUBMED Abstract]
Smith JD, Ruby JA, Goodman KA, et al.: Nonoperative management of rectal cancer with complete clinical response after neoadjuvant therapy. Ann Surg 256 (6): 965-72, 2012. [PUBMED Abstract]
Dalton RS, Velineni R, Osborne ME, et al.: A single-centre experience of chemoradiotherapy for rectal cancer: is there potential for nonoperative management? Colorectal Dis 14 (5): 567-71, 2012. [PUBMED Abstract]
Renehan AG, Malcomson L, Emsley R, et al.: Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol 17 (2): 174-83, 2016. [PUBMED Abstract]
Verheij FS, Omer DM, Williams H, et al.: Long-Term Results of Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J Clin Oncol 42 (5): 500-506, 2024. [PUBMED Abstract]
Garcia-Aguilar J, Patil S, Gollub MJ, et al.: Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy. J Clin Oncol 40 (23): 2546-2556, 2022. [PUBMED Abstract]
Le DT, Uram JN, Wang H, et al.: PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 372 (26): 2509-20, 2015. [PUBMED Abstract]
Overman MJ, Lonardi S, Wong KYM, et al.: Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol 36 (8): 773-779, 2018. [PUBMED Abstract]
André T, Shiu KK, Kim TW, et al.: Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med 383 (23): 2207-2218, 2020. [PUBMED Abstract]
Cercek A, Lumish M, Sinopoli J, et al.: PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N Engl J Med 386 (25): 2363-2376, 2022. [PUBMED Abstract]
Cividalli A, Ceciarelli F, Livdi E, et al.: Radiosensitization by oxaliplatin in a mouse adenocarcinoma: influence of treatment schedule. Int J Radiat Oncol Biol Phys 52 (4): 1092-8, 2002. [PUBMED Abstract]
Gérard JP, Chapet O, Nemoz C, et al.: Preoperative concurrent chemoradiotherapy in locally advanced rectal cancer with high-dose radiation and oxaliplatin-containing regimen: the Lyon R0-04 phase II trial. J Clin Oncol 21 (6): 1119-24, 2003. [PUBMED Abstract]
Machiels JP, Duck L, Honhon B, et al.: Phase II study of preoperative oxaliplatin, capecitabine and external beam radiotherapy in patients with rectal cancer: the RadiOxCape study. Ann Oncol 16 (12): 1898-905, 2005. [PUBMED Abstract]
Rödel C, Liersch T, Hermann RM, et al.: Multicenter phase II trial of chemoradiation with oxaliplatin for rectal cancer. J Clin Oncol 25 (1): 110-7, 2007. [PUBMED Abstract]
Ryan DP, Niedzwiecki D, Hollis D, et al.: Phase I/II study of preoperative oxaliplatin, fluorouracil, and external-beam radiation therapy in patients with locally advanced rectal cancer: Cancer and Leukemia Group B 89901. J Clin Oncol 24 (16): 2557-62, 2006. [PUBMED Abstract]
Valentini V, Coco C, Minsky BD, et al.: Randomized, multicenter, phase IIb study of preoperative chemoradiotherapy in T3 mid-distal rectal cancer: raltitrexed + oxaliplatin + radiotherapy versus cisplatin + 5-fluorouracil + radiotherapy. Int J Radiat Oncol Biol Phys 70 (2): 403-12, 2008. [PUBMED Abstract]
García-Aguilar J, Hernandez de Anda E, Sirivongs P, et al.: A pathologic complete response to preoperative chemoradiation is associated with lower local recurrence and improved survival in rectal cancer patients treated by mesorectal excision. Dis Colon Rectum 46 (3): 298-304, 2003. [PUBMED Abstract]
Guillem JG, Chessin DB, Cohen AM, et al.: Long-term oncologic outcome following preoperative combined modality therapy and total mesorectal excision of locally advanced rectal cancer. Ann Surg 241 (5): 829-36; discussion 836-8, 2005. [PUBMED Abstract]
Rödel C, Martus P, Papadoupolos T, et al.: Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol 23 (34): 8688-96, 2005. [PUBMED Abstract]
Gérard JP, Azria D, Gourgou-Bourgade S, et al.: Comparison of two neoadjuvant chemoradiotherapy regimens for locally advanced rectal cancer: results of the phase III trial ACCORD 12/0405-Prodige 2. J Clin Oncol 28 (10): 1638-44, 2010. [PUBMED Abstract]
Aschele C, Cionini L, Lonardi S, et al.: Primary tumor response to preoperative chemoradiation with or without oxaliplatin in locally advanced rectal cancer: pathologic results of the STAR-01 randomized phase III trial. J Clin Oncol 29 (20): 2773-80, 2011. [PUBMED Abstract]
Roh MS, Yothers GA, O’Connell MJ, et al.: The impact of capecitabine and oxaliplatin in the preoperative multimodality treatment in patients with carcinoma of the rectum: NSABP R-04. [Abstract] J Clin Oncol 29 (Suppl 15): A-3503, 2011.
Rödel C, Liersch T, Becker H, et al.: Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol 13 (7): 679-87, 2012. [PUBMED Abstract]
André T, Boni C, Mounedji-Boudiaf L, et al.: Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 350 (23): 2343-51, 2004. [PUBMED Abstract]
André T, Boni C, Navarro M, et al.: Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 27 (19): 3109-16, 2009. [PUBMED Abstract]
de Gramont A, Boni C, Navarro M, et al.: Oxaliplatin/5FU/LV in the adjuvant treatment of stage II and stage III colon cancer: efficacy results with a median follow-up of 4 years. [Abstract] J Clin Oncol 23 (Suppl 16): A-3501, 246s, 2005.
Treatment of Stage IV and Recurrent Rectal Cancer
Treatment of patients with advanced or recurrent rectal cancer depends on the location of the disease.
Treatment Options for Stage IV and Recurrent Rectal Cancer
Treatment options for stage IV and recurrent rectal cancer include:
Surgery with or without chemotherapy or radiation therapy
For patients with locally recurrent, liver-only, or lung-only metastatic disease, surgical resection, if feasible, is the only potentially curative treatment.[1] Patients with limited pulmonary metastasis, and patients with both pulmonary and hepatic metastasis, may also be considered for surgical resection, with 5-year survival possible in highly selected patients.[2–5] The presence of hydronephrosis associated with recurrence appears to be a contraindication to surgery with curative intent.[6]
Locally recurrent rectal cancer may be resectable, particularly if an inadequate prior operation was performed. For patients with local recurrence alone after an initial, attempted curative resection, aggressive local therapy with repeat low anterior resection and coloanal anastomosis, abdominoperineal resection, or posterior or total pelvic exenteration can lead to long-term disease-free survival.[7,8]
The use of induction chemoradiation therapy for previously nonirradiated patients with locally advanced pelvic recurrence (pelvic side-wall, sacral, and/or adjacent organ involvement) may increase resectability and allow for sphincter preservation.[9,10] Intraoperative radiation therapy in patients who underwent previous external-beam radiation therapy may improve local control in patients with locally recurrent disease, with acceptable morbidity.[11]
Systemic therapy
The following drugs are used alone and in combination with other drugs for patients with metastatic colorectal cancer:
When 5-FU was the only active chemotherapy drug, trials in patients with locally advanced, unresectable, or metastatic disease demonstrated partial responses and prolongation of the time-to-progression (TTP) of disease,[12,13] and improved survival and quality of life in patients who received chemotherapy versus best supportive care.[14–16] Several trials have analyzed the activity and toxic effects of various 5-FU/LV regimens using different doses and administration schedules and showed essentially equivalent results with a median survival time in the approximately 12-month range.[17]
Irinotecan and oxaliplatin
Three randomized studies in patients with metastatic colorectal cancer demonstrated improved response rates, progression-free survival (PFS), and overall survival (OS) when irinotecan or oxaliplatin was combined with 5-FU/LV.[18–20]
Evidence (irinotecan vs. oxaliplatin):
An intergroup study (NCCTG-N9741 [NCT00003594]) compared irinotecan/5-FU/LV (IFL) with oxaliplatin/LV/5-FU (FOLFOX4) in first-line treatment for patients with metastatic colorectal cancer.[21][Level of evidence A1]
Patients assigned to FOLFOX4 experienced an improved PFS compared with patients randomly assigned to IFL (median, 8.7 months vs. 6.9 months; P = .014; hazard ratio [HR], 0.74; 95% confidence interval [CI], 0.61–0.89) and OS (19.5 months vs. 15.0 months; P = .001; HR, 0.66; 95% CI, 0.54–0.82).
Subsequently, two studies compared FOLFOX with LV/5-FU/irinotecan (FOLFIRI), and patients were allowed to cross over after progression on first-line therapy.[22,23][Level of evidence B1]
PFS and OS were identical between the treatment arms in both studies.
The Bolus, Infusional, or Capecitabine with Camptosar-Celecoxib (BICC-C [NCT00094965]) trial evaluated several different irinotecan-based regimens in patients with previously untreated metastatic colorectal cancer: FOLFIRI, irinotecan plus bolus 5-FU/LV (mIFL), and capecitabine/irinotecan (CAPIRI).[24] The study randomly assigned 430 patients and was closed early due to poor accrual.
The patients who received FOLFIRI had a better PFS than the patients who received either mIFL (7.6 months vs. 5.9 months; P = .004) or CAPIRI (7.6 months vs. 5.8 months; P = .015).
Patients who received CAPIRI had the highest (grade 3 or higher) rates of nausea, vomiting, diarrhea, dehydration, and hand-foot syndrome.
Since the publication of these studies, the use of either FOLFOX or FOLFIRI is considered acceptable for first-line treatment of patients with metastatic colorectal cancer. However, when using an irinotecan-based regimen as first-line treatment of metastatic colorectal cancer, FOLFIRI is preferred.[24][Level of evidence B1]
Capecitabine
Before the advent of multiagent chemotherapy, two randomized studies demonstrated that capecitabine was associated with equivalent efficacy when compared with the Mayo Clinic regimen of 5-FU/LV.[25,26][Level of evidence A1]
Randomized phase III trials have addressed the equivalence of substituting capecitabine for infusional 5-FU. Two phase III studies have evaluated capecitabine/oxaliplatin (CAPOX) versus 5-FU/oxaliplatin regimens (FUOX or FUFOX).[27,28]
Evidence (oxaliplatin vs. capecitabine):
The Arbeitsgemeinschaft Internische Onkologie (AIO) Colorectal Study Group randomly assigned 474 patients to either CAPOX or FUFOX.
The median PFS was 7.1 months for the CAPOX arm and 8.0 months for the FUFOX arm (HR, 1.17; 95% CI, 0.96–1.43; P = .117), and the HR was in the prespecified equivalence range.[28]
The Spanish Cooperative Group randomly assigned 348 patients to CAPOX or FUOX.[27][Level of evidence B1]
The TTP was 8.9 months for CAPOX versus 9.5 months for FUOX (P = .153) and met the prespecified range for noninferiority.
When using an oxaliplatin-based regimen as first-line treatment of metastatic colorectal cancer, a CAPOX regimen is not inferior to a 5-FU/oxaliplatin regimen.
Bevacizumab
Bevacizumab can reasonably be added to either FOLFIRI or FOLFOX for patients undergoing first-line treatment of metastatic colorectal cancer. There are currently no completed randomized controlled studies evaluating whether continued use of bevacizumab in second-line or third-line treatment after progressing on a first-line bevacizumab regimen extends survival.
Evidence (bevacizumab):
After bevacizumab was approved, the BICC-C trial was amended, and an additional 117 patients were randomly assigned to receive FOLFIRI/bevacizumab or mIFL/bevacizumab.[24]
Although the primary end point of PFS was not significantly different, patients who received FOLFIRI/bevacizumab had a significantly better OS (28.0 months vs. 19.2 months; P = .037; HR for death, 1.79; 95% CI, 1.12–2.88).
In the Hurwitz study, patients with previously untreated metastatic colorectal cancer were randomly assigned to either IFL or IFL/bevacizumab.[29]
The patients randomly assigned to the IFL/bevacizumab arm experienced a significantly better PFS (10.6 months in the IFL/bevacizumab arm compared with 6.2 months in the IFL/placebo arm; HRdisease progression, 0.54; P < .001) and OS (20.3 months in the IFL/bevacizumab arm compared with 15.6 months in the IFL/placebo arm; HRdeath, 0.66; P < .001).[29]
Despite the lack of direct data, in standard practice bevacizumab was added to FOLFOX as a standard first-line regimen based on the results of NCCTG-N9741.[21] Subsequently, in a randomized phase III study, 1,401 patients with untreated, stage IV colorectal cancer were randomly assigned in a 2 × 2 factorial design to CAPOX versus FOLFOX4, then to bevacizumab versus placebo. PFS was the primary end point.[30][Level of evidence B1]
The median PFS was 9.4 months for patients who received bevacizumab and 8.0 months for the patients who received placebo (HR, 0.83; 97.5% CI, 0.72–0.95; P = .0023).
Median OS was 21.3 months for patients who received bevacizumab and 19.9 months for patients who received placebo (HR, 0.89; 97.5% CI, 0.76–1.03; P = .077).
The median PFS (intention-to-treat analysis) was 8.0 months in the pooled CAPOX-containing arms versus 8.5 months in the FOLFOX4-containing arms (HR, 1.04; 97.5% CI, 0.93–1.16), with the upper limit of the 97.5% CI being below the predefined noninferiority margin of 1.23.[30,31]
The effect of bevacizumab on OS is likely to be less than what was seen in the original Hurwitz study.
Investigators from the Eastern Cooperative Oncology Group randomly assigned patients who had progressed on 5-FU/LV and irinotecan to either FOLFOX or FOLFOX/bevacizumab.
Patients randomly assigned to FOLFOX/bevacizumab experienced a statistically significant improvement in PFS compared with patients assigned to FOLFOX alone (7.43 months vs. 4.7 months; HR, 0.61; P < .0001) and OS (12.9 months vs. 10.8 months; HR, 0.75; P = .0011).[32][Level of evidence A1]
FOLFOXIRI
Evidence (FOLFOXIRI):
The combination of FOLFOXIRI with bevacizumab was compared with FOLFIRI with bevacizumab in a randomized, phase III study of 508 patients with untreated metastatic colorectal cancer.[33]
The median PFS was 12.1 months in the FOLFOXIRI group, compared with 9.7 months in the FOLFIRI group (HR for progression, 0.75; 95% CI, 0.62–0.90; P = .003). OS was not significantly different between the groups (31.0 vs. 25.8 months; HRdeath, 0.79; 95% CI, 0.63–1.00; P = .054).[33][Level of evidence B1]
Patients who received FOLFOXIRI had significantly more grade 3 and 4 toxicities, including neutropenia, stomatitis, and peripheral neuropathy.
Cetuximab
Cetuximab is a partially humanized monoclonal antibody against EGFR. Importantly, patients with KRAS-altered tumors may experience worse outcome when cetuximab is added to multiagent chemotherapy regimens containing bevacizumab.
Evidence (cetuximab):
For patients who had disease progression while receiving irinotecan-containing regimens, a randomized phase II study was performed that used either cetuximab or irinotecan/cetuximab.[34][Level of evidence C3]
The median TTP for patients who received cetuximab was 1.5 months, compared with median TTP of 4.2 months for patients who received irinotecan and cetuximab. Based on this study, cetuximab was approved for use in patients with metastatic colorectal cancer refractory to 5-FU and irinotecan.
The Crystal Study (EMR 62202-013 [NCT00154102]) randomly assigned 1,198 patients with stage IV colorectal cancer to FOLFIRI with or without cetuximab.[35][Level of evidence B1]
The addition of cetuximab was associated with an improved PFS (HR, 0.85; 95% CI, 0.72–0.99; stratified log-rank P = .048) but not OS.
Retrospective studies of patients with metastatic colorectal cancer have suggested that responses to anti-EGFR antibody therapy are confined to patients with tumors that harbor wild types of KRAS (i.e., lack activating variants at codon 12 or 13 of the KRAS gene).
A subset analysis evaluating efficacy in relation to KRAS status was done in patients enrolled in the Crystal Study. There was a significant interaction for KRAS variant status and treatment for tumor response (P = .03) but not for PFS (P = .07). Among patients with KRAS wild-type tumors, the HR favored the FOLFIRI/cetuximab group (HR, 0.68; 95% CI, 0.50–0.94).
In a randomized trial, patients with metastatic colorectal cancer received capecitabine/oxaliplatin/bevacizumab with or without cetuximab.[36][Level of evidence B1]
The median PFS was 9.4 months in the group who received cetuximab and 10.7 months in the group who did not receive cetuximab (P = .01).
In a subset analysis, patients with KRAS-altered tumors who received cetuximab had significantly decreased PFS compared with patients with wild-type KRAS tumors who received cetuximab (8.1 months vs. 10.5 months; P = .04).
Among patients with KRAS-altered tumors, PFS was significantly shorter in those who received cetuximab than those did not receive cetuximab (8.1 months vs. 12.5 months; P = .003). OS was also significantly shorter (17.2 months vs. 24.9 months, respectively; P = .03).
The Medical Research Council (MRC) COIN trial (NCT00182715) sought to determine if adding cetuximab to combination chemotherapy with a fluoropyrimidine and oxaliplatin in first-line treatment for patients with KRAS wild-type tumors was beneficial.[37,38] In addition, the MRC sought to evaluate the effect of intermittent chemotherapy versus continuous chemotherapy. The 1,630 patients were randomly assigned to three treatment groups:
Arm A: fluoropyrimidine/oxaliplatin.
Arm B: fluoropyrimidine/oxaliplatin/cetuximab.
Arm C: intermittent fluoropyrimidine/oxaliplatin.
The comparisons between arms A and B and arms A and C were analyzed and published separately.[37,38]
In patients with KRAS wild-type tumors (arm A, n = 367; arm B, n = 362), OS did not differ between treatment groups (median survival, 17.9 months [interquartile range (IQR), 10.3–29.2] in the control group vs. 17.0 months [IQR, 9.4–30.1] in the cetuximab group; HR, 1.04; 95% CI, 0.87–1.23; P = .67). Similarly, there was no effect on PFS (8.6 months [IQR, 5.0–12.5] in the control group vs. 8.6 months [IQR, 5.1–13.8] in the cetuximab group; HR, 0.96; 95% CI, 0.82–1.12, P = .60).[37,38][Level of evidence A1]
The reasons for lack of benefit in adding cetuximab are unclear. Subset analyses suggest that the use of capecitabine was associated with an inferior outcome, and the use of second-line therapy was less in patients treated with cetuximab.
There was no difference between the continuously treated patients (arm A) and the intermittently treated patients (arm C).
Median survival in the intent-to-treat population (n = 815 in both groups) was 15.8 months (IQR, 9.4–26.1) in arm A and 14.4 months (IQR, 8.0–24.7) in arm C (HR, 1.084; 80% CI, 1.008–1.165).
In the per-protocol population, which included only those patients who were free from progression at 12 weeks and randomly assigned to continue treatment or go on a chemotherapy holiday (arm A, n = 467; arm C, n = 511), median survival was 19.6 months (IQR, 13.0–28.1) in arm A and 18.0 months (IQR, 12.1–29.3) in arm C (HR, 1.087, 95% CI, 0.986–1.198).
The upper limits of CIs for HRs in both analyses were greater than the predefined noninferiority boundary. While intermittent chemotherapy was not deemed noninferior, there appeared to be clinically insignificant differences in patient outcomes.
Ziv-aflibercept
Ziv-aflibercept is an anti-VEGF molecule and has been evaluated as a component of second-line therapy in patients with metastatic colorectal cancer.
Evidence (ziv-aflibercept):
In one trial, 1,226 patients were randomly assigned to receive ziv-aflibercept (4 mg/kg intravenously) or placebo every 2 weeks in combination with FOLFIRI.[39][Level of evidence A2]
Patients who received ziv-aflibercept plus FOLFIRI had significantly improved OS rates, with median survival times of 13.50 months compared with patients who received placebo plus FOLFIRI, with median survival times of 12.06 months (HR, 0.817; 95.34% CI, 0.713–0.937; P = .0032).
Patients who received ziv-aflibercept plus FOLFIRI also had significantly improved PFS rates, with median PFS rates of 6.90 months compared with patients who received placebo plus FOLFIRI, with median PFS rates of 4.67 months (HR, 0.758; 95% CI, 0.661–0.869; P < .0001).
Based on these results, the use of FOLFIRI plus ziv-aflibercept is an acceptable second-line regimen for patients previously treated with FOLFOX-based chemotherapy. Whether to continue bevacizumab or initiate ziv-aflibercept in second-line therapy has not been addressed as yet in any clinical trial, and there are no data available.
Ramucirumab
Ramucirumab is a fully humanized monoclonal antibody that binds to vascular endothelial growth factor receptor-2 (VEGFR-2).
Evidence (ramucirumab):
In the randomized, unblinded, phase III RAISE study (NCT01183780), 1,072 patients with stage IV colorectal cancer who had progressed on first-line chemotherapy were randomly assigned to FOLFIRI with or without ramucirumab (8 mg/kg).[40][Level of evidence A1]
Patients assigned to FOLFIRI plus ramucirumab had a significant improvement in median OS (13.3 months vs. 11.7 months; HR, 0.84; P = .0219) and PFS (5.7 months vs. 4.5 months; HR, 0.793; P = .0005).
Grade 3 adverse events were more common in the ramucirumab group, including grade 3 neutropenia.
Based on this data, FOLFIRI plus ramucirumab is an acceptable second-line regimen for patients previously treated with FOLFOX-bevacizumab. Whether to continue bevacizumab in second-line chemotherapy or use ramucirumab in second-line chemotherapy has not yet been addressed in a clinical trial.
Panitumumab
Panitumumab is a fully humanized antibody against the EGFR. The U.S. Food and Drug Administration (FDA) approved panitumumab for use in patients with metastatic colorectal cancer refractory to chemotherapy.[41] In clinical trials, panitumumab demonstrated efficacy as a single agent or in combination therapy, which was consistent with the effects on PFS and OS with cetuximab. There appears to be a consistent class effect.
Evidence (panitumumab):
In a phase III trial, patients with chemotherapy-refractory colorectal cancer were randomly assigned to panitumumab or best supportive care.[41][Level of evidence B1]
Patients who received panitumumab experienced an improved PFS (8 weeks vs. 7.3 weeks; HR, 0.54; 95% CI, 0.44–0.66; P < .0001).
There was no difference in OS, which could be because 76% of patients on best supportive care crossed over to panitumumab.
In the Panitumumab Randomized Trial in Combination With Chemotherapy for Metastatic Colorectal Cancer to Determine Efficacy (PRIME [NCT00364013]) study, 1,183 patients were randomly assigned to FOLFOX4 with or without panitumumab as first-line therapy for metastatic colorectal cancer. The study was amended to enlarge the sample size to address patients with KRAS wild-type tumors and patients withKRAS-altered tumors separately.[42][Level of evidence B1]
For patients with KRAS wild-type tumors, a statistically significant improvement in PFS was observed in those who received panitumumab/FOLFOX4 compared with those who received only FOLFOX4 (HR, 0.80; 95% CI, 0.66–0.97; stratified log-rank P = .02).
Median PFS was 9.6 months (95% CI, 9.2–11.1 months) for patients who received panitumumab/FOLFOX4 and 8.0 months (95% CI, 7.5–9.3 months) for patients who received FOLFOX4. OS was not significantly different between the groups (HR, 0.83; 95% CI, 0.67–1.02; P = .072).
For patients with KRAS-altered tumors, PFS was worse with the addition of panitumumab (HR, 1.29; 95% CI, 1.04–1.62; stratified log-rank P = .02).
Median PFS was 7.3 months (95% CI, 6.3–8.0 months) for panitumumab/FOLFOX4 and 8.8 months (95% CI, 7.7–9.4 months) for FOLFOX4 alone.
Subsequently, a retrospective analysis evaluated patients with wild-type KRAS exon 2 wild-type status for other KRAS and BRAF variants.[43][Level of evidence C1]
Of the 620 patients who were initially identified as not having a variant in exon 2 of KRAS, 108 patients (17%) were found to have additional RAS variants and 53 patients (8%) were found to have BRAF variants. In a retrospective analysis, patients without any RAS or BRAF variants had a longer PFS (10.8 months vs. 9.2 months, P = .002) and OS (28.3 months vs. 20.9 months, P = .02) when assigned to the FOLFOX-4/panitumumab arm than the patients assigned to the FOLFOX-4 arm.
Similarly, the addition of panitumumab to a regimen of FOLFOX/bevacizumab resulted in a worse PFS and worse toxicity compared with a regimen of FOLFOX/bevacizumab alone in patients not selected for KRAS variant in metastatic rectal cancer (11.4 months vs. 10.0 months; HR, 1.27; 95% CI, 1.06–1.52).[44][Level of evidence B1]
In another study (NCT00339183), patients with metastatic colorectal cancer who had already received a fluoropyrimidine regimen were randomly assigned to either FOLFIRI or FOLFIRI/panitumumab.[45][Level of evidence B1]
In a post hoc analysis, patients with KRAS wild-type tumors experienced a statistically significant PFS advantage (HR, 0.73; 95% CI, 0.59–0.90; stratified log-rank P = .004).
Median PFS was 5.9 months (95% CI, 5.5–6.7 months) for FOLFIRI/panitumumab and 3.9 months (95% CI, 3.7–5.3 months) for FOLFIRI alone.
OS was not significantly different. Median OS was 14.5 months for the FOLFIRI/panitumumab group versus 12.5 months for the FOLFIRI alone group.
Patients with KRAS-altered tumors experienced no benefit from the addition of panitumumab.
Anti-EGFR antibody versus anti-VEGF antibody with first-line chemotherapy
In the management of patients with stage IV colorectal cancer, it is unknown whether patients with KRAS wild-type cancer should receive an anti-EGFR antibody with chemotherapy or an anti-VEGF antibody with chemotherapy. Two studies attempted to answer this question.[46,47]
Evidence (anti-EGFR antibody vs. anti-VEGF antibody with first-line chemotherapy):
The FIRE-3 study (NCT00433927) randomly assigned 592 patients with KRAS exon 2 wild-type tumors who were previously untreated to FOLFIRI plus cetuximab (297 patients) or FOLFIRI plus bevacizumab (295 patients). The primary end point of the study was objective response rate.[46][Level of evidence A1]
The objective response rate was not significantly different between the groups (objective response rate, 62.0%; 95% CI, 56.2–67.5 vs. objective response rate, 58.0%; 95% CI, 52.1–63.7; odds ratio, 1.18; 95% CI, 0.85–1.64; P = .18).
Median PFS was 10.0 months (95% CI, 8.8–10.8) in the cetuximab group and 10.3 months (95% CI, 9.8–11.3) in the bevacizumab group (HR, 1.06; 95% CI, 0.88–1.26; P = .55).
Median OS was 28.7 months (95% CI, 24.0–36.6) in the cetuximab group compared with 25.0 months (range, 22.7–27.6 months) in the bevacizumab group (HR, 0.77; 95% CI, 0.62–0.96; P = .017).
In a post hoc analysis of patients with expanded RAS wild-type tumors (sequencing for mutational hot spots within KRAS and NRAS genes, including exon 2 codons 12 and 13; exon 3 codons 59 and 61; and exon 4 codons 117 and 146), the median OS was 33.1 months (95% CI, 24.5–39.4) in the cetuximab group compared with 25.0 months (95% CI, 23.0–28.1) in the bevacizumab group (HR, 0.70; 95% CI, 0.54–0.90; P = .0059).[48]
Of note, only 52% of patients assigned to the bevacizumab arm subsequently received cetuximab or panitumumab.[49]
The Cancer and Leukemia Group B Intergroup study 80405 (NCT00265850) was presented at the American Society of Clinical Oncology meeting in 2014. This study randomly assigned 2,334 previously untreated patients with KRAS wild-type cancer to chemotherapy (FOLFOX or FOLFIRI) plus bevacizumab or chemotherapy plus cetuximab. OS was the primary end point.[47][Level of evidence B1]
There was no statistically significant difference in OS among the patients assigned to bevacizumab or cetuximab (for OS differences, chemotherapy/bevacizumab = 29.04 months [range, 25.66–31.21 months] vs. chemotherapy/cetuximab = 29.93 months [range, 27.56–31.21 months]; HR, 0.92 [0.78–1.09]; P = .34).
Based on these two studies, no apparent significant difference is evident about starting treatment with chemotherapy/bevacizumab or chemotherapy/cetuximab in patients with KRAS wild-type metastatic colorectal cancer. However, in patients with KRAS wild-type cancer, administration of an anti-EGFR antibody at some point during management improves OS.
Regorafenib
Regorafenib is an inhibitor of multiple tyrosine kinase pathways including VEGF. In 2012, the FDA granted approval for the use of regorafenib in patients who had progressed on previous therapy.
Evidence (regorafenib):
The safety and effectiveness of regorafenib were evaluated in a single, clinical study of 760 patients with previously treated metastatic colorectal cancer. Patients were randomly assigned in a 2:1 fashion to receive regorafenib or a placebo in addition to the best supportive care.[50,51]
Patients treated with regorafenib had a statistically significant improvement in OS (6.4 months in the regorafenib group vs. 5.0 months in the placebo group; HR, 0.77; 95% CI, 0.64–0.94; one-sided P = .0052).
Fruquintinib
Fruquintinib is an inhibitor of VEGF receptors 1, 2 and 3. In 2023, the FDA approved fruquintinib for adults with metastatic colorectal cancer who had previously received fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy and an anti-VEGF therapy. If patients had RAS wild-type disease and were medically appropriate, an anti-EGFR therapy was also required
Evidence (fruquintinib):
The phase III, international, double-blind, placebo-controlled FRESCO-2 trial (NCT04322539) included 691 patients with metastatic colorectal adenocarcinoma who had received all standard approved cytotoxic and targeted therapies. Patients had disease progression during, or were intolerant of, trifluridine-tipiracil, regorafenib, or both. Patients had received a median of four lines of prior systemic therapy. Patients were randomly assigned in a 2:1 fashion to receive one of the following regimens:
Fruquintinib (5 mg orally once daily on days 1–21 of a 28-day cycle).
Placebo (orally once daily on days 1–21 of a 28-day cycle).
All patients received best supportive care. A total of 461 patients received fruquintinib, and 230 received placebo. The primary end point was OS.[52] The results were as follows:
The median OS was significantly longer in the fruquintinib group (7.4 months; 95% CI, 6.7–8.2) than in the placebo group (4.8 months; 95% CI, 4.0–5.8) (HR, 0.66; 95% CI, 0.55–0.80; P < .0001).[52][Level of evidence A1]
The median PFS was 3.7 months (95% CI. 3.5–3.8) in the fruquintinib group and 1.8 months (95% CI, 1.8–1.9) in the placebo group (HR, 0.26; 95% CI, 0.21–0.34; P < .001).
Subgroup analyses demonstrated the benefit of fruquintinib as opposed to placebo in most subgroups. Notably, this benefit was seen in patients with both RAS variants and RAS wild-type disease, patients with liver metastases, and patients pretreated with trifluridine-tipiracil with or without regorafenib.
The disease control rate was significantly longer in the fruquintinib group (56%) than in the placebo group (16%), with an adjusted difference of 39% (95% CI, 32.8%–46.0%; P < .0001).
Grade 3 or higher adverse events occurred in 65% of patients in the fruquintinib group. The most common adverse events were hypertension (14%), asthenia (8%), abnormal hepatic function (8%), dermatologic toxicity (7%), and hand-foot syndrome (6%). Grade 3 or higher adverse events occurred in 50% of patients in the placebo group. The most common were abnormal hepatic function (9%), infection (6%), and asthenia (4%).
Trifluridine-tipiracil
Trifluridine-tipiracil (Lonsurf; also called TAS-102) is an orally administered combination of a thymidine-based nucleic acid analogue, trifluridine, and a thymidine phosphorylase inhibitor, tipiracil hydrochloride. Trifluridine, in its triphosphate form, inhibits thymidylate synthase; therefore, trifluridine, in this form, has an anti-tumor effect. Tipiracil hydrochloride is a potent inhibitor of thymidine phosphorylase, which actively degrades trifluridine. The combination of trifluridine and tipiracil allows for adequate plasma levels of trifluridine.
Evidence (trifluridine-tipiracil):
A phase III double-blind study (RECOURSE [NCT01607957]) randomly assigned 800 patients with stage IV colorectal cancer whose cancer had been refractory to two previous therapies. Patients were required to have received 5-FU, oxaliplatin, irinotecan, bevacizumab and, if the patients had KRAS wild-type cancer, cetuximab or panitumumab. Patients were randomly assigned in a 2:1 ratio to receive best supportive care plus trifluridine-tipiracil (n = 534) or placebo (n = 266). The median age of patients was 63 years, and most patients (60%–63%) received four or more previous lines of therapy. All patients had formerly received a fluoropyrimidine, irinotecan, oxaliplatin, and bevacizumab, and 52% of them had received an EGFR inhibitor. Approximately 20% of the patients had received previous treatment with regorafenib.[53][Level of evidence A1]
Trifluridine-tipiracil was administered at 35 mg/m2 twice daily with meals for 5 days, with 2 days of rest for 2 weeks, followed by a 14-day rest period.
The primary end point of the study was OS. The median OS for patients with metastatic colorectal cancer who received trifluridine-tipiracil was 7.1 months compared with 5.3 months for those who received a placebo (HR, 0.68; P < .0001).
The median PFS in the trifluridine-tipiracil arm was 2 months versus 1.7 months with a placebo (HR, 0.48; P < .0001).
Secondary end points focused on PFS, overall response rate, and disease control rate.
The overall response rate was 1.6% with trifluridine-tipiracil, which consisted of a complete response in one patient and partial responses in other patients. The overall response rate with a placebo was 0.4% (P = .29).
The FDA approved trifluridine-tipiracil for the treatment of patients with metastatic colorectal cancer, based on the results of the RECOURSE trial.
Evidence (combination of trifluridine-tipiracil and bevacizumab):
A phase III, international, multi-institutional trial (SUNLIGHT [NCT04737187]) included 492 patients with stage IV colorectal cancer whose cancer was refractory to up to two prior chemotherapy regimens. Patients were required to have received 5-FU, oxaliplatin, irinotecan, an anti-VEGF monoclonal antibody, or an anti-EGFR monoclonal antibody (for patients with RAS wild-type disease). Patients were randomly assigned 1:1 to receive either trifluridine-tipiracil monotherapy (n = 246) or trifluridine-tipiracil combined with bevacizumab (n = 246). The median patient age was 62 years for the combination arm, and 64 years for the monotherapy arm, and most patients (93% and 91%, respectively) had received two prior lines of therapy. More than 98% of patients in both arms had received 5-FU, irinotecan, and oxaliplatin, and more than 93% of patients with RAS wild-type variants in both arms had received anti-EGFR monoclonal antibody therapy. The median follow-up was 14.2 months. Trifluridine-tipiracil was given at 35 mg/m2 twice daily on days 1 to 5 and 8 to 12 of a 28-day cycle. Bevacizumab was given on days 1 and 15 of each cycle at 5 mg/kg. The primary end point of the study was OS.[54]
The median OS was 10.8 months for patients who received trifluridine-tipiracil and bevacizumab and 7.5 months for patients who received trifluridine-tipiracil monotherapy (HR, 0.61; 95% CI, 0.49–0.77; P < .001).[54][Level of evidence A1]
OS was significant across subgroups, including patients with RAS variants and wild-type variants, patients with microsatellite instability-high (MSI-H) and microsatellite stability cancers, and both for patients previously treated with bevacizumab and bevacizumab-naïve patients.
The median PFS was 5.6 months in the combination arm and 2.4 months in the trifluridine-tipiracil monotherapy arm (HR, 0.44; 95% CI, 0.36–0.54; P < .001).
Secondary end points focused on PFS, overall response rate, and safety.
The overall response rate was 6.1% for the combination arm and 1.2% for the monotherapy arm.
Adverse events leading to therapy discontinuation were observed in 12.6% of patients in both arms. Dose reductions occurred in 16.3% of patients in the combination group and 12.2% of patients in the trifluridine-tipiracil monotherapy group. The most common adverse event was neutropenia, with grade 3 or 4 neutropenia observed in 43% of patients in the combination arm and 32% of patients in the monotherapy arm.
The FDA approved the combination of trifluridine-tipiracil and bevacizumab for the treatment of patients with previously treated metastatic colorectal cancer based on the results of the SUNLIGHT trial.
Encorafenib with cetuximab for patients with BRAF V600E variants
BRAF V600E variants occur in about 10% of metastatic colorectal cancers and are an indicator of poor prognosis. Unlike in melanoma, BRAF inhibitor monotherapy has not shown a benefit in colorectal cancer, and multiple studies have evaluated concurrent targeting of the EGFR-MAPK pathway.
Evidence (encorafenib with cetuximab for patients with BRAF V600E variants):
Encorafenib (BRAF inhibitor), binimetinib (MEK inhibitor), and cetuximab (EGFR inhibitor): In the international, open-label, randomized, phase III BEACON trial, patients with metastatic colorectal cancer and BRAF V600E variants who previously received one or two treatment regimens were enrolled.[55] The trial randomly assigned 665 patients in a 1:1:1 ratio to receive one of the following regimens:
Triplet therapy: encorafenib (300 mg PO daily), binimetinib (45 mg PO twice daily), and cetuximab (400 mg/m2 IV loading dose followed by 250 mg/m2 IV weekly) (n = 224).
Doublet therapy: encorafenib and cetuximab (as per triplet therapy dosing) (n = 220).
Control group: FOLFIRI or irinotecan (every 2 weeks) with cetuximab (400 mg/m2 IV loading dose followed by 250 mg/m2 IV weekly) (n = 221).
The primary end points were OS and objective response in the triplet-therapy group when compared with the control group.
The OS was 9.0 months in the triplet-therapy arm and 5.4 months in the control group (HR, 0.52; 95% CI, 0.39–0.70, P < .0001).[55][Level of evidence A1]
Grade 3 or higher side effects occurred in 58% of patients in the triplet-therapy arm, with 10% of patients experiencing diarrhea and 11% of patients experiencing anemia. Grade 3 or higher side effects occurred in 50% of patients in the doublet-therapy arm and 61% of patients in the control arm. Fourteen percent of patients who received the doublet regimen developed melanocytic nevi.
Updated data were presented in abstract form in 2020:[56]
The median OS was 9.3 months in both the triplet-therapy and doublet-therapy arms and 5.9 months in the control arm (HR, 0.60 for triplet therapy vs. control; 95% CI, 0.47–0.75; HR, 0.61 for doublet therapy vs. control; 95% CI, 0.48–0.77).
The objective response rate was 26.8% for patients who received triplet therapy (95% CI, 21.1%–33.1%) and 19.5% for patients who received doublet therapy (95% CI, 14.5%–
Based on these data, the FDA approved the combination of encorafenib with cetuximab for patients with previously treated metastatic colorectal cancer and BRAF V600E variants.
Sotorasib with panitumumab for patients with KRAS G12C variants
KRAS G12C variants are found in approximately 4% of patients with colorectal cancer and are associated with poor prognosis.[57–60] Sotorasib and adagrasib are two of the first KRAS G12C–specific inhibitors to show benefit in patients with KRAS G12C–mutated cancers.[61,62] Given that EGFR reactivation is a well-described resistance mechanism to KRAS G12C inhibition, sotorasib was combined with the anti-EGFR antibody panitumumab in patients with colorectal cancer and KRAS G12C variants.
The phase III, multicenter, open-label CodeBreaK 300 trial (NCT05198934) included patients with metastatic colorectal cancer and KRAS G12C variants who previously received treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.[61] The trial randomly assigned 160 patients 1:1:1 to receive one of the following regimens:
Doublet therapy with sotorasib 960 mg once daily plus panitumumab (6 mg/kg IV every 2 weeks) (n = 53).
Doublet therapy with sotorasib 240 mg once daily plus panitumumab (6 mg/kg IV every 2 weeks) (n = 53).
Investigator’s choice standard-of-care therapy with trifluridine-tipiracil (35 mg/m2) or regorafenib (160 mg once daily) (control group).
The primary end point was PFS assessed by blinded independent central review according to RECIST 1.1. Secondary end points included OS and objective response rate.
The median PFS was 5.6 months (95% CI, 4.2–6.3) in the 960 mg-sotorasib/panitumumab group, 3.9 months (95% CI, 3.7–5.8) in the 240 mg-sotorasib/panitumumab group, and 2.2 months (95% CI, 1.9–3.9) in the standard-of-care group.[61][Level of evidence B1]
The HR for progression of disease or death was 0.49 (95% CI, 0.3–0.8; P = .006) for the 960 mg-sotorasib/panitumumab group and 0.58 (95% CI, 0.36–0.98; P = .03) for the 240 mg-sotorasib/panitumumab group.
The objective response rate was 26.4% (95% CI, 15.3%–40.3%) in the 960 mg-sotorasib/panitumumab group, 5.7% (95% CI, 1.2%–15.7%) in the 240 mg-sotorasib/panitumumab group, and 0% (95% CI, 0.0%–6.6%) in the standard-of-care group. OS data are still not mature. However, at data cutoff the HRs were 0.77 (95% CI, 0.4–1.45) for the 960 mg-sotorasib/panitumumab group and 0.91 (95% CI, 0.48–1.71) for the 240 mg-sotorasib/panitumumab group when compared with standard-of-care therapy.
Grade 3 or higher side effects occurred in 35.8% of patients who received 960 mg sotorasib/panitumumab, 30.2% of patients who received 240 mg sotorasib/panitumumab, and 43.1% of patients who received the standard of care. The most common adverse effects with combined sotorasib and panitumumab therapy were skin-related toxicities and hypomagnesemia.
Second-line chemotherapy
Second-line chemotherapy with irinotecan in patients treated with 5-FU/LV as first-line therapy demonstrated improved OS when compared with either infusional 5-FU or supportive care.[63–66]
Similarly, a phase III trial randomly assigned patients who progressed on irinotecan and 5-FU/LV to bolus and infusional 5-FU/LV, single-agent oxaliplatin, or FOLFOX4. The median TTP for FOLFOX4 versus 5-FU/LV was 4.6 months versus 2.7 months (stratified log-rank test, 2-sided P < .001).[67][Level of evidence B1]
Immunotherapy
Approximately 4% of patients with stage IV colorectal cancer have tumors that are mismatch repair deficient (dMMR) or microsatellite unstable/MSI-H. The MSI-H phenotype is associated with germline defects in the MLH1, MSH2, MSH6, and PMS2 genes and is the primary phenotype observed in tumors from patients with hereditary nonpolyposis colorectal cancer (HNPCC) or Lynch syndrome. Patients can also have the MSI-H phenotype because one of these genes was silenced via DNA methylation. Testing for microsatellite instability can be done with molecular genetic tests, which look for microsatellite instability in the tumor tissue, or with immunohistochemistry, which looks for the loss of mismatch repair proteins. MSI-H status has historically been prognostic of increased survival for patients with earlier-stage disease and since 2015, has also been found to predict tumor response to checkpoint inhibition.
The FDA approved pembrolizumab for use in patients with treatment-naïve, metastatic, dMMR/MSI-H colorectal cancer in 2020. Studies regarding first-line treatment with dual checkpoint inhibitors are ongoing. The FDA approved the anti-programmed cell death protein 1 (PD-1) antibodies pembrolizumab in 2017 and nivolumab in 2017 for the treatment of patients with microsatellite-unstable tumors who had previously received 5-FU, oxaliplatin, and irinotecan-based therapy. In 2018, the FDA granted accelerated approval for the combination of nivolumab with ipilimumab (a CTLA-4 inhibitor) to treat MSI-H colorectal cancers that progressed after prior 5-FU, oxaliplatin, and irinotecan-based therapies.
First-line immunotherapy
Pembrolizumab monotherapy
Evidence (pembrolizumab monotherapy):
In the phase III, open-label, international, randomized KEYNOTE-177 trial (NCT02563002), 307 patients with treatment-naïve MSI-H or dMMR metastatic colorectal cancer were randomly assigned in a 1:1 ratio to receive either pembrolizumab (200 mg every 3 weeks) or chemotherapy (FOLFIRI or modified FOLFOX-6 with or without bevacizumab or cetuximab).[68]
The median PFS was 16.5 months for patients who received pembrolizumab and 8.2 months for patients who received chemotherapy (HR, 0.60; 95% CI, 0.45–0.80; P = .0002).[68][Level of evidence A3]
The PFS in prespecified subgroups showed HRs that favored the pembrolizumab arm, except in patients with KRAS or NRAS variants.
The objective response rate was 43.8% in the pembrolizumab arm and 33.3% in the chemotherapy arm. The median duration of response was not reached in the pembrolizumab arm (range, 2.3–41.4 months) and was 10.6 months in the chemotherapy arm (range, 2.8–37.5 months).
Grade 3 or higher adverse events occurred in 56% of patients who received pembrolizumab (with 9% experiencing grade 3 or higher infusion-related adverse events), compared with 78% of patients who received chemotherapy.
A final review of OS, presented in abstract form, showed that median OS was not reached in the pembrolizumab arm and was 36.7 months in the chemotherapy arm (HR, 0.74; 95% CI, 0.53–1.03; P = .0359).[69]
Nivolumab and ipilimumab
Evidence (nivolumab and ipilimumab):
In a single-arm cohort of the phase II, multicenter CheckMate-142 study (NCT02060188) presented in abstract form, 45 treatment-naïve patients with MSI-H/dMMR metastatic colorectal cancer received nivolumab (3 mg/kg every 2 weeks) with ipilimumab (1 mg/kg every 6 weeks). The primary end point was objective response rate.[70]
The objective response rate was 69% among all enrolled patients and 80% for patients with KRAS variants (n = 10).[70][Level of evidence C2]
At a 2-year clinical follow-up, the median PFS and OS had not been reached.
In the CheckMate 8HW trial (NCT04008030), published in abstract form, 303 patients who had received various lines of treatment were randomly assigned to receive either nivolumab and ipilimumab (n = 202) or chemotherapy alone (n = 101). Some patients were also randomly assigned to receive nivolumab, but results from these patients were not presented in the abstract. Treatments were continued until progression or unacceptable toxicity (all arms), or for up to 2 years (nivolumab-ipilimumab arm). A total of 171 patients who received nivolumab and ipilimumab and 84 patients who received chemotherapy alone were centrally confirmed to have dMMR/MSI-H metastatic colorectal cancer.[71]
At a median follow-up of 31.5 months, the PFS was superior for patients who received nivolumab and ipilimumab compared with those who received chemotherapy alone (HR, 0.21; 97.91% CI, 0.13–0.35; P < .0001). Of note, in the chemotherapy arm, 67% of patients received subsequent immunotherapy.
Two grade 5 deaths occurred in the nivolumab-ipilimumab arm. Grade 3 to 4 events occurred in 23% of patients in the nivolumab-ipilimumab arm and 48% of patients in the chemotherapy-alone arm.
Second-line immunotherapy
Pembrolizumab monotherapy
Evidence (pembrolizumab monotherapy):
The FDA approval of pembrolizumab monotherapy was based on data from 149 patients with MSI-H or dMMR cancers enrolled across five uncontrolled, multicohort, multicenter, single-arm clinical trials. Ninety patients had colorectal cancer, and 59 patients were diagnosed with 1 of 14 other cancer types. Patients received either 200 mg of pembrolizumab every 3 weeks or 10 mg/kg of pembrolizumab every 2 weeks. Treatment continued until unacceptable toxicity or disease progression occurred. The major efficacy outcome measures were objective response rate (assessed by blinded independent central radiologists’ review in accordance with Response Evaluation Criteria in Solid Tumors [RECIST] 1.1) and response duration.
The objective response rate was 39.6% (95% CI, 31.7%–47.9%).
Responses lasted 6 months or longer for 78% of patients who responded to pembrolizumab. There were 11 complete responses and 48 partial responses.
The objective response rate was similar whether patients were diagnosed with colorectal cancer (36%) or a different cancer (46% across the 14 other cancer types).
Nivolumab monotherapy
Evidence (nivolumab monotherapy):
In the CheckMate-142 trial (NCT02060188), 74 patients with previously treated dMMR/MSI-H colorectal cancer were enrolled in an open-label, single-arm, phase II study to receive nivolumab (3 mg/kg every 2 weeks). The primary end point was objective response as per RECIST 1.1.[72]
The objective response rate was 31.1% (95% CI, 20.8%–42.9%).
Grade 3 to 4 treatment-related adverse events occurred in 21% of patients.
Nivolumab and ipilimumab
Evidence (nivolumab and ipilimumab):
CheckMate-142 (NCT02060188) was a multicenter, open-label, phase II trial with a cohort for patients with recurrent or metastatic dMMR and/or MSI-H colorectal cancer who had progressed on, were intolerant of, or declined at least one line of chemotherapy (including 5-FU and oxaliplatin and/or irinotecan). The trial enrolled 119 patients who received four doses of nivolumab (3 mg/kg) and ipilimumab (1 mg/kg) every 3 weeks (induction), then nivolumab (3 mg/kg IV) every 2 weeks (maintenance). The primary end point was objective response rate.[72]
The objective response rate was 55% (95% CI, 45.2%–63.8%).
Among patients experiencing a response, 83% had responses lasting more than 6 months.
Grade 3 to 4 treatment-related adverse events occurred in 32% of patients.
Palliative therapy
Palliative radiation therapy,[11,66] chemotherapy,[13,73–78] and chemoradiation therapy [79,80] may be indicated. Palliative, endoscopically-placed stents may be used to relieve obstruction.[81]
Treatment of Liver Metastasis
Approximately 15% to 25% of patients with colorectal cancer will present with liver metastases at diagnosis, and another 25% to 50% will develop metachronous hepatic metastasis after resection of the primary tumor.[82–84] Although only a small proportion of patients with liver metastasis are candidates for surgical resection, advances in tumor ablation techniques and in both regional and systemic chemotherapy administration provide a number of treatment options. These include:
Hepatic metastasis may be considered resectable on the basis of the following factors:[65,85–97]
Limited number of lesions.
Intrahepatic locations of lesions.
Lack of major vascular involvement.
Absent or limited extrahepatic disease.
Sufficient functional hepatic reserve.
For patients with resectable hepatic metastasis, a negative margin resection has been associated with 5-year survival rates of 25% to 40% in mostly nonrandomized studies, such as the North Central Cancer Treatment Group trial NCCTG-934653 (NCT00002575).[98–102][Level of evidence C3] Improved surgical techniques and advances in preoperative imaging have improved patient selection for resection. In addition, multiple studies with multiagent chemotherapy have demonstrated that patients with metastatic disease isolated to the liver, which historically would be considered unresectable, can occasionally be made resectable after the administration of neoadjuvant chemotherapy.[103]
For patients with unresectable liver metastases, excellent outcomes have been achieved with liver transplant. The optimal patient cohort for this therapy is still being determined, but in general, the goal is to achieve good initial systemic control with chemotherapy, followed by transplant. In one study of 91 patients, 11% underwent live donor liver transplant. At a median follow-up of 1.5 years after transplant, the recurrence-free survival rate was 62%, and the OS rate was 100%.[104][Level of evidence C3]
In the TRANSMET study (NCT02597348), published in abstract form, 94 patients were randomly assigned to receive either chemotherapy and liver transplant (n = 47) or chemotherapy alone (n = 47). In an intent-to-treat analysis, the 5-year OS rate was 57% in the chemotherapy and liver transplant arm and 13% in the chemotherapy-alone arm. In a per-protocol analysis, the 5-year OS rate was 73% in the chemotherapy and liver transplant arm and 9% in the chemotherapy-alone arm.[105][Level of evidence A1]
Neoadjuvant chemotherapy for unresectable liver metastases
Patients with hepatic metastases that are deemed unresectable will occasionally become candidates for resection if they have a good response to chemotherapy. These patients have 5-year survival rates similar to patients who initially had resectable disease.[103]
Local ablation for unresectable liver metastases
Radiofrequency ablation has emerged as a safe technique (2% major morbidity and <1% mortality rate) that may provide long-term tumor control.[106–112] Radiofrequency ablation and cryosurgical ablation remain options for patients with tumors that cannot be resected and for patients who are not candidates for liver resection.
Adjuvant chemotherapy
The role of adjuvant chemotherapy after potentially curative resection of liver metastases is uncertain.
Evidence (adjuvant chemotherapy):
A trial of hepatic arterial floxuridine and dexamethasone plus systemic 5-FU/LV compared with systemic 5-FU/LV alone showed improved 2-year PFS (57% vs. 42%; P =.07) and OS (86% vs. 72%; P = .03) for patients in the combined therapy arm but did not show a significant statistical difference in median survival when compared with systemic 5-FU therapy alone.[113][Level of evidence A1]
Median survival in the combined therapy arm was 72.2 months versus 59.3 months in the monotherapy arm (P = .21).
A second trial preoperatively randomly assigned patients with one to three potentially resectable colorectal hepatic metastases to either no further therapy or postoperative hepatic arterial floxuridine plus systemic 5-FU.[114] Among those randomly assigned patients, 27% were deemed ineligible at the time of surgery, leaving only 75 patients evaluable for recurrence and survival.
While liver recurrence was decreased, median or 4-year survival was not significantly different between the patient groups.
Additional studies are required to evaluate this treatment approach and to determine whether more effective systemic combination chemotherapy alone would provide results similar to hepatic intra-arterial therapy plus systemic treatment.
Intra-arterial chemotherapy after liver resection
Hepatic intra-arterial chemotherapy with floxuridine for liver metastases has produced higher overall response rates but no consistent improvement in survival when compared with systemic chemotherapy.[93,115–119] Controversy regarding the efficacy of regional chemotherapy was the basis of a large, multicenter, phase III trial (Leuk-9481 [NCT00002716]) of hepatic arterial infusion versus systemic chemotherapy. The use of combination intra-arterial chemotherapy with hepatic radiation therapy, especially employing focal radiation of metastatic lesions, is under evaluation.[120]
Several studies show increased local toxic effects after hepatic infusional therapy, including liver function abnormalities and fatal biliary sclerosis.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Wanebo HJ, Koness RJ, Vezeridis MP, et al.: Pelvic resection of recurrent rectal cancer. Ann Surg 220 (4): 586-95; discussion 595-7, 1994. [PUBMED Abstract]
Girard P, Ducreux M, Baldeyrou P, et al.: Surgery for lung metastases from colorectal cancer: analysis of prognostic factors. J Clin Oncol 14 (7): 2047-53, 1996. [PUBMED Abstract]
McAfee MK, Allen MS, Trastek VF, et al.: Colorectal lung metastases: results of surgical excision. Ann Thorac Surg 53 (5): 780-5; discussion 785-6, 1992. [PUBMED Abstract]
Headrick JR, Miller DL, Nagorney DM, et al.: Surgical treatment of hepatic and pulmonary metastases from colon cancer. Ann Thorac Surg 71 (3): 975-9; discussion 979-80, 2001. [PUBMED Abstract]
Tepper JE, O’Connell M, Donna H, et al.: Analysis of surgical salvage after failure of primary therapy in rectal cancer: results from INT 0114. [Abstract] Proceedings of the American Society of Clinical Oncology 21: A-507, 2002.
Rodriguez-Bigas MA, Herrera L, Petrelli NJ: Surgery for recurrent rectal adenocarcinoma in the presence of hydronephrosis. Am J Surg 164 (1): 18-21, 1992. [PUBMED Abstract]
Ogunbiyi OA, McKenna K, Birnbaum EH, et al.: Aggressive surgical management of recurrent rectal cancer–is it worthwhile? Dis Colon Rectum 40 (2): 150-5, 1997. [PUBMED Abstract]
Vermaas M, Ferenschild FT, Verhoef C, et al.: Total pelvic exenteration for primary locally advanced and locally recurrent rectal cancer. Eur J Surg Oncol 33 (4): 452-8, 2007. [PUBMED Abstract]
Lowy AM, Rich TA, Skibber JM, et al.: Preoperative infusional chemoradiation, selective intraoperative radiation, and resection for locally advanced pelvic recurrence of colorectal adenocarcinoma. Ann Surg 223 (2): 177-85, 1996. [PUBMED Abstract]
Valentini V, Morganti AG, De Franco A, et al.: Chemoradiation with or without intraoperative radiation therapy in patients with locally recurrent rectal carcinoma: prognostic factors and long term outcome. Cancer 86 (12): 2612-24, 1999. [PUBMED Abstract]
Haddock MG, Gunderson LL, Nelson H, et al.: Intraoperative irradiation for locally recurrent colorectal cancer in previously irradiated patients. Int J Radiat Oncol Biol Phys 49 (5): 1267-74, 2001. [PUBMED Abstract]
Petrelli N, Herrera L, Rustum Y, et al.: A prospective randomized trial of 5-fluorouracil versus 5-fluorouracil and high-dose leucovorin versus 5-fluorouracil and methotrexate in previously untreated patients with advanced colorectal carcinoma. J Clin Oncol 5 (10): 1559-65, 1987. [PUBMED Abstract]
Petrelli N, Douglass HO, Herrera L, et al.: The modulation of fluorouracil with leucovorin in metastatic colorectal carcinoma: a prospective randomized phase III trial. Gastrointestinal Tumor Study Group. J Clin Oncol 7 (10): 1419-26, 1989. [PUBMED Abstract]
Scheithauer W, Rosen H, Kornek GV, et al.: Randomised comparison of combination chemotherapy plus supportive care with supportive care alone in patients with metastatic colorectal cancer. BMJ 306 (6880): 752-5, 1993. [PUBMED Abstract]
Expectancy or primary chemotherapy in patients with advanced asymptomatic colorectal cancer: a randomized trial. Nordic Gastrointestinal Tumor Adjuvant Therapy Group. J Clin Oncol 10 (6): 904-11, 1992. [PUBMED Abstract]
Buyse M, Thirion P, Carlson RW, et al.: Relation between tumour response to first-line chemotherapy and survival in advanced colorectal cancer: a meta-analysis. Meta-Analysis Group in Cancer. Lancet 356 (9227): 373-8, 2000. [PUBMED Abstract]
Leichman CG, Fleming TR, Muggia FM, et al.: Phase II study of fluorouracil and its modulation in advanced colorectal cancer: a Southwest Oncology Group study. J Clin Oncol 13 (6): 1303-11, 1995. [PUBMED Abstract]
Saltz LB, Cox JV, Blanke C, et al.: Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med 343 (13): 905-14, 2000. [PUBMED Abstract]
de Gramont A, Figer A, Seymour M, et al.: Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 18 (16): 2938-47, 2000. [PUBMED Abstract]
Douillard JY, Cunningham D, Roth AD, et al.: Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet 355 (9209): 1041-7, 2000. [PUBMED Abstract]
Sanoff HK, Sargent DJ, Campbell ME, et al.: Five-year data and prognostic factor analysis of oxaliplatin and irinotecan combinations for advanced colorectal cancer: N9741. J Clin Oncol 26 (35): 5721-7, 2008. [PUBMED Abstract]
Tournigand C, André T, Achille E, et al.: FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol 22 (2): 229-37, 2004. [PUBMED Abstract]
Colucci G, Gebbia V, Paoletti G, et al.: Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell’Italia Meridionale. J Clin Oncol 23 (22): 4866-75, 2005. [PUBMED Abstract]
Fuchs CS, Marshall J, Mitchell E, et al.: Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol 25 (30): 4779-86, 2007. [PUBMED Abstract]
Van Cutsem E, Twelves C, Cassidy J, et al.: Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol 19 (21): 4097-106, 2001. [PUBMED Abstract]
Hoff PM, Ansari R, Batist G, et al.: Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 19 (8): 2282-92, 2001. [PUBMED Abstract]
Díaz-Rubio E, Tabernero J, Gómez-España A, et al.: Phase III study of capecitabine plus oxaliplatin compared with continuous-infusion fluorouracil plus oxaliplatin as first-line therapy in metastatic colorectal cancer: final report of the Spanish Cooperative Group for the Treatment of Digestive Tumors Trial. J Clin Oncol 25 (27): 4224-30, 2007. [PUBMED Abstract]
Porschen R, Arkenau HT, Kubicka S, et al.: Phase III study of capecitabine plus oxaliplatin compared with fluorouracil and leucovorin plus oxaliplatin in metastatic colorectal cancer: a final report of the AIO Colorectal Study Group. J Clin Oncol 25 (27): 4217-23, 2007. [PUBMED Abstract]
Hurwitz H, Fehrenbacher L, Novotny W, et al.: Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350 (23): 2335-42, 2004. [PUBMED Abstract]
Saltz LB, Clarke S, Díaz-Rubio E, et al.: Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 26 (12): 2013-9, 2008. [PUBMED Abstract]
Cassidy J, Clarke S, Díaz-Rubio E, et al.: Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J Clin Oncol 26 (12): 2006-12, 2008. [PUBMED Abstract]
Giantonio BJ, Catalano PJ, Meropol NJ, et al.: High-dose bevacizumab improves survival when combined with FOLFOX4 in previously treated advanced colorectal cancer: results from the Eastern Cooperative Oncology Group (ECOG) study E3200. [Abstract] J Clin Oncol 23 (Suppl 16): A-2, 1s, 2005.
Loupakis F, Cremolini C, Masi G, et al.: Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med 371 (17): 1609-18, 2014. [PUBMED Abstract]
Cunningham D, Humblet Y, Siena S, et al.: Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351 (4): 337-45, 2004. [PUBMED Abstract]
Van Cutsem E, Köhne CH, Hitre E, et al.: Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med 360 (14): 1408-17, 2009. [PUBMED Abstract]
Tol J, Koopman M, Cats A, et al.: Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl J Med 360 (6): 563-72, 2009. [PUBMED Abstract]
Maughan TS, Adams RA, Smith CG, et al.: Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 377 (9783): 2103-14, 2011. [PUBMED Abstract]
Adams RA, Meade AM, Seymour MT, et al.: Intermittent versus continuous oxaliplatin and fluoropyrimidine combination chemotherapy for first-line treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet Oncol 12 (7): 642-53, 2011. [PUBMED Abstract]
Van Cutsem E, Tabernero J, Lakomy R, et al.: Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol 30 (28): 3499-506, 2012. [PUBMED Abstract]
Tabernero J, Yoshino T, Cohn AL, et al.: Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol 16 (5): 499-508, 2015. [PUBMED Abstract]
Van Cutsem E, Peeters M, Siena S, et al.: Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 25 (13): 1658-64, 2007. [PUBMED Abstract]
Douillard JY, Siena S, Cassidy J, et al.: Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 28 (31): 4697-705, 2010. [PUBMED Abstract]
Douillard JY, Oliner KS, Siena S, et al.: Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 369 (11): 1023-34, 2013. [PUBMED Abstract]
Hecht JR, Mitchell E, Chidiac T, et al.: A randomized phase IIIB trial of chemotherapy, bevacizumab, and panitumumab compared with chemotherapy and bevacizumab alone for metastatic colorectal cancer. J Clin Oncol 27 (5): 672-80, 2009. [PUBMED Abstract]
Peeters M, Price TJ, Cervantes A, et al.: Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol 28 (31): 4706-13, 2010. [PUBMED Abstract]
Heinemann V, von Weikersthal LF, Decker T, et al.: FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol 15 (10): 1065-75, 2014. [PUBMED Abstract]
Venook AP, Niedzwiecki D, Lenz HJ, et al.: CALGB/SWOG 80405: Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC). [Abstract] J Clin Oncol 32 (Suppl 5): A-LBA3, 2014.
Stintzing S, Modest DP, Rossius L, et al.: FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): a post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol 17 (10): 1426-1434, 2016. [PUBMED Abstract]
Modest DP, Stintzing S, von Weikersthal LF, et al.: Impact of Subsequent Therapies on Outcome of the FIRE-3/AIO KRK0306 Trial: First-Line Therapy With FOLFIRI Plus Cetuximab or Bevacizumab in Patients With KRAS Wild-Type Tumors in Metastatic Colorectal Cancer. J Clin Oncol 33 (32): 3718-26, 2015. [PUBMED Abstract]
Grothey A, Sobrero AF, Siena S, et al.: Results of a phase III randomized, double-blind, placebo-controlled, multicenter trial (CORRECT) of regorafenib plus best supportive care (BSC) versus placebo plus BSC in patients (pts) with metastatic colorectal cancer (mCRC) who have progressed after standard therapies. [Abstract] J Clin Oncol 30 (Suppl 4): A-LBA385, 2012.
Grothey A, Van Cutsem E, Sobrero A, et al.: Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 381 (9863): 303-12, 2013. [PUBMED Abstract]
Dasari A, Lonardi S, Garcia-Carbonero R, et al.: Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet 402 (10395): 41-53, 2023. [PUBMED Abstract]
Mayer RJ, Van Cutsem E, Falcone A, et al.: Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med 372 (20): 1909-19, 2015. [PUBMED Abstract]
Prager GW, Taieb J, Fakih M, et al.: Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer. N Engl J Med 388 (18): 1657-1667, 2023. [PUBMED Abstract]
Kopetz S, Grothey A, Yaeger R, et al.: Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N Engl J Med 381 (17): 1632-1643, 2019. [PUBMED Abstract]
Kopetz S, Grothey A, Van Cutsem E, et al.: Encorafenib plus cetuximab with or without binimetinib for BRAF V600E metastatic colorectal cancer: updated survival results from a randomized, three-arm, phase III study versus choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). [Abstract] J Clin Oncol 38 (15) (suppl): A-4001, 2020. Available online. Last accessed January 30, 2025.
Fakih M, Tu H, Hsu H, et al.: Real-World Study of Characteristics and Treatment Outcomes Among Patients with KRAS p.G12C-Mutated or Other KRAS Mutated Metastatic Colorectal Cancer. Oncologist 27 (8): 663-674, 2022. [PUBMED Abstract]
Lee JK, Sivakumar S, Schrock AB, et al.: Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol 6 (1): 91, 2022. [PUBMED Abstract]
Neumann J, Zeindl-Eberhart E, Kirchner T, et al.: Frequency and type of KRAS mutations in routine diagnostic analysis of metastatic colorectal cancer. Pathol Res Pract 205 (12): 858-62, 2009. [PUBMED Abstract]
Henry JT, Coker O, Chowdhury S, et al.: Comprehensive Clinical and Molecular Characterization of KRAS G12C-Mutant Colorectal Cancer. JCO Precis Oncol 5: , 2021. [PUBMED Abstract]
Fakih MG, Salvatore L, Esaki T, et al.: Sotorasib plus Panitumumab in Refractory Colorectal Cancer with Mutated KRAS G12C. N Engl J Med 389 (23): 2125-2139, 2023. [PUBMED Abstract]
Yaeger R, Weiss J, Pelster MS, et al.: Adagrasib with or without Cetuximab in Colorectal Cancer with Mutated KRAS G12C. N Engl J Med 388 (1): 44-54, 2023. [PUBMED Abstract]
Rothenberg ML, Eckardt JR, Kuhn JG, et al.: Phase II trial of irinotecan in patients with progressive or rapidly recurrent colorectal cancer. J Clin Oncol 14 (4): 1128-35, 1996. [PUBMED Abstract]
Conti JA, Kemeny NE, Saltz LB, et al.: Irinotecan is an active agent in untreated patients with metastatic colorectal cancer. J Clin Oncol 14 (3): 709-15, 1996. [PUBMED Abstract]
Rougier P, Van Cutsem E, Bajetta E, et al.: Randomised trial of irinotecan versus fluorouracil by continuous infusion after fluorouracil failure in patients with metastatic colorectal cancer. Lancet 352 (9138): 1407-12, 1998. [PUBMED Abstract]
Cunningham D, Pyrhönen S, James RD, et al.: Randomised trial of irinotecan plus supportive care versus supportive care alone after fluorouracil failure for patients with metastatic colorectal cancer. Lancet 352 (9138): 1413-8, 1998. [PUBMED Abstract]
Rothenberg ML, Oza AM, Bigelow RH, et al.: Superiority of oxaliplatin and fluorouracil-leucovorin compared with either therapy alone in patients with progressive colorectal cancer after irinotecan and fluorouracil-leucovorin: interim results of a phase III trial. J Clin Oncol 21 (11): 2059-69, 2003. [PUBMED Abstract]
André T, Shiu KK, Kim TW, et al.: Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med 383 (23): 2207-2218, 2020. [PUBMED Abstract]
Andre T, Shiu K, Kim TW, et al.: Final overall survival for the phase III KN177 study: pembrolizumab versus chemotherapy in microsatellite instability-high/mismatch repair deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC). [Abstract] J Clin Oncol 39 (15) (suppl): A-3500, 2021. Available online. Last accessed January 30, 2025.
Lenz H, Lonardi S, Zagonel V, et al.: Subgroup analyses of patients (pts) with microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC) treated with nivolumab (NIVO) plus low-dose ipilimumab (IPI) as first-line (1L) therapy: two-year clinical update. [Abstract] J Clin Oncol 39 (3) (suppl): A-58, 2021. Available online. Last accessed January 30, 2025.
Lenz HJ, Lonardi S, Elez E, et al.: Nivolumab (NIVO) plus ipilimumab (IPI) vs chemotherapy (chemo) as first-line (1L) treatment for microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) metastatic colorectal cancer (mCRC): Expanded efficacy analysis from CheckMate 8HW. [Abstract] J Clin Oncol 42 (Suppl 16): A-3503, 2024.
