Drinking plenty of fluids and being physically active can help prevent and treat constipation. Check with your doctor before taking medicine for constipation.
Credit: iStock
What is constipation?
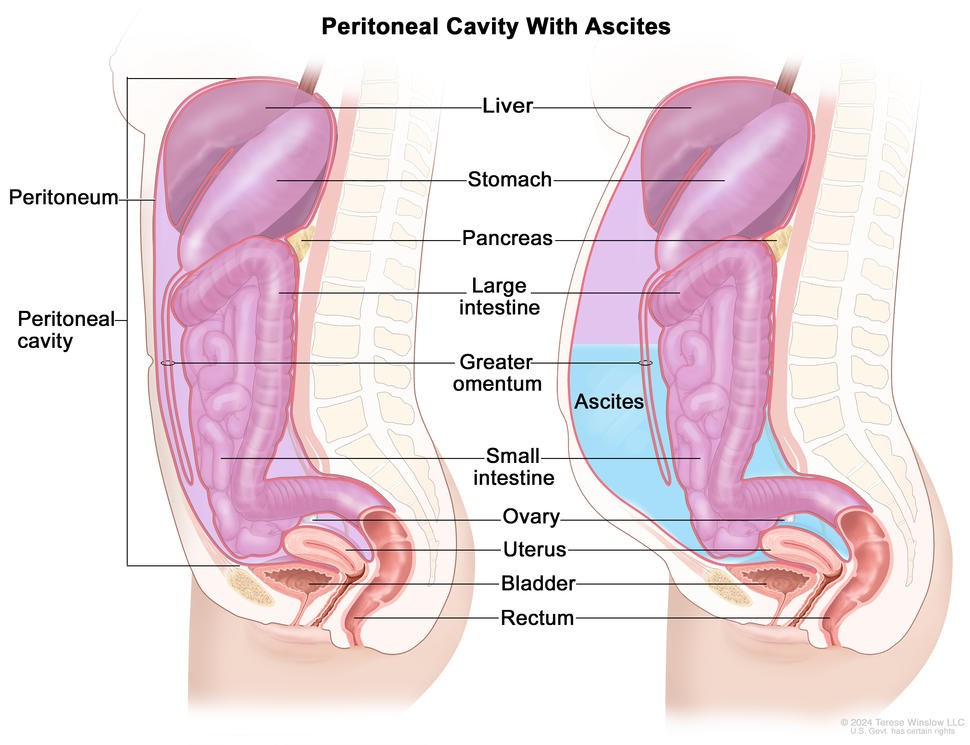
Constipation is the slow movement of stool (poop) through the large intestine. The longer it takes for the stool to move through the large intestine, the more it loses fluid and the drier and harder it becomes.
If you are constipated, you may be unable to have a bowel movement, need to push harder to have a bowel movement, or have fewer than your usual number of bowel movements. Talk to your doctor if you have constipation. Your doctor can recommend medicines and other ways for treating constipation caused by cancer and cancer treatment.
Constipation may last for a short time, or it may be chronic and last for a long time. Long-term (chronic) constipation can lead to fecal impaction or bowel obstruction, two potentially life-threatening conditions that require immediate medical care. Learn more at What is fecal impaction? and Bowel Obstruction.
What are signs and symptoms of constipation?
Learn about other digestive system problems in people with cancer
Constipation in people with cancer may be caused by:
Certain types of cancer. Constipation may be a sign or symptom of cancers that push on organs in the abdomen, block the movement of stool through the bowel, or affect the nerves in your spine connected to your bowel. Some cancers that may cause constipation include colon cancer, rectal cancer, ovarian cancer, and brain tumors.
Cancer treatments such as chemotherapy. Constipation is a common side effect of some types of chemotherapy.
Medicines. Many medicines, including opioid pain medications, antianxiety drugs, antinausea drugs (antiemetics), and diuretics, can cause constipation.
Lifestyle and dietary changes. When you are getting cancer treatment, you may have less energy for exercise and your appetite and diet may change. Being less active and eating different foods than normal can cause constipation.
How is constipation diagnosed in people with cancer?
Finding the cause of constipation is important so you can get relief and avoid serious problems such as fecal impaction. Your doctor will do a physical exam, which will include looking at and feeling the abdomen for areas of swelling or firmness and listening to the sounds of your bowels. Your doctor may also ask questions such as:
How often do you have a bowel movement? How often did you have a bowel movement before you had cancer? Has there been a recent change in your bowel habits?
When was your last bowel movement? What was it like (how much, hard or soft, what color, was there blood)? Did you have to push more than usual?
Do you have a fever, cramps, a feeling of fullness near the rectum, pain, or bloating?
Your doctor may be able to diagnose constipation and suggest treatment based on a physical exam and these questions. Sometimes, your doctor may need to do other tests to better understand what is causing constipation:
Digital rectal examination (DRE): A physical exam in which the doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel for impacted stool or unusual changes.
X-rays: An x-ray is a type of radiation that, in low doses, can be used to make a picture of areas inside the body. An x-ray of the abdomen can show a tumor or fecal impaction that may be causing constipation.
Ways to prevent and treat constipation
If your doctor thinks your cancer or cancer treatments will cause constipation, they will give you tips and prescribe medicine to prevent it. If you become constipated, your doctor will recommend many of these same tips and medicines to help you get relief. Talk with your health care team about what treatment is right for you.
Drink plenty of liquids. Drinking 8 cups of water or clear liquids per day can help you stay hydrated, which helps with constipation. Beverages such as coffee and prune juice can have a laxative effect, and hot drinks can also help stool move through the bowel.
Try to be active every day. Ask your health care team about exercises you can do. Walking, riding a bike, and practicing yoga may be options for you. You can also do light exercise in a bed or chair.
Eat at the same time each day. This routine can help you get back to your normal number of bowel movements.
Keep a record of your bowel movements. Showing this record to your health care team and talking to them about what is normal for you can help your doctor treat the constipation you are experiencing.
Talk with your doctor about dietary fiber. High-fiber foods and fiber supplements can make constipation worse for some people. Ask your doctor if adding fiber to your diet will help relieve constipation for you.
What can people with cancer take for constipation?
Your doctor may prescribe medicines called laxatives that help prevent or relieve constipation. Use only medicines and treatments for constipation that your doctor recommends. Many different types of laxatives are available, and your doctor may recommend others not listed here:
Osmotics pull water into the bowel from other parts of the body, making it easier to have a bowel movement. Polyethylene glycol (MiraLAX), magnesium hydroxide (Milk of Magnesia), lactulose (Enulose), and sorbitol are examples of osmotic laxatives.
Stool softeners, or emollients, soften poop by increasing the amount of water and fat that the poop absorbs. Docusate (Colace) is an example of a stool softener.
Stimulant laxatives cause the intestines to contract so stool moves through the bowel. Bisacodyl (Correctol), senna (Senokot), and castor oil are examples of stimulant laxatives.
Do not use suppositories (capsules you insert into your anus) or enemas (liquid medicine that you inject into your anus) unless your doctor recommends them. In some people with cancer, these treatments may lead to bleeding, infection, or other harmful side effects.
How a caregiver can help
Encourage the person you are caring for to drink plenty of water or other fluids. Make sure they also have access to hot beverages and prune juice, which may help relieve constipation.
Help the person you are caring for stay physically active. Physical activity includes moving from a bed to a chair, walking short distances, or riding an exercise bike. Talk to their care team to find out what exercise is right for them.
Monitor the person’s bowel movements and help them keep a record of their bowel movements. They should have a bowel movement every day or every other day that is not hard and does not require straining.
Notify the care team if the person has had fewer than three bowel movements in one week or is experiencing severe abdominal pain, vomiting, and other signs of fecal impaction.
Long-term constipation can lead to fecal impaction, a potentially life-threatening condition in which hardened stool blocks the flow of waste through the colon or rectum. Fecal impaction requires immediate medical attention.
Fecal impaction is a serious condition in which hardened stool blocks the colon or rectum. Unlike constipation, fecal impaction can be life-threatening and requires immediate medical attention.
What causes fecal impaction?
Causes of fecal impaction include:
opioid pain medicines
little or no physical activity over a long period
dietary changes
constipation that is not treated
inability to push stool out because of weakness or muscle problems
What are signs and symptoms of fecal impaction?
Signs and symptoms of fecal impaction include:
chronic constipation
a feeling of pressure in the rectum or incomplete emptying of stool
lower back pain or pain in the abdomen
urinating more or less often than usual or being unable to urinate
The main treatment for fecal impaction is to moisten and soften the stool using an enema. The softened stool can then pass out of the body. Because enemas can be dangerous for people with cancer, they should be used only when prescribed and given by a doctor.
You may need to have stool manually removed from the rectum after it is softened. Laxatives are generally not used to treat fecal impaction because they may cause cramping and damage to your intestines.
Talking with your doctor about constipation
Tell your doctor or nurse if you are having constipation so you can get treatment as soon as possible. Treating constipation early can help prevent serious problems like fecal impaction and bowel obstruction. Your doctor can help you find ways to treat and manage this side effect of cancer and cancer treatment.
Questions to ask your provider about constipation:
What symptoms or problems should I call you about?
Should I take medicine for constipation? If so, what medicine should I take? What medicine should I avoid?
How much liquid should I drink each day?
What foods can help with constipation? What foods should I avoid?
Side effects like constipation or fecal impaction can be hard to deal with, both physically and emotionally. It’s important to ask for support from your health care team. They can help you prepare for and make it through difficult times. Learn more about ways to cope with cancer, including ways to adjust to daily life during cancer treatment.
For family members and friends who are caring for someone with cancer, you may find these suggestions for caregivers to be helpful.
Bowel obstructions require immediate medical attention. After your doctor finds the cause of the obstruction, they can help you choose a treatment option.
Credit: iStock
What is bowel obstruction?
A bowel (intestinal) obstruction is a serious condition that occurs when the small or large intestine becomes blocked. The blockage stops food and stool (poop) from moving through the intestines. The intestine may be partly or completely blocked and can sometimes be blocked in two places. Bowel obstructions can be life-threatening and require immediate medical attention.
A bowel obstruction may occur soon after cancer treatment ends or many months or years later. Bowel obstruction is most common in people with advanced cancer.
What causes bowel obstruction in people with cancer?
Bowel obstruction in people with cancer may be caused by:
Cancer treatment. Some types of cancer treatment can cause bowel obstruction:
Surgery on the abdomen or pelvis may lead to scar tissue, also called adhesions, that form after surgery. Adhesions can cause the intestines to bind together, creating a blockage.
Radiation therapy directed at the abdomen can damage the intestines, leading to scar tissue, inflammation, radiation enteritis, and irritation that can block the bowel.
A malignant bowel obstruction happens when a tumor forms in the intestines and blocks the flow of waste. The tumor may be from colon or rectal cancer or from cancer that has spread to the intestines from another part of the body.
Cancer itself. Cancers that form in the abdomen, such as colon, ovarian, pancreatic, or stomach cancer, are more likely than other cancer types to cause a bowel obstruction. A bowel obstruction caused by cancer itself is called a malignant bowel obstruction. Cancer can cause a bowel obstruction in different ways:
A tumor that forms in or presses on the bowels can cause a bowel obstruction. A tumor can also cause a bowel obstruction if it grows in an area that affects the nerves that control the movement of food through the intestines.
Advanced cancer can cause a bowel obstruction when cancer spreads to the bowels from another place in the body. Advanced cancer is the most common cause of malignant bowel obstruction.
When an obstruction starts, the intestines may be partly blocked, causing a few mild symptoms. As the obstruction gets worse, your symptoms may happen more often and become more severe. You may have frequent vomiting, extreme bloating, and intense abdominal pain. These are signs of a complete obstruction, in which stool and gas are mostly or totally blocked from leaving the body.
How is bowel obstruction diagnosed?
Finding the cause of a bowel obstruction and the place where the intestine is blocked is important so your doctor can recommend treatment. Your doctor will ask about your symptoms and do a physical exam. They may also use the following tests and procedures to diagnose a bowel obstruction and suggest treatment options:
CT scan (CAT scan) uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This scan helps doctors find the cause and exact location of the obstruction. It is also called computed tomography, computerized tomography, or computerized axial tomography.
Abdominal x-ray is an x-ray of the organs inside the abdomen. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. It can also show the location of the obstruction, but it is not as sensitive as a CT scan.
Blood tests, such as a complete blood count and electrolyte panel, show if you are dehydrated or have an electrolyte imbalance or infection. These problems may be caused by a bowel obstruction.
Urinalysis checks the color of urine and its contents, such as sugar, protein, red blood cells, and white blood cells. A urinalysis shows your fluid levels, signs of infection, and other problems that may be caused by a bowel obstruction.
Treating a bowel obstruction
If you have a bowel obstruction, you will need to be treated in a hospital. Treatment for a bowel obstruction depends on what caused the blockage and whether the intestines are partly or completely blocked. If you have a complete blockage, you will probably need surgery. Partial obstructions may clear up with nonsurgical treatments.
Treatment for a bowel obstruction may include:
Bowel rest. This is when you avoid eating and drinking to keep the obstruction from getting worse. Bowel rest or a liquid diet that is easy on your intestines can help your body clear the blockage. You may also receive fluid replacement therapy (IV fluids) to help the fluids and electrolytes in your body return to normal.
Nasogastric tube. This tube is inserted through the nose and esophagus into the stomach to relieve pressure caused by a bowel obstruction by removing fluid and gas from the digestive system. A nasogastric tube helps control nausea, vomiting, and pain related to the obstruction and may help your body clear the blockage.
Stent. This is a tube placed in the intestine to open the blocked area. Stents relieve bowel obstruction symptoms by temporarily opening the bowels to let food, waste, and gas pass through the body. Stents are most often used to treat bowel obstructions caused by cancer, but they may also be used for obstructions with other causes.
Surgery. If a bowel obstruction does not go away with other treatments or if you have a complete blockage, you may need surgery to remove the obstruction. For an obstruction caused by cancer, surgery will include removing the tumor that is causing the blockage. Your doctor will talk with you about your overall health and potential risks and benefits of surgery to help you decide if surgery is right for you.
Gastrostomy tube. A tube that helps release fluid and air from the stomach to relieve symptoms caused by the obstruction. A tube is inserted through the wall of the abdomen directly into the stomach. The gastrostomy tube can be attached to a drainage bag with a valve. When the valve is open, fluid and air can leave the stomach. Gastrostomy tubes are most often used to treat bowel obstructions caused by cancer.
Antibiotics. Sometimes a bowel obstruction causes a tear in the intestines that lets fluids leak into the abdomen. These fluids can cause your body to have an extreme immune response to an infection (sepsis). Antibiotics can help prevent tissue damage, organ failure, or death from sepsis.
Antinausea and pain medicines. These can treat or control nausea, vomiting, and pain caused by a bowel obstruction.
Considerations for treating a malignant bowel obstruction
If you have a bowel obstruction caused by cancer (also called malignant bowel obstruction), talk to your health care team about available treatments and your goals of care. In most cases, treatments for malignant bowel obstructions relieve symptoms and improve quality of life but may not help you live longer from cancer. You and your family may need to make difficult decisions about your care at this time. If you choose care meant to relieve symptoms over more aggressive treatments, you can learn more about Choices for Care When Treatment May Not Be an Option.
Talking with your doctor about bowel obstruction
If you think you have a bowel obstruction, contact your doctor right away. They can help you decide on a treatment that is right for you.
Questions to ask your provider about bowel obstruction:
What is causing the bowel obstruction?
What treatments are available to me?
What are possible complications of treatments I may receive for bowel obstruction?
What foods should I eat or avoid?
How much liquid should I drink each day?
What symptoms or problems should I call you about?
Will I be at risk of future bowel obstructions?
Getting support if you have a bowel obstruction
Side effects like bowel obstruction can be hard to deal with, both physically and emotionally. It’s important to ask for support from your health care team. They can help you prepare for and make it through difficult times. Learn more about ways to cope with cancer, including ways to adjust to daily life during cancer treatment.
For family members and friends who are caring for someone with cancer, you may find these suggestions for caregivers to be helpful.
How a caregiver can help
Help the person you are caring for eat and drink the foods and liquids their doctor has recommended. Many people treated for a bowel obstruction will need to be on a liquid diet while they recover.
Provide the person you are caring for with a heating pad for their belly that can help relieve pain and cramping.
Talk with the person you are caring for about their goals of care, especially if they have a malignant bowel obstruction, to help them decide on a treatment that is right for them.
Carefully review follow-up care with the person’s doctor to learn what to expect after treatment and how you can help.
Lymphedema occurs when disruption of normal lymphatic drainage leads to accumulation of protein-rich lymph fluid in the interstitial space. Cancer survivors who experience lymphedema report poor physical functioning, impaired ability to engage in normal activities of daily living, and increased psychological distress.[1–5]
Estimates of the prevalence of lymphedema vary widely due to differences in the type of cancer, measurement methods, diagnostic criteria, and timing of evaluations relative to cancer diagnosis and treatment. In a survey conducted in 2006 and 2010, 6,593 cancer survivors were asked to identify ongoing concerns. Approximately 20% of respondents reported concerns related to lymphedema. Of these individuals, 50% to 60% reported receiving care for lymphedema.[6] These results align reasonably well with a survey study of women survivors of ovarian, endometrial, and colorectal cancers, who met criteria for lymphedema based on a validated survey that demonstrated a point prevalence of 37%, 33%, and 31%, respectively.[3] Similarly, a randomized intervention study in women with breast cancer demonstrated, by limb volume measurements or physician diagnosis, that 42% of subjects had lymphedema at 18 months after surgery.[7][Level of evidence: I]
Lymphedema is a common delayed effect of cancer treatment that negatively impacts survivors’ quality of life. This summary reviews the anatomy of the lymphatic system, the pathophysiology of lymphedema secondary to cancer, and epidemiology. The summary also provides clinicians with information related to risk factors, diagnosis, prevention, and treatment. The summary does not deal with congenital lymphedema or lymphedema not related to cancer.
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
Anatomy of the Lymphatic System
The human lymphatic system generally includes superficial or primary lymphatic vessels that form a complex dermal network of capillary-like channels. Primary lymphatic vessels lack muscular walls and do not have valves. They drain into larger, secondary lymphatic vessels located in the subdermal space. Secondary lymphatic vessels run parallel to the superficial veins and drain into deeper lymphatic vessels located in the subcutaneous fat adjacent to the fascia. Unlike the primary vessels, the secondary and deeper lymphatic vessels have muscular walls and numerous valves to accomplish active and unidirectional lymphatic flow.
An intramuscular system of lymphatic vessels that parallels the deep arteries and drains the muscular compartment, joints, and synovium also exists. The superficial and deep lymphatic systems probably function independently, except in abnormal states, although there is evidence that they communicate near lymph nodes.[8] Lymph drains from the lower limbs into the lumbar lymphatic trunk. The lumbar lymphatic trunk joins the intestinal lymphatic trunk and cisterna chyli to form the thoracic duct, which empties into the left subclavian vein. The lymphatic vessels of the left arm drain into the left subclavian lymphatic trunk and then into the left subclavian vein. The lymphatic vessels of the right arm drain into the right subclavian lymphatic trunk and then into the right subclavian vein.
EnlargeThe lymph system is part of the body’s immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, adenoids (not shown), thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph tissue is also found in many other parts of the body, including the small intestine.
Pathophysiology of Lymphedema
Body fluids can be discussed in terms of their composition and the specific fluid compartment where they are located. Intracellular fluid includes all fluid enclosed by the plasma membranes of cells. Extracellular fluid (ECF) surrounds all cells in the body. ECF has two primary constituents: intravascular plasma and the interstitial fluid that surrounds all cells not in the plasma. Lymphedema is the abnormal accumulation of protein-rich fluid in the interstitial space that is accompanied by inflammation and, eventually, fibrosis.
The formation of interstitial fluid comes from the movement of intravascular fluid across the capillary membranes due to arteriolar blood pressure. Much of the interstitial fluid returns to the intravascular fluid via the postcapillary venules. The dynamics of fluid production are influenced by arterial and venous hydrostatic pressures, tissue pressure, oncotic pressures of the intravascular and interstitial fluid, and membrane permeability. Normally, the dynamics favor a net gain of interstitial fluid, with the excess removed via lymphatic channels. Because lymphatic vessels often lack a basement membrane, they can resorb molecules too large for venous uptake as well. In short, the lymphatic system controls the pressure, volume, and composition of the interstitial fluid.
Lymphatic obstruction leads to increased interstitial fluid, which often contains large proteins and cellular debris. Through mechanisms not fully understood, the increased interstitial fluid induces inflammation, destruction or sclerosis of the lymphatic vessels, fibrosis, and, ultimately, adipose tissue hypertrophy.
EnlargeThe lymphatic vessels normally maintain normal interstitial pressures by removing the excess interstitial fluid that results from the imbalance between the intravascular fluid that enters from the arterioles and exits into the venules. Large proteins and cells that cannot exit the interstitial space through the venules leave the interstitial fluid through the lymphatic vessels. As the lymph moves through the lymphatic vessels, it passes through lymph nodes and eventually into one of two lymphatic ducts that empty into a large vein near the heart. In lymphedema, the flow of lymph through the lymphatic vessels is disrupted or blocked. This leads to increased interstitial pressure and an accumulation of interstitial fluid, large proteins, and cellular debris in the interstitial space, which induces inflammation. The inflammation may cause further damage to the lymphatic vessels. The macrophages and lymphocytes release inflammatory markers, which causes fibrosis, fat cell hypertrophy, and the classical sign of swelling. Lymphedema may be caused by cancer or cancer treatment.
Epidemiology and Risk Factors
Accurate estimates of the incidence and prevalence of lymphedema are difficult to provide, due in part to differences in the definition of lymphedema (e.g., patient self-reports vs. objective volume measurements) and the timing of assessment for lymphedema relative to cancer treatment. Other factors are differences in surgical techniques related to the type of lymph node dissection or the total dose, fractions, and field of radiation administered.
Common risk factors for developing lymphedema include the following:
Extent of local surgery.
Anatomical location of lymph node dissection.
Radiation to lymph nodes.
Localized infection or delayed wound healing.
Tumor causing lymphatic obstruction of the anterior cervical, thoracic, axillary, pelvic, or abdominal nodes.
Intrapelvic or intra-abdominal tumors that involve or directly compress lymphatic vessels and/or the cisterna chyli and thoracic duct.
Having a higher disease stage.
Overweight (body mass index [BMI] ≥25 kg/m2) or obesity (BMI ≥30 kg/m2).[9]
Ridner SH: Quality of life and a symptom cluster associated with breast cancer treatment-related lymphedema. Support Care Cancer 13 (11): 904-11, 2005. [PUBMED Abstract]
Dunberger G, Lindquist H, Waldenström AC, et al.: Lower limb lymphedema in gynecological cancer survivors–effect on daily life functioning. Support Care Cancer 21 (11): 3063-70, 2013. [PUBMED Abstract]
Zhang X, McLaughlin EM, Krok-Schoen JL, et al.: Association of Lower Extremity Lymphedema With Physical Functioning and Activities of Daily Living Among Older Survivors of Colorectal, Endometrial, and Ovarian Cancer. JAMA Netw Open 5 (3): e221671, 2022. [PUBMED Abstract]
Pyszel A, Malyszczak K, Pyszel K, et al.: Disability, psychological distress and quality of life in breast cancer survivors with arm lymphedema. Lymphology 39 (4): 185-92, 2006. [PUBMED Abstract]
Gjorup CA, Groenvold M, Hendel HW, et al.: Health-related quality of life in melanoma patients: Impact of melanoma-related limb lymphoedema. Eur J Cancer 85: 122-132, 2017. [PUBMED Abstract]
Beckjord EB, Reynolds KA, van Londen GJ, et al.: Population-level trends in posttreatment cancer survivors’ concerns and associated receipt of care: results from the 2006 and 2010 LIVESTRONG surveys. J Psychosoc Oncol 32 (2): 125-51, 2014. [PUBMED Abstract]
Paskett ED, Le-Rademacher J, Oliveri JM, et al.: A randomized study to prevent lymphedema in women treated for breast cancer: CALGB 70305 (Alliance). Cancer 127 (2): 291-299, 2021. [PUBMED Abstract]
Horsley JS, Styblo T: Lymphedema in the postmastectomy patient. In: Bland KI, Copeland EM, eds.: The Breast: Comprehensive Management of Benign and Malignant Diseases. Saunders, 1991, pp 701-6.
McLaughlin SA, Brunelle CL, Taghian A: Breast Cancer-Related Lymphedema: Risk Factors, Screening, Management, and the Impact of Locoregional Treatment. J Clin Oncol 38 (20): 2341-2350, 2020. [PUBMED Abstract]
Montagna G, Zhang J, Sevilimedu V, et al.: Risk Factors and Racial and Ethnic Disparities in Patients With Breast Cancer-Related Lymphedema. JAMA Oncol 8 (8): 1195-1200, 2022. [PUBMED Abstract]
Disease-Specific Lymphedema
Breast Cancer
A systematic review found the prevalence of lymphedema to be 21.4% (14.9%–29.8%) in patients with breast cancer.[1] The incidence increased for up to 2 years after breast cancer diagnosis or surgery, and it was higher in women who underwent axillary lymph node dissection versus sentinel lymph node biopsy (19.9% vs. 5.6%). As a result, omission of axillary dissection in women with an involved sentinel lymph node is now an accepted practice. This practice is a result of a phase III randomized study (ACOSOG-Z0011) that showed no difference in overall survival in women who did not undergo a complete axillary dissection, compared with those who did.[2] Additional risk factors for lymphedema development included greater number of lymph nodes dissected, having a mastectomy, and overweight or obesity.[1,3] In a prospective study of neoadjuvant chemotherapy followed by axillary lymph node dissection (ACOSOG-Z1071), the incidence of lymphedema after a median follow-up of 3 years was 37.8% (95% confidence interval [CI], 33.1%–43.2%). Increasing body mass index (BMI) (hazard ratio [HR], 1.04; 95% CI, 1.01–1.06), duration of neoadjuvant chemotherapy (HR, 1.48; 95% CI, 1.01–2.17), number of lymph nodes removed, and number of involved lymph nodes were associated with lymphedema symptoms.[4]
Several risk factors for breast cancer–related lymphedema (BCRL) were demonstrated in a study using data from a 2-year, prospective observational study of 304 patients with breast cancer who had axillary lymph node dissection and radiation therapy. The cumulative incidence of lymphedema was measured by a more than 10% increase in arm volume, and univariate and multivariable analyses were performed. On multivariable analysis, Black race and Hispanic ethnicity (odds ratio [OR], 3.88; 95% CI, 2.14–7.08, and OR, 3.01; 95% CI, 1.10–7.62, respectively; P < .001 for each), receipt of neoadjuvant chemotherapy (OR, 2.10; 95% CI, 1.16–3.95; P = .01), older age (OR, 1.04; 95% CI, 1.02–1.07 per 1-year increase; P = .001), and a longer follow-up interval (OR, 1.57; 95% CI, 1.30–1.90 per 6-month increase; P < .001) were independently associated with an increased risk.[5][Level of evidence: II]
Another study examined risk factors for BCRL related to treatment, comorbidities, and lifestyle in 918 women enrolled in a Prospective Surveillance and Early Intervention (PSEI) trial. Women were randomly assigned to either bioimpedance spectroscopy (BIS) or tape measurement (TM).[6] In a secondary analysis, risk factors were used to test for factor associations with outcomes (no lymphedema, subclinical lymphedema, progression to chronic lymphedema after intervention, progression to chronic lymphedema without intervention). Factors associated with BCRL risk included axillary lymph node dissection (P < .001), taxane-based chemotherapy (P < .001), regional nodal irradiation (P ≤ .001), BMI greater than 30 (P = .002), and rurality (P = .037).[6]
Gynecological Cancers
A cohort study supports the evidence that a significant proportion of women experience lower-limb lymphedema after treatment of gynecological cancer or colorectal cancer. The highest prevalence (36.5%) among ovarian cancer survivors, followed by endometrial cancer survivors (32.5%) and colorectal cancer survivors (31.4%).[7]
In one study, 802 of 1,774 women diagnosed with a gynecological cancer between 1999 and 2004 responded to a survey about lymphedema.[8] Twenty-five percent of the respondents reported lower-extremity edema; 10% had been diagnosed with lymphedema. Most respondents (75%) had been diagnosed with these conditions within the first year of a cancer diagnosis. Women with vulvar cancer were most likely to have symptoms (36%). Lymph node dissection increased the risk of symptoms in women with cervical cancer but not uterine cancer. The range of symptoms included heavy legs, pain, and skin tightness. Standing all day, long-distance travel, and hot weather were precipitating conditions. The most common treatments were compression garments, massage, and lymphatic exercises. The findings related to high prevalence in patients with vulvar cancer and occurrence of symptoms within the first year have been verified.[9]
Serial limb volume measurements were obtained from a cohort of women who underwent a lymph node dissection for vulvar (n = 42), endometrial (n = 734), or cervical (n = 138) cancer 4 to 6 weeks after surgery and then every 3 months.[10] The incidence of an increase in limb volume of more than 10% was 43% for vulvar cancer, 34% for endometrial cancer, and 33% for cervical cancer. The incidence of severe lymphedema (>40% increase in volume) was less than 2% in all cohorts. The peak incidence was at the 4- to 6-week time point, but new cases were identified at all time points. The risk-factor analysis identified a reduced risk in women older than 65 years and a higher risk in women who had more than eight lymph nodes removed in the endometrial cohort.
Head and Neck Cancer
Patients with head and neck cancer are susceptible to external and internal lymphedema. External lymphedema typically presents with submental edema or lower neck swelling. Internal lymphedema is more widely distributed in the anatomical regions of the oropharynx. In a small cross-sectional study with video-assisted examinations, 59 of 61 patients had some degree of lymphedema.[11][Level of evidence: II] Sixty-one percent of the patients had only internal lymphedema, 35% had internal and external lymphedema, and 4% had only external lymphedema. Postoperative radiation therapy was a risk factor for combined lymphedema. Chemotherapy was a risk factor for patients with internal lymphedema only.
Melanoma
One single-center, cross-sectional study reported on lymphedema after either sentinel lymph node biopsy or lymph node dissection in 435 patients who were treated for melanoma between 1997 and 2015.[12] The authors reported a lymphedema prevalence of 25%. Forty-eight patients (44%) had International Society of Lymphology (ISL) stage I lymphedema (pitting edema), and 61 patients (56%) had ISL stage II or III lymphedema. Multivariate analyses identified as potential predictive factors the primary site of disease on the affected limb, inguinal surgery, and persistent pain at the site of lymph node surgery. Limb cellulitis was a risk factor for ISL stage II and III lymphedema. The same investigators also reported on health-related quality of life in an earlier publication. In another smaller, single-institution, retrospective study of 66 patients who underwent therapeutic nodal dissection, the rate of permanent lymphedema for inguinal node dissection was 38%, compared with 12% for axillary node dissection.[13] Another potentially relevant variable is the type of dissection. A 2017 systematic review did not find an appreciable difference between the rate of lymphedema after therapeutic lymphadenectomy and completion of lymph node sampling after a positive sentinel lymph node biopsy.[14] In both instances, the rate was around 20%.
Prostate Cancer
There are few studies of lymphedema after prostate cancer therapy. A small cross-sectional survey of men who underwent radical prostatectomy reported that 19 of 54 respondents (35.2%) had bilateral lower-extremity lymphedema.[15][Level of evidence: II] Of note, 25 respondents reported that they had received manual lymphatic drainage therapy. Men who did not experience regression experienced more distress related to physical and mental functioning than those who did. An elevated BMI and poor general health were risk factors for lymphedema.
Sarcoma
One study measured patient demographics, surgical outcomes data, functional outcomes, and lymphedema severity with a validated scale for 289 patients who underwent limb preservation surgery of an extremity sarcoma between 2000 and 2007.[16] The mean time from surgery was 35 months (range, 12–60 months). Eighty-three patients had some degree of lymphedema, including 58 with mild but definite swelling, 22 with moderate swelling, and 3 with considerable swelling. No patients had grade 4 or very severe swelling with shiny skin and skin cracking. Univariate analysis demonstrated that radiation therapy, tumor size, and tumor depth correlated with severity. The location of the sarcoma (upper or lower extremity), lymph node dissection (yes or no), and BMI did not correlate with severity. Multivariable analysis demonstrated that tumor size was the only independent predictor.
