After thymoma or thymic carcinoma has been diagnosed, tests are done to find out if cancer cells have spread to nearby areas or to other parts of the body.
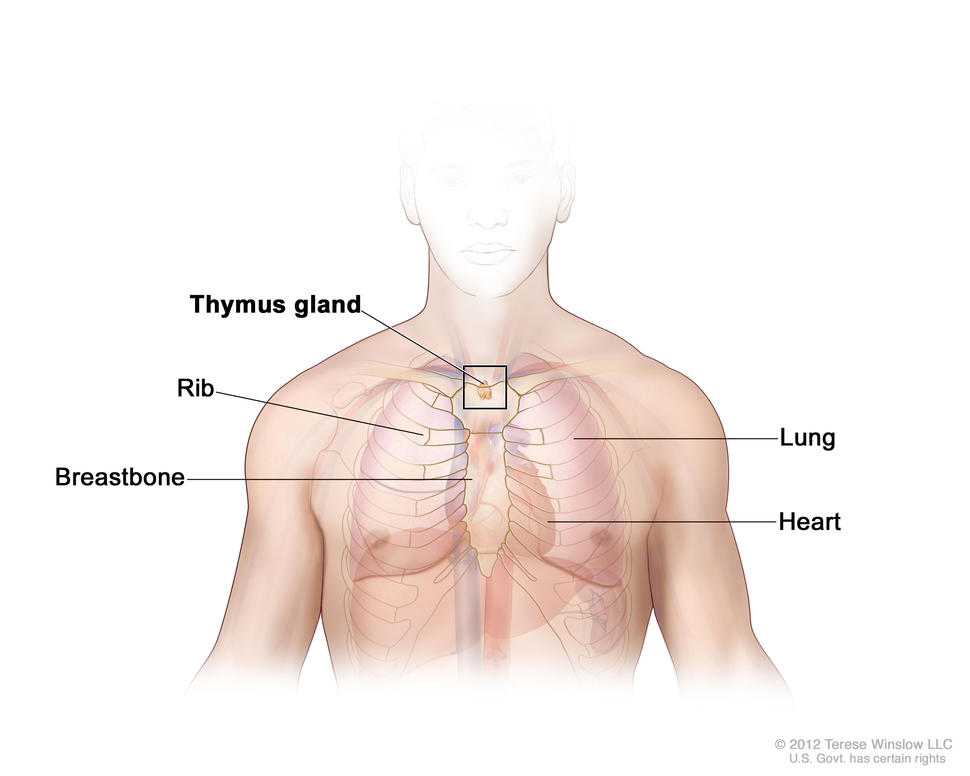
The process used to find out if thymoma or thymic carcinoma has spread from the thymus to nearby areas or other parts of the body is called staging. Thymoma and thymic carcinoma may spread to the lungs, chest wall, major vessels, esophagus, or the lining around the lungs and heart. The results of tests and procedures done to diagnose thymoma or thymic carcinoma are used to help make decisions about treatment.
Thymic carcinomas have usually spread to other parts of the body when diagnosed.
The staging system used for thymomas is sometimes used for thymic carcinomas. The following stages are used for thymoma:
Stage I
In stage I, cancer is found only within the thymus. All cancer cells are inside the capsule (sac) that surrounds the thymus.
Stage II
In stage II, cancer has spread through the capsule and into the fat around the thymus or into the lining of the chest cavity.
Stage III
In stage III, cancer has spread to nearby organs in the chest, including the lung, the sac around the heart, or large blood vessels that carry blood to the heart.
Stage IV
Stage IV is divided into stage IVA and stage IVB, depending on where the cancer has spread.
- In stage IVA, cancer has spread widely around the lungs or heart.
- In stage IVB, cancer has spread to the blood or lymph system.
Recurrent thymoma and thymic carcinoma
Recurrent thymoma and thymic carcinoma are cancers that have recurred (come back) after treatment. The cancer may come back in the thymus or in other parts of the body. Thymic carcinoma is more likely to recur than thymoma.
- Thymomas may recur a long time after treatment is completed. There is also an increased risk of having another type of cancer after having a thymoma. For these reasons, lifelong follow-up is needed.
- Thymic carcinomas often recur.
How cancer spreads in the body
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if thymic carcinoma spreads to the bone, the cancer cells in the bone are actually thymic carcinoma cells. The disease is metastatic thymic carcinoma, not bone cancer.

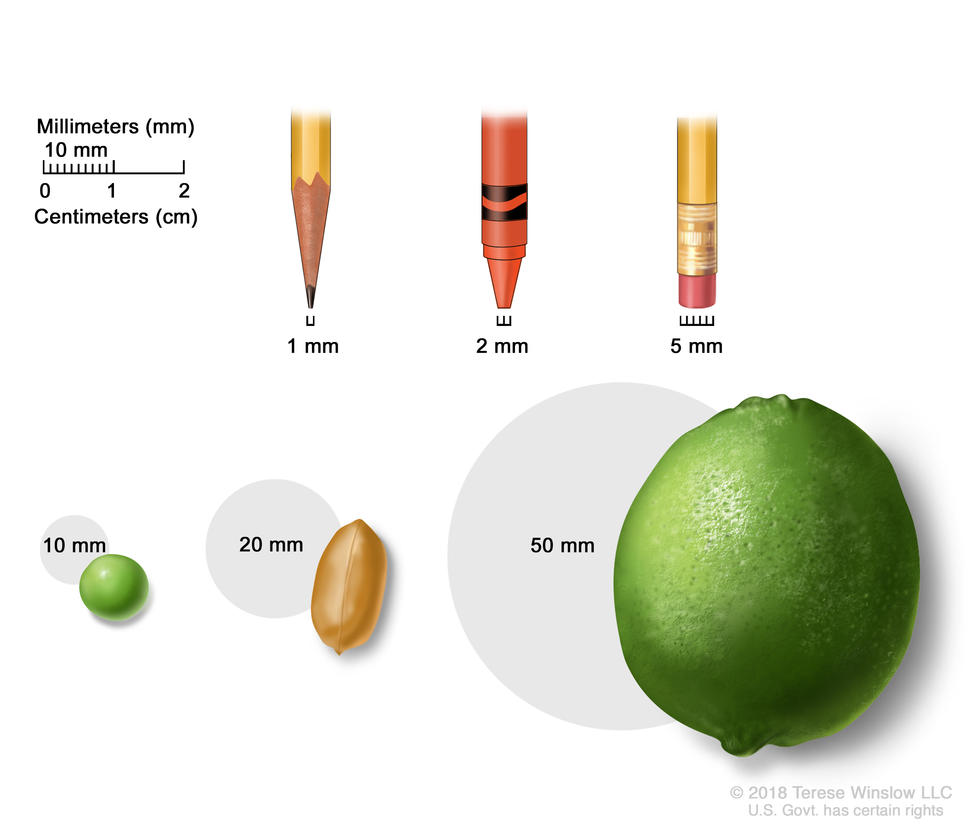

 compared to the size of a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm). Also shown is a 10-cm ruler and a 4-inch ruler.")
 using everyday objects. A sharp pencil point shows 1 mm, a new crayon point shows 2 mm, and a new pencil-top eraser shows 5 mm.")