Overman MJ, McDermott R, Leach JL, et al.: Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol 18 (9): 1182-1191, 2017. [PUBMED Abstract]
Valone FH, Friedman MA, Wittlinger PS, et al.: Treatment of patients with advanced colorectal carcinomas with fluorouracil alone, high-dose leucovorin plus fluorouracil, or sequential methotrexate, fluorouracil, and leucovorin: a randomized trial of the Northern California Oncology Group. J Clin Oncol 7 (10): 1427-36, 1989. [PUBMED Abstract]
Erlichman C, Fine S, Wong A, et al.: A randomized trial of fluorouracil and folinic acid in patients with metastatic colorectal carcinoma. J Clin Oncol 6 (3): 469-75, 1988. [PUBMED Abstract]
Doroshow JH, Multhauf P, Leong L, et al.: Prospective randomized comparison of fluorouracil versus fluorouracil and high-dose continuous infusion leucovorin calcium for the treatment of advanced measurable colorectal cancer in patients previously unexposed to chemotherapy. J Clin Oncol 8 (3): 491-501, 1990. [PUBMED Abstract]
Poon MA, O’Connell MJ, Wieand HS, et al.: Biochemical modulation of fluorouracil with leucovorin: confirmatory evidence of improved therapeutic efficacy in advanced colorectal cancer. J Clin Oncol 9 (11): 1967-72, 1991. [PUBMED Abstract]
Wadler S, Lembersky B, Atkins M, et al.: Phase II trial of fluorouracil and recombinant interferon alfa-2a in patients with advanced colorectal carcinoma: an Eastern Cooperative Oncology Group study. J Clin Oncol 9 (10): 1806-10, 1991. [PUBMED Abstract]
Grem JL, Jordan E, Robson ME, et al.: Phase II study of fluorouracil, leucovorin, and interferon alfa-2a in metastatic colorectal carcinoma. J Clin Oncol 11 (9): 1737-45, 1993. [PUBMED Abstract]
Wong CS, Cummings BJ, Brierley JD, et al.: Treatment of locally recurrent rectal carcinoma–results and prognostic factors. Int J Radiat Oncol Biol Phys 40 (2): 427-35, 1998. [PUBMED Abstract]
Crane CH, Janjan NA, Abbruzzese JL, et al.: Effective pelvic symptom control using initial chemoradiation without colostomy in metastatic rectal cancer. Int J Radiat Oncol Biol Phys 49 (1): 107-16, 2001. [PUBMED Abstract]
Baron TH: Expandable metal stents for the treatment of cancerous obstruction of the gastrointestinal tract. N Engl J Med 344 (22): 1681-7, 2001. [PUBMED Abstract]
Power DG, Healey-Bird BR, Kemeny NE: Regional chemotherapy for liver-limited metastatic colorectal cancer. Clin Colorectal Cancer 7 (4): 247-59, 2008. [PUBMED Abstract]
Khatri VP, Chee KG, Petrelli NJ: Modern multimodality approach to hepatic colorectal metastases: solutions and controversies. Surg Oncol 16 (1): 71-83, 2007. [PUBMED Abstract]
Pawlik TM, Choti MA: Surgical therapy for colorectal metastases to the liver. J Gastrointest Surg 11 (8): 1057-77, 2007. [PUBMED Abstract]
Adson MA, van Heerden JA, Adson MH, et al.: Resection of hepatic metastases from colorectal cancer. Arch Surg 119 (6): 647-51, 1984. [PUBMED Abstract]
Gayowski TJ, Iwatsuki S, Madariaga JR, et al.: Experience in hepatic resection for metastatic colorectal cancer: analysis of clinical and pathologic risk factors. Surgery 116 (4): 703-10; discussion 710-1, 1994. [PUBMED Abstract]
Hughes KS, Simon R, Songhorabodi S, et al.: Resection of the liver for colorectal carcinoma metastases: a multi-institutional study of patterns of recurrence. Surgery 100 (2): 278-84, 1986. [PUBMED Abstract]
Schlag P, Hohenberger P, Herfarth C: Resection of liver metastases in colorectal cancer–competitive analysis of treatment results in synchronous versus metachronous metastases. Eur J Surg Oncol 16 (4): 360-5, 1990. [PUBMED Abstract]
Rosen CB, Nagorney DM, Taswell HF, et al.: Perioperative blood transfusion and determinants of survival after liver resection for metastatic colorectal carcinoma. Ann Surg 216 (4): 493-504; discussion 504-5, 1992. [PUBMED Abstract]
Fong Y, Fortner J, Sun RL, et al.: Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg 230 (3): 309-18; discussion 318-21, 1999. [PUBMED Abstract]
Scheele J, Stangl R, Altendorf-Hofmann A: Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg 77 (11): 1241-6, 1990. [PUBMED Abstract]
Scheele J, Stangl R, Altendorf-Hofmann A, et al.: Indicators of prognosis after hepatic resection for colorectal secondaries. Surgery 110 (1): 13-29, 1991. [PUBMED Abstract]
Wagman LD, Kemeny MM, Leong L, et al.: A prospective, randomized evaluation of the treatment of colorectal cancer metastatic to the liver. J Clin Oncol 8 (11): 1885-93, 1990. [PUBMED Abstract]
Coppa GF, Eng K, Ranson JH, et al.: Hepatic resection for metastatic colon and rectal cancer. An evaluation of preoperative and postoperative factors. Ann Surg 202 (2): 203-8, 1985. [PUBMED Abstract]
Taylor M, Forster J, Langer B, et al.: A study of prognostic factors for hepatic resection for colorectal metastases. Am J Surg 173 (6): 467-71, 1997. [PUBMED Abstract]
Jaeck D, Bachellier P, Guiguet M, et al.: Long-term survival following resection of colorectal hepatic metastases. Association Française de Chirurgie. Br J Surg 84 (7): 977-80, 1997. [PUBMED Abstract]
Weeks JC, Nelson H, Gelber S, et al.: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287 (3): 321-8, 2002. [PUBMED Abstract]
Higgins GA, Amadeo JH, McElhinney J, et al.: Efficacy of prolonged intermittent therapy with combined 5-fluorouracil and methyl-CCNU following resection for carcinoma of the large bowel. A Veterans Administration Surgical Oncology Group report. Cancer 53 (1): 1-8, 1984. [PUBMED Abstract]
Buyse M, Zeleniuch-Jacquotte A, Chalmers TC: Adjuvant therapy of colorectal cancer. Why we still don’t know. JAMA 259 (24): 3571-8, 1988. [PUBMED Abstract]
Laurie JA, Moertel CG, Fleming TR, et al.: Surgical adjuvant therapy of large-bowel carcinoma: an evaluation of levamisole and the combination of levamisole and fluorouracil. The North Central Cancer Treatment Group and the Mayo Clinic. J Clin Oncol 7 (10): 1447-56, 1989. [PUBMED Abstract]
Moertel CG, Fleming TR, Macdonald JS, et al.: Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 322 (6): 352-8, 1990. [PUBMED Abstract]
Leonard GD, Brenner B, Kemeny NE: Neoadjuvant chemotherapy before liver resection for patients with unresectable liver metastases from colorectal carcinoma. J Clin Oncol 23 (9): 2038-48, 2005. [PUBMED Abstract]
Hernandez-Alejandro R, Ruffolo LI, Sasaki K, et al.: Recipient and Donor Outcomes After Living-Donor Liver Transplant for Unresectable Colorectal Liver Metastases. JAMA Surg 157 (6): 524-530, 2022. [PUBMED Abstract]
Adam R, Piedvache C, Chiche L, et al.: Chemotherapy and liver transplantation versus chemotherapy alone in patients with definitively unresectable colorectal liver metastases: A prospective multicentric randomized trial (TRANSMET). [Abstract] J Clin Oncol 46 (Suppl 16): A-3500, 2024.
Rossi S, Buscarini E, Garbagnati F, et al.: Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR Am J Roentgenol 170 (4): 1015-22, 1998. [PUBMED Abstract]
Solbiati L, Livraghi T, Goldberg SN, et al.: Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 221 (1): 159-66, 2001. [PUBMED Abstract]
Lencioni R, Goletti O, Armillotta N, et al.: Radio-frequency thermal ablation of liver metastases with a cooled-tip electrode needle: results of a pilot clinical trial. Eur Radiol 8 (7): 1205-11, 1998. [PUBMED Abstract]
Curley SA, Izzo F, Delrio P, et al.: Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg 230 (1): 1-8, 1999. [PUBMED Abstract]
Oshowo A, Gillams A, Harrison E, et al.: Comparison of resection and radiofrequency ablation for treatment of solitary colorectal liver metastases. Br J Surg 90 (10): 1240-3, 2003. [PUBMED Abstract]
Livraghi T, Solbiati L, Meloni F, et al.: Percutaneous radiofrequency ablation of liver metastases in potential candidates for resection: the “test-of-time approach”. Cancer 97 (12): 3027-35, 2003. [PUBMED Abstract]
Pawlik TM, Izzo F, Cohen DS, et al.: Combined resection and radiofrequency ablation for advanced hepatic malignancies: results in 172 patients. Ann Surg Oncol 10 (9): 1059-69, 2003. [PUBMED Abstract]
Kemeny N, Huang Y, Cohen AM, et al.: Hepatic arterial infusion of chemotherapy after resection of hepatic metastases from colorectal cancer. N Engl J Med 341 (27): 2039-48, 1999. [PUBMED Abstract]
Kemeny MM, Adak S, Gray B, et al.: Combined-modality treatment for resectable metastatic colorectal carcinoma to the liver: surgical resection of hepatic metastases in combination with continuous infusion of chemotherapy–an intergroup study. J Clin Oncol 20 (6): 1499-505, 2002. [PUBMED Abstract]
Kemeny N, Daly J, Reichman B, et al.: Intrahepatic or systemic infusion of fluorodeoxyuridine in patients with liver metastases from colorectal carcinoma. A randomized trial. Ann Intern Med 107 (4): 459-65, 1987. [PUBMED Abstract]
Chang AE, Schneider PD, Sugarbaker PH, et al.: A prospective randomized trial of regional versus systemic continuous 5-fluorodeoxyuridine chemotherapy in the treatment of colorectal liver metastases. Ann Surg 206 (6): 685-93, 1987. [PUBMED Abstract]
Rougier P, Laplanche A, Huguier M, et al.: Hepatic arterial infusion of floxuridine in patients with liver metastases from colorectal carcinoma: long-term results of a prospective randomized trial. J Clin Oncol 10 (7): 1112-8, 1992. [PUBMED Abstract]
Kemeny N, Cohen A, Seiter K, et al.: Randomized trial of hepatic arterial floxuridine, mitomycin, and carmustine versus floxuridine alone in previously treated patients with liver metastases from colorectal cancer. J Clin Oncol 11 (2): 330-5, 1993. [PUBMED Abstract]
Reappraisal of hepatic arterial infusion in the treatment of nonresectable liver metastases from colorectal cancer. Meta-Analysis Group in Cancer. J Natl Cancer Inst 88 (5): 252-8, 1996. [PUBMED Abstract]
McGinn CJ, Lawrence TS: Clinical Results of the Combination of Radiation and Fluoropyrimidines in the Treatment of Intrahepatic Cancer. Semin Radiat Oncol 7 (4): 313-323, 1997. [PUBMED Abstract]
Latest Updates to This Summary (02/12/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of rectal cancer. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Rectal Cancer Treatment are:
Amit Chowdhry, MD, PhD (University of Rochester Medical Center)
Leon Pappas, MD, PhD (Massachusetts General Hospital)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Rectal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/hp/rectal-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389402]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
For most people, the major factor that increases a person’s risk for colorectal cancer (CRC) is advancing age. Risk increases dramatically after age 50 years; 90% of all CRCs are diagnosed after this age. Incidence and mortality rates are higher in African American individuals compared with other races. However, a meta-analysis found no evidence that African American individuals have higher rates of precancerous lesions.[1,2] The history of CRC in a first-degree relative, especially if diagnosed before the age of 55 years, roughly doubles the risk. A personal history of CRC, high-risk adenomas, or ovarian cancer also increase the risk.[3] Other risk factors for CRC have weaker associations than age and family history. People with inflammatory bowel disease, such as ulcerative colitis or Crohn disease, have a much higher risk of CRC starting about 8 years after disease onset and are recommended to have frequent colonoscopic surveillance.[4] A small percentage (<5%) of CRCs occur in people with a genetic predisposition, including familial adenomatous polyposis and Lynch syndrome (hereditary nonpolyposis CRC).
References
Imperiale TF, Abhyankar PR, Stump TE, et al.: Prevalence of Advanced, Precancerous Colorectal Neoplasms in Black and White Populations: A Systematic Review and Meta-analysis. Gastroenterology 155 (6): 1776-1786.e1, 2018. [PUBMED Abstract]
Lansdorp-Vogelaar I, Kuntz KM, Knudsen AB, et al.: Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol Biomarkers Prev 21 (5): 728-36, 2012. [PUBMED Abstract]
Imperiale TF, Juluri R, Sherer EA, et al.: A risk index for advanced neoplasia on the second surveillance colonoscopy in patients with previous adenomatous polyps. Gastrointest Endosc 80 (3): 471-8, 2014. [PUBMED Abstract]
Laukoetter MG, Mennigen R, Hannig CM, et al.: Intestinal cancer risk in Crohn’s disease: a meta-analysis. J Gastrointest Surg 15 (4): 576-83, 2011. [PUBMED Abstract]
Overview
Note: The Overview section summarizes the published evidence on this topic. The rest of the summary describes the evidence in more detail.
Factors With Adequate Evidence of Increased Risk of Colorectal Cancer
Excessive alcohol use
Based on solid evidence from observational studies, excessive alcohol use is associated with an increased risk of colorectal cancer (CRC).[1,2]
Magnitude of Effect: A pooled analysis of eight cohort studies estimated an adjusted relative risk (RR) of 1.41 (95% confidence interval [CI], 1.16–1.72) for consumption exceeding 45 g/day.[1]
Study Design: Cohort studies.
Internal Validity: Fair.
Consistency: Fair.
External Validity: Fair.
Cigarette smoking
Based on solid evidence, cigarette smoking is associated with increased incidence of and mortality from CRC.
Magnitude of Effect: A pooled analysis of 106 observational studies estimated an adjusted RR (current smokers vs. never smokers) of 1.18 for developing CRC (95% CI, 1.11–1.25).[3,4]
Study Design: 106 observational studies.
Internal Validity: Fair.
Consistency: Good.
External Validity: Good.
Obesity
Based on solid evidence, obesity is associated with increased incidence of and mortality from CRC.
Magnitude of Effect: In one large cohort study, the adjusted RR of developing colon cancer for women with a body mass index greater than 29 was 1.45 (95% CI, 1.02–2.07).[5,6] A similar increase in CRC mortality was found in another large cohort study.[7,8]
Study Design: Large cohort studies.
Internal Validity: Fair.
Consistency: Good.
External Validity: Good.
Family/personal history of colorectal cancer and other hereditary conditions
Based on solid evidence, a family history of CRC in a first-degree relative or a personal history of CRC increases the risk of CRC.[9–12] Having a genetic predisposition, including familial adenomatous polyposis and Lynch syndrome (hereditary nonpolyposis CRC), also increases risk of CRC.[13]
Magnitude of Effect: In individuals with familial adenomatous polyposis, the risk of CRC by age 40 can be as high as 100%. Individuals with Lynch syndrome can have a lifetime risk of CRC of about 80%.
Factors With Adequate Evidence for a Decreased Risk of Colorectal Cancer
Physical activity
Based on solid evidence, regular physical activity is associated with a decreased incidence of CRC.
Magnitude of Effect: A meta-analysis of 52 observational studies found a statistically significant 24% reduction in CRC incidence (RR, 0.76; 95% CI, 0.72–0.81).[14]
Study Design: Cohort studies and meta-analysis.
Internal Validity: Fair.
Consistency: Good.
External Validity: Good.
Interventions With Adequate Evidence for a Decreased Risk of Colorectal Cancer
Aspirin: Benefits
Based on solid evidence, daily aspirin (acetylsalicylic acid [ASA]) reduces CRC incidence and mortality after 10 to 20 years. This is based on three individual participant-level data meta-analyses of trials of aspirin used for the primary and secondary prevention of cardiovascular disease.[15–17]
Magnitude of Effect: ASA use reduces the long-term risk of developing CRC by 40% about 10 to 19 years after initiation (hazard ratio [HR], 0.60; 95% CI, 0.47–0.76).[18] Daily doses of 75 to 1,200 mg of ASA reduce the 20-year risk of CRC death by approximately 33% (HR, 0.67; 95% CI, 0.52–0.86).[16,17]
Study Design: Individual patient-level data meta-analyses of randomized controlled trials (RCTs) of ASA for primary and secondary cardiovascular prevention.
Internal Validity: Fair, some data from registries and death certificates, some loss to follow-up; variations in ASA dose and timing; adherence to ASA unknown after end of trials (5–9 years); trials designed to answer a different primary hypothesis (cardiovascular disease prevention).
Consistency: Generally consistent.
External Validity: Fair, most data (>75%) from men.
Aspirin: Harms
Based on solid evidence, harms of ASA use include excessive bleeding, including gastrointestinal bleeding and hemorrhagic stroke.
Magnitude of Effect: Very low-dose ASA use (i.e., ≤100 mg every day or every other day) results in an estimated 14 (95% CI, 7–23) additional major gastrointestinal bleeding events and 3.2 (95% CI, -0.5 to 0.82) extra hemorrhagic strokes per 1,000 individuals over 10 years. These risks increase with advancing age.[19]
Study Design: Evidence obtained from RCTs, cohort studies, and meta-analyses comparing ASA with placebo or no treatment for the primary prevention of cardiovascular disease.[19]
Internal Validity: Fair, data are from clinically and methodologically heterogeneous trials.
Consistency: Good.
External Validity: Fair, data on specific subgroups are limited.
Hormone therapy (estrogen plus progestin): Benefits
Based on solid evidence, combined hormone therapy (conjugated equine estrogen and progestin) decreases the incidence of invasive CRC.[20]
Based on fair evidence, combination conjugated equine estrogen and progestin has little or no benefit in reducing mortality from CRC. Data from the Women’s Health Initiative (WHI), a randomized, placebo-controlled trial evaluating estrogen plus progestin, with a mean intervention of 5.6 years and a follow-up of 11.6 years, showed that women taking combined hormone therapy had a statistically significant higher stage of cancer (regional and distant) at diagnosis but not a statistically significant number of deaths from CRC compared with women taking the placebo.[20]
Magnitude of Effect: There were fewer CRCs in the combined hormone therapy group than in the placebo group (0.12% vs. 0.16%; HR, 0.72; 95% CI, 0.56–0.94). A meta-analysis of cohort studies observed a RR of 0.86 (95% CI, 0.76–0.97) for incidence of CRC associated with combined hormone therapy.
There were 37 CRC deaths in the combined hormone therapy arm compared with 27 deaths in the placebo arm (0.04% vs. 0.03%; HR, 1.29; 95% CI, 0.78–2.11).
Study Design: RCT and cohort studies.
Internal Validity: Good.
Consistency: Good for effect on incidence; not applicable (N/A) for effect on mortality; results were based on one trial.
External Validity: Good.
Hormone therapy (estrogen plus progestin): Harms
Based on solid evidence, harms of postmenopausal combined estrogen-plus-progestin hormone use include increased risk of breast cancer, coronary heart disease, and thromboembolic events.
Magnitude of Effect: The WHI showed a 26% increase in invasive breast cancer in the combined hormone group, a 29% increase in coronary heart disease events, a 41% increase in stroke rates, and a twofold higher rate of thromboembolic events.[21]
Study Design: Evidence from RCTs.
Internal Validity: Good.
Consistency: Good.
External Validity: Fair.
Polyp removal: Benefits
Based on fair evidence, removal of adenomatous polyps reduces the risk of CRC. Much of this reduction likely comes from removal of large (i.e., >1.0 cm) polyps, while the benefit of removing smaller polyps—which are much more common—is unknown. Some but not all observational evidence indicates that this reduction may be greater for left-sided CRC than for right-sided CRC.[22–24]
Magnitude of Effect: Unknown, probably greater for larger polyps (i.e., >1.0 cm) than for smaller ones.[25]
Study Design: Evidence obtained from cohort studies and one RCT of sigmoidoscopy.[23]
Internal Validity: Good.
Consistency: Consistent.
External Validity: Good.
Polyp removal: Harms
Based on solid evidence, the major harms of polyp removal include perforation of the colon and bleeding.
Magnitude of Effect: Seven to nine events per 1,000 procedures.[26–28]
Study Design: Evidence from retrospective cohort studies.[27,28]
Internal Validity: Good.
Consistency: Good.
External Validity: Good.
Factors With Inadequate Evidence of an Association With Colorectal Cancer
There is inadequate evidence that the use of NSAIDs reduces the risk of CRC. In people without genetic predisposition but with a prior history of a colonic adenoma that had been removed, three RCTs found that celecoxib [29,30] and rofecoxib [31] decreased the incidence of recurrent adenoma, although follow-up was too short to determine whether CRC incidence or mortality would have been affected.
Based on solid evidence, NSAIDs reduce the risk of adenomas, but the extent to which this translates into a reduction of CRC is uncertain.[32]
Study Design: No adequate studies with CRC outcome.
Internal Validity: N/A.
Consistency: N/A.
External Validity: N/A.
NSAIDs: Harms
Based on solid evidence, harms of NSAID use are relatively common and potentially serious, and include upper gastrointestinal bleeding, chronic kidney disease, and serious cardiovascular events such as myocardial infarction, heart failure, and hemorrhagic stroke.[33] A recent report compared the cyclooxygenase-2 (COX-2) inhibitor celecoxib (200 mg/d) with the nonselective nonsteroidals naproxen (850 mg/d) and ibuprofen (2,000 mg/d) in individuals with severe arthritis (i.e., not using lower doses as for primary prevention). The results showed that serious cardiovascular events were not less common for those taking the nonselective nonsteroidals. However, this study did not assess the comparative safety of lower doses or the safety of the COX-2 inhibitor rofecoxib.[34]
Magnitude of Effect: The estimated average excess risk of upper gastrointestinal complications in average-risk people attributable to NSAIDs is 4 to 5 per 1,000 people per year.[35,36] The excess risk varies with the underlying gastrointestinal risk; however, it likely exceeds ten extra cases per 1,000 people per year in more than 10% of users.[37] Serious cardiovascular events are increased by 50% to 60%.[36]
Study Design: Evidence obtained from RCTs and high-quality systematic reviews and meta-analyses.[35,36]
Internal Validity: Good.
Consistency: Good.
External Validity: Good.
Calcium supplementation
The evidence is inadequate to determine whether calcium supplementation reduces the risk of CRC.
Dietary factors
There is no reliable evidence that a diet started in adulthood that is low in fat and meat and high in fiber, fruits, and vegetables reduces the risk of CRC by a clinically important degree.
Factors and Interventions With Adequate Evidence of no Association With Colorectal Cancer
Estrogen-only therapy: Benefits
Based on fair evidence, conjugated equine estrogens do not affect the incidence of or mortality from invasive CRC.[38]
Magnitude of Effect: N/A.
Study Design: Evidence from RCTs.
Internal Validity: Good.
Consistency: Good.
External Validity: Fair.
Statins: Benefits
Based on solid evidence, statins do not reduce the incidence of or mortality from CRC.
Based on solid evidence, the harms of statins are small.
Study Design: Observational studies,[42] multiple RCTs, and a review.[43]
Internal Validity: Good.
Consistency: Good.
External Validity: Good.
References
Cho E, Smith-Warner SA, Ritz J, et al.: Alcohol intake and colorectal cancer: a pooled analysis of 8 cohort studies. Ann Intern Med 140 (8): 603-13, 2004. [PUBMED Abstract]
Fedirko V, Tramacere I, Bagnardi V, et al.: Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol 22 (9): 1958-72, 2011. [PUBMED Abstract]
Botteri E, Iodice S, Bagnardi V, et al.: Smoking and colorectal cancer: a meta-analysis. JAMA 300 (23): 2765-78, 2008. [PUBMED Abstract]
Liang PS, Chen TY, Giovannucci E: Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer 124 (10): 2406-15, 2009. [PUBMED Abstract]
Martínez ME, Giovannucci E, Spiegelman D, et al.: Leisure-time physical activity, body size, and colon cancer in women. Nurses’ Health Study Research Group. J Natl Cancer Inst 89 (13): 948-55, 1997. [PUBMED Abstract]
Giovannucci E, Ascherio A, Rimm EB, et al.: Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 122 (5): 327-34, 1995. [PUBMED Abstract]
Calle EE, Rodriguez C, Walker-Thurmond K, et al.: Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348 (17): 1625-38, 2003. [PUBMED Abstract]
Ma Y, Yang Y, Wang F, et al.: Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One 8 (1): e53916, 2013. [PUBMED Abstract]
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Schoen RE, Razzak A, Yu KJ, et al.: Incidence and mortality of colorectal cancer in individuals with a family history of colorectal cancer. Gastroenterology 149 (6): 1438-1445.e1, 2015. [PUBMED Abstract]
Butterworth AS, Higgins JP, Pharoah P: Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer 42 (2): 216-27, 2006. [PUBMED Abstract]
Samadder NJ, Curtin K, Tuohy TM, et al.: Increased risk of colorectal neoplasia among family members of patients with colorectal cancer: a population-based study in Utah. Gastroenterology 147 (4): 814-821.e5; quiz e15-6, 2014. [PUBMED Abstract]
Mork ME, You YN, Ying J, et al.: High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults With Colorectal Cancer. J Clin Oncol 33 (31): 3544-9, 2015. [PUBMED Abstract]
Wolin KY, Yan Y, Colditz GA, et al.: Physical activity and colon cancer prevention: a meta-analysis. Br J Cancer 100 (4): 611-6, 2009. [PUBMED Abstract]
Flossmann E, Rothwell PM; British Doctors Aspirin Trial and the UK-TIA Aspirin Trial: Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet 369 (9573): 1603-13, 2007. [PUBMED Abstract]
Rothwell PM, Wilson M, Elwin CE, et al.: Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 376 (9754): 1741-50, 2010. [PUBMED Abstract]
Rothwell PM, Fowkes FG, Belch JF, et al.: Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet 377 (9759): 31-41, 2011. [PUBMED Abstract]
Chubak J, Whitlock EP, Williams SB, et al.: Aspirin for the Prevention of Cancer Incidence and Mortality: Systematic Evidence Reviews for the U.S. Preventive Services Task Force. Ann Intern Med 164 (12): 814-25, 2016. [PUBMED Abstract]
Whitlock EP, Burda BU, Williams SB, et al.: Bleeding Risks With Aspirin Use for Primary Prevention in Adults: A Systematic Review for the U.S. Preventive Services Task Force. Ann Intern Med 164 (12): 826-35, 2016. [PUBMED Abstract]
Simon MS, Chlebowski RT, Wactawski-Wende J, et al.: Estrogen plus progestin and colorectal cancer incidence and mortality. J Clin Oncol 30 (32): 3983-90, 2012. [PUBMED Abstract]
Writing Group for the Women’s Health Initiative Investigators: Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 288 (3): 321-33, 2002. [PUBMED Abstract]
Brenner H, Hoffmeister M, Arndt V, et al.: Protection from right- and left-sided colorectal neoplasms after colonoscopy: population-based study. J Natl Cancer Inst 102 (2): 89-95, 2010. [PUBMED Abstract]
Atkin WS, Edwards R, Kralj-Hans I, et al.: Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375 (9726): 1624-33, 2010. [PUBMED Abstract]
Brenner H, Chang-Claude J, Seiler CM, et al.: Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med 154 (1): 22-30, 2011. [PUBMED Abstract]
Robertson DJ, Greenberg ER, Beach M, et al.: Colorectal cancer in patients under close colonoscopic surveillance. Gastroenterology 129 (1): 34-41, 2005. [PUBMED Abstract]
Nelson DB, McQuaid KR, Bond JH, et al.: Procedural success and complications of large-scale screening colonoscopy. Gastrointest Endosc 55 (3): 307-14, 2002. [PUBMED Abstract]
Levin TR, Zhao W, Conell C, et al.: Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med 145 (12): 880-6, 2006. [PUBMED Abstract]
Warren JL, Klabunde CN, Mariotto AB, et al.: Adverse events after outpatient colonoscopy in the Medicare population. Ann Intern Med 150 (12): 849-57, W152, 2009. [PUBMED Abstract]
Bertagnolli MM, Eagle CJ, Zauber AG, et al.: Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med 355 (9): 873-84, 2006. [PUBMED Abstract]
Arber N, Eagle CJ, Spicak J, et al.: Celecoxib for the prevention of colorectal adenomatous polyps. N Engl J Med 355 (9): 885-95, 2006. [PUBMED Abstract]
Lanas A, Baron JA, Sandler RS, et al.: Peptic ulcer and bleeding events associated with rofecoxib in a 3-year colorectal adenoma chemoprevention trial. Gastroenterology 132 (2): 490-7, 2007. [PUBMED Abstract]
Chudy-Onwugaje K, Huang WY, Su LJ, et al.: Aspirin, ibuprofen, and reduced risk of advanced colorectal adenoma incidence and recurrence and colorectal cancer in the PLCO Cancer Screening Trial. Cancer 127 (17): 3145-3155, 2021. [PUBMED Abstract]
Bresalier RS, Sandler RS, Quan H, et al.: Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 352 (11): 1092-102, 2005. [PUBMED Abstract]
Nissen SE, Yeomans ND, Solomon DH, et al.: Cardiovascular Safety of Celecoxib, Naproxen, or Ibuprofen for Arthritis. N Engl J Med 375 (26): 2519-29, 2016. [PUBMED Abstract]
Rostom A, Dubé C, Lewin G, et al.: Nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 inhibitors for primary prevention of colorectal cancer: a systematic review prepared for the U.S. Preventive Services Task Force. Ann Intern Med 146 (5): 376-89, 2007. [PUBMED Abstract]
Kearney PM, Baigent C, Godwin J, et al.: Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ 332 (7553): 1302-8, 2006. [PUBMED Abstract]
Hernández-Díaz S, García Rodríguez LA: Cardioprotective aspirin users and their excess risk of upper gastrointestinal complications. BMC Med 4: 22, 2006. [PUBMED Abstract]
Ritenbaugh C, Stanford JL, Wu L, et al.: Conjugated equine estrogens and colorectal cancer incidence and survival: the Women’s Health Initiative randomized clinical trial. Cancer Epidemiol Biomarkers Prev 17 (10): 2609-18, 2008. [PUBMED Abstract]
Baigent C, Keech A, Kearney PM, et al.: Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 366 (9493): 1267-78, 2005. [PUBMED Abstract]
Dale KM, Coleman CI, Henyan NN, et al.: Statins and cancer risk: a meta-analysis. JAMA 295 (1): 74-80, 2006. [PUBMED Abstract]
Browning DR, Martin RM: Statins and risk of cancer: a systematic review and metaanalysis. Int J Cancer 120 (4): 833-43, 2007. [PUBMED Abstract]
Hippisley-Cox J, Coupland C: Unintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch database. BMJ 340: c2197, 2010. [PUBMED Abstract]
Joy TR, Hegele RA: Narrative review: statin-related myopathy. Ann Intern Med 150 (12): 858-68, 2009. [PUBMED Abstract]
Incidence and Mortality
Colorectal cancer (CRC) is the third most common malignant neoplasm worldwide [1] and the second leading cause of cancer deaths in men and women combined in the United States.[2] It is estimated that there will be 154,270 new cases diagnosed in the United States in 2025 and 52,900 deaths caused by this disease.[2] Between 2012 and 2021, incidence rates for CRC in the United States declined by about 1% per year overall. However, this declining incidence is confined to individuals aged 65 years and older. Between 2012 and 2021, incidence rates increased by 2.4% per year in individuals younger than 50 years and by 0.4% per year in individuals aged 50 to 64 years.[2] For the past 50 years, the mortality rate for CRC has been declining in both men and women. Over the last decade, the mortality rate declined by 1.7% per year.[2] Incidence and mortality rates are higher in Black individuals than in those of other races; however, a meta-analysis found no evidence that Black individuals have higher rates of precancerous lesions.[3–5]
The 5-year overall survival rate is 64% for CRC. About 4% of Americans are expected to develop CRC within their lifetimes.[2,6] The risk of CRC begins to increase after the age of 40 years and rises sharply at ages 50 to 55 years; the risk doubles with each succeeding decade and continues to rise exponentially. Despite advances in surgical techniques and adjuvant therapy, there has been only a modest improvement in survival for patients who present with advanced neoplasms.[7,8] Effective primary and secondary preventive approaches must be developed to reduce the morbidity and mortality from CRC.
References
Bray F, Laversanne M, Sung H, et al.: Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 74 (3): 229-263, 2024. [PUBMED Abstract]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Imperiale TF, Abhyankar PR, Stump TE, et al.: Prevalence of Advanced, Precancerous Colorectal Neoplasms in Black and White Populations: A Systematic Review and Meta-analysis. Gastroenterology 155 (6): 1776-1786.e1, 2018. [PUBMED Abstract]
Laiyemo AO, Doubeni C, Pinsky PF, et al.: Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities. J Natl Cancer Inst 102 (8): 538-46, 2010. [PUBMED Abstract]
Lansdorp-Vogelaar I, Kuntz KM, Knudsen AB, et al.: Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol Biomarkers Prev 21 (5): 728-36, 2012. [PUBMED Abstract]
Surveillance Research Program, National Cancer Institute: SEER*Explorer: An interactive website for SEER cancer statistics. Bethesda, MD: National Cancer Institute. Available online. Last accessed December 30, 2024.
Moertel CG, Fleming TR, Macdonald JS, et al.: Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 322 (6): 352-8, 1990. [PUBMED Abstract]
Krook JE, Moertel CG, Gunderson LL, et al.: Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 324 (11): 709-15, 1991. [PUBMED Abstract]
Definition of Prevention
Primary prevention involves the use of medications or other interventions before the clinical appearance of colorectal cancer (CRC) with the intent of preventing clinical CRC and CRC mortality.
Etiology and Pathogenesis of Colorectal Cancer
Genetics,[1,2] experimental,[3,4] and epidemiologic [5–7] studies suggest that colorectal cancer (CRC) results from complex interactions between inherited susceptibility and environmental factors. The exact nature and contribution of these factors to CRC incidence and mortality is the subject of ongoing research.
References
Willett W: The search for the causes of breast and colon cancer. Nature 338 (6214): 389-94, 1989. [PUBMED Abstract]
Fearon ER, Vogelstein B: A genetic model for colorectal tumorigenesis. Cell 61 (5): 759-67, 1990. [PUBMED Abstract]
Reddy B, Engle A, Katsifis S, et al.: Biochemical epidemiology of colon cancer: effect of types of dietary fiber on fecal mutagens, acid, and neutral sterols in healthy subjects. Cancer Res 49 (16): 4629-35, 1989. [PUBMED Abstract]
Reddy BS, Tanaka T, Simi B: Effect of different levels of dietary trans fat or corn oil on azoxymethane-induced colon carcinogenesis in F344 rats. J Natl Cancer Inst 75 (4): 791-8, 1985. [PUBMED Abstract]
Potter JD: Reconciling the epidemiology, physiology, and molecular biology of colon cancer. JAMA 268 (12): 1573-7, 1992 Sep 23-30. [PUBMED Abstract]
Wynder EL, Reddy BS: Dietary fat and fiber and colon cancer. Semin Oncol 10 (3): 264-72, 1983. [PUBMED Abstract]
Chen CD, Yen MF, Wang WM, et al.: A case-cohort study for the disease natural history of adenoma-carcinoma and de novo carcinoma and surveillance of colon and rectum after polypectomy: implication for efficacy of colonoscopy. Br J Cancer 88 (12): 1866-73, 2003. [PUBMED Abstract]
Factors With Adequate Evidence of Increased Risk of Colorectal Cancer
Excessive Alcohol Use
There is evidence of an association of colorectal cancer (CRC) with alcoholic beverage consumption. In a meta-analysis of eight cohort studies, the relative risk (RR) for consumption of 45 g/day (i.e., about three standard drinks per day) compared with nondrinkers was 1.41 (95% confidence interval [CI], 1.16–1.72).[1] Case-control studies suggest a modest-to-strong positive relationship between alcohol consumption and large bowel cancers.[2,3] A meta-analysis found that the association did not vary by sex or cancer location within the large bowel.[4]
Five studies have reported a positive association between alcohol intake and colorectal adenomas.[5] A case-control study of diet, genetic factors, and the adenoma-carcinoma sequence was conducted in Burgundy.[6] It separated adenomas smaller than 10.0 mm in diameter from larger adenomas. A positive association between current alcohol intake and adenomas was found to be limited to the larger adenomas, suggesting that alcohol intake could act at the promotional phase of the adenoma-carcinoma sequence.[6]
A large cohort study found a dose-response relationship between alcohol intake and death from CRC, with a RR of 1.2 (95% CI, 1.0–1.5) for four or more drinks per day compared with nondrinkers.[7]
Cigarette Smoking
Most case-control studies of cigarette exposure and adenomas have found an elevated risk for smokers.[8] In addition, a significantly increased risk of adenoma recurrence following polypectomy has been associated with smoking in both men and women.[8] In the Nurses’ Health Study, the minimum induction period for cancer appeared to be at least 35 years.[9] Similarly, in the Health Professionals Follow-up Study, a history of smoking was associated with both small and large adenomas and with a long induction period of at least 35 years for CRC.[10] In the Cancer Prevention Study II (CPS II), a large nationwide cohort study, multivariate-adjusted CRC mortality rates were highest among current smokers, intermediate among former smokers, and lowest in nonsmokers, with increased risk observed after 20 or more years of smoking in men and women combined.[11] On the basis of CPS II data, it was estimated that 12% of CRC deaths in the U.S. population in 1997 were attributable to smoking. A large population-based cohort study of Swedish twins found that heavy smoking of 35 or more years’ duration was associated with a nearly threefold increased risk of developing colon cancer, although subsite analysis found a statistically significant effect only for rectal cancer, but not colon cancer.[12] Another large population-based case-control study demonstated that current tobacco use and tobacco use within the last 10 years is associated with colon cancer. A 50% increase in risk was associated with smoking more than a pack a day relative to never smoking.[13] However, a 28-year follow-up of 57,000 Finns showed no association between the development of CRC and baseline smoking status, although there was a 57% to 71% increased risk in persistent smokers.[14] No relationship was found between cigarette smoking, even smoking of long duration, and recurrence of adenomas in a population followed for 4 years after initial colonoscopy.[15]
A meta-analysis of 106 observational studies found a RR (ever smokers vs. nonsmokers) for CRC incidence of 1.18 (95% CI, 1.11–1.25), with an absolute risk increase of 10.8 cases per 100,000 person-years (95% CI, 7.9–13.6). There was a statistically significant dose-response effect. In 17 studies with data on CRC mortality, cigarette smoking was associated with CRC death, with a RR (ever smokers vs. never smokers) of 1.25 (95% CI, 1.14–1.37), and an absolute increase in the death rate of 6.0 deaths per 100,000 person-years. For both incidence and mortality, the association was stronger for rectal cancer than for colon cancer.[16]
Obesity
At least three large cohort studies have found an association between obesity and CRC incidence or mortality.[17–19] The Nurses’ Health Study found that women with a body mass index (BMI) of more than 29, compared with women with a BMI of less than 21, had an adjusted RR for CRC incidence of 1.45 (95% CI, 1.02–2.07).[17] In the CPS II,[19] men and women with a BMI of 30 to 34.9 had an adjusted RR for CRC mortality (compared with people with a BMI of 18.5–24.9) of 1.47 (95% CI, 1.30–1.66), with a statistically significant dose-response effect.[19] The effects were similar in men and women.
Family/Personal History of Colorectal Cancer and Other Hereditary Conditions
Some of the earliest studies of family history of CRC were those of Utah families that reported a higher number of deaths from CRC (3.9%) among the first-degree relatives of patients who had died from CRC than among sex-matched and age-matched controls (1.2%). This difference has since been replicated in numerous studies that have consistently found that first-degree relatives of affected cases are themselves at a twofold to threefold increased risk of CRC. Despite the various study designs (case-control, cohort), sampling frames, sample sizes, methods of data verification, analytic methods, and countries where the studies originated, the magnitude of risk is consistent.[20–25]
A systematic review and meta-analysis of familial CRC risk was reported.[26] Of 24 studies included in the analysis, all but one reported an increased risk of CRC if there was an affected first-degree relative. The RR for CRC in the pooled study was 2.25 (95% CI, 2.00–2.53) if there was an affected first-degree family member. In 8 of 11 studies, if the index cancer arose in the colon, the risk was slightly higher than if it arose in the rectum. The pooled analysis revealed an RR in relatives of colon and rectal cancer patients of 2.42 (95% CI, 2.20–2.65) and 1.89 (95% CI, 1.62–2.21), respectively. The analysis did not reveal a difference in RR for colon cancer based on location of the tumor (right side vs. left side).[26]
Hereditary CRC has two well-described forms: Familial adenomatous polyposis (including an attenuated form of polyposis), due to germline mutations in the APC gene,[27–34] and Lynch syndrome (hereditary nonpolyposis CRC), which is caused by germline mutations in DNA mismatch repair genes.[35–38] Many other families exhibit aggregation of CRC and/or adenomas, but with no apparent association with an identifiable hereditary syndrome, and are known collectively as familial CRC.[38]
Cho E, Smith-Warner SA, Ritz J, et al.: Alcohol intake and colorectal cancer: a pooled analysis of 8 cohort studies. Ann Intern Med 140 (8): 603-13, 2004. [PUBMED Abstract]
Newcomb PA, Storer BE, Marcus PM: Cancer of the large bowel in women in relation to alcohol consumption: a case-control study in Wisconsin (United States). Cancer Causes Control 4 (5): 405-11, 1993. [PUBMED Abstract]
Meyer F, White E: Alcohol and nutrients in relation to colon cancer in middle-aged adults. Am J Epidemiol 138 (4): 225-36, 1993. [PUBMED Abstract]
Longnecker MP, Orza MJ, Adams ME, et al.: A meta-analysis of alcoholic beverage consumption in relation to risk of colorectal cancer. Cancer Causes Control 1 (1): 59-68, 1990. [PUBMED Abstract]
Boutron MC, Faivre J: Diet and the adenoma-carcinoma sequence. Eur J Cancer Prev 2 (Suppl 2): 95-8, 1993. [PUBMED Abstract]
Boutron MC, Faivre J: Alcohol, tobacco and the adenoma-carcinoma sequence: a case-control study in Burgundy, France. [Abstract] Gastroenterology 104 (Suppl 4): A-390, 1993.
Thun MJ, Peto R, Lopez AD, et al.: Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med 337 (24): 1705-14, 1997. [PUBMED Abstract]
Giovannucci E, Colditz GA, Stampfer MJ, et al.: A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. women. J Natl Cancer Inst 86 (3): 192-9, 1994. [PUBMED Abstract]
Giovannucci E, Rimm EB, Stampfer MJ, et al.: A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. men. J Natl Cancer Inst 86 (3): 183-91, 1994. [PUBMED Abstract]
Chao A, Thun MJ, Jacobs EJ, et al.: Cigarette smoking and colorectal cancer mortality in the cancer prevention study II. J Natl Cancer Inst 92 (23): 1888-96, 2000. [PUBMED Abstract]
Terry P, Ekbom A, Lichtenstein P, et al.: Long-term tobacco smoking and colorectal cancer in a prospective cohort study. Int J Cancer 91 (4): 585-7, 2001. [PUBMED Abstract]
Slattery ML, Potter JD, Friedman GD, et al.: Tobacco use and colon cancer. Int J Cancer 70 (3): 259-64, 1997. [PUBMED Abstract]
Knekt P, Hakama M, Järvinen R, et al.: Smoking and risk of colorectal cancer. Br J Cancer 78 (1): 136-9, 1998. [PUBMED Abstract]
Baron JA, Sandler RS, Haile RW, et al.: Folate intake, alcohol consumption, cigarette smoking, and risk of colorectal adenomas. J Natl Cancer Inst 90 (1): 57-62, 1998. [PUBMED Abstract]
Botteri E, Iodice S, Bagnardi V, et al.: Smoking and colorectal cancer: a meta-analysis. JAMA 300 (23): 2765-78, 2008. [PUBMED Abstract]
Martínez ME, Giovannucci E, Spiegelman D, et al.: Leisure-time physical activity, body size, and colon cancer in women. Nurses’ Health Study Research Group. J Natl Cancer Inst 89 (13): 948-55, 1997. [PUBMED Abstract]
Giovannucci E, Ascherio A, Rimm EB, et al.: Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 122 (5): 327-34, 1995. [PUBMED Abstract]
Calle EE, Rodriguez C, Walker-Thurmond K, et al.: Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348 (17): 1625-38, 2003. [PUBMED Abstract]
Fuchs CS, Giovannucci EL, Colditz GA, et al.: A prospective study of family history and the risk of colorectal cancer. N Engl J Med 331 (25): 1669-74, 1994. [PUBMED Abstract]
Slattery ML, Kerber RA: Family history of cancer and colon cancer risk: the Utah Population Database. J Natl Cancer Inst 86 (21): 1618-26, 1994. [PUBMED Abstract]
Negri E, Braga C, La Vecchia C, et al.: Family history of cancer and risk of colorectal cancer in Italy. Br J Cancer 77 (1): 174-9, 1998. [PUBMED Abstract]
St John DJ, McDermott FT, Hopper JL, et al.: Cancer risk in relatives of patients with common colorectal cancer. Ann Intern Med 118 (10): 785-90, 1993. [PUBMED Abstract]
Duncan JL, Kyle J: Family incidence of carcinoma of the colon and rectum in north-east Scotland. Gut 23 (2): 169-71, 1982. [PUBMED Abstract]
Rozen P, Fireman Z, Figer A, et al.: Family history of colorectal cancer as a marker of potential malignancy within a screening program. Cancer 60 (2): 248-54, 1987. [PUBMED Abstract]
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Kinzler KW, Nilbert MC, Su LK, et al.: Identification of FAP locus genes from chromosome 5q21. Science 253 (5020): 661-5, 1991. [PUBMED Abstract]
Groden J, Thliveris A, Samowitz W, et al.: Identification and characterization of the familial adenomatous polyposis coli gene. Cell 66 (3): 589-600, 1991. [PUBMED Abstract]
Leppert M, Burt R, Hughes JP, et al.: Genetic analysis of an inherited predisposition to colon cancer in a family with a variable number of adenomatous polyps. N Engl J Med 322 (13): 904-8, 1990. [PUBMED Abstract]
Spirio L, Olschwang S, Groden J, et al.: Alleles of the APC gene: an attenuated form of familial polyposis. Cell 75 (5): 951-7, 1993. [PUBMED Abstract]
Brensinger JD, Laken SJ, Luce MC, et al.: Variable phenotype of familial adenomatous polyposis in pedigrees with 3′ mutation in the APC gene. Gut 43 (4): 548-52, 1998. [PUBMED Abstract]
Soravia C, Berk T, Madlensky L, et al.: Genotype-phenotype correlations in attenuated adenomatous polyposis coli. Am J Hum Genet 62 (6): 1290-301, 1998. [PUBMED Abstract]
Pedemonte S, Sciallero S, Gismondi V, et al.: Novel germline APC variants in patients with multiple adenomas. Genes Chromosomes Cancer 22 (4): 257-67, 1998. [PUBMED Abstract]
Sieber OM, Lamlum H, Crabtree MD, et al.: Whole-gene APC deletions cause classical familial adenomatous polyposis, but not attenuated polyposis or “multiple” colorectal adenomas. Proc Natl Acad Sci U S A 99 (5): 2954-8, 2002. [PUBMED Abstract]
Leach FS, Nicolaides NC, Papadopoulos N, et al.: Mutations of a mutS homolog in hereditary nonpolyposis colorectal cancer. Cell 75 (6): 1215-25, 1993. [PUBMED Abstract]
Papadopoulos N, Nicolaides NC, Wei YF, et al.: Mutation of a mutL homolog in hereditary colon cancer. Science 263 (5153): 1625-9, 1994. [PUBMED Abstract]
Nicolaides NC, Papadopoulos N, Liu B, et al.: Mutations of two PMS homologues in hereditary nonpolyposis colon cancer. Nature 371 (6492): 75-80, 1994. [PUBMED Abstract]
Miyaki M, Konishi M, Tanaka K, et al.: Germline mutation of MSH6 as the cause of hereditary nonpolyposis colorectal cancer. Nat Genet 17 (3): 271-2, 1997. [PUBMED Abstract]
Factors With Adequate Evidence for a Decreased Risk of Colorectal Cancer
Physical Activity
A sedentary lifestyle has been associated with an increased risk of colorectal cancer in some [1,2] but not all [3] studies. Numerous observational studies have examined the relationship between physical activity and colon cancer risk.[4] Most of these studies have shown an inverse relationship between level of physical activity and colon cancer incidence. The average relative risk (RR) reduction is reportedly 40% to 50%. Large U.S. cohort studies have found statistically significant adjusted RRs of 0.54 (95% confidence interval [CI], 0.33–0.90) [5] and 0.53 (95% CI, 0.32–0.88) [6] when comparing people with high versus low average energy expenditure. A meta-analysis of 52 observational studies found an overall adjusted RR of 0.76 (95% CI, 0.72–0.81), with similar results for men and women.[7]
References
White E, Jacobs EJ, Daling JR: Physical activity in relation to colon cancer in middle-aged men and women. Am J Epidemiol 144 (1): 42-50, 1996. [PUBMED Abstract]
Slattery ML, Schumacher MC, Smith KR, et al.: Physical activity, diet, and risk of colon cancer in Utah. Am J Epidemiol 128 (5): 989-99, 1988. [PUBMED Abstract]
Kune GA, Kune S, Watson LF: Body weight and physical activity as predictors of colorectal cancer risk. Nutr Cancer 13 (1-2): 9-17, 1990. [PUBMED Abstract]
Friedenreich CM: Physical activity and cancer prevention: from observational to intervention research. Cancer Epidemiol Biomarkers Prev 10 (4): 287-301, 2001. [PUBMED Abstract]
Martínez ME, Giovannucci E, Spiegelman D, et al.: Leisure-time physical activity, body size, and colon cancer in women. Nurses’ Health Study Research Group. J Natl Cancer Inst 89 (13): 948-55, 1997. [PUBMED Abstract]
Giovannucci E, Ascherio A, Rimm EB, et al.: Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 122 (5): 327-34, 1995. [PUBMED Abstract]
Wolin KY, Yan Y, Colditz GA, et al.: Physical activity and colon cancer prevention: a meta-analysis. Br J Cancer 100 (4): 611-6, 2009. [PUBMED Abstract]
Interventions With Adequate Evidence for a Decreased Risk of Colorectal Cancer
Aspirin
Evidence from individual participant-level data meta-analyses of randomized controlled trials (RCTs) and observational studies [1,2] investigating the use of aspirin for the prevention of cardiovascular disease indicates that acetylsalicylic acid (ASA) use reduces the incidence of colorectal cancer (CRC), but not until at least 10 years after initiation of therapy (pooled relative risk [RR] of CRC incidence within 10 years of initiation, 0.99 [95% confidence interval (CI), 0.85–1.15] vs. RR, 0.60 [95% CI, 0.47–0.76] at 10–19 years after initiation).[3] In the Women’s Health Study, a randomized 2 × 2 factorial trial of 100 mg of ASA every other day for an average of 10 years, CRC incidence was reduced by about 20% after 17.5 years (hazard ratio [HR], 0.80; 95% CI, 0.67–0.97).[4] In a report from the Nurses’ Health Study involving 82,911 women followed for 20 years, the multivariate RR for colon cancer was 0.77 (95% CI, 0.67–0.88) among women who regularly used ASA (≥2 standard 325-mg tablets per week) compared with nonregular use. Significant RR was not observed, however, until more than 10 years of use.[5]
The Cancer Prevention Programme (CAPP2), previously known as the Concerted Action Polyposis Prevention project, investigated chemoprevention of CRC in patients with known Lynch syndrome (hereditary nonpolyposis CRC) across 43 international centers. For more information, see the Lynch Syndrome section in Genetics of Colorectal Cancer. Patients were randomly assigned to receive aspirin (600 mg/day), aspirin-placebo, resistant starch (30 g/day), or starch-placebo for up to 4 years. A planned 10-year analysis of CAPP2 data found reduced CRC incidence in patients with Lynch syndrome who took aspirin for at least 2 years when compared with those who took placebo. An intention-to-treat analysis, using Cox proportional hazards regression, showed that aspirin protected against the primary end point of CRC (HR, 0.65; 95% CI, 0.43–0.97; P = .035).[6]
In a randomized study of 635 patients with prior CRC (T1–T2 N0 M0) who had undergone curative resection, ASA intake at 325 mg/day was associated with a decrease in the adjusted RR of any recurrent adenoma as compared with the placebo group (0.65; 95% CI, 0.46–0.91) after a median duration of treatment of 31 months. The likelihood of detection of a new colonic lesion was lower in the ASA group than in the placebo group (HR for the detection of a new polyp, 0.54; 95% CI, 0.43–0.94; P = .022).[7] In a study of 1,121 patients with a recent history of colorectal adenomas, after a mean duration of treatment of 33 months, the unadjusted RRs of any adenoma (as compared with the placebo group) were 0.81 in the 81 mg/day ASA group (95% CI, 0.69–0.96) and 0.96 in the 325 mg/day ASA group (95% CI, 0.81–1.13). For advanced neoplasms (adenomas ≥10.0 mm in diameter or with tubulovillous or villous features, severe dysplasia, or invasive cancer), the RRs were 0.59 (95% CI, 0.38–0.92) in the 81 mg/day ASA group, and 0.83 (95% CI, 0.55–1.23) in the 325 mg/day ASA group, respectively.[8]
ASA has also been evaluated for its potential effects on CRC mortality. A 2010 individual patient level data meta-analysis analyzed long-term (median follow-up, 18.3 years) data from four RCTs of primary and secondary cardiovascular disease prevention; it found that allocation to use of 75 to 1,200 mg of daily ASA for at least one year reduced the cumulative risk of colon cancer death compared with controls (HR, 0.67; 95% CI, 0.52–0.86). Aspirin reduced CRC mortality beginning 10 to 20 years after randomization, but not before.[2] A 2011 individual participant level data meta-analysis examined data from six RCTs of primary or secondary cardiovascular disease prevention. In trials with allocation to ASA after at least 5 years of in-trial follow-up, the HR for CRC mortality was 0.41 (95% CI, 0.71–1.00). There was no statistically significant effect during the first five years after randomization.[9]
Six RCTs, including five from the United Kingdom, were included in a meta-analysis in which patients were randomly assigned to receive either aspirin or placebo, and the mean scheduled duration of trial treatment was 4 years or more. Individual patient data for all in-trial cancer deaths were obtained. In the three United Kingdom trials, cancer deaths after completion of the trials were obtained via death certification and cancer registration, taking the follow-up to 20 years after randomization. Based on meta-analysis of odds ratios (ORs) from each trial rather than on more sensitive actuarial analysis of the individual patient data, allocation to aspirin in the RCTs reduced the 20-year risk of death due to CRC. ORs for maximum aspirin use were 0.55 for CRC risk (95% CI, 0.41–0.76) and for any aspirin use were 0.58 for CRC risk (95% CI, 0.44–0.78).[10]
The Women’s Health Study, the largest randomized trial of aspirin to date (N = 39,876), found no reduction in CRC mortality rates with the use of every other day low-dose aspirin during the first 10 years of follow-up. The study did not report on longer-term risk for CRC mortality.[4]
Aspirin has several important potential harms associated with its use that should be a part of any consideration of its use as a disease prevention strategy. Regular low-dose aspirin use increases the risks for major gastrointestinal bleeding and intracranial bleeding events, including hemorrhagic strokes. A systematic review of studies of aspirin use for primary cardiovascular disease prevention found that use of 100 mg or more of aspirin daily or every other day increased a person’s risk for a major gastrointestinal bleed by 58% (OR, 1.58; 95% CI, 1.29–1.95) or an intracranial hemorrhage by 30% (OR, 1.30; 95% CI, 1.00–1.68). These risks may be greater among older individuals, men, and those individuals with comorbid risk factors that promote a risk of bleeding.[11]
Hormone Therapy (Estrogen Plus Progestin)
Several observational studies have suggested a decreased risk of colon cancer among users of postmenopausal female hormone supplements.[12–15] For rectal cancer, most studies have observed no association or a slightly elevated risk.[16–18]
The Women’s Health Initiative (WHI) trial examined, as a secondary end point, the effect of combined estrogen-plus-progestin therapy and estrogen-only therapy on CRC incidence and mortality. Among women in the combined estrogen-plus-progestin group of the WHI, an extended follow-up (mean, 11.6 years) confirmed that fewer CRC were diagnosed in the combined hormone therapy group than in the placebo group (HR, 0.72; 95% CI, 0.56–0.94); the CRCs in women in the combined group were more likely to have lymph node involvement than the CRCs in women in the placebo group (50.5% vs. 28.6%; P < .001) and were classified at higher stages (regional and distant) (68.8% vs. 51.4%; P = .003). The number of CRC deaths in the combined group was higher than in the placebo group (37 vs. 27 deaths), but the difference was not statistically significant (HR, 1.29; 95% CI, 0.78–2.11).[19]
Polyp Removal
An analysis of data from the National Polyp Study (NPS), with external, historical controls, has commonly been cited to show a reduction of 76% to 90% in the subsequent incidence of CRC after colonoscopic polypectomy compared with three nonconcurrent, historical control groups.[20] This study may be biased in several ways that inflate the apparent efficacy of polyp removal; the main problem is that potential enrollees in the NPS were excluded if they had CRC at their baseline examination. Because no such exclusions (or baseline colonoscopy examinations) were done in the three comparison groups, individuals who had CRC at baseline would be counted as having incident CRC in subsequent follow-up. Although adjustments were attempted, it is not possible to know the magnitude of the impact of this problem on the result because it is not known how long CRC may be present without causing symptoms.
An additional long-term follow-up study (median follow-up, 15.8 years; maximum, 23 years) of the NPS cohort suggested an approximately 53% reduction in CRC mortality due to polypectomy (not just exclusion of individuals with CRC at initial exam). However, the degree of reduction must be viewed with caution because this study did not have a direct comparison group, relying mainly on comparison to expected data from the National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) Program. Further, details are not clear regarding factors that may have led to decreased mortality. Patients in the NPS were assigned to colonoscopy at years 1 and 3; colonoscopy was also offered to one of the two comparison groups at year 1; all participants were offered colonoscopy at year 6. However, following year 6, the exact surveillance that patients may have undergone and how that surveillance might have been associated with decreased CRC mortality were not well described.[21]
It is expected that further follow-up in the United Kingdom Flexible Sigmoidoscopy Screening Trial will be able to provide more detail about the long-term effect of polypectomy, at least on the left side of the colon.[21]
Other evidence about the benefit of sigmoidoscopy screening (at which time both polyps and early cancer would be removed) suggests that the impact of endoscopic screening, at least on the left side of the colon, is substantial and prolonged. In an RCT, 170,000 individuals were randomly assigned to one-time sigmoidoscopy versus usual care. At sigmoidoscopy, polyps were removed, cancer was detected, and patients were referred for treatment. Based on sigmoidoscopy findings, individuals were considered to have low risk if they had normal exams or only one or two small (<1 cm) tubular adenomas. These individuals were not referred either for colonoscopy workup, or for colonoscopic surveillance. In a follow-up of 10 years, the left-sided CRC incidence in the low-risk group (about 95% of attendees were low risk) was 0.02% to 0.04% per year—a very low risk of CRC compared with average risk. The cause of reduced risk—whether due to detection and removal of large polyps or small ones, or selection of individuals at lower risk—is yet unclear.[22] The natural history of large polyps is not well known, but some evidence suggests that such lesions become clinical CRC at a rate of approximately 1% per year.[23] As a result of the strong data about the impact of endoscopy on the left colon, evidence from multiple studies has raised questions about the ability of endoscopy to reduce CRC mortality in the right colon.[24–26] Thus, it is unclear what the overall impact of endoscopy (e.g., colonoscopy screening) is, and whether there may be a large difference in impact on the left side of the colon compared with the right side.[24]
Other studies suggest that the polyps with the greatest potential to progress to CRC are larger polyps (i.e., >1.0 cm), which include most of those with villous or high-grade histological features. Retrospective cohort studies also show the harms associated with polypectomy, including bleeding.[27,28]
References
Flossmann E, Rothwell PM; British Doctors Aspirin Trial and the UK-TIA Aspirin Trial: Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet 369 (9573): 1603-13, 2007. [PUBMED Abstract]
Rothwell PM, Wilson M, Elwin CE, et al.: Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 376 (9754): 1741-50, 2010. [PUBMED Abstract]
Chubak J, Whitlock EP, Williams SB, et al.: Aspirin for the Prevention of Cancer Incidence and Mortality: Systematic Evidence Reviews for the U.S. Preventive Services Task Force. Ann Intern Med 164 (12): 814-25, 2016. [PUBMED Abstract]
Cook NR, Lee IM, Zhang SM, et al.: Alternate-day, low-dose aspirin and cancer risk: long-term observational follow-up of a randomized trial. Ann Intern Med 159 (2): 77-85, 2013. [PUBMED Abstract]
Wei EK, Colditz GA, Giovannucci EL, et al.: Cumulative risk of colon cancer up to age 70 years by risk factor status using data from the Nurses’ Health Study. Am J Epidemiol 170 (7): 863-72, 2009. [PUBMED Abstract]
Burn J, Sheth H, Elliott F, et al.: Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: a double-blind, randomised, placebo-controlled trial. Lancet 395 (10240): 1855-1863, 2020. [PUBMED Abstract]
Sandler RS, Halabi S, Baron JA, et al.: A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N Engl J Med 348 (10): 883-90, 2003. [PUBMED Abstract]
Baron JA, Cole BF, Sandler RS, et al.: A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med 348 (10): 891-9, 2003. [PUBMED Abstract]
Rothwell PM, Fowkes FG, Belch JF, et al.: Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet 377 (9759): 31-41, 2011. [PUBMED Abstract]
Algra AM, Rothwell PM: Effects of regular aspirin on long-term cancer incidence and metastasis: a systematic comparison of evidence from observational studies versus randomised trials. Lancet Oncol 13 (5): 518-27, 2012. [PUBMED Abstract]
Whitlock EP, Burda BU, Williams SB, et al.: Bleeding Risks With Aspirin Use for Primary Prevention in Adults: A Systematic Review for the U.S. Preventive Services Task Force. Ann Intern Med 164 (12): 826-35, 2016. [PUBMED Abstract]
Calle EE, Miracle-McMahill HL, Thun MJ, et al.: Estrogen replacement therapy and risk of fatal colon cancer in a prospective cohort of postmenopausal women. J Natl Cancer Inst 87 (7): 517-23, 1995. [PUBMED Abstract]
Newcomb PA, Storer BE: Postmenopausal hormone use and risk of large-bowel cancer. J Natl Cancer Inst 87 (14): 1067-71, 1995. [PUBMED Abstract]
Grodstein F, Newcomb PA, Stampfer MJ: Postmenopausal hormone therapy and the risk of colorectal cancer: a review and meta-analysis. Am J Med 106 (5): 574-82, 1999. [PUBMED Abstract]
Terry MB, Neugut AI, Bostick RM, et al.: Risk factors for advanced colorectal adenomas: a pooled analysis. Cancer Epidemiol Biomarkers Prev 11 (7): 622-9, 2002. [PUBMED Abstract]
Risch HA, Howe GR: Menopausal hormone use and colorectal cancer in Saskatchewan: a record linkage cohort study. Cancer Epidemiol Biomarkers Prev 4 (1): 21-8, 1995 Jan-Feb. [PUBMED Abstract]
Gerhardsson de Verdier M, London S: Reproductive factors, exogenous female hormones, and colorectal cancer by subsite. Cancer Causes Control 3 (4): 355-60, 1992. [PUBMED Abstract]
Prihartono N, Palmer JR, Louik C, et al.: A case-control study of use of postmenopausal female hormone supplements in relation to the risk of large bowel cancer. Cancer Epidemiol Biomarkers Prev 9 (4): 443-7, 2000. [PUBMED Abstract]
Simon MS, Chlebowski RT, Wactawski-Wende J, et al.: Estrogen plus progestin and colorectal cancer incidence and mortality. J Clin Oncol 30 (32): 3983-90, 2012. [PUBMED Abstract]
Winawer SJ, Zauber AG, Ho MN, et al.: Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 329 (27): 1977-81, 1993. [PUBMED Abstract]
Zauber AG, Winawer SJ, O’Brien MJ, et al.: Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 366 (8): 687-96, 2012. [PUBMED Abstract]
Atkin WS, Edwards R, Kralj-Hans I, et al.: Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375 (9726): 1624-33, 2010. [PUBMED Abstract]
Stryker SJ, Wolff BG, Culp CE, et al.: Natural history of untreated colonic polyps. Gastroenterology 93 (5): 1009-13, 1987. [PUBMED Abstract]
Brenner H, Chang-Claude J, Seiler CM, et al.: Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med 154 (1): 22-30, 2011. [PUBMED Abstract]
Baxter NN, Goldwasser MA, Paszat LF, et al.: Association of colonoscopy and death from colorectal cancer. Ann Intern Med 150 (1): 1-8, 2009. [PUBMED Abstract]
Brenner H, Hoffmeister M, Arndt V, et al.: Protection from right- and left-sided colorectal neoplasms after colonoscopy: population-based study. J Natl Cancer Inst 102 (2): 89-95, 2010. [PUBMED Abstract]
Levin TR, Zhao W, Conell C, et al.: Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med 145 (12): 880-6, 2006. [PUBMED Abstract]
Warren JL, Klabunde CN, Mariotto AB, et al.: Adverse events after outpatient colonoscopy in the Medicare population. Ann Intern Med 150 (12): 849-57, W152, 2009. [PUBMED Abstract]
Factors With Inadequate Evidence of an Association With Colorectal Cancer
Nonsteroidal Anti-Inflammatory Drugs
One large cohort study (301,240 people with 3,894 colorectal cancer [CRC] cases) found an association between daily or weekly nonaspirin (non-ASA) nonsteroidal anti-inflammatory drug (NSAID) use and reduced 10-year incidence of proximal and distal colon cancer, but not rectal cancer, with a hazard ratio (HR) of 0.67 (95% confidence interval [CI], 0.58–0.77) for daily use for colon cancer. Because exposure to non-ASA NSAIDs was assessed only once, assessment was by self-report, and there is no information on dose or duration of use, the certainty of this single study must be rated low. Further research is needed before this finding can be accepted.[1]
Although evidence is currently inadequate to determine whether NSAIDs reduce CRC incidence, proponents suggest that any effect of these drugs results from their ability to inhibit the activity of cyclooxygenase (COX). COX is important in the transformation of arachidonic acid into prostanoids, prostaglandins, and thromboxane A2. NSAIDs include not only aspirin (ASA, which is considered separately here) and other, first-generation nonselective inhibitors of the two functional isoforms of COX, termed COX-1 and COX-2, but also newer second-generation drugs that inhibit primarily COX-2. Normally, COX-1 is expressed in most tissues and primarily plays a housekeeping role (e.g., gastrointestinal mucosal protection and platelet aggregation). COX-2 activity is crucial in stress responses and in mediating and propagating the pain and inflammation that are characteristic of arthritis.[2]
Nonselective COX inhibitors include indomethacin (Indocin); sulindac (Clinoril); piroxicam (Feldene); diflunisal (Dolobid); ibuprofen (Advil, Motrin); ketoprofen (Orudis); naproxen (Naprosyn); and naproxen sodium (Aleve, Anaprox). Selective COX-2 inhibitors include celecoxib (Celebrex), rofecoxib (Vioxx), and valdecoxib (Bextra). Rofecoxib and valdecoxib are no longer marketed because of an associated increased risk of serious cardiovascular events.
Both celecoxib and rofecoxib have been associated with serious cardiovascular events including dose-related death from cardiovascular causes, myocardial infarction, stroke, or heart failure.[3–6] Four trials that demonstrated this increased risk are summarized in the Table 1. In addition, a network meta-analysis of all large scale randomized controlled trials (RCTs) comparing any NSAID to any other NSAID or placebo found that there is little evidence to suggest that any of the investigated drugs are safe in terms of cardiovascular effects. Naproxen seemed least harmful.[7]
Table 1. Cardiovascular Risks Associated With Celecoxib and Rofecoxib Dose/Drugs
Authors
Dose/Trial Drug
Risk
Study Type
bid = twice a day; qd = every day; CI = confidence interval; HR = hazard ratio; OR = odds ratio; RR = relative risk; Rx = prescription.
Chemoprevention of sporadic adenoma; median study Rx 7.4 months
Other major harms from all NSAIDs are gastrointestinal bleeding and renal impairment. The incidence of reported major gastrointestinal bleeding events appears to be dose-related.[8]
Celecoxib reduces the incidence of adenomas; however, celecoxib does not have a clinical role in reducing the risk of sporadic CRC. Its long-term efficacy in preventing CRC has not been shown because of increased risk of cardiovascular events, and because there are other effective ways, such as screening to reduce CRC mortality.[9] A population-based retrospective cohort study of nonaspirin NSAID use among individuals aged 65 years and older was associated with lower risk of CRC, particularly with longer durations of use.[10]
Several rigorous studies have demonstrated the effectiveness of sulindac in reducing the size and number of adenomas in familial polyposis.[11,12] In a randomized, double-blind, placebo-controlled study of 77 patients with familial adenomatous polyposis, patients receiving 400 mg of celecoxib twice a day had a 28.0% reduction in the mean number of colorectal adenomas (P = .003 for the comparison with placebo) and a 30.7% reduction in the polyp burden (sum of polyp diameters; P = .001) as compared with reductions of 4.5% and 4.9%, respectively, in the placebo group. The reductions in the group receiving 100 mg of celecoxib twice a day were 11.9% (P = .33 for the comparison with placebo) and 14.6% (P = .09), respectively. The incidence of adverse events was similar among the groups.[13]
The NSAID piroxicam, at a dose of 20 mg/day, reduced mean rectal prostaglandin concentration by 50% in individuals with a history of adenomas.[14] Several studies assessing the effect of ASA or other nonsteroidals on polyp recurrence following polypectomy are in progress.[15] In several of these studies, mucosal prostaglandin concentration is being measured.
The potential for use of NSAIDs as a primary prevention measure is being studied. There are, however, several unresolved issues that preclude making general recommendations for their use. These include a paucity of knowledge about the proper dose and duration for these agents, and concern about whether the potential preventive benefits such as a reduction in the frequency or intensity of screening or surveillance could counterbalance long-term risks such as gastrointestinal ulceration and hemorrhagic stroke for the average-risk individual.[16]
Calcium supplements
A randomized placebo-controlled trial tested the effect of calcium supplementation (3 g calcium carbonate daily [1,200 mg elemental calcium]) on the risk of recurrent adenoma.[17] The primary end point was the proportion of patients (72% of whom were male) in whom at least one adenoma was detected following a first and/or second follow-up endoscopy. A modest decrease in risk was found for both developing at least one recurrent adenoma (adjusted risk ratio [ARR], 0.81; 95% CI, 0.67–0.99) and in the average number of adenomas (ARR, 0.76; 95% CI, 0.60–0.96). The investigators found the effect of calcium was similar across age, sex, and baseline dietary intake categories of calcium, fat, or fiber. The study was limited to individuals with a recent history of colorectal adenomas and could not determine the effect of calcium on risk of the first adenoma, nor was it large enough or of sufficient duration to examine the risk of invasive CRC. After calcium supplementation is stopped, the lower risk may persist up to 5 years.[18] The results of other ongoing adenoma recurrence studies are awaited with interest. It is important to note that the dose of calcium salt administered may be important; the usual daily doses in trials have ranged from 1,250 to 2,000 mg of calcium.
In a randomized, double-blind, placebo-controlled trial involving 36,282 postmenopausal women, the administration of 500 mg of elemental calcium and 200 IU of vitamin D3 twice daily for an average of 7.0 years was not associated with a reduction in invasive CRC (HR, 1.08; 95% CI, 0.86–1.34; P = .051).[19] The relatively short duration of follow-up, considering the latency period of CRC of 10 to 15 years, and suboptimal doses of calcium and vitamin D, may account for the negative effects of this trial, although other factors may also be responsible.[20]
Dietary Factors
Dietary fat and meat intake
Colon cancer rates are high in populations with high total fat intakes and are lower in those consuming less fat.[21] On average, fat comprises 40% to 45% of total caloric intake in high-incidence Western countries; in low-risk populations, fat accounts for only 10% of dietary calories.[22] Several case-control studies have explored the association of colon cancer risk with meat or fat consumption, as well as protein and energy intake.[23,24] Although positive associations with meat consumption or with fat intake have been found, the results have been inconsistent.[25] A number of prospective cohort studies have been conducted in the United States and abroad; a systematic review of 13, including the Iowa Women’s Health Study and the Nurses’ Health Study, concluded that there appeared to be a positive association between meat consumption and CRC incidence. However, the authors noted that because only a few studies tried to investigate the independent effect of meat intake on cancer risk, the observed relationship might be attributed entirely to confounding.[26] Similarly, a 2019 systematic review of observational studies, evaluating the association between processed or unprocessed red meat consumption and CRC incidence and mortality, concluded that a reduction of three servings per week resulted in very small to no decreases in those outcomes, although the certainty around these findings was judged low to very low.[27]
A randomized controlled dietary modification study was undertaken among 48,835 postmenopausal women aged 50 to 79 years who were also enrolled in the WHI. The intervention promoted a goal of reducing total fat intake by 20%, while increasing daily intake of vegetables, fruits, and grains. The intervention group accomplished a reduction of fat intake of approximately 10% more than did the comparison group during the 8.1 years of follow-up. There was no evidence of reduction in invasive CRCs between the intervention and comparison groups with an HR of 1.08 (95% CI, 0.90–1.29).[28] Likewise, there was no benefit of the low-fat diet on all-cancer mortality, overall mortality, or cardiovascular disease.[29] This last observation was echoed in a 2019 systematic review of randomized controlled trials of the effect of variable red meat consumption on cancer outcomes. This review relied heavily on the WHI to reach the conclusion that there appears to be little to no effect of red meat intake on CRC incidence, although the certainty around this finding is low because of limitations in available studies.[30]
Explanations for the conflicting results regarding whether dietary fat or meat intake affects the risk of CRC [31] include the following:
Validity of dietary questionnaires used.
Differences in the average age of the population studied.
Variations in methods of meat preparation (in some instances, mutagenic and carcinogenic heterocyclic amines could have been released at high temperatures).[32]
Variability in the consumption of other foods such as vegetables.[33]
Possible unadjusted bias from differential screening uptake between meat intake groups.
Six case-control studies and two cohort studies have explored potential dietary risk factors for colorectal adenomas.[34,35] Three of the eight studies found that higher fat consumption was associated with increased risk. High fat intake has been found to increase the risk of adenoma recurrence following polypectomy.[36] In a multicenter RCT, a diet low in fat (20% of total calories) and high in fiber, fruits, and vegetables did not reduce the risk of recurrence of colorectal adenomas.[37]
Thus, the evidence is inadequate to determine whether reducing dietary fat and meat would reduce CRC incidence.