References
DiSipio T, Rye S, Newman B, et al.: Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol 14 (6): 500-15, 2013. [PUBMED Abstract]
Giuliano AE, Ballman KV, McCall L, et al.: Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 318 (10): 918-926, 2017. [PUBMED Abstract]
McLaughlin SA, Brunelle CL, Taghian A: Breast Cancer-Related Lymphedema: Risk Factors, Screening, Management, and the Impact of Locoregional Treatment. J Clin Oncol 38 (20): 2341-2350, 2020. [PUBMED Abstract]
Armer JM, Ballman KV, McCall L, et al.: Factors Associated With Lymphedema in Women With Node-Positive Breast Cancer Treated With Neoadjuvant Chemotherapy and Axillary Dissection. JAMA Surg 154 (9): 800-809, 2019. [PUBMED Abstract]
Montagna G, Zhang J, Sevilimedu V, et al.: Risk Factors and Racial and Ethnic Disparities in Patients With Breast Cancer-Related Lymphedema. JAMA Oncol 8 (8): 1195-1200, 2022. [PUBMED Abstract]
Koelmeyer LA, Gaitatzis K, Dietrich MS, et al.: Risk factors for breast cancer-related lymphedema in patients undergoing 3 years of prospective surveillance with intervention. Cancer 128 (18): 3408-3415, 2022. [PUBMED Abstract]
Zhang X, McLaughlin EM, Krok-Schoen JL, et al.: Association of Lower Extremity Lymphedema With Physical Functioning and Activities of Daily Living Among Older Survivors of Colorectal, Endometrial, and Ovarian Cancer. JAMA Netw Open 5 (3): e221671, 2022. [PUBMED Abstract]
Beesley V, Janda M, Eakin E, et al.: Lymphedema after gynecological cancer treatment : prevalence, correlates, and supportive care needs. Cancer 109 (12): 2607-14, 2007. [PUBMED Abstract]
Ryan M, Stainton MC, Slaytor EK, et al.: Aetiology and prevalence of lower limb lymphoedema following treatment for gynaecological cancer. Aust N Z J Obstet Gynaecol 43 (2): 148-51, 2003. [PUBMED Abstract]
Carter J, Huang HQ, Armer J, et al.: GOG 244 – The LymphEdema and Gynecologic cancer (LEG) study: The association between the gynecologic cancer lymphedema questionnaire (GCLQ) and lymphedema of the lower extremity (LLE). Gynecol Oncol 155 (3): 452-460, 2019. [PUBMED Abstract]
Jeans C, Brown B, Ward EC, et al.: Comparing the prevalence, location, and severity of head and neck lymphedema after postoperative radiotherapy for oral cavity cancers and definitive chemoradiotherapy for oropharyngeal, laryngeal, and hypopharyngeal cancers. Head Neck 42 (11): 3364-3374, 2020. [PUBMED Abstract]
Gjorup CA, Groenvold M, Hendel HW, et al.: Health-related quality of life in melanoma patients: Impact of melanoma-related limb lymphoedema. Eur J Cancer 85: 122-132, 2017. [PUBMED Abstract]
Deban M, Vallance P, Jost E, et al.: Higher Rate of Lymphedema with Inguinal versus Axillary Complete Lymph Node Dissection for Melanoma: A Potential Target for Immediate Lymphatic Reconstruction? Curr Oncol 29 (8): 5655-5663, 2022. [PUBMED Abstract]
Moody JA, Botham SJ, Dahill KE, et al.: Complications following completion lymphadenectomy versus therapeutic lymphadenectomy for melanoma – A systematic review of the literature. Eur J Surg Oncol 43 (9): 1760-1767, 2017. [PUBMED Abstract]
Neuberger M, Schmidt L, Wessels F, et al.: Onset and burden of lower limb lymphedema after radical prostatectomy: a cross-sectional study. Support Care Cancer 30 (2): 1303-1313, 2022. [PUBMED Abstract]
Friedmann D, Wunder JS, Ferguson P, et al.: Incidence and Severity of Lymphoedema following Limb Salvage of Extremity Soft Tissue Sarcoma. Sarcoma 2011: 289673, 2011. [PUBMED Abstract]
Diagnosis of Lymphedema
Signs, Symptoms, and Physical Examination
Lymphedema is typically evident by clinical findings such as unilateral, nonpitting edema, usually with involvement of the digits, in a patient with known risk factors (e.g., a breast cancer patient with previous axillary dissection). Other causes of limb swelling, including deep venous thrombosis, malignancy, and infection, should be considered in the differential diagnosis and excluded with appropriate studies, if indicated.
Lymphedema in patients with head and neck cancer can present slightly differently. External lymphedema does show swelling in the head and neck area, but internal lymphedema does not. Instead, patients with lymphedema related to internal head and neck cancer can present with complaints of voice changes, dysphagia, and possible difficulty breathing.
Diagnostic Testing
Limb measurements
The wide variety of methods for evaluating limb volume and lack of standardization make it difficult for the clinician to assess the at-risk limb. Options include water displacement, tape measurement, infrared scanning, and bioelectrical impedance measures.[1]
The most common method for diagnosing upper-extremity lymphedema is circumferential upper-extremity measurement using specific anatomical landmarks.[2] Arm circumference measurements are used to estimate volume differences between the affected and unaffected arms. Sequential measurements are taken at four points on both arms: the metacarpal-phalangeal joints, the wrist, 10 cm distal to the lateral epicondyles, and 15 cm proximal to the lateral epicondyles. Differences of 2 cm or more at any point compared with the unaffected arm are considered by some experts to be clinically significant. However, measuring specific differences between arms may have limited clinical relevance because of implications, such as a 3-cm difference between the arm of an obese woman and the arm of a thin woman. In addition, there can be inherent anatomical variations in circumference between the dominant and nondominant limb related to differences in muscle mass. In addition, variations after breast cancer treatment may occur with atrophy of the ipsilateral arm or hypertrophy of the contralateral arm.[3] A small study comparing various methods of assessing upper-limb lymphedema did not show superiority of any one method.[1] Sequential measurements over time, including pretreatment measurements, may prove to be more clinically meaningful.
The water displacement method is another way to evaluate arm edema. A volume difference of 200 mL or more between the affected and opposite arms is typically considered to be a cutoff point to define lymphedema.[4]
Magnetic resonance lymphography (MRL)
This technique involves the intracutaneous injection of a paramagnetic contrast agent, followed by imaging of the lymphatic anatomy, dermal flow patterns, and adjacent fatty tissue. One study of 50 women with breast cancer–related lymphedema compared the lymphatic vessel morphology in their affected and unaffected arms.[5][Level of evidence: II] The lymphedema was staged according to the ISL’s 2016 staging system.[6][Level of evidence: IV] In all patients, the lymph fluid was in the subcutis but not the subfascial compartment of the affected arm. In stage I patients, the lymphatics were tortuous and dilated, but there was no dermal backflow or regeneration of the lymphatics. In stage II patients, there was soft tissue fibrosis and adipose tissue hypertrophy. The lymphatics were tortuous and dilated, with areas of dermal backflow and regeneration. In stage III patients, the lymphatics were unrecognizable, and there was confluent dermal backflow. The soft tissue fibrosis was more advanced. MRL is safe, feasible, and provides high anatomical detail. However, its role in lymphedema diagnosis remains to be determined.
Staging and grading of severity
The staging system of the ISL reflects likely changes over time based on the pathophysiology of lymphedema. The stages include the following:
Stage 0: This stage, referred to as subclinical lymphedema, is characterized by impaired lymph flow.
Stage I: This stage is spontaneously reversible and typically marked by pitting edema, an increase in upper-extremity girth, and heaviness.
Stage II: This moderate stage is characterized by a spongy consistency of the tissue without signs of pitting edema. Tissue fibrosis can then cause the limbs to harden and increase in size.[2] The swelling at this stage is mostly fluid.
Stage III: In the most advanced stage,[2] swelling is mostly secondary to fat hypertrophy, so there is no pitting edema.
The severity of lymphedema may be evaluated using the Common Terminology Criteria for Adverse Events (CTCAE), which was developed for grading adverse events in the context of clinical trials.[7] A key advantage of the CTCAE approach is that it includes both objective measures (interlimb discrepancy) and subjective clinical assessments in diagnosing lymphedema. This approach allows the clinician to address troublesome signs and symptoms that may occur without significant interlimb discrepancy. The CTCAE volume 3 criteria are:
Grade 1: 5% to 10% interlimb discrepancy in volume or circumference at point of greatest visible difference; swelling or obscuration of anatomical architecture on close inspection; pitting edema.
Grade 2: More than 10% to 30% interlimb discrepancy in volume or circumference at point of greatest visible difference; readily apparent obscuration of anatomical architecture; obliteration of skin folds; readily apparent deviation from normal anatomical contour.
Grade 3: More than 30% interlimb discrepancy in volume; lymphorrhea; gross deviation from normal anatomical contour; interference with activities of daily living (ADL).
Grade 3: Severe symptoms; limitation in self-care ADL.
References
Ridner SH, Montgomery LD, Hepworth JT, et al.: Comparison of upper limb volume measurement techniques and arm symptoms between healthy volunteers and individuals with known lymphedema. Lymphology 40 (1): 35-46, 2007. [PUBMED Abstract]
Bicego D, Brown K, Ruddick M, et al.: Exercise for women with or at risk for breast cancer-related lymphedema. Phys Ther 86 (10): 1398-405, 2006. [PUBMED Abstract]
Petrek JA: Commentary: prospective trial of complete decongestive therapy for upper extremity lymphedema after breast cancer therapy. Cancer J 10 (1): 17-9, 2004.
Mondry TE, Riffenburgh RH, Johnstone PA: Prospective trial of complete decongestive therapy for upper extremity lymphedema after breast cancer therapy. Cancer J 10 (1): 42-8; discussion 17-9, 2004 Jan-Feb. [PUBMED Abstract]
Sheng L, Zhang G, Li S, et al.: Magnetic Resonance Lymphography of Lymphatic Vessels in Upper Extremity With Breast Cancer-Related Lymphedema. Ann Plast Surg 84 (1): 100-105, 2020. [PUBMED Abstract]
Executive Committee: The Diagnosis and Treatment of Peripheral Lymphedema: 2016 Consensus Document of the International Society of Lymphology. Lymphology 49 (4): 170-84, 2016. [PUBMED Abstract]
Cheville AL, McGarvey CL, Petrek JA, et al.: The grading of lymphedema in oncology clinical trials. Semin Radiat Oncol 13 (3): 214-25, 2003. [PUBMED Abstract]
National Cancer Institute: Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Bethesda, Md: U.S. Department of Health and Human Services, National Institutes of Health, 2017. Available online. Last accessed Dec. 18, 2024.
Prevention and Treatment Options Overview for Lymphedema
There are many potential interventions to reduce the risk of lymphedema or ameliorate its negative consequences. In general, the prevention and treatment interventions may be divided into nonsurgical and surgical approaches. Nonsurgical interventions may be further divided into pharmacological, compressive, or exercise related. Conservative options should be tried and exhausted prior to considering surgical options. This section provides an overview of the various interventions, followed by a more detailed analysis of individual trials based on the type of cancer.
Nonsurgical Options
Compression garments
Compression garments are used to prevent and treat lymphedema by helping to decrease excess formation of interstitial fluid, prevent reflux of lymphatic fluid, and give a barrier to help muscle pumping of fluid up the lymphatic system.[1][Level of evidence: I] Use of flat knit (inelastic) compression garments is better than elastic compression in both the reduction and maintenance phase of stages II and III lymphedema. Inelastic compression garments allow the lymph fluid to be better propelled through the impaired lymphatic system via skeletal muscles. Flat knit garments also have the advantage of applying pressure to firm and soften edema. This pressure is applied at a uniform gradient over a large area. Circular knit garments deliver more pressure in the distal (narrow) part of the garment and are better for venous insufficiency than lymphedema.
Elastic garments are best used for stage I lymphedema and lymphedema that has been converted to stage II after complete decongestive therapy (CDT).
Intermittent external pneumatic compression
This approach should be used in conjunction with compression garments and only if compression is not enough to prevent or treat lymphedema. Concerns regarding the use of intermittent pneumatic compression include the optimum amount of pressure, treatment schedule, and the need for maintenance therapy after the initial reduction in edema.[2][Level of evidence: I] There is a theoretical concern that pressures higher than 60 mm Hg and long-term use may injure lymphatic vessels.
Intermittent external pneumatic compression may improve lymphedema management when used adjunctively with decongestive lymphatic therapy. A small randomized trial of 23 women with new breast cancer–associated lymphedema found an additional significant volume reduction, compared with manual lymphatic drainage alone (45% vs. 26%).[3][Level of evidence: I] Similarly, improvements were also found in the maintenance phase of therapy.
There are several barriers to multidisciplinary decongestive therapy, including cost, inadequate number of trained therapists, and time commitment. In response to these barriers, a group of researchers conducted a trial of a garment under commercial development.[4] The device was fit to patients, who were instructed to use it twice daily for 8 weeks. The investigators randomly assigned subjects to the device group or a wait-list control group. Use of the device was feasible, although most subjects found twice a day too burdensome. The treated subjects reported greater perceived ability to control lymphedema and subjectively had less swelling. There were no serious adverse events related to device usage. The economic costs of advanced compressive devices in lymphedema related to venous insufficiency compared favorably with other compressive techniques in a study of claims data.[5]
Complete decongestive therapy (CDT)
CDT is the standard of care for stage II lymphedema. However, the optimal program has not been established.
CDT has two phases:
Phase 1—Decongestion/reduction: Skin/wound care, exercise, manual lymphatic drainage, and compression bandages, performed daily for an average of 15 days.
Phase 2—Maintenance: Skin/wound care, exercise, manual lymphatic drainage as needed, and compression garments.
One study compared manual lymphatic drainage with exercise to treat lymphedema in 39 people with oral cavity cancer.[6] Exercise and manual lymphatic drainage each improved neck range of motion and controlled lymphedema, but they appeared to have a better effect when done together.
A systematic review of manual lymphatic drainage in patients with breast cancer reported on ten studies.[7] Four of the studies reported that manual lymphatic drainage could reduce the incidence of lymphedema (risk ratio, 0.58; 95% confidence interval [CI], 0.37–0.93). However, seven of the studies did not show a statistical difference in volumetric changes. They did see a statistical difference in pain control, but not in quality of life.
Physical exercise
Physical exercise may be valuable in the treatment of lymphedema for several reasons, including improvement in lymph flow from muscle contractions and overall cardiovascular function.[8] Conversely, early concerns that exercise may cause harm have not been confirmed.[9,10] Results from a small randomized study suggest that resistance exercise may be offered concurrently with CDT.[11][Level of evidence: I]
A systematic review and meta-analysis reported on 12 prevention and 36 treatment studies of exercise to either prevent or treat cancer-related lymphedema.[8] Most studies (11 of 12 and 32 of 36) enrolled patients with breast cancer. In addition, while most studies investigated some form of resistance training, a few used aerobic exercise alone. The relative risk of developing lymphedema after exercise was 0.90 (95% CI, 0.72–1.13), which was not significant. However, there was a suggested benefit in patients who had more than five lymph nodes removed. In this case, the relative risk was 0.49 (95% CI, 0.28–0.85). For patients in the treatment studies, the standardized mean difference (SMD) in measured outcomes was −0.11 (95% CI, −0.22 to 0.01). The difference compared with the control condition was −0.10 (95% CI, −0.24 to 0.04). Significant differences were detected for discrete outcomes such as pain, upper-body function and strength, lower-body strength, fatigue, and quality of life for those in the exercise group (SMD, 0.3–0.8; P < .05).
The American College of Sports Medicine advises that a supervised, progressive resistance exercise program is safe for patients with or at risk for lymphedema after breast cancer. There is not adequate data about the safety of unsupervised exercise. The safety of exercise in other cancers is unknown.[12][Level of evidence: IV]
Pharmacological therapy
Nonsteroidal anti-inflammatory drugs (NSAIDs)
The potential benefit of the NSAID ketoprofen on lymphedema was demonstrated in a pair of small trials.[13] The rationale for the use of NSAIDs rests on observations of histopathological inflammatory changes in the affected tissue and a possible relationship between persistent inflammation and impaired lymphangiogenesis. The authors reported an open-label trial, followed by a small placebo-controlled trial. In the latter, 18 patients were treated with placebo and 16 patients were treated with ketoprofen for 4 months. In both trials, ketoprofen treatment led to a significant reduction in skin thickness and an improvement in the histopathological appearance of the skin. In neither trial, however, were there changes in limb volume or skin impedance. These promising early results require verification, given the potential gastrointestinal and cardiovascular risks of NSAIDs.
Surgical Options
The surgical options for the treatment of lymphedema include lymphatico-venous anastomoses (LVA), vascularized lymph node transplantation (VLNT), and reduction of excess tissue volume by excision of liposuction. Several informative reviews describe the surgical decision making involved in selecting patients and the type of operation.[14]
There are limited data to guide the choice between liposuction and microsurgical techniques, and some investigators propose a combined approach.[15] The choice of microsurgical techniques may be aided by imaging and clinical grading of lymphedema severity. One proposal suggests that patients are candidates for LVA if they have partial obstruction seen on lymphoscintigraphy and grade 1 or 2 lymphedema with patent lymphatic ducts observed on indocyanine green lymphography . On the other hand, VLNT may be better for patients exhibiting a total obstruction seen on lymphoscintigraphy and grade 3 or 4 lymphedema without patent lymphatic ducts observed on indocyanine green lymphography.[16]
Lymphatico-venous anastomosis
LVA surgery is typically used in patients with early-grade lymphedema due to difficulties in finding lymphatic vessels. One study reported results for 42 patients with later-grade, lower-extremity lymphedema who underwent preoperative magnetic resonance lymphangiography and ultrasound.[17] The imaging allowed patients to have an average of five successful anastomoses per limb. Clinical outcomes were favorable, raising the possibility of expanded indications for this surgery.
Immediate lymphatic reconstruction at the time of cancer surgery is under active investigation.
Vascularized lymph node transfer
VLNT involves harvesting healthy lymph nodes and their relevant venous and arterial vessels from a donor site and transferring them to the nodal basin of the affected extremity. The proposed mechanisms of action include providing alternative routes of lymphatic drainage and encouraging lymphangiogenesis to provide new lymph vessels to the extremity. At present, there is scant but promising clinical data on the efficacy of VLNT.[18]
A systematic review and summary of patients with breast cancer–related lymphedema who underwent CDT or VLNT [19] examined the evidence that both interventions favorably impact health-related quality of life measures. As anticipated, the data for VLNT was more limited (two studies, 65 patients) than for CDT (14 studies, 569 patients). However, within these limits, the data for VLNT indicated that improvements were commonly seen. The data for CDT were more heterogenous, and the improvement was often less significant. These data give clinicians a reason to consider surgical intervention, although at present the standard practice seems to be CDT.
In a retrospective study of 124 patients with breast cancer–related lymphedema, the degree of improvement in limb circumference and reduction in episodes of cellulitis appeared to be greater in patients who underwent VLNT than in those who underwent LVA.[16] In addition to the usual caution in interpreting retrospective data, the patients who underwent VLNT were ineligible for LVA based on lymphography results. This finding seems to support the use of imaging to guide patient selection. Two small cohort studies of VLNT in patients with breast cancer demonstrated apparent improvements in objective limb measurements and subjective measures of patients’ health-related quality of life.[20][Level of evidence: III]; [21][Level of evidence: II]
Liposuction
Nonpitting chronic lymphedema may be due to adipose tissue hypertrophy. In this case, liposuction to remove the excess adipose tissue is an option. Compression garments are still needed after the liposuction. In addition, excision of the redundant skin after liposuction may be required.[22]
One retrospective study compared the frequency of documented episodes of erysipelas in 130 patients before and after they underwent liposuction.[23] As anticipated, the mean excess arm volume decreased from 1,607 mL to negative 43 mL, and the ratio of affected to normal arm decreased from 1.5 to 1.0. The recorded occurrence of erysipelas decreased from 0.47 to 0.06 attacks per year. Similar results were reported in another study,[24] in which the authors reviewed the charts of 105 women with breast cancer–related lymphedema refractory to compressive therapies who underwent liposuction between 1993 and 2012. Notably, patients had to have nonpitting edema. All women benefited, and the benefit persisted for at least 5 years by measurement.
Laser therapy
Low-level laser therapy (LLT) is a noninvasive technique in which affected tissues receive phototherapy of various wavelengths within 650 to 1,000 nanometers. The role of LLT in the care of people with lymphedema is not established, although a 2017 systematic review found promising evidence.[25] The proposed mechanisms of action include cellular proliferation of macrophages with reduction in fibrosis, reduced inflammatory mediators, lymphangiogenesis, and improved lymphatic flow.[25] In addition, carbon dioxide laser treatment may also lead to clinical improvements, though the data are currently only from small case series.[26] The carbon dioxide laser stimulates remodeling of abnormal collagen by matrix metalloproteinases and dermal neocollagenesis by fibroblasts and supports generation of new lymphatic vessels.
References
Nadal Castells MJ, Ramirez Mirabal E, Cuartero Archs J, et al.: Effectiveness of Lymphedema Prevention Programs With Compression Garment After Lymphatic Node Dissection in Breast Cancer: A Randomized Controlled Clinical Trial. Front Rehabil Sci 2: 727256, 2021. [PUBMED Abstract]
Dini D, Del Mastro L, Gozza A, et al.: The role of pneumatic compression in the treatment of postmastectomy lymphedema. A randomized phase III study. Ann Oncol 9 (2): 187-90, 1998. [PUBMED Abstract]
Szuba A, Achalu R, Rockson SG: Decongestive lymphatic therapy for patients with breast carcinoma-associated lymphedema. A randomized, prospective study of a role for adjunctive intermittent pneumatic compression. Cancer 95 (11): 2260-7, 2002. [PUBMED Abstract]
Ridner SH, Dietrich MS, Deng J, et al.: Advanced pneumatic compression for treatment of lymphedema of the head and neck: a randomized wait-list controlled trial. Support Care Cancer 29 (2): 795-803, 2021. [PUBMED Abstract]
Lerman M, Gaebler JA, Hoy S, et al.: Health and economic benefits of advanced pneumatic compression devices in patients with phlebolymphedema. J Vasc Surg 69 (2): 571-580, 2019. [PUBMED Abstract]
Tsai KY, Liao SF, Chen KL, et al.: Effect of early interventions with manual lymphatic drainage and rehabilitation exercise on morbidity and lymphedema in patients with oral cavity cancer. Medicine (Baltimore) 101 (42): e30910, 2022. [PUBMED Abstract]
Lin Y, Yang Y, Zhang X, et al.: Manual Lymphatic Drainage for Breast Cancer-related Lymphedema: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin Breast Cancer 22 (5): e664-e673, 2022. [PUBMED Abstract]
Hayes SC, Singh B, Reul-Hirche H, et al.: The Effect of Exercise for the Prevention and Treatment of Cancer-Related Lymphedema: A Systematic Review with Meta-analysis. Med Sci Sports Exerc 54 (8): 1389-1399, 2022. [PUBMED Abstract]
Schmitz KH, Ahmed RL, Troxel A, et al.: Weight lifting in women with breast-cancer-related lymphedema. N Engl J Med 361 (7): 664-73, 2009. [PUBMED Abstract]
Singh B, Disipio T, Peake J, et al.: Systematic Review and Meta-Analysis of the Effects of Exercise for Those With Cancer-Related Lymphedema. Arch Phys Med Rehabil 97 (2): 302-315.e13, 2016. [PUBMED Abstract]
Do JH, Kim W, Cho YK, et al.: EFFECTS OF RESISTANCE EXERCISES AND COMPLEX DECONGESTIVE THERAPY ON ARM FUNCTION AND MUSCULAR STRENGTH IN BREAST CANCER RELATED LYMPHEDEMA. Lymphology 48 (4): 184-96, 2015. [PUBMED Abstract]
Campbell KL, Winters-Stone KM, Wiskemann J, et al.: Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med Sci Sports Exerc 51 (11): 2375-2390, 2019. [PUBMED Abstract]
Rockson SG, Tian W, Jiang X, et al.: Pilot studies demonstrate the potential benefits of antiinflammatory therapy in human lymphedema. JCI Insight 3 (20): , 2018. [PUBMED Abstract]
Forte AJ, Boczar D, Huayllani MT, et al.: Pharmacotherapy Agents in Lymphedema Treatment: A Systematic Review. Cureus 11 (12): e6300, 2019. [PUBMED Abstract]
Engel H, Lin CY, Huang JJ, et al.: Outcomes of Lymphedema Microsurgery for Breast Cancer-related Lymphedema With or Without Microvascular Breast Reconstruction. Ann Surg 268 (6): 1076-1083, 2018. [PUBMED Abstract]
Cha HG, Oh TM, Cho MJ, et al.: Changing the Paradigm: Lymphovenous Anastomosis in Advanced Stage Lower Extremity Lymphedema. Plast Reconstr Surg 147 (1): 199-207, 2021. [PUBMED Abstract]
Gould DJ, Mehrara BJ, Neligan P, et al.: Lymph node transplantation for the treatment of lymphedema. J Surg Oncol 118 (5): 736-742, 2018. [PUBMED Abstract]
Fish ML, Grover R, Schwarz GS: Quality-of-Life Outcomes in Surgical vs Nonsurgical Treatment of Breast Cancer-Related Lymphedema: A Systematic Review. JAMA Surg 155 (6): 513-519, 2020. [PUBMED Abstract]
Aljaaly HA, Fries CA, Cheng MH: Dorsal Wrist Placement for Vascularized Submental Lymph Node Transfer Significantly Improves Breast Cancer-Related Lymphedema. Plast Reconstr Surg Glob Open 7 (2): e2149, 2019. [PUBMED Abstract]
Gratzon A, Schultz J, Secrest K, et al.: Clinical and Psychosocial Outcomes of Vascularized Lymph Node Transfer for the Treatment of Upper Extremity Lymphedema After Breast Cancer Therapy. Ann Surg Oncol 24 (6): 1475-1481, 2017. [PUBMED Abstract]
Chen WF, Zeng WF, Hawkes PJ, et al.: Lymphedema Liposuction with Immediate Limb Contouring. Plast Reconstr Surg Glob Open 7 (11): e2513, 2019. [PUBMED Abstract]
Lee D, Piller N, Hoffner M, et al.: Liposuction of Postmastectomy Arm Lymphedema Decreases the Incidence of Erysipelas. Lymphology 49 (2): 85-92, 2016. [PUBMED Abstract]
Hoffner M, Ohlin K, Svensson B, et al.: Liposuction Gives Complete Reduction of Arm Lymphedema following Breast Cancer Treatment-A 5-year Prospective Study in 105 Patients without Recurrence. Plast Reconstr Surg Glob Open 6 (8): e1912, 2018. [PUBMED Abstract]
Baxter GD, Liu L, Petrich S, et al.: Low level laser therapy (Photobiomodulation therapy) for breast cancer-related lymphedema: a systematic review. BMC Cancer 17 (1): 833, 2017. [PUBMED Abstract]
Menzer C, Aleisa A, Wilson BN, et al.: Efficacy of laser CO2 treatment for refractory lymphedema secondary to cancer treatments. Lasers Surg Med 54 (3): 337-341, 2022. [PUBMED Abstract]
Disease-Specific Interventions for Prevention or Treatment of Lymphedema
Breast Cancer: Prevention of Lymphedema
Compression garments
A randomized study of women who underwent an axillary dissection suggested that compression sleeves worn from the first postoperative day until 3 months after completion of adjuvant therapy reduced the risk of lymphedema.[1][Level of evidence: I] Women (n = 155) who were randomly assigned to the compression intervention had less arm swelling, as determined by bioimpedance spectroscopy (BIS) thresholds and relative arm volume increase (RAVI), than women assigned to usual care. The cumulative incidence of arm swelling at 1 year was 42% by BIS and 14% by RAVI in women who received compression garments, compared with 52% and 25%, respectively, for usual care. The hazard ratio for developing arm swelling in the compression group relative to the control group was 0.61 (95% confidence interval, 0.43–0.85; P = .004) by BIS and 0.56 (95% CI, 0.33–0.96; P = .034) by RAVI. There were no differences in patient-reported outcomes.
Exercise
A randomized trial suggested that exercise might help prevent lymphedema after breast cancer surgery.[2][Level of evidence: I] The investigators randomly assigned 77 eligible women to a control arm or to 12 months of gym membership with a 13-week training session in weightlifting. Eligibility criteria included a diagnosis of breast cancer within 1 to 5 years, at least two lymph nodes removed, a body mass index (BMI) of less than 50, no prior history of lymphedema, and no asymmetry in the arms greater than 10%. The primary outcome was an increase in affected arm volume of greater than 5% at 1 year. A secondary outcome was clinician-defined lymphedema. The percentages of women who met the criteria for the primary outcome in the control and weightlifting cohorts were 17% and 11%, respectively (P = .04). The reduction in the rate in women who had five or more lymph nodes removed was even greater (22% in the control cohort vs. 7% in the weightlifting cohort; P = .003). However, there were no differences in the rates of clinician-defined lymphedema, which were much lower in each arm (4.4% in the control cohort vs. 1.5% in the weightlifting cohort).
A 2021 randomized trial studied patients with breast cancer who underwent either an axillary or sentinel lymph node dissection.[3][Level of evidence: I] The investigators randomly assigned 568 women to one of two groups. All subjects met with a trained lymphedema prevention educator and received information about lymphedema, including preventive self-care practices. The 315 women receiving the active intervention met with a physical therapist who provided an individual exercise program, weights, and an elastic compression sleeve to wear. The primary end point was the lymphedema-free rate at 18 months. Lymphedema was defined by either an increase in volume of the affected extremity of more than 10% or a doctor’s diagnosis. There were no differences between groups in the primary end point. Overall, 69% of participants in the education-only arm and 70% in the intervention arm were free of lymphedema at 18 months. But adherence in the intervention arm was poor (less than 50%) due to time constraints and a perceived lack of benefit. There were no differences in health-related quality of life between the cohorts.[4]
At present, exercise therapy with compression garments may not effectively prevent lymphedema. Exercise with other interventions has been investigated. For example, one study reported the results of a randomized trial of manual lymphatic drainage in addition to exercise therapy in preventing lymphedema.[5][Level of evidence: I] The investigators randomly assigned 160 women to receive or not receive manual lymphatic drainage in addition to exercise and suggestions to minimize lymphedema. Participants underwent serial volume measurements. At 6 months, 24% of women in the intervention group and 19% in the control group had an increase in volume of greater than 200 mL.
Breast Cancer: Treatment of Lymphedema
Complete decongestive therapy (CDT)
Compression sleeves alone may prevent progression of less severe lymphedema, but women often need more intensive interventions.[6][Level of evidence: I] In one study, 103 women had post–breast cancer lymphedema that caused at least a 10% increase in volume in the affected arm compared with the unaffected arm. Participants were randomly assigned to either CDT comprising elastic compression garments plus 20 daily manual lymphatic drainage sessions with a trained therapist (n = 57) or elastic compression garments alone (n = 46).[7][Level of evidence: I] The primary outcome was the percentage change in excess arm volume from baseline to 6 weeks. The women assigned to CDT experienced greater absolute volume loss than the women treated with compression garments alone (250 mL vs. 143 mL). However, there were no differences in the mean reduction of excess arm volume between the groups due to baseline differences in arm volumes in the two cohorts. In addition, there were no differences in the secondary outcomes and arm function.
Physical exercise
The results of randomized trials of physical exercise compared with usual care do not consistently demonstrate a benefit for patients with breast cancer and lymphedema. One study showed that women who underwent wide excision and axillary dissection and were randomly assigned to a supervised exercise program (3 hours per week for 12 weeks) reported fewer lymphedema-related symptoms than women assigned to a control group.[8][Level of evidence: I] The exercise group demonstrated greater reduction in extracellular fluid, as assessed with bioimpedance spectroscopy, compared with the control group. There was no significant difference in dermal thickness of the breast, as assessed by ultrasound.
Based on promising results of a facility-based exercise intervention, one trial used a 2 x 2 factorial design to test a home-based exercise program, with or without a weight-loss intervention led by a dietitian.[9][Level of evidence: I] The investigators randomly assigned 351 eligible women into one of four groups: control (n = 90), exercise alone (n = 87), weight loss alone (n = 87), and combined exercise and weight loss (n = 87). All patients received compression garments and consultations with certified lymphedema therapists. Eligibility criteria included evidence of lymphedema by clinical exam or history of lymphedema more than 6 months after surgery, a BMI between 25 and 50, and the ability to exercise but no history of consistent exercising. The primary outcome was the percentage difference between affected and nonaffected limbs. Secondary outcomes included clinician evaluation, patient surveys, and rates of lymphedema exacerbation or cellulitis. There were no differences of note between the various groups in the outcomes. This result raises the possibility that home-based therapies are inferior to facility-based treatment. The role of weight loss, if any, remains to be further elucidated.