References
Ruder EH, Laiyemo AO, Graubard BI, et al.: Non-steroidal anti-inflammatory drugs and colorectal cancer risk in a large, prospective cohort. Am J Gastroenterol 106 (7): 1340-50, 2011. [PUBMED Abstract]
Kerr DJ, Dunn JA, Langman MJ, et al.: Rofecoxib and cardiovascular adverse events in adjuvant treatment of colorectal cancer. N Engl J Med 357 (4): 360-9, 2007. [PUBMED Abstract]
Graham DJ, Campen D, Hui R, et al.: Risk of acute myocardial infarction and sudden cardiac death in patients treated with cyclo-oxygenase 2 selective and non-selective non-steroidal anti-inflammatory drugs: nested case-control study. Lancet 365 (9458): 475-81, 2005. [PUBMED Abstract]
Bresalier RS, Sandler RS, Quan H, et al.: Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 352 (11): 1092-102, 2005. [PUBMED Abstract]
Solomon SD, McMurray JJ, Pfeffer MA, et al.: Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med 352 (11): 1071-80, 2005. [PUBMED Abstract]
Chan AT, Giovannucci EL, Meyerhardt JA, et al.: Long-term use of aspirin and nonsteroidal anti-inflammatory drugs and risk of colorectal cancer. JAMA 294 (8): 914-23, 2005. [PUBMED Abstract]
Arber N, Eagle CJ, Spicak J, et al.: Celecoxib for the prevention of colorectal adenomatous polyps. N Engl J Med 355 (9): 885-95, 2006. [PUBMED Abstract]
Smalley W, Ray WA, Daugherty J, et al.: Use of nonsteroidal anti-inflammatory drugs and incidence of colorectal cancer: a population-based study. Arch Intern Med 159 (2): 161-6, 1999. [PUBMED Abstract]
Labayle D, Fischer D, Vielh P, et al.: Sulindac causes regression of rectal polyps in familial adenomatous polyposis. Gastroenterology 101 (3): 635-9, 1991. [PUBMED Abstract]
Giardiello FM, Hamilton SR, Krush AJ, et al.: Treatment of colonic and rectal adenomas with sulindac in familial adenomatous polyposis. N Engl J Med 328 (18): 1313-6, 1993. [PUBMED Abstract]
Steinbach G, Lynch PM, Phillips RK, et al.: The effect of celecoxib, a cyclooxygenase-2 inhibitor, in familial adenomatous polyposis. N Engl J Med 342 (26): 1946-52, 2000. [PUBMED Abstract]
Earnest DL, Hixson LJ, Fennerty MB, et al.: Inhibition of prostaglandin synthesis: potential for chemoprevention of human colon cancer. Cancer Bull 43(6): 561-568, 1991.
Vargas PA, Alberts DS: Colon cancer: the quest for prevention. Oncology (Huntingt) 7 (11 Suppl): 33-40, 1993.
Imperiale TF: Aspirin and the prevention of colorectal cancer. N Engl J Med 348 (10): 879-80, 2003. [PUBMED Abstract]
Baron JA, Beach M, Mandel JS, et al.: Calcium supplements for the prevention of colorectal adenomas. Calcium Polyp Prevention Study Group. N Engl J Med 340 (2): 101-7, 1999. [PUBMED Abstract]
Grau MV, Baron JA, Sandler RS, et al.: Prolonged effect of calcium supplementation on risk of colorectal adenomas in a randomized trial. J Natl Cancer Inst 99 (2): 129-36, 2007. [PUBMED Abstract]
Wactawski-Wende J, Kotchen JM, Anderson GL, et al.: Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med 354 (7): 684-96, 2006. [PUBMED Abstract]
Forman MR, Levin B: Calcium plus vitamin D3 supplementation and colorectal cancer in women. N Engl J Med 354 (7): 752-4, 2006. [PUBMED Abstract]
Rose DP, Boyar AP, Wynder EL: International comparisons of mortality rates for cancer of the breast, ovary, prostate, and colon, and per capita food consumption. Cancer 58 (11): 2363-71, 1986. [PUBMED Abstract]
Reddy BS: Dietary fat and its relationship to large bowel cancer. Cancer Res 41 (9 Pt 2): 3700-5, 1981. [PUBMED Abstract]
Potter JD: Reconciling the epidemiology, physiology, and molecular biology of colon cancer. JAMA 268 (12): 1573-7, 1992 Sep 23-30. [PUBMED Abstract]
Potter JD, McMichael AJ: Diet and cancer of the colon and rectum: a case-control study. J Natl Cancer Inst 76 (4): 557-69, 1986. [PUBMED Abstract]
Bingham SA: Diet and large bowel cancer. J R Soc Med 83 (7): 420-2, 1990. [PUBMED Abstract]
Hirayama T, Tannenbaum SR, Reddy BS, et al.: A large-scale cohort study on the relationship between diet and selected cancers of the digestive organs. In: Bruce WR, Correa P, Lipkin M, et al., eds.: Gastrointestinal cancer: endogenous factors. Cold Spring Harbor Laboratory, 1981, Branbury Report 7, 409-429.
Bjelke E: Epidemiology of colorectal cancer, with emphasis on diet. Int Congr Ser 484: 158-174, 1980.
Beresford SA, Johnson KC, Ritenbaugh C, et al.: Low-fat dietary pattern and risk of colorectal cancer: the Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA 295 (6): 643-54, 2006. [PUBMED Abstract]
Howard BV, Van Horn L, Hsia J, et al.: Low-fat dietary pattern and risk of cardiovascular disease: the Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA 295 (6): 655-66, 2006. [PUBMED Abstract]
Zeraatkar D, Johnston BC, Bartoszko J, et al.: Effect of Lower Versus Higher Red Meat Intake on Cardiometabolic and Cancer Outcomes: A Systematic Review of Randomized Trials. Ann Intern Med 171 (10): 721-731, 2019. [PUBMED Abstract]
Goldbohm RA, van den Brandt PA, van ‘t Veer P, et al.: A prospective cohort study on the relation between meat consumption and the risk of colon cancer. Cancer Res 54 (3): 718-23, 1994. [PUBMED Abstract]
Sugimura T: Carcinogenicity of mutagenic heterocyclic amines formed during the cooking process. Mutat Res 150 (1-2): 33-41, 1985 Jun-Jul. [PUBMED Abstract]
Lee HP, Gourley L, Duffy SW, et al.: Colorectal cancer and diet in an Asian population–a case-control study among Singapore Chinese. Int J Cancer 43 (6): 1007-16, 1989. [PUBMED Abstract]
Kampman E, Giovannucci E, van ‘t Veer P, et al.: Calcium, vitamin D, dairy foods, and the occurrence of colorectal adenomas among men and women in two prospective studies. Am J Epidemiol 139 (1): 16-29, 1994. [PUBMED Abstract]
Neugut AI, Garbowski GC, Lee WC, et al.: Dietary risk factors for the incidence and recurrence of colorectal adenomatous polyps. A case-control study. Ann Intern Med 118 (2): 91-5, 1993. [PUBMED Abstract]
Schatzkin A, Lanza E, Corle D, et al.: Lack of effect of a low-fat, high-fiber diet on the recurrence of colorectal adenomas. Polyp Prevention Trial Study Group. N Engl J Med 342 (16): 1149-55, 2000. [PUBMED Abstract]
Factors and Interventions With Adequate Evidence of no Association With Colorectal Cancer
Estrogen-Only Therapy
The estrogen-only intervention component of the Women’s Health Initiative was conducted among women who had a hysterectomy, with colorectal cancer (CRC) incidence included as a secondary trial end point. CRC incidence was not decreased among women who had taken estrogens. After a median follow-up of 7.1 years, 58 invasive cancers occurred in the estrogen arm compared with 53 invasive cancers in the placebo arm (hazard ratio [HR], 1.12; 95% confidence interval [CI], 0.77–1.63). Tumor stage and grade were similar in the two groups; deaths after CRC were 34% in the hormone group compared with 30% in the placebo group (HR, 1.34; 95% CI, 0.58–3.19).[1]
Statins
Overall, evidence indicates that statin use neither increases nor decreases the incidence or mortality of CRC. Although some case-control studies have shown a reduction in risk, neither a large cohort study [2] nor a meta-analysis of four randomized controlled trials [3] found any effect of statin use.
References
Ritenbaugh C, Stanford JL, Wu L, et al.: Conjugated equine estrogens and colorectal cancer incidence and survival: the Women’s Health Initiative randomized clinical trial. Cancer Epidemiol Biomarkers Prev 17 (10): 2609-18, 2008. [PUBMED Abstract]
Jacobs EJ, Rodriguez C, Brady KA, et al.: Cholesterol-lowering drugs and colorectal cancer incidence in a large United States cohort. J Natl Cancer Inst 98 (1): 69-72, 2006. [PUBMED Abstract]
Dale KM, Coleman CI, Henyan NN, et al.: Statins and cancer risk: a meta-analysis. JAMA 295 (1): 74-80, 2006. [PUBMED Abstract]
Latest Updates to This Summary (04/11/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Updated statistic with estimated new cases and deaths for 2025 (cited Bray et al. as reference 1 and American Cancer Society as reference 2). Also revised text to state that between 2012 and 2021, incidence rates increased by 2.4% per year in individuals younger than 50 years and by 0.4% per year in individuals aged 50 to 64 years.
This summary is written and maintained by the PDQ Screening and Prevention Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about colorectal cancer prevention. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Screening and Prevention Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Screening and Prevention Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Colorectal Cancer Prevention. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/hp/colorectal-prevention-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389222]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Cancer prevention is action taken to lower the chance of getting cancer. By preventing cancer, the number of new cases of cancer in a group or population is lowered. Hopefully, this will lower the number of deaths caused by cancer.
To prevent new cancers from starting, scientists look at risk factors and protective factors. Anything that increases your chance of developing cancer is called a cancer risk factor; anything that decreases your chance of developing cancer is called a cancer protective factor.
Some risk factors for cancer can be avoided, but many cannot. For example, both smoking and inheriting certain genes are risk factors for some types of cancer, but only smoking can be avoided. Regular exercise and a healthy diet may be protective factors for some types of cancer. Avoiding risk factors and increasing protective factors may lower your risk, but it does not mean that you will not get cancer.
Different ways to prevent cancer are being studied, including:
changing lifestyle or eating habits
avoiding things known to cause cancer
taking medicines to treat a precancerous condition or to keep cancer from starting
General Information About Colorectal Cancer
Key Points
Colorectal cancer is a disease in which malignant (cancer) cells form in the tissues of the colon or the rectum.
Colorectal cancer is the second leading cause of death from cancer in the United States.
Colorectal cancer is a disease in which malignant (cancer) cells form in the tissues of the colon or the rectum.
The colon is part of the body’s digestive system. The digestive system removes and processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps pass waste material out of the body. The digestive system is made up of the mouth, throat, esophagus, stomach, and the small and large intestines. The colon (large bowel) is the first part of the large intestine and is about 5 feet long. Together, the rectum and anal canal make up the last part of the large intestine and are 6 to 8 inches long. The anal canal ends at the anus (the opening of the large intestine to the outside of the body).
EnlargeAnatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Cancer that begins in the colon is called colon cancer, and cancer that begins in the rectum is called rectal cancer. Cancer that affects either of these organs may also be called colorectal cancer.
Other PDQ summaries containing information related to colorectal cancer include:
Colorectal cancer is the second leading cause of death from cancer in the United States.
Colorectal cancer is the third most common cancer worldwide and the second leading cause of cancer death in the United States when numbers for men and women are combined. Between 2012 and 2021, the number of new colorectal cancer cases in the United States decreased. This decline was largely driven by falling rates in adults aged 65 and older, who continue to have the highest overall rates of colorectal cancer. The drop in older adults may be due in part to increased colorectal cancer screening, which can detect and remove precancerous growths before they develop into cancer. However, trends vary by age group. Among adults younger than 50, the number of new cases of colorectal cancer rose by about 2.4% per year, the largest increase among all age groups. In people aged 50 to 64, the number of new cases increased slightly per year.
Since 1970, the death rate from colorectal cancer has declined in men and women. However, new cases and deaths from colorectal cancer remain higher among Black people than other racial groups. Studies show that Black people are not more likely than others to have precancerous growths.
Finding and treating colorectal cancer early may prevent death from colorectal cancer. Screening tests may be used to help find colorectal cancer.
Colorectal Cancer Prevention
Key Points
Avoiding risk factors and increasing protective factors may help prevent cancer.
The following risk factors increase the risk of colorectal cancer:
Age
Family history of colorectal cancer
Personal history
Inherited risk
Alcohol
Cigarette smoking
Race
Obesity
The following protective factors decrease the risk of colorectal cancer:
Physical activity
Aspirin
Combination hormone replacement therapy
Polyp removal
It is not clear if the following affect the risk of colorectal cancer:
Nonsteroidal anti-inflammatory drugs (NSAIDs) other than aspirin
Calcium
Diet
The following factors do not affect the risk of colorectal cancer:
Hormone replacement therapy with estrogen only
Statins
Cancer prevention clinical trials are used to study ways to prevent cancer.
New ways to prevent colorectal cancer are being studied in clinical trials.
Avoiding risk factors and increasing protective factors may help prevent cancer.
Avoiding cancerrisk factors may help prevent certain cancers. Risk factors include smoking, having overweight, and not getting enough exercise. Increasing protective factors such as quitting smoking and exercising may also help prevent some cancers. Talk to your doctor or other health care professional about how you might lower your risk of cancer.
The following risk factors increase the risk of colorectal cancer:
Age
The risk of colorectal cancer increases after age 50. Most cases of colorectal cancer are diagnosed after age 50.
Family history of colorectal cancer
Having a parent, brother, sister, or child with colorectal cancer doubles a person’s risk of colorectal cancer.
Personal history
Having a personal history of the following conditions increases the risk of colorectal cancer:
previous colorectal cancer
high-risk adenomas (colorectal polyps that are 1 centimeter or larger in size or that have cells that look abnormal under a microscope)
Drinking 3 or more alcoholic beverages per day increases the risk of colorectal cancer. Drinking alcohol is also linked to the risk of forming large colorectal adenomas (benign tumors).
Cigarette smoking
Cigarette smoking is linked to an increased risk of colorectal cancer and death from colorectal cancer.
Smoking cigarettes is also linked to an increased risk of forming colorectal adenomas. Cigarette smokers who have had surgery to remove colorectal adenomas are at an increased risk for the adenomas to recur (come back).
Race
Black individuals have an increased risk of colorectal cancer and death from colorectal cancer compared to other races.
Obesity
Obesity is linked to an increased risk of colorectal cancer and death from colorectal cancer.
The following protective factors decrease the risk of colorectal cancer:
Physical activity
A lifestyle that includes regular physical activity is linked to a decreased risk of colorectal cancer.
Aspirin
Studies have shown that taking aspirin daily for at least two years lowers the risk of colorectal cancer and the risk of death from colorectal cancer. The decrease in risk begins 10 to 20 years after patients start taking aspirin.
The possible harms of aspirin use (100 mg or less) daily or every other day include an increased risk of stroke and bleeding in the stomach and intestines. These risks may be greater among the elderly, men, and those with conditions linked to a higher-than-normal risk of bleeding.
However, in women who take combination HRT and do develop colorectal cancer, the cancer is more likely to be advanced when it is diagnosed and the risk of dying from colorectal cancer is not decreased.
The possible harms of combination HRT include an increased risk of:
Most colorectal polyps are adenomas, which may develop into cancer. Removing colorectal polyps that are larger than 1 centimeter (pea-sized) may lower the risk of colorectal cancer. It is not known if removing smaller polyps lowers the risk of colorectal cancer.
The possible harms of polyp removal during colonoscopy or sigmoidoscopy include a tear in the wall of the colon and bleeding.
EnlargePolyps in the colon. Some polyps have a stalk and others do not. Inset shows a photo of a polyp with a stalk.
It is not clear if the following affect the risk of colorectal cancer:
Nonsteroidal anti-inflammatory drugs (NSAIDs) other than aspirin
Studies have shown that taking the nonsteroidal anti-inflammatory drug celecoxib reduces the risk of colorectal adenomas (benign tumors) coming back after they have been removed. It is not clear if this results in a lower risk of colorectal cancer.
Taking sulindac or celecoxib has been shown to reduce the number and size of polyps that form in the colon and rectum of people with familial adenomatous polyposis (FAP). It is not clear if this results in a lower risk of colorectal cancer.
It is not known if taking calciumsupplements lowers the risk of colorectal cancer.
Diet
It is not known if a diet low in fat and meat and high in fiber, fruits, and vegetables lowers the risk of colorectal cancer.
Some studies have shown that a diet high in fat, proteins, calories, and meat increases the risk of colorectal cancer, but other studies have not.
The following factors do not affect the risk of colorectal cancer:
Hormone replacement therapy with estrogen only
Hormone replacement therapy with estrogen only does not lower the risk of having invasive colorectal cancer or the risk of dying from colorectal cancer.
Statins
Studies have shown that taking statins (drugs that lower cholesterol) does not increase or decrease the risk of colorectal cancer.
Cancer prevention clinical trials are used to study ways to prevent cancer.
Cancer prevention clinical trials are used to study ways to lower the risk of developing certain types of cancer. Some cancer prevention trials include healthy people who may or may not have an increased risk of cancer. Other prevention trials include people who have had cancer and are trying to prevent recurrence or a second cancer.
The purpose of some cancer prevention clinical trials is to find out whether actions people take can prevent cancer. These may include eating fruits and vegetables, exercising, quitting smoking, or taking certain medicines, vitamins, minerals, or food supplements.
New ways to prevent colorectal cancer are being studied in clinical trials.
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about colorectal cancer prevention. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Screening and Prevention Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Colorectal Cancer Prevention. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/patient/colorectal-prevention-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389376]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Screening is looking for cancer before a person has any symptoms. This can help find cancer at an early stage. When abnormaltissue or cancer is found early, it may be easier to treat. By the time symptoms appear, cancer may have begun to spread.
Scientists are trying to better understand which people are more likely to get certain types of cancer. They also study the things we do and the things around us to see if they cause cancer. This information helps doctors recommend who should be screened for cancer, which screening tests should be used, and how often the tests should be done.
It is important to remember that your doctor does not necessarily think you have cancer if he or she suggests a screening test. Screening tests are given when you have no cancer symptoms. Screening tests may be repeated on a regular basis.
If a screening test result is abnormal, you may need to have more tests done to find out if you have cancer. These are called diagnostic tests.
General Information About Colorectal Cancer
Key Points
Colorectal cancer is a disease in which malignant (cancer) cells form in the tissues of the colon or the rectum.
Colorectal cancer is the second leading cause of death from cancer in the United States.
Different factors increase or decrease the risk of getting colorectal cancer.
Colorectal cancer is a disease in which malignant (cancer) cells form in the tissues of the colon or the rectum.
The colon and rectum are parts of the body’s digestive system. The digestive system removes and processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps pass waste material out of the body. The digestive system is made up of the mouth, throat, esophagus, stomach, and the small and large intestines. The colon (large bowel) is the first part of the large intestine and is about 5 feet long. Together, the rectum and anal canal make up the last part of the large intestine and are 6 to 8 inches long. The anal canal ends at the anus (the opening of the large intestine to the outside of the body).
EnlargeAnatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Cancer that begins in the colon is called colon cancer, and cancer that begins in the rectum is called rectal cancer. Cancer that begins in either of these organs may also be called colorectal cancer.
Other PDQ summaries containing information related to colorectal cancer include:
Colorectal cancer is the second leading cause of death from cancer in the United States.
Colorectal cancer is the third most common cancer worldwide and the second leading cause of cancer death in the United States when numbers for men and women are combined. Between 2012 and 2021, the number of new colorectal cancer cases in the United States decreased. This decline was largely driven by falling rates in adults aged 65 and older, who continue to have the highest overall rates of colorectal cancer. The drop in older adults may be due in part to increased colorectal cancer screening, which can detect and remove precancerous growths before they develop into cancer. However, trends vary by age group. Among adults younger than 50, the number of new cases of colorectal cancer rose by about 2.4% per year, the largest increase among all age groups. In people aged 50 to 64, the number of new cases increased slightly per year.
Since 1970, the death rate from colorectal cancer has declined in men and women. However, new cases and deaths from colorectal cancer remain higher among Black people than other racial groups. Studies show that Black people are not more likely than others to have precancerous growths.
Different factors increase or decrease the risk of getting colorectal cancer.
Anything that increases your chance of getting a disease is called a risk factor. Anything that decreases your chance of getting a disease is called a protective factor.
Tests are used to screen for different types of cancer when a person does not have symptoms.
Studies show that some screening tests for colorectal cancer help find cancer at an early stage and may decrease the number of deaths from the disease.
The following types of tests are used to screen for colorectal cancer:
Fecal occult blood test
Sigmoidoscopy
Colonoscopy
Virtual colonoscopy
DNA stool test
Studies have shown that screening for colorectal cancer using digital rectal exam does not decrease the number of deaths from the disease.
Screening tests for colorectal cancer are being studied in clinical trials.
Tests are used to screen for different types of cancer when a person does not have symptoms.
Scientists study screening tests to find those with the fewest harms and most benefits. Cancer screening trials also are meant to show whether early detection (finding cancer before it causes symptoms) helps a person live longer or decreases a person’s chance of dying from the disease. For some types of cancer, the chance of recovery is better if the disease is found and treated at an early stage.
Studies show that some screening tests for colorectal cancer help find cancer at an early stage and may decrease the number of deaths from the disease.
The following types of tests are used to screen for colorectal cancer:
Fecal occult blood test
A fecal occult blood test (FOBT) is a test to check stool (solid waste) for blood that can only be seen with a microscope. A small sample of stool is placed on a special card or in a special container and returned to the doctor or laboratory for testing. Blood in the stool may be a sign of polyps, cancer, or other conditions.
There are two types of FOBTs:
Guaiac FOBT: The sample of stool on the special card is tested with a chemical. If there is blood in the stool, the special card changes color. EnlargeA guaiac fecal occult blood test (FOBT) checks for occult (hidden) blood in the stool. Small samples of stool are placed on a special card and returned to a doctor or laboratory for testing.
Immunochemical FOBT: A liquid is added to the stool sample. This mixture is injected into a machine that contains antibodies that can detect blood in the stool. If there is blood in the stool, a line appears in a window in the machine. This test is also called fecal immunochemical test or FIT. EnlargeA fecal immunochemical test (FIT) checks for occult (hidden) blood in the stool. A small sample of stool is placed in a special collection tube or on special cards and returned to a doctor or laboratory for testing.
Sigmoidoscopy
Sigmoidoscopy is a procedure to look inside the rectum and sigmoid (lower) colon for polyps, abnormal areas, or cancer. A sigmoidoscope is inserted through the rectum into the sigmoid colon. A sigmoidoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer.
EnlargeSigmoidoscopy. A thin, lighted tube is inserted through the anus and rectum and into the lower part of the colon to look for abnormal areas.
Colonoscopy
Colonoscopy is a procedure to look inside the rectum and colon for polyps, abnormal areas, or cancer. A colonoscope is inserted through the rectum into the colon. A colonoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer.
EnlargeColonoscopy. A thin, lighted tube is inserted through the anus and rectum and into the colon to look for abnormal areas.
Virtual colonoscopy
Virtual colonoscopy is a procedure that uses a series of x-rays called computed tomography to make a series of pictures of the colon. A computer puts the pictures together to create detailed images that may show polyps and anything else that seems unusual on the inside surface of the colon. This test is also called computed tomography colonography or CTC.
Clinical trials are comparing virtual colonoscopy with other colorectal cancer screening tests. Some clinical trials are testing whether drinking a contrast material that coats the stool, instead of using laxatives to empty the colon, shows polyps clearly.
DNA stool test
This test checks DNA in stool cells for genetic changes that may be a sign of colorectal cancer. Newer versions of this test are used to help screen for colorectal cancer.
Studies have shown that screening for colorectal cancer using digital rectal exam does not decrease the number of deaths from the disease.
A digital rectal exam (DRE) is an exam of the rectum that may be done as part of a routine physical exam. A doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel for lumps or anything else that seems unusual. Study results have shown that DRE does not work as a screening method for colorectal cancer.
Screening tests for colorectal cancer are being studied in clinical trials.
The following colorectal cancer screening tests have risks:
Colonoscopy
Sigmoidoscopy
Virtual colonoscopy
Fecal occult blood test (FOBT) or DNA stool test
Screening tests have risks.
Decisions about screening tests can be difficult. Not all screening tests are helpful and most have risks. Different screening tests have different risks or harms. Screening tests may cause anxiety when you are thinking about or getting ready for the test, or when there is a positive test result. Before having any screening test, you may want to discuss the test with your doctor. It is important to know the risks of the test, and whether it has been proven to reduce the risk of dying from cancer.
Talk to your doctor about your risk for colorectal cancer and the need for screening tests.
False-negative test results can occur.
Screening test results may appear to be normal even though colorectal cancer is present. A person who receives a false-negative test result (one that shows there is no cancer when there really is) may delay seeking medical care even if there are symptoms.
False-positive test results can occur.
Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn’t) can cause anxiety and is usually followed by more tests (such as biopsy), which also have risks.
The following colorectal cancer screening tests have risks:
Colonoscopy
Serious problems caused by colonoscopy are rare, but can include tears in the lining of the colon and bleeding. These problems can be serious and need to be treated in a hospital. Tearing of the lining of the colon and bleeding occur more often when a biopsy or polypectomy is done.
Sedation is used to decrease the discomfort from the procedure. Sedation may cause heart and lung problems, such as irregular heartbeat, heart attack, or trouble breathing.
Sigmoidoscopy
There are fewer complications with a sigmoidoscopy than with a colonoscopy. Although tears in the lining of the colon and bleeding can occur, they are less common than with a colonoscopy. There is usually no sedation with sigmoidoscopy, lowering the risk of complications.
Virtual colonoscopy
Virtual colonoscopy has fewer possible physical harms than either colonoscopy or sigmoidoscopy. The harms of being exposed to radiation from x-rays used in virtual colonoscopy are not known. Virtual colonoscopy often finds problems with organs other than the colon, including the kidneys, chest, liver, ovaries, spleen, and pancreas. Some of these findings lead to more testing, such as colonoscopy, that may not improve the patient’s health.
Fecal occult blood test (FOBT) or DNA stool test
The results of an FOBT or DNAstool test may appear to be abnormal even though no cancer is found. A positive test result may lead to more testing, including colonoscopy.
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about colorectal cancer screening. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Screening and Prevention Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Colorectal Cancer Screening. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/patient/colorectal-screening-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389230]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Evidence of Benefit Associated With Colorectal Cancer Screening
Based on solid evidence, screening for colorectal cancer (CRC) reduces CRC mortality. In addition, there is solid evidence that some CRC screening modalities also reduce CRC incidence. A meta-analysis of randomized controlled trials of flexible sigmoidoscopy found that screening with sigmoidoscopy reduces all-cause mortality.
Table 1. Effect of Screening Intervention on Reducing Incidence and Mortality from Colorectal Cancera
aThere are no data from RCTs on the effect of other screening interventions (i.e., barium enema, computed tomographic colonography, and stool DNA mutation tests) on mortality from CRC. There are also no published results of RCTs of FIT with mortality as an end point.
bFIT is being compared with colonoscopy in two RCTs in Europe (NCT00906997 [Spain] and NCT02078804 [Sweden]), one in the United States (NCT01239082), and one in China (ChiCTR1900025257).[1,2] The trial in Sweden compares colonoscopy with FIT and population controls. Mortality results are not available and may be limited for FIT because of the absence of no-screening comparison groups in several trials. Current guideline recommendations have depended on FIT using the same mechanism as guaiac tests, the most sensitive of which had similar sensitivity to FIT [3] and showed significant reductions in both mortality and incidence of CRC.[3–5]
cThe NordICC trial compares a colonoscopy group with a usual-care control group [NCT00883792].[6]
Fecal Occult Blood Test (fecal immunochemical-based: FIT)
RCTs ongoingb
Fair
Fair
Fair
Fair
Fair
Sigmoidoscopy
RCTs
Good
Good
20%–25%
22%–31%; 13%–50% for distal colon
Fair
Digital Rectal Exam
Case-control studies
Fair
Good
No effect
No effect
Poor
Colonoscopy
One RCT (RCTs in-progress)c; case-control studies; observational cohort studies that use historical/other controls
Poor
Poor
About 60%–70% for left colon; uncertain for right colonc[6]
About 60%–70% for distal colon; uncertain for right colon
Fair
References
Quintero E, Castells A, Bujanda L, et al.: Colonoscopy versus fecal immunochemical testing in colorectal-cancer screening. N Engl J Med 366 (8): 697-706, 2012. [PUBMED Abstract]
Dominitz JA, Robertson DJ, Ahnen DJ, et al.: Colonoscopy vs. Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer (CONFIRM): Rationale for Study Design. Am J Gastroenterol 112 (11): 1736-1746, 2017. [PUBMED Abstract]
Church TR, Ederer F, Mandel JS: Fecal occult blood screening in the Minnesota study: sensitivity of the screening test. J Natl Cancer Inst 89 (19): 1440-8, 1997. [PUBMED Abstract]
Mandel JS, Church TR, Bond JH, et al.: The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med 343 (22): 1603-7, 2000. [PUBMED Abstract]
Mandel JS, Bond JH, Church TR, et al.: Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med 328 (19): 1365-71, 1993. [PUBMED Abstract]
Bretthauer M, Løberg M, Wieszczy P, et al.: Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. N Engl J Med 387 (17): 1547-1556, 2022. [PUBMED Abstract]
Hewitson P, Glasziou P, Watson E, et al.: Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): an update. Am J Gastroenterol 103 (6): 1541-9, 2008. [PUBMED Abstract]
Significance
Background
Colorectal cancer (CRC) is the third most common malignant neoplasm worldwide [1] and the second leading cause of cancer deaths in the United States.[2] It is estimated that in 2025 there will be 154,270 new cases diagnosed in the United States and 52,900 deaths due to this disease. From 2012 to 2021, incidence rates for CRC declined by about 1% per year overall due to screening uptake and changing patterns in risk factors. However, this declining incidence is confined to individuals aged 65 years and older. Between 2012 and 2021, incidence rates increased by 2.4% per year in individuals younger than 55 years and by 0.4% per year in individuals aged 50 to 64 years. Over the last decade, the mortality rate from CRC declined by 1.7% per year in both men and women.[2] Incidence is higher in men than in women. The incidence rates range from 34.5 per 100,000 per year in Asian or Pacific Islander men to 53.6 per 100,000 per year in American Indian or Alaska Native men. In women, the incidence rates range from 25.3 per 100,000 per year in Asian or Pacific Islander women to 45.5 per 100,000 per year in American Indian or Alaska Native women. The age-adjusted mortality rates are 15.4 per 100,000 per year in men and 10.8 per 100,000 per year in women. About 4.0% of Americans are expected to develop the disease within their lifetime, and the lifetime risk of dying from CRC is 1.4%.[3] Age-specific incidence and mortality rates show that most cases are diagnosed after age 54 years and 77% of cases occur in individuals aged 55 years and older; about 15% of CRC cases occur in individuals aged 45 to 54 years.[3–5]
An analysis of national data for 1975 to 2010 addressed long-term trends in CRC.[6] Incidence increased for men from 1975 to 1985, but there were marked declines from 1985 to 1995 for both men and women, followed by a nonsignificant increase from 1995 to 1998, then marked declines from 1998 to 2010. Death rates from CRC have declined since 1984 in both men and women, with an accelerated rate of decline since 2002 for men and since 2001 for women. From 1997 to 2010, CRC incidence declined for all racial and ethnic groups. The fastest annual rate of decline occurred in men and women aged 65 years or older. There was a trend of increasing short-term incidence rates for individuals younger than 50 years in most population subgroups. Incidence rates of distal colon and rectal cancers decreased in men and women for all ages combined. Incidence rates of proximal colon cancer also decreased in men and women for all races and ethnicities combined.
Risk Factors
Age and family history
The main risk factor for CRC is increasing age; 90% of all CRCs are diagnosed after age 50 years. History of CRC in a first-degree relative, especially when diagnosed before age 55 years, approximately doubles the risk.
Adenomas
The presence of adenomas (lesions considered to be the histological [neoplastic but nonmalignant] precursors of CRC) is another major risk factor. Adenomas are extremely common. For example, in individuals older than 50 years, the prevalence of adenomas is approximately 30% but can be as high as 50% with the use of high-definition endoscopes, which can detect 1-mm to 2-mm adenomas.[7,8] Adenomas confer risk as they may themselves evolve into CRC. Additionally, even after removal, an adenoma (particularly if it is high risk based on size and histology) may indicate future risk of CRC. Managing adenomas and risk is challenging because adenomas are prevalent as people age, but most will never become CRC.
Understanding risk and risk management has been complicated by the intense focus on adenoma-detection rates in the last 15 years, which has led to increased detection of adenomas, especially very small ones (<0.5 cm). Risk factors for developing CRC are not completely understood, but generally include the following:
Personal history of CRC or high-risk adenomas.
Large adenomas (>1 cm).
Multiple adenomas (>3).
Adenomas with an advanced or worrisome histology (severe dysplasia; serrated, especially in the proximal colon).
Flat or difficult-to-detect lesions (including serrated polyps, which may be more common in the right colon than in the left colon.)
Increased future risk of CRC is indicated by a personal history of CRC or high-risk adenomas (i.e., large [>1 cm] tubular adenomas, sessile-serrated adenomas, or multiple adenomas). Follow-up of individuals with these adenomas after they have undergone screening is considered surveillance and not screening.[9]
The term serrated polyp includes hyperplastic polyps, sessile-serrated adenomas, traditional-serrated adenomas, and mixed-serrated polyps.[10,11] The clinical significance of these lesions is uncertain because the natural history of any polypoid lesion is difficult to learn. However, the histological and molecular characteristics of some serrated lesions suggest possibly important malignant potential (e.g., mutations in the BRAF gene may be an early step toward carcinogenesis in serrated polyps).[12]
Prevalence of adenomas and CRC in asymptomatic populations
In a colonoscopy study of 3,121 predominantly male U.S. veterans (mean age, 63 years), advanced neoplasia (defined as an adenoma ≥10 mm in diameter, a villous adenoma, an adenoma with high-grade dysplasia, or invasive cancer) was identified in 10.5% of the individuals.[8] Among patients with no adenomas distal to the splenic flexure, 2.7% had advanced proximal neoplasia. Patients with large adenomas (≥10 mm) or small adenomas (<10 mm) in the distal colon were more likely to have advanced proximal neoplasia (odds ratio [OR], 3.4; 90% confidence interval [CI], 1.8–6.5) than were patients with no distal adenomas (OR, 2.6; 90% CI, 1.7–4.1). One-half of those with advanced proximal neoplasia had no distal adenomas. In a study of 1,994 adults aged 50 years or older who underwent colonoscopy screening as part of a program sponsored by an employer, 5.6% of adults had advanced neoplasms.[7] Forty-six percent of those with advanced proximal neoplasms had no distal polyps (hyperplastic or adenomatous). If colonoscopy screening had been performed only in patients with distal polyps, about one-half of the cases of advanced proximal neoplasia would not have been detected.
Analysis of data from a colonoscopy-based screening program in Warsaw, Poland, demonstrated higher rates of advanced neoplasia in men than in women. Of the 43,042 participants aged 50 to 66 years, advanced neoplasia was detected in 5.9% of participants (5.7% in women with a family history of CRC, 4.3% in women without a family history of CRC, 12.2% in men with a family history of CRC, and 8.0% in men without a family history of CRC).
In a cohort study within the Polish Colonoscopy Screening Program, nearly 166,000 participants were followed for up to 17 years after a single negative colonoscopy. Standardized incidence ratios that compared the participants to the general population were 0.32 (95% CI, 0.29–0.35) for low-quality colonoscopy (LQC) and 0.16 (95% CI, 0.13–0.20) for high-quality colonoscopy (HQC). Standardized mortality ratios were 0.22 (95% CI, 0.18–0.25) for LQC and 0.10 (95% CI, 0.06–0.14) for HQC. Colonoscopy, especially HQC, was predictive of low CRC incidence and mortality for at least 10 years after a negative exam, suggesting that the currently recommended 10-year interval for screening is safe and could potentially be extended.[13]
References
Bray F, Laversanne M, Sung H, et al.: Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 74 (3): 229-263, 2024. [PUBMED Abstract]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Surveillance Research Program, National Cancer Institute: SEER*Explorer: An interactive website for SEER cancer statistics. Bethesda, MD: National Cancer Institute. Available online. Last accessed December 30, 2024.
National Cancer Institute: SEER Stat Fact Sheets: Colorectal Cancer. Bethesda, Md: National Institutes of Health. Available online. Last accessed April 10, 2024.
Imperiale TF, Wagner DR, Lin CY, et al.: Results of screening colonoscopy among persons 40 to 49 years of age. N Engl J Med 346 (23): 1781-5, 2002. [PUBMED Abstract]
Edwards BK, Noone AM, Mariotto AB, et al.: Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 120 (9): 1290-314, 2014. [PUBMED Abstract]
Imperiale TF, Wagner DR, Lin CY, et al.: Risk of advanced proximal neoplasms in asymptomatic adults according to the distal colorectal findings. N Engl J Med 343 (3): 169-74, 2000. [PUBMED Abstract]
Lieberman DA, Weiss DG, Bond JH, et al.: Use of colonoscopy to screen asymptomatic adults for colorectal cancer. Veterans Affairs Cooperative Study Group 380. N Engl J Med 343 (3): 162-8, 2000. [PUBMED Abstract]
Lieberman DA, Rex DK, Winawer SJ, et al.: Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 143 (3): 844-57, 2012. [PUBMED Abstract]
Kahi CJ, Hewett DG, Norton DL, et al.: Prevalence and variable detection of proximal colon serrated polyps during screening colonoscopy. Clin Gastroenterol Hepatol 9 (1): 42-6, 2011. [PUBMED Abstract]
Snover DC, Jass JR, Fenoglio-Preiser C, et al.: Serrated polyps of the large intestine: a morphologic and molecular review of an evolving concept. Am J Clin Pathol 124 (3): 380-91, 2005. [PUBMED Abstract]
Pilonis ND, Bugajski M, Wieszczy P, et al.: Long-Term Colorectal Cancer Incidence and Mortality After a Single Negative Screening Colonoscopy. Ann Intern Med 173 (2): 81-91, 2020. [PUBMED Abstract]
Evidence of Benefit
Fecal Occult Blood Test (FOBT)
In FOBT testing, stool samples are collected and analyzed for the presence of small amounts of blood. The first generation of FOBTs used guaiac-based assays to detect blood, which are less sensitive and less specific than immunochemical-based testing. The now-classic randomized controlled trials (RCTs) that assessed colorectal cancer (CRC) mortality reduction all used guaiac-based testing. The finding of decreased CRC mortality provided a major foundation to draft CRC screening recommendations. The first-generation guaiac-based tests are being replaced with more sensitive and more specific immunochemical tests, which have not yet been assessed in RCTs with a no-screening control group.
In this setting, the RCT evidence about guaiac-based testing is reviewed briefly here, with further discussion of how immunochemical FOBT (iFOBT or FIT) may provide improved sensitivity and specificity. Generally, if guaiac FOBT (gFOBT) is acceptable as a screening test (as shown in RCTs), then a strong case can be made for using a more sensitive and more specific test like FIT.
gFOBT collection details vary somewhat for different tests, but they typically involve collection of as many as three different specimens on 3 different days, with small amounts from one specimen smeared by a wooden stick on a card with two windows or otherwise placed in a specimen container.
The guaiac test identifies peroxidase-like activity that is characteristic of human and nonhuman hemoglobin. Thus, the test records blood from ingested meat, upper airway bleeding such as epistaxis, upper gastrointestinal (GI) bleeding, and colonic lesions.
A systematic review regarding evidence of benefit was conducted through the Cochrane Collaboration. It examined all CRC screening randomized trials that involved gFOBT testing done on more than one occasion. The combined results showed that trial participants allocated to screening had a 16% lower CRC mortality (relative risk [RR], 0.84; 95% confidence interval [CI], 0.78–0.90). There was no difference in all-cause mortality between the screened groups and the control groups (RR, 1.00; 95% CI, 0.99–1.02). The trials reported a low positive predictive value (PPV) for the FOBT test, suggesting that most positive tests were false positives. The PPV was 5.0% to 18.7% in the trials using nonrehydrated slides (Funen and Nottingham studies), and it was 0.9% to 6.1% in the trials using rehydrated slides (Goteborg and Minnesota studies). The report contained no discussion about contamination in the control arms of the trials and no information about treatment by disease stage.[1,2]
On initial (prevalence) examinations, 1% to 5% of unselected individuals tested with gFOBT had positive test results. Of those who tested positive, approximately 2% to 10% had cancer and approximately 20% to 30% had adenomas,[3,4] depending on how the test was done. Data from RCTs of gFOBT testing are summarized in Table 2.
Four controlled clinical trials to evaluate the efficacy of screening with gFOBT have been completed or are in progress. While more sensitive stool blood tests based on measuring human hemoglobin have been developed (and are discussed later in this summary), results of their performance in RCTs have not yet been reported. For gFOBT, the Swedish trial was a targeted study for individuals aged 60 to 64 years.[5] The English trial selected candidates from lists of family practitioners.[6] The Danish trial offered screening to a population aged 45 to 75 years who were randomly assigned to a control or study group.[7,8]
The Minnesota trial randomly assigned 46,551 men and women aged 50 to 80 years to one of three arms: (1) CRC screening with gFOBT, (2) rehydrated (with some small percentage of unrehydrated) FOBT every year (n = 15,570) or (3) every 2 years (n = 15,587), or a control group (n = 15,394). This trial demonstrated that annual FOBT screening decreased mortality from CRC by 33% after 18 years of follow-up (RR, 0.67; 95% CI, 0.51–0.83, compared with the control group) and that biennial testing resulted in a 21% relative mortality reduction (RR, 0.79; 95% CI, 0.62–0.97).[9] Some part of the reduction may have been attributed to chance detection of cancer by colonoscopies; rehydration of guaiac test slides greatly increased positivity and consequently increased the number of colonoscopies performed.[10] Subsequent analyses by the Minnesota investigators using mathematical modeling suggested that for 75% to 84% of the patients, mortality reduction was achieved because of sensitive detection of CRCs by the test; chance detection played a modest role (16%–25% of the reduction).[11] Nearly 85% of patients with a positive test underwent diagnostic procedures that included colonoscopy or double-contrast barium enema plus flexible sigmoidoscopy (FS). After 18 years of follow-up, the incidence of CRC was reduced by 20% in the annually screened arm and 17% in the biennially screened arm. With follow-up through 30 years, there was a sustained reduction in CRC mortality of 32% in the annually screened arm (RR, 0.68; 95% CI, 0.56–0.82) and 22% in the biennially screened arm (RR, 0.78; 95% CI, 0.65–0.93). There was no reduction in all-cause mortality in either screened arm (RR, 1.00; 95% CI, 0.99–1.01 for the annually screened arm and RR, 0.99; 95% CI, 0.98–1.01 for the biennially screened arm).[12] Important information that was not reported includes the treatment of CRC cases by stage by arm and the extent of CRC screening in each arm by FOBT, sigmoidoscopy, or colonoscopy after the completion of the trial protocol.[12,13]
The English trial allocated approximately 76,000 individuals to each arm. Those in the screened arm were offered nonrehydrated gFOBT testing every 2 years for three to six rounds from 1985 to 1995. At a median follow-up of 7.8 years, 60% completed at least one test, and 38% completed all tests. Cumulative incidence of CRC was similar in both arms, and the trial reported an RR reduction of 15% in CRC mortality (odds ratio [OR], 0.85; 95% CI, 0.74–0.98).[14] The serious complication rate of colonoscopy was 0.5%. There were five deaths within 30 days of surgery for screen-detected CRC or adenoma in a total of 75,253 individuals screened.[15] After a median follow-up of 11.8 years, no difference in CRC incidence between the intervention and control groups was observed. The disease-specific mortality rate ratio associated with screening was 0.87 (0.78–0.97; P = .01). The rate ratio for death from all causes was 1.00 (0.98–1.02; P = .79).[16] When the median follow-up was extended to 19.5 years, there was a 9% reduction in CRC mortality (RR, 0.91; 95% CI, 0.84–0.98) but no reduction in CRC incidence (RR, 0.97; 95% CI, 0.91–1.03), or death from all causes (RR, 1.00; 95% CI, 0.99–1.02).[17]
The Danish trial in Funen, Denmark, entered approximately 31,000 individuals into two arms, in which individuals in the screened arm were offered nonrehydrated gFOBT testing every 2 years for nine rounds over a 17-year period. Sixty-seven percent of participants completed the first screen, and more than 90% of individuals invited to each subsequent screen underwent FOBT testing. This trial demonstrated an 18% reduction in CRC mortality at 10 years of follow-up,[18] 15% at 13 years of follow-up (RR, 0.85; 95% CI, 0.73–1.00),[19] and 11% at 17 years of follow-up (RR, 0.89; 95% CI, 0.78–1.01).[20] CRC incidence and overall mortality were virtually identical in both arms.
The Swedish trial in Goteborg enrolled all 68,308 citizens in the city who were born between 1918 and 1931 and were aged 60 to 64 years, and randomly assigned them to screening and control groups of nearly equal size. Participants in the control group were not contacted and were unaware they were part of the trial. Screening was offered at different frequencies to three different cohorts according to year of birth. Screening was done using the gFOBT Hemoccult-II test after dietary restriction. Nearly 92% of tests were rehydrated. Individuals with a positive test result were invited to an examination consisting of a case history, FS, and double-contrast barium enema. Follow-up ranged from 6 years 7 months to 19 years 5 months, depending on the date of enrollment. The primary end point was CRC-specific mortality. The overall screening compliance rate was 70%, and 47.2% of participants completed all screenings. Of the 2,180 participants with a positive test, 1,890 (86.7%) underwent a complete diagnostic evaluation with 104 cancers and 305 adenomas of at least 10 mm detected. In total, there were 721 CRCs (152 Dukes D, 184 Dukes C) in the screening group and 754 CRCs (161 Dukes D, 221 Dukes C) in the control group, with an incidence ratio of 0.96 (95% CI, 0.86–1.06). Deaths from CRC were 252 in the screening group and 300 in the control group, with a mortality ratio of 0.84 (95% CI, 0.71–0.99). This CRC mortality difference emerged after 9 years of follow-up. Deaths from all causes were very similar in the two groups, with a mortality ratio of 1.02 (95% CI, 0.99–1.06).[5]
Stage distribution
All trials have shown a more favorable stage distribution in the screened population than in controls (see Table 2). Data from the Danish trial indicated that while the cumulative incidence of CRC was similar in the screened and control groups, a higher percentage of CRCs and adenomas were Dukes A and Dukes B lesions in the screened group.[18] A meta-analysis of all previously reported randomized trials using biennial FOBT showed no overall mortality reduction by gFOBT screening (RR, 1.002; 95% CI, 0.989–1.085). The RR of CRC death in the gFOBT arm was 0.87 (95% CI, 0.8–0.95), and the RR of non–CRC death in the gFOBT group was 1.02 (95% CI, 1.00–1.04; P = .015).[21]
Mathematical modeling
Mathematical models have been constructed to extrapolate the results of screening trials and screening programs for benefit of the general population in community health care delivery settings. These models project that using currently available screening methodology can reduce CRC mortality or increase life expectancy.[22]
Immunochemical FOBTs (iFOBT or FIT): Nonrandomized Controlled Trial Evidence to Assess Lesion Detection
The immunochemical FOBT (iFOBT or FIT) was developed to detect intact human hemoglobin. The advantage of FIT over gFOBT is that it does not detect hemoglobin from nonhuman dietary sources. Also, FIT does not detect partly digested human hemoglobin that comes from the upper respiratory or GI tract. Preliminary studies of several commercially developed FIT tests define their sensitivity and specificity compared with concurrently performed colonoscopy. The studies also examine these outcomes for different cutpoints, and the benefit of multiple versus single stool samples.[25,26]
Overall, FIT testing is much more sensitive than gFOBT, and it is more sensitive for cancers than for benign neoplasias. As expected, higher cutpoints decrease sensitivity and increase specificity. Fecal immunochemical tests may vary with regard to numbers of stools tested and cutoff values for a positive result.[26]
A systematic review of FIT studies in 2019 found 31 studies, with 120,255 participants and 18 types of FIT tests, that used screening colonoscopy as the reference standard, thus allowing calculation of test sensitivity and specificity.[27] Performance depended on the threshold for a positive result, so that a threshold of 10 µg/g (micrograms of hemoglobin per gram of feces) resulted in a CRC sensitivity of 0.91 (95% CI, 0.84–0.95) and a specificity of 0.90 (95% CI, 0.86–0.93), while a threshold greater than 20 µg/g resulted in a sensitivity of 0.71 (95% CI, 0.56–0.83) with specificity of 0.95 (95% CI, 0.94–0.96). For advanced adenomas, at a threshold of 10 µg/g, sensitivity was 0.40 (95% CI, 0.33–0.47) with a specificity of 0.90 (95% CI, 0.87–0.93). Comparison of three FITs at three thresholds was inconclusive because CIs overlapped, and the comparisons were across rather than within studies. Overall, FIT appears to provide a substantially improved sensitivity compared with gFOBT, although with some compromise in specificity.
The diagnostic sensitivity of FIT testing may vary depending on lesion location in the colon. Proximal lesions may be harder to detect for several reasons, including that they may arise from serrated lesions that are flat and, because they are less vascular than traditional adenomas, tend to bleed less frequently. In a population-based screening program of every-other-year FIT (set to detect 100 ng of hemoglobin per mL of buffer) testing, individuals who had six FITs over time were assessed to learn the frequency with which proximal and distal lesions were discovered.[28] Over 12 years (2002–2014), 123,000 participants had 441,000 FITs. The detection rate for proximal colon cancer declined only from the first to the second screening round (0.63–0.36 per 1,000 screened participants), while the rate for both distal colon and rectal cancer decreased across all six rounds (distal cancer, 1.65 in the first round to 0.17 in the sixth round). (Similar trends occurred for advanced adenomas.) The proportional interval cancer rate—the number of cancers observed versus expected—was higher in the proximal colon than in the distal colon (25.2% vs. 6.0%), suggesting that many proximal cancers (or their immediate precursors) may have been missed by FIT. These results suggest that FIT is less sensitive for proximal CRC and certainly for advanced adenomas, although it is possible that the miss rate may have been inflated if colonoscopy done in response to a positive FIT had missed a precursor lesion. Overall, these results raise questions about the degree of efficacy of FIT in preventing proximal CRC mortality.
The performance and acceptability of FIT over time was assessed by Kaiser-Permanente of Northern and Southern California in a screening program. A retrospective cohort of 323,349 persons aged 50 to 70 years was followed for up to four screening rounds over 4 years. Of patients invited, participation in round one was 48.2%, and of those remaining eligible, 75.3% to 86.1% participated in subsequent rounds. The authors reported that “programmatic FIT screening detected 80.4% of patients with CRC diagnosed within 1 year of testing, including 84.5% in round one and 73.4% to 78.0% in subsequent rounds.” An important observation was the degree of participation found. One limitation of the study is that it was not clear how work-up bias was addressed; e.g., when individuals with a positive test result are preferentially worked up to ascertain the presence or absence of CRC, while individuals with a negative test, but who might have CRC, are not. Although a look-back method was used to ascertain whether an individual had cancer, it is not clear that the duration of follow-up was long enough to discover everyone who should have been included in the denominator of the sensitivity calculation. Nevertheless, the results suggested that subsequent FIT results were at least partially independent of previous results. Longer follow-up may help clarify this issue. Mortality reduction could not be assessed in this study.[29]
Potential false-positive test results because of an increased risk of upper GI bleeding are of concern with FOBT testing and pretest protocols, therefore; low-dose aspirin regimens are discontinued for a week or more before FOBT. The performance of FIT was tested in an ongoing diagnostic study (2005–2009) at 20 internal medicine GI practices in southern Germany. Nineteen hundred seventy-nine patients (233 regular low-dose aspirin users and 1,746 never users) were identified in the records for inclusion in the analysis. All patients provided one stool sample taken within a week before colonoscopy preparation, which was collected according to instructions in a container that was kept refrigerated or frozen until rendered to the clinic on the day of colonoscopy, and the patients agreed to complete a standard questionnaire regarding the use of analgesics and low-dose aspirin (for prevention of cardiovascular disease). Stool samples were thawed within a median of 4 days after arrival at the central laboratory (shipped frozen from the recipient clinics). Fecal occult blood levels were measured by two automated FIT tests according to the manufacturer’s instructions (RIDASCREEN Haemoglobin and RIDASCREEN Haemo-/Haptoglobin Complex, r-biopharm, Bensheim, Germany) following clinical procedures and blinded to colonoscopy results. Advanced neoplasms were found in 24 aspirin users (10.3%) and in 181 nonusers (10.4%). At the cut point recommended by the manufacturer, sensitivities for the two tests were as follows: 70.8% (95% CI, 48.9%–87.4%) for users compared with 35.9% (95% CI, 28.9%–43.4%) for nonusers for the Haemoglobin test (P = .001) and 58.3% (95% CI, 36.6%–77.9%) for users compared with 32% (95% CI, 25.3%–39.4%) for nonusers for the Haemo-/Haptoglobin test (P = .01). Specificities were as follows: 85.7% (95% CI, 80.2%–90.1%) for users compared with 89.2% (95% CI, 87.6%–90.7%) for nonusers for the Haemoglobin test (P = .13) and 85.7% (95% CI, 80.2%–90.1%) for users compared with 91.1% (95% CI, 89.5%–92.4%) for nonusers for the Haemo-/Haptoglobin test (P = .01). For these FITs, sensitivity for advanced neoplasms was notably higher with the use of low-dose aspirin while specificity was only slightly reduced, suggesting that there might be an advantage of aspirin use to increase sensitivity without much decrease in specificity.[30]
Sigmoidoscopy
The flexible fiberoptic sigmoidoscope was introduced in 1969. The 60 cm flexible sigmoidoscope became available in 1976.[31] The flexible sigmoidoscope permits a more complete examination of the distal colon with more acceptable patient tolerance than the older rigid sigmoidoscope. The rigid instrument can discover 25% of polyps, while the 60-cm scope can find as many as 65% of them. The finding of an adenoma by FS may warrant a colonoscopy to evaluate the more proximal portion of the colon.[32,33] The prevalence of advanced proximal neoplasia is increased in patients with a villous or tubulovillous adenoma distally and is also increased in those aged 65 years or older with a positive family history of CRC and with multiple distal adenomas.[34] Most of these adenomas are polypoid, flat, and depressed lesions, which may be somewhat more prevalent than previously recognized.[35]
Four major sigmoidoscopy screening RCTs have reported incidence and mortality results (a fifth, the Telemark trial in Norway, was very small, with 800 total participants). These are the Norwegian Colorectal Cancer Prevention (NORCCAP) trial; the United Kingdom Flexible Sigmoidoscopy Screening Trial (UKFSST); the Screening for COlon REctum (SCORE) trial in Italy; and the U.S. Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial (see Table 3). Participants were aged 55 to 74 years in PLCO and aged 55 to 64 years in the other three trials. Together, the trials enrolled 166,000 participants in the screened groups and 250,000 participants in the control groups. Median follow-up was approximately 11 years for each group. Results were summarized in three systematic reviews. There was an 18% relative reduction in CRC incidence (RR, 0.82; 95% CI, 0.75–0.89), an overall 28% relative reduction in CRC mortality (RR, 0.72; 95% CI, 0.65–0.80), a 31% relative reduction in the incidence of distal CRC (RR, 0.69; 95% CI, 0.63–0.74), and a 46% relative reduction in the mortality of distal CRC (RR, 0.54; 95% CI, 0.43–0.67).[36] A meta-analysis showed a statistically significant, although clinically small, effect on all-cause mortality (RR, 0.97; 95% CI, 0.96–0.99).[37]
Three of the four trials above published long-term follow-up analyses of trial results. For UKFSST, median follow-up was 17.1 years. The RRs for CRC incidence and mortality were similar to those originally reported: an RR of 0.70 (95% CI, 0.62–0.79) for CRC mortality and an RR of 0.74 (95% CI, 0.70–0.80) for CRC incidence. For the PLCO trial, median follow-up was 15.8 years for incidence and 16.8 years for mortality; RRs were 0.75 (95% CI, 0.66–0.85) for CRC mortality and 0.82 (95% CI, 0.76–0.88) for CRC incidence. Median follow-up in the NORCCAP trial was approximately 15 years; HRs were 0.79 (95% CI, 0.65–0.96) for CRC mortality and 0.78 (95% CI, 0.70–0.87) for CRC incidence.[38,39] A pooled analysis of the four trials, using data through 15 years of follow-up and restricted to those aged 55 to 64 years at randomization, showed a rate ratio of 0.79 (95% CI, 0.75–0.83) for CRC incidence and 0.80 (95% CI, 0.72–0.88) for CRC mortality.[40]
There are no strong direct data from studies of sigmoidoscopy to determine the optimal frequency of screening tests in programs of screening.
Table 3. Randomized Controlled Screening Trials to Assess Outcome: Sigmoidoscopya
bThe FS rate refers to the % of individuals who received FSG in the screened group.
cThe colonoscopy rate refers to the % of individuals who received a colonoscopy as a follow-up to a positive sigmoidoscopy among those who received a sigmoidoscopy. In the U.S. study, individuals with a polyp found at the time of a sigmoidoscopy were referred for diagnostic follow-up, which was generally done with a colonoscopy. In the other studies, the referral criteria for a colonoscopy depended on the histology of lesion(s) found at the time of the sigmoidoscopy.
d Half of the intervention group was also offered FOBT.
eThese data are from Lin et al.[26], eFigure 1. Forest plot of randomized controlled trials of FS screening on distal CRC mortality.
United Kingdom 2010
Intervention: 57,099
71.1
5.0
1.5
Intervention: 30
0.69 (0.59–0.80)
0.58 (0.46–0.74)
0.77 (0.70–0.84)
Control: 112,939
Control: 44
Italy 2011
Intervention: 17,136
57.8
7.8
1.6
Intervention: 35
0.78 (0.56–1.08)
0.73 (0.47–1.12)
0.82 (0.69–0.96)
Control: 17,136
Control: 44
United States 2012
Intervention: 77,445
86.6
25.3
1.5
Intervention: 29
0.74 (0.63–0.87)
0.50 (0.38–0.64)
0.79 (0.72–0.85)
Control: 77,455
Control: 39
Norway 2014
Intervention: 20,572d
63.0
19.5
1.4
Intervention: 31
0.73 (0.56–0.94)
0.87 (0.61–0.043)
0.80 (0.70–0.92)
Control: 78,220
Control: 43
Combination of FOBT and Flexible Sigmoidoscopy: Impact on Neoplasm Detection
A combination of FOBT and sigmoidoscopy might increase the detection of lesions in the left colon (compared with sigmoidoscopy alone) while also increasing the detection of lesions in the right colon. Sigmoidoscopy detects lesions in the left colon directly but detects lesions in the right colon only indirectly when a positive sigmoidoscopy (that may variously be defined as a finding of advanced adenoma, any adenoma, or any polyp) is used to trigger a colonoscopic examination of the whole colon.
In 2,885 veterans (97% male; mean age, 63 years), the prevalence of advanced adenoma at colonoscopy was 10.6%. It was estimated that combined screening with one-time FOBT and sigmoidoscopy would detect 75.8% (95% CI, 71.0%–80.6%) of advanced neoplasms. Examination of the rectum and sigmoid colon during colonoscopy was defined as a surrogate for sigmoidoscopy. This represented a small but statistically insignificant increase in the rate of detection of advanced neoplasia when compared with FS alone (70.3%; 95% CI, 65.2%–75.4%). The latter result could be achieved assuming that all patients with an adenoma in the distal colon undergo complete colonoscopy. Advanced neoplasia was defined as a lesion measuring at least 10 mm in diameter, containing 25% or more villous histology, high-grade dysplasia, or invasive cancer.[41] One-time use of FOBT differs from the annual or biennial application reported in those studies summarized in Table 2.
A study of 21,794 asymptomatic individuals (72% were men) who had both colonoscopy and FIT for occult blood compared the detection of proximal cancers as triggered by different test results. FIT alone resulted in a sensitivity of 58.3% and a specificity of 94.5% for proximal cancer diagnosis. FIT plus the finding of advanced neoplasia in the rectosigmoid colon yielded a sensitivity of 62.5% and a specificity of 93%. In this study, the addition of sigmoidoscopy to FIT did not substantially improve the detection of proximal colon cancers, compared with FIT alone.[42]
Colonoscopy
Randomized controlled trial evidence about colorectal cancer incidence or mortality reduction
The NordICC trial (NCT00883792) was a pragmatic randomized trial of colonoscopy screening, begun in 2009 in Poland, Norway, Sweden, and the Netherlands. Men and women aged 55 to 64 years were identified from population registries and randomly assigned in a 1:2 ratio to receive either an invitation to undergo a single colonoscopy screening (invited group) or no invitation to screening (usual care group). Individuals were randomly assigned before they were asked whether they wanted to participate in the trial. Except for the 6,900 participants from Norway, participants in the usual-care group were not informed of their enrollment in the trial. The primary end points were risk of developing CRC and CRC-related death. The secondary end point was death from any cause.
Data were reported for 84,585 participants in Poland, Norway, and Sweden: 28,220 in the invited group, of whom 42% underwent screening, and 56,365 in the usual-care group. Opportunistic colonoscopy screening activity was monitored in the trial regions, and no additional colonoscopy procedures were identified beyond what would have been expected for clinical indications, indicating minimal, if any, contamination in the usual-care group. Hence, this trial compared colonoscopy screening with no screening. After a median follow-up of 10 years, in intention-to-screen analyses, the risk of developing CRC was 0.98% in the invited group and 1.20% in the usual-care group (risk ratio, 0.82; 95% CI, 0.70–0.93). The risk of death from CRC was 0.28% in the invited group and 0.31% in the usual-care group (risk ratio, 0.90; 95% CI, 0.64–1.16). The risk of death from any cause was 11.03% in the invited group and 11.04% in the usual-care group (risk ratio, 0.99; 95% CI, 0.96–1.04). Since only 42% of invited participants underwent screening, adjusted analyses were performed to estimate the effect of screening if all participants randomly assigned to screening actually had been screened. The risk ratio for CRC was 0.69 (95% CI, 0.55–0.83), and the risk ratio for CRC-related death was 0.50 (95% CI, 0.27–0.77). Fifteen participants had major bleeding after polyp removal, and there were no perforations or screening-related deaths within 30 days after colonoscopy.[43]
Caveats for this trial include the following:
Data from the Netherlands, roughly 10% of the participants, were not included.
Only 42% of invited participants underwent screening.
Follow-up duration may not be long enough to realize the full effect of the screening; additional analyses after 15 years are anticipated.
Colonoscopy is operator dependent, and 29% of the trial endoscopists had an adenoma detection rate (ADR) below the recommended minimum threshold.
There is a suggestion that high-risk individuals in Poland chose to undergo colonoscopy, which could have led to an underestimation of the screening effect.[44]
Indirect evidence of benefit comes from the detection rate of lesions that may be clinically important (like early CRC or advanced adenomas). Some case-control results are available. The sensitivity of a CRC screening test for adenomas (and for CRC) may be helpful in considering its possible clinical usefulness, given that there are no completed RCTs of the impact of colonoscopy on CRC mortality or incidence. Colonoscopy is commonly considered the gold standard because it directly assesses the physical presence of lesions in the colon. However, colonoscopy can miss roughly 10% of cancers and advanced adenomas because of suboptimal bowel cleansing, lesions being hidden behind folds (or haustra) in the colon, or suboptimal examination by the endoscopist. Recent data suggest that the magnitude of an endoscopist’s adenoma-detection rate (commonly measured as the proportion of colonoscopies in which an adenoma is found) is related to reduced incidence of CRC.
Adenoma detection rate (ADR)
Detection rates in colonoscopy screening vary with the rate at which the endoscopist examines the colon while withdrawing the scope. In one study, there were differences among gastroenterologists in the rates of detection of adenomas (range of the mean number of lesions per patient screened, 0.10–1.05; range of the percentage of patients with adenomas, 9.4%–23.7%) and the times of withdrawal of the scope (3.1–16.8 minutes for procedures not including polyp removal). Examiners whose mean withdrawal time was 6 minutes or more had higher detection rates than those with mean withdrawal times of less than 6 minutes (28.3% vs. 11.8%; P < .001 for any neoplasia and 6.4% vs. 2.6%; P < .005 for advanced neoplasia).[45]
In the first 10 years of the German CRC screening program, detection of nonadvanced adenomas increased in men from 13.3% to 22.3% and in women from 8.4% to 14.9%. Most of the nonadvanced adenomas, however, were small (<0.5 cm) and had uncertain clinical significance. The detection of advanced adenomas and CRC increased by a much smaller amount.[46]
Overall detection rates of adenomas and cancer may be affected by how thoroughly endoscopists search for flat adenomas and flat cancer. While the phenomenon of flat neoplasms has been appreciated for years in Japan, it has more recently been described in the United States. In a study in which endoscopists used high-resolution white-light endoscopes, flat or nonpolypoid lesions accounted for only 11% of all superficial colon lesions, but these flat or nonpolypoid lesions were about 9.8 times as likely as polypoid lesions to contain cancer (in situ neoplasia or invasive cancer).[35] However, because the definition of flat or nonpolypoid was height less than one-half of the diameter, it is likely that many lesions classified as nonpolypoid in this study would be routinely found and described by U.S. endoscopists as sessile. The existence of very flat or depressed lesions—depressed lesions are very uncommon but highly likely to contain cancer—requires that endoscopists pay more attention to this problem.[47] Flat lesions may play a role in the phenomenon of missed cancers.[48]
A health maintenance organization assessed the impact of ADRs in follow-up after 314,872 colonoscopies performed from 1998 to 2010 by 136 gastroenterologists, each of whom had done at least 300 colonoscopies during that period. The goal was to determine rates of interval CRC, interval advanced CRC, and CRC death and to relate those rates to a gastroenterologist’s ADR. There were 712 interval cancers (155 advanced) and 147 CRC deaths. The risk of interval cancer from lowest-to-highest quintile of ADR was 9.8, 8.6, 8.0, 7.0, and 4.8 per 10,000 person-years of follow-up. The adjusted hazard ratio (HR) for physicians in the highest quintile compared with those in the lowest quintile was 0.52 for any interval CRC, 0.43 for advanced CRC, and 0.38 for fatal CRC. Each 1.0% increase in ADR was associated with a 3% decrease in risk of cancer, although the CI for each quintile was broad. Limitations of the study include the inability to determine which specific feature of ADR led to reduced interval cancer. For example, it is unclear whether it was due to the following:
Removal of small adenomas that may grow rapidly to become CRC.
ADR being a surrogate outcome for an endoscopist’s ability to remove adenomas more completely.
ADR being a surrogate outcome for an endoscopist’s ability to better detect large, flat, serrated lesions.
Higher ADR leading to recommendations for more frequent postpolypectomy surveillance colonoscopy.
Another limitation is that the harms of a colonoscopy associated with ADR could not be measured.[49]
Nonrandomized controlled trial evidence about colorectal cancer incidence or mortality reduction
Although there is little RCT evidence to assess reduction of CRC incidence or mortality by colonoscopy, some case-control evidence is available.[50] Based on case-control data about sigmoidoscopy, noted above, there was speculation that protection for the right colon might be similar to that for the left colon. A 2009 case-control study of colonoscopy raised questions about whether the impact of colonoscopy on proximal lesions might be different than the impact on distal lesions.[51] Using a province-wide administrative database in Ontario, Canada, investigators compared cases of individuals who were diagnosed with CRC from 1996 to 2001 and had died by 2003. Controls were selected from persons who did not die of CRC. Billing claims were used to assess exposure to previous colonoscopy. The OR for the association between complete colonoscopy and distal lesions was 0.33, suggesting a substantial mortality reduction. For proximal lesions, however, the OR of 0.99 indicated virtually no mortality reduction. However, this study had limited data about whether examinations were complete to the cecum and about bowel prep. Further, many endoscopists were not gastroenterologists.
A case-control study assessed CRC reduction (but not CRC mortality reduction) in the right side versus the left side of the colon. In a population-based study from Germany using data from administrative and medical records, 1,688 patients with CRC were compared with 1,932 participants without CRC, aged 50 years or older.[52] Data were collected about demographics, risk factors, and previous screening examinations. According to colonoscopy records, the cecum was reached 91% of the time. Colonoscopy in the previous 10 years was associated with an OR for any CRC of 0.23, for proximal CRC of 0.44, and for distal CRC of 0.16. While this study did not assess CRC mortality, the results suggested that the magnitude of the right-side versus the left-side difference may be smaller than previously found.[51] It would be extremely useful to assess right-side versus left-side differences in a RCT.
Other case-control data suggest a reduction of CRC incidence on the right side of about 64% compared with about 74% on the left side.[53]
Because there is little RCT evidence and case-control evidence is limited, it is important to consider the degree of mortality reduction from colonoscopy. While a figure of 90% is sometimes cited as the degree of mortality reduction,[54] the question will not be properly answered until the completion of European RCT that has a control group of routine care that involves minimal screening of any kind.[55] Reliable results from colonoscopy RCTs are needed to confirm the studies of FS that suggest a mortality reduction of approximately 50% might occur in the right colon, similar to the demonstrated impact of FS in the left colon. This generalization is limited by a number of factors, including that proximal lesions may have a different pathology (e.g., a serrated appearance and different molecular pathway).
The benefit of continued CRC screening after age 75 years is uncertain. An observational cohort study with the Harvard Nurses’ Health Study (NHS) and Health Professionals Follow-Up Study (HPFS) sought to determine whether CRC mortality or morbidity was affected by lower endoscopy (colonoscopy or sigmoidoscopy) screening in individuals older than 75 years, based on a person’s age, comorbidity, family history of CRC, and screening history. Individuals were followed from 1988 to 2016 and had follow-up questionnaires every 2 years, with a 90% response rate. Among over 50,000 individuals, there were 661 CRCs and 323 CRC-related deaths. Screening after age 75 years was associated with reduced CRC incidence (HR, 0.61; 95% CI, 0.51–0.74) and CRC-related mortality (HR, 0.60; 95% CI, 0.46–0.78), regardless of screening history. It is not clear exactly what past screening history meant, however—i.e., the number and results of exams before age 75 years (no polyps; or some polyps indicating increased future risk). The study also assessed the relation of comorbidity to benefit and found that individuals with serious comorbidity—defined as myocardial infarction, stroke, or three comorbidities (high blood pressure, diabetes, and hypercholesterolemia)—did not benefit from screening. Although observational and not an RCT, this study likely provides the best-available data for a scenario in which a formal RCT is unlikely to be performed. It suggests that healthy people older than 75 years may benefit from continued CRC screening and reduction in mortality and morbidity.[56]
Virtual colonoscopy (also known as CTC or CT pneumocolon) refers to the examination of computer-generated images of the colon constructed from data obtained from an abdominal CT scan. These images simulate the effect of a conventional colonoscopy. Patients must take laxatives to clean the colon before the procedure, and the colon is insufflated with air (sometimes carbon dioxide) by insertion of a rectal tube just before radiographic examination.[57]
The American College of Radiology Imaging Network group conducted a large, paired-design study, with 2,531 participants at average risk (prevalence of polyps or cancer ≥10 mm, 4%; mean age, about 58 years) screened with both CTC and optical colonoscopy (OC). The gold standard was the OC, including repeat OC exams for people with lesions found by CTC but not by OC. Of 109 people with at least one adenoma or cancer 10 mm or larger, 98 (90%) were detected by CTC (referring everyone with a CTC lesion of ≥5 mm). Specificity was 86%, and PPV was 23%. This study raises several concerns, including the following:
Most, but not all, lesions found by CTC and not by OC were followed up with repeat OC.
The design did not allow for following patients, thus potentially missing lesions that grow rapidly and would only be seen after follow-up.
Because the centers conducting the screening were primarily academic centers and the radiologists and endoscopists were carefully trained, the generalizability of the findings is not clear.
Sixteen percent of participants had an extracolonic finding that required further evaluation.
Unknowns from the study include the following for either OC or CTC:[58]
The number of detected polyps that would have progressed to invasive cancer.
The number of people harmed by the screening process.
Another study reported similar sensitivity and specificity in individuals with an increased risk of CRC.[59] In this study, the sensitivity of OC could not be determined because it was done in an unblinded manner. This cross-sectional study suggested that virtual colonoscopy might be an acceptable screening or surveillance test for individuals at high risk of CRC, but it did not address outcome or frequency of testing in those at high risk.
Some studies have assessed how well virtual colonoscopy can detect colorectal polyps without a laxative prep. The question is of great importance for implementation because the laxative prep required by both conventional colonoscopy and virtual colonoscopy is considered a great disadvantage by patients. By tagging feces with iodinated contrast material ingested for several days before the procedure, investigators in one study were able to detect lesions larger than 8 mm with 95% sensitivity and 92% specificity.[60] The particular tagging material used in this study caused about 10% of patients to become nauseated; however, other materials are being assessed.
Another study [61] used a low-fiber diet, orally ingested contrast, and “electronic cleansing,” a process that subtracts tagged feces. CTC identified 91% of adenomas 10 mm or larger, but it detected fewer (70%) lesions of at least 8 mm. Patients who received both CTC and OC preferred CTC to OC (290 vs. 175). This study shows that CTC without a laxative prep detects small 1-cm lesions with high sensitivity and is acceptable to patients. Long-term utilization of CTC will depend on several issues, including the frequency of follow-up exams that would be needed to detect smaller lesions that were undetected and may grow over time.