Lymph node transplantation
A randomized trial of microsurgical lymph node transplantation and compression-physiotherapy versus compression-physiotherapy alone was reported.[10][Level of evidence: I] The 18 patients who underwent surgery had a greater reduction in limb volume (57% vs. 18%), fewer infectious complications from the lymphedema, and improved symptoms and functional status, compared with patients who received only compression-physiotherapy. The authors estimated that the procedure was cost effective when accounting for the reduction in complications from lymphedema.
Cervical Cancer: Prevention of Lymphedema
One study enrolled 120 women with cervical cancer who underwent a laparoscopic radical hysterectomy with pelvic lymphadenectomy. Participants were randomly assigned to an education-alone intervention or a CDT intervention.[11][Level of evidence: I] The CDT consisted of training in manual lymphatic drainage, followed by self-administered manual lymphatic drainage at home, compression hosiery, and an aerobic exercise program. The interventions were initiated 7 to 10 days after surgery. Additional eligibility criteria included more than 20 lymph nodes removed or anticipated radiation therapy (both of which are risk factors for lower-extremity lymphedema after surgery for cervical cancer). The primary outcome was limb volume calculated from multiple circumference measurements. Secondary outcomes included patients’ self-reported symptoms related to lymphedema. After a follow-up of 1 year, 20 of 58 patients (24%) in the control arm and 8 of 59 (14%) in the CDT arm developed lymphedema (P = .008). The excess volume was less in the experimental arm as well. However, there were no differences in patient-reported symptoms or severity grading of the lymphedema. These promising results were supported by a smaller pilot study[12] and a retrospective review of a single-institution experience with women who developed lymphedema after treatment of a variety of gynecological cancers.[13]
Head and Neck Cancer: Treatment of Lymphedema
Systematic review
A systematic review examined publications related to lymphedema treatment in patients who had been treated for head and neck cancers.[14] The authors identified 23 primary studies, including 14 cohort studies, 7 case reports, and 2 randomized controlled trials. The interventions included manual lymphatic drainage, acupuncture, selenium supplementation, and liposuction.
CDT
A small randomized trial in patients with lymphedema after surgery for head and neck cancer assigned 21 patients to one of three groups: control (n = 7), CDT (n = 7), and home-based therapy (n = 7).[15] The patients who received home-based therapy were taught manual lymphatic drainage techniques. The patients who received CDT wore a compression face mask and received manual lymphatic drainage from a trained therapist; the time commitment was significant. Patients in the CDT group experienced greater volume reduction and no fibrotic complications. The small sample size and the time commitment required to receive CDT suggested the effect should be verified in a larger study before wider adoption.
Advanced pneumatic compression device
The shortage of trained lymphedema therapists and the inconvenience of multiple clinic visits have encouraged the development of a device patients can use at home. In a small randomized trial of such a device, patients were assigned to the device (n = 24) or a wait-list control (n = 25).[16] At 8 weeks, subjects in the active treatment arm reported less distressing symptoms, and repeat endoscopic exams revealed less edema, compared with the control subjects. Assessments of function were not changed. The authors noted that patients tended to use the device once daily rather than the prescribed twice daily. Further study is required.
Liposuction
There is a small randomized trial of submental liposuction in patients who complained of swelling after treatment of head and neck cancer. The ten patients who underwent liposuction reported greater improvements in personal appearance, compared with control subjects, at 6 months. No adverse effects from liposuction were reported.[17][Level of evidence: I]
Sarcoma of the Extremity: Prevention of Lymphedema
One study compared the incidence of lymphedema in a cohort of eight patients with thigh sarcoma, who had lymphatico-venous anastomoses performed in combination with resection of thigh soft-tissue tumors, with a historical cohort of 20 patients.[18] Only one of eight patients experienced lymphedema, compared with nine patients in the historical cohort. Patient self-reported symptoms were uncommon in the eight patients.
References
Paramanandam VS, Dylke E, Clark GM, et al.: Prophylactic Use of Compression Sleeves Reduces the Incidence of Arm Swelling in Women at High Risk of Breast Cancer-Related Lymphedema: A Randomized Controlled Trial. J Clin Oncol 40 (18): 2004-2012, 2022. [PUBMED Abstract]
Schmitz KH, Ahmed RL, Troxel AB, et al.: Weight lifting for women at risk for breast cancer-related lymphedema: a randomized trial. JAMA 304 (24): 2699-705, 2010. [PUBMED Abstract]
Paskett ED, Le-Rademacher J, Oliveri JM, et al.: A randomized study to prevent lymphedema in women treated for breast cancer: CALGB 70305 (Alliance). Cancer 127 (2): 291-299, 2021. [PUBMED Abstract]
Naughton MJ, Liu H, Seisler DK, et al.: Health-related quality of life outcomes for the LEAP study-CALGB 70305 (Alliance): A lymphedema prevention intervention trial for newly diagnosed breast cancer patients. Cancer 127 (2): 300-309, 2021. [PUBMED Abstract]
Devoogdt N, Geraerts I, Van Kampen M, et al.: Manual lymph drainage may not have a preventive effect on the development of breast cancer-related lymphoedema in the long term: a randomised trial. J Physiother 64 (4): 245-254, 2018. [PUBMED Abstract]
Blom KY, Johansson KI, Nilsson-Wikmar LB, et al.: Early intervention with compression garments prevents progression in mild breast cancer-related arm lymphedema: a randomized controlled trial. Acta Oncol 61 (7): 897-905, 2022. [PUBMED Abstract]
Dayes IS, Whelan TJ, Julian JA, et al.: Randomized trial of decongestive lymphatic therapy for the treatment of lymphedema in women with breast cancer. J Clin Oncol 31 (30): 3758-63, 2013. [PUBMED Abstract]
Kilbreath SL, Ward LC, Davis GM, et al.: Reduction of breast lymphoedema secondary to breast cancer: a randomised controlled exercise trial. Breast Cancer Res Treat 184 (2): 459-467, 2020. [PUBMED Abstract]
Schmitz KH, Troxel AB, Dean LT, et al.: Effect of Home-Based Exercise and Weight Loss Programs on Breast Cancer-Related Lymphedema Outcomes Among Overweight Breast Cancer Survivors: The WISER Survivor Randomized Clinical Trial. JAMA Oncol 5 (11): 1605-1613, 2019. [PUBMED Abstract]
Dionyssiou D, Demiri E, Tsimponis A, et al.: A randomized control study of treating secondary stage II breast cancer-related lymphoedema with free lymph node transfer. Breast Cancer Res Treat 156 (1): 73-9, 2016. [PUBMED Abstract]
Wang X, Ding Y, Cai HY, et al.: Effectiveness of modified complex decongestive physiotherapy for preventing lower extremity lymphedema after radical surgery for cervical cancer: a randomized controlled trial. Int J Gynecol Cancer 30 (6): 757-763, 2020. [PUBMED Abstract]
Shallwani SM, Towers A, Newman A, et al.: Feasibility of a Pilot Randomized Controlled Trial Examining a Multidimensional Intervention in Women with Gynecological Cancer at Risk of Lymphedema. Curr Oncol 28 (1): 455-470, 2021. [PUBMED Abstract]
Liao SF, Li SH, Huang HY: The efficacy of complex decongestive physiotherapy (CDP) and predictive factors of response to CDP in lower limb lymphedema (LLL) after pelvic cancer treatment. Gynecol Oncol 125 (3): 712-5, 2012. [PUBMED Abstract]
Tyker A, Franco J, Massa ST, et al.: Treatment for lymphedema following head and neck cancer therapy: A systematic review. Am J Otolaryngol 40 (5): 761-769, 2019. [PUBMED Abstract]
Ozdemir K, Keser I, Duzlu M, et al.: The Effects of Clinical and Home-based Physiotherapy Programs in Secondary Head and Neck Lymphedema. Laryngoscope 131 (5): E1550-E1557, 2021. [PUBMED Abstract]
Ridner SH, Dietrich MS, Deng J, et al.: Advanced pneumatic compression for treatment of lymphedema of the head and neck: a randomized wait-list controlled trial. Support Care Cancer 29 (2): 795-803, 2021. [PUBMED Abstract]
Alamoudi U, Taylor B, MacKay C, et al.: Submental liposuction for the management of lymphedema following head and neck cancer treatment: a randomized controlled trial. J Otolaryngol Head Neck Surg 47 (1): 22, 2018. [PUBMED Abstract]
Wagner JM, Dadras M, Ufton D, et al.: Prophylactic lymphaticovenous anastomoses for resection of soft tissue tumors of the thigh to prevent secondary lymphedema-a retrospective comparative cohort analysis. Microsurgery 42 (3): 239-245, 2022. [PUBMED Abstract]
Latest Updates to This Summary (12/18/2024)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the diagnosis and treatment of lymphedema. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Lymphedema are:
Larry D. Cripe, MD (Indiana University School of Medicine)
James T. Pastrnak, MD (Indiana University School of Medicine)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Lymphedema. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/lymphedema/lymphedema-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389244]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Patients with cancer often have comorbid medical problems. Patients older than 65 years bear a disproportionate burden of cancer as well as increased prevalence of medical problems such as chronic obstructive pulmonary disease, heart disease, diabetes, and hypertension.[1] In both primary care and cancer care settings, unexplained symptoms often frustrate physicians and patients.[2] Because many advanced cancers spread to the thorax, symptoms such as dyspnea, cough, chest pain, and palpitations are common. Sorting out the likely cause of these problems and developing appropriate interventions can be difficult. Evidence-based recommendations describing various approaches to cancer-related fatigue, anorexia, depression, and dyspnea have been published.[3] Cancer patients are also often at higher risk of developing pulmonary infections.
Clinicians caring for cancer patients should be familiar with the assessment and treatment of common conditions that manifest as chest symptoms. In addition, these clinicians need to be familiar with some cancer-specific aspects of chest symptoms and syndromes. Dyspnea is a common symptom of certain cancers such as lung cancer and is also common in patients with numerous advanced cancers. Dyspnea is often multifactorial. Optimal treatment requires an understanding of contributing etiologies and pathophysiologies to direct therapeutic interventions as clinically appropriate.
Important cardiopulmonary syndromes include the following:
Malignant pleural effusion.
Malignant pericardial effusion.
Superior vena cava syndrome.
Lymphangitic carcinomatosis.
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
References
Yancik R, Ganz PA, Varricchio CG, et al.: Perspectives on comorbidity and cancer in older patients: approaches to expand the knowledge base. J Clin Oncol 19 (4): 1147-51, 2001. [PUBMED Abstract]
Komaroff AL: Symptoms: in the head or in the brain? Ann Intern Med 134 (9 Pt 1): 783-5, 2001. [PUBMED Abstract]
Dy SM, Lorenz KA, Naeim A, et al.: Evidence-based recommendations for cancer fatigue, anorexia, depression, and dyspnea. J Clin Oncol 26 (23): 3886-95, 2008. [PUBMED Abstract]
Dyspnea in Patients With Advanced Cancer
Introduction
Dyspnea is an uncomfortable awareness of breathing. It is a subjective experience involving many factors that affect the quality and intensity of its perception. Patients with comparable degrees of functional lung impairment and disease burden may describe varying intensities of dyspnea, using various words and phrases such as “tightness” and “suffocating.”[1]
Reports on the frequency of dyspnea also vary, depending on the setting and the extent of disease.[2] In one study, 49% of a general cancer population reported breathlessness, and 20% rated their breathlessness as moderate to severe.[3] Patients with advanced cancer experience dyspnea more frequently and more intensely than patients with limited disease. One study found that 75 of 135 patients with advanced cancer reporting to an outpatient palliative care clinic had moderate-to-severe dyspnea.[4] In addition, 60% of 289 patients with lung cancer reported breathlessness at presentation.[5] Results of a large study showed that 70% of patients suffered from dyspnea in the last 6 weeks of life.[6] About one-third of patients who could report the intensity of their dyspnea rated it as moderate to severe. Another study revealed that one-half of patients with advanced cancer scored their dyspnea as moderate to severe.[7]
Pathophysiology and Etiology
The pathophysiological mechanisms of breathlessness are numerous and complex.[8] Peripheral and central mechanisms, as well as mechanical and chemical pathways, are involved with a variety of sensory afferent sources.[9–11]
The qualities of dyspnea can be seen as work/effort, tightness, and air hunger. The experience of excess work/effort is caused by sensory-perceptual mechanisms similar to those involved in muscles exercising. Tightness is caused by stimulation of airway receptors with bronchoconstriction. The intensity of air hunger and unsatisfied inspiration is caused by the following:[12]
Imbalances of respiratory drive.
Outgoing signals from the brain.
Feedback from afferents in the respiratory system.
Dyspnea in patients with advanced cancer has many possible direct causes, and categorizing them can assist in the etiologic work-up. One approach is to divide direct causes into the following groups:
Direct tumor effects such as intrinsic or extrinsic airway obstruction, pleural involvement, parenchymal involvement by either primary or metastatic disease, superior vena cava syndrome, lymphangitic carcinomatosis, pericardial effusion, and postobstructive pneumonitis.
Indirect tumor effects such as pneumonia, a pulmonary embolus, paralysis of a hemidiaphragm, or weakening of the respiratory muscles from sarcopenia.
Treatment-related causes such as pulmonary fibrosis secondary to radiation therapy or chemotherapy, chemotherapy-induced cardiomyopathy, and immunotherapy-related pneumonitis from targeted therapy. Although uncommon, checkpoint inhibitor immunotherapy–related pneumonitis can be potentially severe or fatal.[13,14] This drug-induced pneumonitis is a diagnosis of exclusion; other differential diagnoses, including infection and worsening malignancy, need to be excluded.
Causes unrelated to cancer include chronic obstructive airway disease, congestive heart failure, anemia, certain acidotic states, and bronchospasm.
Functional causes (e.g., anxiety).
One study found that in patients experiencing dyspnea from advanced cancer, a median of five different abnormalities could have contributed to their shortness of breath.[7] Spirometry was abnormal in 93% of 100 patients examined, with 5% having obstructive patterns, 41% restrictive patterns, and 47% mixed patterns. Also, 49% of patients had lung cancer, 91% had abnormal chest radiographs, and 65% had parenchymal or pleural involvement. These results show that a subset of patients experience shortness of breath without any apparent lung involvement. The potentially correctable causes of dyspnea included:
Hypoxia (40%).
Anemia (20%).
Bronchospasm (52%).
No significant association between the type of respiratory impairment and the degree of dyspnea was found. Most of these patients were current or former smokers and had a significant lowering of their maximum inspiratory pressures, suggesting severe respiratory muscle dysfunction.[7] This finding was duplicated in another study.[4] Of patients admitted to hospice care, 34% had histories of cardiac disease, and 24% had histories of respiratory disease.[6] Only 39% of terminally ill patients who reported dyspnea had lung or pleural involvement. The etiology of dyspnea could not be clearly identified in approximately one-quarter of patients. Another study found that 49% of lung cancer patients presented with airflow obstruction.[7,15]
Respiratory muscle dysfunction is an underrecognized factor contributing to dyspnea. Causes of respiratory muscle dysfunction include:[16]
Neuromuscular disease.
Malnutrition.
Deficiencies of potassium, magnesium, and inorganic phosphate.
Poor oxygenation, muscle fatigue, abnormal cortisol and catecholamine levels, and circulating cytokines are also implicated.[16]
Although anxiety is commonly thought to be associated with breathlessness, researchers have found that anxiety and shortness of breath do not invariably go together.[7] One study demonstrated that the involvement of the lungs by cancer, anxiety, and poor maximal inspiratory pressures were correlates of the intensity of dyspnea in patients with advanced cancer.[4]
Assessment
The multidimensional nature of dyspnea must be noted in the complicated assessment of this symptom. Patient-reported outcome is the gold standard for assessment of dyspnea. There is no consensus on the best instrument for assessing dyspnea, but some of the tools used include:
Visual analog and numerical rating scales, which are commonly used.[8,17–19]
Cancer Dyspnea Scale, a multidimensional instrument that has been shown to be valid and reliable in patients with advanced lung cancer. The subscales measure sense of effort (physical dimension), sense of anxiety (psychological dimension), and sense of discomfort.[20]
These tools are limited, however, because they are unidimensional and do not account for the relative contribution of different factors to a patient’s perception of breathlessness. Assessment should include the impact of dyspnea on the patient’s functional status and recognition of the dynamic component of dyspnea—namely, exertional dyspnea.
Objective signs, such as tachypnea or the use of accessory breathing muscles, frequently do not match a patient’s perception of dyspnea and the degree of functional impairment it causes. Numerous factors, including psychosocial issues, may affect a patient’s experience of dyspnea. Pulmonary function tests, with few exceptions, play a limited role in the assessment of this syndrome.
A comprehensive history and examination are essential to an accurate assessment of dyspnea.[8,17] The temporal onset, qualities of the symptom, associated symptoms, precipitating and relieving events or activities, and responses to medications should be reviewed. Sudden onset may herald a pulmonary embolism or infection, whereas gradual onset may suggest development of a pleural effusion. A history of obstructive airways or cardiac disease can shed some light on possible underlying causes. Investigations such as measuring oxygen saturation can be useful in determining whether a patient is hypoxic. In the setting of advanced, incurable cancer, arterial blood gasses play a limited role.
In the study looking at checkpoint inhibitor immunotherapy–related pneumonitis, one-third of patients were asymptomatic. However, the most common presenting symptoms were dyspnea (53%) and cough (35%).[13]
Melanoma and non-small cell lung cancer were the most common cancers treated in this study. Interestingly, the duration of treatment before the onset of pneumonitis was quite variable, with a median time to onset of 2.8 months (range, 9 days–19 months). In addition, pneumonitis seemed to occur earlier in patients who received combination therapy than in those who received monotherapy (median, 2.7 months vs. 4.6 months).[13]
Diagnostic tests that may help to determine the etiology of dyspnea include the following:[7]
Chest imaging by radiography.
Computed tomography.
Complete blood counts.
Oxygen saturation at rest and with exercise.
Pulmonary function tests, to a much lesser extent.
Maximal inspiratory pressure (MIP) measurements may be helpful, particularly if no apparent cause can be found. MIP is a reliable functional test of the strength of the diaphragm and other respiratory muscles. Functional assessments such as the 6-minute walk test and exercise ergometry may also provide valuable information about the severity and impact of dyspnea.[21,22]
Management of Dyspnea
Management of underlying causes
Lack of a clear understanding of the pathophysiological mechanisms underlying dyspnea hampers the clinician’s overall ability to effectively manage it.[8,17] As with all symptoms, it is essential to identify and treat the underlying cause(s) of dyspnea, if possible and when appropriate. Underlying causes (some of them potentially reversible) and their treatments include the following:
Tumor obstruction (upper airways, bronchus, postobstructive pneumonitis, or superior vena cava): Radiation therapy, hormone therapy, or chemotherapy for sensitive tumors. Bronchoscope-guided cauterization or laser ablation of intraluminal masses in large airways can be considered when such technology and expertise are available.[23]
Carcinomatous lymphangitis: A trial of corticosteroids, e.g., dexamethasone. The optimal dose is not clear. Chemotherapy should be considered in sensitive cancers.
Superior vena cava obstruction: Chemotherapy for sensitive tumors, radiation therapy, stenting, opioids for dyspnea, and/or steroids as appropriate for the clinical context.
Bronchospasms: Bronchodilators. The indiscriminate use of bronchodilators, particularly in the absence of bronchospasm, is discouraged. The treatment of underlying chronic obstructive disease should be optimized with bronchodilators and inhaled corticosteroids as appropriate, particularly because many patients may be current or former smokers.
Postradiation bronchiolitis obliterans: A rare complication that occurs in 0.8% to 2.9% of women receiving radiation therapy for breast cancer.[24] Patients are usually treated with corticosteroids.
Pleural effusions: Pleural aspiration by thoracentesis or chest drain. Pleurodesis in selected patients with recurrent effusions should be considered. Indwelling catheters are available for patients with recurrent effusions who are not suitable for pleurodesis.
Pericardial effusions: Drainage for immediate relief and possibly intrapericardial chemotherapy or definitive surgery, depending on the clinical context and goals of care.
Gross ascites: Abdominal paracentesis to relieve diaphragmatic splinting.
Cardiac failure: Diuretics and other drugs as appropriate.
Chest infections: Antibiotics and chest physiotherapy when appropriate.
Anemia: Blood transfusions in select patients.
Pulmonary embolism: Anticoagulate when appropriate.
Checkpoint inhibitor immunotherapy–related pneumonitis: For patients with a severity of grade 2 or higher (based on the National Cancer Institute Common Terminology Criteria for Adverse Events [25]), withholding of drug treatment, administration of corticosteroids, and close follow-up. If pneumonitis worsens, additional immunosuppression may be considered, though its benefit is not clear.
Anxiety: Psychotropic medications and psychotherapy.
Symptomatic management
Symptomatic management of dyspnea is based primarily on the following:
Oxygen therapy.
Opioids for palliation of dyspnea.
Treatment of underlying causes (e.g., superimposed infection), when appropriate.
Opioids are an extremely effective treatment for dyspnea in cancer patients, and fear of side effects should not prevent their appropriate use. Most authorities believe that, if used appropriately, opioids do not hasten death in dyspneic cancer patients; rather, they reduce physical and psychological distress and exhaustion, and early use improves quality of life.[17,26,27] Clinically significant hypoventilation after opioid therapy depends largely on the history of previous exposure to opioids and the rate of increase of the opioid dose. As with opioid use in pain management, starting at a regular low dose in opioid-naïve patients, followed by appropriate dose titration, is advised. Opioid therapy for dyspnea is administered similarly to, and often concurrent with, opioid therapy for pain control. Most of the evidence supports the role of opioids in relieving dyspnea in malignant and nonmalignant conditions.[28,29][Level of evidence: I];[30–32][Level of evidence: II]
Anecdotal and experimental evidence suggest a role for nebulized opioid administration in the treatment of dyspnea.[33–35] Opioid receptors are present on sensory nerve endings in the airways; however, nebulization is an inefficient way of administering drugs.[33] Pharmacokinetic studies suggest that the systemic bioavailability of nebulized morphine is extremely poor and erratic, varying from 4% to 8%.[36] Some patients may experience claustrophobia. The evidence does not support the clinical use of nebulized opioids. More clinical trials are needed to better determine the role of this mode of treatment.
Patients who are hypoxic in room air are likely to benefit from oxygen therapy, probably through a decrease in the chemoreceptor input to the respiratory center and the brain cortex. In two controlled trials, cancer patients with dyspnea who were randomly assigned to oxygen therapy in a crossover design showed significant improvement in their dyspnea.[37,38][Level of evidence: I] The role of supplemental oxygen has also been examined in patients without hypoxemia in a large randomized controlled trial. Supplemental oxygen given at 2 L/min did not significantly improve dyspnea, compared with supplemental air.[39] Therefore, supplemental oxygen is recommended for cancer patients with hypoxemia but not for those without hypoxemia.
Other investigators have examined the effect of other oxygen delivery modalities on dyspnea in cancer patients, such as:[40]
High-flow oxygen. High-flow oxygen devices deliver up to 40 L of humidified and heated oxygen per minute, and may reduce the intensity of dyspnea in patients who do not respond to low-flow oxygen.[40]
Noninvasive ventilation with bilevel positive airway pressure (BiPAP). BiPAP has been shown in several randomized controlled trials to alleviate dyspnea among hospitalized cancer patients,[40,41] particularly in patients with hypoventilation.
These interventions may be reasonable options for patients with hypoxemia and refractory dyspnea despite the use of low-flow supplemental oxygen.
Other options for symptomatic treatment include:
Methylxanthines.
Sedatives.
Tranquilizers.
Nebulized local anesthetics.
Antiprostaglandins.
The role of methylxanthines in cancer-related dyspnea is unclear. Chlorpromazine and promethazine have been shown to decrease dyspnea without affecting ventilation in patients without cancer, but their role in cancer-related dyspnea is uncertain. Four out of five randomized controlled trials failed to show any benefit for using benzodiazepines in cancer patients.[17];[42][Level of evidence: I]
One randomized single-blind study suggested that the combination of two scheduled medications (subcutaneous morphine and subcutaneous midazolam) and one as needed (subcutaneous morphine) for episodes of breakthrough dyspnea is more effective than the other evaluated combinations, but this approach requires further study.[43][Level of evidence: I]
The role of benzodiazepines appears to be limited to treatment of dyspnea that is a somatic manifestation of a panic disorder or that is concurrent with severe anxiety. In a randomized placebo-controlled trial of 432 cancer patients with moderate-to-severe dyspnea, 20 mg of buspirone, a nonbenzodiazepine anxiolytic drug, did not improve dyspnea or anxiety, compared with placebo.[44][Level of evidence: I] Buspirone cannot be recommended at this time for the treatment of dyspnea in cancer patients. No evidence supports the use of nebulized local anesthetics for the treatment of breathlessness.
Given the role inflammation may play in cancer and dyspnea, dexamethasone has been used for symptomatic treatment of dyspnea. A randomized controlled trial prospectively evaluated dexamethasone in a highly selected group of ambulatory patients who had an average dyspnea score of 4 or greater (on a numerical scale of 0–10).[45][Level of evidence: I] Patients were randomly assigned to receive dexamethasone 8 mg bid for 1 week, then 4 mg bid for 1 week versus a matching placebo. In-person assessments were taken at baseline, day 7, and day 14, as well as telephone assessments every other day from day 1 to day 28. Assessments included average dyspnea intensity, activity-adjusted dyspnea, and dyspnea unpleasantness via a numerical rating scale. Dyspnea was also measured via maximal inspiratory pressure and spirometry. The trial was terminated at the second preplanned interim analysis for futility. A clinically meaningful improvement in dyspnea was seen in both the placebo and the dexamethasone groups, leading to the conclusion that high-dose dexamethasone should not be given routinely to alleviate cancer-related dyspnea. Interestingly, the patients who took dexamethasone had significantly better appetite and well-being scores but worse anxiety, depression, and adverse events.
General support measures
In addition to pharmacological therapies, a number of nonpharmacological measures are suggested for the treatment of dyspnea. These measures include:
Pursed-lip breathing.
Diaphragmatic breathing and muscle training.
Cold air directed across the cheek.
Meditation.
Relaxation training.
Biofeedback techniques.
Psychotherapy.
The effectiveness of these measures in relieving breathlessness appears to be variable.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Wilcock A, Crosby V, Hughes A, et al.: Descriptors of breathlessness in patients with cancer and other cardiorespiratory diseases. J Pain Symptom Manage 23 (3): 182-9, 2002. [PUBMED Abstract]
Ripamonti C, Fulfaro F, Bruera E: Dyspnoea in patients with advanced cancer: incidence, causes and treatments. Cancer Treat Rev 24 (1): 69-80, 1998. [PUBMED Abstract]
Dudgeon DJ, Kristjanson L, Sloan JA, et al.: Dyspnea in cancer patients: prevalence and associated factors. J Pain Symptom Manage 21 (2): 95-102, 2001. [PUBMED Abstract]
Bruera E, Schmitz B, Pither J, et al.: The frequency and correlates of dyspnea in patients with advanced cancer. J Pain Symptom Manage 19 (5): 357-62, 2000. [PUBMED Abstract]
Muers MF, Round CE: Palliation of symptoms in non-small cell lung cancer: a study by the Yorkshire Regional Cancer Organisation Thoracic Group. Thorax 48 (4): 339-43, 1993. [PUBMED Abstract]
Reuben DB, Mor V: Dyspnea in terminally ill cancer patients. Chest 89 (2): 234-6, 1986. [PUBMED Abstract]
Dudgeon DJ, Lertzman M: Dyspnea in the advanced cancer patient. J Pain Symptom Manage 16 (4): 212-9, 1998. [PUBMED Abstract]
Parshall MB, Schwartzstein RM, Adams L, et al.: An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med 185 (4): 435-52, 2012. [PUBMED Abstract]
Naidoo J, Wang X, Woo KM, et al.: Pneumonitis in Patients Treated With Anti-Programmed Death-1/Programmed Death Ligand 1 Therapy. J Clin Oncol 35 (7): 709-717, 2017. [PUBMED Abstract]
Khunger M, Rakshit S, Pasupuleti V, et al.: Incidence of Pneumonitis With Use of Programmed Death 1 and Programmed Death-Ligand 1 Inhibitors in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Trials. Chest 152 (2): 271-281, 2017. [PUBMED Abstract]
Congleton J, Muers MF: The incidence of airflow obstruction in bronchial carcinoma, its relation to breathlessness, and response to bronchodilator therapy. Respir Med 89 (4): 291-6, 1995. [PUBMED Abstract]
Mancini DM, LaManca J, Henson D: The relation of respiratory muscle function to dyspnea in patients with heart failure. Heart Fail 8: 183-9, 1992.
Dudgeon DJ, Rosenthal S: Management of dyspnea and cough in patients with cancer. Hematol Oncol Clin North Am 10 (1): 157-71, 1996. [PUBMED Abstract]
Bausewein C, Farquhar M, Booth S, et al.: Measurement of breathlessness in advanced disease: a systematic review. Respir Med 101 (3): 399-410, 2007. [PUBMED Abstract]
Dorman S, Byrne A, Edwards A: Which measurement scales should we use to measure breathlessness in palliative care? A systematic review. Palliat Med 21 (3): 177-91, 2007. [PUBMED Abstract]
Henoch I, Bergman B, Gaston-Johansson F: Validation of a Swedish version of the Cancer Dyspnea Scale. J Pain Symptom Manage 31 (4): 353-61, 2006. [PUBMED Abstract]
American Thoracic Society, American College of Chest Physicians: ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 167 (2): 211-77, 2003. [PUBMED Abstract]
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories: ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 166 (1): 111-7, 2002. [PUBMED Abstract]
Mantovani G, Astara G, Manca G, et al.: Endoscopic laser ablation as palliative treatment of endobronchial, nonresectable, or recurrent lung cancer: assessment of its impact on quality of life. Clin Lung Cancer 1 (4): 277-85; discussion 286, 2000. [PUBMED Abstract]
Epler GR, Kelly EM: Systematic review of postradiotherapy bronchiolitis obliterans organizing pneumonia in women with breast cancer. Oncologist 19 (12): 1216-26, 2014. [PUBMED Abstract]
National Cancer Institute: Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Bethesda, Md: U.S. Department of Health and Human Services, National Institutes of Health, 2017. Available online. Last accessed Dec. 18, 2024.
Bruera E, Ripamonti C: Dyspnea in patients with advanced cancer. In: Berger A, Portenoy RK, Weissman DE, eds.: Principles and Practice of Supportive Oncology. Lippincott-Raven Publishers, 1998, pp 295-307.