Extracolonic abnormalities are commonly detected with CTC. Fifteen percent of patients in an Australian series of 100 patients, referred for colonography because of symptoms or family history, were found to have extracolonic findings, and 11% of the patients needed further medical workups for renal, splenic, uterine, liver, and gallbladder abnormalities.[62] In another study, 59% of 111 symptomatic patients referred for clinical colonoscopy in a Swedish hospital between June 1998 and September 1999 were found to have moderate or major extracolonic conditions on CTC. CTC was performed immediately before a colonoscopy, and these findings required further evaluation. The extent to which follow-up of these incidental findings benefited patients is unknown.[63]
Sixty-nine percent of 681 asymptomatic patients in Minnesota had extracolonic findings, 10% of which were deemed highly important by the investigators; these patients required further medical workup. Suspected abnormalities involved kidney (34), chest (22), liver (8), ovary (6), renal or splenic arteries (4), retroperitoneum (3), and pancreas (1);[64] however, the extent to which these findings contribute to benefits or harms is uncertain. Two other studies, one large (N = 2,195) and one small (n = 136) examined the moderate or high importance of extracolonic findings from CTC. The larger study [65] found that 8.6% of patients had an extracolonic finding of at least moderate importance, while 24% of patients in the smaller study [66] required some evaluation for an extracolonic finding. The larger study found nine cancers from these evaluations, at a partial cost (they did not include all costs) of $98.56 per patient initially screened. The smaller study found no important lesions from evaluation, at a cost of $248 per person screened. Both of these estimates of cost are higher than previous studies have found. The extent to which any patients benefited from the detection of extracolonic findings is not clear. Because both studies were conducted in academic medical centers, the generalizability to other settings is also not clear. Neither of these studies examined the effect of extracolonic findings on patient anxiety and psychological function.
Technical improvements involving both the interpretation methodology, such as three-dimensional (3-D) imaging, and bowel preparation are under study in many centers. While specificity for detection of polyps is homogeneously high in many studies, sensitivity can vary widely. These variations are attributable to a number of factors including characteristics of the CT scanner and detector, width of collimation, mode of imaging (two dimensional [2-D] vs. 3-D and/or fly-through), and variability in the expertise of radiologists.[67]
Digital Rectal Examination
A case-control study reported that routine digital rectal examination was not associated with any statistically significant reduction in mortality from distal rectal cancer.[68]
Detection of DNA Mutations in the Stool
The molecular genetic changes that are associated with the development of colorectal adenomas and carcinoma have been well characterized.[69] Advanced techniques have been developed to detect several of these gene mutations that shed into the stool.[70–73] Stool DNA testing was recently assessed in a prospective study of asymptomatic individuals who received colonoscopy, three-card FOBT (Hemoccult II), and stool DNA testing based on a panel of markers assessing 21 mutations. Conducted in a blinded way with prestated hypotheses and analyses, the study found that among 4,404 patients, the DNA panel had a sensitivity for CRC of 51.6% (for all stages of CRC) versus 12.9% for Hemoccult II, while the false-positive rates were 5.6% and 4.8%, respectively.[74,75]
A next-generation multitargeted stool test combined methylation markers for NDRG4 and BMP3, several KRAS mutations, and a human hemoglobin immunoassay. The markers, each quantitated separately, were combined using an algorithm in a prespecified multivariable analysis. In the DeeP-C trial, the assay’s sensitivity and specificity were compared with a commercial FIT test (OC FIT-CHEK Polymedco), using colonoscopy as the gold standard. Among 12,776 participants aged 50 to 84 years (weighted toward >65 years) who underwent colonoscopy screening and were enrolled at 90 sites across the United States and Canada between 2011 and 2012, 9,989 had fully evaluable results. There were 65 CRC and 757 advanced adenomas or sessile serrated polyps 1 cm or greater. The sensitivity for CRC was 92.3% (60 of 65 CRC) for the multitargeted test and 73.8% for FIT. Sensitivity for advanced lesions was 42.4% for the multitargeted test and 23.8% for FIT. Sensitivity for high-grade dysplasia was 69.2% for the multitarget test and 46.2% for FIT. Sensitivity for serrated sessile polyps 1 cm or greater was 42.4% for the multitargeted test and 5.1% for FIT. Specificities were 86.6% for the multitargeted test and 94.9% for FIT, using nonadvanced or negative colonoscopy results, and were 89.8% and 96.4% for totally negative colonoscopy results. A receiver operating characteristic (ROC) analysis showed that the multitargeted test has higher sensitivity than FIT alone, even when the FIT cutoff is reduced to try to increase sensitivity. A limitation is that there were no data about performance of repeated testing over time and what may be an appropriate testing interval.[76]
A newer version of the multitargeted stool DNA (mt-sDNA) test was recently developed. This test incorporates a novel molecular marker panel that includes methylated DNA markers of four genes—LASS4, LRRC4, PPP2R5C, and ZDHHC1—while retaining the fecal hemoglobin marker. In the BLUE-C trial, which was structured similarly to the DeeP-C trial, the investigators compared the sensitivity and specificity of the newer version of the mt-sDNA test with FIT (OC FIT-CHEK Polymedco), using colonoscopy as the gold standard for detecting stage I, II, and III CRC and advanced precancerous lesions in average-risk individuals older than 40 years.[77]
Between November 2019 and January 2023, 20,176 participants were enrolled at 186 sites and underwent both colonoscopy and stool tests. The mean age was 63 years; 53% of participants were female, 60% were White individuals, 5.2% had a family history of CRC in a first-degree relative, and 13.4% had a positive next-generation mt-sDNA test. Among those enrolled, 0.5% (98/20,176) had CRC, and 10.6% (2,144/20,176) had advanced precancerous lesions. Among individuals with CRC, 84% (82/98) had stage I, II, or III CRC.
The sensitivity for CRC was 93.9% (92/98) for the mt-sDNA test and 67.3% for FIT. According to the study, sensitivity did not vary substantially based on disease stage or location in the colon. The sensitivity for advanced precancerous lesions (large adenomas, large sessile serrated polyps, villous adenomas, or adenomas with high-grade dysplasia or carcinoma in situ) was 43.4% (931/2,144) for the mt-sDNA test and 23.3% for FIT. However, sensitivity rose to 74.6% (85/114) for the mt-sDNA test and to 47.4% for FIT when limited to lesions with high-grade dysplasia. Approximately 7% of participants had a false-positive test, defined as a positive stool DNA test but no adenomas, advanced precancerous lesions, or CRC were found by colonoscopy. Specificities were 92.7% for the mt-sDNA test and 95.7% for FIT, using nonadvanced or negative colonoscopy results, and 93.4% for the mt-sDNA test and 96.0% for FIT using negative colonoscopy results. The area under the ROC curve analysis also showed that the sensitivity for CRC and advanced neoplasia was greater for the mt-sDNA test compared with FIT alone.
The study was limited by the high proportion of enrolled participants (20,176) whose samples could not be evaluated according to the protocol. This was due in part to the conduct of the study during the coronavirus disease pandemic.
Overall, the multitargeted test was more sensitive than FIT for both CRC and advanced precancerous lesions, but the test was less specific.[76,77]
Cell-Free DNA (cfDNA) Blood Test
A cfDNA blood test was developed for the detection of CRC. This test analyzes plasma cfDNA to identify aberrant DNA-methylation status, abnormal DNA-fragmentation patterns, and the presence or absence of somatic pathogenic variants in the APC and KRAS genes. In the ECLIPSE trial, researchers conducted a prospective multicenter study at 265 primary care sites and endoscopy centers across the United States.[78] The trial aimed to evaluate the performance of the cfDNA blood-based test in detecting asymptomatic and early-stage CRC in a screening-relevant population.
Between October 2019 and September 2022, 22,877 participants were enrolled in the study. Among those enrolled, 0.3% (65/22,877) had CRC, and 4.8% (1,116/22,877) had advanced precancerous lesions. The clinical validation cohort included 10,258 participants, 7,861 of whom met all inclusion and exclusion criteria, had complete colonoscopies, and had evaluable cfDNA blood-based tests. This final study cohort had a mean age of 60 years (range, 45–84 years); 54% were female, and 79% were White individuals. In this cohort, 11.4% had a positive cfDNA blood-based test.
The sensitivity of the cfDNA blood-based test for CRC was 83.1% (54/65) for the participants with CRC detected by colonoscopy. This means that a total of 83.1% of these participants had a positive cfDNA test and 16.9% had a negative test. Sensitivity for stage I, II, or III CRC was 87.5% (42/48), and sensitivity for advanced precancerous lesions was 13.2% (147/1,116). The specificity was 89.6% using nonadvanced adenomas, non-neoplastic findings, and negative colonoscopy results.
Overall, the study team demonstrated the feasibility of using plasma cfDNA to screen for CRC. However, the relatively low sensitivity for detecting advanced precancerous lesions presents a limitation. Currently, the cfDNA blood-based test is still awaiting approval by the U.S. Food and Drug Administration and is not covered by Medicare.[78]
Adherence to Screening
Benefit from CRC screening can only occur if eligible people are screened. There have been problems with screening adherence, particularly for low-income and uninsured people. There are also concerns that some people may be less likely to adhere to screening with a colonoscopy than with fecal tests. One well-conducted RCT found that, among an uninsured population, mailed FIT-kit outreach and follow-up reminder phone calls resulted in an adherence rate of 40.7%. Mailed colonoscopy invitations and follow-up phone reminders resulted in a 24.6% adherence rate. The usual-care adherence rate in this trial was 12.1%.[79]
Tailoring Screening to Risk
Benefit of screening might be improved by tailoring the recommended screening test to a person’s degree of CRC risk. For example, if a subgroup of young women were to have a substantially lower risk of proximal neoplasms, then recommending sigmoidoscopy instead of colonoscopy might lead to higher compliance (the U.S. Preventive Services Task Force recommends both procedures without preference, as part of a program of screening those at average risk).
In a study to identify an average-risk group who had a higher versus lower risk of advanced neoplasia (CRC and advanced adenomas) anywhere in the colon, 2,993 individuals having a screening colonoscopy were stratified by age, sex, waist circumference, smoking, and family history (those in high-risk family categories, e.g., Lynch syndrome or adenomatous polyposis coli, were excluded). In a classification system derived in a training set, the risks of advanced neoplasm in four groups were: 1.92%, 4.88%, 9.93%, and 24%. In the two lowest-risk groups, sigmoidoscopy would have detected 51 (73%) of 70 advanced neoplasms. In the independent validation set, results were similar. Whether this system increases overall compliance has yet to be determined.[80]
A similar stratification system based on age, sex, smoking, and family history—and combined with FIT—was tested in Asia to determine whether use of the stratification system plus FIT could detect which people needed colonoscopy. If either the stratification system or FIT was positive, a person was recommended for colonoscopy. Using this strategy, 95% of those with CRC were correctly told to have colonoscopy.[81]
References
Hewitson P, Glasziou P, Irwig L, et al.: Screening for colorectal cancer using the faecal occult blood test, Hemoccult. Cochrane Database Syst Rev (1): CD001216, 2007. [PUBMED Abstract]
Hewitson P, Glasziou P, Watson E, et al.: Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): an update. Am J Gastroenterol 103 (6): 1541-9, 2008. [PUBMED Abstract]
Eddy DM: Screening for colorectal cancer. Ann Intern Med 113 (5): 373-84, 1990. [PUBMED Abstract]
Allison JE, Feldman R, Tekawa IS: Hemoccult screening in detecting colorectal neoplasm: sensitivity, specificity, and predictive value. Long-term follow-up in a large group practice setting. Ann Intern Med 112 (5): 328-33, 1990. [PUBMED Abstract]
Lindholm E, Brevinge H, Haglind E: Survival benefit in a randomized clinical trial of faecal occult blood screening for colorectal cancer. Br J Surg 95 (8): 1029-36, 2008. [PUBMED Abstract]
Hardcastle JD, Thomas WM, Chamberlain J, et al.: Randomised, controlled trial of faecal occult blood screening for colorectal cancer. Results for first 107,349 subjects. Lancet 1 (8648): 1160-4, 1989. [PUBMED Abstract]
Kronborg O, Fenger C, Søndergaard O, et al.: Initial mass screening for colorectal cancer with fecal occult blood test. A prospective randomized study at Funen in Denmark. Scand J Gastroenterol 22 (6): 677-86, 1987. [PUBMED Abstract]
Kronborg O, Fenger C, Olsen J, et al.: Repeated screening for colorectal cancer with fecal occult blood test. A prospective randomized study at Funen, Denmark. Scand J Gastroenterol 24 (5): 599-606, 1989. [PUBMED Abstract]
Mandel JS, Church TR, Ederer F, et al.: Colorectal cancer mortality: effectiveness of biennial screening for fecal occult blood. J Natl Cancer Inst 91 (5): 434-7, 1999. [PUBMED Abstract]
Lang CA, Ransohoff DF: Fecal occult blood screening for colorectal cancer. Is mortality reduced by chance selection for screening colonoscopy? JAMA 271 (13): 1011-3, 1994. [PUBMED Abstract]
Ederer F, Church TR, Mandel JS: Fecal occult blood screening in the Minnesota study: role of chance detection of lesions. J Natl Cancer Inst 89 (19): 1423-8, 1997. [PUBMED Abstract]
Shaukat A, Mongin SJ, Geisser MS, et al.: Long-term mortality after screening for colorectal cancer. N Engl J Med 369 (12): 1106-14, 2013. [PUBMED Abstract]
Mandel JS, Church TR, Bond JH, et al.: The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med 343 (22): 1603-7, 2000. [PUBMED Abstract]
Hardcastle JD, Chamberlain JO, Robinson MH, et al.: Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 348 (9040): 1472-7, 1996. [PUBMED Abstract]
Robinson MH, Hardcastle JD, Moss SM, et al.: The risks of screening: data from the Nottingham randomised controlled trial of faecal occult blood screening for colorectal cancer. Gut 45 (4): 588-92, 1999. [PUBMED Abstract]
Scholefield JH, Moss S, Sufi F, et al.: Effect of faecal occult blood screening on mortality from colorectal cancer: results from a randomised controlled trial. Gut 50 (6): 840-4, 2002. [PUBMED Abstract]
Scholefield JH, Moss SM, Mangham CM, et al.: Nottingham trial of faecal occult blood testing for colorectal cancer: a 20-year follow-up. Gut 61 (7): 1036-40, 2012. [PUBMED Abstract]
Kronborg O, Fenger C, Olsen J, et al.: Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet 348 (9040): 1467-71, 1996. [PUBMED Abstract]
Jørgensen OD, Kronborg O, Fenger C: A randomised study of screening for colorectal cancer using faecal occult blood testing: results after 13 years and seven biennial screening rounds. Gut 50 (1): 29-32, 2002. [PUBMED Abstract]
Kronborg O, Jørgensen OD, Fenger C, et al.: Randomized study of biennial screening with a faecal occult blood test: results after nine screening rounds. Scand J Gastroenterol 39 (9): 846-51, 2004. [PUBMED Abstract]
Moayyedi P, Achkar E: Does fecal occult blood testing really reduce mortality? A reanalysis of systematic review data. Am J Gastroenterol 101 (2): 380-4, 2006. [PUBMED Abstract]
Knudsen AB, Zauber AG, Rutter CM, et al.: Estimation of Benefits, Burden, and Harms of Colorectal Cancer Screening Strategies: Modeling Study for the US Preventive Services Task Force. JAMA 315 (23): 2595-609, 2016. [PUBMED Abstract]
Mandel JS, Bond JH, Church TR, et al.: Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med 328 (19): 1365-71, 1993. [PUBMED Abstract]
Kewenter J, Björk S, Haglind E, et al.: Screening and rescreening for colorectal cancer. A controlled trial of fecal occult blood testing in 27,700 subjects. Cancer 62 (3): 645-51, 1988. [PUBMED Abstract]
Grazzini G, Visioli CB, Zorzi M, et al.: Immunochemical faecal occult blood test: number of samples and positivity cutoff. What is the best strategy for colorectal cancer screening? Br J Cancer 100 (2): 259-65, 2009. [PUBMED Abstract]
Lin JS, Piper MA, Perdue LA, et al.: Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 315 (23): 2576-94, 2016. [PUBMED Abstract]
Imperiale TF, Gruber RN, Stump TE, et al.: Performance Characteristics of Fecal Immunochemical Tests for Colorectal Cancer and Advanced Adenomatous Polyps: A Systematic Review and Meta-analysis. Ann Intern Med 170 (5): 319-329, 2019. [PUBMED Abstract]
Zorzi M, Hassan C, Capodaglio G, et al.: Divergent Long-Term Detection Rates of Proximal and Distal Advanced Neoplasia in Fecal Immunochemical Test Screening Programs: A Retrospective Cohort Study. Ann Intern Med 169 (9): 602-609, 2018. [PUBMED Abstract]
Jensen CD, Corley DA, Quinn VP, et al.: Fecal Immunochemical Test Program Performance Over 4 Rounds of Annual Screening: A Retrospective Cohort Study. Ann Intern Med 164 (7): 456-63, 2016. [PUBMED Abstract]
Brenner H, Tao S, Haug U: Low-dose aspirin use and performance of immunochemical fecal occult blood tests. JAMA 304 (22): 2513-20, 2010. [PUBMED Abstract]
Fath RB, Winawer SJ: Endoscopic screening by flexible fiberoptic sigmoidoscopy. Front Gastrointest Res 10: 102-111, 1986.
Read TE, Read JD, Butterly LF: Importance of adenomas 5 mm or less in diameter that are detected by sigmoidoscopy. N Engl J Med 336 (1): 8-12, 1997. [PUBMED Abstract]
Wallace MB, Kemp JA, Trnka YM, et al.: Is colonoscopy indicated for small adenomas found by screening flexible sigmoidoscopy? Ann Intern Med 129 (4): 273-8, 1998. [PUBMED Abstract]
Levin TR, Palitz A, Grossman S, et al.: Predicting advanced proximal colonic neoplasia with screening sigmoidoscopy. JAMA 281 (17): 1611-7, 1999. [PUBMED Abstract]
Soetikno RM, Kaltenbach T, Rouse RV, et al.: Prevalence of nonpolypoid (flat and depressed) colorectal neoplasms in asymptomatic and symptomatic adults. JAMA 299 (9): 1027-35, 2008. [PUBMED Abstract]
Tinmouth J, Vella ET, Baxter NN, et al.: Colorectal Cancer Screening in Average Risk Populations: Evidence Summary. Can J Gastroenterol Hepatol 2016: 2878149, 2016. [PUBMED Abstract]
Swartz AW, Eberth JM, Josey MJ, et al.: Reanalysis of All-Cause Mortality in the U.S. Preventive Services Task Force 2016 Evidence Report on Colorectal Cancer Screening. Ann Intern Med 167 (8): 602-603, 2017. [PUBMED Abstract]
Miller EA, Pinsky PF, Schoen RE, et al.: Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: long-term follow-up of the randomised US PLCO cancer screening trial. Lancet Gastroenterol Hepatol 4 (2): 101-110, 2019. [PUBMED Abstract]
Holme Ø, Løberg M, Kalager M, et al.: Long-Term Effectiveness of Sigmoidoscopy Screening on Colorectal Cancer Incidence and Mortality in Women and Men: A Randomized Trial. Ann Intern Med 168 (11): 775-782, 2018. [PUBMED Abstract]
Juul FE, Cross AJ, Schoen RE, et al.: 15-Year Benefits of Sigmoidoscopy Screening on Colorectal Cancer Incidence and Mortality : A Pooled Analysis of Randomized Trials. Ann Intern Med 175 (11): 1525-1533, 2022. [PUBMED Abstract]
Lieberman DA, Weiss DG; Veterans Affairs Cooperative Study Group 380: One-time screening for colorectal cancer with combined fecal occult-blood testing and examination of the distal colon. N Engl J Med 345 (8): 555-60, 2001. [PUBMED Abstract]
Kato J, Morikawa T, Kuriyama M, et al.: Combination of sigmoidoscopy and a fecal immunochemical test to detect proximal colon neoplasia. Clin Gastroenterol Hepatol 7 (12): 1341-6, 2009. [PUBMED Abstract]
Bretthauer M, Løberg M, Wieszczy P, et al.: Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. N Engl J Med 387 (17): 1547-1556, 2022. [PUBMED Abstract]
Dominitz JA, Robertson DJ: Understanding the Results of a Randomized Trial of Screening Colonoscopy. N Engl J Med 387 (17): 1609-1611, 2022. [PUBMED Abstract]
Barclay RL, Vicari JJ, Doughty AS, et al.: Colonoscopic withdrawal times and adenoma detection during screening colonoscopy. N Engl J Med 355 (24): 2533-41, 2006. [PUBMED Abstract]
Brenner H, Altenhofen L, Kretschmann J, et al.: Trends in Adenoma Detection Rates During the First 10 Years of the German Screening Colonoscopy Program. Gastroenterology 149 (2): 356-66.e1, 2015. [PUBMED Abstract]
Lieberman D: Nonpolypoid colorectal neoplasia in the United States: the parachute is open. JAMA 299 (9): 1068-9, 2008. [PUBMED Abstract]
Robertson DJ, Lieberman DA, Winawer SJ, et al.: Colorectal cancers soon after colonoscopy: a pooled multicohort analysis. Gut 63 (6): 949-56, 2014. [PUBMED Abstract]
Corley DA, Jensen CD, Marks AR, et al.: Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med 370 (14): 1298-306, 2014. [PUBMED Abstract]
Nishihara R, Wu K, Lochhead P, et al.: Long-term colorectal-cancer incidence and mortality after lower endoscopy. N Engl J Med 369 (12): 1095-105, 2013. [PUBMED Abstract]
Baxter NN, Goldwasser MA, Paszat LF, et al.: Association of colonoscopy and death from colorectal cancer. Ann Intern Med 150 (1): 1-8, 2009. [PUBMED Abstract]
Brenner H, Chang-Claude J, Seiler CM, et al.: Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med 154 (1): 22-30, 2011. [PUBMED Abstract]
Doubeni CA, Weinmann S, Adams K, et al.: Screening colonoscopy and risk for incident late-stage colorectal cancer diagnosis in average-risk adults: a nested case-control study. Ann Intern Med 158 (5 Pt 1): 312-20, 2013. [PUBMED Abstract]
Smith MJ: Colon cancer screening hitting its stride but obstacles impair reaching final goal. Gastroenterology and Endoscopy News 59 (3): 9, 2008. [Refer to “Screening: it’s not just a good idea, it’s the law … almost” within the article].
Bretthauer M, Ekbom A, Malila N, et al.: [Politics and science in colorectal cancer screening] Tidsskr Nor Laegeforen 126 (13): 1766-7, 2006. [PUBMED Abstract]
Ma W, Wang K, Nguyen LH, et al.: Association of Screening Lower Endoscopy With Colorectal Cancer Incidence and Mortality in Adults Older Than 75 Years. JAMA Oncol 7 (7): 985-992, 2021. [PUBMED Abstract]
Ferrucci JT: Colon cancer screening with virtual colonoscopy: promise, polyps, politics. AJR Am J Roentgenol 177 (5): 975-88, 2001. [PUBMED Abstract]
Johnson CD, Chen MH, Toledano AY, et al.: Accuracy of CT colonography for detection of large adenomas and cancers. N Engl J Med 359 (12): 1207-17, 2008. [PUBMED Abstract]
Regge D, Laudi C, Galatola G, et al.: Diagnostic accuracy of computed tomographic colonography for the detection of advanced neoplasia in individuals at increased risk of colorectal cancer. JAMA 301 (23): 2453-61, 2009. [PUBMED Abstract]
Iannaccone R, Laghi A, Catalano C, et al.: Computed tomographic colonography without cathartic preparation for the detection of colorectal polyps. Gastroenterology 127 (5): 1300-11, 2004. [PUBMED Abstract]
Zalis ME, Blake MA, Cai W, et al.: Diagnostic accuracy of laxative-free computed tomographic colonography for detection of adenomatous polyps in asymptomatic adults: a prospective evaluation. Ann Intern Med 156 (10): 692-702, 2012. [PUBMED Abstract]
Edwards JT, Wood CJ, Mendelson RM, et al.: Extracolonic findings at virtual colonoscopy: implications for screening programs. Am J Gastroenterol 96 (10): 3009-12, 2001. [PUBMED Abstract]
Hellström M, Svensson MH, Lasson A: Extracolonic and incidental findings on CT colonography (virtual colonoscopy). AJR Am J Roentgenol 182 (3): 631-8, 2004. [PUBMED Abstract]
Gluecker TM, Johnson CD, Wilson LA, et al.: Extracolonic findings at CT colonography: evaluation of prevalence and cost in a screening population. Gastroenterology 124 (4): 911-6, 2003. [PUBMED Abstract]
Pickhardt PJ, Hanson ME, Vanness DJ, et al.: Unsuspected extracolonic findings at screening CT colonography: clinical and economic impact. Radiology 249 (1): 151-9, 2008. [PUBMED Abstract]
Kimberly JR, Phillips KC, Santago P, et al.: Extracolonic findings at virtual colonoscopy: an important consideration in asymptomatic colorectal cancer screening. J Gen Intern Med 24 (1): 69-73, 2009. [PUBMED Abstract]
Mulhall BP, Veerappan GR, Jackson JL: Meta-analysis: computed tomographic colonography. Ann Intern Med 142 (8): 635-50, 2005. [PUBMED Abstract]
Herrinton LJ, Selby JV, Friedman GD, et al.: Case-control study of digital-rectal screening in relation to mortality from cancer of the distal rectum. Am J Epidemiol 142 (9): 961-4, 1995. [PUBMED Abstract]
Dong SM, Traverso G, Johnson C, et al.: Detecting colorectal cancer in stool with the use of multiple genetic targets. J Natl Cancer Inst 93 (11): 858-65, 2001. [PUBMED Abstract]
Traverso G, Shuber A, Levin B, et al.: Detection of APC mutations in fecal DNA from patients with colorectal tumors. N Engl J Med 346 (5): 311-20, 2002. [PUBMED Abstract]
Traverso G, Shuber A, Olsson L, et al.: Detection of proximal colorectal cancers through analysis of faecal DNA. Lancet 359 (9304): 403-4, 2002. [PUBMED Abstract]
Ahlquist DA, Skoletsky JE, Boynton KA, et al.: Colorectal cancer screening by detection of altered human DNA in stool: feasibility of a multitarget assay panel. Gastroenterology 119 (5): 1219-27, 2000. [PUBMED Abstract]
Imperiale TF, Ransohoff DF, Itzkowitz SH, et al.: Fecal DNA versus fecal occult blood for colorectal-cancer screening in an average-risk population. N Engl J Med 351 (26): 2704-14, 2004. [PUBMED Abstract]
Woolf SH: A smarter strategy? Reflections on fecal DNA screening for colorectal cancer. N Engl J Med 351 (26): 2755-8, 2004. [PUBMED Abstract]
Imperiale TF, Ransohoff DF, Itzkowitz SH, et al.: Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med 370 (14): 1287-97, 2014. [PUBMED Abstract]
Imperiale TF, Porter K, Zella J, et al.: Next-Generation Multitarget Stool DNA Test for Colorectal Cancer Screening. N Engl J Med 390 (11): 984-993, 2024. [PUBMED Abstract]
Chung DC, Gray DM, Singh H, et al.: A Cell-free DNA Blood-Based Test for Colorectal Cancer Screening. N Engl J Med 390 (11): 973-983, 2024. [PUBMED Abstract]
Gupta S, Halm EA, Rockey DC, et al.: Comparative effectiveness of fecal immunochemical test outreach, colonoscopy outreach, and usual care for boosting colorectal cancer screening among the underserved: a randomized clinical trial. JAMA Intern Med 173 (18): 1725-32, 2013. [PUBMED Abstract]
Imperiale TF, Monahan PO, Stump TE, et al.: Derivation and Validation of a Scoring System to Stratify Risk for Advanced Colorectal Neoplasia in Asymptomatic Adults: A Cross-sectional Study. Ann Intern Med 163 (5): 339-46, 2015. [PUBMED Abstract]
Chiu HM, Ching JY, Wu KC, et al.: A Risk-Scoring System Combined With a Fecal Immunochemical Test Is Effective in Screening High-Risk Subjects for Early Colonoscopy to Detect Advanced Colorectal Neoplasms. Gastroenterology 150 (3): 617-625.e3, 2016. [PUBMED Abstract]
Evidence of Harms
Potential harms are associated with the modalities used to screen for colorectal cancer (CRC), some of which have sufficient evidence and some that do not.
Overview
The tables for each screening test below show the magnitude of burden for several categories of harms encountered along the screening cascade. The magnitude of harms is a combination of the frequency and severity of harm, as perceived by the patient.
Harms are defined broadly as any negative effect on individuals or populations resulting from being involved in the screening process (cascade) compared with not screening. Potential harms are organized according to the type of harm (e.g., physical, psychological, and hassle/opportunity costs) and when they occur in the screening cascade (e.g., screening test/workup; screening test/workup results; surveillance and surveillance results; and early treatment and overtreatment). For example, potential harms of screening colonoscopy include harms of the screening test itself (e.g., perforation and bleeding), results of the screening test (e.g., anxiety from an abnormal result), surveillance (e.g., harms of more frequent colonoscopies), and treatment (e.g., earlier treatment or overtreatment). Harms are also associated with the workup for other colorectal cancer screening tests (e.g., colonoscopy for positive fecal occult blood test [FOBT]). A recent study of three major hospitals found that 71% of endoscopes tested positive for bacteria after cleaning and high-level disinfection of the scopes. This raises concern for endoscopy-associated pathogen transmission and patient safety, although no patients were involved in the study and the implications for patients are unknown.[1] For all aspects of participating in the screening cascade, there are time/effort and opportunity costs (nonfinancial harms) for the patient. The following tables do not include any financial harms to the patient/family, nor any psychological harm from anticipation of future financial costs related to screening.
Table 4. Colonoscopy
Stage of Screening Cascade
Physical
Psychological
Time/Effort, Opportunity
CRC = colorectal cancer.
Screening Test/Workup
Average 0.3% complications requiring hospitalization or resulting in death, higher with polypectomy and in older patients (fair evidence)
Percentage of people who suffer psychological distress on consideration of having colonoscopy; severity and duration (insufficient evidence)
About 38 hours (median) required for preparation, procedure, sedation (one study, fair evidence) [2]
Discomfort of preparation and procedure; adverse effects of preparation (insufficient evidence to determine magnitude and frequency)
Complications from sedation during procedure (insufficient evidence to determine magnitude and frequency)
Screening Test/Workup Results
Increased risk of suicide and cardiovascular mortality soon after diagnosis (insufficient evidence)
Percentage of people who suffer psychological distress after receiving positive screening and/or pathological results; severity and duration (insufficient evidence)
Time and effort required to receive and understand screening test or workup results, including extra physician visits for positive tests (insufficient evidence)
Surveillance/Results
More frequent colonoscopy
Percentage of people who suffer psychological distress after receiving positive screening and/or pathological results; severity and duration (insufficient evidence)
Time and effort required to undergo colonoscopy (median, 38 hours, see above)
Time and effort required to receive and understand surveillance results (insufficient evidence)
Treatment (Early Treatment and Overtreatment)
Overdiagnosis and overtreatment of precursor polyps or earlier treatment of CRC (may or may not receive benefit from earlier treatment) (insufficient evidence)
Percentage of people who suffer psychological distress after undergoing overtreatment or earlier treatment without benefit; severity and duration (insufficient evidence)
Time and effort required to receive overtreatment or earlier treatment without benefit (insufficient evidence)
Table 5. FOBT/FIT, Other Stool-Based Tests (Including Fecal DNA)
aWorkup test is colonoscopy. Descriptions of the associated harms can be found in the colonoscopy section (for more information, see the Colonoscopy section in Evidence of Harms).
bTreatment harms will be the same for all screening tests.
Screening Test
None (no evidence)
Percentage of people who suffer psychological distress on consideration of having CRC screening; severity and duration (insufficient evidence)
Time and effort required to change diet (if required), collect samples, and return to appropriate facility (insufficient evidence)
Screening Test Results
N/A
Percentage of people who suffer psychological distress after receiving positive screening results; severity and duration (insufficient evidence)
Time and effort required to receive and understand screening test results, including extra physician visits or communication for positive tests (insufficient evidence)
Workupa
See colonoscopy
See colonoscopy
See colonoscopy
Workup Results
N/A
See colonoscopy
See colonoscopy
Surveillance/Results
See colonoscopy
See colonoscopy
See colonoscopy
Treatment (Early Treatment and Overtreatment)b
See colonoscopy
See colonoscopy
See colonoscopy
Table 6. Flexible Sigmoidoscopy
Stage of Screening Cascade
Physical
Psychological
Time/Effort, Opportunity
N/A = not applicable.
aWorkup test is colonoscopy. Descriptions of the associated harms can be found in the colonoscopy section (for more information, see the Colonoscopy section in Evidence of Harms).
bTreatment harms will be the same for all screening tests.
Screening Test
Average serious complications for 0.03% of patients (fair evidence) [3]
Percentage of people who suffer psychological distress on consideration of having colonoscopy; severity and duration (insufficient evidence)
Time and effort required to perform preparation, travel to and attend screening, return to usual activities (insufficient evidence)
Screening Test Results
N/A
See colonoscopy
See colonoscopy
Workupa
See colonoscopy
See colonoscopy
See colonoscopy
Surveillance/Results
N/A
See colonoscopy
See colonoscopy
Treatment (Early Treatment and Overtreatment)b
See colonoscopy
See colonoscopy
See colonoscopy
Table 7. Computed Tomography Colonography
Stage of Screening Cascade
Physical
Psychological
Time/Effort, Opportunity
CRC = colorectal cancer.
Screening Test/Workup
Discomfort of preparation and procedure; radiation exposure (insufficient evidence)
Percentage of people who suffer psychological distress on consideration of screening; severity and duration (insufficient evidence)
Time required for preparation, procedure (exact time and effort uncertain) (insufficient evidence)
Screening Test/Workup Results
Increased risk of suicide and cardiovascular mortality soon after diagnosis (insufficient evidence)
Percentage of people who suffer psychological distress after receiving positive screening and/or pathological results; severity and duration (insufficient evidence)
Time and effort required to receive and understand screening test or workup results, including extra physician visits for positive tests (insufficient evidence)
Percentage of people who suffer psychological distress after receiving positive screening and/or pathological results; severity and duration (insufficient evidence)
Time and effort required to undergo colonoscopy (mean, 38 hours, see Table 4)
Time and effort required to receive and understand surveillance results (insufficient evidence)
Treatment (Early Treatment and Overtreatment)
Overdiagnosis and overtreatment of precursor polyps or earlier treatment of CRC (may or may not receive benefit from earlier treatment) (insufficient evidence)
Percentage of people who suffer psychological distress undergoing overtreatment or earlier treatment without benefit; severity and duration (insufficient evidence)
Time and effort required to receive overtreatment or earlier treatment without benefit (insufficient evidence)
Evidence Summary
Colonoscopy
The potential physical harms of colonoscopy include adverse effects from the preparation and adverse effects from the procedure (e.g., colonic perforation, bleeding, effects of sedation).[4–6] A systematic review of 60 studies that assessed complications of colonoscopy screening in asymptomatic patients found infrequent serious morbidity, which comprised major bleeding (0.8/1,000 procedures; 95% confidence interval [CI], 0.18–1.63) and perforation (0.07/1,000 procedures; 95% CI, 0.006–0.17), and only minor and short-lasting psychological harms.[7] These complications can be serious, requiring hospitalization. Colonic perforation and serious bleeding occur more often with biopsy or polypectomy, with an overall average of three to five serious complications per 1,000 procedures. The physical harm of discomfort during the procedure has been reduced by sedation, although sedation has its own potential for physical harm (magnitude and severity uncertain because of insufficient evidence).
Physical harms are also associated with further steps in the screening cascade. These harms include diagnosis of CRC (some large ecological studies have shown an increase in suicide soon after diagnosis) and overdiagnosis/overtreatment due to treating lesions that would never have caused the patient important problems (evidence insufficient to determine magnitude and severity).
The potential psychological harms of colonoscopy include anticipation of the procedure and anxiety while awaiting the results of biopsy reports. For people with polyps, there may be increased distress in considering oneself at increased risk of CRC (evidence insufficient). For people newly diagnosed with CRC, many will experience increased anxiety and depression for at least 6 months, as prognosis and treatment are discussed (evidence insufficient).
The harm of time/effort and opportunity costs involved in moving through the demands of the screening cascade are present throughout the process (evidence insufficient to determine frequency and severity).
FOBT/immunochemical FOBT (FIT)
The potential physical harms of fecal-based testing include the same harms as for colonoscopy for people with a positive test who have been referred for diagnostic colonoscopy.
The potential psychological harms, as well as time/effort and opportunity costs are also similar to the description above for colonoscopy (for more information, see the Colonoscopy section in Evidence of Harms).[8] These harms are associated with moving through the screening cascade, regardless of the initial screening test. Although it is highly likely that these psychological harms, plus time/effort and opportunity costs, do occur, the exact frequency and severity of these harms are uncertain because of insufficient evidence.
Sigmoidoscopy
The potential physical harms of sigmoidoscopy are considerably less than those of colonoscopy, with a less intensive preparation. Serious procedural complications occur in approximately three in 10,000 sigmoidoscopies, compared with in three in 1,000 colonoscopies.[3] There is usually no sedation with sigmoidoscopy, which lowers the potential for complications even further.
The potential psychological harms of sigmoidoscopy screening, as well as the time/effort and opportunity costs of screening, are the same as given above for other screening strategies.
Computed tomography colonography (CTC)
The potential physical harms due directly to CTC are less than either colonoscopy or sigmoidoscopy, with rare procedural complications.[3] However, CTC does involve repeated radiation exposure, with uncertain associated harms, and it also detects a number of extra-colonic incidental findings.[9–13] Incidental findings have been detected in 40% to 98% of CTCs, with a variable number of these considered significant enough to proceed with further diagnostic testing. As there is little evidence that early detection of any of these findings could improve health outcomes for patients, these findings may be considered as harms until proven otherwise.
The potential psychological harms or time/effort and opportunity costs for CTC are similar to the descriptions above for patients moving through the screening cascade (evidence insufficient to determine frequency and severity).
References
Ofstead CL, Heymann OL, Quick MR, et al.: Residual moisture and waterborne pathogens inside flexible endoscopes: Evidence from a multisite study of endoscope drying effectiveness. Am J Infect Control 46 (6): 689-696, 2018. [PUBMED Abstract]
Jonas DE, Russell LB, Sandler RS, et al.: Value of patient time invested in the colonoscopy screening process: time requirements for colonoscopy study. Med Decis Making 28 (1): 56-65, 2008 Jan-Feb. [PUBMED Abstract]
Whitlock EP, Lin JS, Liles E, et al.: Screening for colorectal cancer: a targeted, updated systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 149 (9): 638-58, 2008. [PUBMED Abstract]
Lin JS, Piper MA, Perdue LA, et al.: Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 315 (23): 2576-94, 2016. [PUBMED Abstract]
Levin TR, Zhao W, Conell C, et al.: Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med 145 (12): 880-6, 2006. [PUBMED Abstract]
Warren JL, Klabunde CN, Mariotto AB, et al.: Adverse events after outpatient colonoscopy in the Medicare population. Ann Intern Med 150 (12): 849-57, W152, 2009. [PUBMED Abstract]
Vermeer NC, Snijders HS, Holman FA, et al.: Colorectal cancer screening: Systematic review of screen-related morbidity and mortality. Cancer Treat Rev 54: 87-98, 2017. [PUBMED Abstract]
Bobridge A, Bampton P, Cole S, et al.: The psychological impact of participating in colorectal cancer screening by faecal immuno-chemical testing–the Australian experience. Br J Cancer 111 (5): 970-5, 2014. [PUBMED Abstract]
Kimberly JR, Phillips KC, Santago P, et al.: Extracolonic findings at virtual colonoscopy: an important consideration in asymptomatic colorectal cancer screening. J Gen Intern Med 24 (1): 69-73, 2009. [PUBMED Abstract]
Yee J, Kumar NN, Godara S, et al.: Extracolonic abnormalities discovered incidentally at CT colonography in a male population. Radiology 236 (2): 519-26, 2005. [PUBMED Abstract]
Hara AK, Johnson CD, MacCarty RL, et al.: Incidental extracolonic findings at CT colonography. Radiology 215 (2): 353-7, 2000. [PUBMED Abstract]
Gluecker TM, Johnson CD, Wilson LA, et al.: Extracolonic findings at CT colonography: evaluation of prevalence and cost in a screening population. Gastroenterology 124 (4): 911-6, 2003. [PUBMED Abstract]
Xiong T, McEvoy K, Morton DG, et al.: Resources and costs associated with incidental extracolonic findings from CT colonogaphy: a study in a symptomatic population. Br J Radiol 79 (948): 948-61, 2006. [PUBMED Abstract]
Latest Updates to This Summary (04/10/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Updated statistics with estimated new cases and deaths for 2025 (cited Bray et al. as reference 1 and American Cancer Society as reference 2). Also revised text to state that between 2012 and 2021, incidence rates increased by 2.4% per year in individuals younger than 55 years and by 0.4% per year in individuals aged 50 to 64 years.
This summary is written and maintained by the PDQ Screening and Prevention Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about colorectal cancer screening. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Screening and Prevention Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Screening and Prevention Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Colorectal Cancer Screening. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /types/colorectal/hp/colorectal-screening-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389266]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Genetics of Colorectal Cancer (PDQ®)–Health Professional Version
Executive Summary
This executive summary reviews the topics covered in the PDQ summary on the genetics of colorectal cancer (CRC), with hyperlinks to detailed sections below that describe the evidence on each topic.
Inheritance and Risk
Factors suggestive of a genetic contribution to CRC include the following: (1) a strong family history of CRC and/or polyps; (2) multiple primary cancers in a patient with CRC; (3) the existence of other cancers within the kindred consistent with known syndromes causing an inherited risk of CRC, such as endometrial cancer; and (4) early age at diagnosis of CRC. Hereditary CRC is most commonly inherited in an autosomal dominant pattern, although two syndromes are inherited in an autosomal recessive pattern (MUTYH-associated polyposis and NTHL1).
At least three validated computer models are available to estimate the probability that an individual affected with cancer carries a pathogenic variant in a mismatch repair (MMR) gene associated with Lynch syndrome, the most common inherited CRC syndrome. These include the MMRpro, MMRpredict, and PREMM5 (PREdiction Model for gene Mutations) prediction models. Individuals with a quantified risk of 2.5% or greater on PREMM5 or 5% or greater on MMRpro and MMRpredict are recommended for genetic evaluation referral and testing.
Associated Genes and Syndromes
Hereditary CRC has two well-described forms: (1) polyposis (including familial adenomatous polyposis [FAP] and attenuated FAP [AFAP], which are caused by pathogenic variants in the APC gene; and MUTYH-associated polyposis, which is caused by pathogenic variants in the MUTYH gene); and (2) Lynch syndrome (often referred to as hereditary nonpolyposis colorectal cancer), which is caused by germline pathogenic variants in DNA MMR genes (MLH1, MSH2, MSH6, and PMS2) and EPCAM. Other CRC syndromes and their associated genes include oligopolyposis (POLE, POLD1), NTHL1, juvenile polyposis syndrome (BMPR1A, SMAD4), Cowden syndrome (PTEN), and Peutz-Jeghers syndrome (STK11). Many of these syndromes are also associated with extracolonic cancers and other manifestations. Serrated polyposis syndrome, which is characterized by the appearance of hyperplastic polyps, appears to have a familial component, but the genetic basis remains unknown. The natural history of some of these syndromes is still being described. Many other families exhibit aggregation of CRC and/or adenomas, but with no apparent association with an identifiable hereditary syndrome, and they are known collectively as familial CRC. In addition, most individuals with CRC diagnosed before age 50 years and without a family history of cancer do not have a pathogenic variant associated with an inherited cancer syndrome.
Genome-wide searches are showing promise in identifying common, low-penetrance susceptibility alleles for many complex diseases, including CRCs, but the clinical utility of these findings remains uncertain.
Clinical Management
It is becoming the standard of care at many centers that all individuals with newly diagnosed CRC are evaluated for Lynch syndrome through molecular diagnostic tumor testing assessing MMR deficiency. A universal screening approach to tumor testing is supported, in which all CRC cases are evaluated regardless of age at diagnosis or fulfillment of existing clinical criteria for Lynch syndrome. A more cost-effective approach has been reported whereby all patients aged 70 years or younger with CRC and older patients who meet the revised Bethesda guidelines are tested for Lynch syndrome. Tumor evaluation often begins with immunohistochemistry testing for the expression of the MMR proteins associated with Lynch syndrome or microsatellite instability (MSI) testing, BRAF testing, and MLH1 hypermethylation analyses.
Colonoscopy for CRC screening and surveillance is commonly performed in individuals with hereditary CRC syndromes and has been associated with improved survival outcomes. For example, surveillance of Lynch syndrome patients with colonoscopy every 1 to 2 years, and in one study up to 3 years, has been shown to reduce CRC incidence and mortality. Extracolonic surveillance is also a mainstay for some hereditary CRC syndromes depending on the other cancers associated with the syndrome. For example, regular endoscopic surveillance of the duodenum in FAP patients has been shown to improve survival.
Prophylactic surgery (colectomy) has also been shown to improve survival in patients with FAP. The timing and extent of risk-reducing surgery usually depends on the number of polyps, their size, histology, and symptomatology. For patients with Lynch syndrome and a diagnosis of CRC, extended resection is associated with fewer metachronous CRCs and additional surgical procedures for colorectal neoplasia than in patients who undergo segmental resection for CRC. The surgical decision must consider the age of the patient, comorbidities, clinical stage of the tumor, sphincter function, and the patient’s wishes.
Chemopreventive agents have also been studied in the management of FAP and Lynch syndrome. In FAP patients, celecoxib and sulindac have been associated with a decrease in polyp size and number. A double-blind, randomized, controlled trial evaluating the efficacy of sulindac plus an epidermal growth factor receptor inhibitor, erlotinib, versus placebo in FAP or AFAP patients with duodenal polyps suggested that erlotinib has the potential to inhibit duodenal polyps in FAP patients. An ongoing trial will determine whether lower doses of erlotinib alone will significantly reduce duodenal polyp burden. Aspirin use (600 mg daily) was shown to have a preventive effect on cancer incidence in Lynch syndrome patients in a large randomized trial; lower doses are being examined in an ongoing study.
Novel therapies that stimulate the immune system have been evaluated in MMR-deficient tumors, including those related to Lynch syndrome. The dense immune infiltration and cytokine-rich environment in MMR-deficient tumors may improve clinical outcomes. A critical pathway responsible for mediating tumor-induced immune suppression is the programmed cell death-1 (PD-1)–mediated checkpoint pathway. Two phase 2 studies using anti–PD-1 immune checkpoint inhibitors (pembrolizumab and nivolumab) demonstrated favorable outcomes, including progression-free survival, radiographic response rates, and disease control rates in metastatic CRC with MMR deficiency and MSI that had progressed on prior cytotoxic chemotherapy. Pembrolizumab has shown similar benefit in other noncolorectal cancers with MMR deficiency and MSI, but not in tumors that are microsatellite stable.
Psychosocial and Behavioral Issues
Psychosocial factors influence decisions about genetic testing for inherited cancer risk and risk-management strategies. Uptake of genetic counseling and genetic testing for Lynch syndrome and FAP varies widely across studies. Factors that have been associated with genetic counseling and testing uptake in Lynch syndrome families include having children, the number of affected relatives, perceived risk of developing CRC, and frequency of thoughts about CRC. Psychological studies have shown low levels of distress, particularly in the long term, after genetic testing for Lynch syndrome in both carriers and noncarriers. However, other studies have demonstrated the possibility of increased distress following genetic testing for FAP. Colon and gynecologic cancer screening rates have been shown to increase or be maintained among carriers of MMR pathogenic variants within the year after disclosure of results, while screening rates decrease among noncarriers. The latter is expected as the screening recommendations for unaffected individuals are those that apply to the general population. Studies measuring quality-of-life variables in FAP patients show normal-range results; however, these studies suggest that risk-reducing surgery for FAP may have negative quality-of-life effects for at least some proportion of those affected. Patients’ communication with their family members about an inherited risk of CRC is complex; gender, age, and the degree of relatedness are some elements that affect disclosure of this information. Research is ongoing to better understand and address psychosocial and behavioral issues in high-risk families.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in both men and women.
Estimated new cases and deaths from CRC in 2024 in the United States:[1]
New cases: 152,810.
Deaths: 53,010.
About 75% of patients with CRC have sporadic disease with no apparent evidence of having inherited the disorder. The remaining 10% to 30% of patients have a family history of CRC that suggests a hereditary contribution, common exposures or shared risk factors among family members, or a combination of both.[2] Pathogenic variants in high-penetrancegenes have been identified as the cause of inherited cancer risk in some colon cancer–prone families; these are estimated to account for only 5% to 6% of CRC cases overall.[3,4]
In addition, pathogenic variants in lower-penetrance genes may contribute to familial colon cancer risk. In such cases, gene-gene and gene-environment interactions may contribute to the development of CRC.
Colorectal Polyps as Precursors to Colorectal Cancer (CRC)
Colorectal tumors present with a broad spectrum of neoplasms, ranging from benign growths to invasive cancer, and are predominantly epithelial-derived tumors (i.e., adenomas or adenocarcinomas).
Transformation of any polyp into cancer goes through the adenoma-carcinoma sequence. Polyps that have traditionally been considered nonneoplastic include those of the hyperplastic, juvenile, hamartomatous, inflammatory, and lymphoid types. However, in certain circumstances, hamartomatous and juvenile polyps can progress into cancer.
Research, however, does suggest a substantial risk of colon cancer in individuals with juvenile polyposis syndrome and Peutz-Jeghers syndrome, although the nonadenomatous polyps associated with these syndromes have historically been viewed as nonneoplastic.[5–7]
Epidemiological studies have shown that a personal history of colon adenomas places one at an increased risk of developing colon cancer.[8]
Two complementary interpretations of this observation are as follows:
The adenoma may reflect an innate or acquired tendency of the colon to form tumors.
Adenomas are the primary precursor lesion of colon cancer.
More than 95% of CRCs are carcinomas, and about 95% of these are adenocarcinomas. It is well recognized that adenomatous polyps are benign tumors that may undergo malignant transformation. They have been classified into three histological types, with increasing malignant potential: tubular, tubulovillous, and villous. Adenocarcinomas are generally considered to arise from adenomas,[9–13] based upon the following important observations:
Benign and malignant tissue occur within colorectal tumors.[14]
When patients with adenomas were followed for 20 years, the risk of cancer at the site of the adenoma was 25%, a rate much higher than that expected in the normal population.[15]
The following three characteristics of adenomas are highly correlated with the potential to transform into cancer:[14]
Larger size.
Villous pathology.
The degree of dysplasia within the adenoma.
In addition, removal of adenomatous polyps is associated with reduced CRC incidence.[16,17] While most adenomas are polypoid, flat and depressed lesions may be more prevalent than previously recognized. Large, flat, and depressed lesions may be more likely to be severely dysplastic, although this remains to be clearly proven.[18,19] Specialized techniques may be needed to identify, biopsy, and remove such lesions.[20]
Family History as a Risk Factor for CRC
Some of the earliest studies of family history of CRC were those of Utah families that reported a higher percentage of deaths from CRC (3.9%) among the first-degree relatives (FDRs) of patients who had died from CRC than among sex-matched and age-matched controls (1.2%).[21] This difference has since been replicated in numerous studies that have consistently found that FDRs of affected cases are themselves at a twofold to threefold increased risk of CRC. Despite the various study designs (case-control, cohort), sampling frames, sample sizes, methods of data verification, analytic methods, and countries where the studies originated, the magnitude of risk is consistent.[22–27]
A systematic review and meta-analysis of familial CRC risk has been reported.[28] Of 24 studies included in the analysis, all but one reported an increased risk of CRC if there was an affected FDR. The relative risk (RR) for CRC in the pooled study was 2.25 (95% confidence interval [CI], 2.00–2.53) if there was an affected FDR. In 8 of 11 studies, if the index cancer arose in the colon, the risk was slightly higher than if it arose in the rectum. The pooled analysis revealed an RR in relatives of colon and rectal cancer patients of 2.42 (95% CI, 2.20–2.65) and 1.89 (95% CI, 1.62–2.21), respectively. The analysis did not reveal a difference in RR for colon cancer based on location of the tumor (right side vs. left side).
The number of affected family members and age at cancer diagnosis correlated with the CRC risk. In studies reporting more than one FDR with CRC, the RR was 3.76 (95% CI, 2.56–5.51). The highest RR was observed when the index case was diagnosed in individuals younger than 45 years (RR, 3.87; 95% CI, 2.40–6.22) compared with family members of index cases diagnosed at ages 45 to 59 years (RR, 2.25; 95% CI, 1.85–2.72), and to family members of index cases diagnosed at age 60 years or older (RR, 1.82; 95% CI, 1.47–2.25). In this meta-analysis, the familial risk of CRC associated with adenoma in an FDR was analyzed. The pooled analysis demonstrated an RR for CRC of 1.99 (95% CI, 1.55–2.55) in individuals who had an FDR with an adenoma.[28] This finding has been corroborated.[29] Other studies have reported that age at diagnosis of the adenoma influences the CRC risk, with younger age at adenoma diagnosis associated with higher RR.[30,31] As with any meta-analysis, there could be potential biases that might affect the results of the analysis, including incomplete and nonrandom ascertainment of studies included; publication bias; and heterogeneity between studies relative to design, target populations, and control selection. This study is reinforcement that there are significant associations between familial CRC risk, age at diagnosis of both CRC and adenomas, and multiplicity of affected family members.
Table 1. Estimated Relative and Absolute Risk of Developing Colorectal Cancer (CRC)
CI = confidence interval; FDR = first-degree relative.
aData from the Surveillance, Epidemiology, and End Results Program database.
bThe absolute risks of CRC for individuals with affected relatives was calculated using the relative risks for CRC [28] and the absolute risk of CRC by age 79 yearsa.
No family history
1
4a
One FDR with CRC
2.3 (95% CI, 2.0–2.5)
9b
More than one FDR with CRC
4.3 (95% CI, 3.0–6.1)
16b
One affected FDR diagnosed with CRC before age 45 y
3.9 (95% CI, 2.4–6.2)
15b
One FDR with colorectal adenoma
2.0 (95% CI, 1.6–2.6)
8b
When the family history includes two or more relatives with CRC, the possibility of a genetic syndrome is increased substantially. The first step in this evaluation is a detailed review of the family history to determine the number of relatives affected, their relationship to each other, the age at which the CRC was diagnosed, the presence of multiple primary CRCs, and the presence of any other cancers (e.g., endometrial) consistent with an inherited CRC syndrome. (Refer to the Major Genetic Syndromes section of this summary for more information.) Computer models are now available to estimate the probability of developing CRC.[32] These models can be helpful in providing genetic counseling to individuals at average risk and high risk of developing cancer. In addition, at least three validated models are also available for predicting the probability of carrying a pathogenic variant in a mismatch repair (MMR) gene.[33–35]
Figure 1 shows the proportion of CRC cases that arise in various family risk settings.[36]
EnlargeFigure 1. The fractions of colon cancer cases that arise in various family risk settings. Reprinted from Gastroenterology, Vol. 119, No. 3, Randall W. Burt, Colon Cancer Screening, Pages 837-853, Copyright (2000), with permission from Elsevier.
Inheritance of CRC Predisposition
Several genes associated with CRC risk have been identified; these are described in detail in the Colon Cancer Genes section of this summary. Almost all pathogenic variants known to cause a predisposition to CRC are inherited in an autosomal dominant fashion.[37] One example of autosomal recessive inheritance, MUTYH-associated polyposis (MAP), has been identified. (Refer to the MUTYH-Associated Polyposis [MAP] section of this summary for more information.) Thus, the family characteristics that suggest autosomal dominant inheritance of cancer predisposition are important indicators of high risk and of the possible presence of a cancer-predisposing pathogenic variant. These include the following:
Vertical transmission of cancer predisposition in autosomal dominant conditions. (Vertical transmission refers to the presence of a genetic predisposition in sequential generations.)
Inheritance risk of 50% for both male and female children. When a parent carries an autosomal dominant genetic predisposition, each child has a 50% chance of inheriting the predisposition. The risk is the same for both male and female children.
Other clinical characteristics also suggest the presence of a hereditary CRC syndrome:
Cancers in people with a hereditary predisposition typically occur at an earlier age than in sporadic cases.[38]
A predisposition to CRC may include a predisposition to other cancers, such as endometrial cancer, as detailed in the Major Genetic Syndromes section of this summary.
In addition, two or more primary cancers may occur in a single individual. These could be multiple primary cancers of the same type (e.g., two separate primary CRCs) or primary cancer of different types (e.g., colorectal and endometrial cancer in the same individual).
The presence of nonneoplastic extracolonic features may suggest a hereditary colon cancer predisposition syndrome (e.g., congenital hypertrophy of the retinal pigment epithelium and desmoid tumors in familial adenomatous polyposis [FAP]).
An uncommon tumor (e.g., adrenocortical carcinoma, sebaceous adenoma or carcinoma, and trichilemmoma) may serve as a clue to the presence of a hereditary cancer syndrome.
The presence of multiple polyps may suggest a hereditary colon cancer predisposition syndrome. As susceptibility to oligopolyposis (as few as 10–15 polyps) has become apparent, clinicians, and gastrointestinal endoscopists in particular, may consider multigene (panel) testing of an ever-expanding list of genes associated with CRC. (Refer to Table 2, Genes Associated with a High Susceptibility of Colorectal Cancer, for more information.) Because oligopolyposis also involves diverse pathology (including hamartomas, sessile serrated polyps, and sessile serrated adenomas), careful attention to polyp count and polyp histologies helps to determine whether genetic testing and/or further clinical evaluation is appropriate.
The two most common causes of hereditary CRC are FAP (including AFAP), due to germline pathogenic variants in the APC gene,[39–46] and Lynch syndrome (previously called hereditary nonpolyposis colorectal cancer [HNPCC]), which is caused by germline pathogenic variants in DNA MMR genes.[47–50] (Figure 2 depicts a classic family with Lynch syndrome, highlighting some of the indicators of hereditary CRC that are described above.) Many other families exhibit aggregation of CRC and/or adenomas, but with no apparent association with an identifiable hereditary syndrome, and are known collectively as familial CRC.[37]
EnlargeFigure 2. Lynch syndrome pedigree. This pedigree shows some of the classic features of a family with Lynch syndrome, including affected family members with colon cancer or endometrial cancer, a young age at onset in some individuals, and incomplete penetrance. Lynch syndrome families may exhibit some or all of these features. Lynch syndrome families may also include individuals with other gastrointestinal, gynecologic, and genitourinary cancers, or other extracolonic cancers. As an autosomal dominant syndrome, Lynch syndrome can be transmitted through maternal or paternal lineages, as depicted in the figure. Because the cancer risk is not 100%, individuals who have Lynch syndrome may not develop cancer, such as the mother of the female with colon cancer diagnosed at age 37 years in this pedigree (called incomplete penetrance).
Identification of Individuals at High Genetic Risk of CRC
National Comprehensive Cancer Network (NCCN) guidelines are updated annually to help identify patients who are appropriate for referral to cancer genetic counseling services. Furthermore, NCCN also provides cancer surveillance recommendations for hereditary cancer syndromes. The American College of Medical Genetics and Genomics and the National Society of Genetic Counselors have published a comprehensive set of personal/family history criteria to help identify at-risk individuals for referral to cancer genetics risk consultations.[51] These practice guidelines consider tumor types, other specific tumor features, and related criteria that would prompt a genetics referral. The authors state that these guidelines from ACMG/NSGC are intended to maximize referral of appropriate at-risk individuals to cancer genetic counseling services, but they are not meant to provide genetic testing or treatment recommendations. In addition, the authors note other sources that discuss updated/evolving genetic testing criteria for hereditary cancer syndromes (e.g., NCCN), and they acknowledge the increasing role of nongenetics professionals in facilitating genetic testing, especially to guide cancer treatment.[52]
When such persons are identified, options tailored to the patient situation are considered. (Refer to the Major Genetic Syndromes section of this summary for information on specific interventions for individual syndromes.)
At this time, the use of pathogenic variant testing to identify genetic susceptibility to CRC is not recommended as a screening measure in the general population. The rarity of pathogenic variants in CRC-associated genes and the limited sensitivity of current testing strategies render general population testing potentially misleading and not cost-effective.
Rather detailed recommendations for surveillance in FAP and Lynch syndrome have been provided by several organizations representing various medical specialties and societies. These organizations include the following:
United States Multisociety (American Gastroenterological Association and American Society for Gastrointestinal Endoscopy) Task Force on Colorectal Cancer.[54]
American Society of Colon and Rectal Surgeons.[55]
The evidence bases for recommendations are generally included within the statements or guidelines. In many instances, these guidelines reflect expert opinion resting on studies that are rarely randomized prospective trials.
Early-onset CRC
The epidemiology of CRC with regard to age at diagnosis is shifting, with individuals increasingly being diagnosed before age 55 years,[1] often in the absence of polyposis and without a family history of CRC suggesting an inherited cancer syndrome.[58–60] (Refer to the PDQ summary on Colorectal Cancer Prevention for more information about CRC incidence trends in the general population.) One study that examined the prevalence of highly penetrant pathogenic variants in 450 individuals with early-onset CRC (mean age at diagnosis, 42.5 y) and a family history including at least one FDR with colon, endometrial, breast, ovarian, and/or pancreatic cancer identified 75 germline pathogenic or likely pathogenic variants in 72 patients (16%).[58] The spectrum of variants identified included Lynch syndrome and non-Lynch syndrome–associated genes, including several genes that have not traditionally been associated with CRC (e.g., BRCA1/BRCA2, ATM, CHEK2, PALB2, and CDKN2A). Given the high frequency and variety of hereditary cancer syndromes identified, the authors suggested that multigene (panel) testing in this population may be warranted.
In the absence of an additional family or personal history suggestive of Lynch syndrome, isolated cases of CRC diagnosed before age 36 years are uncommonly associated with MMR gene pathogenic variants. One study found MMR pathogenic variants in only 6.5% of such individuals,[59] whereas another study of patients with CRC younger than 50 years with no more than one FDR with CRC found abnormal microsatellite instability (MSI) in 21% of tumors and overrepresentation of defects in the PMS2 and MSH6 genes.[60] Therefore, isolated cases of very early-onset CRC in the absence of polyposis should be offered tumor screening with MSI/immunohistochemistry rather than proceeding directly to germline pathogenic variant analysis.
The use of polygenic risk scores (PRS) is being studied in the context of early-onset CRC in individuals who have tested negative for common CRC susceptibility variants (NCT02863107), with data from one large analysis [61] demonstrating that the predictive capacity of a 95-gene PRS may be particularly strong in assessing for CRC risk among young individuals (age, <50 y) who lack a family history of CRC in an FDR, and who would otherwise not be selected for early initiation of colonoscopic screening, by current practice.
Difficulties in Identifying a Family History of CRC Risk
The accuracy and completeness of family history data must be considered when using family history to assess individual risk in clinical practice and when identifying families appropriate for cancer research. A reported family history may be erroneous, or a person may be unaware of relatives with cancer.[62] Increased use of colonoscopy may result in fewer CRCs and more precancerous colon polyps in a family history. Individuals are much less likely to know about their family history of polyps (i.e., type of polyps and total number of polyps in their relatives) than they are to know about their family history of cancer. In addition, small family sizes and premature deaths may limit how informative a family history may be. Also, due to incomplete penetrance, some individuals may carry a genetic predisposition to CRC but do not develop cancer, giving the impression of skipped generations in a family tree.
Accuracy of patient-reported family history of colon cancer has been shown to be good, but it is not optimal. Patient report should be verified by obtaining medical records whenever possible, especially for reproductive tract cancers that may be relevant in identifying risk of Lynch syndrome and less reliably reported by some patients. (Refer to the Accuracy of the family history section in the PDQ summary on Cancer Genetics Risk Assessment and Counseling for more information.)
Several approaches are available to evaluate a patient with newly diagnosed CRC who may or may not be suspected of having a cancer genetics syndrome. The clinician may suspect a potential inherited disposition based on the family history and physical exam, and genetic tests are available to confirm these suspicions. The American College of Medical Genetics and Genomics has published guidelines for evaluating patients with suspected colon cancer susceptibility syndromes.[51] The guidelines aim to identify individuals whose clinical features warrant referral for genetics consultation. If an individual has multiple polyps (>20), depending on the histology, specific gene-directed testing can be a useful diagnostic tool. Similarly, if a patient’s clinical presentation is suspicious for Lynch syndrome, germline genetic testing can be directed towards this syndrome. However, diagnosis is more challenging when the clinical picture is less clear. Currently, tumor screening for Lynch syndrome is the most commonly accepted approach. However, increasingly, panels characterizing somatic variants in tumors are being utilized for a variety of clinical decisions.
A priori risk-assessment testing (which models risk based on a variety of factors, such as age at cancer onset and the spectrum of tumors in the family) may be an appropriate alternative in many cases. Application of such risk models does anticipate the use of multigene (panel) testing; however, their exact role remains to be established.
Molecular Events Associated With Colon Carcinogenesis
Much of our initial understanding of the molecular pathogenesis of CRC derived from rare hereditary CRC syndromes and revealed heterogeneity of CRC both molecularly and clinically. It is well accepted that most CRCs develop from adenomas. The transition from normal epithelium to adenoma to carcinoma is associated with acquired molecular events.[63–65] Presently, CRC can be separated into three categories based on similar molecular genetic features, suggesting divergent pathways of tumorigenesis: chromosomal instability (CIN), MSI, and CpG island methylator phenotype (CIMP). The understanding of the molecular genetic pathways of colorectal tumorigenesis is still evolving, and each new level of understanding has occurred in the context of the preceding level of knowledge. In addition, these pathways emerged from important clinical and histological heterogeneity of colorectal polyps and cancers. Thus, the introduction below captures the chronological evolution of our current understanding of colorectal tumorigenesis.
Chromosomal instability (CIN) pathway
Most CRCs develop through the CIN pathway. Key changes in CIN cancers include widespread alterations in chromosome number (aneuploidy) and frequent detectable losses at the molecular level of portions of chromosomes (loss of heterozygosity), such as 5q, 18q, and 17p; and pathogenic variants of the KRAS oncogene. The important genes involved in these chromosome losses are APC (5q), DCC/MADH2/MADH4 (18q), and TP53 (17p).[64,66] These chromosomal losses are indicative of genetic instability at the molecular and chromosomal levels.[65] Among the earliest and most common events in the colorectal tumor progression pathway is loss or pathogenic variant–inactivation of the APC gene. Pathogenic variant–inactivation of APC was first shown to be important to CRC in FAP, a hereditary CRC syndrome in which affected individuals harbor germline APC alterations, resulting in its loss of function and a dramatically increased incidence of colorectal polyps and cancers. Acquired or inherited pathogenic variants of DNA damage-repair genes, for example, base excision repair, nucleotide excision repair, double stranded repair, and MMR, also play a role in predisposing colorectal epithelial cells to pathogenic variants.
Microsatellite instability (MSI) pathway
Soon thereafter, a subset (10%–15%) of CRCs was identified that lacked evidence of chromosomal instability but exhibited aberrations in microsatellite repeat sequences,[67,68] a characteristic of tumors in patients with Lynch syndrome.[69] It was later found that hypermethylation of the MLH1 promoter is responsible for many sporadic CRCs with MSI. Germline variants in DNA MMR genes were discovered in patients with Lynch syndrome, whose CRCs frequently displayed MSI. Thus, the microsatellite instability pathway (MSI, sometimes referred to as MIN) was proposed.
The key characteristics of MSI cancers are that they have a largely intact chromosome complement and, as a result of defects in the DNA MMR system, more readily acquire pathogenic variants in important and often unique cancer-associated genes. These types of cancers are detectable at the molecular level by alterations in repeating units of DNA that occur normally throughout the genome, known as DNA microsatellites.
The rate of adenoma-to-carcinoma progression appears to be faster in microsatellite-unstable tumors than in microsatellite-stable tumors.[70] The foundation for this is the repeated reports of interval cancers in patients with recent, normal colonoscopy. Further support for this is seen in the serrated pathway (see below), in which high rates of interval cancer have also been observed.[71,72] Characteristic histological changes, such as increased mucin production, can be seen in tumors that demonstrate MSI, intratumoral T lymphocyte infiltration/Crohn-like reaction, etc., distinguishing the colorectal tumors in this pathway.
The knowledge derived from the study of inherited CRC syndromes has provided important clues regarding the molecular events that mediate tumor initiation and tumor progression in people without germline abnormalities. Among the earliest events in the colorectal tumor progression pathway (both MSI and CIN) is loss of function of the APC gene product.
CpG island methylator phenotype (CIMP) and the serrated polyposis pathway
Beginning in the 1980s, studies began reporting an increased risk of CRC in patients with hyperplastic polyposis syndrome (HPS), now referred to as serrated polyposis syndrome (SPS).[6,7,73–78] Only a minority of SPS appear to be familial, but no common germline variant has been identified in these families to date. A comparison of the hyperplastic polyps (HPs) found in SPS patients and controls revealed that SPS polyps are histologically distinct and are similar to previously described serrated adenomas, polyps with features of HPs and adenomatous polyps (APs).[79] This led to observations that these sessile serrated adenomas (SSA) tend to occur in the right colon, where they are frequently large and sessile, and exhibit increased proliferation, dilation and serration of the crypt bases, decreased endocrine cells, and lack of dysplasia.[80]
Further histological characterization of serrated polyps led to subtypes: traditional serrated adenomas (TSA), mixed serrated polyps (MP), and more recently, sessile serrated adenoma/sessile serrated polyp (SSA/SSP).[81] TSAs are characterized by a protuberant morphology, ectopic crypt formation (suggestive of deficient bone morphogenetic protein signaling), and villiform and dysplastic histopathology.[80,82] TSAs are not simply SSAs with dysplasia, and evidence that SSAs are precursors of TSAs is lacking. MPs have overlapping features of HPs, SSAs, and TSAs.
In colonoscopy screening studies, large serrated polyps were strongly and independently associated with the development of advanced colorectal neoplasms, while left-sided HPs were not. The term SSA has been a concern to clinicians as these characteristically lack nuclear atypia, the traditional hallmark of adenomas, but rather are termed adenomas due to other architectural features. The classification of SSA is supported by the knowledge that the molecular characteristics denote an increased cancer risk.[79,83,84]
While APs in Lynch syndrome patients can exhibit MSI, sporadic adenomas rarely do. However, serrated polyps with dysplasia can exhibit MSI with hypermethylation of the MLH1 promoter. Large (>1 cm) serrated polyps carry greater cancer risk than do conventional hyperplastic polyps and, when developing into cancers, characteristically exhibit MSI.[82,85–87] In a review of resected serrated polyps with a malignant focus, all of the polyps originated in the right colon and were SSAs.[85] The malignant foci were MSI and demonstrated loss of MLH1 immunoreactivity, suggesting an association between SSAs and sporadic MSI colon cancers.
The MSI seen in sporadic CRCs is due to hypermethylation of the promoter of MLH1, which abrogates its expression. As promoter regions of other tumor suppressor genes were “silenced” through hypermethylation, cancer genome studies of CRC ensued. These showed a consistent pattern of hypermethylation in the evaluated genes in approximately 50% of CRCs.[88] Studies of larger numbers of unselected CRC patients show that a minority of CRCs (20%–30%) demonstrate CIMP, defined as hypermethylation of two or more of the CpG islands in MINT1, MINT2, MINT31, CDKN2A (p16), and MLH1.[89,90] The term CIMP was coined to classify these cancers, which shared clinical features. Early attempts to differentiate CIMP-positive and CIMP-negative CRCs were unsuccessful.[91] However, subsequent studies using unbiased hierarchical cluster analysis of heavily methylated genes in CRCs and a population-based study design successfully identified unique clinical and molecular characteristics supporting a CIMP pathway.[88,92]
CIMP-high CRCs were much more likely (82.1%; P < .0001) to express MSI than were microsatellite-stable CRCs (24.4%; P < .0001).[88] In one study, microsatellite-stable, CIMP-high (>2 CIMP markers mentioned above) colorectal tumors were significantly more associated with BRAF V600E variants, KRAS2 variants, proximal site, higher American Joint Committee on Cancer stage, older patient age, poor differentiation, and mucinous histology than were CIMP-low (<2 CIMP markers mentioned above) colorectal tumors.[88] Microsatellite-unstable, CIMP-high colorectal tumors were significantly more associated with BRAF V600E pathogenic variants, proximal site, older patient age, and absence of KRAS2 pathogenic variants than were microsatellite unstable, CIMP-low tumors.[88] There was a significantly greater presence of BRAF V600E pathogenic variants in CIMP-high colorectal tumors regardless of MSI.[88] Thus, unlike a previous study that questioned the biological significance of CIMP once unstable colorectal tumors were excluded,[91] this study demonstrated several clinicopathologic variables were indeed associated with CIMP in microsatellite-stable and microsatellite-unstable colorectal tumors.[88]
Studies of polyps revealed CIMP-positive polyps in SPS patients and most frequently in right-sided SSAs.[72,93–96] More recently, a hotspot BRAF pathogenic variant (V600E) was found to be common in MSI colon cancers and serrated polyps.[97–99] A BRAF pathogenic variant is absent in CRCs from Lynch syndrome patients and is rare in sporadic adenomatous colorectal polyps, but it is present in the vast majority of serrated polyps, especially SSAs.[94,96,100–102] CIMP positivity is commonly found in microvesicular hyperplastic polyps (MVHP), suggesting progression of MVHP to SSA and then to colon cancer.[94]
Conclusion
The characterization of CIMP CRCs and evidence that MSI occurs later in the adenoma-carcinoma sequence leads to modification of the previous colorectal tumorigenesis model, which was comprised of two pathways: MSI (MIN) and CIN. There is much overlap between the MSI and CIMP pathways. At the heart of the CIMP pathway are serrated polyps harboring BRAF pathogenic variants. The CIN pathway is characterized by AP precursors of which the vast majority harbor APC pathogenic variants that occur early in the pathway.