Kloke M, Cherny N; ESMO Guidelines Committee: Treatment of dyspnoea in advanced cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol 26 (Suppl 5): v169-73, 2015. [PUBMED Abstract]
Bruera E, MacEachern T, Ripamonti C, et al.: Subcutaneous morphine for dyspnea in cancer patients. Ann Intern Med 119 (9): 906-7, 1993. [PUBMED Abstract]
Allard P, Lamontagne C, Bernard P, et al.: How effective are supplementary doses of opioids for dyspnea in terminally ill cancer patients? A randomized continuous sequential clinical trial. J Pain Symptom Manage 17 (4): 256-65, 1999. [PUBMED Abstract]
Bruera E, Macmillan K, Pither J, et al.: Effects of morphine on the dyspnea of terminal cancer patients. J Pain Symptom Manage 5 (6): 341-4, 1990. [PUBMED Abstract]
Cohen MH, Anderson AJ, Krasnow SH, et al.: Continuous intravenous infusion of morphine for severe dyspnea. South Med J 84 (2): 229-34, 1991. [PUBMED Abstract]
Boyd KJ, Kelly M: Oral morphine as symptomatic treatment of dyspnoea in patients with advanced cancer. Palliat Med 11 (4): 277-81, 1997. [PUBMED Abstract]
Zeppetella G: Nebulized morphine in the palliation of dyspnoea. Palliat Med 11 (4): 267-75, 1997. [PUBMED Abstract]
Farncombe M, Chater S: Clinical application of nebulized opioids for treatment of dyspnoea in patients with malignant disease. Support Care Cancer 2 (3): 184-7, 1994. [PUBMED Abstract]
Farncombe M, Chater S, Gillin A: The use of nebulized opioids for breathlessness: a chart review. Palliat Med 8 (4): 306-12, 1994. [PUBMED Abstract]
Masood AR, Thomas SH: Systemic absorption of nebulized morphine compared with oral morphine in healthy subjects. Br J Clin Pharmacol 41 (3): 250-2, 1996. [PUBMED Abstract]
Bruera E, de Stoutz N, Velasco-Leiva A, et al.: Effects of oxygen on dyspnoea in hypoxaemic terminal-cancer patients. Lancet 342 (8862): 13-4, 1993. [PUBMED Abstract]
Bruera E, Schoeller T, MacEachern T: Symptomatic benefit of supplemental oxygen in hypoxemic patients with terminal cancer: the use of the N of 1 randomized controlled trial. J Pain Symptom Manage 7 (6): 365-8, 1992. [PUBMED Abstract]
Abernethy AP, McDonald CF, Frith PA, et al.: Effect of palliative oxygen versus room air in relief of breathlessness in patients with refractory dyspnoea: a double-blind, randomised controlled trial. Lancet 376 (9743): 784-93, 2010. [PUBMED Abstract]
Hui D, Morgado M, Chisholm G, et al.: High-flow oxygen and bilevel positive airway pressure for persistent dyspnea in patients with advanced cancer: a phase II randomized trial. J Pain Symptom Manage 46 (4): 463-73, 2013. [PUBMED Abstract]
Nava S, Ferrer M, Esquinas A, et al.: Palliative use of non-invasive ventilation in end-of-life patients with solid tumours: a randomised feasibility trial. Lancet Oncol 14 (3): 219-27, 2013. [PUBMED Abstract]
Moroni M, Porta C, Gualtieri G, et al.: Inhaled sodium cromoglycate to treat cough in advanced lung cancer patients. Br J Cancer 74 (2): 309-11, 1996. [PUBMED Abstract]
Navigante AH, Cerchietti LC, Castro MA, et al.: Midazolam as adjunct therapy to morphine in the alleviation of severe dyspnea perception in patients with advanced cancer. J Pain Symptom Manage 31 (1): 38-47, 2006. [PUBMED Abstract]
Peoples AR, Bushunow PW, Garland SN, et al.: Buspirone for management of dyspnea in cancer patients receiving chemotherapy: a randomized placebo-controlled URCC CCOP study. Support Care Cancer 24 (3): 1339-47, 2016. [PUBMED Abstract]
Hui D, Puac V, Shelal Z, et al.: Effect of dexamethasone on dyspnoea in patients with cancer (ABCD): a parallel-group, double-blind, randomised, controlled trial. Lancet Oncol 23 (10): 1321-1331, 2022. [PUBMED Abstract]
Chronic Cough
Chronic coughing may be the source of major suffering for some patients.[1] Chronic cough can:
Cause pain.
Interfere with sleep.
Aggravate dyspnea.
Worsen fatigue.
The causes of cough can be classified much like the causes of dyspnea.
For chronic cough in patients receiving palliative care, consider the following differential diagnoses:
Malignancy-related causes of cough, e.g., direct irritation by the presence of a tumor or tracheo-esophageal fistula.
Drug-related cough: rule out cough induced by medications such as angiotensin-converting enzyme inhibitors.
Other noncancer causes of cough: rule out asthma, chronic obstructive pulmonary disease, postnasal drip, reflux issues, and chronic heart failure.
The optimal therapy for chronic cough is treatment of the underlying disorder, such as:
Radiation therapy for the underlying endobronchial tumor mass irritating the airway.
Stenting of tracheo-esophageal fistula.
Drainage of a pleural effusion.
Corticosteroids for lymphangitic carcinomatosis.
Cough-suppressing agents such as opioids are commonly used. Anecdotal evidence suggests a role for inhaled local anesthetics, which should be used judiciously and sparingly because of their unpleasant taste, suppression of the gag reflex, and anaphylactic reactions to preservatives in these solutions. Opioid and nonopioid antitussives, such as dextromethorphan, may act synergistically, but further studies are required to confirm this hypothesis.[1] Gabapentin was found to be efficacious compared with placebo for chronic refractory cough, although this study did not include cancer patients.[2]
In cases of increased sputum production, expectorants and mucolytics have been used, but the effects have not been well evaluated. Inhaled sodium cromoglycate has shown promise as a safe method of controlling chronic coughing related to lung cancer.[3]
References
Dudgeon DJ, Rosenthal S: Management of dyspnea and cough in patients with cancer. Hematol Oncol Clin North Am 10 (1): 157-71, 1996. [PUBMED Abstract]
Ryan NM, Birring SS, Gibson PG: Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet 380 (9853): 1583-9, 2012. [PUBMED Abstract]
Moroni M, Porta C, Gualtieri G, et al.: Inhaled sodium cromoglycate to treat cough in advanced lung cancer patients. Br J Cancer 74 (2): 309-11, 1996. [PUBMED Abstract]
Malignant Pleural Effusion
Significance
Malignant pleural effusions are a common complication of malignancy, and malignancy is a common cause of pleural effusions in general. Malignancy causes roughly 40% of symptomatic pleural effusions, with congestive heart failure and infection being the other leading causes.[1] The cancers that account for approximately 75% of all malignancy-associated effusions include the following:
Lung cancer.
Breast cancer.
Lymphoma.
Leukemia.
Significant use of health care resources is attributable to malignant effusions, with approximately 100,000 cases per year diagnosed in the United States and 43 cases detected per 100,000 hospital admissions.[2]
Pathogenesis
The normal pleural fluid space is occupied with approximately 10 mL of fluid with 2 g/dL protein. A pleural effusion is an accumulation of an abnormal amount of fluid between the visceral and parietal pleura of the chest. Normally, pleural fluid is absorbed by pulmonary venous capillaries (80%–90%), with some of it also absorbed by pleural lymphatics. Malignant effusions are usually exudative rather than transudative. Exudative effusions exhibit any one of the following characteristics:[3]
Pleural fluid to serum protein ratio greater than 0.5.
Pleural fluid to serum lactate dehydrogenase (LDH) ratio greater than 0.6.
Pleural fluid LDH greater than two-thirds of the upper limit of serum LDH.
These exudative malignant effusions are generally caused by:
Pleural metastases.
Disruption of pulmonary capillary endothelium.
Malignant obstruction of pleural lymphatics.
Paramalignant effusions may result from chemotherapy, radiation therapy, atelectasis, or lymph node involvement.
Assessment
Common symptoms associated with malignant pleural effusions include:
Dyspnea.
Cough.
Chest discomfort.
About 20% of patients may experience weight loss and malaise. A chest x-ray is most commonly used for radiographic assessment. About 175 mL of pleural fluid will cause a blunted costophrenic angle discernible on chest radiography. A chest computed tomography scan is more sensitive than a simple chest x-ray and is often used for assessment of loculated effusions because, in some instances, up to 500 mL of loculated fluid can be obscured behind the dome of the diaphragm.[1]
Not all pleural effusions detected in cancer patients are malignant effusions. Cancer patients are prone to developing conditions such as:[1]
Congestive heart failure.
Pneumonia.
Pulmonary embolism.
Malnutrition.
Associated low serum albumin.
Each of these conditions may cause a symptomatic effusion for which clinical management would substantially differ from management of a malignant effusion. For this reason, cytological assessment is important. Pleural fluid cytology requires a minimum sample of 250 mL. The morphology of cells obtained from the pleural space can be difficult to assess because of mesothelial and macrophage abnormalities. The diagnostic sensitivity of pleural fluid cytology is approximately 65%, with a specificity of 97%.[1]
Flow cytometry can be applied to these specimens and is often useful, especially for assessment of lymphomas.
Thoracoscopy and pleural biopsy are rarely needed for a definitive diagnosis, but these techniques may be useful when routine pleural fluid collection and assessment are difficult because of loculation of the effusion.
Thoracoscopy-guided biopsy is generally performed under local anesthesia and has a yield of more than 80%, with a lower risk of complications than thoracotomy.
Management of Malignant Pleural Effusions
To treat or not to treat
Pleural effusions are generally markers of advanced, unresectable disease or disease progression. The median survival for patients with malignant pleural effusions is around 3 to 4 months.[4,5] Because a paramalignant effusion resulting from pneumonia or atelectasis may be present, the cytology should be confirmed before making major treatment decisions. The management strategy depends on the underlying primary malignancy and the number and type of previous therapies. For example, patients with newly diagnosed small cell carcinoma or malignant lymphoma are likely to respond to systemic chemotherapy; however, patients with gastric or ovarian cancer in whom several lines of chemotherapy have failed are unlikely to obtain significant palliation with systemic therapy.
About three-quarters of patients exhibit symptoms such as cough, dyspnea, and chest discomfort. Such patients may benefit from efforts to reduce the fluid burden, depending on the following:
Their performance status.
Their expected survival.
Their preference for risks versus benefits.
The literature on the efficacy of treatment for pleural effusions is difficult to interpret because of the paucity of randomized trials, and wide variability in the response criteria and the timing and duration of follow-up in uncontrolled trials.[6,7] Generally, the goal of therapy is palliation of symptoms. Measures of success may include:
Complete drainage of the effusion.
Lung re-expansion.
Lack of fluid reaccumulation (i.e., duration of response).
Subjective report of symptom relief.
The choice of treatment depends on patient prognosis, functional status, and goals of care.
Thoracentesis
Thoracentesis involves percutaneous insertion of a needle for drainage of the effusion. Thoracentesis is not expected to permanently resolve the problem but rather to alleviate acute and severe symptoms. The use of thoracentesis is also appropriate as a therapeutic trial to determine whether fluid drainage is beneficial when the relationship between symptoms and effusion is unclear.
Most effusions will reaccumulate a few days after thoracentesis. The reaccumulation rate is approximately 98% by day 30.[8] Repeated thoracenteses carry the potential risks of bleeding, infection, and pneumothorax. Other potential complications of thoracentesis include noncardiogenic pulmonary edema from rapid lung re-expansion (usually with the rapid removal of >1,500 mL) and pleural shock caused by an excessive vagal response to penetration of the parietal pleura. Any of these complications may be lethal, especially for the cancer patient with poor cardiopulmonary reserve.
Indwelling pleural catheters (IPCs) represent an alternative to pleurodesis for patients with malignant pleural effusion whose dyspnea has responded to thoracentesis. IPCs are relatively contraindicated in patients with a short life expectancy, pleural infections, multiloculated collections, and chylothorax. The insertion of chronic long-term indwelling tunneled pleural catheters is useful to treat recurrent and symptomatic malignant pleural effusions, including for patients with trapped lung. These tunneled pleural catheters allow up to 96% of patients to achieve symptom improvement, with spontaneous pleurodesis occurring in up to 44% of patients.[9] Published results indicate significantly shorter hospital stays for patients with IPCs versus those receiving doxycycline pleurodesis (1 day vs. 6 days). In the IPC group, spontaneous pleurodesis was achieved in 42 of 91 patients. Both the IPC group and doxycycline pleurodesis group reported modest improvement in quality of life (QOL) and dyspnea.[10]
A randomized controlled trial comparing IPC and talc pleurodesis showed similar reduction of dyspnea (24 mm of 100 mm) and similar QOL.[11] IPC use was associated with a shorter initial hospitalization and lower rates of re-treatment, with a spontaneous pleurodesis rate of 51%. However, IPCs also had higher rates of adverse effects, such as infections and catheter blockage. A second randomized controlled trial compared the effect of IPC versus talc pleurodesis on the total number of hospitalization days from procedure to death or to 12 months.[12] There was a statistically significant reduction in the number of hospitalization days for patients with IPCs compared with those who received talc pleurodesis (median,10 days [interquartile range (IQR), 3–17] vs. 12 days [IQR, 7–21], respectively; P = .03). IPC use also resulted in fewer hospitalization days related to pleural effusion management and fewer additional invasive pleural drainage procedures. There were no significant differences in improvement in breathlessness or QOL between the two procedures. The choice between IPC and pleurodesis should be based on patient preference and local resource availability.
Use of pleural sclerosing agents after chest tube drainage
Chemical sclerosants may be administered through a chest tube to create inflammation and subsequent fusion of the parietal and visceral pleura so that fluid cannot reaccumulate in this potential space. Numerous chemical agents can cause the irritation necessary to produce this kind of fusion, called pleurodesis. The ideal agent would produce effective pleurodesis with minimal cost and minimal side effects. Agents that have been studied include:
Several uncontrolled trials and case series have reported the efficacy of pleurodesis,[14];[15,16][Level of evidence: II];[17,18] as have numerous randomized trials.[19–25][Level of evidence: I] A meta-analysis of pleurodesis studies that were reported between 1966 and 1992 indicated that about two-thirds of patients responded to pleurodesis, and that the most effective agents appeared to be tetracyclines (or tetracycline replacement agents, such as doxycycline and minocycline), bleomycin, and talc.[26]
A prospective, randomized study of video-assisted thoracoscopic pleurodesis with talc versus doxycycline in 33 patients with malignant pleural effusion suggested that talc provides superior short-term and long-term results.[27][Level of evidence: I] Talc appears to be the least expensive agent, at least when given as a slurry rather than by video-assisted thoracoscopic talc insufflation.[25][Level of evidence: I] However, bleomycin is the only agent approved by the U.S. Food and Drug Administration for the prevention of recurrent pleural effusions.[1] An observational cohort study investigated the use of intrapleural urokinase in 48 patients with loculated pleural effusions or trapped lungs. Lung reexpansion and resolution of dyspnea occurred in approximately 60% of patients, suggesting that intrapleural urokinase may be useful in treating loculated pleural effusions or trapped lungs in medically inoperable patients with cancer. Most responders maintained pleurodesis when urokinase was followed by minocycline pleurodesis.[28][Level of evidence: II]
Surgical treatment
For rare patients, standard management of the malignant effusion is unsuccessful and aggressive treatment remains appropriate. Pleuroperitoneal shunting can be considered for these patients. This procedure involves implantation of a shunt with one-way valves that allow the transfer of fluid from the pleural space to the peritoneal space, in which the fluid creates less hazard and is more easily removed. Another option is surgical pleurectomy, which requires general anesthesia. The risk of significant acute and chronic pain as well as other morbidity approaches 20% to 25%, and the risk of mortality at 1 month is 5% to 10%.[2]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Maghfoor I, Doll DC, Yarbro JW: Effusions. In: Abeloff MD, Armitage JO, Lichter AS, et al., eds.: Clinical Oncology. Churchill Livingstone, 2000, pp 922-49.
Fiocco M, Krasna MJ: The management of malignant pleural and pericardial effusions. Hematol Oncol Clin North Am 11 (2): 253-65, 1997. [PUBMED Abstract]
Light RW: Useful tests on the pleural fluid in the management of patients with pleural effusions. Curr Opin Pulm Med 5 (4): 245-9, 1999. [PUBMED Abstract]
Burrows CM, Mathews WC, Colt HG: Predicting survival in patients with recurrent symptomatic malignant pleural effusions: an assessment of the prognostic values of physiologic, morphologic, and quality of life measures of extent of disease. Chest 117 (1): 73-8, 2000. [PUBMED Abstract]
Sahn SA: Malignant pleural effusions. Semin Respir Crit Care Med 22 (6): 607-16, 2001. [PUBMED Abstract]
Tattersall M: Management of malignant pleural effusion. Aust N Z J Med 28 (3): 394-6, 1998. [PUBMED Abstract]
Schafers SJ, Dresler CM: Update on talc, bleomycin, and the tetracyclines in the treatment of malignant pleural effusions. Pharmacotherapy 15 (2): 228-35, 1995 Mar-Apr. [PUBMED Abstract]
Anderson CB, Philpott GW, Ferguson TB: The treatment of malignant pleural effusions. Cancer 33 (4): 916-22, 1974. [PUBMED Abstract]
Tremblay A, Michaud G: Single-center experience with 250 tunnelled pleural catheter insertions for malignant pleural effusion. Chest 129 (2): 362-8, 2006. [PUBMED Abstract]
Putnam JB, Light RW, Rodriguez RM, et al.: A randomized comparison of indwelling pleural catheter and doxycycline pleurodesis in the management of malignant pleural effusions. Cancer 86 (10): 1992-9, 1999. [PUBMED Abstract]
Davies HE, Mishra EK, Kahan BC, et al.: Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA 307 (22): 2383-9, 2012. [PUBMED Abstract]
Thomas R, Fysh ETH, Smith NA, et al.: Effect of an Indwelling Pleural Catheter vs Talc Pleurodesis on Hospitalization Days in Patients With Malignant Pleural Effusion: The AMPLE Randomized Clinical Trial. JAMA 318 (19): 1903-1912, 2017. [PUBMED Abstract]
Akopov AL, Egorov VI, Varlamov VV, et al.: Thoracoscopic collagen pleurodesis in the treatment of malignant pleural effusions. Eur J Cardiothorac Surg 28 (5): 750-3, 2005. [PUBMED Abstract]
Gravelyn TR, Michelson MK, Gross BH, et al.: Tetracycline pleurodesis for malignant pleural effusions. A 10-year retrospective study. Cancer 59 (11): 1973-7, 1987. [PUBMED Abstract]
Markman M, Cleary S, King ME, et al.: Cisplatin and cytarabine administered intrapleurally as treatment of malignant pleural effusions. Med Pediatr Oncol 13 (4): 191-3, 1985. [PUBMED Abstract]
Heffner JE, Standerfer RJ, Torstveit J, et al.: Clinical efficacy of doxycycline for pleurodesis. Chest 105 (6): 1743-7, 1994. [PUBMED Abstract]
Holoye PY, Jeffries DG, Dhingra HM, et al.: Intrapleural etoposide for malignant effusion. Cancer Chemother Pharmacol 26 (2): 147-50, 1990. [PUBMED Abstract]
Ostrowski MJ, Priestman TJ, Houston RF, et al.: A randomized trial of intracavitary bleomycin and Corynebacterium parvum in the control of malignant pleural effusions. Radiother Oncol 14 (1): 19-26, 1989. [PUBMED Abstract]
Martínez-Moragón E, Aparicio J, Rogado MC, et al.: Pleurodesis in malignant pleural effusions: a randomized study of tetracycline versus bleomycin. Eur Respir J 10 (10): 2380-3, 1997. [PUBMED Abstract]
Emad A, Rezaian GR: Treatment of malignant pleural effusions with a combination of bleomycin and tetracycline. A comparison of bleomycin or tetracycline alone versus a combination of bleomycin and tetracycline. Cancer 78 (12): 2498-501, 1996. [PUBMED Abstract]
Zimmer PW, Hill M, Casey K, et al.: Prospective randomized trial of talc slurry vs bleomycin in pleurodesis for symptomatic malignant pleural effusions. Chest 112 (2): 430-4, 1997. [PUBMED Abstract]
Patz EF, McAdams HP, Erasmus JJ, et al.: Sclerotherapy for malignant pleural effusions: a prospective randomized trial of bleomycin vs doxycycline with small-bore catheter drainage. Chest 113 (5): 1305-11, 1998. [PUBMED Abstract]
Yim AP, Chan AT, Lee TW, et al.: Thoracoscopic talc insufflation versus talc slurry for symptomatic malignant pleural effusion. Ann Thorac Surg 62 (6): 1655-8, 1996. [PUBMED Abstract]
Nio Y, Nagami H, Tamura K, et al.: Multi-institutional randomized clinical study on the comparative effects of intracavital chemotherapy alone versus immunotherapy alone versus immunochemotherapy for malignant effusion. Br J Cancer 80 (5-6): 775-85, 1999. [PUBMED Abstract]
Noppen M, Degreve J, Mignolet M, et al.: A prospective, randomised study comparing the efficacy of talc slurry and bleomycin in the treatment of malignant pleural effusions. Acta Clin Belg 52 (5): 258-62, 1997. [PUBMED Abstract]
Walker-Renard PB, Vaughan LM, Sahn SA: Chemical pleurodesis for malignant pleural effusions. Ann Intern Med 120 (1): 56-64, 1994. [PUBMED Abstract]
Kuzdzał J, Sładek K, Wasowski D, et al.: Talc powder vs doxycycline in the control of malignant pleural effusion: a prospective, randomized trial. Med Sci Monit 9 (6): PI54-9, 2003. [PUBMED Abstract]
Hsu LH, Soong TC, Feng AC, et al.: Intrapleural urokinase for the treatment of loculated malignant pleural effusions and trapped lungs in medically inoperable cancer patients. J Thorac Oncol 1 (5): 460-7, 2006. [PUBMED Abstract]
Malignant Pericardial Effusion
Malignant pericardial effusions occur in up to 21% of cancer patients [1–3] and are frequently not suspected until clinical signs or symptoms of pericardial tamponade develop.[4] Two-thirds of patients have subclinical pericardial effusions with no overt cardiovascular signs or symptoms.[5,6] One-half of cases of pericardial effusion initially present with symptoms of cardiac tamponade.[7] In 50% of cases, pericardial effusion is the first sign of malignant disease.[8] Symptoms of pericardial effusion are often attributed to the underlying cancer and may include the following:[9]
Dyspnea.
Fatigue.
Asthenia.
Symptomatic pericardial effusions are often a preterminal event; however, significant symptom palliation can be achieved with prompt diagnosis and management.
Of patients with malignant pericardial effusions, 50% will have concomitant pleural effusions, and one-third will have pulmonary parenchymal disease.[4]
One-third of patients with pericardial metastases will eventually die of pericardial tamponade.[4] Pericardial involvement contributed to the cause of death in 85% of patients in a series reported in 1962 but in only 46% of patients in a more recent study.[10] Improvements in diagnostic and therapeutic options account for the decrease in mortality over the past 40 years.
Incidence and Prevalence
Malignant pericardial effusion occurs in up to 21% of autopsy cases in patients with common malignancies.[4,7] Of patients with lung cancer, 33% have pericardial metastases at autopsy, and one-third of cases of pericardial metastases are caused by lung cancer. Breast cancer causes 25% of pericardial effusions, and about 25% of patients with breast cancer have pericardial effusions. Hematological malignancies (leukemia, Hodgkin disease, non-Hodgkin lymphoma) cause 15% of cases of malignant pericardial effusions.[11]
A retrospective review of 23,592 effusions over a 24-year period revealed 65 malignant effusions (17%) out of 375 pericardial effusions. Lung cancer was the most common cancer found among the malignant pericardial effusions in males, and breast cancer was the most common in females. In 43% of cases, pericardial effusion was the first detected sign of cancer. Of patients diagnosed with malignant pericardial effusions, 86% died within 1 year of diagnosis, with nearly one-third dying within the first month.[8]
In a study of 31 patients with both cancer and pericardial effusions, malignant pericardial effusion accounted for 58% of the effusions, benign idiopathic pericarditis caused 32% of the cases, and radiation pericarditis caused 10% of cases.[11,12]
Pathophysiology
Malignant involvement of the pericardium is the most common reason for development of pericardial effusions, which result from blockage of venous and lymphatic circulation of pericardial fluid. Such blockage may be caused by primary malignancy of the pericardium, such as pericardial mesothelioma, or by tumors arising in the myocardium, including angiosarcoma, rhabdomyosarcoma, and malignant fibrous histiocytosis. Malignancies can also involve the pericardium through direct extension from carcinomas of the lung or esophagus, thymoma, or lymphoma.[9] Lymphatic or hematogenous metastasis to the pericardium occurs most commonly with the following cancers:
Carcinomas of the breast and lung.
Leukemia.
Lymphoma.
Melanoma.
Primary tumors of the pleura or pericardium have been termed primary intrathoracic malignant effusions.[13]
Nonmalignant causes of pericardial effusion include:[14–16]
Pericarditis.
Myocardial infarction.
Uremia.
Hypothyroidism.
Systemic lupus erythematosus.
Trauma.
Postsurgical pericardiotomy syndrome.
Intrapericardial hematomas.
AIDS may also cause pericardial effusion with pericarditis.[17] Radiation therapy or chemotherapy drugs can cause pericarditis without metastatic involvement of the pericardium. Radiation pericarditis is usually associated with radiation doses to the cardiac window exceeding 30 Gy [10] and occurs most frequently in patients who have received mediastinal radiation for Hodgkin lymphoma or breast cancer.[10] Doxorubicin and cyclophosphamide have been associated with the development of acute pericarditis with effusions.[11,12] Other drugs that may cause acute pericarditis include procainamide, hydralazine, isoniazid, methysergide, phenytoin, and anticoagulants.
Pericardial tamponade results from progressive fluid accumulation in the pericardial sac, causing the following:[15]
Elevated intrapericardial pressure.
Diminished stroke volume.
Decreased cardiac output.
Progressive decrease in cardiac diastolic filling.
Hemodynamic compromise resulting in death if not treated.
Hemodynamic compromise occurs when the normal amount of pericardial fluid (approximately 15–50 mL) increases to 200 mL to 1,800 mL.[15,18] When fluid accumulates rapidly, as little as 250 mL of fluid can result in tamponade.[11,19]
Dyspnea occurs in 93% of patients with pericardial effusions.[6] Common symptoms include the following:
Cough.
Chest pain.
Orthopnea (discomfort with breathing while lying flat).
Other symptoms of pericardial effusion include:
Upper abdominal distention or pressure caused by downward hepatic distention.
Hiccups resulting from pressure on the diaphragm.
Pleuritic pain caused by stretching of the pericardium (especially when lying flat).
Signs of effusion include the following:
Kussmaul’s sign (increased distention of jugular veins with inspiration).
Friedreich’s sign (rapid diastolic descent of the venous pulse).
Pulsus paradoxus (decrease of more than 10 mm Hg in the diastolic pressure on inspiration).
Pericardial friction rubs and fever are more commonly associated with nonmalignant causes of pericardial effusions than with malignant etiologies.[9]
Signs of pericardial tamponade include:
Tachycardia.
Pulsus paradoxus.
Elevated jugular venous pressure.
Hypotension.
However, some patients may develop tamponade without this clinical pattern.[4]
Diagnosis
A chest x-ray may show widening of the cardiac silhouette [7] if the amount of pericardial fluid collection exceeds 250 mL.[20] However, a chest x-ray cannot determine the degree of cardiac dysfunction or tamponade. Loculated pericardial effusions may not be apparent on standard posterior/anterior or lateral chest radiographic views.[15]
Transthoracic echocardiography using apical, subxiphoid, and parasternal views can evaluate the presence, quantity, and quality of suspected pericardial effusions, as well as associated pericardial masses and inflammation. Moderate effusions on echocardiography show an echo-free space of 10 mm to 20 mm during diastole in M-mode or 2-dimensional echocardiography, whereas severe effusions have an echo-free space exceeding 20 mm.[21,22] Echocardiography can also determine right and left ventricular function and the possibility of right ventricular or atrial diastolic collapse.[7] Left ventricular collapse caused by large pleural effusions without clinically significant pericardial effusions has been reported.[4,16,23,24] However, transesophageal echocardiography may be useful for loculated effusions resulting from adhesions adjacent to the atria, where the thinness of the atrial wall may not be well visualized on transthoracic echocardiography.[4,16]
Echocardiography in pericardial effusion with tamponade shows right atrial or right ventricular compression, or left atrial compression, decreased left ventricular dimension, and absence of collapse of the inferior vena cava on deep inspiration.[6,25] Echocardiography findings predictive of pericardial tamponade have been reported.[26] Right atrial collapse has a sensitivity of 55% to 60% and a specificity of 50% to 68%. Right ventricular diastolic collapse has a lower sensitivity of 38% to 48% but a higher specificity ranging from 84% to 100%. Because neither finding provides 100% sensitivity and specificity, patients who are clinically symptomatic should have a diagnostic pericardiocentesis, even in the absence of definitive findings on echocardiography.[4,27] One study found right atrial collapse present in only 42% of patients and right ventricular collapse in 62%.[27] Nonetheless, 80% of patients with malignant pericardial effusions had symptomatic relief following pericardiocentesis.
The most definitive test for the diagnosis of cardiac tamponade is equalization of diastolic pressures between all cardiac chambers on right-heart cardiac catheterization.[7] However, this invasive technique is not necessary to diagnose tamponade.
An electrocardiogram (ECG) in patients with pericardial effusions typically shows diminished QRS amplitude in all leads. A classic but uncommonly seen finding in large effusions with pericardial tamponade is variation in the amplitude of the P wave and QRS complex in successive beats on ECG, referred to as electrical alternans. This finding results from movement of the heart within the pericardial sac.[6] Electrocardiography is not sufficiently sensitive to diagnose pericardial effusions.
Pericardial fluid cytology has an accuracy of 80% to 90% in diagnosing malignant pericardial effusion.[6,28] Lymphomas and mesothelioma have higher false-negative detection rates on cytology evaluation.[6,29] Pericardial fluid cytology has a specificity of up to 100%, but sensitivity ranges from 57% to 100% [10][Level of evidence: II] in patients with a known cancer diagnosis and pericardial fluid. Because nonmalignant causes of pericardial effusion can occur in 42% to 62% of patients with cancer and pericardial fluid, a negative cytology examination of pericardial fluid does not help distinguish malignant from nonmalignant causes. The use of more than one cytological preparation (such as concentrating the sample via cytospin, using special markers, or analyzing DNA content) increases the yield over a single preparation. However, multiple samples using the same technique did not significantly increase the diagnostic yield in a retrospective study of 215 patients.[30] In a survey of 80 samples, measurement of DNA index via flow cytometry of pericardial fluid has a sensitivity of 94.8% and a specificity of 100%, compared with routine cytology, which has a sensitivity of 98.5% and a specificity of 92.3%.[31][Level of evidence: II]
Pericardial biopsy may increase the sensitivity of diagnosing pericardial effusions of malignant origin. However, because pericardial effusions usually occur in advanced disease and portend a shorter survival than other sites of metastatic involvement, the relief of symptoms rather than diagnosis should be the overriding factor in determining the extent of the evaluation and the course of treatment. Two studies failed to show a difference in survival in cancer patients with pericardial effusion dependent on the results of fluid cytology.[10,32]
In a study of patients with stage I esophageal cancer who underwent radiation and chemotherapy, risk factors for developing pericardial effusion included advanced age, higher pericardial volume 30 (≥41.6 percentage of cardiac volume receiving more than 30 Gy), high body mass index, and diabetes mellitus.[33]
Treatment
No large controlled, randomized, prospective clinical trials demonstrate the optimal management of malignant pericardial effusions or tamponade. Treatment should therefore be individualized to maximize symptom relief with minimal impact on quality of life. Treatment options include the following:[34][Level of evidence: III]
Percutaneous pericardiocentesis.
Percutaneous balloon pericardiotomy.
Pericardial sclerosis.
Subxiphoid pericardial window.
Pericardiectomy.
Pericardiotomy by thoracotomy or video-assisted thoracoscopy.
Shortened hospitalization for patients with advanced disease.
The patient’s prognosis.
Large, symptomatic, malignant pericardial effusions are managed by draining the fluid, unless the goals of therapy dictate a less invasive, conservative approach, with concomitant shorter survival balanced against quality-of-life concerns. If treatment is indicated for tamponade, percutaneous subxiphoid pericardiocentesis is the treatment of choice in the acute setting. Echocardiography is recommended for catheter guidance.[6,35] Catheter drainage is recommended for large effusions to prevent rapid reaccumulation of fluid and subsequent tamponade and for the anticipated survival of the patient.
Recurrent pericardial effusion occurs in 21% [36] to 50% [34,35] of patients following pericardiocentesis. Limited case series suggest rates of pericardial fluid reaccumulation at 30 days ranging from 5% to 33% after pericardial drainage followed by intrapericardial treatment with sclerosing agents or phosphorus-colloid, compared with more than 50% for patients treated with pericardial drainage alone.[34,35]
Prolonged catheter drainage can be effective in preventing fluid reaccumulation; however, the mechanism is unclear. One series reported recurrence in 30% of patients at a median time of 39 days. In another series, the reported recurrence rate of the pericardial effusion was 13% by 1 year of follow-up.[37,38]
The prolonged catheter drainage could be left in for several days.[38,39] The catheter should be left in situ until the drainage is minimal (<25–50 mL in a 24-hour period) to none. In one series of 171 patients with malignant pericardial effusion who received echocardiography-guided pericardiocentesis followed by extended catheter drainage, the average time to very little catheter output (<50 mL in 24 hours) was about 3 days.[39] Other treatment options to prevent reaccumulation include intrapericardial sclerosis to obliterate the space within the pericardial sac or pericardiotomy to increase the quantity of fluid drained from the pericardium.
The most effective sclerosing agent for malignant pericardial effusions had been tetracycline, with success rates of up to 80%.[6] However, this agent is no longer available as an intravenous drug in the United States. Alternative sclerosants that have been used include the following:
Most patients may require three or more treatments to achieve adequate sclerosis.[6] Significant pain is reported by 16% of patients undergoing pericardial sclerosis.[6] The side effects of various sclerosing agents (e.g., chest pain and arrhythmias) must be considered. Of patients undergoing pericardial sclerotherapy, 70% to 80% have no fluid reaccumulation within 30 days of the procedure.[35]
A retrospective comparison of pericardiocentesis with sclerotherapy to open surgical drainage in 60 patients showed similar rates of treatment complications, incidence of recurrent effusion, and survival following treatment in both groups.[44] A retrospective review of 59 patients found similar success rates, whether patients were managed with surgical subxiphoid pericardial window or by pericardiocentesis with or without sclerosis.[34] Patients who underwent pericardiocentesis followed by pericardial window had the longest survival, with a median of 6 months. However, selection bias toward patients with better performance status undergoing more aggressive surgical techniques may contribute this reported survival advantage. The surgical procedure group had significantly higher average costs of $4,830 compared with $1,625 for patients managed with pericardiocentesis.[34]
Other studies have reported mortality, recurrence, and survival rates for sclerosis that are similar to or slightly lower than those for subxiphoid window or video-assisted thoracoscopy.[44,45];[46][Level of evidence: II][34][Level of evidence: III] Pericardiocentesis with or without sclerotherapy should be considered instead of more invasive procedures in patients with advanced disease or poor functional status.[47]
Transcutaneous balloon pericardiostomy is another technique that is less invasive than open surgical approaches, which include subxiphoid pericardial windows, thoracotomy with pericardiopleural window formation,[48] and thoracotomy with pericardectomy.
Video pericardioscopy has a diagnostic sensitivity of 97% for detecting malignant effusions.[49] Pericardioscopy also is useful for drainage of loculated effusions.[50][Level of evidence: II] Video-assisted thoracoscopy is preferable to more invasive surgical management and should be considered for patients requiring repeated pericardiocentesis to control symptomatic effusions.[47]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Lam KY, Dickens P, Chan AC: Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med 117 (10): 1027-31, 1993. [PUBMED Abstract]
Silvestri F, Bussani R, Pavletic N, et al.: Metastases of the heart and pericardium. G Ital Cardiol 27 (12): 1252-5, 1997. [PUBMED Abstract]
Galli M, Politi A, Jemoli R, et al.: Transcatheter management of cardiac and pericardial metastatic involvement. G Ital Cardiol 28 (6): 687-90, 1998. [PUBMED Abstract]
Bisel HF, Wroblewski F, Ladue JS: Incidence and clinical manifestations of cardiac metastases. J Am Med Assoc 153 (8): 712-5, 1953. [PUBMED Abstract]
Fiocco M, Krasna MJ: The management of malignant pleural and pericardial effusions. Hematol Oncol Clin North Am 11 (2): 253-65, 1997. [PUBMED Abstract]
DeCamp MM, Mentzer SJ, Swanson SJ, et al.: Malignant effusive disease of the pleura and pericardium. Chest 112 (4 Suppl): 291S-295S, 1997. [PUBMED Abstract]
Wang PC, Yang KY, Chao JY, et al.: Prognostic role of pericardial fluid cytology in cardiac tamponade associated with non-small cell lung cancer. Chest 118 (3): 744-9, 2000. [PUBMED Abstract]
Chiles C, Woodard PK, Gutierrez FR, et al.: Metastatic involvement of the heart and pericardium: CT and MR imaging. Radiographics 21 (2): 439-49, 2001 Mar-Apr. [PUBMED Abstract]
Posner MR, Cohen GI, Skarin AT: Pericardial disease in patients with cancer. The differentiation of malignant from idiopathic and radiation-induced pericarditis. Am J Med 71 (3): 407-13, 1981. [PUBMED Abstract]
Ang P, Tan EH, Leong SS, et al.: Primary intrathoracic malignant effusion: a descriptive study. Chest 120 (1): 50-4, 2001. [PUBMED Abstract]
Guberman BA, Fowler NO, Engel PJ, et al.: Cardiac tamponade in medical patients. Circulation 64 (3): 633-40, 1981. [PUBMED Abstract]
Beauchamp KA: Pericardial tamponade: an oncologic emergency. Clin J Oncol Nurs 2 (3): 85-95, 1998. [PUBMED Abstract]
D’Cruz IA, Kanuru N: Echocardiography of serous effusions adjacent to the heart. Echocardiography 18 (5): 445-56, 2001. [PUBMED Abstract]
White CS: MR evaluation of the pericardium and cardiac malignancies. Magn Reson Imaging Clin N Am 4 (2): 237-51, 1996. [PUBMED Abstract]
Celermajer DS, Boyer MJ, Bailey BP, et al.: Pericardiocentesis for symptomatic malignant pericardial effusion: a study of 36 patients. Med J Aust 154 (1): 19-22, 1991. [PUBMED Abstract]
Mercé J, Sagristà-Sauleda J, Permanyer-Miralda G, et al.: Correlation between clinical and Doppler echocardiographic findings in patients with moderate and large pericardial effusion: implications for the diagnosis of cardiac tamponade. Am Heart J 138 (4 Pt 1): 759-64, 1999. [PUBMED Abstract]
Weitzman LB, Tinker WP, Kronzon I, et al.: The incidence and natural history of pericardial effusion after cardiac surgery–an echocardiographic study. Circulation 69 (3): 506-11, 1984. [PUBMED Abstract]
Sagristà-Sauleda J, Mercé J, Permanyer-Miralda G, et al.: Clinical clues to the causes of large pericardial effusions. Am J Med 109 (2): 95-101, 2000. [PUBMED Abstract]
Kisanuki A, Shono H, Kiyonaga K, et al.: Two-dimensional echocardiographic demonstration of left ventricular diastolic collapse due to compression by pleural effusion. Am Heart J 122 (4 Pt 1): 1173-5, 1991. [PUBMED Abstract]
Kaplan LM, Epstein SK, Schwartz SL, et al.: Clinical, echocardiographic, and hemodynamic evidence of cardiac tamponade caused by large pleural effusions. Am J Respir Crit Care Med 151 (3 Pt 1): 904-8, 1995. [PUBMED Abstract]
Himelman RB, Kircher B, Rockey DC, et al.: Inferior vena cava plethora with blunted respiratory response: a sensitive echocardiographic sign of cardiac tamponade. J Am Coll Cardiol 12 (6): 1470-7, 1988. [PUBMED Abstract]
Cooper JP, Oliver RM, Currie P, et al.: How do the clinical findings in patients with pericardial effusions influence the success of aspiration? Br Heart J 73 (4): 351-4, 1995. [PUBMED Abstract]
Meyers DG, Meyers RE, Prendergast TW: The usefulness of diagnostic tests on pericardial fluid. Chest 111 (5): 1213-21, 1997. [PUBMED Abstract]
Thurber DL, Edwards JE, Achor RW: Secondary malignant tumors of the pericardium. Circulation 26: 228-41, 1962. [PUBMED Abstract]
Garcia LW, Ducatman BS, Wang HH: The value of multiple fluid specimens in the cytological diagnosis of malignancy. Mod Pathol 7 (6): 665-8, 1994. [PUBMED Abstract]
Decker D, Stratmann H, Springer W, et al.: Benign and malignant cells in effusions: diagnostic value of image DNA cytometry in comparison to cytological analysis. Pathol Res Pract 194 (11): 791-5, 1998. [PUBMED Abstract]
Okamoto H, Shinkai T, Yamakido M, et al.: Cardiac tamponade caused by primary lung cancer and the management of pericardial effusion. Cancer 71 (1): 93-8, 1993. [PUBMED Abstract]
Tamari K, Isohashi F, Akino Y, et al.: Risk factors for pericardial effusion in patients with stage I esophageal cancer treated with chemoradiotherapy. Anticancer Res 34 (12): 7389-93, 2014. [PUBMED Abstract]
Anderson TM, Ray CW, Nwogu CE, et al.: Pericardial catheter sclerosis versus surgical procedures for pericardial effusions in cancer patients. J Cardiovasc Surg (Torino) 42 (3): 415-9, 2001. [PUBMED Abstract]
Martinoni A, Cipolla CM, Civelli M, et al.: Intrapericardial treatment of neoplastic pericardial effusions. Herz 25 (8): 787-93, 2000. [PUBMED Abstract]
Tsang TS, Seward JB, Barnes ME, et al.: Outcomes of primary and secondary treatment of pericardial effusion in patients with malignancy. Mayo Clin Proc 75 (3): 248-53, 2000. [PUBMED Abstract]
Allen KB, Faber LP, Warren WH, et al.: Pericardial effusion: subxiphoid pericardiostomy versus percutaneous catheter drainage. Ann Thorac Surg 67 (2): 437-40, 1999. [PUBMED Abstract]
Patel N, Rafique AM, Eshaghian S, et al.: Retrospective comparison of outcomes, diagnostic value, and complications of percutaneous prolonged drainage versus surgical pericardiotomy of pericardial effusion associated with malignancy. Am J Cardiol 112 (8): 1235-9, 2013. [PUBMED Abstract]
Lekhakul A, Assawakawintip C, Fenstad ER, et al.: Safety and Outcome of Percutaneous Drainage of Pericardial Effusions in Patients with Cancer. Am J Cardiol 122 (6): 1091-1094, 2018. [PUBMED Abstract]
Colleoni M, Martinelli G, Beretta F, et al.: Intracavitary chemotherapy with thiotepa in malignant pericardial effusions: an active and well-tolerated regimen. J Clin Oncol 16 (7): 2371-6, 1998. [PUBMED Abstract]
Moriya T, Takiguchi Y, Tabeta H, et al.: Controlling malignant pericardial effusion by intrapericardial carboplatin administration in patients with primary non-small-cell lung cancer. Br J Cancer 83 (7): 858-62, 2000. [PUBMED Abstract]
Norum J, Lunde P, Aasebø U, et al.: Mitoxantrone in malignant pericardial effusion. J Chemother 10 (5): 399-404, 1998. [PUBMED Abstract]
Girardi LN, Ginsberg RJ, Burt ME: Pericardiocentesis and intrapericardial sclerosis: effective therapy for malignant pericardial effusions. Ann Thorac Surg 64 (5): 1422-7; discussion 1427-8, 1997. [PUBMED Abstract]
Maher EA, Shepherd FA, Todd TJ: Pericardial sclerosis as the primary management of malignant pericardial effusion and cardiac tamponade. J Thorac Cardiovasc Surg 112 (3): 637-43, 1996. [PUBMED Abstract]
Liu G, Crump M, Goss PE, et al.: Prospective comparison of the sclerosing agents doxycycline and bleomycin for the primary management of malignant pericardial effusion and cardiac tamponade. J Clin Oncol 14 (12): 3141-7, 1996. [PUBMED Abstract]
Lin JC, Hazelrigg SR, Landreneau RJ: Video-assisted thoracic surgery for diseases within the mediastinum. Surg Clin North Am 80 (5): 1511-33, 2000. [PUBMED Abstract]
Olson JE, Ryan MB, Blumenstock DA: Eleven years’ experience with pericardial-peritoneal window in the management of malignant and benign pericardial effusions. Ann Surg Oncol 2 (2): 165-9, 1995. [PUBMED Abstract]
Porte HL, Janecki-Delebecq TJ, Finzi L, et al.: Pericardoscopy for primary management of pericardial effusion in cancer patients. Eur J Cardiothorac Surg 16 (3): 287-91, 1999. [PUBMED Abstract]
Millaire A, Wurtz A, de Groote P, et al.: Malignant pericardial effusions: usefulness of pericardioscopy. Am Heart J 124 (4): 1030-4, 1992. [PUBMED Abstract]
Superior Vena Cava Syndrome
Overview
Superior vena cava syndrome (SVCS) is an array of symptoms caused by the impairment of blood flow through the superior vena cava (SVC) to the right atrium. Symptoms that suggest this syndrome include the following:[1]
Dyspnea.
Coughing.
Swelling of the face, neck, upper trunk, and extremities.
In rare instances, patients may complain of hoarseness, chest pain, dysphagia, and hemoptysis.
Physical signs that may be noted on presentation include the following:
Neck vein distention.
Thoracic vein distention.
Edema of the face or upper extremities.
Plethora.
Tachypnea.
Rarely, cyanosis, Horner syndrome, and a paralyzed vocal cord may also be present.[1]
SVCS is usually a sign of locally advanced bronchogenic carcinoma. Survival depends on the status of the patient’s disease. When small cell bronchogenic carcinoma is treated with chemotherapy, the median survival times with or without SVCS are almost identical (42 weeks or 40 weeks, respectively). The 24-month survival rate is 9% in patients without SVCS and 3% in those with the syndrome. When the malignancy is treated with radiation therapy, 46% of patients who have non-small cell lung cancer experience relief of symptoms, compared with 62% of patients who have small cell bronchogenic carcinoma. The 2-year survival rate of 5% is almost the same for both groups.[2]
Most patients with non-Hodgkin lymphoma and SVCS respond to appropriate chemotherapy or to combined-modality regimens.
Etiology and Physiology
Since William Hunter first described SVCS in 1757, the spectrum of underlying conditions associated with it has shifted from tuberculosis and syphilitic aneurysms of the ascending aorta to malignant disorders. Almost 95% of SVCS cases described in published modern series result from cancer. The most common cause is small cell bronchogenic carcinoma, followed by squamous cell carcinoma of the lung, adenocarcinoma of the lung, non-Hodgkin lymphoma, and large cell carcinoma of the lung.[3] Nonmalignant causes of SVCS in cancer patients include thrombosis that is associated with intracaval catheters or pacemaker wires.[4] A rare cause of SVCS is fibrosing mediastinitis, either idiopathic or associated with histoplasmosis.[5] Additional rare causes of SVCS include metastatic germ cell neoplasms, metastatic breast cancer, colon cancer, Kaposi sarcoma, esophageal carcinoma, fibrous mesothelioma, Behçet syndrome, thymoma, substernal thyroid goiter, Hodgkin lymphoma, and sarcoidosis.[6]
Knowledge of the anatomy of the SVC and its relationship to the surrounding lymph nodes is essential to understand development of the syndrome. The SVC is formed by the junction of the left and right brachiocephalic veins in the mid third of the mediastinum. The SVC extends caudally for 6 to 8 cm, coursing anterior to the right mainstem bronchus and terminating in the superior right atrium, and extends anteriorly to the right mainstem bronchus. The SVC is joined posteriorly by the azygos vein as it loops over the right mainstem bronchus and lies posterior to and to the right of the ascending aorta. The mediastinal parietal pleura is lateral to the SVC, creating a confined space, and the SVC is adjacent to the right paratracheal, azygous, right hilar, and subcarinal lymph node groups. The vessel itself is thin-walled, and the blood flowing in it is under low pressure. Thus, when the nodes or ascending aorta enlarge, the SVC is compressed, blood flow slows, and complete occlusion may occur.
The severity of SVCS depends on the speed of onset and location of the obstruction. The more rapid the onset, the more severe the symptoms because the collateral veins do not have time to distend to accommodate an increased blood flow.[7]
If the obstruction is above the entry of the azygos vein, the syndrome is less pronounced because the azygous venous system can readily distend to accommodate the shunted blood with less venous pressure developing in the head, arms, and upper thorax.
If the obstruction is below the entry of the azygos vein, more florid symptoms and signs are seen because the blood must be returned to the heart via the upper abdominal veins and the inferior vena cava, which requires higher venous pressure.
One study suggested that the general recruitment of venous collaterals over time may lead to remission of the syndrome, although the SVC remains obstructed.[8]
Assessment and Diagnosis
Once SVCS is recognized, prompt clinical attention is important. A diagnosis should be established before therapy begins because:[3]
75% of patients have symptoms and signs for longer than 1 week before seeking medical attention.
Cancer patients diagnosed with SVCS do not die of the syndrome itself but rather their underlying disease.
3% to 5% of the patients diagnosed with SVCS do not have cancer.
In the absence of tracheal obstruction, SVCS is unlikely to be a life-threatening oncologic emergency, and treatment before definitive diagnosis is not justified.
The initial evaluation of the patient should include a chest x-ray to look for mediastinal masses and associated findings, such as pleural effusion, lobar collapse, or cardiomegaly. Computed tomography (CT) scanning of the thorax yields the most useful diagnostic information and can define the anatomy of the involved mediastinal nodes. Venous patency and the presence of thrombi are assessed using contrast and rapid scanning techniques.[9] Depending on local expertise, contrast or nuclear venography, magnetic resonance imaging, and ultrasonography may be valuable in assessing the site and nature of the obstruction.
If bronchogenic carcinoma is suspected, a sputum specimen should be obtained. If the specimen is negative, a biopsy specimen should be taken from the most accessible site that is clinically involved with disease. The biopsy approach depends on the working diagnosis, location of the tumor, physiological status of the patient, and expertise at the facility. It may include:[10]
Bronchoscopy.
Biopsy of palpable cervical or supraclavicular lymph nodes.
Needle biopsy of a lung mass or mediastinal nodes using either CT or ultrasonography guidance.
Mediastinoscopy.
Mediastinotomy.
Median sternotomy.
Video-assisted thoracoscopy.
Conventional thoracotomy.
The biopsy findings will help the clinician plan appropriate treatment.
Treatment Options for SVCS
The treatment of SVCS depends on the following:
The etiology of the obstruction.
The severity of symptoms.
The patient’s prognosis.
Patient preferences and goals for therapy.
Radiation therapy or chemotherapy should be withheld until the etiology of the obstruction is clear. The treatments discussed here focus on SVC obstruction caused by a malignant tumor. Because the treatment of malignant obstruction may depend on tumor histology, a histological diagnosis should be made before starting treatment. Unless there is airway obstruction or cerebral edema, treatment may be delayed until after an assessment, with no negative effect on outcome.[1,11–15]
Medical management
A patient with sufficient collateral blood flow and minimal symptoms may not need treatment. If the lesion is above the azygous vein or if the onset of SVC occlusion is slow enough to allow sufficient collateral circulation, the symptoms and signs may stabilize, and further therapy may not be needed. Short-term palliation of a symptomatic patient who does not want aggressive treatment may be achieved by elevating the head and using corticosteroids and diuresis. Although no definitive studies prove the effectiveness of steroids, they may be useful to treat respiratory compromise. Diuretics may relieve edema but can cause systemic complications, such as dehydration.[9,16]
Radiation therapy
If the obstruction of the SVC is caused by a tumor that is not sensitive to chemotherapy, radiation therapy should be given. Treatment with larger fractions of radiation is thought to help. However, one study shows no obvious need for large radiation fraction sizes for the first few radiation treatments as was previously believed.[17] Many fractionation schemes have been used, with doses ranging from 30 Gy in 10 fractions to 50 Gy in 25 fractions. Relief of symptoms is reported to be 62% to 80% in patients with small cell lung cancer and about 46% in patients with non-small cell lung cancer.[2,18] In one study, more than 90% of the patients achieved a partial or complete response with a 3-week regimen of 8 Gy given once a week for a total dose of 24 Gy.[19]
Chemotherapy
Chemotherapy is the treatment of choice for sensitive tumors such as lymphoma or small cell lung cancer. SVCS does not appear to be an independent prognostic factor, and its presence should not change the treatment approach. Rapid initiation of chemotherapy can result in complete and partial response rates of the SVCS of more than 80% in patients with small cell lung cancer.[2,18]
Thrombolysis
It has been suggested that SVCS arises when a thrombus forms in a partially occluded vein. In patients with a documented thrombus in the SVC, treatment may include thrombectomy, with or without tissue plasminogen activator or other thrombolytic agents, such as streptokinase or urokinase.[1]
Stent placement
Numerous small studies have reported the use of an intravascular expandable stent to reopen the occluded SVC; however, no prospectively designed comparative studies have been published.[20] The reported response rates have been about 90% or greater.[21][Level of evidence: II] There is no agreement on the need for anticoagulant therapy after stent placement. In one series that used anticoagulant therapy as part of the treatment protocol, there were reports of reocclusion after this therapy was stopped.[22][Level of evidence: II] However, in another study, 17 patients with cancer who were treated with stents and did not receive anticoagulant therapy had no occlusions.[23][Level of evidence: II]
Surgery
Surgical bypass of an obstructed SVC is more appropriate for patients with a benign obstruction than with a malignant obstruction,[24] although surgical bypass has also been used for patients with malignant obstructions.
Psychosocial Considerations
Patients and family members are often frightened and anxious about the symptoms of SVCS, particularly swelling, dysphagia, coughing, and hoarseness. Patients and family members need information about the cause of the symptoms and short-term measures for palliation, especially during the diagnostic period. When aggressive treatment is declined because of the terminal nature of the underlying disease, symptom management can be offered to patients and family members.
Because most adult patients who develop SVCS have lung cancer, the treatment and psychological support approaches for SVCS should take into account the patient’s prognosis and mental condition, goals of care, and other symptoms caused by the malignancy.[25]
Pediatric Considerations
As described in this summary, SVCS refers to the symptoms associated with the compression or obstruction of the SVC; the compression of the trachea is termed superior mediastinal syndrome (SMS). Because SMS and the resulting respiratory compromise frequently occur in children with SVCS, the two syndromes have become almost synonymous in pediatric practice.[26,27] In adults, the trachea and the right mainstem bronchus are relatively rigid structures compared with the vena cava, but in children, these structures are more susceptible to compression. In addition, the relatively smaller intraluminal diameters of a child’s trachea and bronchus can tolerate little edema before respiratory symptoms occur. Because of this accompanying respiratory component, SVCS in children differs from the adult syndrome and is a serious medical emergency.
The most common symptoms of SVCS in children are similar to those in adults and include the following:[26]
Coughing.
Hoarseness.
Dyspnea.
Orthopnea.
Chest pain.
Less common but more serious symptoms include the following:
Syncope.
Anxiety.
Confusion.
Lethargy.
Headache.
Distorted vision.
A sense of fullness in the ears.
SVCS is rare in children, appearing at presentation in 12% of pediatric patients with malignant mediastinal tumors.[28,29] The etiology, diagnosis, and treatment of SVCS in children differ from those in adults. The most frequent cause of SVCS in adults is bronchogenic carcinoma;[3] in children, it is non-Hodgkin lymphoma. As in adults, a frequent nonmalignant cause is thrombosis from catheterization for venous access.[26]
A physical examination, chest radiograph, and medical history are usually sufficient to diagnose SVCS. If lymphomas or other malignant diseases are suspected, a tissue sample may aid diagnosis. However, the procedure to obtain the specimen may involve significant risk and may not be clinically feasible. Children with SVCS have a poor tolerance for the necessary general anesthesia because the accompanying cardiovascular and pulmonary changes aggravate the SVCS, often making intubation impossible. Also, extubation may be difficult or impossible, requiring prolonged airway provision (intubation). A CT scan of the chest to determine tracheal size, upright and supine echocardiography, and a flow volume loop may help evaluate anesthetic risk. Because anesthesia use is a serious risk, the diagnosis should be made with the least invasive means possible.[30] Published reports suggest a stepwise approach.[26]
When a malignant mass causes SVCS, the situation may be a medical emergency with no opportunity to establish a tissue diagnosis. In these cases, the most appropriate course may be to initiate empiric therapy before biopsy. The traditional empiric therapy is radiation therapy, with the daily dose governed by the presumed radiosensitivity of the tumor. After radiation therapy, respiratory deterioration from the apparent tracheal swelling may occur. This swelling occurs because narrow lumens in children cannot accommodate edema and because of the greater degree of edema at onset, the result of rapid tumor growth in children. In these situations, a course of prednisone at 10 mg/m2 of body surface area 4 times per day may be necessary.[26]
In addition to radiation, empiric therapy for SVCS has included chemotherapeutic agents incorporating steroids, cyclophosphamide, or both in combination with an anthracycline and vincristine.[26] If the tumor fails to respond, it may be a benign lesion.
If surgery becomes necessary, it should be performed with the patient in the semi-Fowler’s position, allowing the surgeon the ability to rapidly change the patient’s position to lateral or prone. Cardiopulmonary bypass facilities and a rigid bronchoscope should be available in a standby capacity.[30]
References
Gauden SJ: Superior vena cava syndrome induced by bronchogenic carcinoma: is this an oncological emergency? Australas Radiol 37 (4): 363-6, 1993. [PUBMED Abstract]
Urban T, Lebeau B, Chastang C, et al.: Superior vena cava syndrome in small-cell lung cancer. Arch Intern Med 153 (3): 384-7, 1993. [PUBMED Abstract]
Yellin A, Rosen A, Reichert N, et al.: Superior vena cava syndrome. The myth–the facts. Am Rev Respir Dis 141 (5 Pt 1): 1114-8, 1990. [PUBMED Abstract]
Gray BH, Olin JW, Graor RA, et al.: Safety and efficacy of thrombolytic therapy for superior vena cava syndrome. Chest 99 (1): 54-9, 1991. [PUBMED Abstract]
Goodwin RA, Nickell JA, Des Prez RM: Mediastinal fibrosis complicating healed primary histoplasmosis and tuberculosis. Medicine (Baltimore) 51 (3): 227-46, 1972. [PUBMED Abstract]
Yahalom J: Oncologic emergencies: superior vena cava syndrome. In: DeVita VT, Hellman S, Rosenberg SA, eds.: Cancer: Principles and Practice of Oncology. JB Lippincott Company, 4th Edition, 1993, pp 2111-2118.
Netter FH: Superior vena cava syndrome. In: Netter FH: The CIBA Collection of Medical Illustrations: Respiratory System. CIBA Pharmaceutical Company, 1980, pp 164.
Ahmann FR: A reassessment of the clinical implications of the superior vena caval syndrome. J Clin Oncol 2 (8): 961-9, 1984. [PUBMED Abstract]
Abner A: Approach to the patient who presents with superior vena cava obstruction. Chest 103 (4 Suppl): 394S-397S, 1993. [PUBMED Abstract]
Hsu JW, Chiang CD, Hsu WH, et al.: Superior vena cava syndrome in lung cancer: an analysis of 54 cases. Gaoxiong Yi Xue Ke Xue Za Zhi 11 (10): 568-73, 1995. [PUBMED Abstract]
Chen JC, Bongard F, Klein SR: A contemporary perspective on superior vena cava syndrome. Am J Surg 160 (2): 207-11, 1990. [PUBMED Abstract]
Stanford W, Doty DB: The role of venography and surgery in the management of patients with superior vena cava obstruction. Ann Thorac Surg 41 (2): 158-63, 1986. [PUBMED Abstract]
Salsali M, Cliffton EE: Superior vena caval obstruction with lung cancer. Ann Thorac Surg 6 (5): 437-42, 1968. [PUBMED Abstract]
Schraufnagel DE, Hill R, Leech JA, et al.: Superior vena caval obstruction. Is it a medical emergency? Am J Med 70 (6): 1169-74, 1981. [PUBMED Abstract]
Shimm DS, Logue GL, Rigsby LC: Evaluating the superior vena cava syndrome. JAMA 245 (9): 951-3, 1981. [PUBMED Abstract]
Baker GL, Barnes HJ: Superior vena cava syndrome: etiology, diagnosis, and treatment. Am J Crit Care 1 (1): 54-64, 1992. [PUBMED Abstract]
Chan RH, Dar AR, Yu E, et al.: Superior vena cava obstruction in small-cell lung cancer. Int J Radiat Oncol Biol Phys 38 (3): 513-20, 1997. [PUBMED Abstract]
Würschmidt F, Bünemann H, Heilmann HP: Small cell lung cancer with and without superior vena cava syndrome: a multivariate analysis of prognostic factors in 408 cases. Int J Radiat Oncol Biol Phys 33 (1): 77-82, 1995. [PUBMED Abstract]
Rodrigues CI, Njo KH, Karim AB: Hypofractionated radiation therapy in the treatment of superior vena cava syndrome. Lung Cancer 10 (3-4): 221-8, 1993. [PUBMED Abstract]
Tanigawa N, Sawada S, Mishima K, et al.: Clinical outcome of stenting in superior vena cava syndrome associated with malignant tumors. Comparison with conventional treatment. Acta Radiol 39 (6): 669-74, 1998. [PUBMED Abstract]
Nicholson AA, Ettles DF, Arnold A, et al.: Treatment of malignant superior vena cava obstruction: metal stents or radiation therapy. J Vasc Interv Radiol 8 (5): 781-8, 1997 Sep-Oct. [PUBMED Abstract]
Dyet JF, Nicholson AA, Cook AM: The use of the Wallstent endovascular prosthesis in the treatment of malignant obstruction of the superior vena cava. Clin Radiol 48 (6): 381-5, 1993. [PUBMED Abstract]
Irving JD, Dondelinger RF, Reidy JF, et al.: Gianturco self-expanding stents: clinical experience in the vena cava and large veins. Cardiovasc Intervent Radiol 15 (5): 328-33, 1992 Sep-Oct. [PUBMED Abstract]
Doty DB: Bypass of superior vena cava: Six years’ experience with spiral vein graft for obstruction of superior vena cava due to benign and malignant disease. J Thorac Cardiovasc Surg 83 (3): 326-38, 1982. [PUBMED Abstract]
Holland JC: Lung Cancer. In: Holland JC, Rowland JH, eds.: Handbook of Psychooncology: Psychological Care of the Patient With Cancer. Oxford University Press, 1989, pp 180-187.
Lange B, O’Neill JA, D’Angio G, et al.: Oncologic emergencies. In: Pizzo PA, Poplack DG: Principles and Practice of Pediatric Oncology. 2nd ed. JB Lippincott, 1993, pp 951-972.
Ingram L, Rivera GK, Shapiro DN: Superior vena cava syndrome associated with childhood malignancy: analysis of 24 cases. Med Pediatr Oncol 18 (6): 476-81, 1990. [PUBMED Abstract]
Pokorny WJ, Sherman JO: Mediastinal masses in infants and children. J Thorac Cardiovasc Surg 68 (6): 869-75, 1974. [PUBMED Abstract]
King RM, Telander RL, Smithson WA, et al.: Primary mediastinal tumors in children. J Pediatr Surg 17 (5): 512-20, 1982. [PUBMED Abstract]
Neuman GG, Weingarten AE, Abramowitz RM, et al.: The anesthetic management of the patient with an anterior mediastinal mass. Anesthesiology 60 (2): 144-7, 1984. [PUBMED Abstract]
Latest Updates to This Summary (02/20/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the pathophysiology and treatment of cardiopulmonary syndromes, including dyspnea, malignant pleural effusion, malignant pericardial effusion, and superior vena cava syndrome. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Cardiopulmonary Syndromes. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/cardiopulmonary-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389275]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Cardiopulmonarysyndromes are conditions of the heart and lung that may be caused by cancer or by other health problems. Five cardiopulmonary syndromes that may be caused by cancer are covered in this summary:
This summary is about cardiopulmonary syndromes in adults and children with cancer. Section titles show when the information is about children.
Dyspnea During Advanced Cancer
Key Points
Many conditions can cause dyspnea.
A physical exam and health history are important in finding out the cause of dyspnea.
There are different ways to treat the causes of dyspnea in cancer patients.
Treatment of dyspnea will depend on what is causing it.
Treatment may be to control the signs and symptoms of dyspnea.
Many conditions can cause dyspnea.
Dyspnea is the feeling that you can’t catch your breath or you can’t breathe in enough air. It also may be called shortness of breath, breathlessness, or air hunger. In cancer patients, dyspnea can be caused by the following:
Tumor-related effects:
The tumor blocks the airways in the chest and lung or it blocks the vein that carries blood through the chest to the heart.
Immunotherapy-related pneumonitis. Pneumonitis linked to immunotherapy with a checkpoint inhibitor is uncommon but can be serious or life-threatening. In one study of patients treated for immunotherapy-related pneumonitis, melanoma and non-small cell lung cancer were the most common cancers. The length of time that patients received immunotherapy before developing pneumonitis varied from several days to over a year. In addition, pneumonitis seemed to occur earlier in patients who received combination therapy than in those who received one type of treatment.
Physical exam and health history: An exam of the body to check general signs of health, including checking for signs or symptoms of dyspnea, such as breathing fast or using the neck or chest muscles to breathe. A history of your health habits and past illnesses and treatments will also be taken. Your doctor will also ask about when the dyspnea occurs, what it feels like, other signs or symptoms that happen at the same time as the dyspnea, and anything that makes it better or worse.