References
American Cancer Society: Cancer Facts and Figures 2024. American Cancer Society, 2024. Available online. Last accessed December 30, 2024.
Kanth P, Grimmett J, Champine M, et al.: Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management. Am J Gastroenterol 112 (10): 1509-1525, 2017. [PUBMED Abstract]
Lynch HT, Smyrk TC, Watson P, et al.: Genetics, natural history, tumor spectrum, and pathology of hereditary nonpolyposis colorectal cancer: an updated review. Gastroenterology 104 (5): 1535-49, 1993. [PUBMED Abstract]
Rustgi AK: The genetics of hereditary colon cancer. Genes Dev 21 (20): 2525-38, 2007. [PUBMED Abstract]
Howe JR, Mitros FA, Summers RW: The risk of gastrointestinal carcinoma in familial juvenile polyposis. Ann Surg Oncol 5 (8): 751-6, 1998. [PUBMED Abstract]
Jeevaratnam P, Cottier DS, Browett PJ, et al.: Familial giant hyperplastic polyposis predisposing to colorectal cancer: a new hereditary bowel cancer syndrome. J Pathol 179 (1): 20-5, 1996. [PUBMED Abstract]
Rashid A, Houlihan PS, Booker S, et al.: Phenotypic and molecular characteristics of hyperplastic polyposis. Gastroenterology 119 (2): 323-32, 2000. [PUBMED Abstract]
Shinya H, Wolff WI: Morphology, anatomic distribution and cancer potential of colonic polyps. Ann Surg 190 (6): 679-83, 1979. [PUBMED Abstract]
Fenoglio CM, Lane N: The anatomical precursor of colorectal carcinoma. Cancer 34 (3): suppl:819-23, 1974. [PUBMED Abstract]
Morson B: President’s address. The polyp-cancer sequence in the large bowel. Proc R Soc Med 67 (6): 451-7, 1974. [PUBMED Abstract]
Muto T, Bussey HJ, Morson BC: The evolution of cancer of the colon and rectum. Cancer 36 (6): 2251-70, 1975. [PUBMED Abstract]
Stryker SJ, Wolff BG, Culp CE, et al.: Natural history of untreated colonic polyps. Gastroenterology 93 (5): 1009-13, 1987. [PUBMED Abstract]
O’Brien MJ, Winawer SJ, Zauber AG, et al.: The National Polyp Study. Patient and polyp characteristics associated with high-grade dysplasia in colorectal adenomas. Gastroenterology 98 (2): 371-9, 1990. [PUBMED Abstract]
Winawer SJ, Stewart ET, Zauber AG, et al.: A comparison of colonoscopy and double-contrast barium enema for surveillance after polypectomy. National Polyp Study Work Group. N Engl J Med 342 (24): 1766-72, 2000. [PUBMED Abstract]
Winawer SJ, Zauber AG, Ho MN, et al.: Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 329 (27): 1977-81, 1993. [PUBMED Abstract]
Müller AD, Sonnenberg A: Prevention of colorectal cancer by flexible endoscopy and polypectomy. A case-control study of 32,702 veterans. Ann Intern Med 123 (12): 904-10, 1995. [PUBMED Abstract]
O’brien MJ, Winawer SJ, Zauber AG, et al.: Flat adenomas in the National Polyp Study: is there increased risk for high-grade dysplasia initially or during surveillance? Clin Gastroenterol Hepatol 2 (10): 905-11, 2004. [PUBMED Abstract]
Zauber AG, O’Brien MJ, Winawer SJ: On finding flat adenomas: is the search worth the gain? Gastroenterology 122 (3): 839-40, 2002. [PUBMED Abstract]
Rembacken BJ, Fujii T, Cairns A, et al.: Flat and depressed colonic neoplasms: a prospective study of 1000 colonoscopies in the UK. Lancet 355 (9211): 1211-4, 2000. [PUBMED Abstract]
Woolf CM: A genetic study of carcinoma of the large intestine. Am J Hum Genet 10 (1): 42-7, 1958. [PUBMED Abstract]
Fuchs CS, Giovannucci EL, Colditz GA, et al.: A prospective study of family history and the risk of colorectal cancer. N Engl J Med 331 (25): 1669-74, 1994. [PUBMED Abstract]
Slattery ML, Kerber RA: Family history of cancer and colon cancer risk: the Utah Population Database. J Natl Cancer Inst 86 (21): 1618-26, 1994. [PUBMED Abstract]
Negri E, Braga C, La Vecchia C, et al.: Family history of cancer and risk of colorectal cancer in Italy. Br J Cancer 77 (1): 174-9, 1998. [PUBMED Abstract]
St John DJ, McDermott FT, Hopper JL, et al.: Cancer risk in relatives of patients with common colorectal cancer. Ann Intern Med 118 (10): 785-90, 1993. [PUBMED Abstract]
Duncan JL, Kyle J: Family incidence of carcinoma of the colon and rectum in north-east Scotland. Gut 23 (2): 169-71, 1982. [PUBMED Abstract]
Rozen P, Fireman Z, Figer A, et al.: Family history of colorectal cancer as a marker of potential malignancy within a screening program. Cancer 60 (2): 248-54, 1987. [PUBMED Abstract]
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Cottet V, Pariente A, Nalet B, et al.: Colonoscopic screening of first-degree relatives of patients with large adenomas: increased risk of colorectal tumors. Gastroenterology 133 (4): 1086-92, 2007. [PUBMED Abstract]
Winawer SJ, Zauber AG, Gerdes H, et al.: Risk of colorectal cancer in the families of patients with adenomatous polyps. National Polyp Study Workgroup. N Engl J Med 334 (2): 82-7, 1996. [PUBMED Abstract]
Ahsan H, Neugut AI, Garbowski GC, et al.: Family history of colorectal adenomatous polyps and increased risk for colorectal cancer. Ann Intern Med 128 (11): 900-5, 1998. [PUBMED Abstract]
Win AK, Macinnis RJ, Hopper JL, et al.: Risk prediction models for colorectal cancer: a review. Cancer Epidemiol Biomarkers Prev 21 (3): 398-410, 2012. [PUBMED Abstract]
Chen S, Wang W, Lee S, et al.: Prediction of germline mutations and cancer risk in the Lynch syndrome. JAMA 296 (12): 1479-87, 2006. [PUBMED Abstract]
Balmaña J, Stockwell DH, Steyerberg EW, et al.: Prediction of MLH1 and MSH2 mutations in Lynch syndrome. JAMA 296 (12): 1469-78, 2006. [PUBMED Abstract]
Barnetson RA, Tenesa A, Farrington SM, et al.: Identification and survival of carriers of mutations in DNA mismatch-repair genes in colon cancer. N Engl J Med 354 (26): 2751-63, 2006. [PUBMED Abstract]
Burt RW, Petersen GM: Familial colorectal cancer: diagnosis and management. In: Young GP, Rozen P, Levin B, eds.: Prevention and Early Detection of Colorectal Cancer. WB Saunders, 1996, pp 171-194.
Mork ME, You YN, Ying J, et al.: High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults With Colorectal Cancer. J Clin Oncol 33 (31): 3544-9, 2015. [PUBMED Abstract]
Kinzler KW, Nilbert MC, Su LK, et al.: Identification of FAP locus genes from chromosome 5q21. Science 253 (5020): 661-5, 1991. [PUBMED Abstract]
Groden J, Thliveris A, Samowitz W, et al.: Identification and characterization of the familial adenomatous polyposis coli gene. Cell 66 (3): 589-600, 1991. [PUBMED Abstract]
Leppert M, Burt R, Hughes JP, et al.: Genetic analysis of an inherited predisposition to colon cancer in a family with a variable number of adenomatous polyps. N Engl J Med 322 (13): 904-8, 1990. [PUBMED Abstract]
Spirio L, Olschwang S, Groden J, et al.: Alleles of the APC gene: an attenuated form of familial polyposis. Cell 75 (5): 951-7, 1993. [PUBMED Abstract]
Brensinger JD, Laken SJ, Luce MC, et al.: Variable phenotype of familial adenomatous polyposis in pedigrees with 3′ mutation in the APC gene. Gut 43 (4): 548-52, 1998. [PUBMED Abstract]
Soravia C, Berk T, Madlensky L, et al.: Genotype-phenotype correlations in attenuated adenomatous polyposis coli. Am J Hum Genet 62 (6): 1290-301, 1998. [PUBMED Abstract]
Pedemonte S, Sciallero S, Gismondi V, et al.: Novel germline APC variants in patients with multiple adenomas. Genes Chromosomes Cancer 22 (4): 257-67, 1998. [PUBMED Abstract]
Sieber OM, Lamlum H, Crabtree MD, et al.: Whole-gene APC deletions cause classical familial adenomatous polyposis, but not attenuated polyposis or “multiple” colorectal adenomas. Proc Natl Acad Sci U S A 99 (5): 2954-8, 2002. [PUBMED Abstract]
Leach FS, Nicolaides NC, Papadopoulos N, et al.: Mutations of a mutS homolog in hereditary nonpolyposis colorectal cancer. Cell 75 (6): 1215-25, 1993. [PUBMED Abstract]
Papadopoulos N, Nicolaides NC, Wei YF, et al.: Mutation of a mutL homolog in hereditary colon cancer. Science 263 (5153): 1625-9, 1994. [PUBMED Abstract]
Nicolaides NC, Papadopoulos N, Liu B, et al.: Mutations of two PMS homologues in hereditary nonpolyposis colon cancer. Nature 371 (6492): 75-80, 1994. [PUBMED Abstract]
Miyaki M, Konishi M, Tanaka K, et al.: Germline mutation of MSH6 as the cause of hereditary nonpolyposis colorectal cancer. Nat Genet 17 (3): 271-2, 1997. [PUBMED Abstract]
Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015. [PUBMED Abstract]
Bashford MT, Kohlman W, Everett J, et al.: Addendum: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 21 (12): 2844, 2019. [PUBMED Abstract]
Smith RA, Cokkinides V, Eyre HJ: American Cancer Society guidelines for the early detection of cancer, 2006. CA Cancer J Clin 56 (1): 11-25; quiz 49-50, 2006 Jan-Feb. [PUBMED Abstract]
Winawer S, Fletcher R, Rex D, et al.: Colorectal cancer screening and surveillance: clinical guidelines and rationale-Update based on new evidence. Gastroenterology 124 (2): 544-60, 2003. [PUBMED Abstract]
Church J, Simmang C; Standards Task Force, et al.: Practice parameters for the treatment of patients with dominantly inherited colorectal cancer (familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer). Dis Colon Rectum 46 (8): 1001-12, 2003. [PUBMED Abstract]
National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal, Endometrial, and Gastric. Version 3.2024. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2024. Available with free registration. Last accessed December 13, 2024.
Syngal S, Brand RE, Church JM, et al.: ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol 110 (2): 223-62; quiz 263, 2015. [PUBMED Abstract]
Pearlman R, Frankel WL, Swanson B, et al.: Prevalence and Spectrum of Germline Cancer Susceptibility Gene Mutations Among Patients With Early-Onset Colorectal Cancer. JAMA Oncol 3 (4): 464-471, 2017. [PUBMED Abstract]
Jasperson KW, Vu TM, Schwab AL, et al.: Evaluating Lynch syndrome in very early onset colorectal cancer probands without apparent polyposis. Fam Cancer 9 (2): 99-107, 2010. [PUBMED Abstract]
Goel A, Nagasaka T, Spiegel J, et al.: Low frequency of Lynch syndrome among young patients with non-familial colorectal cancer. Clin Gastroenterol Hepatol 8 (11): 966-71, 2010. [PUBMED Abstract]
Archambault AN, Su YR, Jeon J, et al.: Cumulative Burden of Colorectal Cancer-Associated Genetic Variants Is More Strongly Associated With Early-Onset vs Late-Onset Cancer. Gastroenterology 158 (5): 1274-1286.e12, 2020. [PUBMED Abstract]
Glanz K, Grove J, Le Marchand L, et al.: Underreporting of family history of colon cancer: correlates and implications. Cancer Epidemiol Biomarkers Prev 8 (7): 635-9, 1999. [PUBMED Abstract]
Fearon ER, Vogelstein B: A genetic model for colorectal tumorigenesis. Cell 61 (5): 759-67, 1990. [PUBMED Abstract]
Vogelstein B, Kinzler KW: The multistep nature of cancer. Trends Genet 9 (4): 138-41, 1993. [PUBMED Abstract]
Lengauer C, Kinzler KW, Vogelstein B: Genetic instabilities in human cancers. Nature 396 (6712): 643-9, 1998. [PUBMED Abstract]
Kinzler KW, Vogelstein B: Colorectal tumors. In: Vogelstein B, Kinzler KW, eds.: The Genetic Basis of Human Cancer. 2nd ed. McGraw-Hill, 2002, pp 583-612.
Thibodeau SN, Bren G, Schaid D: Microsatellite instability in cancer of the proximal colon. Science 260 (5109): 816-9, 1993. [PUBMED Abstract]
Ionov Y, Peinado MA, Malkhosyan S, et al.: Ubiquitous somatic mutations in simple repeated sequences reveal a new mechanism for colonic carcinogenesis. Nature 363 (6429): 558-61, 1993. [PUBMED Abstract]
Peltomäki P, Lothe RA, Aaltonen LA, et al.: Microsatellite instability is associated with tumors that characterize the hereditary non-polyposis colorectal carcinoma syndrome. Cancer Res 53 (24): 5853-5, 1993. [PUBMED Abstract]
Jass JR, Cottier DS, Pokos V, et al.: Mixed epithelial polyps in association with hereditary non-polyposis colorectal cancer providing an alternative pathway of cancer histogenesis. Pathology 29 (1): 28-33, 1997. [PUBMED Abstract]
Jass JR: Serrated route to colorectal cancer: back street or super highway? J Pathol 193 (3): 283-5, 2001. [PUBMED Abstract]
Wynter CV, Walsh MD, Higuchi T, et al.: Methylation patterns define two types of hyperplastic polyp associated with colorectal cancer. Gut 53 (4): 573-80, 2004. [PUBMED Abstract]
Bengoechea O, Martínez-Peñuela JM, Larrínaga B, et al.: Hyperplastic polyposis of the colorectum and adenocarcinoma in a 24-year-old man. Am J Surg Pathol 11 (4): 323-7, 1987. [PUBMED Abstract]
Hyman NH, Anderson P, Blasyk H: Hyperplastic polyposis and the risk of colorectal cancer. Dis Colon Rectum 47 (12): 2101-4, 2004. [PUBMED Abstract]
Leggett BA, Devereaux B, Biden K, et al.: Hyperplastic polyposis: association with colorectal cancer. Am J Surg Pathol 25 (2): 177-84, 2001. [PUBMED Abstract]
McCann BG: A case of metaplastic polyposis of the colon associated with focal adenomatous change and metachronous adenocarcinomas. Histopathology 13 (6): 700-2, 1988. [PUBMED Abstract]
Place RJ, Simmang CL: Hyperplastic-adenomatous polyposis syndrome. J Am Coll Surg 188 (5): 503-7, 1999. [PUBMED Abstract]
Koide N, Saito Y, Fujii T, et al.: A case of hyperplastic polyposis of the colon with adenocarcinomas in hyperplastic polyps after long-term follow-up. Endoscopy 34 (6): 499-502, 2002. [PUBMED Abstract]
Torlakovic E, Snover DC: Serrated adenomatous polyposis in humans. Gastroenterology 110 (3): 748-55, 1996. [PUBMED Abstract]
Torlakovic EE, Gomez JD, Driman DK, et al.: Sessile serrated adenoma (SSA) vs. traditional serrated adenoma (TSA). Am J Surg Pathol 32 (1): 21-9, 2008. [PUBMED Abstract]
Snover DC, Jass JR, Fenoglio-Preiser C, et al.: Serrated polyps of the large intestine: a morphologic and molecular review of an evolving concept. Am J Clin Pathol 124 (3): 380-91, 2005. [PUBMED Abstract]
Lash RH, Genta RM, Schuler CM: Sessile serrated adenomas: prevalence of dysplasia and carcinoma in 2139 patients. J Clin Pathol 63 (8): 681-6, 2010. [PUBMED Abstract]
Torlakovic E, Skovlund E, Snover DC, et al.: Morphologic reappraisal of serrated colorectal polyps. Am J Surg Pathol 27 (1): 65-81, 2003. [PUBMED Abstract]
Jass JR, Baker K, Zlobec I, et al.: Advanced colorectal polyps with the molecular and morphological features of serrated polyps and adenomas: concept of a ‘fusion’ pathway to colorectal cancer. Histopathology 49 (2): 121-31, 2006. [PUBMED Abstract]
Goldstein NS: Small colonic microsatellite unstable adenocarcinomas and high-grade epithelial dysplasias in sessile serrated adenoma polypectomy specimens: a study of eight cases. Am J Clin Pathol 125 (1): 132-45, 2006. [PUBMED Abstract]
Lu FI, van Niekerk de W, Owen D, et al.: Longitudinal outcome study of sessile serrated adenomas of the colorectum: an increased risk for subsequent right-sided colorectal carcinoma. Am J Surg Pathol 34 (7): 927-34, 2010. [PUBMED Abstract]
Schreiner MA, Weiss DG, Lieberman DA: Proximal and large hyperplastic and nondysplastic serrated polyps detected by colonoscopy are associated with neoplasia. Gastroenterology 139 (5): 1497-502, 2010. [PUBMED Abstract]
Toyota M, Ahuja N, Ohe-Toyota M, et al.: CpG island methylator phenotype in colorectal cancer. Proc Natl Acad Sci U S A 96 (15): 8681-6, 1999. [PUBMED Abstract]
Ahuja N, Mohan AL, Li Q, et al.: Association between CpG island methylation and microsatellite instability in colorectal cancer. Cancer Res 57 (16): 3370-4, 1997. [PUBMED Abstract]
Samowitz WS, Albertsen H, Herrick J, et al.: Evaluation of a large, population-based sample supports a CpG island methylator phenotype in colon cancer. Gastroenterology 129 (3): 837-45, 2005. [PUBMED Abstract]
Yamashita K, Dai T, Dai Y, et al.: Genetics supersedes epigenetics in colon cancer phenotype. Cancer Cell 4 (2): 121-31, 2003. [PUBMED Abstract]
Weisenberger DJ, Siegmund KD, Campan M, et al.: CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat Genet 38 (7): 787-93, 2006. [PUBMED Abstract]
Chan AO, Issa JP, Morris JS, et al.: Concordant CpG island methylation in hyperplastic polyposis. Am J Pathol 160 (2): 529-36, 2002. [PUBMED Abstract]
Kambara T, Simms LA, Whitehall VL, et al.: BRAF mutation is associated with DNA methylation in serrated polyps and cancers of the colorectum. Gut 53 (8): 1137-44, 2004. [PUBMED Abstract]
O’Brien MJ, Yang S, Clebanoff JL, et al.: Hyperplastic (serrated) polyps of the colorectum: relationship of CpG island methylator phenotype and K-ras mutation to location and histologic subtype. Am J Surg Pathol 28 (4): 423-34, 2004. [PUBMED Abstract]
Yang S, Farraye FA, Mack C, et al.: BRAF and KRAS Mutations in hyperplastic polyps and serrated adenomas of the colorectum: relationship to histology and CpG island methylation status. Am J Surg Pathol 28 (11): 1452-9, 2004. [PUBMED Abstract]
Chan TL, Zhao W, Leung SY, et al.: BRAF and KRAS mutations in colorectal hyperplastic polyps and serrated adenomas. Cancer Res 63 (16): 4878-81, 2003. [PUBMED Abstract]
Rajagopalan H, Bardelli A, Lengauer C, et al.: Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature 418 (6901): 934, 2002. [PUBMED Abstract]
Yuen ST, Davies H, Chan TL, et al.: Similarity of the phenotypic patterns associated with BRAF and KRAS mutations in colorectal neoplasia. Cancer Res 62 (22): 6451-5, 2002. [PUBMED Abstract]
Deng G, Bell I, Crawley S, et al.: BRAF mutation is frequently present in sporadic colorectal cancer with methylated hMLH1, but not in hereditary nonpolyposis colorectal cancer. Clin Cancer Res 10 (1 Pt 1): 191-5, 2004. [PUBMED Abstract]
McGivern A, Wynter CV, Whitehall VL, et al.: Promoter hypermethylation frequency and BRAF mutations distinguish hereditary non-polyposis colon cancer from sporadic MSI-H colon cancer. Fam Cancer 3 (2): 101-7, 2004. [PUBMED Abstract]
Wang L, Cunningham JM, Winters JL, et al.: BRAF mutations in colon cancer are not likely attributable to defective DNA mismatch repair. Cancer Res 63 (17): 5209-12, 2003. [PUBMED Abstract]
Colorectal Cancer Susceptibility Genes
Major Genes
Major genes are defined as those that are necessary and sufficient for disease causation, with important pathogenic variants (e.g., nonsense, missense, frameshift) of the gene as causal mechanisms. Major genes are typically considered those that are involved in single-gene disorders, and the diseases caused by major genes are often relatively rare. Most pathogenic variants in major genes lead to a very high risk of disease, and environmental contributions are often difficult to recognize.[1] Historically, most major colon cancer susceptibility genes have been identified by linkage analysis using high-risk families; thus, these criteria were fulfilled by definition, as a consequence of the study design.
The functions of the major colorectal (CRC) cancer genes have been reasonably well characterized over the past decade.[2] Tumor suppressor genes constitute the most important class of genes responsible for hereditary cancer syndromes and represent the class of genes responsible for familial adenomatous polyposis (FAP), Lynch syndrome, and juvenile polyposis syndrome (JPS), among others. Table 2 summarizes the genes that confer a substantial risk of CRC, with their corresponding diseases.
Table 2. Genes Associated with a High Susceptibility of Colorectal Cancer
Until the 1990s, the diagnosis of genetically inherited polyposis syndromes was based on clinical manifestations and family history. Now that some of the genes involved in these syndromes have been identified, a few studies have attempted to estimate the spontaneous pathogenic variant rate (de novo pathogenic variant rate) in these populations. Interestingly, FAP, JPS, Peutz-Jeghers syndrome, Cowden syndrome, and Bannayan-Riley-Ruvalcaba syndrome are all thought to have high rates of spontaneous pathogenic variants, in the 25% to 30% range,[3–5] while estimates of de novo pathogenic variants in the MMR genes associated with Lynch syndrome are thought to be low, in the 0.9% to 5% range.[6–8] These estimates of spontaneous pathogenic variant rates in Lynch syndrome seem to overlap with the estimates of nonpaternity rates in various populations (0.6% to 3.3%),[9–11] making the de novo pathogenic variant rate for Lynch syndrome seem quite low in contrast to the relatively high rates in the other polyposis syndromes.
Genetic Polymorphisms and CRC Risk
It is widely acknowledged that the familial clustering of colon cancer also occurs outside of the setting of well-characterized colon cancer family syndromes.[12] Based on epidemiological studies, the risk of colon cancer in a first-degree relative (FDR) of an affected individual can increase an individual’s lifetime risk of colon cancer 2-fold to 4.3-fold.[13] The relative risk (RR) and absolute risk of CRC for different family history categories is estimated in Table 1. In addition, the lifetime risk of colon cancer also increases in FDRs of individuals with colon adenomas.[14] The magnitude of risk depends on the age at diagnosis of the index case, the degree of relatedness of the index case to the at-risk case, and the number of affected relatives. It is currently believed that many of the moderate- and low-risk cases are influenced by alterations in single low-penetrance genes or combinations of low-penetrance genes.[15] Given the public health impact of identifying the etiology of this increased risk, an intense search for the responsible genes is under way.
Each locus would be expected to have a relatively small effect on CRC risk and would not produce the dramatic familial aggregation seen in Lynch syndrome or FAP. However, in combination with other common genetic loci and/or environmental factors, variants of this kind might significantly alter CRC risk. These types of genetic variations are often referred to as polymorphisms. Most loci that are polymorphic have no influence on disease risk or human traits (benign polymorphisms), while those that are associated with a difference in risk of disease or a human trait (however subtle) are sometimes termed disease-associated polymorphisms or functionally relevant polymorphisms. When such variation involves changes in single nucleotides of DNA they are referred to as single nucleotide variants (SNVs).
Several genome-wide association studies (GWAS) have been conducted with relatively large, unselected series of patients with CRC, who have been evaluated for patterns of polymorphisms in candidate and anonymous genes throughout the genome.[16–19] The use of genome-wide scans in thousands of CRC cases and controls has led to the discovery of multiple common, low-risk CRC SNVs, which can be found in the National Human Genome Research Institute GWAS catalog. For more information on GWAS, see Cancer Genetics Overview.
A goal of these studies has been to identify SNVs that may confer mildly increased CRC risks. This risk stratification could potentially enhance usability of CRC screening by influencing patient decision making regarding the ages to begin/end CRC screening and the amount of time between screening studies. There is increasing interest about using SNVs to expand germline risk assessment. This could be expanded from only searching for monogenic forms of CRC predisposition with high-/moderate-penetrance to searching for forms of CRC predisposition with polygenic risk, which may have broader applicability in the general population. Additionally, multiple studies have examined if polygenic risk scores (PRS) can be used to personalize CRC risk assessment in individuals with average risk of developing CRC.[20,21] While the growing body of data on CRC risk SNVs and PRS have been promising, PRS are not currently used in routine clinical settings and are not considered clinically actionable to guide the use of CRC screening procedures. Formal implementation studies are warranted to analyze how PRS can guide CRC risk assessment and screening in routine clinical care.
APC I1307K
The APC I1307K polymorphism deserves special mention, given that it is commonly identified in individuals of Ashkenazi Jewish ancestry undergoing multigene (panel) testing [22,23] and is associated with an increased risk of CRC; however, it does not cause colonic polyposis. The I1307K polymorphism occurs almost exclusively in people of Ashkenazi Jewish descent and results in a twofold increased risk of colonic adenomas and adenocarcinomas compared with the general population.[24,25] The I1307K polymorphism results from a transition from T to A at nucleotide 3920 in the APC gene and appears to create a region of hypermutability by virtue of the fact that this results in an A8 microsatellite coding sequence.[24] Although clinical assays to assess for the APC I1307K polymorphism are currently available, the associated CRC risk is not high enough to support their routine use. Based on currently available data, it is not yet known whether the I1307K carrier status should guide decisions regarding the age to initiate screening, the frequency of screening, or the choice of screening strategy.
References
Caporaso N, Goldstein A: Cancer genes: single and susceptibility: exposing the difference. Pharmacogenetics 5 (2): 59-63, 1995. [PUBMED Abstract]
Vogelstein B, Kinzler KW: Cancer genes and the pathways they control. Nat Med 10 (8): 789-99, 2004. [PUBMED Abstract]
Aretz S, Uhlhaas S, Caspari R, et al.: Frequency and parental origin of de novo APC mutations in familial adenomatous polyposis. Eur J Hum Genet 12 (1): 52-8, 2004. [PUBMED Abstract]
Westerman AM, Entius MM, Boor PP, et al.: Novel mutations in the LKB1/STK11 gene in Dutch Peutz-Jeghers families. Hum Mutat 13 (6): 476-81, 1999. [PUBMED Abstract]
Schreibman IR, Baker M, Amos C, et al.: The hamartomatous polyposis syndromes: a clinical and molecular review. Am J Gastroenterol 100 (2): 476-90, 2005. [PUBMED Abstract]
Morak M, Laner A, Scholz M, et al.: Report on de-novo mutation in the MSH2 gene as a rare event in hereditary nonpolyposis colorectal cancer. Eur J Gastroenterol Hepatol 20 (11): 1101-5, 2008. [PUBMED Abstract]
Plasilova M, Zhang J, Okhowat R, et al.: A de novo MLH1 germ line mutation in a 31-year-old colorectal cancer patient. Genes Chromosomes Cancer 45 (12): 1106-10, 2006. [PUBMED Abstract]
Win AK, Jenkins MA, Buchanan DD, et al.: Determining the frequency of de novo germline mutations in DNA mismatch repair genes. J Med Genet 48 (8): 530-4, 2011. [PUBMED Abstract]
Anderson KG: How well does paternity confidence match actual paternity? Evidence from worldwide nonpaternity rates. Curr Anthropol 47 (3): 513-20, 2006. Also available online. Last accessed May 13, 2025.
Sasse G, Müller H, Chakraborty R, et al.: Estimating the frequency of nonpaternity in Switzerland. Hum Hered 44 (6): 337-43, 1994 Nov-Dec. [PUBMED Abstract]
Voracek M, Haubner T, Fisher ML: Recent decline in nonpaternity rates: a cross-temporal meta-analysis. Psychol Rep 103 (3): 799-811, 2008. [PUBMED Abstract]
Burt RW, Bishop DT, Lynch HT, et al.: Risk and surveillance of individuals with heritable factors for colorectal cancer. WHO Collaborating Centre for the Prevention of Colorectal Cancer. Bull World Health Organ 68 (5): 655-65, 1990. [PUBMED Abstract]
Butterworth AS, Higgins JP, Pharoah P: Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer 42 (2): 216-27, 2006. [PUBMED Abstract]
Johns LE, Houlston RS: A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96 (10): 2992-3003, 2001. [PUBMED Abstract]
Wei C, Peng B, Han Y, et al.: Mutations of HNRNPA0 and WIF1 predispose members of a large family to multiple cancers. Fam Cancer 14 (2): 297-306, 2015. [PUBMED Abstract]
Houlston RS, Webb E, Broderick P, et al.: Meta-analysis of genome-wide association data identifies four new susceptibility loci for colorectal cancer. Nat Genet 40 (12): 1426-35, 2008. [PUBMED Abstract]
Houlston RS, Cheadle J, Dobbins SE, et al.: Meta-analysis of three genome-wide association studies identifies susceptibility loci for colorectal cancer at 1q41, 3q26.2, 12q13.13 and 20q13.33. Nat Genet 42 (11): 973-7, 2010. [PUBMED Abstract]
Whiffin N, Hosking FJ, Farrington SM, et al.: Identification of susceptibility loci for colorectal cancer in a genome-wide meta-analysis. Hum Mol Genet 23 (17): 4729-37, 2014. [PUBMED Abstract]
Peters U, Jiao S, Schumacher FR, et al.: Identification of Genetic Susceptibility Loci for Colorectal Tumors in a Genome-Wide Meta-analysis. Gastroenterology 144 (4): 799-807.e24, 2013. [PUBMED Abstract]
Kastrinos F, Kupfer SS, Gupta S: Colorectal Cancer Risk Assessment and Precision Approaches to Screening: Brave New World or Worlds Apart? Gastroenterology 164 (5): 812-827, 2023. [PUBMED Abstract]
Sassano M, Mariani M, Quaranta G, et al.: Polygenic risk prediction models for colorectal cancer: a systematic review. BMC Cancer 22 (1): 65, 2022. [PUBMED Abstract]
Pearlman R, Frankel WL, Swanson B, et al.: Prevalence and Spectrum of Germline Cancer Susceptibility Gene Mutations Among Patients With Early-Onset Colorectal Cancer. JAMA Oncol 3 (4): 464-471, 2017. [PUBMED Abstract]
Boursi B, Sella T, Liberman E, et al.: The APC p.I1307K polymorphism is a significant risk factor for CRC in average risk Ashkenazi Jews. Eur J Cancer 49 (17): 3680-5, 2013. [PUBMED Abstract]
Laken SJ, Petersen GM, Gruber SB, et al.: Familial colorectal cancer in Ashkenazim due to a hypermutable tract in APC. Nat Genet 17 (1): 79-83, 1997. [PUBMED Abstract]
Lothe RA, Hektoen M, Johnsen H, et al.: The APC gene I1307K variant is rare in Norwegian patients with familial and sporadic colorectal or breast cancer. Cancer Res 58 (14): 2923-4, 1998. [PUBMED Abstract]
Major Genetic Syndromes
Introduction
Originally described in the 1800s and 1900s by their clinical findings, the colon cancer susceptibility syndrome names often reflected the physician or patient and family associated with the syndrome (e.g., Gardner syndrome, Turcot syndrome, Muir-Torre syndrome, Lynch syndrome, Peutz-Jeghers syndrome [PJS], Bannayan-Riley-Ruvalcaba syndrome, and Cowden syndrome). These syndromes were associated with an increased lifetime risk of colorectal adenocarcinoma. They were mostly thought to have autosomal dominant inheritance patterns. Adenomatous colonic polyps were characteristic of the first four, while hamartomas were found to be characteristic in the last three.
With the development of the Human Genome Project and the identification in 1990 of the adenomatous polyposis coli (APC) gene on chromosome 5q, overlap and differences between these familial syndromes became apparent. Gardner syndrome and familial adenomatous polyposis (FAP) were shown to be synonymous, both caused by pathogenic variants in the APC gene. Attenuated FAP (AFAP) was recognized as a syndrome with less adenomas and extraintestinal manifestations due to an APC pathogenic variant at the 3’ or 5’ ends of the gene. MUTYH-associated polyposis (MAP) was recognized as a separate adenomatous polyp syndrome with autosomal recessive inheritance. Once the pathogenic variants were identified, the absolute risk of colorectal cancer (CRC) could be better assessed for carriers of pathogenic variants (refer to Table 3).
Table 3. Absolute Risks of Colorectal Cancer (CRC) for Carriers of Pathogenic Variants in Hereditary CRC Syndromes
Syndrome
Absolute Risk of CRC in Carriers of a Pathogenic Variant
With these discoveries genetic testing and risk management became possible. Genetic testing refers to searching for variants in known cancer susceptibility genes using a variety of techniques. Comprehensive genetic testing includes sequencing the entire coding region of a gene, the intron–exon boundaries (splice sites), and assessment of rearrangements, deletions, or other changes in copy number (with techniques such as multiplex ligation-dependent probe amplification [MLPA] or Southern blot). Despite extensive accumulated experience that helps distinguish pathogenic variants from benign variants and polymorphisms, genetic testing sometimes identifies variants of uncertain significance (VUS) that cannot be used for predictive purposes.
Familial Adenomatous Polyposis (FAP)
Introduction
By 1900, several reports had demonstrated that patients with a large number of polyps (later subclassified as adenomas) were at very high risk of CRC and that the pattern of transmission in families was autosomal dominant. In the 20th century, the adenoma-to-carcinoma progression was confirmed, and FAP was recognized as the prototypical model for this progression.[11] Classic FAP is characterized by numerous (hundreds to thousands) adenomatous polyps in the colon and rectum developing after the first decade of life (refer to Figure 3).
EnlargeFigure 3. Familial adenomatous polyposis is characterized by multiple (>100) adenomatous polyps in the colon and rectum developing after the first decade of life.
There is also a subset of classic FAP that has an attenuated phenotype. AFAP is a heterogeneous clinical entity characterized by fewer adenomatous polyps in the colon and rectum than in classic FAP. (Refer to the Attenuated Familial Adenomatous Polyposis [AFAP] section of this summary for more information.)
FAP is one of the most clearly defined and well understood of the inherited colon cancer syndromes.[1,12,13] It is an autosomal dominant condition, and the reported incidence varies from 1 in 7,000 to 1 in 22,000 live births.[14] The presence of ethnic differences in the prevalence of FAP has been suggested [14] but a large study did not find significant differences in ethnic variation in more than 6,169 individuals with a personal and/or family history of CRC and polyps who were referred for genetic testing at a large reference laboratory.[15] Most cases of FAP result from pathogenic variants in the APC gene on chromosome 5q21. (Refer to the Genetics of FAP section of this summary for more information about the APC gene and genetic testing.)
In addition to a high risk of colon adenomas in FAP patients, various extracolonic manifestations have also been described, including upper gastrointestinal (GI) tract adenomas and adenocarcinomas; fundic gland stomach polyps; nonepithelial benign tumors (osteomas, epidermal cysts, dental abnormalities); desmoid tumors; congenital hypertrophy of retinal pigment epithelium (CHRPE); and malignant tumors (thyroid and brain tumors, hepatoblastoma). Refer to Table 4 for the risks of these extracolonic manifestations in FAP.
Table 4. Extracolonic Tumor Risks in Familial Adenomatous Polyposis
Malignancy
Relative Risk
Absolute Lifetime Risk (%)
Adapted from Giardiello et al.,[16] Jagelman et al.,[17] Sturt et al.,[18] Lynch et al.,[19] Bülow et al.,[20] Burt et al.,[21] and Galiatsatos et al.[22]
aThe Leeds Castle Polyposis Group.
Desmoid tumor
852.0
15.0
Duodenal tumors and cancer
330.8
5.0–12.0
Thyroid cancer
7.6
2.0
Brain cancer
7.0
2.0
Ampullary cancer
123.7
1.7
Pancreatic cancer
4.5
1.7
Hepatoblastoma
847.0
1.6
Gastric cancer
Not defined
0.6a
FAP has also been known as familial polyposis coli or adenomatous polyposis coli (APC). Gardner syndrome was previously the diagnosis for FAP patients who manifested with colorectal polyposis, osteomas, and soft tissue tumors. However, Gardner syndrome has been shown genetically to be a variant of FAP, and thus the term Gardner syndrome is essentially obsolete in clinical practice.[23]
Clinical phenotype
Colon adenomas and CRC
Individuals who inherit a pathogenic variant in the APC gene have a very high likelihood of developing colonic adenomas; the risk has been estimated to be more than 90%.[1,12,13] The age at onset of adenomas in the colon is variable, and the median age for the appearance of colorectal adenomas is 16 years.[24] By age 10 years, only 15% of carriers of the APCgermline variant manifest adenomas; by age 20 years, the probability rises to 75%; and by age 30 years, 90% will have presented with FAP.[1,12,13,24,25] The exception is AFAP, in which affected individuals typically have fewer colon polyps, which are predominantly in the right colon, and later onset of CRC. (Refer to the Attenuated Familial Adenomatous Polyposis [AFAP] section of this summary for more information.) Without any intervention, most individuals with FAP will develop CRC by the fourth decade of life.[1,12,13] Thus, surveillance and intervention for carriers of an APC pathogenic variant and at-risk individuals have conventionally consisted of annual colonoscopy beginning around puberty for early detection of colonic polyps and to help plan when to perform colectomy.[26,27] (Refer to the Interventions for FAP section of this summary for more information.)
Extracolonic manifestations
Congenital hypertrophy of the retinal pigment epithelium (CHRPE)
CHRPE are flat, darkly pigmented lesions in the retina that are present in approximately 75% of patients with FAP [28,29] compared with a general population frequency of 1.2%.[30] The lesions are often present at birth or in early childhood and are frequently multiple or bilateral in FAP patients.[31] A study of 17 individuals diagnosed with FAP and 13 at-risk family members reported a sensitivity of the presence of a CHRPE lesion in association with colonic polyps in FAP of 76%, a specificity of 92%, a positive predictive value of 93%, and a negative predictive value of 75%; thus, screening at-risk individuals for CHRPE can be a reasonable method of detecting FAP.[28]
Desmoid tumors
Desmoid tumors are proliferative, locally invasive, nonmetastasizing, fibromatous tumors in a collagen matrix. Although they do not metastasize, they can grow very aggressively and be life threatening.[32] Desmoids may occur sporadically, as part of classical FAP, or in a hereditary manner without the colon findings of FAP.[19,33] Desmoids have been associated with hereditary APC pathogenic variants even when not associated with typical adenomatous polyposis of the colon.[33,34]
Most studies have found that 10% of FAP patients develop desmoids, with reported ranges of 8% to 38%. The incidence varies with the means of ascertainment and the location of the pathogenic variant in the APC gene.[33,35,36] APC pathogenic variants occurring between codons 1445 and 1578 have been associated with an increased incidence of desmoid tumors in FAP patients.[34,37–39] Desmoid tumors with a late onset and a milder intestinal polyposis phenotype (hereditary desmoid disease) have been described in patients with pathogenic variants at codon 1924.[33]
A desmoid risk factor scale has been described in an attempt to identify patients who are likely to develop desmoid tumors.[40] The desmoid risk factor scale was based on gender, presence or absence of extracolonic manifestations, family history of desmoids, and genotype, if available. By utilizing this scale, it was possible to stratify FAP patients into low-, medium-, and high-risk groups for developing desmoid tumors. The authors concluded that the desmoid risk factor scale could be used for surgical planning. Validation of the risk factors comprising this scale was supported by a large, multiregistry, retrospective study from Europe.[41]
The natural history of desmoids is variable. Some authors have proposed a model for desmoid tumor formation whereby abnormal fibroblast function leads to mesenteric, plaque-like desmoid precursor lesions, which in some cases occur before surgery and progress to mesenteric fibromatosis after surgical trauma, ultimately giving rise to desmoid tumors.[42] It is estimated that 10% of desmoids resolve, 50% remain stable for prolonged periods, 30% fluctuate, and 10% grow rapidly.[43] Desmoids often occur after surgical or physiological trauma, and both endocrine and genetic factors have been implicated. Approximately 80% of intra-abdominal desmoids in FAP occur after surgical trauma.[44,45]
The desmoids in FAP are often intra-abdominal, may present early, and can lead to intestinal obstruction or infarction and/or obstruction of the ureters.[36] In some series, desmoids are the second most common cause of death after CRC in FAP patients.[46,47] A staging system has been proposed to facilitate the stratification of intra-abdominal desmoids by disease severity.[48] The proposed staging system for intra-abdominal desmoids is as follows: stage I for asymptomatic nongrowing desmoids; stage II for symptomatic nongrowing desmoids of 10 cm or less in maximum diameter; stage III for symptomatic desmoids of 11 cm to 20 cm or for asymptomatic slow-growing desmoids; and stage IV for desmoids larger than 20 cm, or rapidly growing, or with life-threatening complications.[48]
These data suggest that genetic testing could be of value in the medical management of patients with FAP and/or multiple desmoid tumors. Those with APC genotypes predisposing to desmoid formation (e.g., at the 3’ end or codon 1445 of the APC gene) appear to be at high risk of developing desmoids after any surgery, including risk-reducing colectomy and surgical surveillance procedures such as laparoscopy.[35,43,49]
Stomach tumors
The most common FAP-related gastric polyps are fundic gland polyps (FGPs). FGPs are often diffuse and not amenable to endoscopic removal. The incidence of FGPs has been estimated to be as high as 60% in patients with FAP, compared with 0.8% to 1.9% in the general population.[20,22,50–54] These polyps consist of distorted fundic glands containing microcysts lined with fundic-type epithelial cells or foveolar mucous cells.[55,56]
The hyperplastic surface epithelium is, by definition, nonneoplastic. Accordingly, FGPs have not been considered precancerous. However, case reports of stomach cancer appearing to arise from FGPs have led to a reexamination of this issue.[22,57] In one FAP series, focal dysplasia was evident in the surface epithelium of FGPs in 25% of patients versus 1% of sporadic FGPs.[56] In a prospective study of patients with FAP undergoing surveillance with esophagogastroduodenoscopy, FGPs were detected in 88% of the patients. Low-grade dysplasia was detected in 38% of these patients, whereas high-grade dysplasia was detected in 3% of these patients. The study’s authors recommended that, if a polyp with high-grade dysplasia is identified, polypectomy be considered with repeat endoscopic surveillance in 3 to 6 months.[58]
Complicating the issue of differential diagnosis, FGPs have been increasingly recognized in non-FAP patients consuming proton pump inhibitors (PPIs).[56,59] FGPs in this setting commonly show a PPI effect consisting of congestion of secretory granules in parietal cells, leading to irregular bulging of individual cells into the lumen of glands. To the trained eye, the presence of dysplasia and the concomitant absence of a characteristic PPI effect can be considered highly suggestive of the presence of underlying FAP. The number of FGPs tends to be greater in FAP than that seen in patients consuming PPIs, although there is some overlap.
Gastric adenomas also occur in patients with FAP. The incidence of gastric adenomas in Western patients is reported to be between 2% and 12%, whereas in Japan, incidence is reported to be between 39% and 50%.[60–63] These adenomas can progress to carcinoma. Patients with FAP in Korea and Japan have a threefold to fourfold increased risk of gastric cancer when compared with individuals in the general population in these countries. This finding was not observed in Western populations.[64–68] The increased prevalence of gastric adenomas in Asian patients with FAP may be due to the high prevalence of Helicobacter pylori infections in this population.[61]
More recently, a rise in incidence of gastric adenocarcinoma was observed in a Western FAP database.[69] Alterations in the promoter (1B) of APC were discovered in families with gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS), who express numerous, predominantly fundic gland, gastric polyps restricted to the body and fundus with regions of dysplasia or gastric adenocarcinoma, and no evidence of colorectal or duodenal polyposis. These variants segregated with the gastric phenotype in multiple GAPPS families. Although penetrance of the gastric polyposis phenotype is high, the phenotype can vary ranging from asymptomatic adults to teenagers presenting with massive symptomatic gastric polyposis, as well as unaffected carriers who had clean endoscopies at ages ranging from 42 to 77 years. However, the penetrance for gastric cancer is less clear. Promoter 1B APC alterations rarely occur in FAP families with gastric fundic gland polyps and colonic polyposis.[70]
Duodenum/small bowel tumors
Whereas the incidence of duodenal adenomas is only 0.4% in unselected patients undergoing upper GI endoscopy,[71] duodenal adenomas are found in 80% to 100% of FAP patients. Most are located in the first and second portions of the duodenum, especially in the periampullary region.[50,51,72] In a prospective multicenter surveillance study of duodenal adenomas in 368 participants from northern Europe with FAP, 65% had adenomas at baseline evaluation (mean age, 38 y), with cumulative prevalence reaching 90% by age 70 years. In contrast to earlier beliefs regarding an indolent clinical course, the adenomas increased in size and degree of dysplasia during the 8 years of average surveillance, although only 4.5% developed cancer while under prospective surveillance.[20] This is a large study; however, it is limited by the use of forward-viewing rather than side-viewing endoscopy and the large number of investigators involved in the study. Intestinal polyps can also be assessed in FAP patients using capsule endoscopy.[73–75] One study of computed tomography (CT) duodenography found that larger adenoma size could be accurately measured but smaller, flatter adenomas could not be accurately counted.[76]
Approximately 1.7% of all duodenal cancer cases are attributed to FAP.[17,66,77–79] The incidence of duodenal adenocarcinoma in FAP is 4% to 12% lifetime. A retrospective review of FAP patients suggested that the adenoma-carcinoma sequence occurred in a temporal fashion for periampullary adenocarcinomas with a diagnosis of adenoma at a mean age of 39 years, high-grade dysplasia at a mean age of 47 years, and adenocarcinoma at a mean age of 54 years.[80] A decision analysis of 601 FAP patients suggested that the benefit of periodic surveillance starting at age 30 years led to an increased life expectancy of 7 months.[77] Although polyps in the duodenum can be difficult to treat, small series suggest that they can be managed successfully with endoscopy but with potential morbidity—primarily from pancreatitis, bleeding, and duodenal perforation.[81,82]
FAP patients with particularly severe duodenal polyposis, sometimes called dense polyposis, or with histologically advanced duodenal adenomas appear to be at the highest risk of developing duodenal adenocarcinoma.[20,78,83,84] Because the risk of duodenal adenocarcinoma is correlated with the number and size of polyps and the severity of dysplasia of the polyps, a stratification system that incorporates these features was developed to attempt to identify those individuals with FAP at the highest risk of developing duodenal adenocarcinoma.[84] According to this system, known as the Spigelman classification (refer to Table 5), 36% of patients with the most advanced stage will develop carcinoma.[78]
The predictive utility of the Spigelman classification has been called into question. The point system for dysplasia classifies dysplasia as mild, moderate, or severe, yet pathologists do not customarily attempt to distinguish moderate dysplasia from low-grade. There are no studies validating interobserver concordance in classifying a villous component or interpretation of the degree of dysplasia. A study from the Cleveland Clinic comparing Spigelman classification and its components in patients with FAP with and without cancer found neither adenoma count nor villous component to be predictive of cancer risk.[85] While patients with advanced (Spigelman IV) classification were more likely to develop cancer, nearly half of those with cancer did not meet Spigelman IV criteria.
Table 5. Spigelman Classification
Points
Polyp Number
Polyp Size (mm)
Histology
Dysplasia
Stage I, 1–4 points; Stage II, 5–6 points; Stage III, 7–8 points; Stage IV, 9–12 points.[84]
1
1–4
1–4
Tubular
Mild
2
5–20
5–10
Tubulovillous
Moderate
3
>20
>10
Villous
Severe
Other tumors
Other extracolonic tumors arising in FAP patients include papillary thyroid cancer, adrenal tumors, hepatoblastoma, and brain tumors.
Papillary thyroid cancer (cribriform morular type) has been reported to affect 1% to 2% of patients with FAP.[86] However, a study [87] of papillary thyroid cancers in six women with FAP failed to demonstrate loss of heterozygosity (LOH) or pathogenic variants of the wild-type allele in codons 545 and 1061 to 1678 of the six tumors. In addition, four of five of these patients had detectable somaticRET/PTC chimeric genes. This pathogenic variant is generally restricted to sporadic papillary thyroid carcinomas, suggesting the involvement of genetic factors other than APC pathogenic variants. Further studies are needed to show whether other genetic factors such as the RET/PTC chimeric gene are independently responsible for or cooperative with APC variants in causing papillary thyroid cancers in FAP patients.
Adrenal tumors have been reported in FAP patients, and one study demonstrated LOH at the APClocus in an adrenocortical carcinoma (ACC) in an FAP patient.[88] In a study of 162 FAP patients who underwent abdominal CT for evaluation of intra-abdominal desmoid tumors, 15 patients (11 women) were found to have adrenal tumors.[89] Of these, two had symptoms attributable to cortisol hypersecretion. Three of these patients underwent subsequent surgery and were found to have ACC, bilateral nodular hyperplasia, or adrenocortical adenoma. The prevalence of an unexpected adrenal neoplasia in this cohort was 7.4%, which compares with a prevalence of 0.6% to 3.4% (P < .001) in non-FAP patients.[89] No molecular genetic analyses were provided for the tumors resected in this series. A subsequent study identified adrenal lesions in 26% (23 of 90) of patients with FAP, 18% (2 of 11) of patients with AFAP, and 24% (5 of 21) of patients with MAP. Most lesions in this series followed a benign and slowly progressive course; no cases of ACC were reported.[90]
Hepatoblastoma is a rare, rapidly progressive, and usually fatal childhood malignancy that, if confined to the liver, can be cured by radical surgical resection. Multiple cases of hepatoblastoma have been described in children with an APC pathogenic variant.[91–100] Some series have also demonstrated LOH of APC in these tumors.[92,94,101] No specific genotype-phenotype correlations have been identified in FAP patients with hepatoblastoma.[102] (Refer to the Hepatoblastoma section in the PDQ summary on Childhood Liver Cancer Treatment for more information.)
The constellation of CRC and brain tumors has been referred to as Turcot syndrome; however, Turcot syndrome is molecularly heterogeneous. Molecular studies have demonstrated that colon polyposis and medulloblastoma are associated with pathogenic variants in APC (thus representing FAP), while colon cancer and glioblastoma are associated with pathogenic variants in mismatch repair (MMR) genes (thus representing Lynch syndrome).[103]
Medulloblastoma, a highly malignant embryonal central nervous system tumor, accounts for approximately 80% of the brain tumors found in FAP and primarily occurs in children with 70% diagnosed before age 16 years. High-grade astrocytomas and ependymomas have also been described in FAP patients. Although the relative lifetime risk of any brain tumor among members of an FAP family is increased 7-fold and that of medulloblastoma 90-fold, the absolute lifetime risk of any brain tumor is approximately 1% to 2%.[103]
Genetics of FAP
APC gene
The APC gene on chromosome 5q21 encodes a 2,843-amino acid protein that is important in cell adhesion and signal transduction; the main function of the APC protein is to regulate intracellular concentrations of beta-catenin, a major mediator of the Wnt signal transduction pathway. APC is a tumor suppressor gene, and the loss of APC is among the earliest events in the chromosomal instability colorectal tumor pathway. FAP and AFAP can be diagnosed genetically by testing for germline pathogenic variants in the APC gene in DNA from peripheral blood leukocytes. More than 300 different disease-associated pathogenic variants of the APC gene have been reported.[104] Most of these changes are insertions, deletions, and nonsense variants that lead to frameshifts and/or premature stop codons in the resulting transcript of the gene. The most common APC pathogenic variant (10% of FAP patients) is a deletion of AAAAG in codon 1309; no other pathogenic variants appear to predominate. Variants that reduce rather than eliminate production of the APC protein may also lead to FAP.[105]
Genotype-phenotype correlations
Most APC pathogenic variants that occur between codon 169 and codon 1249 result in the classic FAP phenotype.[106–108] There has been much interest in correlating the location of the pathogenic variant within the gene with the clinical phenotype:
Researchers have found that dense carpeting of colonic polyps, a feature of classic FAP, is seen in most patients with APC pathogenic variants, particularly those variants that occur between codons 1250 and 1464. AFAP is associated with pathogenic variants that occur in or upstream of exon 4 and in the latter two-thirds of exon 15.[106–109] (Refer to the Attenuated Familial Adenomatous Polyposis [AFAP] section of this summary for more information.)
CHRPE are rarely associated with pathogenic variants that occur before exon 9.[39,108] Individuals with exon 9 variants tend not to have duodenal adenomas.[70,110]
Families with GAPPS, who express numerous, predominantly fundic gland gastric polyps restricted to the body and fundus with regions of dysplasia or gastric adenocarcinoma, and no evidence of colorectal or duodenal polyposis, were found to possess variants in the promoter (1B) of APC.[70]
APC pathogenic variants occurring between codons 1445 and 1578 have been associated with an increased incidence of desmoid tumors in FAP patients.[34,37–39]
A low-penetrance APC variant, I1307K, has been studied for its association with CRC. (Refer to the APC I1307K section in the Colorectal Cancer Susceptibility Genes section of this summary for more information.)
Genetic testing for FAP
Probands
Individuals who present with a classic FAP phenotype are candidates for APC testing. However, in many probands with a personal or family history of polyposis, multigene panel testing is an appropriate option to consider given the genetic heterogeneity of polyposis conditions and the phenotypic overlap among associated syndromes.
In particular, patients who develop fewer than 100 colorectal adenomatous polyps may pose a diagnostic challenge. The differential diagnosis includes AFAP, MAP, polymerase proofreading–associated polyposis (PPAP), and constitutional mismatch repair deficiency (CMMRD).[111] AFAP can be diagnosed by testing for germline APC pathogenic variants. (Refer to the Attenuated Familial Adenomatous Polyposis [AFAP] section of this summary for more information.) MAP is caused by biallelic germline pathogenic variants in the MUTYH gene, inherited in an autosomal recessive manner.[112] PPAP is caused by heterozygous pathogenic variants in POLE and POLD1.[113,114] CMMRD is a condition in which individuals inherit pathogenic variants in both alleles of one MMR gene (MLH1, MSH2, MSH6, PMS2, or EPCAM).[115] For more information, see the MUTYH-Associated Polyposis (MAP), Oligopolyposis, and IHC in constitutional mismatch repair deficiency (CMMRD) syndrome sections.
For example, in a large cross-sectional study, pathogenic variants in APC were found in 80% (95% confidence interval [CI], 71%–87%) of individuals with more than 1,000 adenomas, 56% (95% CI, 54%–59%) in those with 100 to 999 adenomas, 10% (95% CI, 9%–11%) in those with 20 to 99 adenomas, and 5% (95% CI, 4%–7%) in those with 10 to 19 adenomas.[116] In this same study, the prevalence of biallelic MUTYH pathogenic variants was similar to APC for those with the attenuated phenotype (20–99 adenomas), but MUTYH pathogenic variants were also observed in a small minority (2%) of those with classic polyposis.[116]
Most commercial laboratories perform not only full gene sequencing but also deletion/duplication analysis of the APC and other genes. However, it is important to verify the testing methodology with each laboratory. Deletion analysis is especially important for individuals with FAP because 8% to 12% of affected individuals have a whole exon deletion or promoter 1B deletion in the APC gene, which would not be detected with sequencing.[117–120] As mentioned, for patients who present with polyposis, multigene panels that include multiple polyposis genes are often ordered, which simplifies and lowers the cost of testing by assessing all genes at the same time. (Refer to the Multigene [panel] testing section in the PDQ summary on Cancer Genetics Risk Assessment and Counseling for more information.)
Cascade testing
In families in which a pathogenic variant in the APC gene is identified, predictive testing for at-risk relatives can definitively identify or rule out the variant. Such testing is important to determine whether at-risk relatives need to undergo aggressive screening or whether such procedures are not necessary or can be discontinued (i.e., in relatives who test negative for the familial pathogenic variant).
Most patients with FAP have an affected parent, and a pattern of autosomal dominant inheritance may be observed in the family. Accordingly, cascade genetic counseling and testing may then be extended to at-risk family members. However, it is estimated that 25% of patients with FAP have a de novo pathogenic variant in APC, meaning that the variant does not appear to be inherited from either parent.[121] In cases where the variant cannot be identified in leukocyte DNA of either parent, it is possible that germlinemosaicism may explain the finding. Thus, siblings of an individual should always be offered APC testing, but testing aunts, uncles, and cousins of the proband would not be indicated.
The early appearance of FAP clinical features and the subsequent recommendations for surveillance beginning at puberty raise special considerations relating to the genetic testing of minors.[122] Hereditary cancer genetic testing is not recommended for minors unless results will affect medical management in childhood. Thus, FAP presents an example in which possible medical benefit justifies genetic testing of minors in families with a known pathogenic variant, especially for the anticipated 50% of at-risk children who will be found not to be carriers of pathogenic variants and who can thus be spared surveillance. In addition, testing infants for FAP can allow for hepatoblastoma surveillance until age 5 years. Otherwise, if at-risk minors are not tested, high-quality colonoscopy is initiated between ages 10 and 15 years.[123] The psychological impact of such testing is addressed in the Psychosocial Issues in Hereditary Colon Cancer Syndromes section of this summary.
Interventions for FAP
Colon surveillance
Individuals at risk of FAP, because of a known APC pathogenic variant in either the family or themselves, are evaluated for onset of polyposis by flexible sigmoidoscopy or colonoscopy. Once an FAP family member is found to manifest polyps, the only effective management to prevent CRC is colectomy. Prophylactic surgery has been shown to improve survival in patients with FAP.[124] If feasible, the patient and his/her family members should be included in a registry because it has been shown retrospectively that registration and surveillance reduce CRC incidence and mortality.[125] In patients with classic FAP identified very early in their course, the surgeon, endoscopist, and family may choose to delay surgery for several years in the interest of achieving social milestones. In addition, in carefully selected patients with AFAP (those with minimal polyp burden and advanced age), deferring a decision about colectomy may be reasonable with surgery performed only in the face of advancing polyp burden or dysplasia.
A Finnish nationwide, population-based, retrospective study evaluating whether surveillance of family members with FAP reduced overall mortality and improved survival demonstrated that family members of probands who were recruited to the screening program had equivalent survival to the general population up to 20 years after diagnosis of FAP.[126] The study included 154 families with at least one family member clinically diagnosed with FAP from 1963 to 2015. There were 194 probands and 225 family members (83 diagnosed by genetic testing and 142 by endoscopy) with a median time of follow-up of 11.8 years. In this study, the survival analysis of members of FAP families was calculated using the relative survival estimate.[127] This estimate compares survival among FAP probands and family members with the survival expected in the absence of FAP among individuals of the same gender and age in each calendar year. The relative survival rate was 67% for probands (95% CI, 60%–75%) at 10 years of follow-up and 66% (95% CI, 58%–76%) at 20 years of follow-up. For family members, the relative survival rate was 98% (95% CI, 95%–101%) at 10 years of follow-up and 94% (95% CI, 88%–100%) at 20 years of follow-up. The relative survival rate was 87% (95% CI, 79%–96%) for family members at 25 years of follow-up. The relative survival rate for probands was significantly lower than the relative survival rate for family members (P < .001). The standardized mortality ratio was elevated in probands in both the 0- to 5-year and 5- to 10-year periods of follow-up whereas it remained stable for family members until 20 years of follow-up. This difference was more marked in the beginning of follow-up for probands, considering that most of them were probably symptomatic and most likely had CRC when they were diagnosed with FAP. The authors mentioned that if the CRC was treated successfully without recurrence, the survival of the probands approached that of the family members.
Colonoscopic surveillance usually begins at an early age (10–15 y) in individuals with FAP.[123] (Refer to the Psychosocial Issues in Hereditary Colon Cancer Syndromes section of this summary for more information on the social and emotional implications of early surveillance.) Colonoscopy is the screening tool of choice for individuals with FAP for the following reasons: (a) improved instrumentation for full colonoscopy, (b) sedation, (c) recognition of AFAP, in which the disease typically manifests in the right colon, and (d) the growing tendency to defer surgery for a number of years.[123] The National Comprehensive Cancer Network (NCCN) recommends that individuals who test negative for a known familial APC pathogenic variant undergo average-risk population screening. However, clinical surveillance is warranted in families in which an APC pathogenic variant has not been identified in an affected individual. NCCN also recommends that individuals with an APC pathogenic variant continue colon cancer screening, even if they have not developed colon polyps, since adenomas may not manifest until later in life.[123] (Refer to the PDQ summary on Colorectal Cancer Screening for more information on these methods.)
Colorectal surgery
Colon adenomas will develop in nearly 100% of individuals who are APC pathogenic variant positive; risk-reducing surgery comprises the standard of care to prevent CRC after polyps have appeared and are too numerous or histologically advanced to monitor safely using endoscopic resection.
FAP patients and their doctors should have an individualized discussion to decide when surgery will be performed. It is useful to incorporate into the discussion the risk of developing desmoid tumors after surgery, as well as fecundity for women. Timing of risk-reducing surgery usually depends on the number of polyps, their size, histology, and symptomatology.[128] Once numerous polyps have developed, surveillance colonoscopy is no longer useful in timing the colectomy because polyps are so numerous that it is not possible to biopsy or remove all of them. At this time, it is appropriate for patients to consult with a surgeon who is experienced with available options, including total colectomy and restorative proctocolectomy.[129] Rectum-sparing surgery, with sigmoidoscopic surveillance of the remaining rectum, is a reasonable alternative to total colectomy in those compliant individuals with relative rectal sparing of polyps who understand the consequences and make an informed decision to accept the residual risk of rectal cancer occurring despite periodic surveillance.[130]
Surgical options include restorative proctocolectomy with ileal pouch–anal anastomosis (IPAA), total colectomy with ileorectal anastomosis (IRA), or total proctocolectomy with ileostomy (TPC). TPC is reserved for patients with low rectal cancer in which the sphincter cannot be spared or for patients on whom an IPAA cannot be performed because of technical problems. There is no risk of developing rectal cancer after TPC because the whole mucosa at risk is removed. These procedures can be performed using minimally invasive techniques.
Irrespective of whether a colectomy and an IRA or a restorative proctocolectomy is performed, most experts suggest that periodic and lifelong surveillance of the rectum or the ileal pouch be performed to remove or ablate any polyps. In earlier unselected studies, the risk of rectal cancer after total colectomy 20 years after IRA was reported to be as high as 25%.[131,132] This risk has been reported to be much lower with better selection of patients for IRA.[129,133] Factors that have been reported to increase rectal cancer risk after IRA include the number of polyps throughout the colon, the number of polyps in the rectum, the presence of colon cancer at the time of IRA, the length of the rectal stump, the duration of follow-up after IRA, and the genotype.[39,134–136] An abdominal colectomy with IRA as the primary surgery for FAP does not preclude later conversion to an IPAA for uncontrolled rectal polyps and/or rectal cancer. In the Danish Polyposis Registry, the morbidity and functional results of a secondary IPAA (after a previous IRA) in 24 patients were reported to be similar to those of 59 patients who underwent primary IPAA.[137]
In most cases, the clinical polyp burden in the rectum at the time of surgery dictates the type of surgical intervention, namely, restorative proctocolectomy with IPAA versus IRA. Patients with a mild phenotype (<1,000 colonic adenomas) and fewer than 20 rectal polyps may be candidates for IRA at the time of prophylactic surgery.[138] In some cases, however, the polyp burden is equivocal, and in such cases, investigators have considered the role of genotype in predicting subsequent outcomes with respect to the rectum.[139] Several APC pathogenic variants can increase an individual’s rectal cancer risk and can therefore increase an individual’s risk for eventual completion proctectomy after IRA. These APC pathogenic variants are located in exon 15 in codon 1250, codon 1309, codon 1328, and between codons 1250 and 1464.[140,131,141,142] A meta-analysis examined quality of life after restorative proctocolectomy and IPAA in patients with ulcerative colitis and FAP. The results suggested that patients with FAP do marginally better than patients with ulcerative colitis regarding fistula formation, pouchitis, stool frequency, and seepage.[143]
It is important to continue annual surveillance of the ileal pouch in patients who have undergone IPAA because they are at risk of developing neoplasia in the anal transitional zone/residual rectal mucosa and in the ileal pouch. The cumulative risk of developing adenomas in the ileal pouch can be up to 75% for 15 years after surgery has been completed.[144,145] A retrospective study from the Cleveland Clinic Registry followed patients with FAP who underwent IPAA. After a median follow-up period of 10.1 years and a median of four pouchoscopies, 47% of patients (78 of 165) developed rectal mucosa/transitional zone adenomas. Adenomas were more frequently diagnosed in patients who had undergone stapled IPAA (52.3% [72 of 137]) when compared with those who had undergone mucosectomy and handsewn IPAA (21.4% [6 of 28]; P < .005).[146] Although they are rare, carcinomas have been reported in the ileal pouch and anal transition zone after restorative proctocolectomy in patients with FAP.[147] In the Cleveland Clinic study, six patients developed cancer after IPAA (three patients developed cancer while under surveillance, and three patients developed cancer after missing surveillance pouchoscopies).[146]
Chemoprevention
Celecoxib, a specific cyclooxygenase 2 (COX-2) inhibitor, and nonspecific COX-2 inhibitors, such as sulindac (a nonsteroidal anti-inflammatory drug [NSAID]), have been associated with a decrease in polyp size and number in FAP patients, suggesting a role for chemopreventive agents in the treatment of this disorder.[148,149] Although celecoxib had been approved by the U.S. Food and Drug Administration (FDA), its license was voluntarily withdrawn by the manufacturer. Currently, there are no FDA-approved drugs for chemoprevention in FAP. Nevertheless, agents such as celecoxib and sulindac are used so commonly that chemopreventive clinical trials typically use one of these agents as a control. A randomized trial showed possible marginal improvement in polyp burden with the combination of celecoxib and eflornithine (i.e., difluoromethylornithine [DFMO]) when compared with celecoxib alone.[150] An international randomized trial analyzed the use of daily sulindac, eflornithine, or sulindac plus eflornithine in 171 individuals with FAP. In the three study arms, there were no significant differences between the frequencies of FAP-related events (i.e., primary end points), which were composites of major surgeries (colectomies/proctocolectomies/pouchectomies/duodenal resections), excisions of advanced adenomas, diagnoses of cancer/high-grade dysplasia, and/or progressions of duodenal polyposis by more than one Spigelman stage.[151] A post-hoc analysis was performed on 158 participants with FAP who were at risk for lower GI neoplasia. Results demonstrated a significant, marked reduction in the likelihood of lower GI tract polyposis progression (hazard ratio [HR], <0.2) in the sulindac plus eflornithine arm versus sulindac alone (HR, 0.195; 95% CI, 0.048–0.803) and versus eflornithine alone (HR, 0.171; 95% CI, 0.042–0.698). Lower GI tract polyposis progression was defined as the need for colectomy, proctocolectomy, proctectomy, pouchectomy, the excision of any polyp that was more than 10 mm, and/or the diagnosis of cancer/high-grade dysplasia. Moreover, 0 of 54 participants randomly assigned to the sulindac plus eflornithine arm required major surgery, versus 7 of 53 (13.2%) in the sulindac-only arm, and 8 of 51 (15.7%) in the eflornithine-only arm (P ≤ .005).[152]
A small, randomized, placebo-controlled, dose-escalation trial of celecoxib in a pediatric population (aged 10–14 y) demonstrated the safety of celecoxib at all dosing levels when administered over a 3-month period.[153] This study found a dose-dependent reduction in adenomatous polyp burden. At a dose of 16 mg/kg/day, which approximates the approved dose of 400 mg twice daily in adults, the reduction in polyp burden paralleled that demonstrated with celecoxib in adults.
Omega-3-polyunsaturated fatty acid eicosapentaenoic acid in the free fatty acid form has been shown to reduce rectal polyp number and size in a small study of patients with FAP after subtotal colectomy.[154] Although not directly compared in a randomized trial, the effect appeared to be similar in magnitude to that previously observed with celecoxib.
It is unclear at present how to incorporate COX-2 inhibitors into the management of FAP patients who have not yet undergone risk-reducing surgery. A double-blind placebo-controlled trial of 41 child and young adult carriers of APC pathogenic variants who had not yet manifested polyposis demonstrated that sulindac may not be effective as a primary treatment in FAP. There were no statistically significant differences between the sulindac and placebo groups over 4 years of treatment in incidence, number, or size of polyps.[149]
Consistent with the effects of COX-2 inhibitors on colonic polyps, in a randomized, prospective, double-blind, placebo-controlled trial, celecoxib reduced, but did not eliminate, the number of duodenal polyps in 32 patients with FAP after a 6-month course of treatment. Of importance, a statistically significant effect was seen only in individuals who had more than 5% of the duodenum involved with polyps at baseline and with an oral dose of 400 mg, given twice daily.[155] A previous randomized study of 24 FAP patients treated with sulindac for 6 months showed a nonsignificant trend in the reduction of duodenal polyps.[156] The same issues surrounding the use of COX-2 inhibitors for the treatment of colonic polyps apply to their use for the treatment of duodenal polyps (e.g., only partial elimination of the polyps, complications secondary to the COX-2 inhibitors, and loss of effect after the medication is discontinued).[155]
Because of the common clustering of adenomatous polyps around the duodenal papilla (where bile enters the intestine) and preclinical data suggesting that ursodeoxycholate inhibits intestinal adenomas in mice that harbor an Apc germline variant,[157] two trials that employ ursodeoxycholate have been performed.[158,159] In both studies, ursodeoxycholate did not have a significant chemopreventive effect on duodenal polyps; paradoxically, in one study, ursodeoxycholate in combination with celecoxib appeared to promote polyp density in patients with FAP.
Because of reports demonstrating an increase in cardiac-related events in patients taking rofecoxib and celecoxib,[160–162] it is unclear whether this class of agents will be safe for long-term use for patients with FAP and in the general population. Also, because of the short-term (6 months) nature of these trials, there is currently no clinical information about cardiac events in FAP patients taking COX-2 inhibitors on a long-term basis.
One cohort study has demonstrated regression of colonic and rectal adenomas with sulindac treatment in FAP. The reported outcome of this trial was the number and size of polyps, a surrogate for the clinical outcome of main interest, CRC incidence.[163]
Preclinical studies of a small-molecule epidermal growth factor receptor (EGFR) inhibitor and low-dose sulindac in the Apcmin/+ mouse diminished intestinal adenoma development by 87% [164] suggesting that EGFR inhibitors had the potential to inhibit duodenal polyps in FAP patients. A 6-month double-blind, randomized, placebo-controlled trial tested the efficacy of sulindac, 150 mg twice daily, and erlotinib, 75 mg daily, versus placebo in FAP or AFAP patients with duodenal polyps.[165] Ninety-two patients with FAP or AFAP were randomly assigned to receive study drugs or placebo and underwent pretreatment and posttreatment upper endoscopies to determine the changes in the sum diameter of the polyps and number of polyps in a 10 cm segment of proximal duodenum. The trial was terminated prematurely because the primary endpoint was met. The intent-to-treat analysis demonstrated a median decrease in duodenal polyp burden (sum of diameters) of 8.5 mm in the sulindac/erlotinib arm while there was an 8 mm increase in the placebo arm (P < .001). Significantly higher rates of grade 1 and grade 2 adverse events occurred in the treatment arm than in the placebo arm: in the treatment arm, 60.9% developed an acneiform rash and 32.6% developed oral mucositis; in the placebo arm, 19.6% developed an acneiform rash and 10.9% developed oral mucositis. A 2018 trial in 82 individuals with FAP found that combination treatment with sulindac (150 mg twice daily) and erlotinib (75 mg daily) compared with placebo resulted in a significantly lower (69.4%) colorectal polyp burden after 6 months of treatment (95% CI, 28.8%–109.2%; P = .009).[166] There was a reduction in polyp burden in both those with an entire colorectum and those with only a rectal pouch or rectum. However, it is unclear to what extent erlotinib contributed to this reduction given that sulindac has been proven effective in the lower GI tract.