Functional assessment: An exam to check how the dyspnea affects your ability to perform activities of daily living such as eating, bathing, or climbing stairs. This exam may include a 6-minute walk test (6MWT) to measure how far you can walk on a flat, hard surface in 6 minutes.
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. EnlargeA chest x-ray is used to take pictures of the structures and organs inside the chest. X-rays pass through the patient’s body onto film or a computer.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Complete blood count: A procedure in which a sample of blood is taken and checked for the following:
The portion of the blood sample made of red blood cells.
Oxygen saturation test: A procedure to check for the amount of oxygen being carried by the red blood cells. A lower than normal amount of oxygen may be a sign of lung disease or other health problems. One method uses a device clipped to the finger. The device senses the amount of oxygen in the blood flowing through the small blood vessels in the finger. Another method uses a sample of blood taken from an artery, usually in the wrist, that is tested for the amount of oxygen.
Maximum inspiratory pressure (MIP) test: The MIP is the highest pressure that can be reached in the lungs when you take a deep breath. When you breathe through a device called a manometer, the device measures the pressure. The information is sent to a computer. The pressure level shows how strong the breathing muscles are.
There are different ways to treat the causes of dyspnea in cancer patients.
Treatment may include the following:
Radiation therapy: Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the cancer.
Chemotherapy: Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Laser therapy for tumors inside large airways: Use of a laser beam (a narrow beam of intense light) as a knife to remove the tumor.
Cauterization of tumors inside large airways: Use of a hot instrument, an electric current, or a caustic substance to destroy the tumor.
Stent placement: Surgery to place a stent (thin tube) in an airway to keep it open. This may be done if a large airway is blocked by a tumor that is pressing on it from the outside.
Treatment may be to control the signs and symptoms of dyspnea.
Treatment to control the signs and symptoms of dyspnea may include the following:
Oxygen therapy: If you cannot breathe in enough oxygen, you may be given extra oxygen to inhale from a tank. Devices that deliver a high flow of oxygen or air mixed with oxygen may also be prescribed.
Medicines: Opioids, such as morphine, may help with distress, fatigue, and the feeling that you cannot get enough air. Other drugs may be used to treat dyspnea that is related to panic disorder or severe anxiety.
Non-drug treatments:
Breathing methods, such as breathing with the lips pursed (almost closed).
Chronic coughing may cause much physical distress.
It may be possible to treat the cause of chronic coughing.
Medicines may be used to control chronic coughing.
Chronic coughing may cause much physical distress.
Chronic cough may cause pain, trouble sleeping, dyspnea, or fatigue. The causes of chronic coughing are almost the same as the causes of dyspnea. See Dyspnea section for list of causes.
It may be possible to treat the cause of chronic coughing.
Pleural effusion may be caused by cancer, cancer treatment, or other conditions.
Signs and symptoms of pleural effusion include dyspnea (shortness of breath) and cough.
Finding out the cause of pleural effusion will help plan the treatment.
Treatment may be to control signs and symptoms of pleural effusion and improve quality of life.
Pleural effusion is extra fluid around the lungs.
The pleural cavity is the space between the pleura (thin layer of tissue) that covers the outer surface of each lung and lines the inner wall of the chest cavity. Pleural tissue usually makes a small amount of fluid that helps the lungs move smoothly in the chest while a person is breathing. A pleural effusion is extra fluid in the pleural cavity. The fluid presses on the lungs and makes it hard to breathe.
Pleural effusion may be caused by cancer, cancer treatment, or other conditions.
Finding out the cause of pleural effusion will help plan the treatment.
Treatment for a malignant pleural effusion is different from treatment for a nonmalignant effusion, so the right diagnosis is important. Diagnostic tests used to find the cause of the pleural effusion include the following:
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. EnlargeA chest x-ray is used to take pictures of the structures and organs inside the chest. X-rays pass through the patient’s body onto film or a computer.
CT scan: A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram.
Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells. This procedure may be used to reduce pressure on the lungs.
Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If thoracentesis is not possible, a biopsy may be done during a thoracoscopy. A thoracoscopy is a procedure to look at the organs inside the chest to check for abnormal areas. An incision (cut) is made between two ribs and a thoracoscope (a thin, lighted tube with a lens for viewing) is inserted into the chest. A cutting tool at the end of the thoracoscope is used to remove a sample of tissue.
Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light.
The type of cancer, previous treatment for cancer, and your choices also are important in planning treatment.
Treatment may be to control signs and symptoms of pleural effusion and improve quality of life.
A malignant pleural effusion often occurs in cancer that is advanced, cannot be removed by surgery, or continues to grow or spread during treatment. It is also common during the last few weeks of life. The goal of treatment is usually palliative, to relieve signs and symptoms and improve quality of life.
Treatment of the signs and symptoms of malignant pleural effusion includes the following:
Thoracentesis. Thoracentesis is a procedure to remove extra fluid from the pleural cavity between the lung and the chest wall using a needle. Removal of the fluid may help to relieve severe symptoms for a short time. A few days after the extra fluid is removed, it is likely it will begin to come back. The risk of a thoracentesis includes bleeding, infection, collapsed lung, fluid in the lungs, and a sudden drop in blood pressure.
Indwelling pleural catheter (IPC). An indwelling pleural catheter (IPC) is a small tube that is inserted and left in place to keep fluid from building up around the lungs. One end of the tube stays inside the chest and the other passes outside the body to allow fluid to drain. This type of catheter may be used for long-term care so that a separate procedure won’t need to be done each time draining is needed. Risks of IPCs include infection and blockage of the catheter.
Pleurodesis. This is a procedure to close the pleural space so that fluid cannot collect there. Fluid is first removed by thoracentesis, using a chest tube. A drug that causes the pleural space to close is then inserted into the space through a chest tube. Drugs such as bleomycin or talc may be used.
Surgery. Surgery may be done to put in a shunt (tube) to carry the fluid from the pleural cavity to the abdominal cavity, where the fluid is easier to remove. Pleurectomy is another type of surgery that may be used. In this procedure, the part of the pleura that lines the chest cavity is removed.
Malignant Pericardial Effusion
Key Points
Pericardial effusion is extra fluid around the heart.
Pericardial effusion may be caused by cancer or other conditions.
Signs and symptoms of pericardial effusion include dyspnea (shortness of breath) and cough.
Pericardial effusion usually occurs in advanced cancer.
Treatment may be to control the symptoms of pericardial effusion and improve quality of life.
Pericardial effusion is extra fluid around the heart.
Pericardial effusion is extra fluid inside the sac that surrounds the heart. The extra fluid causes pressure on the heart, which stops it from pumping blood normally. If fluid builds up, a condition called cardiac tamponade may occur. In cardiac tamponade, the heart cannot pump enough blood to the rest of the body. This is life-threatening and must be treated right away.
Pericardial effusion may be caused by cancer or other conditions.
Signs and symptoms of pericardial effusion include dyspnea (shortness of breath) and cough.
At first, a pericardial effusion may not cause any signs or symptoms. These and other signs and symptoms may be caused by a pericardial effusion or cardiac tamponade. Check with your doctor if you have any of the following:
Pericardial effusion usually occurs in advanced cancer.
Pericardial effusion usually occurs in advanced cancer or in the last few weeks of life. During these times, it may be more important to relieve the symptoms than to diagnose the condition. However, in some cases, the following tests and procedures may be used to diagnose pericardial effusion:
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. EnlargeA chest x-ray is used to take pictures of the structures and organs inside the chest. X-rays pass through the patient’s body onto film or a computer.
Echocardiography: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs of the chest. The echoes form a picture of the heart’s position, motion of the walls, and internal parts such as the valves.
Electrocardiogram (EKG or ECG): A line graph recording of the heart’s electrical activity to check its rate and rhythm. A number of electrodes (small pads) are placed on the patient’s chest, arms, and legs. The electrodes are connected by wires to the EKG machine. Heart activity is then recorded on paper. Electrical activity that is faster or slower than normal may be a sign of heart problems.
Pericardiocentesis: A procedure to remove fluid from the pericardium using a needle inserted through the chest wall. The doctor may use echocardiography to watch the movement of the heart and needle inside the chest. The fluid is viewed under a microscope by a pathologist to check for cancer cells or signs of infection. This procedure can also be used to treat pericardial effusion. Removing the fluid lessens the pressure on the heart.
Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light.
Treatment may be to control the symptoms of pericardial effusion and improve quality of life.
Pericardiocentesis. A procedure to remove the extra fluid from the sac around the heart using a needle inserted through the chest wall. The doctor may use echocardiography to watch the movement of the heart and needle inside the chest. Removing the fluid can reduce pressure on the heart. In some patients, fluid may again collect in the sac around the heart after pericardiocentesis. A catheter (flexible tube used to put fluids into or take blood out of a vein) may be inserted and left in place for several days until there is little to no fluid drainage. For patients with advanced cancer, this procedure may be used instead of more serious surgery.
Pericardial sclerosis. A procedure to close the pericardial space so fluid cannot collect in the sac around the heart. Fluid is first removed by pericardiocentesis. A drug or chemical is then injected through a catheter (flexible tube used to put fluids into or take blood out of a vein) into the pericardial space to cause it to close. Three or more treatments may be needed to completely close the pericardial space.
Pericardiotomy. A procedure to insert a drainage tube. An incision (cut) is made in the chest and then in the pericardium and a drainage tube is put in place. This increases the amount of fluid that can be drained from the pericardium.
Pericardiectomy. Surgery to remove part of the pericardium. This may be done to drain fluid quickly when cardiac tamponade occurs. This surgery is also called pericardial window.
Balloon pericardiostomy. A catheter (flexible tube used to put fluids into or take blood out of a vein) with a balloon tip is inserted through the chest and into the pericardium. The balloon is then inflated to make the pericardial opening bigger. The balloon is then deflated and removed. The bigger opening allows the fluid to drain into the pleural cavity. This may be used when an effusion has recurred (come back) after pericardiocentesis or instead of more serious surgery.
Video-assisted thoracoscopic surgery. Surgery that uses a video camera in the chest area that shows an enlarged image on a television screen. This may be preferred since it uses a small incision instead of a larger one.
Superior Vena Cava Syndrome
Key Points
Superior vena cava syndrome (SVCS) is a group of signs and symptoms that occur when the superior vena cava is partly blocked.
SVCS is usually caused by cancer.
Common signs and symptoms of SVCS include breathing problems and coughing.
Tests are done to find and diagnose the blockage.
Treatment for SVCS caused by cancer depends on the cause, signs and symptoms, and prognosis.
Treatments for SVCS include watchful waiting, chemotherapy, radiation therapy, thrombolysis, stent placement, and surgery.
Palliative care may be given to relieve signs and symptoms of SVCS.
Superior vena cava syndrome (SVCS) is a group of signs and symptoms that occur when the superior vena cava is partly blocked.
The superior vena cava is a major vein that leads to the heart. The heart is divided into four parts. The right and left atrium make up the top parts of the heart and the right and left ventricle make up the bottom parts of the heart. The right atrium of the heart receives blood from two major veins:
The superior vena cava returns blood from the upper body to the heart.
Different conditions can slow the flow of blood through the superior vena cava. These include a tumor in the chest, nearby lymph nodes that are swollen (from cancer), or a blood clot in the superior vena cava. The vein may become completely blocked. Sometimes, smaller veins in the area become larger and take over for the superior vena cava if it is blocked, but this takes time. Superior vena cava syndrome (SVCS) is the group of signs and symptoms that occur when this vein is partly blocked.
SVCS is usually caused by cancer.
SVCS is usually caused by cancer. In adults, SVCS is most common in the following types of cancer:
A blood clot that forms during the use of an intravenouscatheter (flexible tube used to put fluids into or take blood out of a vein) in the superior vena cava. A clot may also be caused by pacemaker wires.
Infection or cancer in the chest that causes affected tissues to become thick and hard.
Common signs and symptoms of SVCS include breathing problems and coughing.
The signs and symptoms of SVCS are more severe if the vein becomes blocked quickly. This is because the other veins in the area do not have time to widen and take over the blood flow that cannot pass through the superior vena cava.
The most common signs are:
Trouble breathing.
Coughing.
Swelling in the face, neck, upper body, or arms.
Less common signs and symptoms include the following:
Hoarse voice.
Trouble swallowing or talking.
Coughing up blood.
Swollen veins in the chest or neck.
Chest pain.
Rapid breathing.
Tests are done to find and diagnose the blockage.
The following tests may be done to diagnose SVCS and find the blockage:
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. The radiologist will look for any masses, a pleural effusion, a collapsed lung, or an enlarged heart. EnlargeA chest x-ray is used to take pictures of the structures and organs inside the chest. X-rays pass through the patient’s body onto film or a computer.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the chest, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Venography: A procedure to x-ray veins. A contrast dye is injected into the veins to outline them on the x-rays.
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Ultrasound: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
It is important to find out the cause of SVCS before starting treatment. The type of cancer can affect the type of treatment needed. Unless the airway is blocked or the brain is swelling, waiting to start treatment while a diagnosis is made usually causes no problem in adults. If doctors think lung cancer is causing the problem, a sputum sample may be taken and a biopsy may be done.
Treatment for SVCS caused by cancer depends on the cause, signs and symptoms, and prognosis.
Treatment for SCVS caused by cancer depends on the following:
Whether treatment is meant to cure, control, or relieve the signs and symptoms of cancer.
The patient’s wishes.
Treatments for SVCS include watchful waiting, chemotherapy, radiation therapy, thrombolysis, stent placement, and surgery.
Watchful waiting. Watchful waiting is closely monitoring a patient’s condition without giving any treatment unless signs or symptoms appear or change. A patient who has good blood flow through smaller veins in the area and mild symptoms may not need treatment.
The following may be used to relieve signs or symptoms and keep the patient comfortable:
Keeping the upper body raised higher than the lower body.
Diuretics (drugs that make excess fluid pass from the body in urine). Patients taking diuretics are closely watched because these drugs can cause dehydration (loss of too much fluid from the body).
Chemotherapy. Chemotherapy is the usual treatment for tumors that respond to anticancer drugs, including small cell lung cancer and lymphoma. Chemotherapy stops the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Radiation therapy. If the blockage of the superior vena cava is caused by a tumor that does not usually respond to chemotherapy, radiation therapy may be given. Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Thrombolysis. SVCS may occur when a thrombus (blood clot) forms in a partly blocked vein. Thrombolysis is a way to break up and remove blood clots. This may done by a thrombectomy. Thrombectomy is surgery to remove the blood clot or the use of a device inserted into the vein to remove the blood clot. This may be done with or without the use of drugs to break up the clot.
Stent placement. If the superior vena cava is partly blocked by the tumor, an expandable stent (tube) may be placed inside the superior vena cava to help keep it open and allow blood to pass through. This helps most patients. Drugs to keep more blood clots from forming may also be used.
Surgery. Surgery to bypass (go around) the blocked part of the vein is sometimes used for cancer patients, but is used more often for patients who do not have cancer.
Palliative care may be given to relieve signs and symptoms of SVCS.
The signs and symptoms of superior vena cava syndrome can be upsetting. It is important that you and your family ask questions about superior vena cava syndrome and how to treat it. This can help relieve anxiety about signs and symptoms such as swelling, trouble swallowing, coughing, and hoarseness.
If you have advanced cancer you may decide not to have any more treatment. Palliative care can help keep you comfortable by relieving signs and symptoms to improve your quality of life.
Superior Vena Cava Syndrome in Children
Key Points
Superior vena cava syndrome (SVCS) in a child is a serious medical emergency because the child’s windpipe can become blocked.
The most common symptoms of SVCS in children are a lot like those in adults.
The most common cause of SVCS in children is non-Hodgkin lymphoma.
SVCS in children may be diagnosed and treated before a diagnosis of cancer is made.
Treatment for SVCS in children may include radiation therapy, drugs, or surgery.
Superior vena cava syndrome (SVCS) in a child is a serious medical emergency because the child’s windpipe can become blocked.
Superior vena cava syndrome (SVCS) is rare in children, but when it occurs, it can be life-threatening. In adults, the windpipe is stiff, but in children, it is softer and can more easily be squeezed shut or blocked. A child’s windpipe is narrow, so any amount of swelling can cause breathing problems. Squeezing of the trachea is called superior mediastinalsyndrome (SMS). Because SVCS and SMS usually happen together in children, the two syndromes are considered to be the same.
The most common symptoms of SVCS in children are a lot like those in adults.
SVCS in children may be diagnosed and treated before a diagnosis of cancer is made.
A physical exam, chest x-ray, and medical history are usually all that are needed to diagnose superior vena cava syndrome in children. Even if doctors think cancer is causing SVCS, a biopsy may not be done. This is because the lungs and heart of a child with SVCS may not be able to handle the anesthesia needed. Other imaging tests may be done to help find out if anesthesia can be safely used. In most cases, treatment for SVCS will begin before a diagnosis of cancer is made.
Treatment for SVCS in children may include radiation therapy, drugs, or surgery.
There are several ways to treat SVCS in children.
Radiation therapy. Radiation therapy is usually used to treat a tumor that is blocking the vein. After radiation therapy, there may be more trouble breathing because swelling narrows the windpipe. A drug to reduce swelling or tumor size may be given.
Drugs. Chemotherapy, steroids, or other drugs may be used.
Surgery. Surgery may be needed to bypass (go around) the blocked part of the vein or to place a stent (thin tube) to open the vein.
Current Clinical Trials
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the pathophysiology and treatment of cardiopulmonary syndromes, including dyspnea, malignant pleural effusion, malignant pericardial effusion, and superior vena cava syndrome. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Cardiopulmonary Syndromes. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/cardiopulmonary-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389457]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
After finding the cause of ascites and reviewing your symptoms, your doctor will talk with you about treatment options.
Credit: iStock
What is ascites?
Ascites is the abnormal buildup of fluid in your belly (abdomen) that may cause swelling. It occurs when fluid builds up between the two layers of tissue, called the peritoneum, that cover the organs in your abdomen.
Causes of ascites
Certain types of cancer may cause ascites, especially advanced cancer that
Ascites may also be caused by conditions that are not related to cancer. The most common cause of ascites is a liver disease called cirrhosis, kidney failure, chronic hepatitis, congestive heart failure, and infection. Ascites may develop slowly or rapidly, depending on what is causing it.
The peritoneal cavity is the space that contains most of the organs in the abdomen, including the liver, stomach, and intestines. Ascites is as an abnormal buildup of fluid in the peritoneal cavity that may cause swelling.
Ascites may cause the following signs and symptoms:
abdominal swelling
bloating that causes an enlarged and painful belly
weight gain and/or clothes that become tight
shortness of breath and coughing, as more fluid collects
Additional symptoms of ascites may include appetite loss, constipation, fatigue, fever, nausea, vomiting, and swelling in your ankles or legs.
How is ascites diagnosed?
Your doctor will perform a physical exam. These procedures and tests may also be used to diagnose and determine what is causing ascites:
Scans: Often an imaging test such as ultrasound or a CT scan is used to see if the tissues and organs in your abdomen are surrounded by excess fluid. Sometimes an MRI may be advised.
Paracentesis: This medical procedure uses a needle and catheter to remove ascitic fluid from your abdomen or belly area (the peritoneal cavity). The ascitic fluid is then analyzed. Paracentesis may be used to both diagnose the cause of the ascites and to provide relief from symptoms caused by ascites.
Ascitic fluid analysis: After the fluid is collected using paracentesis, it is analyzed for cancer cells as well as infectious agents, proteins, and other substances to determine what is causing the buildup of fluid. If cancer cells are found in the fluid, it means that you have malignant ascites.
Treatment and management of ascites
Treatment for malignant ascites is based on the severity of your symptoms, as well as the type and extent of the cancer. Treatments include:
Cancer treatment: Sometimes cancer treatments, such as chemo, hormone therapy, or surgery, may be used to help lower symptoms caused by ascites. Cancer treatments work by shrinking the tumor so it does not produce the fluid that causes ascites.
Diet: You may be advised to avoid foods high in sodium (salt), which can cause the body to retain fluid. Avoiding alcohol can also help minimize fluid retention. Your doctor or nurse will talk with you about food and drink choices that are best for you.
Diuretics(sometimes called water pills): Medicines called diuretics are sometimes prescribed to help your body get rid of fluid in your abdomen and other areas of your body. These medicines cause the kidneys to make more urine, but they also come with side effects that your doctor will discuss with you.
Paracentesis: Paracentesis may be used to both diagnose and treat ascites, as explained in the section above. This procedure may provide temporary relief of symptoms, although it may need to be repeated if fluid builds up again.
Surgery: A shunt or catheter is inserted into your abdomen, where it remains in place to help drain the fluid, as needed. If a shunt or catheter is advised, your doctor will help you or your caregivers learn how to drain it at home.
Talking with your doctor about ascites
Tell your doctor or nurse if you notice abdominal swelling or other symptoms of ascites. They will work to determine the cause of swelling and talk with you about treatment options.
Questions to ask your provider about ascites:
Is the cancer I have or the treatment I’m receiving likely to cause ascites?
What urgent problems should I call you about?
What treatment options do you recommend based on my symptoms?
What are the advantages and disadvantages of the ascites treatment that you recommend for me?
Will treating the cancer help the ascites to go away?
What are the chances that ascites may come back after treatment?
Ascites research and clinical trials
Research studies called clinical trials help find better ways to prevent and treat side effects such as ascites. Your doctor may have information about open clinical trials. You can also search for clinical trials supported by the National Cancer Institute at NCI-supported clinical trials and clinical trials supported by other organizations at ClinicalTrials.gov. For help finding a clinical trial, contact NCI’s Cancer Information Service.
Getting support if you have ascites
Side effects like ascites can be hard to deal with, both physically and emotionally. It’s important to ask for support from your health care team. They can help you prepare for and make it through difficult times. Learn more about ways to cope with cancer, including ways to adjust to daily life during cancer treatment.
For family members and friends who are caring for someone with cancer, you may find these suggestions for caregivers to be helpful.
Good nutrition is important for people with cancer.
Nutrition goals are set for each person with cancer.
A registered dietitian is an important part of the healthcare team.
Cancer and cancer treatments may cause side effects that affect nutrition.
Cancer and cancer treatments may cause malnutrition.
Anorexia and cachexia are common causes of malnutrition in people with cancer.
Good nutrition is important for people with cancer.
Nutrition is a process in which food is taken in and used by the body for growth, to keep the body healthy, and to replace tissue. Good nutrition is important for good health. A healthy diet includes foods and liquids that have important nutrients (vitamins, minerals, proteins, carbohydrates, fats, and water) the body needs.
Nutrition goals are set for each person with cancer.
Nutrition goals during cancer therapy are based on a person’s cancer type, cancer stage, and other medical conditions. Eating the right amount of protein and calories is important for healing, fighting infection, and having enough energy.
A registered dietitian is an important part of the healthcare team.
A registered dietitian (or nutritionist) is a part of the team of health professionals that help with cancer treatment and recovery. A dietitian will work with you, your family, and the rest of the medical team to manage your diet during and after cancer treatment.
Cancer and cancer treatments may cause side effects that affect nutrition.
Cancer and cancer treatments may cause malnutrition.
Cancer and cancer treatments may affect taste, smell, appetite, and the ability to eat enough food or absorb the nutrients from food. This can cause malnutrition, which is a condition caused by a lack of key nutrients.
Malnutrition can cause a person to be weak, tired, and unable to fight infection or finish cancer treatment. As a result, malnutrition can decrease the person’s quality of life and become life-threatening. Malnutrition may get worse if the cancer grows or spreads.
Anorexia and cachexia are common causes of malnutrition in people with cancer.
Anorexia is the loss of appetite or desire to eat. It is a common symptom and the most common cause of malnutrition in people with cancer. Anorexia may occur early in the disease or later, if the cancer grows or spreads. Some people already have anorexia when they are diagnosed with cancer. Most people who have advanced cancer will have anorexia.
Cachexia is a condition marked by weakness, weight loss, and fat and muscle loss. It is common in people with tumors that affect eating and digestion. It can occur in people with cancer who are eating well, but are not storing fat and muscle because of tumor growth.
Some tumors change the way the body uses certain nutrients. The body’s use of protein, carbohydrates, and fat may change when tumors are in the stomach, intestines, or head and neck. A person may seem to be eating enough, but the body may not be able to absorb all the nutrients from the food.
People with cancer may have cachexia and anorexia at the same time (CAS), causing weight loss and decreased lean body mass. Treating high-risk patients to prevent this condition, rather than treating those already diagnosed with CAS, may lead to better outcomes. Olanzapine, a drug used to treat certain mental disorders, has side effects including increased appetite and weight gain. It is being studied in the treatment of CAS with mixed success. More clinical trials are needed to develop the best possible therapies for CAS.
Effects of Cancer Treatment on Nutrition
Key Points
Chemotherapy and Hormone Therapy
Chemotherapy and hormone therapy affect nutrition in different ways.
Chemotherapy and hormone therapy cause different nutrition problems.
Radiation Therapy
Radiation therapy kills cells in the treatment area.
Radiation therapy may affect nutrition.
Surgery
Surgery increases the body’s need for nutrients and energy.
Surgery to the head, neck, esophagus, stomach, or intestines may affect nutrition.
Immunotherapy
Immunotherapy may affect nutrition.
Stem Cell Transplant
People who receive a stem cell transplant have special nutrition needs.
Chemotherapy and Hormone Therapy
Chemotherapy and hormone therapy affect nutrition in different ways.
Chemotherapy affects cells all through the body. Chemotherapy uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. Healthy cells that normally grow and divide quickly may also be killed. These include cells in the mouth and digestive tract.
Hormone therapy adds, blocks, or removes hormones. It may be used to slow or stop the growth of certain cancers. Some types of hormone therapy may cause weight gain.
Chemotherapy and hormone therapy cause different nutrition problems.
Side effects from chemotherapy may cause problems with eating and digestion. When more than one chemotherapy drug is given, each drug may cause different side effects, or when drugs cause the same side effect, the side effect may be more severe.
Radiation therapy to any part of the digestive system has side effects that cause nutrition problems. Most of the side effects begin two to three weeks after radiation therapy begins and go away a few weeks after it is finished. Some side effects can continue for months or years after treatment ends.
The following are some of the more common side effects:
For radiation therapy to the brain or head and neck
Loss of appetite.
Nausea.
Vomiting.
Dry mouth or thick saliva. Medication may be given to treat a dry mouth.
Surgery to the head, neck, esophagus, stomach, or intestines may affect nutrition.
Most people with cancer are treated with surgery. Surgery that removes all or part of certain organs can affect a person’s ability to eat and digest food.
The following are nutrition problems caused by surgery:
Loss of appetite.
Trouble chewing.
Trouble swallowing.
Feeling full after eating a small amount of food.
Immunotherapy
Immunotherapy may affect nutrition.
The side effects of immunotherapy are different for each person and the type of immunotherapy drug given.
People who receive a stem cell transplant have special nutrition needs.
Chemotherapy, radiation therapy, and other medicines used before or during a stem cell transplant may cause side effects that keep a person from eating and digesting food as usual.
People who receive a stem cell transplant have a high risk of infection. Chemotherapy or radiation therapy given before the transplant decrease the number of white blood cells, which fight infection. It is important that these people learn about safe food handling and avoid foods that may cause infection.
After a stem cell transplant, people are at risk for acute or chronic graft-versus-host disease (GVHD). GVHD may affect the gastrointestinal tract or liver and change the person’s ability to eat or absorb nutrients from food.
Nutrition Assessment in Cancer Care
Key Points
The healthcare team may ask questions about diet and weight history.
Counseling and diet changes are made to improve the person’s nutrition.
The goal of nutrition therapy for people who have advanced cancer depends on the overall plan of care.
The healthcare team may ask questions about diet and weight history.
Ability to walk and do other activities of daily living (dressing, getting into or out of a bed or chair, taking a bath or shower, and using the toilet).
A physical exam is done. Your doctor will check for signs of weight, fat, and muscle loss, and for fluid buildup in your body.
Counseling and diet changes are made to improve the person’s nutrition.
A registered dietitian can counsel you and your family on ways to improve your nutrition. The registered dietitian gives care based on your nutritional and dietary needs during cancer treatment and recovery. Changes to the diet are made to help decrease symptoms from cancer or cancer treatment. These changes may be in the types and amount of food, how often you eat, and how food is eaten (for example, at a certain temperature or taken with a straw).
In addition to the dietitian, the healthcare team may include the following:
People with advanced cancer may be treated with anticancer therapy and palliative care, palliative care alone, or may be in hospice care. Nutrition goals will be different for each person. Some types of treatment may be stopped.
As the focus of care goes from cancer treatment to hospice or end-of-life care, nutrition therapy may become less aggressive to keep the person as comfortable as possible. For more information, see the Nutrition Needs at End of Life section.
Treatment of Symptoms
Key Points
Anorexia
Nausea
Vomiting
Dry Mouth
Mouth Sores
Taste Changes
Sore Throat and Trouble Swallowing
Lactose Intolerance
Weight Gain
When side effects of cancer or cancer treatment affect normal eating, changes can be made to help you get the nutrients you need. Eating foods that are high in calories, protein, vitamins, and minerals is important. Meals should be planned to meet your nutritional needs and tastes in food.
The following are common symptoms caused by cancer and cancer treatment and ways to treat or control them.
Anorexia
The following may help people with cancer who have anorexia (loss of appetite or desire to eat):
Eat foods that are high in protein and calories. The following are high-protein food choices:
Beans.
Chicken.
Fish.
Meat.
Yogurt.
Eggs.
Add extra protein and calories to food, such as using protein-fortified milk.
Eat high-protein foods first in your meal when your appetite is strongest.
Sip only small amounts of liquids during meals.
Drink milkshakes, smoothies, juices, or soups if you do not feel like eating solid foods.
Eat foods that smell good.
Try new foods and new recipes.
Try blenderized drinks that are high in nutrients (check with your doctor or registered dietitian first).
Eat small meals and healthy snacks often throughout the day.
Eat larger meals when you feel well and are rested.
Eat your largest meal when you feel hungriest, whether at breakfast, lunch, or dinner.
Make and store small amounts of favorite foods so they are ready to eat when you are hungry.
Be as active as possible so that you will have a good appetite.
Brush your teeth and rinse your mouth to relieve symptoms and aftertastes.
Talk to your doctor or registered dietitian if you have eating problems such as nausea, vomiting, or changes in how foods taste and smell.
If these diet changes do not help with the anorexia, tube feedings may be needed.
The following may help people with cancer control nausea:
Choose foods that appeal to you. Do not force yourself to eat food that makes you feel sick. Do not eat your favorite foods, to avoid linking them to being sick.
Eat foods that are bland, soft, and easy-to-digest, rather than heavy meals.
Eat dry foods such as crackers, bread sticks, or toast throughout the day.
Eat foods that are easy on your stomach, such as white toast, plain yogurt, and clear broth.
Eat dry toast or crackers before getting out of bed if you have nausea in the morning.
Eat foods and drink liquids at room temperature (not too hot or too cold).
Slowly sip liquids throughout the day.
Suck on hard candies such as peppermints or lemon drops if your mouth has a bad taste.
Stay away from foods and drinks with strong smells.
Eat 5 or 6 small meals every day instead of 3 large meals.
Sip on only small amounts of liquid during meals to avoid feeling full or bloated.
Do not skip meals and snacks. An empty stomach may make your nausea worse.
Rinse your mouth before and after eating.
Don’t eat in a room that has cooking odors or that is very warm. Keep the living space at a comfortable temperature and well-ventilated.
Sit up or lie with your head raised for one hour after eating.
Plan the best times for you to eat and drink.
Relax before each cancer treatment.
Wear clothes that are loose and comfortable.
Keep a record of when you feel nausea and why.
Talk with your doctor about using antinausea medicine.
Vomiting
The following may help people with cancer control vomiting:
Do not eat or drink anything until the vomiting stops.
Drink small amounts of clear liquids after vomiting stops.
After you are able to drink clear liquids without vomiting, drink liquids such as strained soups, or milkshakes, that are easy on your stomach.
Eat 5 or 6 small meals every day instead of 3 large meals.
Sit upright and bend forward after vomiting.
Ask your doctor to order medicine to prevent or control vomiting.
Dry Mouth
The following may help people with cancer who have dry mouth:
Eat foods that are easy to swallow.
Moisten food with sauce, gravy, or salad dressing.
Eat foods and drinks that are very sweet or tart, such as lemonade, to help make more saliva.
Chew gum or suck on hard candy, ice pops, or ice chips.
Check your mouth each day for sores, white patches, or puffy and red areas.
Rinse your mouth 3 to 4 times a day. Mix ¼ teaspoon baking soda, ⅛ teaspoon salt, and 1 cup warm water for a mouth rinse. Do not use mouthwash that contains alcohol.
Do not use toothpicks or other sharp objects.
Taste Changes
The following may help people with cancer who have taste changes:
Eat poultry, fish, eggs, and cheese instead of red meat.
Add spices and sauces to foods (marinate foods).
Eat meat with something sweet, such as cranberry sauce, jelly, or applesauce.
Try tart foods and drinks.
Use sugar-free lemon drops, gum, or mints if there is a metallic or bitter taste in your mouth.
Use plastic utensils and do not drink directly from metal containers if foods have a metal taste.
Try to eat your favorite foods, if you are not nauseated. Try new foods when feeling your best.
Find nonmeat, high-protein recipes in a vegetarian or Chinese cookbook.
Chew food longer to allow more contact with taste buds, if food tastes dull but not unpleasant.
Keep foods and drinks covered, drink through a straw, turn a kitchen fan on when cooking, or cook outdoors if smells bother you.
Brush your teeth and take care of your mouth. Visit your dentist for checkups.
Sore Throat and Trouble Swallowing
The following may help people with cancer who have a sore throat or trouble swallowing:
Eat soft foods that are easy to chew and swallow, such as milkshakes, scrambled eggs, oatmeal, or other cooked cereals.
Eat foods and drinks that are high in protein and calories.
Moisten food with gravy, sauces, broth, or yogurt.
Stay away from the following foods and drinks that can burn or scratch your throat:
Eat calcium-rich vegetables, such as broccoli and greens.
Take lactase tablets when eating or drinking dairy products. Lactase breaks down lactose, so it is easier to digest.
Prepare your own low-lactose or lactose-free foods.
Weight Gain
The following may help people with cancer prevent weight gain:
Eat a lot of fruits and vegetables.
Eat foods that are high in fiber, such as whole-grain breads, cereals, and pasta.
Choose lean meats, such as lean beef, pork trimmed of fat, and poultry (such as chicken or turkey) without skin.
Choose low-fat milk products.
Eat less fat (eat only small amounts of butter, mayonnaise, desserts, and fried foods).
Cook with low-fat methods, such as broiling, steaming, grilling, or roasting.
Eat less salt.
Eat foods that you enjoy so you feel satisfied.
Eat only when hungry. Consider counseling or medicine if you eat because of stress, fear, or depression. If you eat because you are bored, find activities you enjoy.
Eat smaller amounts of food at meals.
Exercise daily.
Talk with your doctor before going on a diet to lose weight.
Types of Nutrition Support
Key Points
Nutrition support helps people who cannot eat or digest food normally.
Nutrition support can be given in different ways.
Enteral Nutrition
Enteral nutrition is also called tube feeding.
Parenteral Nutrition
Parenteral nutrition carries nutrients directly into the blood stream.
The catheter may be placed into a vein in the chest or in the arm.
Nutrition support helps people who cannot eat or digest food normally.
It is best to take in food by mouth whenever possible. Some people may not be able to take in enough food by mouth because of problems from cancer or cancer treatment.
A person who is not able to take in the right amount of calories and nutrients by mouth may be fed using the following:
Enteral nutrition: Nutrients are given through a tube inserted into the stomach or intestines.
Parenteral nutrition: Nutrients are infused into the bloodstream.
Nutrition support can improve a person’s quality of life during cancer treatment, but may cause problems that should be considered before making the decision to use it. The patient, family, and healthcare team should discuss the harms and benefits of each type of nutrition support. For more information on the use of nutrition support at the end of life, see the Nutrition Needs at End of Life section.
Enteral Nutrition
Enteral nutrition is also called tube feeding.
Enteral nutrition gives the patient nutrients in liquid form (formula) through a tube that is placed into the stomach or small intestine. The following types of feeding tubes may be used:
A nasogastric tube is inserted through the nose and down the throat into the stomach or small intestine. This is used when enteral nutrition is only needed for a few weeks.
A gastrostomy tube is inserted into the stomach, or a jejunostomy tube is inserted into the small intestine through an opening made on the outside of the abdomen. This is usually used for long-term enteral feeding or for people who cannot use a tube in the nose and throat.
The type of formula used is based on the person’s specific needs. There are formulas for people who have special health conditions, such as diabetes, or other needs, such as religious or cultural diets.
Parenteral Nutrition
Parenteral nutrition carries nutrients directly into the blood stream.
Parenteral nutrition is used when a person cannot take food by mouth or by enteral feeding. Parenteral feeding does not use the stomach or intestines to digest food. Nutrients are given to the patient directly into the blood, through a catheter inserted into a vein. These nutrients include proteins, fats, vitamins, and minerals.
The catheter may be placed into a vein in the chest or in the arm.
A central venous access catheter is placed beneath the skin and into a large vein in the upper chest. The catheter is put in place by a surgeon. This type of catheter is used for long-term parenteral feeding.
EnlargeCentral venous catheter. A central venous catheter is a thin, flexible tube that is inserted into a vein, usually below the right collarbone, and guided (threaded) into a large vein above the right side of the heart called the superior vena cava. It is used to give intravenous fluids, blood transfusions, chemotherapy, and other drugs. The catheter is also used for taking blood samples. It may stay in place for weeks or months and helps avoid the need for repeated needle sticks.
A peripheral venous catheter is placed into a vein in the arm. A peripheral venous catheter is put in place by trained medical staff. This type of catheter is usually used for short-term parenteral feeding for patients who do not have a central venous access catheter.
EnlargePeripheral venous catheter. A peripheral venous catheter is a thin, flexible tube that is inserted into a vein. It is usually inserted into the lower part of the arm or the back of the hand. It is used to give intravenous fluids, blood transfusions, chemotherapy, and other drugs.
The patient is checked often for infection or bleeding at the place where the catheter enters the body.
Medicines to Treat Loss of Appetite and Weight Loss
Key Points
Medicine may be given with nutrition therapy to treat loss of appetite and weight loss.
Different types of medicine may be used to treat loss of appetite and weight loss.
Medicine may be given with nutrition therapy to treat loss of appetite and weight loss.
It is important that cancersymptoms and side effects that affect eating and cause weight loss are treated early. Both nutrition therapy and medicine can help lessen the effects that cancer and its treatment have on weight loss.
Different types of medicine may be used to treat loss of appetite and weight loss.
Medicines that improve appetite and cause weight gain, such as prednisone and megestrol, may be used to treat loss of appetite and weight loss. Studies have shown that the effects of these medicines may not last long, or there may be no effects. Treatment with a combination of medicines may work better than treatment with one medicine but may have more side effects.
Nutrition Needs at End of Life
Key Points
Nutrition needs change at end of life.
People with cancer and their families decide how much nutrition and fluids will be given at the end of life.
People who have problems swallowing may find it easier to swallow thick liquids than thin liquids.
People with cancer often do not feel much hunger at all and may want very little food. Sips of water, ice chips, and mouth care can decrease thirst in the last few days of life. Good communication with the healthcare team is important to understand the patient’s changes in nutrition needs.
People with cancer and their families decide how much nutrition and fluids will be given at the end of life.
People with cancer and their caregivers have the right to make informed decisions. The person’s religious and cultural preferences may affect their decisions. The healthcare team may work with the person’s religious and cultural leaders when making decisions. The healthcare team and a registered dietitian can explain the benefits and risks of using nutrition support for people at the end of life. In most cases, there are more harms than benefits if the person is not expected to live longer than a month.
Possible benefits of nutrition support for people expected to live longer than a month include the following:
Sores and breakdown of the skin where the enteral feeding tube is inserted.
Diarrhea with the use of enteral and parenteral nutrition.
Complications caused by fluid overload (a condition where there is too much fluid in the blood) with the use of enteral and parenteral nutrition.
Nutrition Trends in Cancer
Key Points
Some people with cancer try special diets to improve their prognosis.
Some people with cancer may take dietary supplements.
Some people with cancer try special diets to improve their prognosis.
People with cancer may try special diets to make their treatment work better, preventside effects from treatment, or to treat the cancer itself. However, for most of these special diets, there is no evidence that shows they work.
Vegetarian or vegan diet
It is not known if following a vegetarian or vegan diet can help side effects from cancer treatment or the person’s prognosis. If the person already follows a vegetarian or vegan diet, there is no evidence that shows they should switch to a different diet.
A study in patients with non-muscle-invasivebladder cancer showed some benefits from eating a diet rich in ITC, a phytochemical found in raw cruciferous vegetables. Patients who ate large amounts of cruciferous vegetables were less likely to have two or more recurrences of their disease and a lower risk of their disease becoming muscle-invasive cancer. More research on the benefits of phytochemicals is needed.
Macrobiotic diet
A macrobiotic diet is a high-carbohydrate, low-fat, plant-based diet. No studies have shown that this diet will help people with cancer.
Ketogenic diet
A ketogenic diet limits carbohydrates and increases fat intake. The purpose of the diet is to decrease the amount of glucose (sugar) the tumorcells can use to grow and reproduce. It is a hard diet to follow because exact amounts of fats, carbohydrates, and proteins are needed.
Several clinical trials are recruiting people with glioblastoma to study whether a ketogenic diet affects glioblastoma tumor activity. People with glioblastoma who want to start a ketogenic diet should talk to their doctor and work with a registered dietitian. However, it is not yet known how the diet will affect the tumor or its symptoms.
Similarly, a study comparing the ketogenic diet to a high-fiber, low fat diet in women with ovarian cancer or endometrial cancer found that the ketogenic diet was safe and acceptable. There is not enough evidence to know how the ketogenic diet will affect ovarian or endometrial tumors or their symptoms.
Some people with cancer may take dietary supplements.
A dietary supplement is a product that is added to the diet. It is usually taken by mouth, and usually has one or more dietary ingredients. People with cancer may take dietary supplements to improve their symptoms or treat their cancer.
Vitamin C
Vitamin C is a nutrient that the body needs in small amounts to function and stay healthy. It helps fight infection, heal wounds, and keep tissues healthy. Vitamin C is found in fruits and vegetables. It can also be taken as a dietary supplement. For information about the use of intravenous vitamin C as treatment for people with cancer, see Intravenous Vitamin C.
Studies have shown that taking probiotics during radiation therapy and chemotherapy can help prevent diarrhea caused by those treatments. People with cancer who are receiving radiation therapy to the abdomen or chemotherapy that is known to cause diarrhea may be helped by probiotics. Similarly, studies are looking at potential benefits of taking probiotics for people with cancer who are receiving immunotherapy.
Melatonin
Melatonin is a hormone made by the pineal gland (tiny organ near the center of the brain). Melatonin helps control the body’s sleep cycle. It can also be made in a laboratory and taken as a dietary supplement.
Several small studies have shown that taking a melatonin supplement with chemotherapy and/or radiation therapy for treatment of solid tumors may be helpful. It may help reduce side effects of treatment. Melatonin does not appear to have side effects.
Oral glutamine
Oral glutamine is an amino acid that is being studied for the treatment of diarrhea and mucositis (inflammation of the lining of the digestive system, often seen as mouth sores) caused by chemotherapy or radiation therapy. Oral glutamine may help prevent mucositis or make it less severe.
People with cancer who are receiving radiation therapy to the abdomen may benefit from oral glutamine. Oral glutamine may reduce the severity of diarrhea. This can help people continue with their treatment plan.
American Cancer Society’s Healthy Eating Cookbook: A Celebration of Food, Friends, and Healthy Living. 3rd ed. Atlanta, GA: The American Cancer Society, 2005.
Bloch A, Cassileth BR, Holmes MD, Thomson CA, eds.: Eating Well, Staying Well During and After Cancer. Atlanta, GA: American Cancer Society, 2004.
Ghosh K, Carson L, and Cohen E: Betty Crocker’s Living with Cancer Cookbook: Easy Recipes and Tips Through Treatment and Beyond. New York, NY: Hungry Minds, 2002.
Weihofen DL, Robbins J, Sullivan PA: Easy-to-Swallow, Easy-to-Chew Cookbook: Over 150 Tasty and Nutritious Recipes for People Who Have Difficulty Swallowing. New York, NY: John Wiley & Sons, Inc., 2002.
Wilson JR: I-Can’t-Chew Cookbook: Delicious Soft Diet Recipes for People with Chewing, Swallowing, or Dry Mouth Disorders. Alameda, Calif: Hunter House Inc., 2003.
Current Clinical Trials
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about nutrition before, during, and after cancer treatment. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Nutrition in Cancer Care. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/appetite-loss/nutrition-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389440]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Hot flashes and night sweats are common in people with cancer and survivors.
In women and men, hot flashes and night sweats may be caused by surgery, radiation therapy, and taking certain medications.
Women
Men
Hot flashes and night sweats are common in people with cancer and survivors.
A hot flash is a sudden warm feeling over your face, neck, and chest that may cause you to sweat and your face to turn red. Sweating is your body’s way of lowering body temperature by causing heat loss through your skin. Hot flashes combined with sweats that happen while sleeping are often called night sweats or hot flushes. Hot flashes and night sweats are common in people receiving cancer treatment. Some people continue to have hot flashes and night sweats after cancer treatment.
In women and men, hot flashes and night sweats may be caused by surgery, radiation therapy, and taking certain medications.
Women
Menopause occurs when the ovaries stop making estrogen. Hot flashes and night sweats are common symptoms of menopause. Early menopause is a condition in which the ovaries stop making estrogen at a younger age than usual. Early menopause can occur when both ovaries are removed by surgery, such as a bilateral oophorectomy to lessen the chance cancer will occur or as part of a hysterectomy to treat cancer.
Other treatments that can cause hot flashes and night sweats include:
In men, the testes produce testosterone. Surgery to remove one or both testicles for the treatment of prostate cancer can trigger a set of symptoms that include hot flashes and night sweats. Hormone therapy with gonadotropin-releasing hormone or estrogen also causes these symptoms in men.
Other drug therapy, such as opioids, tricyclic antidepressants, and steroids, may also cause hot flashes and night sweats.
Drug Treatment for Hot Flashes and Night Sweats in People with Cancer and Survivors
Key Points
Hot flashes and night sweats may be controlled with estrogen replacement therapy.
Other drugs may be useful in some people.
Side effects from drug therapy for hot flashes and night sweats may develop.
Hot flashes and night sweats may be controlled with estrogen replacement therapy.
Studies of non-estrogen drugs to treat hot flashes in women with a history of breast cancer have reported that many of them do not work as well as estrogen replacement or have side effects. Megestrol and medroxyprogesterone (drugs like progesterone), certain antidepressants, anticonvulsants, and clonidine (a drug used to treat high blood pressure) are non-estrogen drugs used to control hot flashes.
Side effects from drug therapy for hot flashes and night sweats may develop.
Antidepressants used to treat hot flashes over a short period of time may cause nausea, fatigue, dry mouth, and changes in appetite. Some antidepressants may change how other drugs, such as tamoxifen, work in the body.
Anticonvulsants used to treat hot flashes may cause fatigue, dizziness, and trouble concentrating.
Side effects from drug therapy may vary from person to person, so treatment and dose will be specific to your needs. If one medicine does not improve your symptoms, switching to another medicine may help.
Non-Drug Treatment for Hot Flashes and Night Sweats in People with Cancer and Survivors
Key Points
Treatments that help people cope with stress and anxiety may help manage hot flashes.
Comfort measures may help relieve hot flashes and night sweats.
Herbs and dietary supplements should be used with caution.
Acupuncture has been studied in the treatment of hot flashes.
Treatments that help people cope with stress and anxiety may help manage hot flashes.
Hypnosis has also been used as a treatment for hot flashes. It is a trance-like state that allows you to be more aware, focused, relaxed, and open to suggestion. Under hypnosis, you can concentrate more clearly on a specific thought or feeling without becoming distracted. A therapist helps you to deeply relax and focus on cooling thoughts. This may lower stress levels, balance body temperature, and calm the heart rate and breathing rate.
Cognitive behavioral therapy, relaxation techniques, or hypnosis may help hot flashes and related problems when used together with drug therapy.
Comfort measures may help relieve hot flashes and night sweats.
Comfort measures may be used to treat hot flashes and night sweats related to cancer treatment. Since body temperature goes up before a hot flash, doing the following may control body temperature and help control symptoms:
Studies of vitamin E for the relief of hot flashes show that it is only slightly better than a placebo (pill or procedure that has no effect). Most studies of soy and black cohosh show they are no better than a placebo in reducing hot flashes. Soy is rich in estrogen-like substances, but how it affects cells in the body is unknown. Studies of ground flaxseed and magnesiumoxide to treat hot flashes have shown mixed results.
Claims are made about several other plant-based and natural products as remedies for hot flashes. These include dong quai, milk thistle, red clover, licorice root extract, and chaste tree berry. Since little is known about how these products work or whether they affect the risk of breast cancer, you should talk with your doctor before using them.
Acupuncture has been studied in the treatment of hot flashes.
Pilot studies of acupuncture and randomized clinical trials that compare true acupuncture and sham (placebo) treatment have been done in people with hot flashes and results are mixed. A review of many studies combined showed that acupuncture had slight or no effects in people with breast cancer who had hot flashes. In contrast, a randomized clinical trial that was not included in the review showed that people with breast cancer who were given acupuncture had fewer hot flashes. Another randomized clinical trial showed that breast cancer survivors who were given electroacupuncture had a reduction in hot flash symptoms. To learn more, visit the Vasomotor symptoms section in the health professional version of Acupuncture.
Current Clinical Trials
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the causes and treatment of hot flashes and night sweats. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Hot Flashes and Night Sweats. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/hot-flashes-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389162]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Hot flashes and night sweats are common in cancer survivors, particularly women, but they can also occur in men. Pathophysiologic mechanisms are complex. Treatment options are broad-based and include hormonal agents, nonhormonal pharmacotherapies, and diverse integrative medicine modalities.[1]
Hot flashes occur in approximately two-thirds of postmenopausal women with a history of breast cancer and are associated with night sweats in 44% of these women.[2,3] The severity of hot flashes in patients with breast cancer has been associated with sleep difficulty, higher pain severity, and poor psychological functioning.[4] In premenopausal breast cancer survivors, vasomotor symptoms—including hot flashes and night sweats—have been associated with depression, an effect that may be mediated by sleep disturbance.[5] For most patients with breast cancer or prostate cancer, hot flash intensity is moderate to severe. Sweating can be part of the hot flash complex that characterizes the vasomotor instability of menopause. Physiologically, sweating mediates core body temperature by producing transdermal evaporative heat loss.[6,7] Hot flashes accompanied by sweating that occur during the sleeping hours are often called night sweats.[8] Another synonym found in the literature is hot flushes.
Approximately 20% of women without breast cancer seek medical treatment for postmenopausal symptoms, including symptoms related to vasomotor instability.[9] Vasomotor symptoms resolve spontaneously in most patients in this population, with only 20% of affected women reporting significant hot flashes 4 years after the last menses.[9] There are no comparable data for women with metastatic breast cancer. Three-quarters of men with locally advanced or metastatic prostate cancer treated with medical or surgical orchiectomy experience hot flashes.[10]
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
References
Dalal S, Zhukovsky DS: Pathophysiology and management of hot flashes. J Support Oncol 4 (7): 315-20, 325, 2006 Jul-Aug. [PUBMED Abstract]
Couzi RJ, Helzlsouer KJ, Fetting JH: Prevalence of menopausal symptoms among women with a history of breast cancer and attitudes toward estrogen replacement therapy. J Clin Oncol 13 (11): 2737-44, 1995. [PUBMED Abstract]
Carpenter JS, Andrykowski MA, Cordova M, et al.: Hot flashes in postmenopausal women treated for breast carcinoma: prevalence, severity, correlates, management, and relation to quality of life. Cancer 82 (9): 1682-91, 1998. [PUBMED Abstract]
Chang HY, Jotwani AC, Lai YH, et al.: Hot flashes in breast cancer survivors: Frequency, severity and impact. Breast 27: 116-21, 2016. [PUBMED Abstract]
Accortt EE, Bower JE, Stanton AL, et al.: Depression and vasomotor symptoms in young breast cancer survivors: the mediating role of sleep disturbance. Arch Womens Ment Health 18 (3): 565-8, 2015. [PUBMED Abstract]
8 Causes of Night Sweats. New York, NY: WebMD, 2020. Available online. Last accessed Oct. 19, 2022.
Johnson SR: Menopause and hormone replacement therapy. Med Clin North Am 82 (2): 297-320, 1998. [PUBMED Abstract]
Charig CR, Rundle JS: Flushing. Long-term side effect of orchiectomy in treatment of prostatic carcinoma. Urology 33 (3): 175-8, 1989. [PUBMED Abstract]
Etiology
Causes of menopausal hot flashes include the occurrence of natural menopause, surgical menopause, or chemical menopause. In the cancer patient, chemical menopause may be caused by the following:
Cytotoxic chemotherapy.
Radiation therapy.
Androgen treatment.
Causes of so-called male menopause include the following:
Orchiectomy.
Gonadotropin-releasing hormone use.
Estrogen use.
Drug-associated causes of hot flashes and night sweats in men and women include use of the following:
Tamoxifen.
Aromatase inhibitors.
Opioids.
Tricyclic antidepressants.
Steroids.
Women who are extensive metabolizers of tamoxifen related to CYP2D6 may have more severe hot flashes than do women who are poor metabolizers;[1] however, there are conflicting data surrounding this topic.[2]
References
Lynn Henry N, Rae JM, Li L, et al.: Association between CYP2D6 genotype and tamoxifen-induced hot flashes in a prospective cohort. Breast Cancer Res Treat 117 (3): 571-5, 2009. [PUBMED Abstract]
Jansen LE, Teft WA, Rose RV, et al.: CYP2D6 genotype and endoxifen plasma concentration do not predict hot flash severity during tamoxifen therapy. Breast Cancer Res Treat 171 (3): 701-708, 2018. [PUBMED Abstract]
Primary Interventions
Hormone Replacement Therapy
Estrogen replacement effectively controls hot flashes associated with biological or treatment-associated postmenopausal states in women. The proposed mechanism of action of estrogen replacement therapy is that it ameliorates hot flashes by raising the core body temperature sweating threshold;[1][Level of evidence: I] however, many women have relative or absolute contraindications to estrogen replacement. Physicians and breast cancer survivors often think there is an increased risk of breast cancer recurrence or de novo breast malignancy with hormone replacement therapies and defer hormonal management of postmenopausal symptoms. Methodologically strong data evaluating the risk of breast cancer associated with hormone replacement therapy in healthy women have been minimal, despite strong basic science considerations suggesting the possibility of such a risk.[2]
In May 2002, the Women’s Health Initiative, a large, randomized, placebo-controlled trial of the risks and benefits of estrogen plus progestin in healthy postmenopausal women, was stopped prematurely at a mean follow-up of 5.2 years (±1.3) because of the detection of a 1.26-fold increased risk of breast cancer (95% confidence interval [CI], 1.00–1.59) in women receiving hormone replacement therapy. Tumors among women in the hormone replacement therapy group were slightly larger and more advanced than tumors among women in the placebo group, with a substantial and statistically significant rise in the percentage of abnormal mammograms at first annual screening; such a rise might hinder breast cancer diagnosis and account for the later stage at diagnosis.[3,4][Level of evidence: I] These results are supported by a population-based case-control study suggesting a 1.7-fold increased risk of breast cancer (95% CI, 1.3–2.2) in women using combined hormone replacement therapy. The risk of invasive lobular carcinoma was increased 2.7-fold (95% CI, 1.7–4.3), the risk of invasive ductal carcinoma was increased 1.5-fold (95% CI, 1.1–2.0), and the risk of estrogen receptor–positive/progesterone receptor–positive breast cancer was increased 2.0-fold (95% CI, 1.5–2.7). The increased risk was highest for invasive lobular tumors and in women who used hormone replacement therapy for longer periods. The risk was not increased with unopposed estrogen therapy.[5]
The very limited data available do not indicate an increased risk of breast cancer recurrence with single-agent estrogen use in patients with a history of breast cancer.[6,7] A series of double-blind, placebo-controlled trials suggested that low-dose megestrol acetate is a promising agent for hot flash management in this population.[8][Level of evidence: I];[9][Level of evidence: II] Limited data suggest that brief cycles of intramuscular depot medroxyprogesterone acetate also play a role in the management of hot flashes.[10][Level of evidence: I] The risk associated with progestin use is unknown.[2]
Examples of hormone-based pharmacological treatments for vasomotor symptoms are summarized in Table 1.
Table 1. Hormone-Based Treatment of Vasomotor Symptoms
Drug Category
Medication
Dose
Comment
Reference
IM = intramuscular; PO = by mouth; qd = every day.
Estrogen
Example: 17-beta-estradiol
0.5 mg PO q24h
Multiple routes available; consider use of estrogen/progestin combination products for women with intact uteri.
Numerous nonestrogenic, pharmacological treatment interventions for hot flash management in women with a history of breast cancer and in some men who have undergone androgen deprivation therapy have been evaluated. Options with reported efficacy include the following: [15–17][Level of evidence: I]
One study compared the efficacy and patient preference of venlafaxine, 75 mg once daily, to gabapentin, 300 mg 3 times per day, for the reduction of hot flashes. Sixty-six women with histories of breast cancer were randomly assigned in an open-label fashion to receive venlafaxine or gabapentin for 4 weeks; after a 2-week washout period, they received the opposite treatment for an additional 4 weeks. Both treatments reduced hot flash scores (severity multiplied by frequency) by approximately 66%. However, significantly more women preferred venlafaxine to gabapentin (68% vs. 32%, respectively).[22]
A study using citalopram to evaluate hot flashes examined how much of a reduction in hot flashes was needed to have a positive impact on activities of daily living and general health-related quality of life.[32] The authors reported that hot flashes had to be reduced at least 46% for women to report significant improvements in the degree of bother they experienced in daily activities.
In a randomized study of paroxetine versus placebo in postmenopausal survivors of gynecological cancer, paroxetine significantly reduced the severity and frequency of hot flashes and nighttime awakening attributed to vasomotor symptoms, with improvement in sleep duration.[20][Level of evidence: I]
Agents that have been evaluated in phase II trials but have not shown efficacy include bupropion,[33] aprepitant,[34] and desipramine.[35][Level of evidence: II] Interestingly, these agents do not primarily modulate serotonin. In addition, randomized clinical trials with sertraline have not provided convincing evidence of its efficacy in hot flash management.[36–38][Level of evidence: I]
Examples of nonhormonal pharmacological treatments for vasomotor symptoms are summarized in Table 2.
Table 2. Nonhormonal Treatment of Vasomotor Symptoms
Drug Category
Medication
Dose
Comment
Reference
bid = twice a day; CR = controlled release; ER = extended release; GABA = gamma-aminobutyric acid; IR = immediate release; PO = by mouth; qam = every morning; qhs = once daily at bedtime; VMS = vasomotor symptoms.
If nighttime hot flashes or night sweats are a particular problem without causing much bother during daytime, strategies to simultaneously improve sleep and hot flashes are in order. Limited data exist related to effective treatments that can target both symptoms. One pilot trial evaluated mirtazapine (a tetracyclic antidepressant that mainly affects serotonin) for hot flashes because it is often prescribed for sleep difficulties. Twenty-two women were titrated up to 30 mg per day of mirtazapine at bedtime over a 3-week period; then they could choose 15 mg or 30 mg at bedtime daily for the fourth week. Hot flashes were reduced by approximately 53% in this nonrandomized trial, and women were statistically significantly satisfied with their hot flash control.[44] However, only 16 of the 22 women stayed on the agent for the entire study period because of excessive grogginess. Although this agent could be further studied in a larger randomized trial, it would be particularly important to evaluate the risk/benefit ratio.
In the short term, side effects for antidepressant agents in the doses used to treat hot flashes are minimal and primarily include:
Nausea.
Sedation.
Dry mouth.
Appetite suppression or stimulation.
In the long term, the prevalence of decreased sexual function with the use of SSRIs at doses for treating hot flashes is not known. The anticonvulsants gabapentin and pregabalin can cause sedation, dizziness, and difficulty concentrating, while clonidine can cause dry mouth, sedation, constipation, and insomnia.[25,27,46][Level of evidence: I] Patients respond as individuals to both the efficacy and the toxicity of various medications. Therefore, careful assessment and tailored treatment chosen collaboratively by the provider and patient are needed.
Data indicate that if a medication does not help an individual, switching to another medication—whether a different antidepressant or gabapentin—may be worthwhile. In a randomized phase III trial (NCCTG-N03C5) of gabapentin alone versus gabapentin with an antidepressant in women who had inadequate control of their hot flashes with an antidepressant alone,[47][Level of evidence: I] gabapentin use resulted in an approximately 50% median reduction in hot flash frequency and score, regardless of whether the antidepressant was continued. In other words, for women who were using antidepressants exclusively for the management of hot flashes that were inadequately controlled, initiation of gabapentin with discontinuation of the antidepressant produced results equal to those obtained with combined therapy, resulting in the need for fewer medications. Similarly, in a pilot study of women receiving inadequate benefit from venlafaxine for hot flash reduction, switching to open-label citalopram, 20 mg per day, resulted in a 50% reduction in hot flash frequency and score.[48]
Drug Interactions
Many SSRIs can inhibit the cytochrome P450 enzymes involved in the metabolism of tamoxifen, which is commonly used in the treatment of breast cancer. When SSRIs are being used, drug-drug interactions are noted. Tamoxifen is metabolized by the cytochrome P450 enzyme system, specifically CYP2D6. Wild-type CYP2D6 metabolizes tamoxifen to an active metabolite, 4-hydroxy-N-desmethyl-tamoxifen, also known as endoxifen. A prospective trial evaluating the effects of the coadministration of tamoxifen and paroxetine, a CYP2D6 inhibitor, on tamoxifen metabolism, found that paroxetine coadministration resulted in decreased concentrations of endoxifen. The magnitude of decrease was greater in women with the wild-type CYP2D6 genotype than in those with a variant genotype (P = .03).[49][Level of evidence: II]
In a prospective observational study of 80 women initiating adjuvant tamoxifen therapy for newly diagnosed breast cancer, variant CYP2D6 genotypes and concomitant use of SSRI CYP2D6 inhibitors resulted in reduced endoxifen levels. Variant CYP2D6 genotypes do not produce functional CYP2D6 enzymes.[50][Level of evidence: II] Since this study was published, several researchers have evaluated the clinical implications of this finding.[51];[52–54][Level of evidence: II] One study followed more than 1,300 women for a median of 6.3 years and concluded that women who were poor metabolizers or heterozygous extensive/intermediate metabolizers (hence, less CYP2D6 activity) had higher rates of recurrence, worse event-free survival, and worse disease-free survival than did women who were extensive metabolizers.[53] Similarly, authors of a retrospective cohort study of more than 2,400 women in Ontario, Canada, who were being treated with tamoxifen and had overlapping treatment with an SSRI concluded that women who concomitantly used paroxetine and tamoxifen had an increased risk of death that was proportionate to the amount of time they used these agents together.[54][Level of evidence: II]
The clinical implications of these changes and of other CYP2D6 genotypes [55] have not yet been elucidated, but the pharmacokinetic interaction between tamoxifen and the newer antidepressants used to treat hot flashes merits further study.[56] Likewise, the risk of soy phytoestrogen use on breast cancer recurrence and/or progression has not yet been clarified. Soy phytoestrogens are weak estrogens found in plant foods. In vitro models suggest that these compounds have a biphasic effect on mammary cell proliferation that is dependent on intracellular concentrations of phytoestrogen and estradiol.[57]
Information Specific to Men
Data are scant regarding the pathophysiology and management of hot flashes in men with prostate cancer. The rate of hot flashes in men receiving androgen deprivation therapy is approximately 75%.[58] The limited data suggest that hot flashes in men are related to changes in sex hormone levels that cause instability in the hypothalamic thermoregulatory center. This is analogous to the proposed mechanism of hot flashes that occur in women. As in women with breast cancer, hot flashes impair the quality of life for men with prostate cancer who are receiving androgen deprivation therapy. The vasodilatory neuropeptide, calcitonin gene–related peptide, may be instrumental in the genesis of hot flashes.[58]
In a prespecified secondary analysis of a prostate cancer clinical trial, 93% of men receiving 12 months of androgen deprivation therapy experienced hot flashes. The hot flashes occurred at castrate levels of testosterone, and cessation of hot flashes preceded full recovery of testosterone in most men, with 99% of men reporting resolution of hot flashes.[59][Level of evidence: I]
Cognitive behavioral therapy (CBT) has been studied for the treatment of hot flashes in men undergoing androgen deprivation therapy for prostate cancer.[60][Level of evidence: I] Patients were randomly assigned to a guided self-help CBT regimen that included a booklet and CD with relaxation and breathing exercises, or to treatment as usual. At 6 weeks, those assigned to CBT experienced a statistically significant 40% reduction in hot flash/night sweat symptoms versus a 12% reduction in patients who received treatment as usual. Symptom reduction continued but was not statistically significant at 32 weeks. Adherence to CBT was good, with 88% reading all or more than half of the booklet and 79% using the relaxation CD.