On the basis of the previously modest effects of sulindac and celecoxib on duodenal polyps in patients with FAP [149,163] and the dramatic effect of genetic EGFR inhibition on intestinal adenoma development in the Apcmin/+ mouse,[167] it is likely that erlotinib was responsible for the success of these trials. An ongoing clinical trial (NCT02961374) is determining whether lower doses of erlotinib alone are sufficient for significantly reducing duodenal polyp burden in patients with FAP and AFAP.
Patients who carry APC germline pathogenic variants are at increased risk of other types of malignancies, including desmoid tumors, gastric tumors, duodenal cancer, small bowel cancer, hepatoblastoma, thyroid cancer, and brain tumors. The management of these extracolonic tumors is described below.
Desmoid tumors
The management of desmoids in FAP can be challenging and can complicate prevention efforts. There is no accepted standard treatment for desmoid tumors. Multiple medical treatments have generally been unsuccessful in the management of desmoids. Treatments have included antiestrogens, NSAIDs, chemotherapy, and radiation therapy, among others. Studies have evaluated the use of raloxifene alone, tamoxifen or raloxifene combined with sulindac, and pirfenidone alone.[168–170]
Thirteen patients with intra-abdominal desmoids and/or unfavorable response to other medical treatments who had expression of estrogen-alpha receptors in their desmoid tissues were included in a prospective study of raloxifene, given in doses of 120 mg daily.[168] Six patients had been on tamoxifen or sulindac before treatment with raloxifene, and seven patients were previously untreated. All 13 patients with intra-abdominal desmoid disease had either a partial or a complete response 7 months to 35 months after starting treatment, and most desmoids decreased in size at 4.7 months (± 1.8 mo) after treatment. Response occurred in patients with desmoid plaques and with distinct lesions. Study limitations include small sample size and the clinical evaluation of response, which was not consistent in all patients. Several questions remain concerning the outcomes of patients with desmoid tumors not expressing estrogen-alpha receptors who have received raloxifene, as well as which patients may benefit from this potential treatment.
A second study of 13 patients with FAP-associated desmoid tumors, who were treated with tamoxifen 120 mg/day or raloxifene 120 mg/day in combination with sulindac 300 mg/day, reported that ten patients had either stable disease (n = 6) or a partial or complete response (n = 4) for more than 6 months and that three patients had stable disease for more than 30 months.[169] These results suggest that the combination of these agents may be effective in slowing the growth of desmoid tumors. However, the natural history of desmoids is variable, with both spontaneous regression and variable growth rates.
A third study reported mixed results in 14 patients with FAP-associated desmoid tumors treated with pirfenidone for 2 years.[170] In this study, some patients had disease regression, some patients had disease progression, and some patients had stable disease.
There are reports of using imatinib mesylate to treat desmoid tumors in FAP patients with some success.[171,172] Nilotinib demonstrated potential to stabilize desmoid tumor growth after treatment failure with imatinib in patients with desmoid tumors.[173]
The benefit of the tyrosine kinase inhibitor sorafenib in the treatment of desmoid tumors was demonstrated in a phase III randomized trial comparing sorafenib (400 mg daily) with placebo in 87 patients with unresectable progressive or symptomatic desmoid tumors.[174] Crossover to the sorafenib group was permitted for patients in the placebo group who had disease progression on the placebo arm of the study. Objective responses were demonstrated in 16 of 49 patients treated with sorafenib (33%) compared with 7 of 35 placebo-treated patients (20%). Additionally, the 2-year progression-free survival (PFS) rate was significantly higher for sorafenib (81%) than placebo (36%); the HR for progression or death was 0.13 (95% CI, 0.05–0.31; P < .001). The most frequently reported adverse events were grade 1 or grade 2 rash (73%), fatigue (67%), hypertension (55%), and diarrhea (51%). Despite a relatively favorable toxicity profile, approximately 20% of patients discontinued sorafenib due to toxicity, emphasizing the importance of appropriate dose delays and interruptions for the treatment of adverse events.
Because of the high rates of morbidity and recurrence, in general, surgical resection is not recommended in the treatment of intra-abdominal desmoid tumors. A review of experiences at one hospital suggested that surgical outcomes with intra-abdominal desmoid tumors may be better than previously believed.[175,176] Issues of subject selection are critical in evaluating surgical outcome data.[175] Abdominal wall desmoid tumors can be treated with surgical resection, but the recurrence rate is high.
Stomach tumors
It is not clear how to manage gastric adenomas. Only retrospective case series are available and point to a relatively low prevalence of gastric adenocarcinoma development in FAP patients.[177,178] More recently, a rise in incidence of gastric adenocarcinoma was observed in a Western FAP database [69] suggesting that a possible change in the management of gastric tumorigenesis in FAP may be in order. One group recommends endoscopic polypectomy for the management of gastric adenomas.[69] The management of adenomas in the stomach is usually individualized based on the size of the adenoma and the degree of dysplasia.
Endoscopic surveillance usually begins between ages 20 to 25 years in patients with FAP. Baseline upper endoscopy may be performed at an earlier age if the patient has a family history of large duodenal adenoma burden or duodenal/ampullary cancer.[67] The subsequent intervals between endoscopy vary according to the findings of the previous endoscopy, often based on Spigelman stage. Recommended intervals are based on expert opinion although the relatively liberal intervals for stage 0 to stage II disease are based in part on the natural history data generated by the Dutch/Scandinavian duodenal surveillance trial (refer to Table 6 for available recommendations regarding screening frequency by Spigelman stage).[20]
The main advantages of the Spigelman classification are its long-standing familiarity to and usage by those in the field, which allows reasonable standardization of outcome comparisons across studies.[63,179] However, the following are limitations of application of the Spigelman classification:
Most pathologists do not employ the term moderate dysplasia, preferring a simpler low- versus high-grade dysplasia system.
Because of the villous nature of normal duodenal epithelium, pathologists commonly disagree over the classification of tubular, tubulovillous, and villous.
Spigelman staging requires biopsy, which is not always essential when only a few small plaques are present; conversely, for larger adenomas, sampling variation leads to understaging.[180,181]
Table 6. Recommended Screening Intervals and Interventions by Spigelman Stage
ESMO = European Society of Medical Oncology; NCCN = National Comprehensive Cancer Network.
See below for additional information about the use of surgical resection in Spigelman stage IV disease.
0 (no polyps)
Endoscopy every 3–5 y
Not specified
I
Endoscopy every 2–3 y
Endoscopy every 5 y
II
Endoscopy every 1–2 y
Endoscopy every 3 y
III
Endoscopy every 6–12 mo
Endoscopy every 1–2 y
IV
Expert endoscopic surveillance every 3–6 mo
Endoscopy every 6-12 mo
Excision/ablation of resectable large or villous adenomatous polyps and endoscopic ampullectomy are options that may help individuals avoid surgery
Surgical evaluation and counseling for individuals with high-grade dysplasia, invasive carcinoma, or dense polyposis that cannot be removed endoscopically
Surgical options include duodenotomy with polypectomy, pancreas-sparing duodenectomy and pancreaticoduodenectomy (Whipple procedure)
The results of long-term duodenal adenoma surveillance of FAP patients in Nordic countries and the Netherlands revealed significant duodenal cancer risk in FAP patients.[183] According to the protocol, biennial frontal-viewing endoscopy was performed from 1990 through 2000. Subsequently, patients were followed up with surveillance according to international guidelines. The study group comprised 261 of 304 patients (86%) who had more than one endoscopy. Median follow-up was 14 years (range, 9–17 y). The lifetime risk of duodenal adenomatosis was 88%. Forty-four percent of patients had worsening Spigelman stage over time, whereas 12% improved and 34% remained unchanged. Twenty patients (7%) developed duodenal cancer at a median age of 56 years (range, 44–82 y). The cumulative cancer incidence was 18% at age 75 years (95% CI, 8%–28%). Survival in patients with symptomatic cancers was worse than those diagnosed at surveillance endoscopy.
Many factors, including severity of polyposis, comorbidities, patient preferences, and availability of adequately trained physicians, determine whether surgical or endoscopic therapy is selected for polyp management. Endoscopic resection or ablation of large or histologically advanced adenomas appears to be safe and effective in reducing the short-term risk of developing duodenal adenocarcinoma;[81,82,184] however, patients managed with endoscopic resection of adenomas remain at substantial risk of developing recurrent adenomas in the duodenum.[180] The most definitive procedure for reducing the risk of adenocarcinoma is surgical resection of the ampulla and duodenum, although these procedures also have higher morbidity and mortality associated with them than do endoscopic treatments. Duodenotomy and local resection of duodenal polyps or mucosectomy have been reported, but invariably, the polyps recur after these procedures.[185] In a series of 47 patients with FAP and Spigelman stage III or stage IV disease who underwent definitive radical surgery, the local recurrence rate was reported to be 9% after a mean follow-up period of 44 months. This local recurrence rate was dramatically lower than any local endoscopic or surgical approach from the same study.[180] Pancreaticoduodenectomy and pancreas-sparing duodenectomy are appropriate surgical therapies that are believed to substantially reduce the risk of developing periampullary adenocarcinoma.[181,185–187] If such surgical options are considered, preservation of the pylorus will benefit this patient group because most will have undergone a subtotal colectomy with IRA or total colectomy with IPAA. A matched case-control study of 32 people with FAP (all patients had pancreaticoduodenectomy after IPAA) found that pancreaticoduodenectomy did not impact quality of life.[188] As noted in a Northern European study,[20] and others,[189,190] most patients with duodenal adenomas will not develop cancer and can be followed with endoscopy. However, individuals with advanced adenomas (Spigelman stage III or stage IV disease) generally require endoscopic or surgical treatment of the polyps. Chemoprevention studies for duodenal adenomas in FAP patients are under way and may offer an alternate strategy in the future. (Refer to the Chemoprevention section of this summary for more information.)
The endoscopic approach to larger and/or flatter adenomas of the duodenum depends on whether the ampulla is involved. Endoscopic mucosal resection (EMR) after submucosal injection of saline, with or without epinephrine and/or dye, such as indigo carmine, can be employed for nonampullary lesions. Ampullary lesions require even greater care including endoscopic ultrasound evaluation for evidence of bile or pancreatic duct involvement. Stenting of the pancreatic duct is commonly performed to prevent stricturing and pancreatitis. The stents require endoscopic removal at an interval of 1 to 4 weeks. Because the ampulla is tethered at the ductal orifices, it typically does not uniformly lift with injection, so injection is commonly not used. Any consideration of EMR or ampullectomy requires great experience and judgment, with careful consideration of the natural history of untreated lesions and an appreciation of the high rate of adenoma recurrence despite aggressive endoscopic intervention.[82,180,181,186,191–194] The literature uniformly supports duodenectomy for Spigelman stage IV disease. For Spigelman stage II and stage III disease, there is a role for endoscopic treatment invariably focusing on the one or two worst lesions that are present.
Reluctance to consider surgical resection is related to the short-term morbidity and mortality and the long-term complications related to surgery. Although these concerns are likely overstated,[180,181,187,191,195–201] fear of surgical intervention can lead to aggressive and somewhat ill-advised endoscopic interventions. In some circumstances, endoscopic resection of ampullary and/or other duodenal adenomas cannot be accomplished completely or safely by endoscopic means, and duodenectomy cannot be accomplished without risking a short-gut syndrome or cannot be done at all because of mesenteric fibrosis. In such cases, surgical transduodenal ampullectomy/polypectomy can be performed. However, this is associated with a high risk of local recurrence similar to that of endoscopic treatment.
Although level 1 evidence is lacking for the following surveillance methods, they are based on expert opinion. NCCN recommends baseline thyroid ultrasound beginning in the late teenage years to screen for papillary thyroid cancer in patients with FAP, with a repeat ultrasound every 2 to 5 years if results are normal. When individuals have a family history of thyroid cancer, shorter screening intervals can be used.[123,202,203]
Although level 1 evidence is lacking for the following surveillance methods, they are based on expert opinion. NCCN has suggested that the following be considered for children with a predisposition to FAP: liver palpation, abdominal ultrasound, and measurement of serum alpha-fetoprotein every 3 to 6 months for the first 5 years of life.[123,204] It is not necessary to continue screening after age 5 years.
Although level 1 evidence is lacking for the following surveillance methods, they are based on expert opinion. Medulloblastoma is a highly malignant tumor that is usually only symptomatic 6 months or less before diagnosis; annual surveillance of asymptomatic patients may be insufficient. Thus, surveillance by means of regular CT or magnetic resonance imaging (MRI) cannot be advocated. FAP family members who do not yet have polyposis but have signs or symptoms suggestive of a brain tumor should be evaluated with neuroimaging because brain tumors present before polyposis in more than half of FAP patients. Careful evaluation is also important among FAP families in which one member already has a brain tumor because familial clustering occurs. Of such families with FAP-associated brain tumors, 40% had two affected members.[103]
Attenuated Familial Adenomatous Polyposis (AFAP)
Clinical phenotype
AFAP was first described clinically in 1990 in a large kindred with a variable number of adenomas. The average number of adenomas in this kindred was 30, although they ranged in number from a few to hundreds.[205] It has been recommended that the management of AFAP patients include colonoscopy rather than flexible sigmoidoscopy because the adenomas can be predominantly right-sided.[206] Adenomas in AFAP are believed to form around the age of mid-twenties to late twenties.[57] Similar to classic FAP, the risk of CRC is higher in individuals with AFAP; the average age at diagnosis, however, is older than classic FAP at 56 years.[106,107,207] Affected family members have developed CRCs with very few synchronous polyps.[2] Extracolonic manifestations similar to those in classic FAP also occur in AFAP. These manifestations include upper GI polyps (FGPs, duodenal adenomas, and duodenal adenocarcinoma), osteomas, epidermoid cysts, and desmoid tumors.[57] Because of the specific sites of APC pathogenic variants causing AFAP, these patients typically lack CHRPE lesions.
Genetics of AFAP
AFAP is associated with particular subsets of APC pathogenic variants. Three groups of site-specific APC pathogenic variants causing AFAP have been characterized:[106–109,208,209]
Pathogenic variants associated with the 5’ end of APC and exon 4 in which patients can manifest 2 to more than 500 adenomas, including the classic FAP phenotype and upper GI polyps. Any pathogenic variant in the first four exons,[106] as there is an internal ribosomal entry site in exon 4 that permits the ribosome to skip premature truncation pathogenic variants.[210]
Exon 9–associated phenotypes in which patients may have 1 to 150 adenomas but no upper GI manifestations.
3’ region pathogenic variants in which patients have very few adenomas (<50).
In the absence of family history of similarly affected relatives, the differential diagnosis may include AFAP (including MAP), Lynch syndrome, CMMRD, germline variants in the DNA polymerase proofreading subunits (POLD1 or POLE), or an otherwise unclassified sporadic or genetic problem. A careful family history may implicate AFAP or Lynch syndrome.
APC testing is an important component of the evaluation of patients suspected of having AFAP.[206] If germline APC pathogenic variant testing is negative in suspected AFAP individuals, genetic testing for MUTYH, POLE, and POLD1 pathogenic variants may be warranted.[117]
Clinical management
Patients found to have an unusually or unacceptably high adenoma count at an age-appropriate colonoscopy pose a differential diagnostic challenge.[211,212] The role for and timing of risk-reducing colectomy in AFAP is controversial.[213]
Table 7 summarizes the clinical practice guidelines from different professional societies regarding surveillance of AFAP.
Table 7. Clinical Practice Guidelines for Colon Surveillance of Attenuated Familial Adenomatous Polyposis (AFAP)
Organization
Condition
Screening Method
Screening Frequency
Age Screening Initiated
Comment
FDA = U.S. Food and Drug Administration; IPAA = ileal pouch–anal anastomosis; IRA = ileorectal anastomosis; NCCN = National Comprehensive Cancer Network.
aColonoscopy with polypectomy can adequately remove polyps when individuals have a small adenoma burden, which is defined as fewer than 20 adenomas that do not have advanced histology and are each <1 cm in diameter.
Personal history of AFAP with small adenoma burdena
High-quality colonoscopy and polypectomy
Every 1–2 y
If patient had colectomy with IRA, endoscopic evaluation every 6–12 mo, depending on the patient’s polyp burden
Chemoprevention may be considered in patients with progressive polyp burdens to manage the remaining rectum or pouch postcolectomy; at this time, the FDA has not approved medications for this specific indication; NCCN recommends that patients seek the advice of providers with expertise in FAP/AFAP
Personal history of AFAP with adenoma burden that cannot be handled endoscopically
Not applicable
Not applicable
Not applicable
Colectomy with IRA preferred. Consider proctocolectomy with IPAA if patient has dense rectal polyposis
Asymptomatic at-risk family member; familial pathogenic variant known; APC pathogenic variant status positive
High-quality colonoscopy
Every 1–2 y if APC positive
Late teens
If adenomas are found, follow AFAP screening guidelines
Asymptomatic at-risk family member; familial pathogenic variant known; APC pathogenic variant status unknown
High-quality colonoscopy
If genetic testing is not performed, colonoscopy can be done every 2 y; if adenomas are found, follow AFAP screening guidelines; if adenomas are not found on multiple subsequent exams, a prolonged screening interval (>2 y) may be considered
Late teens
Discuss benefits of genetic testing
MUTYH-Associated Polyposis (MAP)
MAP is an autosomal recessively inherited polyposis syndrome caused by pathogenic variants in the Mut Y homolog gene. The Mut Y homolog gene, which is known as MUTYH, was initially called MYH, but was subsequently corrected because the myosin heavy chain gene already had that designation. MUTYH is located on chromosome 1p34.3-32.1.[215] The protein encoded by MUTYH is a base excision repair glycosylase, which repairs one of the most common forms of oxidative damage. Over one hundred unique sequence variants of MUTYH have been reported. A founder pathogenic variant with ethnic differentiation is assumed for MUTYH pathogenic variants. In White populations of northern European descent, two major variants, Y179C and G396D (formerly known as Y165C and G382D), account for 70% of biallelic pathogenic variants in MAP patients; 90% of these patients carry at least one of these pathogenic variants.[216] Other causative variants that have been found include P405L (formerly known as P391L) (Netherlands),[217,218] E480X (India),[219] Y104X (Pakistan),[220] 1395delGGA (Italy),[221,222] 1186-1187insGG (Portugal),[223] and p.A359V (Japan and Korea).[224–226]
The MUTYH gene was first linked to polyposis in 2002 in three siblings with multiple colonic adenomas and CRC but no APC pathogenic variant.[112] MAP has a broad clinical spectrum. Most often it resembles the clinical picture of AFAP, but it has been reported in individuals with phenotypic resemblance to classical FAP and Lynch syndrome.[227] MAP patients tend to develop fewer adenomas at a later age than patients with APC pathogenic variants [228,229] but still carry a high risk of CRC (35%–75%).[7,230,231] A 2012 study of colorectal adenoma burden in 7,225 individuals reported a prevalence of biallelic MUTYH pathogenic variants of 4% (95% CI, 3%–5%) among those with 10 to 19 adenomas, 7% (95% CI, 6%–8%) among those with 20 to 99 adenomas, and 7% (95% CI, 6%–8%) among those with 100 to 999 adenomas.[116] This broad clinical presentation results from the MUTYH gene’s ability to cause disease in its homozygous or compound heterozygous forms. Based on studies from multiple FAP registries, approximately 7% to 19% of patients with an FAP phenotype and without a detectable APC germline pathogenic variant carry biallelic variants in the MUTYH gene.[7,219,229,232]
Adenomas, serrated adenomas, and hyperplastic polyps can be seen in MAP patients.[233] The CRCs tend to be right-sided and synchronous at presentation and seem to carry a better prognosis than sporadic CRC.[215] Clinical management guidelines for MAP recommend screening with high-quality colonoscopy and polypectomy every 1 to 2 years if fewer than 20 adenomas are found. Colonoscopy begins no later than age 25 to 30 years (although screening at a younger age may be considered based on family history).[123,214,230] Upper endoscopic surveillance begins at age 30 to 35 years.[214] (Refer to Table 8 for more information about available clinical practice guidelines for colon surveillance in MAP patients.) The recommended upper endoscopic surveillance interval can be based on the burden of involvement according to Spigelman criteria.[214] Total colectomy with ileorectal anastomosis or subtotal colectomy may be necessary for patients with MAP depending on overall polyp burden.[230,234]
Although MAP is the only known biallelic (recessive) adenoma cancer predisposition syndrome described to date, there are examples of biallelic cases presenting with childhood tumors in which MMR genes are involved. For more information, see the IHC in constitutional mismatch repair deficiency (CMMRD) syndrome section.
Table 8 summarizes the clinical practice guidelines from different professional societies regarding colon surveillance of biallelic MAP.
Table 8. Clinical Practice Guidelines for Colon Surveillance of MUTYH-Associated Polyposis (MAP)
Organization
Condition
Screening Method
Screening Frequency
Age Screening Initiated
Comment
CRC = colorectal cancer; FDR = first-degree relative; IPAA = ileal pouch–anal anastomosis; IRA = ileorectal anastomosis; NCCN = National Comprehensive Cancer Network.
aColonoscopy with polypectomy can adequately remove polyps when individuals have a small adenoma burden, which is defined as fewer than 20 adenomas that do not have advanced histology and are each <1 cm in diameter.
Biallelic MUTYH pathogenic variants; personal history of MAP, small adenoma burdena
High-quality colonoscopy and polypectomy
Every 1–2 y
No later than age 25 to 30 y
If patient had colectomy with IRA, endoscopic evaluation every 6–12 mo, depending on the patient’s polyp burden
Chemoprevention may be considered in certain individuals (especially those with a high polyp burden postcolectomy), but data are limited in patients with MAP; consider referring patients to a center that has experience with MAP to discuss chemoprevention and surgery options
Biallelic MUTYH pathogenic variants; personal history of MAP with adenoma burden that cannot be managed endoscopically
Not applicable
Not applicable
Not applicable
Colectomy with IRA. Consider proctocolectomy with IPAA if patient has dense rectal polyposis. If patient had colectomy with IRA, endoscopic evaluation of the rectum may be done every 6–12 mo based on polyp burden
Asymptomatic, at-risk family member; familial pathogenic variant known; MUTYH pathogenic variant status unknown
High-quality colonoscopy
Every 1–2 y
No later than age 25–30 y
Repeat screening every 1–2 years if polyps are not found; the screening interval can be lengthened if an individual does not have polyps on multiple subsequent colonoscopies, based on a provider’s judgment; if polyps are found, use MAP screening guidelines. Discuss benefits of genetic testing if the patient’s pathogenic variant status is unknown
Asymptomatic, at-risk family member; familial pathogenic variant known; no MUTYH pathogenic variant found
General population screening
One MUTYH pathogenic variant (monoallelic/MUTYH heterozygote); proband has a personal history or an FDR with CRC/colon polyps
Increased frequency of screening based on the patient’s personal or family history of CRC/colon polyps (refer to NCCN guidelines for CRC screening) [235]
One MUTYH pathogenic variant (monoallelic/MUTYH heterozygote); proband does not have a personal history or an FDR with CRC/colon polyps
General population screening
Many extracolonic cancers have been reported in patients with MAP including gastric, small intestinal, endometrial, liver, ovarian, bladder, thyroid, and skin cancers (melanoma, squamous epithelial, and basal cell carcinomas).[236,237] Additionally, noncancerous extracolonic manifestations have been reported in a few MAP patients including lipomas, congenital hypertrophy of the retinal pigment epithelium, osteomas, and desmoid tumors.[221,229,237,238] Female MAP patients have an increased risk of breast cancer.[239] These extracolonic manifestations seem to occur less frequently in MAP than in FAP, AFAP, or Lynch syndrome.[240,241]
Duodenal polyps in MAP
Similar to FAP, individuals with MAP often develop duodenal adenomas, and are at risk of developing duodenal cancer. Given the relatively recent identification of MAP compared with FAP, the incidence of duodenal polyps and risk of duodenal cancer in MAP is less well defined. Small case series have suggested the incidence of duodenal polyps in MAP to be approximately 30%, considerably lower than that of FAP. In a registry-based study the prevalence of duodenal polyps was 17%; however, only 50% of individuals in this study had undergone an upper GI endoscopy, suggesting the incidence of duodenal polyps was likely underestimated. The lifetime risk of duodenal cancer was estimated to be 4%.[237]
A registry study from the United Kingdom and the Netherlands explored incidence of duodenal polyps and duodenal cancer in a group of patients with MAP who were undergoing regular duodenal surveillance.[242] Of 92 patients, 31 (34%) had evidence of duodenal polyps. The median age at duodenal adenoma detection was 50 years, and in 65% of patients, duodenal adenomas were diagnosed at baseline endoscopy. Eighty-four percent of patients had Spiegelman stage I or stage II polyposis at first detection of polyps, with no patients with stage IV polyposis and no high-grade dysplasia detected. In subsequent surveillance only two patients progressed to Spiegelman stage IV polyposis, after 3.6 and 7.0 years, respectively. There additionally appeared to be sparing of the ampulla, with only two individuals having diminutive polyps without dysplasia in the ampulla. No cancers were detected in patients enrolled in upper GI surveillance programs within these registries. Two individuals with MAP were diagnosed with ampullary and duodenal cancer respectively at ages 83 and 63 years at the time of first-ever upper GI endoscopies. Therefore, duodenal polyps appear less frequently in MAP when compared with FAP; duodenal polyps also appear at a later age in MAP. Based on these results, the authors suggest upper GI endoscopic screening in MAP be initiated at age 35 years.
Because MAP has an autosomal recessive inheritance pattern, siblings of an affected patient have a 25% chance of also carrying biallelic MUTYH pathogenic variants and should be offered genetic testing. Similarly, testing can be offered to the partner of an affected patient so that the risk in their children can be assessed.
The clinical phenotype of monoallelic MUTYH pathogenic variants is less well characterized with respect to incidence and associated clinical phenotypes, and its role in susceptibility to polyposis and colorectal carcinoma remains unclear. Approximately 1% to 2% of the general population carry a pathogenic variant in MUTYH.[7,112,229] A 2011 meta-analysis found that carriers of monoallelic MUTYH pathogenic variants are at modestly increased risk of CRC (odds ratio [OR], 1.15; 95% CI, 0.98–1.36); however, given the rarity of carriers of monoallelic pathogenic variants, they account for only a trivial proportion of all CRC cases.[243] A large study of 2,332 heterozygotes among 9,504 relatives of 264 CRC cases with a MUTYH pathogenic variant found that the risk of CRC at age 70 years was 7.2% for men and 5.6% for women, irrespective of family history. Among those with an FDR with a CRC diagnosis before age 50 years, the risk at age 70 years was 12.5% for men and 10% for women.[231] Caution should be exercised in the interpretation of this study as the vast majority of carrier status from this study was imputed and not based on genotype. The authors felt the risk for MUTYH heterozygotes with an FDR with CRC was sufficiently high to warrant more intensive surveillance than the general population (but the same as for anyone with an FDR with CRC diagnosed before age 50 y).[228,231]
MMR genes may interact with MUTYH and increase the risk of CRC. An association between MUTYH and MSH6 has been reported. Both proteins interact together in base excision repair processes. A study reported a significant increase of MSH6 pathogenic variants in carriers of monoallelic MUTYH pathogenic variants with CRC compared with noncarriers with CRC (11.5% vs. 0%; P = .037).[244] However, a German study failed to duplicate these findings.[245] Additionally, a larger study found no increased cancer risk for carriers of MMR pathogenic variants with a MUTYH variant compared with those with a MMR pathogenic variant alone.[246]
Lynch Syndrome
Introduction
Lynch syndrome is the most common inherited CRC syndrome and accounts for approximately 3% of all newly diagnosed cases of CRC. It is an autosomal dominant condition caused by pathogenic variants in the MMR genes MLH1 (mutL homolog 1), MSH2 (mutS homolog 2), MSH6 (mutS homolog 6), and PMS2 (postmeiotic segregation 2), as well as the gene EPCAM (epithelial cellular adhesion molecule, formerly known as TACSTD1), in which deletions in EPCAM cause epigenetic silencing of MSH2. Lynch syndrome is also associated with a predisposition for developing several extracolonic manifestations, including sebaceous adenomas and cancers of the endometrium and ovaries, stomach, small intestine, transitional cell carcinoma of the ureters and renal pelvis, hepatobiliary system, pancreas, and brain. Lynch syndrome–associated cancers exhibit MSI; therefore, tumor testing is a key component in the diagnosis of Lynch syndrome, in addition to family history. Universal tumor testing of all CRCs is now recommended as a strategy to screen for Lynch syndrome and identify those individuals who may subsequently benefit from germline genetic testing. Intensive cancer screening and surveillance strategies, including frequent colonoscopy, along with risk-reducing surgeries, are mainstays in patients with Lynch syndrome.
History of Lynch syndrome
Between 1913 and 1993, numerous case reports of families with apparent increases in CRC were reported. As series of such reports accumulated, certain characteristic clinical features emerged: early age at onset of CRC; high risk of synchronous (and metachronous) colorectal tumors; preferential involvement of the right colon; improved clinical outcome; and a range of associated extracolonic sites including the endometrium, ovaries, other sites in the GI tract, uroepithelium, brain, and skin (sebaceous tumors). Terms such as cancer family syndrome and hereditary nonpolyposis colorectal cancer (HNPCC) were used to describe this entity.[247]
The term Lynch syndrome replaced HNPCC and is applied to cases in which the genetic basis can be confidently linked to a germline pathogenic variant in a DNA MMR gene. Moreover, HNPCC is misleading as many patients have polyps and many have tumors other than CRC.
With the increased recognition of families that were considered to have a genetic predisposition to the development of CRC, research for a causative etiology led to the development of the Amsterdam criteria in 1990.[248] The Amsterdam criteria were originally used for the identification of high-risk families and included fulfillment of all of the following: three or more cases of CRC over two or more generations, with at least one diagnosed before age 50 years, and no evidence of FAP.
In 1987, a chromosomal deletion of a small segment of 5q led to the detection of a genetic linkage between FAP and this genomic region,[249] from which the APC gene was eventually cloned in 1991.[250] This led to searches for similar linkage in families suspected of having Lynch syndrome who had multiple cases of CRC inherited in an autosomal dominant fashion and young onset of cancer development. The APC gene was one of several genes (along with DCC and MCC) evaluated in families that fulfilled Amsterdam criteria, but no linkage was found among the Lynch kindreds. In 1993, an extended genome-wide search resulted in the recognition of a candidate chromosome 2 susceptibility locus in large families. Once MSH2, the first Lynch syndrome–associated gene, was sequenced, it was evident from the somatic variant patterns in the CRC tumors that the MMR family of genes was likely involved. Additional MMR genes were subsequently linked to Lynch syndrome, including MLH1, MSH6, and PMS2. Lynch syndrome now refers to the genetic disorder caused by a germline variant in one of these DNA MMR genes, distinguishing it from other familial clusters of CRC.
In 2009, a germline deletion in the EPCAM gene was identified as another cause of MSH2 inactivation in the absence of a germline pathogenic variant in MSH2. The variant in EPCAM led to hypermethylation of the MSH2 promoter. Thus, EPCAM, which is not a DNA MMR gene, is also implicated in Lynch syndrome and is now routinely tested in at-risk patients along with the DNA MMR genes listed above.
Defining Lynch syndrome families
Families with a preponderance of CRC and a possible genetic predisposition were initially categorized as having Lynch syndrome based on family history criteria, as well as personal history of young-onset CRC. With the advent of molecular tumor diagnostic testing and the discovery of the germline alterations associated with Lynch syndrome, the clinical criteria have currently fallen out of favor due to their underperformance. However, their use, or the risk estimates provided by the Lynch syndrome prediction models, may be applicable among individuals without personal history of cancer but with a family history suggestive of Lynch syndrome, or for those individuals with CRC but without available tumor for molecular diagnostic testing. (Refer to the Universal tumor testing to screen for Lynch syndrome and the Clinical risk assessment models that predict the likelihood of an MMR gene pathogenic variant sections of this summary for more information.)
The first criteria for defining Lynch syndrome families were established by the International Collaborative Group meeting in Amsterdam in 1990 and are known as the Amsterdam criteria.[248] These research criteria were limited to diagnoses of familial CRC. In 1999, the Amsterdam criteria were revised to include some extracolonic cancers, predominantly endometrial cancer.[251] These criteria provide a general approach to identifying Lynch syndrome families, but they are not considered comprehensive; nearly half of families meeting the Amsterdam criteria do not have detectable pathogenic variants.[252]
Amsterdam criteria I (1990):
One family member diagnosed with CRC before age 50 years.
Two affected generations.
Three affected relatives, one of them an FDR of the other two.
FAP should be excluded.
Tumors should be verified by pathological examination.
Amsterdam criteria II (1999):
Same as Amsterdam criteria I, but tumors of the endometrium, small bowel, ureter, or renal pelvis can be used to substitute an otherwise qualifying CRC.
These criteria were subsequently used beyond research purposes to identify potential candidates for microsatellite and germline testing. However, the Amsterdam criteria failed to identify a substantial proportion of Lynch syndrome kindreds; families that fulfilled Amsterdam criteria I but did not have evidence of MSI and were without a pathogenic germline variant in a DNA MMR gene, were referred to as familial colorectal cancer type X (FCCX).
With the hallmark feature of MSI associated with Lynch syndrome tumors, and the limitations of the Amsterdam criteria related to low sensitivity, the Bethesda guidelines were introduced in 1997. The Bethesda guidelines are a combination of clinical, histopathologic, and family cancer history features that identify cases of CRC that warrant MSI tumor screening. The Bethesda guidelines (with a subsequent revision in 2004) were formulated to target patients in whom evaluation of CRC tumors for MMR deficiency should be considered, and to improve the sensitivity of clinical criteria used to identify individuals who are candidates for mutational DNA analysis.[253,254] (Refer to the Genetic and molecular testing for Lynch syndrome section of this summary for more information about testing for MSI and IHC.)
Bethesda guidelines (1997):
Cancer in families that meet the Amsterdam criteria.
The presence of two Lynch syndrome–related cancers, including synchronous and metachronous CRCs or associated extracolonic cancers. [Note: Endometrial, ovarian, gastric, hepatobiliary, or small-bowel cancer or transitional cell carcinoma of the renal pelvis or ureter.]
The presence of CRC and an FDR with CRC and/or Lynch syndrome–related extracolonic cancer and/or a colorectal adenoma; one of the cancers diagnosed before age 45 years, and the adenoma diagnosed before age 40 years.
CRC or endometrial cancer diagnosed before age 45 years.
Right-sided CRC with an undifferentiated pattern (solid/cribriform) on histopathology diagnosed before age 45 years. [Note: Solid/cribriform defined as poorly differentiated or undifferentiated carcinoma composed of irregular, solid sheets of large eosinophilic cells and containing small gland-like spaces.]
Signet-ring–cell CRC diagnosed before age 45 years. [Note: Composed of more than 50% signet ring cells.]
Adenomas diagnosed before age 40 years.
Revised Bethesda guidelines (2004)*:
CRC diagnosed in an individual younger than 50 years.
Presence of synchronous, metachronous colorectal, or other Lynch syndrome–associated tumors.**
CRC with MSI-high (MSI-H) pathological associated features diagnosed in an individual younger than 60 years. [Note: Presence of tumor-infiltrating lymphocytes, Crohn-like lymphocytic reaction, mucinous/signet-ring differentiation, or medullary growth pattern.]
CRC or Lynch syndrome–associated tumor** diagnosed in at least one FDR younger than 50 years.
CRC or Lynch syndrome–associated tumor** diagnosed at any age in two FDRs or second-degree relatives (SDRs).
*One criterion must be met for the tumor to be considered for MSI testing.
**Lynch syndrome–associated tumors include colorectal, endometrial, stomach, ovarian, pancreatic, ureter and renal pelvis, biliary tract, and brain tumors; sebaceous gland adenomas and keratoacanthomas in Muir-Torre syndrome; and carcinoma of the small bowel.[254,255]
Although the Bethesda guidelines were able to identify a higher proportion of Lynch syndrome carriers than the Amsterdam criteria, they still missed approximately 30% of Lynch syndrome families.[256] Furthermore, the Bethesda guidelines were not consistently used in clinical practice to identify the subset of individuals with CRC who should have MSI tumor testing; the guidelines were deemed cumbersome and difficult to remember by health care providers and the opportunity to refer for genetic evaluation was missed.[257]
With the advent of alternative approaches, including universal testing of all newly diagnosed cases of CRC for MSI (regardless of age at diagnosis or family history of cancer), clinical criteria for Lynch syndrome have been rendered obsolete. While the Bethesda guidelines were intended for individuals with cancer, their performance in individuals unaffected by cancer may still be of use. Given the limited modalities available to assess unaffected individuals for Lynch syndrome, family history and the use of clinical criteria may be appropriate in identifying those who warrant further genetic evaluation and testing.
Clinical risk assessment models that predict the likelihood of an MMR gene pathogenic variant
Because health care providers ineffectively use clinical criteria to select individuals with CRC for genetic referral and evaluation for Lynch syndrome, computer-based clinical prediction models were developed and introduced in 2006 as alternative modalities to provide systematic genetic risk assessment for Lynch syndrome. The risk models include the PREMM (PREdiction Model for gene Mutations) models, MMRpredict, and MMRpro.[258–261]
Four models (PREMM[1,2,6], PREMMplus, MMRpredict, and MMRpro) quantify an individual’s probability of carrying a pathogenic variant in one of the following MMR genes: MLH1, MSH2, and MSH6. The PREMM(1,2,6) model was subsequently extended to include prediction of pathogenic PMS2 and EPCAM variants (PREMM5).[261] While PREMM5, MMRpredict, and MMRpro are specific to Lynch syndrome, PREMMplus quantifies an individual’s risk of having a pathogenic variant in one of 19 genes (including all five Lynch syndrome genes).[262] However, it is unclear if one of these models is preferred for predicting when an individual has Lynch syndrome.
While the models were all created for the same purpose, they differ in the way they were developed and the variables used to predict risk. In addition, the populations in which they were validated reveal each model’s specific characteristics that may impact accuracy.[262–272] Deciding on which model to use in the risk assessment process depends on both the clinical setting in which it is applied and the patient population that is being evaluated. MMRpro’s predictions account for family size and unaffected relatives, the possibility of including molecular tumor data in the risk analysis, and the option of predicting pathogenic variant carrier status following germline testing. The major limitation in the widespread use of MMRpro in routine practice is the need to input data from the entire pedigree (including individuals without cancer), which is relatively time-consuming. Its best use is likely to be as a genetic counseling tool in a specialized high-risk clinic or research setting, as its accessibility is also limited. PREMM’s major advantages include that it is easy to use, available as an online tool, and has been extensively validated, including in a self-administered setting in a GI clinic.[273] It includes risk prediction based on personal and family cancer history up to SDRs for a broad spectrum of extracolonic cancers. However, the model does not consider family size and may overestimate the likelihood of a pathogenic variant in a pedigree that includes multiple elderly family members who are unaffected by CRC or endometrial cancer. Given the ease with which one can use the PREMM model (it has been deemed less time-consuming than MMRpro in validation studies),[268] it may be used by diverse health care providers whose primary aim is to identify patients who should be referred for genetic evaluation, and is likely to be most useful in the pretesting decision-making process. MMRpredict’s use may be limited overall because of its less accurate risk estimates [274] when used to evaluate families with Lynch syndrome–associated cancers and older individuals affected by CRC; the model was developed using data from young-onset CRC cases (patients diagnosed at age <55 y) and did not include extracolonic malignancies. Furthermore, the model does not incorporate tumor testing results or provide post-hoc risk estimates based on gene sequencing results. Lastly, PREMMplus assesses the likelihood of finding a pathogenic variant on a multigene panel of 19 high- and moderate-penetrance genes, and it is not limited to genes associated with CRC.[262]
Overall, there is ample evidence that each of the models has superior performance characteristics of sensitivity, specificity, and positive and negative predictive values that support their use when compared with the existing clinical guidelines for diagnosis and evaluation of Lynch syndrome. Because of the diverse clinical settings in which a health care provider could assess an individual for Lynch syndrome, prediction models offer a potentially feasible and useful strategy to systematically identify at-risk individuals, whether or not they are affected with CRC.
Summary
In conclusion, the presence of tumor MSI in CRCs, along with a compelling personal and family history of cancer, warrants germline genetic testing for Lynch syndrome, and most clinical practice guidelines provide for such an approach. These guidelines combine genetic counseling and testing strategies with clinical screening and treatment measures. Providers and patients alike can use these guidelines to better understand available options and key decisions. (Refer to Table 13 for more information about practice guidelines for diagnosis and colon surveillance in Lynch syndrome.)
Genetics of Lynch syndrome
The genetics of both the tumor and the germline have an important role in the development and diagnosis of Lynch syndrome. Tumor DNA in Lynch syndrome–associated tumors exhibits characteristic MSI, and in these cases, there is typically loss of IHC expression for one or more of the proteins associated with the MMR genes. Molecular testing with MSI and/or IHC has been adopted as a universal screen for diagnosis of Lynch syndrome in newly diagnosed patients with CRC and endometrial cancer. IHC testing results can potentially direct gene-specific germline testing. Many genetic testing laboratories offer multigene (panel) tests that simultaneously test for pathogenic variants in all of the Lynch syndrome–associated genes (and often additional genes associated with inherited cancer susceptibility).
Genetic and molecular testing for Lynch syndrome
MSI
The presence of MSI in colorectal tumor specimens is a hallmark feature of Lynch syndrome and can be cause for suspicion of a germline pathogenic MMR gene variant. Microsatellites are short, repetitive sequences of DNA (mononucleotides, dinucleotides, trinucleotides, or tetranucleotides) located throughout the genome, primarily in intronic or intergenic sequences.[275,276] The term MSI is used when colorectal, endometrial, or metastatic tumor DNA [277] shows insertions or deletions in microsatellite regions when compared with normal tissue. MSI indicates probable defects in MMR genes, which may be due to somatic variants, germline variants, or epigenetic alterations.[278] In most instances, MSI is associated with absence of protein expression of one or more of the MMR proteins (MSH2, MLH1, MSH6, and PMS2). However, loss of protein expression may not be seen in all tumors with MSI and not all tumors with loss of protein expression on IHC will be microsatellite unstable.
Certain histopathologic features are strongly suggestive of MSI phenotype, including the presence of tumor-infiltrating lymphocytes (refer to Figure 4), Crohn-like reaction, mucinous histology, and histological heterogeneity.[279]
EnlargeFigure 4. Tumor-infiltrating lymphocytes are a histopathologic feature suggestive of microsatellite instability.
Initial designation of a colorectal adenocarcinoma as microsatellite unstable was based on the detection of a specified percentage of unstable loci from a panel of three dinucleotide and two mononucleotide repeats that were selected at a National Institutes of Health (NIH) Consensus Conference and referred to as the Bethesda panel. If more than 30% of a tumor’s markers were unstable, it was scored as MSI-H; if at least one, but fewer than 30% of markers were unstable, the tumor was designated MSI-low (MSI-L). If no loci were unstable, the tumor was designated microsatellite stable (MSS). Most tumors arising in the setting of Lynch syndrome will be MSI-H.[280] The clinical relevance of MSI-L tumors remains controversial; the probability is very small that these tumors are associated with a germline pathogenic variant in an MMR gene.
The original Bethesda panel has been replaced by a pentaplex panel of five mononucleotide repeats,[280] which has improved the detection of MSI-H tumors.
(Refer to the Universal tumor testing to screen for Lynch syndrome section of this summary for information about the utilization of MSI status in the diagnostic workup of a patient with suspected Lynch syndrome.)
IHC
IHC methods are cheaper, easier to understand, and more widely available as a surrogate for MSI and, for these reasons, have replaced polymerase chain reaction (PCR)–based MSI testing in most institutions. IHC is performed in the colorectal or endometrial tumor (or metastatic sites) [277] for protein expression using monoclonal antibodies for the MLH1, MSH2, MSH6, and PMS2 proteins. Isolated loss of expression of any one of these proteins may suggest which specific MMR gene is altered in a particular patient.[281–284] However, certain proteins can form heterodimers (or have other binding partners) and yield loss of two proteins expressed on IHC.
MSI can lead to nucleotide-pairing slippage (looping) in which single nucleotide mispairs are introduced. Heterodimers of MMR proteins are formed to identify the errors and bind the DNA at these sites.[278,285] For example, MSH2 protein complexes with MSH6 protein to form MutSα, which has the main ability to repair single base pair mismatches and single base pair loop-out lesions that can occur during the replication of a mononucleotide repeat sequence. In the absence of MSH6 protein, the MSH2 protein will dimerize with the MSH3 protein forming the MutSβ complex, which can trigger repair of larger loop-out DNA mismatches, but also has some overlapping activity to repair lesions usually repaired by MutSα.
EnlargeFigure 5. Immunohistochemical tumor testing for protein expression of the mismatch repair genes associated with Lynch syndrome, depicted for a single patient with colorectal cancer. Protein expression is preserved for MSH2 and MSH6 (inset) and absent for MLH1 and PMS2 (inset). Absence of MMR protein expression is suggestive of Lynch syndrome and warrants additional evaluation.
As a result, when the germline pathogenic variant is in the MSH2 gene, the tumor IHC may not express both MSH2 and MSH6, as the latter protein requires binding to MSH2 for stability. In this case, if no pathogenic variant is found in either gene, germline pathogenic variant testing for EPCAM should be considered if it was not already included. Approximately 20% of patients with absence of MSH2 and MSH6 protein expression by IHC and no MSH2 or MSH6 pathogenic variant identified will have germline deletions in EPCAM.[286] The latter mechanism accounts for approximately 5% of all Lynch syndrome cases.[286] A deletion of one exon 9 allele in the EPCAM (TACSTD1) gene, which is immediately upstream of MSH2‘s start site and in the same orientation, can lead to transcriptional read-through and methylation of the MSH2 promoter. This can lead to subsequent silencing of MSH2 in any tissue that expresses EPCAM. The presence of EPCAM pathogenic variants showing similar methylation-mediated MSH2 loss has been reported in numerous families.[287] On the strength of these observations, germline EPCAM testing is performed in patients with loss of MSH2 protein expression on IHC testing of their CRCs but who lack a detectable MSH2 germline pathogenic variant and is included with MSH2 testing in all colon cancer gene panels. For more information, see the EPCAM section.
Similarly, the loss of MLH1 (either by germline pathogenic variant or hypermethylation of the MLH1 promoter) results in the absence of expression of both MLH1 and PMS2 proteins in the tumor. The most common abnormal IHC pattern for DNA MMR proteins in colorectal adenocarcinomas is loss of expression of MLH1 and PMS2. PMS2 and MLH1 function as a stable heterodimer known as MutLα. MutLα binds to MutSβ and guides excision repair of the newly synthesized DNA strand.[278] A functional defect in MLH1 results in degradation of both MLH1 and PMS2, while a defect in PMS2 negatively affects only PMS2 expression. Thus, a loss of MLH1 and PMS2 indicates that there is an alteration in MLH1 (promoter hypermethylation or germline variant), while loss of PMS2 expression often indicates that there is a germline PMS2 variant. However, among 88 individuals with PMS2-deficient CRC, PMS2 germline pathogenic variant testing followed by MLH1 germline pathogenic variant testing revealed pathogenic PMS2 variants in 49 individuals (74%) and MLH1 pathogenic variants in 8 individuals (12%).[288] Eighty-three percent of the alterations in MLH1 were missense variants, but two relatives carried identical MLH1 variants, and one individual, who developed two tumors with retained MLH1 expression, carried an intronic variant that led to skipping of exon 8.[288] Therefore, in CRCs with solitary loss of PMS2 expression, an MLH1 germline pathogenic variant should be sought if no PMS2 germline variant is found. Tumors with MSI and loss of MSH2 and MSH6 protein expression are generally indicative of an underlying MSH2 germline variant (inferred MSH2 pathogenic variant). Unlike the case with MLH1, MSI with MSH2 loss is rarely associated with somatic hypermethylation of the promoter.
Unlike MLH1 and MSH2 (which both dimerize with other proteins or have other binding partners), germline pathogenic variants in MSH6 and PMS2 result in the isolated loss of those specific proteins by IHC. However, tumors from MSH6 pathogenic variant carriers may not display the MSI phenotype at a frequency as high as MLH1 and MSH2 carriers (despite an inactive DNA MMR system), as there are pathogenic missense variants that do not completely abrogate protein expression yielding false negative results by IHC testing.[267,289] In a study that reported tumor testing results among MMR germline carriers enrolled through the Colon Cancer Family Registry, 7 of 24 carriers (28%) with MSH6 pathogenic variants had tumors that displayed normal protein expression on IHC staining. IHC tumor testing was more informative for MLH1 and MSH2 pathogenic variant carriers in which 93% of MLH1 carriers had correlating loss of MLH1 protein expression and 96% of MSH2 carriers had loss of MSH2 protein expression.[267]
In some cases, tumors manifest MSI and/or IHC shows loss of DNA MMR protein expression, but no germline pathogenic variant is identified. This tumor phenotype is predominantly due to biallelic somatic inactivation of the DNA MMR genes and is not a pathogenic germline alteration. This phenomenon has been labeled Lynch-like syndrome (sometimes called LLS in the literature), although this terminology may cause confusion since this term represents a mechanism of sporadic carcinogenesis, rather than a stand-alone genetic syndrome. For more information, see the Somatic biallelic mismatch repair deficiency (sometimes called Lynch-like syndrome) section.
Table 9. Protein Loss and Potential Germline Defect(s)
Loss of Protein Expression
Germline MMR Defect Predicted by IHC Protein Expression Loss
It is important to recognize that hypermethylation of the MLH1 promoter, a somatic event confined to the tumor, can lead to abnormal protein expression of MLH1 on IHC. Approximately 10% to 15% of sporadic CRC cases have a microsatellite unstable tumor phenotype due to MLH1 hypermethylation and are not heritable. These sporadic MSI colon cancers [290] have a generalized excess of DNA methylation referred to as CIMP.[291] (Refer to the CIMP and the serrated polyposis pathway section in the Introduction section of this summary for more information.) Because loss of MLH1 protein expression on IHC occurs in both Lynch syndrome and sporadic tumors, its specificity for predicting germline MMR gene variants is lower than for the other MMR proteins, and additional molecular testing is often necessary to clarify the etiology of MLH1 absence.
BRAF pathogenic variants have been detected in 68% of CRC tumors with MLH1 promoter hypermethylation and very rarely, if ever, in CRC from patients with Lynch syndrome.[292–295] This suggests that detection of somatic BRAF V600E variant detection in CRC may be useful in excluding individuals from germline variant testing. As a result, BRAF V600 testing and/or MLH1 hypermethylation assays are increasingly used in universal Lynch syndrome–testing algorithms in an attempt to distinguish between an absence of MLH1 protein expression caused by hypermethylation and germline MLH1 pathogenic variants. Making such a distinction is also a more cost-effective approach in excluding individuals from germline testing.
Somatic biallelic mismatch repair deficiency (sometimes called Lynch-like syndrome)
Prior to the widespread use of somatic tumor sequencing, somatic MLH1 hypermethylation was thought to be the only major sporadic pathway for a tumor to have MSI-H/MMR-deficient (MMR-D) biology. It was presumed that any MSI-H/MMR-D CRC or endometrial cancer with patterns of MMR deficiency (other than MLH1/PMS2 loss) was due to Lynch syndrome, even if a germline pathogenic variant in an MMR gene could not be identified. However, as IHC is more routinely performed for all CRCs and endometrial cancers, it has become clear that other patterns of MMR deficiency can arise via sporadic mechanisms, typically by somatic biallelic MMR gene inactivation.[296] This phenomenon has been labeled Lynch-like syndrome (sometimes called LLS in the literature), although this terminology may cause confusion since this term represents a mechanism of sporadic carcinogenesis, rather than a stand-alone genetic syndrome.
Work from the Ohio Colorectal Cancer Prevention Initiative found that 88.4% of CRCs and 100% of endometrial cancers with unexplained MMR-D statuses (i.e., cancers did not have a germline pathogenic variant in an MMR gene or MLH1 promoter hypermethylation) had somatic biallelic MMR deficiency found on somatic tumor sequencing.[297,298] In an additional series of MMR-D cancers (mostly CRCs and endometrial cancers) that underwent paired germline and somatic MMR variant analyses, somatic biallelic genetic alterations were found in 49% of the tumors that lacked causal germline pathogenic variants, MLH1 promoter hypermethylation, and BRAF V600E variants.[299]
When CRCs, endometrial cancers, or other tumors have unexplained MMR-deficiency, in which somatic sequencing fails to identify somatic biallelic MMR deficiency, it is possible that a small fraction of these cases could represent occult Lynch syndrome (or other forms of unidentifiable inherited cancer risk). In these cases, it is recommended that patients’ clinical and family histories be carefully examined for possible inherited cancer risk. This will help determine if patients and their families will be clinically managed as if they have suspected Lynch syndrome. In these cases, careful scrutiny of any germline MMR gene VUS is also warranted to assess whether these VUSs could harbor pathogenicity. For more information about VUS genetic test results, see the Value of testing an affected family member first section in Cancer Genetics Risk Assessment and Counseling.
Some studies have attempted to define the risk of CRC and other Lynch syndrome–associated malignancies in cohorts of individuals with Lynch-like syndrome. However, the ability to clinically interpret these data may be limited since these populations presumably include a mix of individuals with sporadic MMR-D cancers and others with inherited cancer risk.[300,301]
IHC in constitutional mismatch repair deficiency (CMMRD) syndrome
In contrast with Lynch syndrome (which is defined by the presence of a single, germline, heterozygous, deleterious variant in an MMR gene), rarely, individuals can have deleterious germline variants in both alleles of the same MMR gene. These cases can present with homozygous or compound heterozygous genotypes. This is termed biallelic mismatch repair deficiency (BMMRD) or constitutional mismatch repair deficiency (CMMRD). The likelihood of CMMRD involving homozygous MMR gene pathogenic variants will inevitably be higher among consanguineous unions. Rates of consanguinity may be higher in rural and geographically and/or culturally isolated populations.[302]
Tumor studies yield characteristic abnormalities. In a series of 28 patients with CMMRD,[115] 17 brain tumors showed loss of staining for MMR protein in normal stromal cells and in neoplastic cells. This differs from tumors in patients with Lynch syndrome, in which normal staining is retained in nontumor cells. In contrast to this characteristic feature seen with IHC, PCR-based MSI analysis was not reliable, as 20 of 28 tumors from patients with CMMRD were MSS. Essentially all of the MSI-H tumors were colon cancers.
The PMS2 gene is markedly overrepresented in cases of CMMRD. It has been suggested that the presence of homozygosity in other MMR gene variants is a prenatally lethal state, while milder expression of PMS2 variants is consistent with survival when present in both parental alleles.
For more information about CMMRD’s clinical phenotype, see the CMMRD section.
Table 10. Hereditary Colorectal Cancer (CRC) Syndromes and Associated Tumor Phenotypesa
Sporadic CRC with hypermethylation of MLH1 promoter
Absent
+BRAF
MSI
CMMRD
Present in two alleles
Absent
MSI (tumor and normal tissue)
Somatic biallelic MMR deficiency (sometimes called Lynch-like syndrome)
Absent
Present in two alleles
MSI
FCCX
Absent
Absent
MSS
Constitutional epimutation
While somatic hypermethylation of the MLH1 promoter is acquired and not uncommon, examples of MLH1 promoter hypermethylation have been described in the germline and are generally not associated with a stable Mendelian inheritance. This constitutional methylation of MMR genes occurs most often in MLH1 and, to a lesser extent, MSH2 and is termed constitutional epimutation.[303] A constitutional epimutation (also referred to as a primary epimutation) is an acquired alteration in normal tissue that silences an active gene or activates an inactive gene.[304] Such epimutations occur most often in maternal alleles. In some cases, all somatic cells appear involved, while in others there is evidence of mosaicism. Tumors in patients with primary epimutations are generally indistinguishable from those otherwise typical of Lynch syndrome germline variant carriers, including age at onset, tumor spectrum, and presence of abnormal MSI and IHC. Since these are not inherited in a Mendelian fashion, antecedent family history of tumors is minimal, and risk to offspring somewhat unpredictable. Epimutations present in a de novo case seem to typically be “erased” in the process of gametogenesis and to not be passed to the next generation. Very rare cases of inherited MLH1 epimutations have been reported.[305,306]
Interpreting molecular alterations in tumors and distinguishing the likely primary epimutation cases from those of sporadic MSI poses significant challenges. Most instances of absence of MLH1 expression are caused by the sporadic hypermethylation of the MLH1 promoter. Rare instances of a de novo constitutional epimutation in MLH1 [307] or an inherited germline MLH1 methylation [308] add some complexity to the interpretation of MSI associated with absence of MLH1 expression. Akin to sporadic MSI, primary epimutation tumors show methylation of the MLH1 promotor and may show BRAF variants as well. As noted above, family history of cancer in such cases tends to be minimal or absent, as in true sporadic MSI. Distinguishing such cases from sporadic cases may call for assaying normal tissue (e.g., blood or normal colon mucosa) for evidence of MLH1 methylation, which will be absent from true sporadic cases and absent from carriers of conventional Lynch syndrome MMR pathogenic variants.
Such MLH1-predominant primary epimutations are to be distinguished from secondary epimutations such as those occurring when MSH2 is methylated as a consequence of inherited variants in the upstream EPCAM gene. (Refer to the EPCAM section of this summary for more information.)
Molecular diagnostic tumor testing to screen for Lynch syndrome in clinical practice
While many molecular pathology laboratories can assess both MSI and IHC, an approach that uses IHC testing as the initial screen for defective MMR activity has been favored because it is less labor intensive and more cost-effective.[309,310] Part of this rationale is that the information provided by IHC may target germline genetic testing toward one specific MMR gene (with the exception of loss of MLH1 expression) as opposed to a comprehensive testing strategy of all Lynch syndrome–related MMR genes that would be directed by the use of MSI alone.[256,309,311–314] While MSI testing was originally favored in the oncologic evaluation of individuals with CRC for its prognostic and therapeutic implications, screening for Lynch syndrome can be more effectively directed by IHC testing.
Universal tumor testing to screen for Lynch syndrome
Use of MSI and/or IHC testing in all newly diagnosed cases of CRC, regardless of the age at diagnosis or family history of cancer, increases the sensitivity of the initial screen for Lynch syndrome. This approach is more sensitive than existing clinical criteria, as many individuals with Lynch syndrome are diagnosed at older ages (>50 y) and have less striking family histories of CRC than previously appreciated. This universal testing of colorectal (and endometrial) tumors using either MSI or IHC testing has been recommended by many professional organizations and is being widely adopted.[123,315–318]
Genetic risk assessment and MMR gene variant testing in individuals with newly diagnosed CRC can lead to improved outcomes for the patient and at-risk family members. Dating back to 2009, the Evaluation of Genomic Applications in Practice and Prevention (EGAPP), a project developed by the Office of Public Health Genomics at the Centers for Disease Control and Prevention (CDC), reported that there was sufficient evidence to recommend offering tumor screening for Lynch syndrome to individuals with newly diagnosed CRC to reduce morbidity and mortality in relatives.[319,320] At that time, there was insufficient evidence to recommend a specific testing strategy between MSI and IHC.
Several studies have demonstrated the feasibility of universal screening for Lynch syndrome. Initial experience from one institution found that among 1,566 patients screened using MSI and IHC, 44 patients (2.8%) had Lynch syndrome. For each proband, an average of three additional family members were subsequently diagnosed with Lynch syndrome.[256] A subsequent pooled analysis of 10,206 incident CRC patients tested with MSI/IHC as part of four large studies revealed a pathogenic variant detection rate of 3.1%.[321] This study compared four strategies for tumor testing for the diagnosis of Lynch syndrome: (1) testing all individuals meeting at least one criterion of the Bethesda guidelines; (2) testing all individuals meeting Jerusalem recommendations;[322] (3) testing all individuals with CRC aged 70 years or younger, or older than 70 and meeting at least one criterion of the Bethesda guidelines; and (4) universal testing of all individuals with CRC.[321] Tumor testing with MSI involved panels individualized at each institution and IHC involved testing all four of the DNA MMR genes involved with Lynch syndrome, across all institutions. The strategy of tumor testing in all individuals diagnosed with CRC at age 70 years or younger and testing individuals over age 70 who met one of the revised Bethesda guidelines yielded a sensitivity of 95.1%, a specificity of 95.5%, and a diagnostic yield of 2.1%. This strategy missed 4.9% of Lynch syndrome cases, but 34.8% fewer cases required IHC/MSI testing, and 28.6% fewer cases underwent germline testing than in the universal approach.
The consideration to further stratify the recommendation for molecular tumor testing by age (i.e., 70 y) warrants attention as it influences the cost-effectiveness of universal screening strategy.
Loss of MLH1 and PMS2 due to somatic hypermethylation is not uncommon, and is more frequently detected with increasing age at CRC diagnosis.[323] Therefore, additional molecular tumor testing including BRAF and MLH1 hypermethylation testing is recommended in cases in which there is loss of MLH1 and PMS2 expression on IHC, thereby decreasing the number of individuals referred for unnecessary germline genetic testing. A testing strategy including MLH1 hypermethylation analyses in individuals aged 70 years or younger with CRC who had loss of MLH1 on IHC was shown to be cost-effective in a population-based study of 1,117 individuals.[324]
Screening individuals with CRC for Lynch syndrome is most often performed in a stepwise fashion based on IHC tumor testing results that evaluate protein expression for the four MMR genes related to Lynch syndrome. One proposed strategy is summarized in Figure 6. This framework does not incorporate a germline testing approach that simultaneously evaluates multiple cancer susceptibility genes (multigene [panel] testing), which may be useful in select patient populations. (Refer to the Multigene [panel] testing section of this summary for more information.)
EnlargeFigure 6. A proposed strategy to evaluate individuals with colorectal cancer for Lynch syndrome based on immunohistochemical tumor testing results. Adapted from Geiersbach KB, Samowitz WS. Microsatellite instability and cancer. Arch Pathol Lab Med 135(10):1269-77, 2011.
Clinicians are increasingly utilizing tumor sequencing to advance therapeutic decisions in a more personalized approach, particularly in patients with metastatic disease. The performance of next-generation tumor sequencing (NGS) of CRCs for the detection of Lynch syndrome was compared with existing screening protocols that include MSI testing and IHC staining (with BRAF p.V600E testing) in 419 CRC cases recruited in a multicenter, population-based study.[325] Twelve participants were identified as Lynch syndrome carriers by germline DNA testing and all were correctly identified by tumor sequencing, while MSI plus BRAF testing and IHC plus BRAF testing missed five and six Lynch syndrome cases, respectively. Tumor sequencing had a higher sensitivity than IHC plus BRAF testing (100% vs. 89.7%; P = .04) and MSI plus BRAF testing (100% vs. 91.4%; P = .07) while specificity was comparable across all strategies (95.3% for tumor sequencing, 94.6% for IHC plus BRAF, and 94.8% for MSI plus BRAF; P = not significant). In a validation cohort of 46 known Lynch syndrome pathogenic variant carriers with CRC, tumor sequencing yielded similar results and correctly identified 100% of carriers. In addition, the authors highlighted potential therapeutic implications by reporting on somatic alterations identified by tumor sequencing in 283 participants. This study suggested that tumor sequencing is a highly effective mode of identifying Lynch syndrome; however, the cost-effectiveness of this strategy remains to be determined.
A 2019 retrospective study using data from a large, community-based, integrated U.S. health care system compared the diagnostic performance of age-restricted screening strategies for Lynch syndrome by reflex MMR IHC of all CRCs versus a universal screening strategy without an upper age limit.[326] Lynch syndrome identification decreased substantially after age 70 years to age 75 years, with minimal incremental gain after age 80 years. The number of CRCs needed to be screened to identify one Lynch syndrome case was 20 among patients diagnosed with CRC at age 50 years or younger but increased to 208 for those with CRC at age 71 years to age 80 years, and 668 for those diagnosed after age 80 years.
Cost-effectiveness of universal tumor screening for Lynch syndrome
Results are available from a Markov model that incorporated the risks of colorectal, endometrial, and ovarian cancers to estimate the effectiveness and cost-effectiveness of strategies to identify Lynch syndrome among individuals aged 70 years or younger with newly diagnosed CRC.[310] The strategies incorporated in the model were based on clinical criteria, prediction algorithms, and tumor testing or up-front germline pathogenic variant testing followed by directed screening and risk-reducing surgery. IHC followed by BRAF pathogenic variant testing was the preferred strategy in this study. An incremental cost-effectiveness ratio of $36,200 per life-year gained resulted from this strategy. In this model, the number of relatives tested (3–4) per proband was a critical determinant of both effectiveness and cost-effectiveness. These results were similar to earlier analyses conducted by EGAPP which found that the most cost-effective approach was to test all tumors for absence of protein expression of MSH2, MLH1, MSH6, and PMS2 followed by targeted germline testing of MSH2, MLH1, or MSH6 offered depending on which protein was absent. If there was absence of MLH1, testing was offered for BRAF variant-negative tumors.[320]
NCCN 2024 guidelines support using universal screening on all CRCs to help identify individuals who may have Lynch syndrome. Universal screening can include the following testing methods: IHC testing, MSI testing, and comprehensive tumor NGS panel testing.[123] Universal screening in all individuals irrespective of age was associated with a doubling of incremental cost per life-year saved compared with screening only those younger than 70 years.[310] The authors of this analysis conclude that screening individuals younger than 70 years appears reasonable, while screening all individuals regardless of age might also be acceptable, depending on willingness to pay.
However, it is important to note that the conclusions from this study were contingent upon the number of at-risk relatives who underwent germline testing (through a process known as cascade screening) based on the identification of a germline MMR gene variant in the index case of CRC in the family. In their model, to meet the accepted $50,000 cost-effective threshold, testing a minimum of three to four relatives was necessary.[310] This emphasizes the importance of provider-to-patient communication, family communication, and the need to ensure improved uptake of germline testing in Lynch syndrome families with a known causative gene. (Refer to the Psychosocial Issues in Hereditary Colon Cancer Syndromes section of this summary for more information about family communication and uptake of genetic testing in families with Lynch syndrome.)
Another study addressed the cost-effectiveness of testing for pathogenic variants in the Lynch syndrome–associated genes and evaluated 21 screening strategies, including clinical criteria, use of clinical Lynch syndrome prediction models, and molecular tumor testing.[327] The model included two steps: (1) measurement of the newly identified number of Lynch syndrome diagnoses; and (2) measurement of the life-years gained as a result of confirming Lynch syndrome in a healthy carrier. Among all of the strategies modeled, screening the proband with a predictive model such as PREMM(1,2,6) followed by IHC for MMR protein expression and germline genetic testing was the best approach, with an incremental cost-effectiveness ratio of $35,143 per life-year gained. Germline genetic testing on all probands was the most effective approach, but at a cost of $996,878 per life-year gained. The authors concluded that the initial step of Lynch syndrome screening should utilize a predictive model in the proband, and that both universal testing and general population screening strategies were not cost-effective screening strategies for Lynch syndrome.
Establishment of an upper age limit for universal tumor testing remains controversial. Some experts have endorsed testing only individuals with CRC who are younger than 70 years (reserving testing in individuals ≥70 y for only those meeting the revised Bethesda criteria; with this strategy, 5% of carriers would be missed).[328] However, others have advocated against an upper age limit for testing given the potential benefit to younger generations via cascade screening and the opportunity for increased surveillance and other prophylactic interventions in individuals found to carry a known familial pathogenic variant.
Another cost-effectiveness analysis was performed using data from 179 consecutive endometrial cancer patients diagnosed at or before age 70 years and screened with MMR IHC and reflex MLH1 promoter hypermethylation, among whom seven Lynch syndrome carriers (3.9%) were identified.[329] Only one of the seven Lynch syndrome probands was age 50 years or younger at endometrial cancer diagnosis. The authors calculated that screening women diagnosed with endometrial cancer at age 51 to 70 years resulted in an additional 29.3 life-years gained (on top of the 45.4 life-years gained by screening women diagnosed at age ≤50 y), and the incremental cost-effectiveness ratio for screening all diagnoses at age 70 years or younger versus diagnoses at age 50 years or younger was 5,252 euro per life-year gained. Universal tumor-based screening of all women aged 70 years or younger was also cost-effective, compared with strategies using the Bethesda guidelines to guide MMR and MSI testing with an incremental cost-effectiveness ratio of 6,668 euro per life-year gained.
The cost-effectiveness of universal tumor testing in both CRC and endometrial cancer is largely driven by the assumption of cascade screening through which other at-risk family members will be identified, tested, and subsequently pursue their own cancer risk reduction.[310]
The cost of germline genetic testing continues to decrease with advancements in DNA analyses, including simultaneous testing of multiple germline variants associated with malignancy, through multigene (panel) tests. As a result, additional cost-effective analyses using more updated data related to germline testing will need to be conducted. Multigene (panel) testing may become a more favorable and cost-effective approach in the future.
Considerations and limitations related to universal tumor testing for Lynch syndrome
While universal screening continues to be adopted nationally, there is significant variability in the uptake and approach to molecular testing. A 2011 survey of the National Society of Genetic Counselors revealed that more than 25% of respondents had some form of universal screening implemented at their center. Tumor screening methods varied; 34 (64.2%) of 53 centers started with IHC, 11 (20.8%) of 53 centers started with MSI testing, and 8 (15.1%) of 53 centers performed both tests on newly diagnosed colorectal tumors.[330] A 2012 survey suggested that some form of universal screening was being routinely performed at 71% of the National Cancer Institute (NCI) Comprehensive Cancer Centers, but utilization dropped to 15% among a random sample of community hospital cancer programs.[331]
Because adherence to universal screening for Lynch syndrome may be poor (many patients are not referred for genetic evaluation and testing), a prospective quality improvement study utilizing the Six Sigma conceptual framework was conducted to improve the implementation of universal genetic screening among young patients with CRC.[332] The main aim of the study was to increase the proportion of tumor studies for deficient MMR among patients with early-onset CRC (aged 18–50 y). The intervention involved patient and provider education, in addition to visual cues provided at point of care. The study demonstrated an improvement of 21.5% in the rate of IHC testing in young adults with CRC over the 12-month postintervention period compared with the preintervention period.
Studies reporting uptake of genetic testing for Lynch syndrome have largely focused on individuals and families who were selected for potential risk of Lynch syndrome based on family history or clinical characteristics. While universal tumor screening is increasingly being adopted to identify newly diagnosed patients who may have a germline variant, few studies have examined the uptake of genetic testing after universal tumor testing. An important implication of universal screening for Lynch syndrome is that it does not result in automatic germline testing in appropriate individuals. In the clinical setting, more follow-up by health care teams to facilitate referral to genetic counseling for patients with abnormal tumor screening results may improve completion of genetic testing.[333] Higher levels of patient completion of genetic testing after abnormal tumor screening may be associated with having genetic counselors involved in this process to disclose screen-positive results, provide counseling after tumor testing, or facilitate referrals.[334]
Subsequent genetic counseling requires coordination between the pathologist, the referring surgeon or oncologist, and a cancer genetics service. As an illustration, a population-based screening study found that only 54% of patients with an IHC-deficient tumor (that was BRAF pathogenic variant negative) ultimately consented to and proceeded with germline MMR testing.[335] One institution found 21 pathogenic variants among 1,100 patients who underwent routine MSI and IHC testing after a diagnosis of CRC. This study found markedly increased uptake of genetic counseling and germline MMR gene testing when both the surgeon and a genetic counselor received a copy of abnormal MSI/IHC results, especially when the genetic counselor played an active role in patient follow-up.[333]
In contrast to tumor testing, which is commonly performed without a patient’s prior knowledge, germline genetic testing, such as germline testing for MMR pathogenic variants, generally includes genetic counseling and requires patient permission before it is performed. A cross-sectional survey of U.S. cancer programs (20 NCI–designated Comprehensive Cancer Centers and 49 community hospital cancer programs) found that, of those that performed MSI and/or IHC testing as part of standard pathological evaluation at the time of colon cancer diagnosis in all or select cases, none required written informed consent before tumor testing.[331]
Diagnostic strategies for all individuals diagnosed with endometrial cancer
Given the increased prevalence of endometrial cancer among carriers of MMR pathogenic variants, there is a growing consensus to screen patients with endometrial cancer for Lynch syndrome.
In a study that examined the feasibility and desirability of performing tumor screening of all endometrial cancers, regardless of age at diagnosis or family history of cancer, at least 2.3% (95% CI, 1.3%–4.0%) of newly diagnosed patients had Lynch syndrome.[336,337] Eight of thirteen cases diagnosed with Lynch syndrome were aged 50 years or older, eight did not meet published family history criteria for Lynch syndrome, and two would have been missed by MSI testing. Because of the increased prevalence of endometrial cancer and the results of this study, the authors support universal screening of endometrial cancers for Lynch syndrome. (Refer to the IHC section of this summary for more information about performing IHC for MMR protein expression.)
Another smaller study of 242 consecutive endometrial cases demonstrated a 4.5% (11/242) prevalence of MMR-deficient cases lacking somatic MLH1 promoter hypermethylation, including four cases (1.7%) with germline MMR variants, four cases (1.7%) with two somatic MMR alterations on NGS, and two cases (0.8%) with otherwise unexplained MMR-deficiency.[338] Such findings demonstrate that universal MMR tumor screening of endometrial cancers will identify individuals with underlying Lynch syndrome and a spectrum of non-Lynch syndrome cases with various forms of MMR-deficiency.
Another study prospectively evaluated universal IHC-based screening of both CRC and endometrial cancer cases, irrespective of age at diagnosis.[339] In both the tertiary and community settings, 1,290 CRC and 484 endometrial cancer cases were screened between 2011 and 2013. The study additionally calculated PREMM(1,2,6) and PREMM5 scores for all patients in whom a germline pathogenic variant was detected. Abnormal staining was observed in 22% of endometrial cancers and 18.8% of CRCs. After excluding those cases felt to be sporadic because of the presence of BRAF and/or hypermethylation of MLH1, 10.8 % of patients with CRC and 6.6% of patients with endometrial cancer were referred for genetic counseling. Lynch syndrome was diagnosed in 24 individuals (1.4%), 66% of whom had CRC. The overall detection rate of Lynch syndrome was 1.7% in endometrial cancer cases and 1.2% in CRC cases. Among Amsterdam criteria, Bethesda guidelines, PREMM(1,2,6), and PREMM5, the best performing model was PREMM5, which would have detected 82% of cases identified by universal screening.
The cost-effectiveness of tumor testing of women diagnosed with endometrial cancer was examined in a model-based simulation study and included IHC testing in the following scenarios: (1) diagnosis before age 50 years; (2) diagnosis before age 60 years; (3) any age at diagnosis with the presence of an FDR with any Lynch syndrome–associated cancer; and (4) all cases irrespective of diagnosis age and family history. Women fulfilling Amsterdam II criteria or those diagnosed before age 50 years with at least one FDR with any Lynch syndrome–associated cancer were directly referred for genetic counseling and genetic testing without IHC testing. A strategy of IHC testing for MMR protein expression in all patients with endometrial cancer and an FDR with any Lynch syndrome–associated cancer was reported to be cost-effective in the detection of Lynch syndrome.[340] This strategy had an incremental cost ratio of $9,126 per life-year gained relative to the least-costly strategy, which was genetic testing on all women diagnosed with endometrial cancer before age 50 years with at least one FDR with a Lynch syndrome–related cancer. Life expectancy was highest with the most inclusive testing strategy of IHC testing of all women with endometrial cancer irrespective of age at diagnosis or family history but had the least favorable incremental cost ratio of $648,494 per life-year gained. NCCN recommends tumor testing with IHC and/or MSI and a comprehensive tumor NGS panel testing for all endometrial cancers.[123] Despite these recommendations, the uptake of universal screening in women newly diagnosed with endometrial cancer is unclear.
Use of MSI testing across all tumor types has become an important screening tool to select cases that may have a favorable response to immune checkpoint inhibitor therapy. These results may potentially be used to screen for Lynch syndrome in tumors other than CRC. A study evaluated MSI across a wide variety of malignancies and evaluated its use as a potential means to identify Lynch syndrome, regardless of tumor type.[341] In a study of more than 15,000 patients with more than 50 types of cancers evaluated in a single-center study, data on well-annotated tumor and matched normal DNA sequencing results with paired germline MMR gene testing, were used to determine MSI status. MSI was determined using a software tool that reports the percentage of unstable microsatellites as a score from paired tumor-normal genome sequencing data and allows for comprehensive investigation of MSI sites simultaneously. The approach used has been reported to be more sensitive across cancers not typically screened for MMR-deficiency (dMMR) than MSI testing of five mononucleotide microsatellite foci using PCR.[342] CRC and endometrial cancer comprised the majority of cancers with MSI-H in this study, but 38% (125 of 326) of MSI-H tumors and more than 90% of those with intermediate-level MSI were other cancer types. Germline testing confirmed a diagnosis of Lynch syndrome in 16.3% and 1.9% of tumors with MSI-H and intermediate-level MSI, respectively, in addition to 0.3% of cases that lacked MSI. Importantly, half of all Lynch syndrome carriers with MSI-H/intermediate tumors had primary cancers other than CRC or endometrial cancer, with many malignancies not associated with Lynch syndrome. Among those individuals with a noncanonical Lynch syndrome cancer, nearly half failed to meet clinical criteria for Lynch syndrome testing on the basis of their cancer diagnosis or family cancer history. Furthermore, intermediate-level MSI and MSS phenotypes were most often observed in cancers not classically related to Lynch syndrome and in individuals with germline PMS2 variants. This study supports other findings related to the variable phenotypic expression of Lynch syndrome on the basis of the altered MMR gene and its broad constellation of associated malignancies that make it difficult to be identified by clinical criteria alone. In addition, the investigators further analyzed a unique gene variant signature in every tumor and correlated results to the observed MSI phenotype and germline MMR status to provide some indirect data on whether a gene variant carrier’s cancer was caused by Lynch syndrome and MMR deficiency or possibly an incidental finding. This is pertinent in evaluating those cancers whose association with Lynch syndrome is unclear and debatable, such as breast and prostate cancer. The authors’ finding that none of the breast cancer patients with Lynch syndrome in this very large cohort had tumors with MSI lends support to the hypothesis that these individuals’ germline MMR gene variants may simply be incidental findings and not etiologic to their cancer diagnosis.
A single-institution study of 100 histologically confirmed small bowel adenocarcinomas with MSI/MMR tumor studies identified 26 cases with MMR deficiency, 10 of which were due to Lynch syndrome. Most cancers were located in the duodenum, followed by the jejunum and the ileum. The authors recommended that individuals with small bowel adenocarcinomas be screened for Lynch syndrome, given the implications of MMR deficiency on treatment and clinical management.[343]
Germline genetic testing
Genetic testing for germline pathogenic variants in MLH1, MSH2, MSH6, PMS2, and EPCAM can help formulate appropriate intervention strategies for the affected variant-positive individual and at-risk family members, many of whom may be unaffected by cancer.
If a pathogenic variant is identified in an affected person, then testing for that same pathogenic variant should be offered to all at-risk family members. At-risk relatives who test negative for the identified pathogenic variant in the family are not at increased risk of CRC or other Lynch syndrome–associated malignancies and can follow surveillance recommendations applicable to the general population. Family members who carry the familial pathogenic variant are referred to surveillance and management guidelines for Lynch syndrome. (Refer to the Management of Lynch syndrome section of this summary for more information.)
If no pathogenic variant is identified in the affected family member, then testing is considered negative for Lynch syndrome in that individual. With advances made in DNA sequencing technologies, it is unlikely that current gene testing is not sensitive enough to detect a pathogenic variant in the genes tested. Advances in testing, including the common use of NGS by most commercial testing laboratories have improved upon the detection of certain alterations such as large deletions or genomic rearrangements as well as the presence of a pseudogenePMSCL in PMS2.
Possible reasons why a pathogenic variant may not be detected include the following:
The family could have a variant in a yet-unidentified gene that causes Lynch syndrome or a predisposition to colon cancer.
The individual tested in the family may have developed colon cancer through a nongenetic mechanism (i.e., it is a sporadic case also known as a phenocopy), while the other cases in the family are really the result of a germline variant. If this scenario is suspected, testing another affected individual who has had a Lynch syndrome–associated cancer is recommended.
In cases in which a CRC tumor displayed MSI and/or abnormal IHC, but no germline pathogenic variant was detected, biallelic somatic variants may be the resulting etiology. These are sometimes, confusingly, called Lynch-like syndrome cases, even though they are typically not considered to be familial.
Failure to detect a pathogenic variant could mean that the family truly is not at genetic risk despite a clinical presentation that suggests a genetic basis (e.g., the patient may have biallelic somatic variants in an MMR gene). If no variant can be identified in an affected family member, testing should not be offered to at-risk members because results would be uninformative for the relatives. They would remain at increased risk of CRC by virtue of their family history and should continue with recommended intensive screening.
Germline variant analysis of MLH1, MSH2 (including EPCAM), MSH6, and PMS2 may be considered in instances in which tumor tissue is not available from individuals to test for MSI and/or MMR protein IHC. This approach has become less expensive with the advent of multigene (panel) testing, which is now offered by several clinical laboratories at a cost that may be comparable to single-gene testing. The cost of multigene testing may also approach the cost of tumor screening and may prove to be a cost-effective approach in individuals affected by CRC. At present, multigene tests are not routinely recommended for universal screening for Lynch syndrome among all newly diagnosed CRC patients, but they may be very useful in select populations, such as those with early-onset CRC [344] or from familial, high-risk clinic-based populations. It is also important to note that pathogenic variants may be detected in other cancer-associated genes beyond Lynch syndrome. In a study of 1,112 individuals who met NCCN criteria for Lynch syndrome testing and who underwent multigene testing with a 25-gene panel, as expected, 114 individuals (9.0%) were found to have pathogenic variants in MMR genes; however, 71 individuals (5.6%) were found to have a pathogenic variant in non-Lynch syndrome cancer predisposition genes, such as BRCA1, BRCA2, APC, MUTYH (biallelic), and STK11. Lastly, multigene tests yield a high proportion of VUS. In the aforementioned study, a total of 479 patients (38%) had one or more VUS.[345]
Individuals with early-onset CRC have been shown to have a high frequency and wide spectrum of germline pathogenic variants, indicating that panel testing in this population may be beneficial. In a study of 450 patients with early-onset CRC (mean age at diagnosis, 42.5 y) and a family history including at least one FDR with colon, endometrial, breast, ovarian, and/or pancreatic cancer, 75 germline pathogenic or likely pathogenic variants were identified in 72 patients (16%).[344] The spectrum of variants identified included Lynch syndrome and non-Lynch syndrome–associated genes, including several genes that have not traditionally been associated with CRC (e.g., BRCA1/BRCA2, ATM, CHEK2, PALB2, and CDKN2A). Given the high frequency and variety of hereditary cancer syndromes identified, the authors suggested that multigene testing in this population may be warranted. Similarly, another smaller single-institution analysis of 151 individuals with CRC identified pathogenic germline variants in 9.9% of individuals.[346]
Multigene testing has also been examined in a larger study of 1,058 individuals with CRC who were unselected for age at diagnosis, personal or family history, or MSI/MMR test results.[347] Germline pathogenic variants in cancer susceptibility genes were identified in 105 individuals (9.9%). While 33 individuals (3.1%) carried pathogenic variants in Lynch syndrome genes, 74 (7.0%) had pathogenic variants in non-Lynch syndrome–associated genes, including APC, MUTYH, BRCA1/BRCA2, PALB2, CDKN2A, TP53, and CHEK2. These data illustrate the breadth of variants that may be identified in unselected CRC patients; thus, use of a comprehensive multigene test may be warranted.
A 2017 study examined the frequency of pathogenic Lynch syndrome–associated gene variants in individuals undergoing multigene testing at a single commercial United States laboratory between 2012 and 2015, and reported on the characteristics of those carriers identified with Lynch syndrome.[348] The study reports on the largest cohort of individuals tested through multigene testing to date; data was reported on 34,980 individuals who had undergone various multigene panel tests that included the MMR and EPCAM genes, where the indication for testing was not limited to Lynch syndrome. A total of 618 pathogenic variants were identified in 612 individuals (1.7%) and analyses were conducted on 579 subjects (after exclusion of 33 individuals who had a Lynch syndrome–associated variant and a second MMR variant or other pathogenic alteration in another cancer predisposition gene). The majority of carriers were affected by cancer, including non-Lynch syndrome–associated malignancies, where breast cancer was most frequently reported (124/423, 23.5%). MSH6 variants were most prevalent (29.3%), followed by PMS2 (24.2%), MSH2 (23.7%), MLH1 (21.6%), and EPCAM (1.2%). This finding differs from previous data where MSH2 and MLH1 variants were more prevalent, as individuals were more often selected for Lynch syndrome–specific testing due to a personal and/or family history of CRC.
The study reports on genotype-phenotype correlations on 528 Lynch syndrome carriers, the majority of whom had CRC (186, 35.2%) and endometrial cancer (136, 25.8%), followed by breast cancer (124, 23.5%) and ovarian cancer (74, 14%).[348] One hundred forty-five carriers presented with breast or ovarian cancer as their sentinel tumor and did not carry a prior diagnosis of CRC or endometrial cancer prior to the time of multigene testing. When examining MMR gene variant distribution among tumor-specific subgroups, a higher frequency of MSH6 and PMS2 variants were detected in carriers with breast cancer only than MLH1 and MSH2, where the latter pathogenic variants were more frequent in subjects with CRC only. For patients with breast cancer only, the frequency of PMS2 gene variants was significantly higher than population estimates, which was not the case for MLH1, MSH2, or MSH6. A comparable retrospective study reported similar findings. Standardized incidence ratios (SIRs) of breast cancer were calculated by comparing observed breast cancer frequencies in a population of 423 women with pathogenic or likely pathogenic variants in MMR genes with those in the general population. The authors reported a statistically significant age-standardized risk of breast cancer for MSH6 carriers (SIR, 2.11; 95% CI, 1.56–2.86) and PMS2 carriers (SIR, 2.92; 95% CI, 2.17–3.92).[349] A critical limitation of both of these studies was the excess of breast cancer cases in the overall referral population as well as the known high background population prevalence of MSH6 and PMS2 germline pathogenic variants.
Clinical criteria for the identification of Lynch syndrome, including the Amsterdam criteria, revised Bethesda guidelines, or the PREMM(1,2,6) risk prediction model, would have failed to identify 27.3% of Lynch syndrome carriers in this study.[348] Given the increased prevalence of breast and ovarian cancers, 58.9% met the NCCN guidelines for BRCA1/BRCA2 testing and of these, 36.7% also met NCCN guidelines for Lynch syndrome testing. Lastly, there were limited data on tumor testing results, available only on 18.8% of pathogenic variant carriers, where results were often discordant with the altered gene, which was most often reported in MSH6 and PMS2 carriers. Results of this study support the use of multigene testing for Lynch syndrome and further study of the respective cancer risks, as current testing strategies limit identification of Lynch syndrome carriers and associated malignancies.
Lastly, germline MMR genes have been detected unexpectedly among individuals undergoing multigene testing for cancers not commonly associated with Lynch syndrome, such as breast and prostate cancer. As a result, the cancer spectrum associated with Lynch syndrome may be wider than previously appreciated. For more information, see the Breast cancer and Prostate cancer sections and Genetics of Prostate Cancer.
As genetic testing becomes routine rather than the exception, questions regarding the cost of testing are inevitable. Historically, a cost-effectiveness ratio of $50,000 per quality-adjusted life-year (QALY) has been used as the benchmark for good value for care.[350] Over time it has been suggested that this threshold is too low and that other thresholds such as $100,000 or $150,000 be used.[350]
A 2015 study evaluated the cost-effectiveness of multigene testing for CRC and polyposis syndromes in patients referred to a cancer genetics clinic.[351] These authors developed a decision model to estimate the immediate and downstream costs for patients referred for evaluation and of CRC surveillance in family members identified as carriers of pathogenic variants. The costs were estimated on the basis of published models from the CDC and from an academic molecular genetics laboratory. They classified the syndromes on the basis of inheritance pattern and penetrance of CRC. Four custom panels were compared with the standard of care. The four panels tested for (1) Lynch syndrome–associated genes only (MLH1, MSH2, MSH6, PMS2, and EPCAM); (2) genes in panel 1 and additional genes associated with autosomal dominant inheritance and high CRC penetrance (APC, BMPR1A, SMAD4, and STK11); (3) genes in panels 1 and 2 and those associated with autosomal recessive inheritance with high CRC penetrance (MUTYH); or (4) all genes in the first three panels and those associated with autosomal dominant conditions with low penetrance (PTEN, TP53, CDH1, GALNT12, POLE, POLD1, GREM1, AKT1, and PIK3CA). The respective costs were as follows: panel 1, $144,235 per QALY; panel 2, $37,467 per QALY; panel 3, $36,500 per QALY; and panel 4, $77,300 per QALY when compared with panel 3. The authors concluded that the use of an NGS multigene test that includes highly penetrant CRC and polyposis syndromes and Lynch syndrome cancer genes was the approach most likely to provide clinically meaningful results in a cost-effective fashion.
The cost of germline genetic testing continues to decrease with advancements in technology since the time this model analysis was conducted; additional studies are needed to continue to assess the cost-effectiveness of this testing approach.
Prevalence, clinical manifestations, and cancer risks associated with Lynch syndrome
Lynch syndrome is an autosomal dominant syndrome characterized by an early age of onset of CRC, excess synchronous and metachronous colorectal neoplasms, right-sided predominance, and extracolonic tumors, notably endometrial cancer. Lynch syndrome is caused by pathogenic variants in the DNA MMR genes, namely MLH1 on chromosome 3p21;[352,353] MSH2 on chromosome 2p22-21;[354,355] MSH6 on chromosome 2p16;[356] and PMS2 on chromosome 7p22.[352–355,357–360] The function of these genes is to maintain the fidelity of DNA during replication. Lynch syndrome is also associated with pathogenic variants of the EPCAM gene on chromosome 2p21, which causes epigenetic silencing of MSH2, located immediately downstream of this gene.[361,362]
Lynch syndrome accounts for about 3% of all newly diagnosed cases of CRC.[309] In earlier studies, the average age of CRC diagnosis in Lynch syndrome pathogenic variant carriers was as young as 44 to 52 years. [256,309,363] In contrast, from 2015 to 2019, the median age of CRC diagnosis was 66 years in individuals with sporadic CRC.[364] In subsequent studies that corrected for ascertainment bias to determine cancer-related risk estimates and genotype-phenotype correlations, the average age at CRC diagnosis was 61 years among Lynch syndrome–associated pathogenic variant carriers.[365]
Original reports related to overall and gene-specific prevalence estimates in Lynch syndrome relied heavily on retrospective data from familial cancer registries worldwide. Earlier risk estimates of CRC (and endometrial cancer) reported in Lynch syndrome were subject to ascertainment bias and overestimation, given that data were derived largely from familial cancer registries and cases were often ascertained based on young-onset CRC or an increased number of CRC cases among relatives. Correction of these cancer risk estimates has been made possible through modified segregation analyses, where statistical methodology provides more accurate estimates and adjusts for ascertainment bias. Conversely, risk estimates related to extracolonic malignancies, with the exception of endometrial cancer, may be prone to underestimation because many families may have underreported these cancers in relatives, and Lynch syndrome–related tumors may have occurred later in life.
In a large population-based study of 5,744 CRC cases who were recruited irrespective of family cancer history from the United States, Australia, and Canada, it was estimated that 1 in 279 individuals in the population carry an MMR pathogenic variant associated with Lynch syndrome.[366]
In another population-based study of 450 individuals with CRC but limited to young onset with diagnoses occurring before age 50 years, germline pathogenic variants were identified in 72 of 450 individuals (16%), as detected by multigene (panel) testing for inherited cancer susceptibility genes. As expected, the majority of identified variants were in genes known to be associated with CRC, predominantly Lynch syndrome (37 of 72 patients, 51.4%). However, 13 of 72 patients (18.1%) had pathogenic variants in genes not traditionally associated with CRC, including but not limited to BRCA1/BRCA2, which accounted for 8% of the identified variants. Because of the high frequency and wide variety of pathogenic variants identified, the authors suggested consideration of multigene testing for all individuals with early-onset CRC.[344]
Gene-specific considerations and associated CRC risk
The MLH1 and MSH2 genes were originally thought to account for most pathogenic variants of the MMR genes found in Lynch syndrome. However, the prevalence of MSH6 and PMS2 pathogenic variants has been increasing with improved DNA analyses and universal tumor screening of all CRCs.[366] MSH6 and PMS2 variants may be more common in unselected cases of CRC (and endometrial cancer),[366] compared with MLH1 and MSH2 variants which were more commonly identified in individuals from high-risk CRC clinics.[367,368]
MLH1
In early studies, the prevalence of MLH1 pathogenic variants in individuals with Lynch syndrome was reported to be between 41.7% [369] and 50%,[370] making MLH1 the most commonly altered MMR gene in Lynch syndrome families. It was not until a report on the population-based prevalence of Lynch syndrome that the MLH1 pathogenic variant was estimated to be 1 in 1,946, ranking third after PMS2 (1 in 714) and MSH6 (1 in 758), as estimated in a large international study of 5,744 CRC cases.[366]
MLH1 pathogenic variants are associated with the entire spectrum of malignancies associated with Lynch syndrome.[370] The lifetime risk of any Lynch syndrome–associated cancer by age 70 years has been found to range between 59% and 65% in MLH1 pathogenic variant carriers.[285] The highest risk among carriers of pathogenic MLH1 variants is for CRC, which is estimated to be between 41% and 68%,[3,4,365] and the mean age at diagnosis of CRC was 42.8 years (range, 16–81 y) in one study that included 137 affected individuals.[371] In a more recent prospective study using pooled European registry data of 944 MLH1 carriers without cancer, the cumulative CRC incidence was 46% at age 70 years, despite colonoscopic surveillance (albeit at various intervals).[5]
Unlike the APC gene of FAP, in which several phenotypes of differing severity and spectrum of disease occur, genotype-phenotype relationships have been elusive in the MMR genes. In a large series of MLH1 pathogenic variant carriers, women with truncating MLH1 pathogenic variants had significantly later onset of endometrial cancer than did those with nontruncating variants.[372] A nonsignificant trend toward later CRC onset in those with truncating MLH1 pathogenic variants was also identified. As no other correlations were found with specific types of variants in MLH1 or other MMR genes, these associations could be artifactual and warrant further validation.
MSH2
The prevalence of MSH2 pathogenic variants in individuals or families with Lynch syndrome has varied across studies. MSH2 pathogenic variants were reported in 38% to 54% of Lynch syndrome families in studies including large cancer registries and among cohorts of early-onset CRC (younger than age 55 y).[258,373] The reported prevalence of MSH2 pathogenic variants was 32.8% in 2012 in the database of the International Society for Gastrointestinal Hereditary Tumors (InSiGHT), a large professional organization devoted to the collaborative study of familial GI cancer,[369] with families readily ascertained based on the presence of extracolonic cancers in MSH2-associated Lynch syndrome. However, the prevalence of MSH2 pathogenic variants was estimated to be 1 in 2,841 in a population-based cohort of 5,744 CRC cases recruited from the United States, Australia, and Canada;[366] MSH2 was the least prevalent of the MMR gene variants associated with Lynch syndrome.
The risk of any Lynch syndrome–associated cancer by age 70 years has been found to range between 57% to nearly 80% in MSH2 pathogenic variant carriers.[285] The lifetime risk of colon cancer associated with MSH2 pathogenic variants is estimated to be between 48% and 68%.[3,4,365] In a case series of Lynch syndrome patients, those carrying germline MSH2 pathogenic variants (49 individuals, 45% women) had a lifetime (cutoff age, 60 y) risk of extracolonic cancers of 48% compared with 11% for MLH1 carriers (56 individuals, 50% women).[374] In a more recent prospective study using pooled European registry data of 616 MSH2 carriers without cancer, the cumulative CRC incidence was 35% at age 70 years, despite colonoscopic surveillance.[5]
The mean age at diagnosis of CRC in MSH2 carriers has been comparable to MLH1 carriers. One study that included 143 affected individuals with MSH2 pathogenic variants found a mean age at CRC diagnosis of 43.9 years (range, 16–90 y). The same study reported a mean age at CRC diagnosis of 42.8 years (range, 16–81 y) in 137 MLH1 pathogenic variant carriers.[371]
MSH6
Most series have reported a prevalence of germline MSH6 pathogenic variants in approximately 10% of Lynch syndrome families from high-risk clinics and a higher proportion of unselected CRC patients, at approximately 50%.[356,375–380] The reported prevalence of MSH6 pathogenic variants in the InSiGHT database was 18% in 2012.[369] The wide range of prevalence estimates for pathogenic MSH6 variants was a result of small sample sizes, ascertainment bias, and the later age of CRC onset and less striking family histories in MSH6-associated Lynch syndrome families compared with MLH1- and MSH2-associated Lynch syndrome families.[375] This is in line with findings from a population-based study of 42 carriers of deleteriousMSH6 germline pathogenic variants, 30 (71%) of whom had a family cancer history that did not meet the Amsterdam II criteria.[6] In a recent, international, population-based study of 5,744 CRC cases, the prevalence of MSH6 pathogenic variants was estimated to be 1 in 758, ranking as the second most prevalent of the MMR genes following PMS2.[366]
The lifetime risk of any Lynch syndrome–associated cancer among MSH6 pathogenic variant carriers is approximately 25% [285] with CRC lifetime risk estimated to be between 12% and 22% [4,6] with MSH6 carriers diagnosed with CRC at a later age than MLH1 and MSH2 carriers. In an earlier study of 146 MSH6 carriers (59 men and 87 women) from 20 families, all of whom had truncating pathogenic variants in MSH6, there was a similar prevalence of CRC by age 70 years among MLH1, MSH2, and MSH6 carriers (P = .0854). However, the mean age at diagnosis for colorectal carcinoma was (a) 55 years for male MSH6 carriers (n = 21; range, 26–84 y) versus 43 years and 44 years in carriers of MLH1 and MSH2 pathogenic variants, respectively; and (b) 57 years for female MSH6 carriers (n = 15; range, 41–81 y) versus 43 years and 44 years in carriers of MLH1 and MSH2 pathogenic variants, respectively.[381]
The largest series of carriers of MSH6 pathogenic variants reported to date includes 113 families from five countries who were ascertained through family cancer clinics and population-based cancer registries.[6] Compared with the incidence for the general population, MSH6 pathogenic variant carriers had an eightfold increased incidence of CRC (HR, 7.6; 95% CI, 5.4–10.8), which was independent of sex and age. By age 70 years, 22% (95% CI, 14%–32%) of male carriers of MSH6 pathogenic variants developed CRC compared with 10% (95% CI, 5%–17%) of female carriers. By age 80 years, the CRC prevalence doubled to 44% (95% CI, 28%–62%) of male carriers of MSH6 pathogenic variants diagnosed with CRC compared with 20% (95% CI, 11%–35%) among female carriers.
In a more recent prospective study using pooled European registry data of 305 MSH6 carriers without cancer, the cumulative CRC incidence was 20% at age 70 years despite colonoscopic surveillance.[5]
PMS2
PMS2 was the last of the genes in the MMR family of genes to be identified. This was because lower penetrance among families made it more difficult to identify [382] using clinical criteria, and also because of limitations of DNA mutational analysis that result from pseudogene interference.
In earlier studies of individuals with CRC and suspected Lynch syndrome, the prevalence of PMS2 pathogenic variants was variable from 2.2% to 5%,[256,383] with an increase to 7.5% as reported in the InSiGHT database in 2012.[369] From a study examining universal tumor testing results from unselected cases of CRC in Switzerland, IHC evaluation of 1,000 consecutive cases found isolated absence of PMS2 expression in 1.5% of all tumors. If this frequency of PMS2-deficient CRCs were representative of all PMS2-associated Lynch syndrome, PMS2 would be the most common gene associated with Lynch syndrome.[384] Results from a large, population-based CRC cohort found that the prevalence of PMS2 pathogenic variants was the highest among all MMR variants, in which 1 person in 714 carried a pathogenic PMS2 gene variant.[366]
The lifetime risk of any cancer has been found to range between 25% and 32% for heterozygous PMS2 pathogenic variant carriers.[285] A meta-analysis of three population-based studies and one clinic-based study estimated that for carriers of PMS2 pathogenic variants, the risk of CRC to age 70 years was 20% among men and 15% among women, and the risk of endometrial cancer was 15%.[385] Similarly, a European consortium of clinic-based registries, taking care to correct for ascertainment bias, found a cumulative lifetime (to age 70 y) CRC risk of only 19% in men and 11% in women with PMS2 pathogenic variants.[386] In addition, patients with PMS2 pathogenic variants presented with CRC 7 to 8 years later than did those with MLH1 and MSH2 pathogenic variants.[383] In a prospective study using pooled European registry data of 77 PMS2 carriers without cancer, the cumulative CRC incidence was 10% at age 70 years despite colonoscopic surveillance.[5] An analysis of nearly 5,000 patients from 284 PMS2 families from the European consortium, supplemented by data from two more registries, was intended to provide more robust PMS2-associated cancer risk estimates.[387] The risk of CRC up to age 80 years was 13% (95% CI, 7.9%–22%) for men and 12% (95% CI, 6.7%–21%) for women, compared with general population risk estimates of 6.6% and 4.7%, respectively. Endometrial cancer risk was found to be 13% (95% CI, 7%–24%). No excess risk of other Lynch syndrome–spectrum tumors was identified in these cohorts. The authors concluded that these data justify consideration of delaying initiation of colonoscopy until age 35 to 40 years, and with longer follow-up intervals (2–3 y), although this was not specifically studied. As with the original reports from the European Prospective Lynch Syndrome Database, it was not possible to assess the extent to which such colonoscopies and polypectomies might have reduced the rate of detected CRCs.
The PLSD is a major ongoing initiative to assess cancer risks in Lynch syndrome. Although it lacks specific details regarding screening practices, it includes outcome data from many European programs, classified by age, gender, and MMR gene.[5,388,389] Recognizing limitations in the larger PLSD, a subset with more detailed surveillance data has been provided.[390] These prospective colonoscopy data from Germany, Holland, and Finland included 2,747 patients of whom 62 had no prior cancer at surveillance initiation. Because of differences in surveillance practices, the colonoscopy interval approximated 1 year in Germany, 2 years in Holland, and 3 years in Finland. The median number of colonoscopies was five and the median per-patient observation time was approximately 8 years. Despite the differences in surveillance intervals, similar adenoma detection rates were found in those patients with a history of cancer (14%) and those without (15.6%). At 10 years of follow-up, rates of first cancer were 8.4% and 14% for metachronous tumors. Factors increasing risk were male sex, prior CRC, presence of MLH1 or MSH2 pathogenic variants, age older than 40 years, and adenoma at index colonoscopy. Notably, no significant difference in CRC detection or in stage at detection was noted between screening intervals of 1, 2, or 3 years.
A subset of individuals with Lynch syndrome (approximately 1%) have a pathogenic variant in EPCAM, which leads to hypermethylation and inactivation of the MSH2 promoter.[391] In a European study of 194 EPCAM deletion carriers, the cumulative risk of CRC up to age 70 years was 75% with the average age at onset of 43 years. This is comparable to the risk in MSH2 carriers (up to 68% by age 70 y). However, the risk of endometrial cancer among women with an EPCAM deletion was only 12% in this study, compared with a risk of up to 71% in MSH2 carriers.[392] The associated phenotype is dependent on the location of the deletion variant in the 3’ end of the EPCAM gene; if the deletion is large and includes parts of the promoter of MSH2, the phenotype will be similar to other MSH2-associated Lynch syndrome families.[392] When the deletion involves the termination signal of EPCAM but spares all of the MSH2 gene and promoter, the phenotype is mainly confined to CRC.[393]
One study of two families with the same EPCAM deletion limited to the 3’ end of the gene and not extending into the promoter of MSH2 found few extracolonic cancers and no endometrial cancers.[393] However, a subsequent study demonstrated that women with MSH2 protein expression loss caused by EPCAM variants are also at risk of endometrial cancer.[392]
Intragenic variability in CRC penetrance among carriers of MMR pathogenic variants
While it is known that MMR pathogenic variant carriers have high lifetime risks of CRC, estimates of these risks vary considerably between studies. Additional factors, including ascertainment bias, heritable modifiers of risk, and nonheritable risk factors may contribute substantially to variation in lifetime risk estimates.
A study from the Colon Cancer Family Registry reported that, depending on the gene that has the pathogenic variant and an individual’s sex, 16% to 23% of MLH1 and MSH2 carriers had lifetime CRC risks of less than 10% (i.e., their risks approached average risk for the general population).[394] Conversely, 10% to 17% of carriers had lifetime risks of more than 90% (i.e., these carriers were almost certain to develop CRC).
An international registry–based study used retrospective data to examine variation in CRC risk in 5,255 families with Lynch syndrome.[395] The study used a segregation analysis conditioned on ascertainment to estimate mean CRC penetrance and modeled unmeasured polygenic factors to estimate variations in penetrance. Nearly 80,000 individuals were included in the study. The number of patients with EPCAM pathogenic variants was insufficient to include in the analysis. Therefore, only families with MLH1, MSH2, MSH6 and PMS2 pathogenic variants were included. Patients were clustered by continent (North America, Europe, and Australasia). There was strong evidence that unknown familial risk factors modified CRC risk for Lynch syndrome carriers across all continents. This resulted in wide variation in CRC risk for each MMR gene. This variation was most pronounced for MLH1 and MSH2, in which 7% to 56% of carriers had a CRC penetrance of less than 20%, 9% to 44% of carriers had a CRC penetrance of more than 80%, and only 10% to 19% of carriers had a CRC penetrance of 40% to 60%. Wide variation in CRC risk was observed even when the analysis was restricted to the 250 families carrying the most common variant in the dataset (the MSH2 pathogenic c.942+3A>T variant). In this MSH2 cohort, 9% to 15% of carriers had a CRC penetrance of less than 20%, and 33% to 45% of carriers had a CRC penetrance of more than 80%. Limitations of the study included the following: (1) 94% of patients were ascertained from high-risk clinics, (2) there were limited data on screening and polypectomy, and (3) multiple assumptions and models were used. These results suggest that published mean cancer risks may not be representative for most Lynch syndrome carriers. Therefore, the authors suggested that current screening guidelines might not be applicable to large proportions of Lynch syndrome patients. Until additional studies have identified and characterized genetic and environmental risk modifiers, contemporary guidelines are recommended for most Lynch syndrome carriers.
The occurrence of such biallelic variants is associated with a characteristic but not diagnostic clinical phenotype. Clinical features include hematologic malignancies and brain tumors in children. When GI tumors occur, the age of onset is strikingly low, sometimes before age 20 years. Café au lait spots and features otherwise suggesting neurofibromatosis are characteristic. Occasionally, patients present with multiple adenomas.
Ethnic variation and founder pathogenic variants in Lynch syndrome
The frequency of MMR variants does not differ markedly from population to population, with similar frequencies identified in a host of different countries. As with hereditary breast and ovarian cancer (HBOC), there are certain variants that occur at higher frequencies within a particular ethnic group. Notable in HBOC are the commonly recurring Ashkenazi Jewish variants, so common that direct-to-consumer testing is offered for these common variants. (Refer to the Prevalence of BRCA1/2 Pathogenic Variants section in BRCA1 and BRCA2: Cancer Risks and Management and the Direct-to-Consumer [DTC] Genetic Tests section in Cancer Genetics Risk Assessment and Counseling for more information.) The ancientness of apparent founder variants is generally established by haplotype analysis. In some instances, what may appear to be a founder variant is simply a frequently recurring de novo variant.[396]
Among the first population findings regarding the MMR genes of Lynch syndrome was the recognition of two very common MLH1 variants in Finland, accounting for most cases of Lynch syndrome in this country.[397,398] Since that time, founder variants have been identified in most populations in which relatively unselected series of patients with CRC have undergone variant testing. Many of the reports originate in Europe. As in Finland, these may be straightforward to identify in the setting of fairly homogeneous ethnicity with low immigration. Founder variants in Europe have been found in the United Kingdom, Sweden, Switzerland, Italy,[399] Portugal, France, Spain, and Hungary, and are likely present in all ethnic groups. Fewer such reports have come from Asia,[400] Latin America, the Middle East, and Africa.
In the United States, a deletion in exons 1–6 of the MSH2 gene has been estimated to account for as much as 20% of variants in that gene. This so-called American Founder Mutation has been determined by haplotype analysis to date back about 500 years.[401]
A South American study combining data from Uruguay, Colombia, Brazil, Argentina, and Chile also selected cases of interest according to Amsterdam and Bethesda features, yielding a 60% frequency of MLH1 and 40% frequency of MSH2. MSH6 and PMS2 were not evaluated. Selection bias likely influenced the frequency of variants and perhaps the relative contributions by MLH1 and MSH2. A possible founder variant in Colombia was noted.[402]
Although testing for commonly recurring founder variants in a given ethnic/geographic area has been considered to be a cost-effective first step when a stepwise strategy is employed, it is likely not necessary when the increasingly common approach of broad panel testing is undertaken as a basic strategy.
In this section, the data exploring the distribution of MMR gene variants amongst differing ethnic groups in the United States are presented. The interpretation of these studies is challenging given the presence of selection and ascertainment bias. In addition, even population-based studies are limited by small sample sizes for many ethnic groups and self-reporting of ethnicity/race.
There are few data suggesting the presence of much variation in Lynch syndrome frequency according to geography or ethnicity. Within a small and/or homogeneous ethnic group the presence of founder variants may seem to increase the prevalence of variants in that particular gene. Slight differences in the proportion of MLH1 and MSH2 variants exist from one population to another. MSH6 and PMS2 have been insufficiently studied at the population level as to enable inferences about their relative frequencies.
The most representative population-based studies in the United States, such as that in Columbus, Ohio, have been overrepresented by White individuals, in accordance with their greater overall numbers. Consequently, data on racial and ethnic minorities such as Hispanic and African American individuals suffer from smaller and less rigorously representative samples.
A study conducted in Puerto Rico considered variants in 89 Caribbean Hispanic patients with Lynch syndrome suspected on the grounds of Amsterdam criteria or Bethesda guidelines.[403] Patients underwent either immediate germline testing or step-wise evaluation beginning with tumor MSI/IHC. Frequencies of variants by gene were 67% for MSH2, 25% for MLH1, and 8% for MSH6. No definite founder variants were evident. Clearly, the selection of participants according to clinical family history criteria would have led to an underreporting of the less penetrant MSH6 and PMS2 genes.
Clinic-based series from California, Texas, and Puerto Rico yielded an overall variant prevalence similar to those described, with somewhat more MLH1 than MSH2, but also including MSH6 and PMS2. Presence of potential founder variants traceable back to Spain and Europe were noted.[404]
The closest population-based information on Lynch syndrome in Hispanic individuals is a Southern California study based on the California Tumor Registry, in which 265 patients were identified.[405] Of those with MSI-H tumors, 13 (62%) had MMR variants. Frequencies of MMR variants were 46% for MLH1 (6 of 13), 31% for MSH2 (4 of 13), 15% for MSH6 (2 of 13), and 8% for PMS2 (1 of 13).
The problem of small numbers is highlighted by the findings from the more truly population-based studies that have been done in the United States. In a study from Columbus, Ohio, only 8% of the consecutive series patients were African American and the proportion of Hispanic individuals as a subset of White individuals was not stated.[344] In another study involving panel testing of nearly all CRC patients treated at Dana-Farber Cancer Institute, less than 5% were Black and less than 3% were Hispanic, underscoring the challenge of extracting meaningful data from small subsets.[347]
Lynch syndrome in African Americans
The issues in evaluating prevalence of Lynch syndrome and cancer risks associated with MMR variants in African American individuals are similar to those in Hispanic individuals: a heterogeneous population that has been understudied. A study of clinic-based data from 13 referral centers in the United States identified 51 families with Lynch syndrome with frequencies of MMR gene variants as follows: 61% MLH1, 21% MSH2, 6% MSH6, and 12% PMS2. Age of cancer onset distribution curves were very similar to those seen in White populations.[406] As with most of the studies in Hispanic individuals, cases were not identified according to any consistent, programmatic evaluation such as universal tumor testing.
Risk of metachronous CRC
A hallmark feature of Lynch syndrome is that carriers of pathogenic MMR gene variants have an increased risk of development of synchronous and metachronous colorectal neoplasms.[388,407,408] In one study of 382 individuals with Lynch syndrome from the Colon Cancer Family Registry, the incidence of metachronous CRCs was 16% at 10 years, 41% at 20 years, and 63% at 30 years after segmental colectomy.[407] The risk of metachronous CRC decreased in a stepwise fashion by 31% for every 10 cm of the colon that was removed, with none of the 50 individuals who had extensive colectomies diagnosed with metachronous CRC. Another prospective study of 1,273 patients with Lynch syndrome who had prior cancer reported a cumulative incidence of subsequent CRC of 46% for MLH1 carriers, 48% for MSH2 carriers, and 23% for MSH6 carriers. This represents only a slightly greater risk of new cancers than pathogenic variant carriers with no previous cancer diagnosis. Excellent survival was again seen and was regarded as a combination of favorable tumor pathology and the effect of surveillance.[388]
Risk of extracolonic malignancies associated with Lynch syndrome
Patients with Lynch syndrome are at an increased risk of other cancers, especially those of the endometrium. The cumulative risk of extracolonic cancer has been estimated to be 20% by age 70 years in 1,018 women in 86 families, compared with 3% in the general population.[409] There is some evidence that the rate of individual cancers varies from kindred to kindred.[410–412]
Endometrial cancer
The most common extracolonic malignancy in Lynch syndrome is endometrial adenocarcinoma, which affects at least one female member in about 50% of Lynch syndrome families. In addition, 50% of women with an MMR gene pathogenic variant will present with endometrial cancer as her first malignancy.[413]
The lifetime risk of endometrial cancer has been estimated to be from 44% in carriers of MLH1 pathogenic variants to 71% in carriers of MSH2 pathogenic variants, although some earlier studies may have overestimated risk due to ascertainment bias.[6,260,365,373,414] Lifetime risk of endometrial cancer in carriers of MSH6 pathogenic variants in 113 families was estimated to be 26% at age 70 years and 44% at age 80 years;[6] overall, female carriers of MSH6 pathogenic variants had an endometrial cancer risk that was 25 times higher than women in the general population (HR, 25.5; 95% CI, 16.8–38.7; P < .001).[6] In another study, the cumulative lifetime risk of uterine cancer was higher in MSH6 carriers (71%) than in carriers of MLH1 (27%) and MSH2 (40%) pathogenic variants (P = .02), with an older mean age at diagnosis of 54 years in carriers of MSH6 pathogenic variants (n = 29; range, 43–65 y) versus 48 years in carriers of MLH1 and 49 years in carriers of MSH2 pathogenic variants.[381] In carriers of PMS2 pathogenic variants, the endometrial cancer risk at age 70 years has been reported to be 15%.[385] Prospective data collected in the Colon Cancer Family Registry program yielded 5-year endometrial cancer risks of about 3% and 10-year endometrial cancer risks of about 10% among women with MMR gene pathogenic variants.[415] A prospective study using pooled European registry data of 1,942 MMR carriers without prior cancer reported a cumulative incidence of endometrial cancer of 34% in MLH1 carriers, 51% in MSH2 carriers, 49% in MSH6 carriers, and 24% in PMS2 carriers.[5] Women with loss of MSH2 protein expression caused by an EPCAM pathogenic variant are also at risk of endometrial cancer depending upon the location of the variant in EPCAM. One study found a 12% (95% CI, 0%–27%) cumulative risk of endometrial cancer in EPCAM deletion carriers.[392]
A study of 127 women with Lynch syndrome who had endometrial cancer as their index cancer were found to be at significantly increased risk of other cancers. The following elevated risks were reported: CRC, 48% (95% CI, 27.2%–58.3%); kidney, renal pelvis, and ureter cancer, 28% (95% CI, 11.9%–48.6%); urinary bladder cancer, 24.3% (95% CI, 8.56%–42.9%; and breast cancer, 2.51% (95% CI, 1.17%–4.14%).[416]
In a study of 113 families that carried MSH6 pathogenic variants from the Colon Cancer Family Registry, female MSH6 carriers had a 26-fold increased incidence of endometrial cancer (HR, 25.5; 95% CI, 16.8–38.7) compared with the general population. A sixfold increased incidence of other cancers associated with Lynch syndrome (HR, 6.0; 95% CI, 3.4–10.7) was observed compared with the general population, but not among male MSH6 carriers.[6]
Lynch syndrome–associated endometrial cancer is not limited to the endometrioid subtype, and the spectrum of uterine tumors in Lynch syndrome may include clear cell carcinoma, uterine papillary serous carcinoma, and malignant mixed Müllerian tumors.[417] Also, endometrial cancer most commonly arises from the lower uterine segment. (Refer to the Endometrial cancer screening in Lynch syndrome section of this summary for information about screening methods.)
Cancer risk in Lynch syndrome beyond CRC and endometrial cancer
Multiple studies demonstrate an increased risk of additional malignancies associated with Lynch syndrome, including cancers of the stomach, pancreas, ovary, small intestine, and brain, transitional cell carcinoma of the bladder, ureters, and renal pelvis, and sebaceous adenomas of the skin.[409,410,418–421] In addition, some studies have suggested an association with breast, prostate, and adrenal cortex cancers.[415,419,422–424] The strength of the association for many of these malignancies is limited by the majority of studies having a small sample size (and consequently, wide CIs associated with relative risk [RR]), the retrospective nature of the analyses, and referral or ascertainment bias.
The largest prospective study to date is of 446 unaffected carriers of pathogenic variants from the Colon Cancer Family Registry.[415] The Colon Cancer Family Registry is an international cohort with both population-based and clinic-based recruitment from six centers in North America and Australia. Control subjects were noncarriers from families with a known MMR pathogenic variant. Three subcohorts were used to analyze the risk of CRC (365 carriers, 903 noncarriers), endometrial cancer (215 carriers, 523 noncarriers), and other cancers (446 carriers, 1,029 noncarriers). Participants who were followed for up to 10 years demonstrated an increased SIR for CRC (SIR, 20.48; 95% CI, 11.71–33.27; P < .01), endometrial cancer (SIR, 30.62; 95% CI, 11.24–66.64; P < .001), ovarian cancer (SIR, 18.81; 95% CI, 3.88–54.95; P < .001), gastric cancer (SIR, 9.78; 95% CI, 1.18–35.30; P = .009), renal cancer (SIR, 11.22; 95% CI, 2.31–32.79; P < .001), bladder cancer (SIR, 9.51; 95% CI, 1.15–34.37; P = .009), pancreatic cancer (SIR, 10.68; 95% CI, 2.68–47.70; P = .001), and female breast cancer (SIR, 3.95; 95% CI, 1.59–8.13; P = .001).[415]
A well-described variant of Lynch syndrome whose phenotype includes multiple cutaneous neoplasms (including sebaceous adenomas, sebaceous carcinomas, and keratoacanthomas) and CRC is Muir-Torre syndrome.[425,426] Pathogenic variants in the MLH1, MSH2, and MSH6 genes have been found in Muir-Torre families with an increased prevalence described among MSH2 carriers.[427–434] A study of 1,914 unrelated MLH1 and MSH2 probands found MSH2 to be more common in individuals with the Muir-Torre syndrome phenotype. Of 15 individuals with sebaceous skin tumors, 13 (87%) had MSH2 pathogenic variants compared with two individuals who had MLH1 pathogenic variants (P = .05).[435] Evidence of defective DNA MMR activity using IHC or MSI testing was reported in 69 of 163 randomly collected sebaceous neoplasms (42%), suggesting that this is a common mechanism for the development of these lesions, and that testing for defective MMR in sebaceous neoplasms would be an ineffective means to screen for Lynch syndrome or Muir-Torre syndrome.[436] (Refer to the Sebaceous Carcinoma section in the PDQ summary on Genetics of Skin Cancer for more information about cutaneous neoplasms in Muir-Torre syndrome.)
Table 12. Lynch Syndrome–Associated Cancers and Cumulative Risk Up to Age 70 Yearsa
bEvolving data suggest a potential association between Lynch syndrome and breast and prostate cancers. (Refer to the Additional cancers potentially associated with Lynch syndrome section of this summary for more information about these cancers.)
Additional cancers potentially associated with Lynch syndrome
Additional tumors are being considered as part of the spectrum of Lynch syndrome, but this is controversial. Breast and prostate cancers have been raised as possible Lynch syndrome–associated tumors such that MMR genes are now included on multigene (panel) tests for these cancers.
Breast cancer
The issue of breast cancer risk in Lynch syndrome has been controversial.
Retrospective studies have been inconsistent, but several have demonstrated microsatellite instability in a proportion of breast cancers from individuals with Lynch syndrome;[452–455] one of these studies evaluated breast cancer risk in individuals with Lynch syndrome and found that it is not elevated.[455] However, the largest prospective study to date of 446 unaffected carriers of pathogenic variants from the Colon Cancer Family Registry [415] who were followed for up to 10 years reported an elevated SIR of 3.95 for breast cancer (95% CI, 1.59–8.13; P = .001).[415] The same group subsequently analyzed data on 764 carriers of MMR gene pathogenic variants with a prior diagnosis of colorectal cancer. Results showed that the 10-year risk of breast cancer following colorectal cancer was 2% (95% CI, 1%–4%) and that the SIR was 1.76 (95% CI, 1.07–2.59).[456] A series from the United Kingdom composed of clinically referred Lynch syndrome kindreds, with efforts to correct for ascertainment, showed a twofold increased risk of breast cancer in 157 MLH1 carriers but not in carriers of other MMR variants.[457] Results from a meta-analysis of breast cancer risk in Lynch syndrome among 15 studies with molecular tumor testing results revealed that 62 of 122 breast cancers (51%; 95% CI, 42%–60%) in MMR pathogenic variant carriers were MMR-deficient. In addition, breast cancer risk estimates among a total of 21 studies showed an increased risk of twofold to 18-fold in eight studies that compared MMR variant carriers with noncarriers, while 13 studies did not observe statistical evidence for an association of breast cancer risk with Lynch syndrome.[458]
A number of subsequent studies have suggested the presence of higher breast cancer risks than previously published,[348,349,459,460] although this has not been consistently observed.[341] Through a study of 325 Canadian families with Lynch syndrome, primarily encompassing MLH1 and MSH2 carriers, the lifetime cumulative risk for breast cancer among MSH2 carriers was reported to be 22%.[459] Similarly, breast cancer risks were elevated in a study of 423 women with Lynch syndrome, with substantially higher risks among those with MSH6 and PMS2 pathogenic variants, compared with MLH1 and MSH2 pathogenic variants.[349] In fact, breast cancer risk to age 60 years was 37.7% for PMS2, 31.1% for MSH6, 16.1% for MSH2, and 15.5% for MLH1. These findings are consistent with another study of 528 patients with Lynch syndrome–associated pathogenic variants (including MLH1, MSH2, MSH6, PMS2, and EPCAM) in which PMS2 and MSH6 variants were much more frequent among patients with only breast cancer, compared with those with only colorectal cancer (P = 2.3 x 10-5).[348] Additional data to support an association of MSH6 with breast cancer were provided through a study of over 10,000 cancer patients across the United States who had genetic testing.[460] Findings indicated that MSH6 was associated with breast cancer with an odds ratio (OR) of 2.59 (95% CI, 1.35–5.44). Taken together, these studies highlight how the risk profile among patients with Lynch syndrome is continuing to evolve as more individuals are tested through multigene panel testing, with representation of larger numbers of individuals with PMS2 and MSH6 pathogenic variants compared with prior studies. In the absence of definitive risk estimates, individuals with Lynch syndrome are screened for breast cancer on the basis of family history.[461]
Prostate cancer
Prostate cancer was found to be associated with Lynch syndrome in a study of 198 families from two U.S. Lynch syndrome registries in which prostate cancer had not originally been part of the family selection criteria. Prostate cancer risk in relatives of carriers of MMR gene pathogenic variants was 6.3% at age 60 years and 30% at age 80 years, versus a population risk of 2.6% at age 60 years and 18% at age 80 years, with an overall HR of 1.99 (95% CI, 1.31–3.03).[422] A 2014 meta-analysis supports this association, finding an estimated RR of 3.67 (95% CI, 2.32–6.67) for prostate cancer in men with a known MMR pathogenic variant.[462] This risk is possibly increased in those with MSH2 pathogenic variants.[424,462] Notwithstanding prevalent controversy surrounding routine prostate-specific antigen (PSA) screening, the authors suggested that screening by means of PSA and digital rectal exam beginning at age 40 years in male MMR gene carriers would be “reasonable to consider.”[422] A study of 692 men with metastatic prostate cancer unselected for family history of cancer or age at diagnosis identified germline MMR pathogenic variants in four men (0.5%).[463] Currently, molecular and epidemiological evidence supports prostate cancer as one of the Lynch syndrome cancers. As with breast cancer,[462] additional studies are needed to define absolute risks and age distribution before surveillance guidelines for prostate cancer can be developed for carriers of MMR pathogenic variants. For more information about prostate cancer and Lynch syndrome, see the DNA mismatch repair genes (Lynch syndrome) section in Genetics of Prostate Cancer.
Adrenocortical cancer
In a series of 114 ACC cases, of which 94 patients had a detailed family history assessment and Li-Fraumeni syndrome was excluded, three patients had family histories that were suggestive of Lynch syndrome. The prevalence of MMR gene pathogenic variants in 94 families was 3.2%, similar to the proportion of Lynch syndrome among unselected colorectal and endometrial cancer patients. In a retrospective review of 135 MMR gene pathogenic variant–positive Lynch syndrome families from the same program, two probands were found to have had a history of ACC. Of the four ACCs in which MSI testing could be performed, all were MSS. These data suggest that if Lynch syndrome is otherwise suspected in an ACC index case, an initial evaluation of the ACC using MSI or IHC testing may be misleading.[423]
Other cancers
Several additional cancers have been found to be associated with Lynch syndrome in some studies, but further investigation is warranted. Table 12 compares the risk of these cancers in the general population with that of individuals with Lynch syndrome.
Management of Lynch syndrome
Screening and surveillance in Lynch syndrome
Colon cancer screening and surveillance in Lynch syndrome
Several aspects of the biologic behavior of CRC and its precursor lesion, the adenomatous polyp, in individuals with Lynch syndrome support a different approach to CRC screening in this population as compared with those recommendations for average-risk people in the general population. At present, the recommendations for cancer screening and surveillance in Lynch syndrome consider the differences in cancer risks as compared with those in the general population due to the causative germline deficiency in the MMR system. The following biological differences form the basis of the currently implemented screening strategies in Lynch syndrome:
Carriers of Lynch syndrome pathogenic variants have an increased risk of developing colon adenomas and the onset of adenomas appears to occur at a younger age than in pathogenic variant–negative individuals from the same families.[464] The risk of a carrier of MMR pathogenic variants developing adenomas has been reported to be 3.6 times higher than the risk in noncarriers.[464] By age 60 years, 70% of the carriers developed adenomas, compared with 20% of noncarriers. Most of the adenomas in carriers had absence of MMR protein expression and were more likely to have dysplastic features, compared with adenomas from control subjects.[464]
In one study, the mean age at diagnosis of adenoma in carriers was 43.3 years (range, 23–63.2 y), and the mean age at diagnosis of carcinoma was 45.8 years (range, 25.2–57.6 y).[464]
There is a right-sided predominance of colon cancer.
A larger proportion of Lynch syndrome CRCs (60%–70%) occur in the right colon, suggesting that sigmoidoscopy alone is not an appropriate screening strategy and that a colonoscopy provides a more complete structural examination of the colon. Evidence-based reviews of surveillance colonoscopy in Lynch syndrome have been reported.[125,465,466] The incidence of CRC throughout life is substantially higher in patients with Lynch syndrome, suggesting that the most-sensitive test available should be used. (Refer to Table 13 for available colon surveillance recommendations.)
The adenoma-carcinoma sequence is accelerated.
The progression from normal mucosa to adenoma to cancer is accelerated,[467,468] suggesting that screening should be performed at shorter intervals (every 1–2 years) and with colonoscopy.[468–471] It has been demonstrated that carriers of MMR gene pathogenic variants develop detectable adenomas at an earlier age than do noncarriers.[464,464] It is not known whether this reflects a greater prevalence of adenomas or the presence of larger adenomas with better detection in Lynch syndrome.
Evidence for the use of colonoscopy for CRC screening and surveillance in Lynch syndrome
The risk of CRC in Lynch syndrome has been studied and updated in a Finnish screening trial, which spans from the early 1980s to present.[468,472] Over the course of this trial, the design of the longitudinal study has evolved. In the earliest period, information about each individual’s variant status was unknown and study participants were eligible based on fulfillment of clinical criteria; the study consisted of some people with a previous cancer or adenoma diagnosis and others without such history who were undergoing asymptomatic screening while the comparison group was composed of individuals from those same families who refused screening. Many of these people (68%) had screening with x-ray contrast/barium enema. Colonoscopy was the approach used for carriers of MMR pathogenic variants when this information was obtainable and the interval between exams was shortened from 5 years to 3 years to 2 years, based on results from the study over time.
A 15-year controlled screening trial conducted in this series demonstrated a reduction in the incidence of CRC, CRC-specific mortality, and overall mortality with colonoscopy in individuals from Lynch syndrome families.[468] Colonic screening was provided at 3-year intervals in 133 individuals from Lynch syndrome families and 119 controls from these families had no screening. Among those screened, 8 individuals (6%) developed CRC compared with 19 control subjects (16%), for a risk reduction of 62% with screening. Furthermore, all CRCs in the screened group were local, causing no deaths, while there were 9 deaths caused by CRC in the control group. There was also a benefit in overall mortality in the screened group with 10 deaths in the screened group and 26 deaths in the control group (P = .003).
The series subsequently limited its attention to subjects without prior diagnosis of adenoma or cancer. The eligible 420 carriers of pathogenic variants had a mean age of 36 years and underwent an average of 2.1 colonoscopies, with a median follow-up of 6.7 years. Adenomas were detected in 28% of subjects. Cumulative risk of one or more adenomas by age 60 years was 68.5% in men and 48.3% in women. Notably, risk of detecting cancer in those free of cancer at baseline exam, and thus regarded as interval cancers, by age 60 years was 34.6% in men and 22.1% in women. The combined cumulative risk of adenoma or cancer by age 60 years was 81.8% in men and 62.9% in women. For both adenomas and carcinomas, about one-half were located proximal to the splenic flexure. While the rates for CRC despite colonoscopy surveillance appear high, the recommended short intervals were not regularly adhered to in this nonrandomized series. These authors recommended surveillance at 2-year intervals. This is in line with most consensus guidelines (refer to Table 13), in which the appropriate colonoscopy screening interval remains every 1 to 2 years. Analysis of colonoscopic surveillance data in 242 carriers of pathogenic variants 10 years after testing shows 95% compliance in surveillance procedures for CRC and endometrial cancer. Although not all CRCs were prevented, mortality was comparable with variant-negative relatives. However, this may be attributable to the modest sample size of the study.[472]
Individuals with Lynch syndrome are at an increased risk of developing synchronous CRC. Of 5,304 CRC cases in the Danish HNPCC Register, including 774 with Lynch syndrome, the relative risks of synchronous CRC (>1 CRC) diagnosed within 1 year of primary CRC for Lynch syndrome, familial CRC (cases meeting Amsterdam I or II criteria) and metachronous CRC (1 CRC at age <50 y or >2 CRCs at age >50 y) were 5.6, 3.2, and 1.9, respectively, compared with sporadic CRC. Thus, the increased risk of synchronous CRC in patients with a strong family history of CRC, and especially Lynch syndrome, should be considered in preoperative colonoscopic examinations.[473]
Given that colonoscopy is the accepted measure for colon cancer surveillance, preliminary data suggest that the use of chromoendoscopy, such as with indigo carmine, may increase the detection of diminutive, histologically advanced adenomas.[474,475]
When an adenoma is detected, the question of whether to test the adenoma for MSI/IHC is raised. One study of patients with prior CRC and known MMR pathogenic variants found eight of 12 adenomas to have both MSI and IHC protein loss.[476] However, the study authors emphasized that normal MSI/IHC testing in an adenoma does not exclude Lynch syndrome. Abnormal MSI/IHC are uncommon in the smallest adenomas, and more prevalent in adenomas larger than 8 mm, which also suggests that the MMR defect is acquired in the growing adenoma.[477]
Special considerations: The impact of gene-specific variability in cancer risk on CRC screening recommendations in Lynch syndrome
Because of the variability of gene-specific CRC risks, experts in the field have proposed gene-specific screening and surveillance recommendations. For example, a European consortium [386] made a clinical recommendation for delaying the onset of colorectal and endometrial cancer screening to age 30 years, in line with their recommendation for later initiation of screening for carriers of MSH6 pathogenic variants. Additionally, a 2015 review by an ad hoc American virtual workgroup involved in the care of Lynch syndrome patients and families concluded that despite multiple studies indicating reduced penetrance in monoallelic PMS2 carriers, they could not recommend any changes to Lynch syndrome cancer surveillance guidelines for this group.[382]
Available recommendations for colon surveillance in individuals with Lynch syndrome are summarized in Table 13. Most organizations tailor surveillance recommendations for each specific gene.[123,478–480] All of the screening recommendations assume findings are normal. A more aggressive screening schedule might be considered on an individualized basis.
Table 13. Gene-Specific Practice Guidelines for Colon Surveillance of Lynch Syndromea
Organization
MLH1
MSH2
MSH6
PMS2
EPCAM
CRC = colorectal cancer; EHTG = European Hereditary Tumor Group; ESCP = European Society of Coloproctology; ESMO = European Society for Medical Oncology; MMR = mismatch repair; NCCN = National Comprehensive Cancer Network.
aThis table summarizes available guidelines from 2014 and later. Other organizations, including the American Cancer Society, have published guidelines before 2014.[481]
bU.S. Multi-Society Task Force on Colorectal Cancer includes the following organizations: American Academy of Family Practice, American College of Gastroenterology, American College of Physicians-American Society of Internal Medicine, American College of Radiology, American Gastroenterological Association, American Society of Colorectal Surgeons, and American Society for Gastrointestinal Endoscopy.
High-quality colonoscopy at age 20–25 y or 2–5 y prior to earliest CRC in the family if it was diagnosed before age 25 y; repeat colonoscopy every 1–2 y
High-quality colonoscopy at age 20–25 y or 2–5 y prior to earliest CRC in the family if it was diagnosed before age 25 y; repeat colonoscopy every 1–2 y
High-quality colonoscopy at age 30–35 y or 2–5 y prior to earliest CRC in the family if it was diagnosed before age 30 y; repeat colonoscopy every 1–3 y
High-quality colonoscopy at age 30–35 y or 2–5 y prior to earliest CRC in the family if it was diagnosed before age 30 y; repeat colonoscopy every 1–3 y
NCCN recommends that EPCAM carriers be managed the same as MSH2 carriers. High-quality colonoscopy at age 20–25 y or 2–5 y prior to the earliest CRC in the family if it was diagnosed before age 25 y; repeat colonoscopy every 1–2 y
Colonoscopy at age 25 y or 5 y prior to earliest CRC if diagnosed before age 25 y; repeat every 1–2 y
Colonoscopy at age 25 y or 5 y prior to earliest CRC if diagnosed before age 25 y; repeat every 1–2 y
Colonoscopy at age 35 y or 5 y prior to earliest CRC if diagnosed before age 25 yc; repeat every 1–2 y
Colonoscopy at age 35 y or 5 y prior to earliest CRC if diagnosed before age 25 y; repeat every 1–2 y
Not addressed
British Society of Gastroenterology (BSG)/ Association of Coloproctology of Great Britain and Ireland (ACPGBI)/ United Kingdom Cancer Genetics Group (UKCGG) (2020) [478]
Colonoscopy at age 25 y; repeat every 2 y until age 75 y
Colonoscopy at age 25 y; repeat every 2 y until age 75 y
Colonoscopy at age 35 y; repeat every 2 y until age 75 y
Colonoscopy at age 35 y; repeat every 2 y until age 75 y
EPCAM carriers should be managed as those with MSH2 pathogenic variants
European guidelines from the EHTG and ESCP; updated Mallorca group guidelines (2021) [479]
Colonoscopy at age 25 y; repeat every 2–3 y
Colonoscopy at age 25 y; repeat every 2–3 y
Colonoscopy at age 35 y; repeat every 2–3 y
Colonoscopy at age 35 y; repeat every 2–3 yd
Not addressed
U.S. Multi-Society Task Force on Colorectal Cancer (2014)b [316]
Colonoscopy beginning at age 20–25 y for 2–5 y prior to earliest CRC if before age 25 y; repeat every 1–2 ye
Cancer of the endometrium is the most common extracolonic cancer observed in Lynch syndrome families, affecting at least one female in about 50% of Lynch syndrome families. (Refer to the Endometrial cancer section of this summary for more information about gene-specific risks of endometrial cancer in carriers of MMR pathogenic variants.)
In the general population, the diagnosis of endometrial cancer is generally made when women present with symptoms like abnormal or postmenopausal bleeding. Endometrial sampling is performed to provide a histological specimen for diagnosis. Eighty percent of women with endometrial cancer present with stage I disease, and there are no data to suggest that the clinical presentation in women with Lynch syndrome differs from that in the general population.
Given their substantial increased risk of endometrial cancer, endometrial cancer screening has been suggested for women with Lynch syndrome who have not had risk-reducing hysterectomies. Proposed screening methods include transvaginal ultrasound (TVUS) (not recommended in premenopausal patients) and/or endometrial biopsy. However, current NCCN guidelines suggest that these screening methods may not benefit women with Lynch syndrome. Screening via endometrial biopsy can be considered in patients with Lynch syndrome, due to its high levels of sensitivity and specificity. Screening may begin at age 30 to 35 years and can be repeated every 1 to 2 years. TVUS, on the other hand, is not sensitive or specific at detecting endometrial cancer. However, this screening method can be considered in women with Lynch syndrome based on a provider’s judgment.[123]
Two studies have examined the use of TVUS in endometrial screening for women with Lynch syndrome.[482,483] In one study of 292 women from Lynch syndrome families or “Lynch syndrome-like/HNPCC-like” families, TVUS did not detect any endometrial cancer cases. However, two interval cancers developed in symptomatic women.[482] In a second study, 41 women with Lynch syndrome were enrolled in a TVUS screening program. Of 179 TVUS procedures performed, 17 scans were abnormal. Three of the 17 women with abnormal scans had complex atypical hyperplasia on endometrial sampling, while 14 had normal endometrial sampling. However, TVUS failed to identify one patient who presented with abnormal bleeding 8 months after a normal TVUS was performed; this patient was diagnosed with stage IB endometrial cancer.[483] Both of these studies concluded that TVUS is neither sensitive nor specific.
A study of 175 women with Lynch syndrome, which included both endometrial sampling and TVUS, showed that endometrial sampling improved sensitivity when compared with TVUS. Endometrial sampling found 11 of the 14 cases of endometrial cancer. Two of these cases were interval cancers that developed in symptomatic women, and one case was an occult endometrial cancer found at the time of hysterectomy. Endometrial sampling also identified 14 additional cases of endometrial hyperplasia. Among the group of 14 women with endometrial cancer, ten also had TVUS screening with endometrial sampling. Four of the ten women had abnormal TVUS, while six women had normal TVUS.[484] While this cohort study demonstrated that endometrial sampling may have benefits over TVUS for endometrial screening, there are no data that predict that screening with any other modality has benefits for endometrial cancer survival in women with Lynch syndrome.
Estimates of the cumulative lifetime risk of ovarian cancer in Lynch syndrome patients range from 3.4% to 22%.[4,365,440–442] NCCN does not recommend routine ovarian cancer screening in individuals with Lynch syndrome. However, CA-125 and pelvic ultrasound are recommended for planning risk-reducing surgery.[123]
Level of evidence: None assigned
Risk-reducing surgeries for the prevention of gynecologic cancers in Lynch syndrome
Risk-reducing surgery is an effective strategy for preventing endometrial and ovarian cancers in Lynch syndrome families. A retrospective study of 315 women with pathogenic MMR gene variants compared the rate of endometrial and ovarian cancers among women who did and did not have hysterectomies and oophorectomies. The mean follow-up periods for endometrial cancer were 13.3 years in the surgical group and 7.4 years in the nonsurgical group. The mean follow-up periods for ovarian cancer were 11.2 years in the surgical group and 10.6 years in the nonsurgical group. In the surgical group, no cancers were diagnosed. In contrast, 33% of women were diagnosed with endometrial cancer, and 5.5% of women were diagnosed with ovarian cancer in the nonsurgical group.[487] Cost-effectiveness–analysis modeling of risk-reducing surgeries (prophylactic hysterectomy and bilateral salpingo-oophorectomy) versus nonsurgical screening was conducted in a theoretical population of 30-year old MMR pathogenic variant carriers. This analysis revealed that prophylactic surgery was cost-effective and yielded higher QALY.[447] A subsequent modeling study evaluated multiple screening and surgical strategies. This study found that annual screening beginning at age 30 years followed by risk-reducing surgery at age 40 years was the most effective strategy.[488]
Additional extracolonic cancer screening in Lynch syndrome
The decision to screen for other Lynch syndrome–associated cancers is done on an individual basis and relies on the cancers reported among FDRs and SDRs with Lynch syndrome.
Gastric and small bowel cancers
The lifetime risk of gastric cancer is approximately 8% for male Lynch syndrome carriers and 5% for female Lynch syndrome carriers.[443] Recent epidemiological data report a decreasing trend in the diagnosis of gastric cancer than was previously reported, which was as high as 13%. The histological characterization of most Lynch syndrome–associated gastric cancers are of the intestinal type and may therefore be detected using screening esophagogastroduodenoscopy (EGD).[443,489] NCCN recommends that EGD with random biopsy of the proximal and distal stomach be initiated at age 30 to 40 years in individuals with Lynch syndrome. This screening can be repeated every 2 to 4 years. Screening can be initiated before age 30 years if any of the following are present: a family history of cancers in the upper GI system, incomplete or extensive gastric intestinal metaplasia, gastric/duodenal adenomas, or Barrett’s esophagus with dysplasia. Other risk factors for gastric cancer include the following: male sex, older age, an MLH1 or MSH2 pathogenic variant, Asian ethnicity, residing in or emigrating from countries with a high background incidence of gastric cancer, and chronic autoimmune gastritis.[123]
There are variable reports on the lifetime risk of small bowel cancer associated with Lynch syndrome, ranging from less than 1% to 12%.[4,371,439–441,444] Approximately 6.9% of all duodenal cancer cases are attributed to Lynch syndrome.[79] Most small bowel malignancies are confined to the duodenum and the ileum, which are within endoscopic reach using EGD and colonoscopy (with dedicated ileal intubation), respectively. Other modalities to assess for small bowel lesions include CT enterography and capsule endoscopy but cost-effectiveness analyses do not support use of these evaluations for routine screening in Lynch syndrome.[442]
In a single-center retrospective study, researchers analyzed the prevalence of clinically actionable endoscopic findings in 323 asymptomatic Lynch syndrome carriers undergoing EGD for upper GI cancer surveillance.[490] Sixty-five clinically actionable findings were identified in 57 patients (17.6%), including five individuals with upper GI cancers (1.5%)–which were all detected at an early stage. Cancers were diagnosed at a mean age of 60.2 years (range, 50–73 y). Three of the individuals with upper GI cancers were women. Four out of five individuals with upper GI cancers had an MSH2 pathogenic variant, and one had an MLH1 pathogenic variant. One patient had Barrett’s esophagus–related esophageal adenocarcinoma, one patient had a type 3 gastric neuroendocrine tumor, one patient had a gastric adenocarcinoma, and two patients had duodenal adenocarcinomas. These malignancies were detected in Lynch syndrome carriers on baseline EGDs or up to 16 months after surveillance EGDs. The study’s investigators concluded that additional research is needed to investigate the upper GI cancers that developed in the short interval between EGDs.
Esophageal findings in this study included Barrett’s esophagus, which was detected in 6.5% of participants. This percentage is similar to the prevalence of Barrett’s esophagus in North American individuals with gastroesophageal reflux disease.[490]
In addition, 261 subjects underwent gastric biopsy sampling, and the following findings were observed:
Ten patients had H. pylori (3.8%).
Fifteen patients had gastric intestinal metaplasia (5.7%).
Five patients had duodenal adenomas (1.5%) at a mean age of 55.8 years (range, 27–75 y). One patient had an adenoma with high-grade dysplasia, and one patient had an adenoma with tubulovillous histology. Four adenomas were found in the third part of the duodenum, and one adenoma was found in the second part of the duodenum.
Two patients had gastric adenomas (0.6%). One of these patients had an adenoma with high-grade dysplasia. Patients had gastric adenomas at a mean age of 71.6 years (range, 70–73 y).
EGD surveillance is strongly recommended in patients with Lynch syndrome, given the high prevalence and high incidence of clinically actionable findings on EGD and the favorable benefit of identifying these findings at an early stage.
Urinary tract malignancies include those of the transitional cell type of the renal pelvis and ureters, and the bladder. The associated lifetime risk of these malignancies is variable, ranging from less than 1% to as high as 25%, with higher estimates related to pooling the cancers found in different locations within the urinary tract and including the bladder.[4,371,440,441,444,445] Studies that have evaluated urinary cytology as a potential screening modality revealed that it was associated with low sensitivity and a high false-positive rate and ultimately leads to additional evaluation that is often invasive (i.e., cystoscopy). Screening for renal pelvis, ureter, and/or bladder cancers is generally not recommended in individuals with Lynch syndrome. However, NCCN suggests considering urothelial cancer surveillance for individuals with a family history of urothelial cancer or for individuals (especially men) with an MSH2 pathogenic variant. Annual urinalysis can begin at age 30 to 35 years in these individuals.[123]
An elevated risk of pancreatic cancer among Lynch syndrome carriers has been supported by two cohort studies that adjust for ascertainment bias. One study reported a cumulative risk of pancreatic cancer of 3.7% by age 70 years and an 8.6-fold increase compared with the general population. [451] Another prospective study using data from the Colon Cancer Family Registry reported an SIR of 10.7 with cumulative risk of 0.95%.[415] Results of these studies have supported an expert consensus that recommended screening for pancreatic cancer in individuals with Lynch syndrome and an FDR with pancreatic cancer, similar to other high-risk populations with comparable risk.[491]
Pancreatic cancer screening may be considered in individuals with MLH1, MSH2, or MSH6 pathogenic variants if they have one or more FDRs or SDRs with exocrine pancreatic cancer (if these family members are on the same side of the family as the individual with Lynch syndrome). Pancreatic cancer screening can begin at age 50 years or 10 years before the youngest pancreatic cancer diagnosis in the family. Screening typically consists of annual contrast-enhanced magnetic resonance imaging/magnetic resonance cholangiopancreatography (MRCP) and/or endoscopic ultrasound (EUS). However, screening can be done more frequently if abnormal findings are found on MRCP/EUS. NCCN recommends that MRCP/EUS occur at a high-volume center that has experience screening individuals with Lynch syndrome. Health care providers are encouraged to have a discussion with patients about pancreatic screening limitations, including the following: the cost of annual pancreatic cancer screening, the high occurrence of benign and indeterminate pancreatic lesions, and the uncertainty regarding the effectiveness of pancreatic cancer screening.[123]
The Colorectal Adenoma/Carcinoma Prevention Programme (CAPP2) was a double-blind, placebo-controlled, randomized trial to determine the role of aspirin in preventing CRC in patients with Lynch syndrome who were in surveillance programs at a number of international centers.[492] The study randomly assigned 861 participants (mean age, 45 y) to receive aspirin (600 mg/day), aspirin-placebo, resistant starch (30 g/day), or starch-placebo for up to 4 years. Initial CAPP2 trial results for 746 Lynch syndrome patients enrolled in the study were published in 2008 [493] and failed to show a significant preventive effect on incident colonic adenomas or carcinomas (relative risk, 1.0; 95% CI, 0.7–1.4) with a short-term follow-up (mean, 29 months; range, 7–74 months). In 2011 (mean follow-up, 55.7 months), subsequent data were published on 861 individuals randomly assigned to receive aspirin versus aspirin-placebo, which demonstrated that participants who completed at least 2 years of aspirin (per-protocol analysis) had significantly fewer incident CRCs than individuals randomly assigned to receive aspirin-placebo (HR, 0.41; 95% CI, 0.19–0.86, P = .02; incidence rate ratio [IRR], 0.37; 95% CI, 0.18–0.78, P = .008), although there was no significant difference by intention-to-treat analysis (HR, 0.63; 95% CI, 0.35–1.13, P = .12).[492]
In 2020, long-term follow-up data with all participants having surpassed 10 years of follow-up demonstrated a significant reduction in CRC incidence for participants randomly assigned to receive aspirin both by per-protocol analysis (HR, 0.56; 95% CI, 0.34–0.91) and intention-to-treat analysis (HR, 0.65; 95% CI, 0.43–0.97).[494] These long-term data showed that the protective effects of aspirin did not emerge until approximately 5 years after initiation of aspirin and, intriguingly, the protective effects of aspirin (taken in this study for only a finite period of time, although the data on aspirin use post unblinding do not exist) persisted to at least 20 years of follow-up. These data demonstrated that only 24 Lynch syndrome carriers needed to be treated with this finite course of aspirin to prevent one incident CRC. Female CAPP2 participants randomly assigned to receive aspirin versus aspirin-placebo also developed fewer incident endometrial cancers (7 vs. 17 cases), although this difference did not reach statistical significance (HR, 0.50; 95% CI, 0.22–1.11, P = .09). There was no significant difference seen in the incidence of cancers other than CRC and endometrial cancer in individuals randomly assigned to receive aspirin versus aspirin-placebo. There were no significant differences in adverse events between the aspirin and placebo groups, and no serious adverse effects were noted with any treatment.[492] The CAPP2 investigators concluded that aspirin 600 mg/day has a clear benefit for protecting against CRC in individuals with Lynch syndrome. A key limitation of the CAPP2 trial is that the frequency of surveillance studies at the various centers was not reported as being standardized.
To date, there has been no significant preventive benefit identified in CAPP2 participants randomly assigned to receive resistant starch versus starch-placebo (HR for incident CRC, 0.92; 95% CI, 0.62–1.34; P = .63).[495] However, at a planned 10-year follow-up, participants who had been randomized to receive resistant starch had significantly fewer non-CRC Lynch syndrome cancers than patients who received starch-placebo (IRR, 0.52; 95% CI, 0.32–0.84; P = .0075). This difference seems to have been driven by reduced rates of incident upper-GI tract cancers (gastric, pancreas, biliary, and small bowel cancers).There were 5 upper-GI cancers in participants randomized to take resistant starch and 21 upper-GI cancers in those randomized to take starch-placebo. The biological mechanisms that led to reduced upper-GI tract cancer incidence in Lynch syndrome patients who took resistant starch remain speculative. However, this data have renewed interest in the potential for dietary interventions to be a component of Lynch syndrome cancer prevention.
Experts have speculated that certain Lynch syndrome carriers with lower risks of future incident CRCs (e.g., those with germline PMS2 pathogenic variants, those with prior colectomy, or older individuals) may be less likely to derive benefit from aspirin chemoprevention and may be appropriate for lower dosing.[496] Furthermore, a subgroup analysis of the CAPP2 study also suggested that the chemopreventive effects may be primarily in obese individuals,[497] suggesting that efforts to personalize aspirin chemoprevention recommendations may be appropriate in Lynch syndrome.
The CAPP3 trial, which is evaluating the effect of lower doses of aspirin (blinded 100 mg, 300 mg, and 600 mg enteric-coated aspirin) completed accrual of 1,882 Lynch syndrome carriers in 2019 and data are not expected until at least 5 years of follow-up is complete.[498]
Because of the level 1 evidence in support of aspirin chemoprevention, clinical practice guidelines consistently recommend that individuals with Lynch syndrome consider taking aspirin daily. Optimal aspirin dosage can be determined by the patient’s provider, after having a discussion with the patient about his/her personal risk factors (including pregnancy, in which aspirin use may be contraindicated). NCCN also recommends that providers explain potential advantages and disadvantages of aspirin use to the patient.[123]
For Lynch syndrome carriers unable to take aspirin, it is unclear whether NSAIDs may have a comparable chemopreventive benefit. A 2015 survey of 1,858 participants in the Colon Cancer Family Registry suggested that aspirin and ibuprofen might both reduce incident CRC in Lynch syndrome carriers.[499] Additionally, a recent translational study demonstrated that Lynch syndrome carriers randomly assigned to take naproxen for 6 months had significantly lower colorectal mucosal prostaglandin E2 (versus those randomly assigned to take placebo), and that this was accompanied by immune cell activation and gene expression patterns consistent with epithelial differentiation, suggesting the potential underlying mechanism for CRC chemoprevention in Lynch syndrome.[500]
One of the hallmark features of Lynch syndrome is the presence of synchronous and metachronous CRCs. The incidence of metachronous CRCs has been reported to be 16% at 10 years, 41% at 20 years, and 63% at 30 years after segmental colectomy.[407] Because of the increased incidence of synchronous and metachronous neoplasms, the recommended surgical treatment for a patient with Lynch syndrome with neoplastic colonic lesions is generally an extended colectomy (total or subtotal). Nevertheless, treatment has to be individualized and has often included segmental colectomy. Mathematical models suggest that there are minimal benefits of extended procedures in individuals older than 67 years, compared with the benefits seen in younger individuals with early-onset cancer. In one Markov decision analysis model, the survival advantage for a young individual with early-onset CRC undergoing an extended procedure could be up to 4 years longer than that seen in the same individual undergoing a segmental resection.[501] The recommendation for an extended procedure must be balanced with the comorbidities of the patient, the clinical stage of the disease, the wishes of the patient, and surgical expertise. No prospective or retrospective study has shown a survival advantage for patients with Lynch syndrome who underwent an extended resection versus a segmental procedure.
Two studies have shown that patients who undergo extended procedures have fewer metachronous CRCs and additional surgical procedures related to CRC than do patients who undergo segmental resections.[407,502] Balancing functional results of an extended procedure versus a segmental procedure is of paramount importance. Although most patients adapt well after an abdominal colectomy, some patients will require antidiarrheal medication. A decision model compared QALYs for a patient aged 30 years undergoing an abdominal colectomy versus a segmental colectomy.[503] In this model, there was not much difference between the extended and segmental procedure, with QALYs being 0.3 years more in patients undergoing a segmental procedure than in those undergoing an extended procedure.[503]
A retrospective study from the Creighton University Hereditary Cancer Center evaluated the incidence of metachronous CRC and survival in 64 Lynch syndrome pathogenic variant carriers with right-sided colon cancer undergoing either proximal colectomy or total or subtotal colectomy.[504] Disease incidence was lower in those undergoing a more extensive resection, with one of 16 patients (6.3%) developing metachronous CRC. In those undergoing proximal colectomy, metachronous CRC developed in 13 of 48 patients (27%). There was no statistical difference in survival within a 25-year period after initial surgery. The authors concluded that the treatment of Lynch syndrome patients with right-sided colon cancer at presentation should be individualized to consider quality of life, functional outcomes, and patient preferences.
When considering surgical options, it is important to recognize that a subtotal or total colectomy will not eliminate the rectal cancer risk. The lifetime risk of developing cancer in the rectal remnant after an abdominal colectomy has been reported to be 12% at 12 years post-colectomy.[505] In addition to the general complications of surgery are the potential risks of urinary and sexual dysfunction and diarrhea after an extended colectomy; these risks increase as the anastomosis becomes more distal. Therefore, the choice of surgery must be made on an individual basis by the surgeon and the patient.
In patients with Lynch syndrome and rectal cancer, similar surgical options (extended vs. segmental resection) and considerations must be given. Extended procedures include restorative proctocolectomy and IPAA if the sphincter can be saved, or proctocolectomy with loop ileostomy if the sphincter cannot be saved. The risk of metachronous colon cancer after segmental resection for an index rectal cancer has been reported to be between 15% and 27%.[456,506] Two retrospectives studies reported a 15% and 18% incidence of metachronous colon cancer after segmental rectal cancer–resection in patients with Lynch syndrome.[507,508] In one of the studies, the combined risk of metachronous high-risk adenomas and cancers was 51% at a median follow-up of 101.7 months after proctectomy.[508]
There are no data about fertility after surgery in Lynch syndrome patients. In female FAP patients, no difference in fecundity after abdominal colectomy and IRA has been reported, whereas there is a 54% decrease in fecundity in patients who undergo restorative proctocolectomy with IPAA compared with the general population.[509] Another study in which a questionnaire was sent to FAP patients reported a similar prevalence of fertility problems among patients who had undergone IRA, IPAA, and proctocolectomy with end ileostomy. In that study, it was reported that earlier age at the time of surgery was associated with more fertility problems.[510]
In a large Danish registry study, the incidence rate for metachronous CRC was fivefold higher in Lynch syndrome patients, but not significantly higher in familial CRC and moderate familial risk CRC cases when compared with sporadic CRC, demonstrating that the risk of metachronous CRC occurred almost exclusively in Lynch syndrome cases.[473] The IRRs for metachronous CRC were highest in Lynch syndrome patients with MLH1 and MSH2 germline alterations, intermediate in MSH6 carriers, but not in PMS2 carriers when compared with sporadic CRC cases. Furthermore, when comparing the extent of the colon resections performed for primary CRC in Lynch syndrome cases, the IRRs for metachronous CRC were 5.5 for total and subtotal colectomies and 0.9 for segmental colon resections. The absolute risk reduction of metachronous CRC in Lynch syndrome cases with a primary CRC diagnosed before age 60 years and total/subtotal versus segmental colectomies was 63.5% in men and 40.9% in women. These results strongly support subtotal or total versus segmental colectomies for resectable CRC in Lynch syndrome patients with underlying MLH1 or MSH2, and possibly MSH6 germline alterations.
Most clinicians who treat patients with Lynch syndrome will favor an extended procedure at the time of CRC diagnosis. However, as stated above, the choice of surgery must be made on an individual basis by the surgeon and the patient.[511–513]
As discussed in previous sections, MSI is not only a molecular feature of Lynch syndrome but is also present in 10% to 15% of sporadic cases of CRC (largely due to MLH1 hypermethylation or biallelic somatic variants in an MMR gene). Although MSI testing was initially used to screen patients who might harbor pathogenic MMR gene variants, it has been increasingly recognized that MSI has important prognostic and therapeutic implications. The utility of MSI testing beyond identifying Lynch syndrome has made the case for universal MSI screening more compelling and has contributed to its widespread adoption. Several studies have suggested that stage-specific survival is better for MSI-H CRC compared with MSS cancers. Additionally, the chemotherapeutic agent fluorouracil (5-FU) appears ineffective in the adjuvant treatment of resected MSI-H CRC, in contrast to MSS CRC in which this agent is widely utilized for this purpose. Finally, immunomodulation with agents such as checkpoint inhibitors appears effective in the treatment of advanced MSI-H CRC based on early phase 1 and phase 2 studies, while these agents, at least when utilized as monotherapy, show little activity in MSS CRC.
Prognosis of MSI
Although MSI-H tumors account for 15% of all sporadic CRC, they appear to be more frequent in stage II compared with stage III CRC,[514] and are even less common in metastatic disease, being present in only 3% to 4% of metastatic cases.[515] This stage distinction alludes to the possibility of a better prognosis associated with underlying MSI-H status.
Several studies subsequently confirmed the improved survival of stage II MSI-H CRC compared with MSS cases. A meta-analysis of 32 studies of 7,642 cases, including 1,277 with MSI-H, showed a combined HR estimate for overall survival (OS) associated with MSI of 0.65 (95% CI, 0.59–0.71; heterogeneity P = .16; I2 [a measure of the percentage of variation across studies that is due to heterogeneity rather than chance] = 20%).[516] However, while data were limited, tumors with MSI derived no benefit from adjuvant 5-FU (HR, 1.24; 95% CI, 0.72–2.14). Subsequent data from several large randomized clinical trials confirmed the favorable prognosis associated with MSI-H. These included the QUick And Simple And Reliable (QUASAR) trial, which explored the benefit of adjuvant 5-FU–based chemotherapy compared with surgery alone in 1,900 patients with resected stage II CRC. In this study, MSI-H tumors were associated with a recurrence risk of half that of MSS tumors (risk ratio [RR], 0.53; 95% CI, 0.40–0.70).[517] Similar results were seen in the Pan European Trial Adjuvant Colon Cancer (PETACC)-3 trial, a randomized trial of 5-FU with or without irinotecan in resected stage II or stage III CRC.[518] MSI-H status was associated with an OS odds ratio (OR) of 0.39 (95% CI, 0.24–0.65) and this advantage was seen in both stage II and stage III disease.
Consistent with other prior data, clinicopathologic analysis of 85 Lynch syndrome–associated CRCs and 67 sporadic dMMR CRCs demonstrated a significantly superior survival among patients with Lynch syndrome, as well as younger ages at diagnosis and higher numbers of tumor-infiltrating lymphocytes (TILs).[519] Exome sequencing and neoantigen data from a subset of 16 CRC tumors (eight Lynch syndrome CRCs and eight sporadic dMMR CRCs) from this cohort suggest that somatic mutational burden and neoantigen load is significantly higher among Lynch syndrome–associated CRCs than sporadic dMMR CRCs; this was speculated to be the source of the improved survival outcomes and increased TILs.
Given the predilection for MSI-H tumors to involve the right side of the colon, there is a paucity of data on the outcome and prognosis of MSI-H tumors involving the rectum. One study suggested only 2% of rectal cancers are MSI-H.[517] A study of 62 patients with MSI-H rectal cancers from a single institution were followed for a median of 6.8 years. The 5-year rectal cancer–specific survival was 100% for stage I and stage II, 85.1% for stage III, and 60.0% for stage IV disease, suggesting the favorable prognosis associated with MSI-H may also apply to cancers involving the rectum.[506] The authors additionally reported a favorable 26% pathological complete response rate with 5-FU combined with radiation therapy, suggesting that 5-FU given with radiation for the locoregional treatment of rectal cancer may still be effective in the setting of MSI-H tumors. The substantial rate of pathological complete responses demonstrated in this study also reinforces the need for adequate biopsies to assess MSI status before commencing treatment.
The use of adjuvant chemotherapy after surgery for CRC in Lynch syndrome
The finding of MSI in a CRC has been shown in several studies to predict the lack of benefit of adjuvant chemotherapy with 5-FU in resected stage II or stage III colon cancer.[520] This has been a controversial area historically. It was known that loss of DNA MMR activity in cultured colon cancer cells conferred resistance to DNA-damaging agents (the common mechanism of cytotoxic chemotherapy) through loss of the signal to arrest the cell cycle in response to DNA damage that cannot be repaired.[521] This led to the prediction that DNA dMMR tumors may not be fully sensitive to alkylating agents, 5-FU, and platinum-containing drugs.[522–524] Unexpectedly, in 2000, a paper was published suggesting that patients with Dukes C (stage III) CRC with MSI had a substantial survival benefit when given 5-FU–based adjuvant chemotherapy.[525] However, the patients in this analysis had not been randomized to therapy; they were selected for adjuvant chemotherapy based upon clinical status, and inadvertently, the median age in the treatment group was 13 years younger than the controls.
In 2003, however, the outcomes in a randomized controlled prospective trial of adjuvant chemotherapy in 570 colon cancer patients demonstrated no benefit from adjuvant 5-FU in the group with MSI. Moreover, there were nonsignificant trends towards increased mortality when colon cancers with MSI were treated: twofold for stage III cancers and threefold for stage II cancers.[526] Subsequently, ten studies confirmed this, as all failed to show benefit when CRC patients were given 5-FU–based chemotherapy.[520] In contrast, a meta-analysis of randomized trials of 5-FU versus observation suggested a potential benefit of 5-FU in patients with MSI stage III disease. An exploratory subset analysis suggested benefit only in those patients with Lynch syndrome–related MSI. An analysis of stage II patients was not undertaken in this study.[527]
Preclinical data suggests the addition of oxaliplatin to 5-FU can overcome the resistance to 5-FU monotherapy seen in MSI-H tumors.[528] A retrospective analysis of 433 MSI-H stage II and stage III CRC cases (both sporadic and secondary to Lynch syndrome) suggested a benefit in disease-free survival (DFS) with FOLFOX (5-FU and oxaliplatin) compared with surgery alone.[529] There was a trend towards improved DFS utilizing FOLFOX in the subset of patients with MSI due to Lynch syndrome, however, the result was not statistically significant. Additional studies have demonstrated similar survival outcomes irrespective of MSI status with adjuvant chemotherapy including FOLFOX.[530,531]
Tumors that develop via the MSI pathway have more somatic variants than tumors that develop via other pathways. This could imply that dMMR tumors may have more potential antigens (termed neoantigens) and may be more responsive to immune system manipulation than proficient MMR (pMMR) tumors. Microscopically, MSI-H tumors often exhibit abundant tumor-infiltrating lymphocytes, sometimes resulting in a Crohn-like reaction. This histological feature has long suggested the possibility of increased tumor immune surveillance in MSI-H cancers and is one of the main hypotheses for the better stage-specific survival seen in MSI-H compared with MSS cancers.
To test the hypothesis of efficacy of immunomodulation in MSI-H tumors, a phase 2 trial of programmed cell death-1 (PD-1) inhibition was carried out in a small cohort of patients with MSI-H or MSS cancers. Patients with metastatic disease that had failed various chemotherapy regimens were treated with pembrolizumab, an anti–PD-1 immune checkpoint inhibitor.[532] In this small phase 2 study, 32 patients with CRC (11 were dMMR, 21 were pMMR, and 9 others had noncolorectal dMMR tumors) were treated with intravenous pembrolizumab every 14 days. The immune-related response among evaluable patients was 40% (4 of 10) for dMMR CRC tumors, 0% (0 of 18) for pMMR CRC tumors, and 71% (5 of 7) for non-CRC dMMR tumors. The immune-related 20-week progression-free survival was 78% (7 of 9) in patients with dMMR CRC tumors, 11% (2 of 18) in patients with pMMR CRC tumors, and 67% (4 of 6) in patients with non-CRC dMMR tumors. dMMR tumors had a mean of 24-fold more somatic variants than pMMR tumors. Additionally, in this study somatic variants load was associated with prolonged PFS. The authors concluded that MMR status predicted clinical benefit to immune checkpoint blockade with pembrolizumab.
A single-arm phase 2 study (CheckMate 142) of another PD-1 inhibitor, nivolumab, was performed in 74 patients with MSI-H/dMMR CRC that had progressed on prior cytotoxic chemotherapy (including 5-FU, irinotecan, and oxaliplatin).[533] Overall, 31% of patients (23 of 74) experienced an objective response to therapy, and 69% (51 of 74) had disease control for at least 12 weeks. Among patients who responded to nivolumab, the median duration of response was not reached at the time of study analysis (median follow up of 12 months). There was no significant difference in the response rates among individuals with Lynch syndrome–associated metastatic MSI-H/dMMR CRC versus non-Lynch metastatic MSI-H/dMMR CRC in this study. Twenty percent of study participants experienced grade 3 or greater toxicities, most commonly elevations in amylase and/or lipase, and there were no deaths that were attributed to nivolumab.
Based on these data, pembrolizumab 200 mg given intravenously every 3 weeks was approved by the FDA in May 2017 for the treatment of any MSI-H/dMMR metastatic cancer that is refractory to standard therapy and nivolumab 240 mg given intravenously every 2 weeks was granted accelerated approval by the FDA in August 2017 for the treatment of MSI-H/dMMR CRC that is refractory to cytotoxic chemotherapy.
In 2020, treatment-naïve patients with MSI-H/dMMR CRC were enrolled in a phase III trial (KEYNOTE-177) where they were randomized to receive pembrolizumab or chemotherapy. Patients who received pembrolizumab had an increase in PFS when compared with patients who received chemotherapy.[534,535] Subsequently, pembrolizumab became the standard of care for treating metastatic MSI-H/dMMR CRC in the first-line setting. (Refer to the Colon Cancer Treatment summary for more information.)
In another arm of CheckMate 142, 119 individuals with metastatic dMMR CRC were treated with nivolumab plus ipilimumab.[536] The objective response rate was 55% with a 12-week disease control rate of 80%, a 12-month PFS of 71%, and a median duration of response that was not reached. Grade 3 and grade 4 toxicities occurred in 32% of participants (most commonly increased liver function tests) and 13% of all participants discontinued therapy due to toxicity. This was a nonrandomized study, and thus questions remain as to whether the combination of immune checkpoint blockade is superior to PD-1 inhibition alone, especially given the apparent increase in toxicity with combination therapy. On the basis of these data, in July 2018 the FDA granted accelerated approval to nivolumab plus ipilimumab therapy for the treatment of dMMR/MSI-H metastatic CRC that has progressed through prior chemotherapy with a fluoropyrimidine, oxaliplatin, and irinotecan.
A retrospective analysis described the pathological responses of 14 patients with MSI-H tumors after treatment with PD-1 inhibitors (with or without CTLA-4 inhibitors). Eight of the patients in this study had Lynch syndrome and all of the patients had unresectable/metastatic CRCs. Patients underwent resection after they completed treatment. The study demonstrated a pathological complete response (PCR) in 13 of the 14 patients, despite radiographic evidence of persistent disease in 12 of these patients. The discordance between imaging and PCR may be related to significant lymphocyte infiltration in patient tumors. The median duration of treatment was 12 months. However, a PCR was demonstrated in a patient who was treated for only 3 months.[537]
There is debate about when immunotherapeutic agents can be used in patients with non-CRC, MSI-H cancers. Many providers question in which line of therapy immunotherapeutics should be initiated. This question is the subject of multiple ongoing clinical trials. (Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria.)
Vaccines in the treatment or prevention of MSI-related CRC
An alternative approach to immunotherapy in MSI-H CRC involves the use of tumor-directed vaccines. The most promising approaches thus far involve the use of tumor-related neoantigens as epitopes to increase tumor-specific T-cell immunity. Studies are currently under way in the adjuvant treatment of resected stage III CRC (NCT01461148), in patients with metastatic disease (NCT01885702), and in the prevention of CRC in patients with Lynch syndrome (NCT01885702).
Lynch syndrome–related syndromes
Lynch-like or HNPCC-like syndrome
Somatic biallelic MMR gene inactivation is now recognized as a common cause of sporadic MMR deficiency. The literature variably labels these cases as Lynch-like syndrome (LLS). However, this nomenclature can be confusing, since this is a sporadic form of MMR-deficiency, rather than a stand-alone genetic syndrome. For more information, see the Somatic biallelic mismatch repair deficiency (sometimes called Lynch-like syndrome) section and Table 10.
Hamartomatous Polyposis Syndromes
Hamartomatous polyposis syndromes are a distinct and rare group of polyposis diseases characterized by the presence of hamartomatous growths throughout the GI tract. Each syndrome manifests differently, depending on histological type, the number of GI polyps, the number of benign growths, GI cancer risks, and extra-GI cancer risks. Hamartomatous polyposis syndromes include the following:
Cowden syndrome and Bannayan-Riley-Ruvalcaba syndrome (BRRS) are part of a spectrum of conditions known collectively as PTEN hamartoma tumor syndromes (PHTS). Approximately 85% of patients diagnosed with Cowden syndrome, and approximately 60% of patients with BRRS have an identifiable PTEN pathogenic variant.[538] In addition, PTEN pathogenic variants have been identified in patients with very diverse clinical phenotypes.[539] The term PHTS refers to any patient with a PTEN pathogenic variant, irrespective of clinical presentation.
PTEN functions as a dual-specificity phosphatase that removes phosphate groups from tyrosine, serine, and threonine. PTEN pathogenic variants are diverse and can present as nonsense, missense, frameshift, or splice-site variants. Approximately 40% of variants are found in exon 5, which encodes the phosphatase core motif; several recurrent pathogenic variants have been observed at this location.[540] Pathogenic variants in the 5’ end of PTEN or within the phosphatase core of PTEN tend to affect more organ systems.[541]
Operational criteria for the diagnosis of Cowden syndrome have been published and subsequently updated.[542,543] These include major, minor, and pathognomonic criteria that consist of certain mucocutaneous manifestations and adult-onset dysplastic gangliocytoma of the cerebellum (Lhermitte-Duclos disease). An updated set of criteria based on a systematic literature review has been suggested [544] and is currently utilized in the National Comprehensive Cancer Network (NCCN) guidelines.[545] Contrary to previous criteria, the authors concluded that there was insufficient evidence for any features to be classified as pathognomonic. Increased genetic testing (especially multigene panels) has identified individuals with germline PTEN pathogenic variants who do not meet diagnostic criteria for PHTS. Diagnostic criteria will need to be reconciled with these recently discovered phenotypes. Hence, it is unclear whether PHTS diagnoses should be based on clinical features or a positive PTEN genetic test result. The American College of Medical Genetics and Genomics (ACMG) suggests that referral for genetics consultation be considered for individuals with a personal history of or a first-degree relative with the following: 1) adult-onset Lhermitte-Duclos disease or 2) any three of the major or minor criteria that have been established for the diagnosis of Cowden syndrome.[546] Detailed recommendations, including diagnostic criteria for Cowden syndrome, can be found in the NCCN and ACMG guidelines.[545,546] Additionally, a predictive model that uses clinical criteria to estimate the probability of a PTEN pathogenic variant is available; a cost-effectiveness analysis suggests that germline PTEN testing is cost effective if the probability of a variant is greater than 10%.[547]
Over a 10-year period, the International Cowden Consortium (ICC) prospectively recruited a consecutive series of adult and pediatric patients meeting relaxed ICC criteria for PTEN testing in the United States, Europe, and Asia.[548] Most individuals did not meet the clinical criteria for a diagnosis of Cowden syndrome or BRRS. Of the 3,399 individuals recruited and tested, 295 probands (8.8%) and an additional 73 family members carried a germline PTEN pathogenic variant. The authors concluded that melanoma, kidney cancer, and colorectal cancer should be added to the spectrum of cancers associated with PTEN germline pathogenic variants (in addition to breast cancer, thyroid cancer, and endometrial cancer). This conclusion was based on the high melanoma, kidney, and colorectal cancer lifetime risk estimates found in individuals with PTEN pathogenic variants. A second study of approximately 100 patients with a germline PTEN pathogenic variant confirmed these findings and suggested a cumulative cancer risk of 85% by age 70 years.[549]
The age-adjusted risk of CRC was increased in individuals with PTEN pathogenic variants in both studies (SIR, 5.7–10.3).[548,549] In addition, one study found that 93% of individuals with PTEN pathogenic variants who had undergone at least one colonoscopy had polyps.[548] Hyperplastic polyps were the most common polyp histology identified, although adenomas and sessile serrated polyps were also observed. The increased CRC risk in individuals with PTEN pathogenic variants has led to the recommendation of surveillance colonoscopy in these patients.[549,550] However, both the age at which to begin (30–40 y) and the subsequent frequency of colonoscopies (biennial to every 3–5 y) vary considerably and are based on expert opinion.
Table 14. Cancer Risk in Individuals with Germline PTEN Pathogenic Variantsa
Cancer
Age-Adjusted SIR (95% CI)
Age-Related Penetrance Estimates
CI = confidence interval; SIR = standardized incidence ratio.
bOther historical studies have suggested a lower lifetime risk of breast cancer, in the range of 25%–50%.[544] (Refer to the PTEN Hamartoma Tumor Syndromes [Including Cowden Syndrome] section in Genetics of Breast and Gynecologic Cancers for more information.)
Breast
25.4 (19.8–32.0)
85% starting around age 30 yb
Colorectal
10.3 (5.6–17.4)
9% starting around age 40 y
Endometrial
42.9 (28.1–62.8)
28% starting around age 25 y
Kidney
30.6 (17.8–49.4)
34% starting around age 40 y
Melanoma
8.5 (4.1–15.6)
6% with risk beginning in infancy
Thyroid
51.1 (38.1–67.1)
35% with risk beginning in infancy
Peutz-Jeghers syndrome
PJS is an early-onset autosomal dominant disorder characterized by melanocytic macules on the lips, the perioral region, and buccal region; and multiple GI polyps, both hamartomatous and adenomatous.[551–553] Germline pathogenic variants in the STK11 gene at chromosome 19p13.3 have been identified in the vast majority of PJS families.[554–558] GI cancers (including colorectal adenocarcinoma, gastric adenocarcinoma, small intestinal adenocarcinoma, and pancreatic adenocarcinoma) are some of the most common malignancies seen in individuals with PJS. PJS also increases the risk of developing cancers in other organs. For example, the cumulative risks have been estimated to be 32% to 54% for breast cancer [8,559,560] and 21% for ovarian cancer (mainly ovarian sex-cord tumors).[559] The risk of developing pancreatic cancer in individuals with PJS is estimated to be more than 100-fold higher than that of the general population (although these statistics are based on calculations from a small number of individuals with PJS).[559] A systematic review found a lifetime cumulative cancer risk, all sites combined, of up to 93% in patients with PJS.[559,561] Table 15 shows the cumulative risk of these tumors.
Females with PJS are also predisposed to the development of cervical adenoma malignum, a rare and very aggressive adenocarcinoma of the cervix.[562] In addition, females with PJS commonly develop benign ovarian sex-cord tumors with annular tubules, whereas males with PJS are predisposed to development of Sertoli-cell testicular tumors;[563] although neither of these two tumor types is malignant, they can cause symptoms related to increased estrogen production.
Although the risk of malignancy appears to be exceedingly high in individuals with PJS based on the published literature, the possibility that selection and referral biases have resulted in overestimates of these risks should be considered.
Table 15. Cumulative Cancer Risks in Peutz-Jeghers Syndrome Up To Specified Agea
Site
Age (y)
Cumulative Risk (%)b
Reference(s)
GI = gastrointestinal.
aReprinted with permission from Macmillan Publishers Ltd: Gastroenterology [561], copyright 2010.
bAll cumulative risks were increased compared with the general population (P < .05), with the exception of cervix and testes.
cGI cancers include colorectal, small intestinal, gastric, esophageal, and pancreatic.
dWesterman et al.: GI cancer does not include pancreatic cancer.[564]
eDid not include adenoma malignum of the cervix or Sertoli cell tumors of the testes.
PJS is caused by pathogenic variants in the STK11 (also called LKB1) tumor suppressor gene located on chromosome 19p13.[555,556] Unlike the adenomas seen in familial adenomatous polyposis, the polyps arising in PJS are hamartomas. Studies of the hamartomatous polyps and cancers of PJS show allelic imbalance (LOH) consistent with the two-hit hypothesis, demonstrating that STK11 is a tumor suppressor gene.[566,567] However, heterozygous STK11 knockout mice develop hamartomas without inactivation of the remaining wild-type allele, suggesting that haploinsufficiency may be sufficient for initial tumor development in PJS.[568] Subsequently, the cancers that develop in STK11 +/- mice do show LOH;[569] indeed, compound mutant mice heterozygous for pathogenic variants in STK11 +/- and homozygous for pathogenic variants in TP53 -/- have accelerated development of both hamartomas and cancers.[570]
Germline variants of the STK11 gene represent a spectrum of nonsense, frameshift, and missense variants, and splice-site variants and large deletions.[8,554]
Approximately 85% of variants are localized to regions of the kinase domain of the expressed protein. No strong genotype-phenotype correlations have been identified.[8] Up to 30% of variants are large deletions involving one or more exons of STK11, underscoring the importance of deletion analysis in suspected cases of PJS.[554]
STK11 has been unequivocally demonstrated to cause PJS. Although earlier estimates using direct DNA sequencing showed a 50% pathogenic variant detection rate in STK11, studies adding techniques to detect large deletions have found pathogenic variants in up to 94% of individuals meeting clinical criteria for PJS.[554,561,571] Given the results of these studies, it is unlikely that other major genes cause PJS.
Clinical management
NCCN and the U.S. Multi-Society Task Force (USMSTF) on Colorectal Cancer recommend upper endoscopy and high-quality colonoscopy with polypectomy beginning between the ages of 8 to 10 years.[572,573]
Management of small bowel hamartomas is important because patients with PJS have risks of bleeding, intussusception, and malignancy. In PJS, cumulative lifetime risk of small bowel cancer is approximately 13%. NCCN guidelines recommend computed tomography enterography (CTE), magnetic resonance enterography (MRE), or video capsule endoscopy (VCE) beginning between the ages of 8 to 10 years for small bowel surveillance in PJS.[572] These studies are repeated at intervals that are based on study findings up to age 18 years. Afterwards, screening is repeated every 2 to 3 years. Few studies have directly compared yields of these different small bowel cancer surveillance tools. One Australian study of 20 patients with PJS undergoing paired VCE and MRE found that more small bowel polyps (>1 cm) were detected by VCE than MRE.[574] However, balloon enteroscopy detected more small bowel polyps (>1 cm) than both VCE and MRE. NCCN guidelines also include recommendations for other PJS manifestations.
Juvenile polyposis syndrome
JPS is a genetically heterogeneous, rare, childhood- to early adult–onset, autosomal dominant disease that presents characteristically as hamartomatous polyposis throughout the GI tract, although colorectal polyps predominate.[575] JPS can present with diarrhea, GI tract hemorrhage, protein-losing enteropathy, and prolapsing polyps.[575–577] JPS is characterized by the presence of a specific type of hamartomatous polyp called a juvenile polyp, often when a family history of JPS is present. In spite of the histological nomenclature, juvenile polyp diagnosis is based on the polyp’s histological appearance, rather than the patient’s age when a polyp is found. Solitary juvenile polyps of the colon/rectum are seen sporadically in infants and young children and do not imply a JPS diagnosis.
JPS can be diagnosed clinically (based on fulfillment of specific clinical criteria) or genetically (based on the presence of germline pathogenic variants in SMAD4 or BMPR1A).
A clinical diagnosis of JPS is met by individuals fulfilling one or more of the following criteria:[578]
More than five juvenile polyps of the colon or rectum.
Juvenile polyps in other parts of the GI tract.
Any number of juvenile polyps and a positive family history of JPS.
Approximately 15% to 60% of JPS cases have germline pathogenic variants in the SMAD4 gene, and 25% to 40% of cases have germline pathogenic variants in the BMPR1A gene.[575,579,580]
Individuals with germline SMAD4 pathogenic variants may have a greater risk to develop severe gastric polyposis [581] and hereditary hemorrhagic telangiectasia (HHT) (see the features of HHT below).[575]
Individuals with JPS and germline pathogenic variants in SMAD4/BMPR1A have a 38% to 68% lifetime risk of developing CRC by age 60 years, with an average diagnosis occurring between the ages of 34 and 44 years.[437,582,583] Individuals who have clinical diagnoses of JPS but no identifiable germline SMAD4/BMPR1A pathogenic variants likely have decreased CRC risk. The lifetime risk of gastric cancer in patients with JPS and germline pathogenic variants in SMAD4/BMPR1A has been estimated to be as high as 21%.[123,437] However, the incidences of gastric cancer and gastric polyposis appear to be far lower in individuals with clinical diagnoses of JPS who do not have identifiable germline pathogenic variants in SMAD4/BMPR1A.[583]
Roughly 22% of JPS patients with germline SMAD4 pathogenic variants also have manifestations of HHT, such as arteriovenous malformations, mucocutaneous telangiectasias, digital clubbing, osteoarthropathy, hepatic arteriovenous malformations, and cerebellar cavernous hemangioma, suggesting that the two syndromes overlap.[584] One small case series showed that patients with JPS can infrequently have an adenomatous oligopolyposis phenotype as well.[575,585,586]
NCCN and the USMSTF on Colorectal Cancer recommend that patients with JPS undergo both high-quality colonoscopy with polypectomy and upper endoscopy with polypectomy beginning between ages 12 and 15 years.[123,573] Various clinical practice guidelines recommend that patients with JPS and germline SMAD4 pathogenic variants undergo screening for HHT manifestations.[123,437,575,587]
A severe form of JPS, in which polyposis develops in the first few years of life, is referred to as JPS of infancy. JPS of infancy is often caused by microdeletions of chromosome 10q22-23, a region that includes BMPR1A and PTEN. For more information about PTEN, see the PTEN hamartoma tumor syndromes (including Cowden syndrome) section. The phenotype often includes features such as macrocephaly and developmental delay, possibly as a result of loss of PTEN function.[588] Recurrent GI bleeding, diarrhea, exudative enteropathy, in addition to associated developmental delay, are associated with a very high rate of morbidity and mortality in these infants, thereby limiting the heritability of such cases.[588]
Oligopolyposis
Oligopolyposis (derived from the Greek prefix, oligo, meaning few) describes polyp counts that are greater than anticipated in average-risk patients but are fewer than 100 polyps. Here, oligopolyposis is used to describe situations in which an individual’s polyp count is large enough to suspect a hereditary polyposis syndrome (generally between 10–100 polyps), regardless of the presence or lack of a family history of colorectal polyps/CRC. Since oligopolyposis specifically refers to polyp count, multiple syndromes can present with an oligopolyposis phenotype. It is recommended that most individuals with oligopolyposis have germline genetic testing.[123] These individuals are managed with frequent endoscopic surveillance, based on their underlying hereditary syndrome or guided by their endoscopic presentation.
Multiple syndromes can present with oligopolyposis. These syndromes vary based on polyp histology and the pathogenic variant that is identified. FAP is the most well-described adenomatous polyposis syndrome that occasionally presents with fewer than 100 tubular adenomas. Since the APC gene was discovered in 1992 (pathogenic variants in APC cause FAP), other rare genes have also been implicated in oligopolyposis and cancer. These genes include NTHL1, POLE/POLD1, GREM1, MUTYH, and AXIN2. The hamartomatous polyposis syndromes and serrated polyposis syndrome (SPS) are nonadenomatous polyposis syndromes that can present with oligopolyposis. Individuals with adenomatous polyposis who do not have an identified germline pathogenic variant have colonic adenomatous polyposis of unknown etiology (CPUE).
In a cross-sectional study of 3,789 patients with 10 or more colorectal polyps, patients underwent multigene panel testing for the following genes: APC, BMPR1A, CDH1, CHEK2, EPCAM, MLH1, MSH2, MSH6, MUTYH, PMS2, PTEN, SMAD4, STK11, and TP53. In this study, pathogenic variants were found in 5% of participants, regardless of the participant’s age or polyp cohort.[589] GREM1, POLD1, and POLE were only evaluated in 2,353 patients because these genes were added to the multigene panel assay during the study period. The number of pathogenic variants in adenomatous polyposis genes decreased as participants increased in age in all polyp-count groups in the adenoma cohort. This, however, was not true for the nonpolyposis-related CRC genes. The prevalence of pathogenic variants in hamartomatous polyposis genes was high in the hamartoma cohort, regardless of polyp count (40% of participants had 10–19 polyps, 72.1% of participants had 20–99 polyps, and 50% of participants had 100 or more polyps). The study provides additional support for multigene panel testing in individuals with 10 or more colorectal polyps, given that more than 5% of patients had pathogenic variants in all age groups. For more information about genetic testing for polyposis, see the Genetic testing for FAP section.
NTHL1, POLE, POLD1, and GREM1 pathogenic variant testing is being incorporated into the multigene panel tests for CRC susceptibility (offered commercially with APC and MUTYH testing so a polyposis panel can be ordered up front for patients with oligopolyposis). There are minimal data on the optimal surveillance approach for individuals with germline pathogenic variants in NTHL1 (biallelic carriers only), POLE, or POLD1. It is presumed that CRC risk for these pathogenic variants is comparable to that seen in Lynch syndrome. Hence, some guidelines are endorsing early and frequent colonoscopic screening, similar to that which is conducted in Lynch syndrome patients.
Lastly, oligopolyposis with varying polyp histologies (e.g., adenomas, serrated, inflammatory, and hamartomatous polyps) has been reported in two small case series of individuals previously treated with chemotherapy and radiation therapy for a prior childhood malignancy.[590,591] This phenomenon, termed therapy-associated polyposis (TAP), may be an acquired, nonfamilial phenotype caused by prior antineoplastic therapy. TAP is on the differential diagnosis list when nonfamilial oligopolyposis is identified in individuals previously treated with chemotherapy and/or radiation therapy. Another recent study identified oligopolyposis fulfilling World Health Organization (WHO) criteria for serrated polyposis syndrome (SPS) in 6% of a cohort of 101 Hodgkin lymphoma survivors treated with prior chemotherapy and/or radiation therapy.[592] This finding suggests that Hodgkin lymphoma survivors may be a particularly important population in TAP.
Polymerase Proofreading–Associated Polyposis (POLE and POLD1 Genes)
Pathogenic variants in related DNA polymerase genes, POLE and POLD1, have been described in families with oligopolyposis, CRC, and endometrial cancer. This condition is called polymerase proofreading–associated polyposis (PPAP).[593,594] PPAP is an autosomal dominant hereditary cancer syndrome, in which the main replicative DNA polymerases, POLE and POLD1, are unable to proofread newly synthesized DNA strands. Several other malignancies (including endometrial, ovarian, small bowel, and brain cancers), have also been described in POLE and POLD1 carriers. PPAP-associated tumors often present with an ultramutator phenotype characterized by mutational loads exceeding 100 variants per megabase. PPAP-associated cancers can be highly responsive to immune checkpoint inhibitor therapy, irrespective of MSI/MMR status.[595,596] Identifying POLE and POLD1 carriers can be challenging since all known, putative, causal POLE and POLD1 variants are exonuclease-domain missense variants, which are notoriously difficult to classify. In addition, studies on the prevalence and penetrance of PPAP are limited, since this condition is rare, and risk estimates may be subject to ascertainment bias.
The prevalence of POLE and POLD1 pathogenic variants was determined in a prospective cohort of 2,309 unrelated patients with hereditary cancer. These patients all underwent genetic testing with a multigene hereditary cancer panel, in which PPAP was responsible for 0.1% to 0.4% of familial cancer cases (and reaching 0.3% to 0.7% when only CRC and polyposis were considered).[597] The tumors most commonly associated with PPAP included CRC, endometrial cancer, and ovarian cancer.
While PPAP is rare, the age-specific cumulative risks (penetrance) of CRC for POLE and POLD carriers is important to quantify and update, in order to better guide and optimize clinical management. In a retrospective study in which families with POLE or POLD1 pathogenic variants were identified via a PubMed search of relevant studies (prior to 2016) and genotypic data from 669 population-based CRC cases diagnosed in patients under 60 (from the Australasian Colorectal Cancer Family Registry), age-specific cumulative risks were estimated using modified segregation analyses.[598] Sixty-seven CRCs were identified in 364 first-degree relatives (FDRs) and second-degree relatives (SDRs) in 41 POLE families, and 6 CRCs were identified in 69 relatives from 9 POLD1 families. CRC risk to age 70 years for males and females, respectively, was 40% (95% CI, 26%–57%) and 32% (95% CI, 20%–47%) in POLE carriers and 63% (95% CI, 15%–99%) and 52% (95% CI, 11%–99%) in POLD1 carriers. CRC risk for POLE carriers was high enough to consider annual colonoscopy screening and the possible implementation of management guidelines similar to those used in Lynch syndrome. The authors concluded that clinical management recommendations for POLD1 carriers could be similar to those used in POLE carriers, but refinement of POLD1 CRC risk estimates (from larger cohorts) are needed to further refine recommendations.
Lifetime risk estimates of CRC in POLE carriers were higher than expected in a subsequent study of 354 individuals with early-onset/familial CRC (n = 218) and/or attenuated adenomatous polyposis (n = 136) at a single center between 2014 and 2017.[599] In 51 POLE carriers (from 10 families), risk estimates for CRC and extracolonic PPAP-associated cancers were calculated using nonparametric methods (based on a survival analysis approach) to account for unknown genotypes in relatives. Risks of CRC at ages 30 years, 50 years, and 70 years were 11.1% (95% CI, 4.2–17.5), 48.5% (96% CI, 33.2–60.3), and 74% (95% CI, 51.6–86.1), respectively. These risk estimates were similar in both men and women. These results provided additional support for frequent CRC surveillance in POLE carriers, similar to the surveillance used in highly penetrant Lynch syndrome genotypes. Extracolonic cancers like glioblastoma, small bowel cancer, endometrial cancer, and ovarian cancer were observed at low frequencies, limiting the ability to establish screening recommendations for these cancer types.
In POLD1 and POLE carriers, NCCN recommends high-quality colonoscopy starting at age 25 to 30 years. Colonoscopy screening can also begin 2 to 5 years before the earliest CRC in the family, if the CRC was diagnosed before age 25 years. Afterwards, colonoscopy is repeated every 1 to 2 years if polyps are identified or every 2 to 3 years if polyps are not identified.[123] There is insufficient evidence to provide recommendations on extracolonic cancer prevention for patients with variants in these genes.
NTHL1-Associated Polyposis
NTHL1-associated polyposis (or NTHL1 tumor syndrome) was first described in 2015. A study used whole-exome sequencing in 51 individuals (from 48 families) with multiple colonic adenomas.[600] This study found homozygous germline nonsense pathogenic variants in NTHL1 (a base-excision repair gene) in seven affected individuals from three unrelated families. These individuals had CRC and multiple adenomas (8–50 adenomas). None of the adenomas were hyperplastic or serrated. Three affected females also had endometrial cancer or endometrial complex hyperplasia. One individual developed duodenal adenomas, and another individual developed duodenal cancer. All pedigrees were consistent with autosomal recessive inheritance. Three cancers and five adenomas from different affected individuals did not show MSI. These neoplasms did show enrichment of cytosine to thymine transitions.
A subsequent study of 863 families with CRC and 1,600 families without CRC confirmed an association between biallelic NTHL1 pathogenic variants and inherited CRC risk.[601]
In a systematic review of 21 papers, the phenotypic and genotypic spectrum of NTHL1 tumor syndrome, including the occurrence of both benign and malignant tumors, were reported in both biallelic and monoallelic carriers.[602]
In 47 patients with biallelic pathogenic variants (from 32 families), 23 (49%) were diagnosed with CRC (mean age, 55 y; range, 31–73 y). In addition, 12 of the 22 female patients (55%) were diagnosed with breast cancer (mean age, 49 y; range, 36–63 y). In those who underwent colonoscopy, 93% had colonic adenomas ranging from 2 to 150 polyps, and three patients (6%) had duodenal adenomatosis. Overall, 37 carriers (79%) had at least one primary cancer (cancers occurred in different organs). All ten patients without cancer diagnoses had colonic adenomas. Six female patients (27%) also had gynecological cancers (four patients had endometrial cancer, one patient had ovarian cancer, and one patient had cervical cancer).
In 158 patients with monoallelic germline NTHL1 variants, 29 individuals (18%) were diagnosed with CRC (mean age, 56 y; range, 36–75 y). Twenty-six out of 68 (38%) monoallelic carriers who underwent colonoscopy had colon polyps or adenomas (1–70 polyps or adenomas). Six patients had more than ten adenomas or polyps. Breast cancer was diagnosed in 59 out of 120 (49%) female monoallelic carriers (mean age, 50 y; range, 24–79 y).
Limitations of this review included the following: (1) CRC and breast cancer may have been overrepresented due to ascertainment bias; (2) there may have been overlap with other germline pathogenic variants (one Lynch syndrome case and three BRCA2 cases were included in analyses of monoallelic NTHL1 carriers with breast cancer); (3) available data were inconsistent in studies involving monoallelic NTHL1 carriers.
Based on these results, the authors concluded that early endoscopic CRC surveillance can start before age 30 years in biallelic NTHL1 carriers, similar to the surveillance used in MUTYH carriers.[602] Given inconsistent reporting on duodenal polyposis and cancer in biallelic NTHL1 carriers, estimated duodenal neoplasia risk remains unclear, and upper GI tract surveillance could likely be postponed to the third or fourth decade of life. In addition, annual mammography or breast MRI can begin at age 40 years. However, this surveillance can begin at an earlier age if there is a young breast cancer diagnosis in the family. Gynecologic examination with TVUS can be considered every other year, starting at age 40 years.
Consistent with prior reports, monoallelic NTHL1 carriers do not have significantly increased cancer risk. It is not recommended, that these individuals undergo intensive cancer surveillance for GI, breast, or gynecologic cancers.
AXIN2-Related Polyposis
Pathogenic variants in AXIN2, a gene encoding a protein that forms part of the beta-catenin destruction complex, have been associated with oligodontia, ectodermal dysplasia, colorectal polyposis, and CRC in populations enriched with polyposis and CRC.[603,604] The beta-catenin destruction complex consists of several proteins, including AXIN2, and it downregulates beta-catenin, a transcriptional coactivator of Wnt-targeted gene expression.
The prevalence of AXIN2 pathogenic variants and their contribution to both colorectal polyposis and CRC remains unclear. An AXIN2 pathogenic variant was first implicated in a Finnish family (with multiple members) who had oligodontia (absence of >6 nonwisdom teeth in family members), CRC, and polyposis with autosomal dominant inheritance.[605] Subsequent reports had similar results, with other manifestations that included variable penetrance and ectodermal dysplasia (i.e., little hair and eyebrows).[606,607] Affected individuals with AXIN2 pathogenic variants from eight families in Australia/New Zealand were identified based on personal histories of unexplained colonic polyposis (presented with 10 to >100 colorectal polyps) and multiple CRC cases.[603] Similarly, 10 out of 11 French individuals with ten different AXIN2 pathogenic variants were ascertained based on histories of colorectal polyposis or CRC diagnosed at young ages. These individuals presented with adenomatous, serrated, and hyperplastic polyposis by a mean age of 55 years.[604] In three populations, extracolonic cancers included breast cancer, ampullary cancer, ovarian cancer, and melanoma. Multiple cases of tooth agenesis and ectodermal dysplasia (such as sparse hair and eyebrows) were frequently reported.[603,604]
In AXIN2 carriers, NCCN recommends the initiation of high-quality colonoscopy at age 25 to 30 years. Colonoscopy can be repeated every 2 to 3 years if polyps are not identified or every 1 to 2 years if polyps are found. Surgery can be considered in cases with unmanageable polyposis.[123] Given the lack of penetrance data for extracolonic cancers, no further recommendations are provided for AXIN2 carriers.
Hereditary Mixed Polyposis Syndrome (GREM1 Gene)
HMPS is a rare hereditary cancer syndrome characterized by the development of various types of colon polyps including serrated adenomas, atypical juvenile polyps, adenomas, and colonic adenocarcinoma. A small number of individuals/families with HMPS harbor a large, 40-kb, single-copy germline duplication upstream of gremlin 1 (GREM1)—the gene that is thought to cause the HMPS phenotype and increased CRC risk.[608]
Germline GREM1 pathogenic duplications have been observed primarily in individuals/families of Ashkenazi Jewish descent, with varying clinical presentations. Although polyposis appears to be a unifying feature in most families with this duplication, there is a high degree of variability with respect to polyp number, histology, and age of onset. In addition, extracolonic malignancies have been described in several GREM1 pathogenic variant carriers, although the small number of affected individuals limits the ability to definitively demonstrate a causal link to the GREM1 pathogenic variant.
Evidence-based strategies for managing individuals with germline GREM1 pathogenic duplications do not yet exist. However, NCCN guidelines recommend that GREM1 carriers initiate colonoscopic surveillance between ages 25 and 30 years.[123] Colonoscopy is repeated every 2 to 3 years if polyps are not identified or every 1 to 2 years if polyps are identified.
CHEK2
Several studies have suggested that germline CHEK2 pathogenic variants may confer increased risks of colorectal cancer.[609–611] CHEK2 pathogenic variants have been seen in up to 2% of individuals with CRC.[612] However, data have suggested that CHEK2 variants are associated with, at most, a modestly increased risk of CRC (i.e., low penetrance).[613] Two large retrospective studies of CHEK2 cases ascertained from two genetic testing laboratories did not find an increased risk of CRC in CHEK2 carriers.[614,615] In fact, one study found that individuals with germline CHEK2 pathogenic variants had lower risks of CRC when compared with those who had negative results on germline genetic testing panels.[614]
NCCN guidelines recommend that individuals with germline CHEK2 pathogenic variants (and no other CRC risk factors) participate in general population screening for CRC.[123] When a CHEK2 carrier has additional CRC risk factors (e.g., personal/family history of CRC, personal history of colorectal adenomas), the timing and frequency of surveillance colonoscopies is typically determined by the individual’s clinical history.
For more information, see the CHEK2 section in Genetics of Breast and Gynecologic Cancers.
Serrated Polyposis Syndrome
The term serrated polyposis syndrome (SPS) has been used to characterize individuals who have mostly sessile serrated polyps/lesions (SSPs/SSLs) in the large intestine. Although the term syndrome is used in SPS, most cases appear to be nonfamilial, and the underlying etiology of these polyps is typically unidentifiable.
Germline evaluation of individuals with serrated polyposis is typically unrevealing.[616–620] Rarely, germline RNF43 pathogenic variants are found in families with serrated polyposis.[621–623] Occasional MUTYH biallelic pathogenic variants and Lynch syndrome pathogenic variants have been found in patients with serrated polyps or features of serrated polyposis.
The WHO states that an individual meets SPS diagnostic criteria if either of the following criteria are fulfilled:[624]
A personal history of at least five histologically diagnosed serrated lesions (this includes hyperplastic polyps, SSPs, or SSLs) that are all 5 mm or larger, occurring proximal to the rectum. At least two of these polyps/lesions must be 10 mm or larger.
A personal history of 20 or more serrated lesions (of any size) in the colon/rectum, with 5 or more lesions occurring proximal to the rectum.
Studies have shown that colorectal adenocarcinoma incidence in patients who met formally defined diagnostic criteria for SPS range from 19.9% to greater than 50%.[625–633] A small fraction (<5%) of individuals who fulfill SPS diagnostic criteria harbor germline RNF43 pathogenic variants. Clinical germline genetic testing can be offered to those who meet SPS diagnostic criteria, especially if there is a concomitant family history of CRC and/or SSPs/SSLs.[621–623] While only a small fraction of SPS cases are attributable to monogenic inherited risk, data have suggested that FDRs of individuals with SPS are at increased risk of CRC. Lifestyle factors like smoking, alcohol use, and increased body mass index were associated with SPS in case-control data.[634]
In some individuals with therapy-associated polyposis (TAP), an acquired, mixed-histology form of colorectal and GI tract oligopolyposis, polyps can be seen in childhood/young-adult cancer survivors who were treated with chemotherapy and/or radiotherapy. Some of these individuals will have clinical histories that fulfill SPS diagnostic criteria.[635,636] For more information, see the Oligopolyposis section.
Evidence-based management guidelines for individuals with SPS do not yet exist. NCCN guidelines recommend undergoing high-quality colonoscopy to clear all SSPs/SSLs that are 5 mm or larger (after the SPS phenotype is clinically identified in an individual).[123] Then, colonoscopy is repeated every 1 to 3 years, depending on the number and size of polyps.
MBD4
MBD4-associated neoplasia syndrome is associated with an increased risk of GI polyposis (comparable to AFAP). For more information, see MBD4-Associated Neoplasia Syndrome.
Advances in Endoscopic Imaging in Hereditary CRC
Performance of endoscopic therapies for adenomas in FAP and Lynch syndrome, and decision-making regarding surgical referral and planning, require accurate estimates of the presence of adenomas. In both AFAP and Lynch syndrome the presence of very subtle adenomas poses special challenges—microadenomas in the case of AFAP and flat, though sometimes large, adenomas in Lynch syndrome.
Chromoendoscopy
The need for sensitive means to endoscopically detect subtle polyps has increased with the recognition of flat adenomas and sessile serrated polyps in otherwise average-risk subjects, very attenuated adenoma phenotypes in AFAP, and subtle flat adenomas in Lynch syndrome. Modern high-resolution endoscopes improve adenoma detection yield, but the use of various vital dyes, especially indigo carmine dye-spray, has further improved detection. Several studies have shown that the improved mucosal contrast achieved with the use of indigo carmine can improve the adenoma detection rate. Whether family history is significant or not, careful clinical evaluation consisting of dye-spray colonoscopy (indigo carmine or methylene blue),[474,637–642] with or without magnification, or possibly newer imaging techniques such as narrow-band imaging,[643] may reveal the characteristic right-sided clustering of more numerous microadenomas. Upper GI endoscopy may be informative if duodenal adenomas or fundic gland polyps with surface dysplasia are found. Such findings will increase the likelihood of variant detection if APC or MUTYH testing is pursued.
In various large series of average-risk populations, subtle flat lesions were detected in about 5% to 10% of cases, including adenomas with high-grade dysplasia and invasive adenocarcinoma.[644] Some of these studies involved tandem procedures—white-light exam followed by randomization to “intensive” (> 20-minute pull-back from cecum) inspection versus chromoendoscopy—with significantly more adenomas detected in the chromoendoscopy group.[645] However, in several randomized trials, no significant difference in yield was seen.[646,647]
In a randomized trial of subjects with Lynch syndrome,[648] standard colonoscopy, with polypectomy as indicated, was followed by either indigo carmine chromoendoscopy or repeat “intensive” white-light colonoscopy (a design very nearly identical to the average-risk screening group noted above). In this series, no significant difference in adenoma yield between the chromoendoscopy and intensive white-light groups was detected. However, these patients were younger and, in many cases, had undergone several previous exams that might have resulted in polyp clearing.
In a German study,[649] one series of Lynch syndrome patients underwent white-light exam followed by chromoendoscopy, while a second series underwent colonoscopy with narrow-band imaging followed by chromoendoscopy. Significant differences in flat polyp detection favored chromoendoscopy in both series, although some of the detected lesions were hyperplastic. In a French series of Lynch syndrome subjects that also employed white-light exam followed by chromoendoscopy, significantly more adenomas were detected with chromoendoscopy.[475]
Fewer evaluations of chromoendoscopy have been performed in AFAP than in Lynch syndrome. One study examined four patients with presumed AFAP and fewer than 20 adenomas upon white-light examination.[650] All had more than 1,000 diminutive adenomas found on chromoendoscopy, in agreement with pathology evaluation after colectomy.
A similar role for chromoendoscopy has been suggested to evaluate the duodenum in FAP. One study from Holland that used indigo carmine dye-spray to detect duodenal adenomas showed an increase in the number and size of adenomas, including some large ones. Overall Spigelman score was not significantly affected.[651]
Small bowel imaging
Patients with PJS and JPS are at greater risk of disease-related complications in the small bowel (e.g., bleeding, obstruction, intussusception, or cancer). FAP patients, although at great risk of duodenal neoplasia, have a relatively low risk of jejunoileal involvement. The RR of small bowel malignancy is very high in Lynch syndrome, but absolute risk is less than 10%. Although the risks of small bowel neoplasia are high enough to warrant consideration of surveillance in each disease, the technical challenges of doing so have been daunting. Because of the technical challenges and relatively low prevalences, there is virtually no evidence base for small-bowel screening in Lynch syndrome.
Historically, the relative endoscopic inaccessibility of the mid and distal small bowel required radiographic measures for its evaluation, including the barium small bowel series or a variant called tube enteroclysis, in which a nasogastroduodenal tube is placed so that all of the contrast goes into the small intestine quickly and undiluted by gastric juice for more precise imaging. None of these measures were sensitive for small lesions. Previously, therapeutic removal of lesions required laparotomy. However, multiple novel endoscopic approaches have been developed to overcome the technical limitations of small bowel endoscopy, which has enabled jejunal and ileal access for purposes of polypectomy.
For patients with PJS, double-balloon endoscopy or other forms of deep enteroscopy (single-balloon overtube or spiral overtube) are the preferred methods for evaluation of the small bowel.[652] This may involve either peroral enteroscopy or retrograde enteroscopy to achieve more complete evaluation of the small bowel. Because these procedures are time-consuming and involve risks of complication, deep enteroscopy is usually preceded by more imaging, including barium exams, capsule endoscopy, CT or magnetic resonance enterography.[73]
In FAP, data from capsule endoscopy [73] show a 50% to 100% prevalence of jejunal and/or ileal polyps in patients with Spigelman stage III or stage IV duodenal involvement but virtually no such polyps in Spigelman stage I or stage II disease. Polyps smaller than 10 mm and were not biopsied or removed. Consequently, their clinical significance remains uncertain but is likely limited, given the infrequency of jejunoileal cancer reports in FAP.
Capsule endoscopy in the small series of PJS patients described above [73] showed the presence of a similar frequency (50%–100%) of polyps, but the prevalent polyps were much larger than in FAP, were more likely to become symptomatic, and warranted endoscopic or surgical excision. Capsule studies were suggested as an appropriate replacement for radiographic studies because of the sensitivity of capsule endoscopy.
References
Bussey HJ: Familial Polyposis Coli: Family Studies, Histopathology, Differential Diagnosis, and Results of Treatment. The Johns Hopkins University Press, 1975.
Burt RW, Leppert MF, Slattery ML, et al.: Genetic testing and phenotype in a large kindred with attenuated familial adenomatous polyposis. Gastroenterology 127 (2): 444-51, 2004. [PUBMED Abstract]
Choi YH, Cotterchio M, McKeown-Eyssen G, et al.: Penetrance of colorectal cancer among MLH1/MSH2 carriers participating in the colorectal cancer familial registry in Ontario. Hered Cancer Clin Pract 7 (1): 14, 2009. [PUBMED Abstract]
Bonadona V, Bonaïti B, Olschwang S, et al.: Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA 305 (22): 2304-10, 2011. [PUBMED Abstract]
Møller P, Seppälä T, Bernstein I, et al.: Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective Lynch syndrome database. Gut 66 (3): 464-472, 2017. [PUBMED Abstract]
Baglietto L, Lindor NM, Dowty JG, et al.: Risks of Lynch syndrome cancers for MSH6 mutation carriers. J Natl Cancer Inst 102 (3): 193-201, 2010. [PUBMED Abstract]
Aretz S, Uhlhaas S, Goergens H, et al.: MUTYH-associated polyposis: 70 of 71 patients with biallelic mutations present with an attenuated or atypical phenotype. Int J Cancer 119 (4): 807-14, 2006. [PUBMED Abstract]
Hearle N, Schumacher V, Menko FH, et al.: Frequency and spectrum of cancers in the Peutz-Jeghers syndrome. Clin Cancer Res 12 (10): 3209-15, 2006. [PUBMED Abstract]
Coburn MC, Pricolo VE, DeLuca FG, et al.: Malignant potential in intestinal juvenile polyposis syndromes. Ann Surg Oncol 2 (5): 386-91, 1995. [PUBMED Abstract]
Inra JA, Steyerberg EW, Grover S, et al.: Racial variation in frequency and phenotypes of APC and MUTYH mutations in 6,169 individuals undergoing genetic testing. Genet Med 17 (10): 815-21, 2015. [PUBMED Abstract]
Giardiello FM, Offerhaus JG: Phenotype and cancer risk of various polyposis syndromes. Eur J Cancer 31A (7-8): 1085-7, 1995 Jul-Aug. [PUBMED Abstract]
Jagelman DG, DeCosse JJ, Bussey HJ: Upper gastrointestinal cancer in familial adenomatous polyposis. Lancet 1 (8595): 1149-51, 1988. [PUBMED Abstract]
Sturt NJ, Gallagher MC, Bassett P, et al.: Evidence for genetic predisposition to desmoid tumours in familial adenomatous polyposis independent of the germline APC mutation. Gut 53 (12): 1832-6, 2004. [PUBMED Abstract]
Lynch HT, Fitzgibbons R: Surgery, desmoid tumors, and familial adenomatous polyposis: case report and literature review. Am J Gastroenterol 91 (12): 2598-601, 1996. [PUBMED Abstract]
Bülow S, Björk J, Christensen IJ, et al.: Duodenal adenomatosis in familial adenomatous polyposis. Gut 53 (3): 381-6, 2004. [PUBMED Abstract]
Bisgaard ML, Bülow S: Familial adenomatous polyposis (FAP): genotype correlation to FAP phenotype with osteomas and sebaceous cysts. Am J Med Genet A 140 (3): 200-4, 2006. [PUBMED Abstract]
Petersen GM, Slack J, Nakamura Y: Screening guidelines and premorbid diagnosis of familial adenomatous polyposis using linkage. Gastroenterology 100 (6): 1658-64, 1991. [PUBMED Abstract]
Berk T, Cohen Z, Bapat B, et al.: Negative genetic test result in familial adenomatous polyposis: clinical screening implications. Dis Colon Rectum 42 (3): 307-10; discussion 310-2, 1999. [PUBMED Abstract]
Jagelman DG: Clinical management of familial adenomatous polyposis. Cancer Surv 8 (1): 159-67, 1989. [PUBMED Abstract]
Neale K, Ritchie S, Thomson JP: Screening of offspring of patients with familial adenomatous polyposis: the St. Mark’s Hospital polyposis register experience. In: Herrera L, ed.: Familial Adenomatous Polyposis. Alan R. Liss Inc, 1990, pp 61-66.
Nusliha A, Dalpatadu U, Amarasinghe B, et al.: Congenital hypertrophy of retinal pigment epithelium (CHRPE) in patients with familial adenomatous polyposis (FAP); a polyposis registry experience. BMC Res Notes 7: 734, 2014. [PUBMED Abstract]
Chen CS, Phillips KD, Grist S, et al.: Congenital hypertrophy of the retinal pigment epithelium (CHRPE) in familial colorectal cancer. Fam Cancer 5 (4): 397-404, 2006. [PUBMED Abstract]
Coleman P, Barnard NA: Congenital hypertrophy of the retinal pigment epithelium: prevalence and ocular features in the optometric population. Ophthalmic Physiol Opt 27 (6): 547-55, 2007. [PUBMED Abstract]
Traboulsi EI, Apostolides J, Giardiello FM, et al.: Pigmented ocular fundus lesions and APC mutations in familial adenomatous polyposis. Ophthalmic Genet 17 (4): 167-74, 1996. [PUBMED Abstract]
Anthony T, Rodriguez-Bigas MA, Weber TK, et al.: Desmoid tumors. J Am Coll Surg 182 (4): 369-77, 1996. [PUBMED Abstract]
Eccles DM, van der Luijt R, Breukel C, et al.: Hereditary desmoid disease due to a frameshift mutation at codon 1924 of the APC gene. Am J Hum Genet 59 (6): 1193-201, 1996.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.

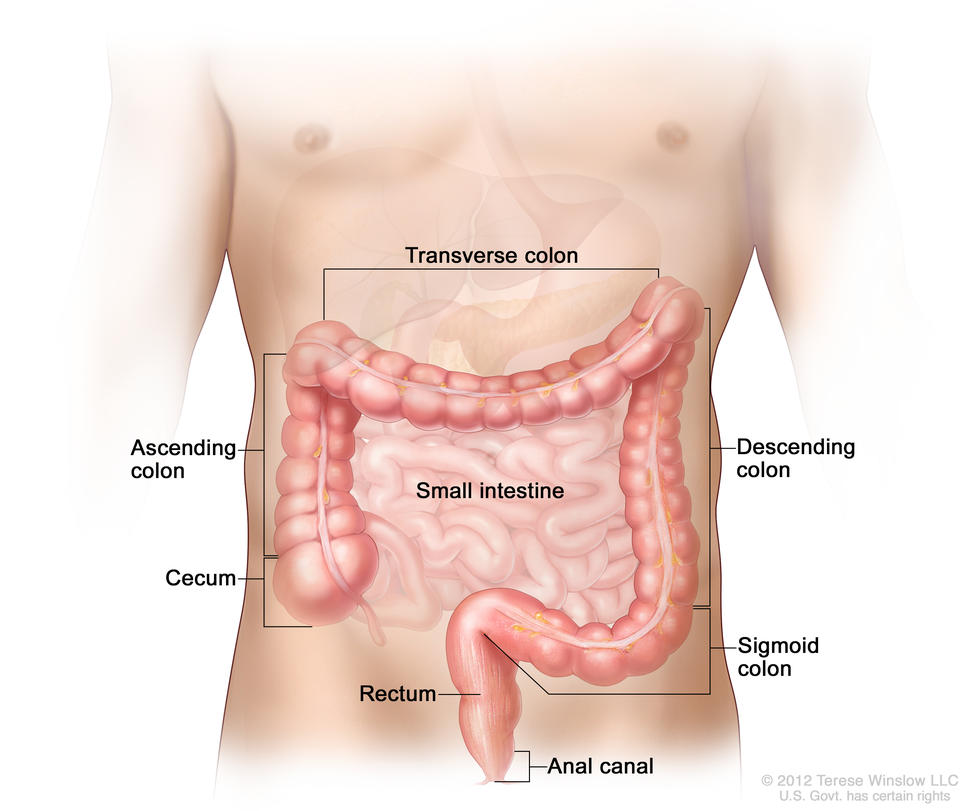

 system anatomy; drawing shows the esophagus, liver, stomach, colon, small intestine, rectum, and anus.")
 inside the colon. Inset shows photo of a pedunculated polyp.")
 kit; shows card, applicator, and return envelope.")
; drawing shows a FIT kit, which includes the package insert, the collection paper, and a collection tube with a small brush inside of it. Also shown are the biohazard bag, the return envelope, and a paper with information about colorectal cancer and colorectal cancer screening.")












; Lynch syndrome (hereditary nonpolyposis colorectal cancer) (2%–3%); familial adenomatous polyposis (<1%); and hamartomatous polyposis syndrome (<0.1%).")



 show the presence of MSH2 and MSH6 (the dark stain is visible) and absence of MLH1 and PMS2 (the dark stain is not visible).")