With the exception of clonidine, the agents mentioned previously were effective in treating hot flashes in women have shown similar efficacy rates in men. For more information, see the Other Pharmacological Interventions section.Treatment modalities for men have included the following:[61]
Estrogens.
Progesterone.
SSRIs.
Gabapentin.
One large, multisite study from France [62] randomly assigned men who were taking leuprorelin for prostate cancer to receive venlafaxine, 75 mg; cyproterone acetate (an antiandrogen), 100 mg; or medroxyprogesterone acetate, 20 mg, when they reported at least 14 hot flashes per week. All three treatments significantly reduced hot flashes, with cyproterone acetate resulting in a 100% median reduction, medroxyprogesterone resulting in a 97% reduction, and venlafaxine resulting in a 57% reduction at 8 weeks. More adverse events were reported with cyproterone acetate, including one serious adverse event (dyspnea) attributable to the drug. Venlafaxine was not associated with any serious adverse events and overall had a 20% adverse event rate. Medroxyprogesterone was the best-tolerated drug, with an adverse event rate of 12%, but with one serious event, urticaria. The most frequent side effects for all agents were gastrointestinal issues: nausea, constipation, diarrhea, and abdominal pain.[62]
On the basis of its efficacy in women, the combination of venlafaxine and soy was studied in hot flash reduction in androgen-deprived men.[63][Level of evidence: I] Patients were randomly assigned to receive venlafaxine with soy protein, venlafaxine with milk protein placebo, soy protein with placebo, or dual placebos during a 12-week period. The number and severity of hot flashes fell for all arms during the study period, but there was no significant difference between arms. The authors concluded that neither agent should be used to treat hot flashes in men, that there is a significant placebo effect in the study of hot flash treatment, and that agents demonstrating success for hot flashes in women may not be successful in men.
A small, multicenter, retrospective review evaluated the use of two doses of intramuscular medroxyprogesterone acetate (400 mg and 150 mg) as a single dose to treat and prevent hot flashes associated with luteinizing hormone-releasing hormone agonist therapy for prostate cancer.[14][Level of evidence: III] Of the 48 men studied, 91% experienced symptomatic improvement in hot flashes, and 46% experienced complete resolution of hot flashes. The trial was not powered to detect a difference between the two doses; however, the authors concluded that they would now use the 400-mg dose.
Pilot studies of the efficacy of the SSRIs paroxetine and fluvoxamine suggest that these drugs decrease the frequency and severity of hot flashes in men with prostate cancer.[64,65] As in women with hormonally sensitive tumors, there are concerns about the effects of hormone use on the outcome of prostate cancer, in addition to other well-described side effects.[58]
Cognitive and Behavioral Methods
Comprehensive nonpharmacological interventions have been developed and evaluated for their ability to reduce hot flashes, night sweats, and the related perception of burden or problems. These interventions have typically included the following:[66–69]
Psychoeducation about managing general symptoms, including stress, anxiety, and sexual and other menopausal concerns.
Relaxation exercises, including slow, deep breathing, called paced breathing.
Cognitive restructuring that addresses catastrophizing, negative beliefs, and avoidance behaviors.
Behavioral interventions as a primary or adjunctive modality may also play a role in hot flash management. Core body temperature has been shown to increase before a hot flash;[70] therefore, interventions that control body temperature could improve hot flash management. Some methods of controlling body temperature include the use of the following:
Loose-fitting cotton clothing.
Fans and open windows to keep air circulating.
Since serotonin may be involved as a central hot flash trigger, behavioral interventions such as stress management may modulate serotonin, causing a decrease in hot flashes.
Relaxation training and paced breathing were initially found to decrease hot flash intensity by as much as 40% to 50% in controlled pilot trials;[71,72] however, randomized trials with control arms using a different pace of breathing have not demonstrated significant benefit for paced-breathing interventions.[73,74]
Three large studies [67–69] of similar interventions have been completed using no treatment, usual care, or wait-list control comparison groups. While all of the studies demonstrated significant reductions in problem ratings or bother ratings related to hot flashes and night sweats, none showed actual reductions in hot flash frequency. Only one of the three studies demonstrated some significant improvements in night sweats at some data points.[68] Similar results were seen in a large trial of Internet-based CBT with and without therapist support.[75][Level of evidence: I] Cognitive behavioral interventions may be an important addition to pharmacological treatment to improve a patient’s overall experience with symptoms related to hot flashes. However, data have not supported the sole use of CBT for reducing hot flashes.
Medical hypnosis is a newer intervention for hot flashes that has been shown to be helpful. In medical hypnosis, the provider facilitates a deep relaxation and trance state in the patient and gives suggestions to the subconscious to mitigate the symptom or problem being addressed. For hot flashes, medical hypnosis uses cooling suggestions and stress reduction to prevent rises in core body temperature and to decrease sympathetic activation. On the basis of strong pilot data, a randomized controlled trial of 187 postmenopausal women used an attention-control comparison and demonstrated significantly greater reductions in hot flashes in the hypnosis group than in the control group. The hypnosis intervention was 5 weeks long. At week 6, hot flash frequency was reduced in the hypnosis group by 64%, compared with a 9% reduction in the control group. At week 12, the reduction in the hypnosis group was 75%, compared with a 17% reduction in the control group.[76] Cancer survivors were not included in this study, but previous research has not demonstrated that interventions have a differential effect on hot flashes on the basis of breast cancer history.
Future research on hot flash management may be aided by the development of psychometrically sound assessment tools such as the Hot Flash Related Daily Interference Scale, which evaluates the impact of hot flashes on a wide variety of daily activities.[77]
Integrative Approaches
Herbs/dietary supplements
Numerous herbs and dietary supplements are popularly used for hot flash reduction. Several of these substances have not been well studied in rigorous clinical trials. Furthermore, the biological activity of various over-the-counter supplements has yet to be determined and is far from standardized. Some of the more well-studied agents include soy phytoestrogen, black cohosh, and vitamin E.
Vitamin E, 400 IU twice a day, appears to confer a modest reduction in hot flashes that is only slightly better than that seen with placebo. The reduction in hot flashes is roughly 35% to 40%.[78,79][Level of evidence: I]
Soy has been a dietary supplement of interest for decreasing menopausal symptoms and breast cancer for some time. The interest comes primarily from association studies of a high-soy diet and decreased breast cancer/menopausal symptoms in Asia. Soy is rich in isoflavones, which are part of a much larger class of plant compounds called flavonoids. Among the isoflavones in soy products are three compounds that are responsible for hormonal effects: genistein, daidzein, and glycitein.
Isoflavones are often referred to as phytoestrogens or plant-based estrogens because they have been shown, in cell line and animal studies, to have the ability to bind with the estrogen receptor.[80]
There is some confusion about the mechanisms of action and safety of these plant-based estrogens. Isoflavones have properties that can cause estrogen-like effects in some cells, causing them to proliferate (divide and grow). But in other cells, isoflavones can stop or block estrogen effects, causing unwanted cells to not grow or die. There is continuing debate about the following questions:[81]
What doses and types of soy products inhibit estrogen as a growth factor?
Under what circumstances do soy products inhibit estrogen as a growth factor?
In what doses or circumstances do soy products promote estrogen-related growth?
Definitive answers to these questions are not known, but phytoestrogens continue to be investigated for chemopreventive properties. On the other hand, soy has been well studied in numerous randomized, placebo-controlled trials for its effects on reducing hot flashes.[82–86][Level of evidence: I] Most trials show that soy is no better than placebo in reducing hot flashes.[87][Level of evidence: I];[88] While clinical evidence indicates the general safety of soy products, there are no compelling data that would inspire the use of soy for hot flash management.
Similarly, trials of black cohosh that have been well designed with a randomized, placebo-controlled arm have found that black cohosh is no better than a placebo in reducing hot flashes.[86,89,90][Level of evidence: I] Furthermore, a meta-analysis that included 14 randomized controlled trials of black cohosh concluded there is a lack of evidence to support its use in the treatment of hot flashes.[91]
Black cohosh used to be thought of as having estrogenic properties, but it is now known that black cohosh acts on serotonin receptors. One study evaluated black cohosh, red clover, estrogen and progesterone, and placebo in a randomized, double-blind trial.[92][Level of evidence: I] Each treatment arm was small (n = 22); however, over 12 months, hot flashes were reduced 34% by black cohosh, 57% by red clover, 63% by placebo, and 94% by hormone therapy. Of note, adherence rates were approximately 89% across the four groups during this long-term study. At 12 months, physiological markers such as endometrial thickness, estradiol, estrone, follicle-stimulating hormone, sex hormone–binding globulin, and liver function were not statistically different for those who took either red clover or black cohosh, compared with those who took a placebo. However, because these groups were small, the power for this secondary analysis was not reported, and it was likely underpowered to detect important differences.
Flaxseed is a plant that is part of the genus Linum, native to the area around the eastern Mediterranean and India. Flaxseed is a rich source of fiber, lignans and omega-3 fatty acids. Lignans found in flaxseed are secoisolariciresinol diglucoside and alpha-linolenic acid. Lignans are a type of phytoestrogen (plant estrogen) that, like soy, are thought to have estrogen agonist-antagonist effects as well as antioxidant properties. Lignans are converted by colonic bacteria to enterodiol and enterolactone, which are metabolites believed to have important physiological properties such as decreasing cell proliferation and inhibiting aromatase, 5-alpha reductase, and 17-beta hydroxysteroid activity. Cell line studies have shown properties of aromatase inhibition with enterolactone but less so with enterodiol.[93] It is thought that these properties can reduce the risk of hormone-sensitive cancers.[94–96] In addition, studies have shown that flaxseed can reduce estrogen levels through excretion in the urine.[97,98]
Following preliminary test results of flaxseed for its effect on hot flashes and related endpoints,[99,100][Level of evidence: I] an open-label pilot study evaluated 40 g of flaxseed in decreasing hot flashes. This study of 30 women showed a 57% reduction in hot flash scores and a 50% reduction in hot flash frequency over a 6-week period.[101] However, a follow-up phase III, randomized, controlled trial conducted by the North Central Cancer Treatment Group with 188 women failed to show any benefit of 410 mg of lignans in a flaxseed bar over placebo.[102][Level of evidence: I]
Similarly, on the basis of two pilot studies suggesting that magnesium oxide supplementation significantly reduced hot flashes, a double-blind, randomized, placebo-controlled trial of magnesium oxide, 800 or 1,200 mg daily, versus placebo was conducted in postmenopausal women with a history of breast cancer and symptomatic hot flashes.[103][Level of evidence: I] No benefit was observed for magnesium oxide.
Many other plants and natural products are advertised or marked as remedies for hot flashes. Some of these products, such as red clover, contain phytoestrogens, and some have unknown properties. The agents include dong quai, milk thistle, licorice, and chaste tree berry. There is incomplete understanding of the biology of these agents and whether taking them would impact breast cancer risk or recurrence in a negative or positive way. Data suggest that these plants have different effects, dependent not only on the dose used but also on a woman’s hormone environment when she takes them. Little is known about these agents, and caution is needed with respect to taking them—if a woman is to avoid estrogen supplementation.[104–107]
Acupuncture
Pilot and randomized sham trials have evaluated the use of acupuncture to treat hot flashes.[108–112][Level of evidence: I] Research in acupuncture is difficult to conduct, owing to the lack of novel methodology—specifically, the conundrum of what serves as an adequate control arm. In addition, the philosophy surrounding acupuncture practice is quite individualized, in that two women experiencing hot flashes would not necessarily receive the same treatment. It would be important to study acupuncture utilizing relevant clinical procedures; so far, acceptable research methods to accomplish this are lacking. Therefore, the data with respect to the effect of acupuncture on hot flashes are quite mixed. However, a 2016 meta-analysis of 12 trials studying acupuncture for the treatment of hot flashes in patients with breast cancer showed limited or no effects.[113] Included trials ranged in size from 10 to 84 patients, with 5 to 16 treatment sessions and 1 to 24 months of follow-up. Comparator arms included hormone therapy, relaxation techniques, sham acupuncture, and antidepressants. The authors concluded that acupuncture failed to demonstrate a significant effect on the frequency of hot flashes in a population of breast cancer patients.
In contrast, a randomized controlled trial that was not included in the 2016 meta-analysis showed a statistically significant reduction in hot flash score with acupuncture.[114][Level of evidence: I] The trial randomly assigned women to ten acupuncture sessions plus enhanced self-care versus enhanced self-care alone. Women were included if they had breast cancer; at least moderate-level hot flashes, defined as six or more hot flashes a day; and/or a score of 15 or higher on the Greene Climacteric Scale. Random assignment to acupuncture resulted in fewer hot flashes and higher quality of life. The reduction in hot flash score was maintained through the 3- and 6-month follow-up visits.
In a randomized controlled trial, breast cancer survivors with hot flashes (120 women) were randomly assigned to receive electroacupuncture (using a transcutaneous electrical nerve stimulation unit to induce a current between two acupuncture points) or gabapentin, 900 mg daily, with sham electroacupuncture (needles that did not penetrate the skin and without electricity) and placebo capsules as controls.[24] Electroacupuncture produced the greatest reduction in hot flash symptoms, followed by sham acupuncture, gabapentin, and placebo capsules. In a separately published, prespecified secondary analysis of sleep outcomes in women assigned to the active treatment arms, electroacupuncture was comparable to gabapentin for improving sleep quality; significant associations were seen between reduction in hot flash severity/frequency and improved sleep latency and sleep quality in the full sample.[115]
For more information, see the Vasomotor symptoms section in Acupuncture.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Freedman RR, Blacker CM: Estrogen raises the sweating threshold in postmenopausal women with hot flashes. Fertil Steril 77 (3): 487-90, 2002. [PUBMED Abstract]
Pritchard KI: Hormone replacement in women with a history of breast cancer. Oncologist 6 (4): 353-62, 2001. [PUBMED Abstract]
Writing Group for the Women’s Health Initiative Investigators: Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 288 (3): 321-33, 2002. [PUBMED Abstract]
Chlebowski RT, Hendrix SL, Langer RD, et al.: Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA 289 (24): 3243-53, 2003. [PUBMED Abstract]
Li CI, Malone KE, Porter PL, et al.: Relationship between long durations and different regimens of hormone therapy and risk of breast cancer. JAMA 289 (24): 3254-63, 2003. [PUBMED Abstract]
Vassilopoulou-Sellin R, Asmar L, Hortobagyi GN, et al.: Estrogen replacement therapy after localized breast cancer: clinical outcome of 319 women followed prospectively. J Clin Oncol 17 (5): 1482-7, 1999. [PUBMED Abstract]
Decker DA, Pettinga JE, VanderVelde N, et al.: Estrogen replacement therapy in breast cancer survivors: a matched-controlled series. Menopause 10 (4): 277-85, 2003 Jul-Aug. [PUBMED Abstract]
Goodwin JW, Green SJ, Moinpour CM, et al.: Phase III randomized placebo-controlled trial of two doses of megestrol acetate as treatment for menopausal symptoms in women with breast cancer: Southwest Oncology Group Study 9626. J Clin Oncol 26 (10): 1650-6, 2008. [PUBMED Abstract]
Loprinzi CL, Michalak JC, Quella SK, et al.: Megestrol acetate for the prevention of hot flashes. N Engl J Med 331 (6): 347-52, 1994. [PUBMED Abstract]
Bertelli G, Venturini M, Del Mastro L, et al.: Intramuscular depot medroxyprogesterone versus oral megestrol for the control of postmenopausal hot flashes in breast cancer patients: a randomized study. Ann Oncol 13 (6): 883-8, 2002. [PUBMED Abstract]
Joffe H, Guthrie KA, LaCroix AZ, et al.: Low-dose estradiol and the serotonin-norepinephrine reuptake inhibitor venlafaxine for vasomotor symptoms: a randomized clinical trial. JAMA Intern Med 174 (7): 1058-66, 2014. [PUBMED Abstract]
Loprinzi CL, Levitt R, Barton D, et al.: Phase III comparison of depomedroxyprogesterone acetate to venlafaxine for managing hot flashes: North Central Cancer Treatment Group Trial N99C7. J Clin Oncol 24 (9): 1409-14, 2006. [PUBMED Abstract]
Langenstroer P, Kramer B, Cutting B, et al.: Parenteral medroxyprogesterone for the management of luteinizing hormone releasing hormone induced hot flashes in men with advanced prostate cancer. J Urol 174 (2): 642-5, 2005. [PUBMED Abstract]
Barton D, Loprinzi CL: Making sense of the evidence regarding nonhormonal treatments for hot flashes. Clin J Oncol Nurs 8 (1): 39-42, 2004. [PUBMED Abstract]
Loprinzi CL, Stearns V, Barton D: Centrally active nonhormonal hot flash therapies. Am J Med 118 (Suppl 12B): 118-23, 2005. [PUBMED Abstract]
Loprinzi CL, Barton DL, Sloan JA, et al.: Mayo Clinic and North Central Cancer Treatment Group hot flash studies: a 20-year experience. Menopause 15 (4 Pt 1): 655-60, 2008 Jul-Aug. [PUBMED Abstract]
Loprinzi CL, Kugler JW, Sloan JA, et al.: Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 356 (9247): 2059-63, 2000. [PUBMED Abstract]
Stearns V, Beebe KL, Iyengar M, et al.: Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA 289 (21): 2827-34, 2003. [PUBMED Abstract]
Capriglione S, Plotti F, Montera R, et al.: Role of paroxetine in the management of hot flashes in gynecological cancer survivors: Results of the first randomized single-center controlled trial. Gynecol Oncol 143 (3): 584-588, 2016. [PUBMED Abstract]
Stearns V, Slack R, Greep N, et al.: Paroxetine is an effective treatment for hot flashes: results from a prospective randomized clinical trial. J Clin Oncol 23 (28): 6919-30, 2005. [PUBMED Abstract]
Bordeleau L, Pritchard KI, Loprinzi CL, et al.: Multicenter, randomized, cross-over clinical trial of venlafaxine versus gabapentin for the management of hot flashes in breast cancer survivors. J Clin Oncol 28 (35): 5147-52, 2010. [PUBMED Abstract]
Loprinzi CL, Dueck AC, Khoyratty BS, et al.: A phase III randomized, double-blind, placebo-controlled trial of gabapentin in the management of hot flashes in men (N00CB). Ann Oncol 20 (3): 542-9, 2009. [PUBMED Abstract]
Mao JJ, Bowman MA, Xie SX, et al.: Electroacupuncture Versus Gabapentin for Hot Flashes Among Breast Cancer Survivors: A Randomized Placebo-Controlled Trial. J Clin Oncol 33 (31): 3615-20, 2015. [PUBMED Abstract]
Pandya KJ, Morrow GR, Roscoe JA, et al.: Gabapentin for hot flashes in 420 women with breast cancer: a randomised double-blind placebo-controlled trial. Lancet 366 (9488): 818-24, 2005 Sep 3-9. [PUBMED Abstract]
Biglia N, Sgandurra P, Peano E, et al.: Non-hormonal treatment of hot flushes in breast cancer survivors: gabapentin vs. vitamin E. Climacteric 12 (4): 310-8, 2009. [PUBMED Abstract]
Loprinzi CL, Qin R, Baclueva EP, et al.: Phase III, randomized, double-blind, placebo-controlled evaluation of pregabalin for alleviating hot flashes, N07C1. J Clin Oncol 28 (4): 641-7, 2010. [PUBMED Abstract]
Barton DL, LaVasseur BI, Sloan JA, et al.: Phase III, placebo-controlled trial of three doses of citalopram for the treatment of hot flashes: NCCTG trial N05C9. J Clin Oncol 28 (20): 3278-83, 2010. [PUBMED Abstract]
Loprinzi CL, Sloan JA, Perez EA, et al.: Phase III evaluation of fluoxetine for treatment of hot flashes. J Clin Oncol 20 (6): 1578-83, 2002. [PUBMED Abstract]
Goldberg RM, Loprinzi CL, O’Fallon JR, et al.: Transdermal clonidine for ameliorating tamoxifen-induced hot flashes. J Clin Oncol 12 (1): 155-8, 1994. [PUBMED Abstract]
Pandya KJ, Raubertas RF, Flynn PJ, et al.: Oral clonidine in postmenopausal patients with breast cancer experiencing tamoxifen-induced hot flashes: a University of Rochester Cancer Center Community Clinical Oncology Program study. Ann Intern Med 132 (10): 788-93, 2000. [PUBMED Abstract]
Barton D, Loprinzi C, Diekmann B, et al.: Citalopram for hot flashes: “the rest of the story”. [Abstract] Support Care Cancer 16 (6): A-20-201, 730, 2008.
Pérez DG, Loprinzi CL, Sloan J, et al.: Pilot evaluation of bupropion for the treatment of hot flashes. J Palliat Med 9 (3): 631-7, 2006. [PUBMED Abstract]
Bardia A, Thompson S, Atherton PJ, et al.: Pilot evaluation of aprepitant for the treatment of hot flashes. Support Cancer Ther 3 (4): 240-6, 2006. [PUBMED Abstract]
Barton DL, Loprinzi CL, Atherton P, et al.: Phase II Evaluation of Desipramine for the Treatment of Hot Flashes. Support Cancer Ther 4 (4): 219-24, 2007. [PUBMED Abstract]
Kimmick GG, Lovato J, McQuellon R, et al.: Randomized, double-blind, placebo-controlled, crossover study of sertraline (Zoloft) for the treatment of hot flashes in women with early stage breast cancer taking tamoxifen. Breast J 12 (2): 114-22, 2006 Mar-Apr. [PUBMED Abstract]
Gordon PR, Kerwin JP, Boesen KG, et al.: Sertraline to treat hot flashes: a randomized controlled, double-blind, crossover trial in a general population. Menopause 13 (4): 568-75, 2006 Jul-Aug. [PUBMED Abstract]
Wu MF, Hilsenbeck SG, Tham YL, et al.: The efficacy of sertraline for controlling hot flashes in women with or at high risk of developing breast cancer. Breast Cancer Res Treat 118 (2): 369-75, 2009. [PUBMED Abstract]
Carpenter JS, Guthrie KA, Larson JC, et al.: Effect of escitalopram on hot flash interference: a randomized, controlled trial. Fertil Steril 97 (6): 1399-404.e1, 2012. [PUBMED Abstract]
Freeman EW, Guthrie KA, Caan B, et al.: Efficacy of escitalopram for hot flashes in healthy menopausal women: a randomized controlled trial. JAMA 305 (3): 267-74, 2011. [PUBMED Abstract]
Loibl S, Schwedler K, von Minckwitz G, et al.: Venlafaxine is superior to clonidine as treatment of hot flashes in breast cancer patients–a double-blind, randomized study. Ann Oncol 18 (4): 689-93, 2007. [PUBMED Abstract]
Buijs C, Mom CH, Willemse PH, et al.: Venlafaxine versus clonidine for the treatment of hot flashes in breast cancer patients: a double-blind, randomized cross-over study. Breast Cancer Res Treat 115 (3): 573-80, 2009. [PUBMED Abstract]
Biglia N, Bounous VE, Susini T, et al.: Duloxetine and escitalopram for hot flushes: efficacy and compliance in breast cancer survivors. Eur J Cancer Care (Engl) 27 (1): , 2018. [PUBMED Abstract]
Perez DG, Loprinzi CL, Barton DL, et al.: Pilot evaluation of mirtazapine for the treatment of hot flashes. J Support Oncol 2 (1): 50-6, 2004 Jan-Feb. [PUBMED Abstract]
Boekhout AH, Vincent AD, Dalesio OB, et al.: Management of hot flashes in patients who have breast cancer with venlafaxine and clonidine: a randomized, double-blind, placebo-controlled trial. J Clin Oncol 29 (29): 3862-8, 2011. [PUBMED Abstract]
Guttuso T, Kurlan R, McDermott MP, et al.: Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 101 (2): 337-45, 2003. [PUBMED Abstract]
Loprinzi CL, Kugler JW, Barton DL, et al.: Phase III trial of gabapentin alone or in conjunction with an antidepressant in the management of hot flashes in women who have inadequate control with an antidepressant alone: NCCTG N03C5. J Clin Oncol 25 (3): 308-12, 2007. [PUBMED Abstract]
Loprinzi CL, Flynn PJ, Carpenter LA, et al.: Pilot evaluation of citalopram for the treatment of hot flashes in women with inadequate benefit from venlafaxine. J Palliat Med 8 (5): 924-30, 2005. [PUBMED Abstract]
Stearns V, Johnson MD, Rae JM, et al.: Active tamoxifen metabolite plasma concentrations after coadministration of tamoxifen and the selective serotonin reuptake inhibitor paroxetine. J Natl Cancer Inst 95 (23): 1758-64, 2003. [PUBMED Abstract]
Jin Y, Desta Z, Stearns V, et al.: CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst 97 (1): 30-9, 2005. [PUBMED Abstract]
Desmarais JE, Looper KJ: Interactions between tamoxifen and antidepressants via cytochrome P450 2D6. J Clin Psychiatry 70 (12): 1688-97, 2009. [PUBMED Abstract]
Bijl MJ, van Schaik RH, Lammers LA, et al.: The CYP2D6*4 polymorphism affects breast cancer survival in tamoxifen users. Breast Cancer Res Treat 118 (1): 125-30, 2009. [PUBMED Abstract]
Schroth W, Goetz MP, Hamann U, et al.: Association between CYP2D6 polymorphisms and outcomes among women with early stage breast cancer treated with tamoxifen. JAMA 302 (13): 1429-36, 2009. [PUBMED Abstract]
Kelly CM, Juurlink DN, Gomes T, et al.: Selective serotonin reuptake inhibitors and breast cancer mortality in women receiving tamoxifen: a population based cohort study. BMJ 340: c693, 2010. [PUBMED Abstract]
Bonanni B, Macis D, Maisonneuve P, et al.: Polymorphism in the CYP2D6 tamoxifen-metabolizing gene influences clinical effect but not hot flashes: data from the Italian Tamoxifen Trial. J Clin Oncol 24 (22): 3708-9; author reply 3709, 2006. [PUBMED Abstract]
Goetz MP, Loprinzi CL: A hot flash on tamoxifen metabolism. J Natl Cancer Inst 95 (23): 1734-5, 2003. [PUBMED Abstract]
This P, De La Rochefordière A, Clough K, et al.: Phytoestrogens after breast cancer. Endocr Relat Cancer 8 (2): 129-34, 2001. [PUBMED Abstract]
Spetz AC, Zetterlund EL, Varenhorst E, et al.: Incidence and management of hot flashes in prostate cancer. J Support Oncol 1 (4): 263-6, 269-70, 272-3; discussion 267-8, 271-2, 2003 Nov-Dec. [PUBMED Abstract]
Dosani M, Morris WJ, Tyldesley S, et al.: The Relationship between Hot Flashes and Testosterone Recovery after 12 Months of Androgen Suppression for Men with Localised Prostate Cancer in the ASCENDE-RT Trial. Clin Oncol (R Coll Radiol) 29 (10): 696-701, 2017. [PUBMED Abstract]
Stefanopoulou E, Yousaf O, Grunfeld EA, et al.: A randomised controlled trial of a brief cognitive behavioural intervention for men who have hot flushes following prostate cancer treatment (MANCAN). Psychooncology 24 (9): 1159-66, 2015. [PUBMED Abstract]
Moraska AR, Atherton PJ, Szydlo DW, et al.: Gabapentin for the management of hot flashes in prostate cancer survivors: a longitudinal continuation Study-NCCTG Trial N00CB. J Support Oncol 8 (3): 128-32, 2010 May-Jun. [PUBMED Abstract]
Irani J, Salomon L, Oba R, et al.: Efficacy of venlafaxine, medroxyprogesterone acetate, and cyproterone acetate for the treatment of vasomotor hot flushes in men taking gonadotropin-releasing hormone analogues for prostate cancer: a double-blind, randomised trial. Lancet Oncol 11 (2): 147-54, 2010. [PUBMED Abstract]
Vitolins MZ, Griffin L, Tomlinson WV, et al.: Randomized trial to assess the impact of venlafaxine and soy protein on hot flashes and quality of life in men with prostate cancer. J Clin Oncol 31 (32): 4092-8, 2013. [PUBMED Abstract]
Loprinzi CL, Barton DL, Carpenter LA, et al.: Pilot evaluation of paroxetine for treating hot flashes in men. Mayo Clin Proc 79 (10): 1247-51, 2004. [PUBMED Abstract]
Nishiyama T, Kanazawa S, Watanabe R, et al.: Influence of hot flashes on quality of life in patients with prostate cancer treated with androgen deprivation therapy. Int J Urol 11 (9): 735-41, 2004. [PUBMED Abstract]
Tremblay A, Sheeran L, Aranda SK: Psychoeducational interventions to alleviate hot flashes: a systematic review. Menopause 15 (1): 193-202, 2008 Jan-Feb. [PUBMED Abstract]
Mann E, Smith MJ, Hellier J, et al.: Cognitive behavioural treatment for women who have menopausal symptoms after breast cancer treatment (MENOS 1): a randomised controlled trial. Lancet Oncol 13 (3): 309-18, 2012. [PUBMED Abstract]
Ayers B, Smith M, Hellier J, et al.: Effectiveness of group and self-help cognitive behavior therapy in reducing problematic menopausal hot flushes and night sweats (MENOS 2): a randomized controlled trial. Menopause 19 (7): 749-59, 2012. [PUBMED Abstract]
Duijts SF, van Beurden M, Oldenburg HS, et al.: Efficacy of cognitive behavioral therapy and physical exercise in alleviating treatment-induced menopausal symptoms in patients with breast cancer: results of a randomized, controlled, multicenter trial. J Clin Oncol 30 (33): 4124-33, 2012. [PUBMED Abstract]
Freedman RR, Woodward S: Core body temperature during menopausal hot flushes. Fertil Steril 65 (6): 1141-44, 1996. [PUBMED Abstract]
Freedman RR: Hot flashes: behavioral treatments, mechanisms, and relation to sleep. Am J Med 118 (Suppl 12B): 124-30, 2005. [PUBMED Abstract]
Wijma K, Melin A, Nedstrand E, et al.: Treatment of menopausal symptoms with applied relaxation: a pilot study. J Behav Ther Exp Psychiatry 28 (4): 251-61, 1997. [PUBMED Abstract]
Carpenter JS, Burns DS, Wu J, et al.: Paced respiration for vasomotor and other menopausal symptoms: a randomized, controlled trial. J Gen Intern Med 28 (2): 193-200, 2013. [PUBMED Abstract]
Sood R, Sood A, Wolf SL, et al.: Paced breathing compared with usual breathing for hot flashes. Menopause 20 (2): 179-84, 2013. [PUBMED Abstract]
Atema V, van Leeuwen M, Kieffer JM, et al.: Efficacy of Internet-Based Cognitive Behavioral Therapy for Treatment-Induced Menopausal Symptoms in Breast Cancer Survivors: Results of a Randomized Controlled Trial. J Clin Oncol 37 (10): 809-822, 2019. [PUBMED Abstract]
Elkins GR, Fisher WI, Johnson AK, et al.: Clinical hypnosis in the treatment of postmenopausal hot flashes: a randomized controlled trial. Menopause 20 (3): 291-8, 2013. [PUBMED Abstract]
Carpenter JS: The Hot Flash Related Daily Interference Scale: a tool for assessing the impact of hot flashes on quality of life following breast cancer. J Pain Symptom Manage 22 (6): 979-89, 2001. [PUBMED Abstract]
Barton DL, Loprinzi CL, Quella SK, et al.: Prospective evaluation of vitamin E for hot flashes in breast cancer survivors. J Clin Oncol 16 (2): 495-500, 1998. [PUBMED Abstract]
Ziaei S, Kazemnejad A, Zareai M: The effect of vitamin E on hot flashes in menopausal women. Gynecol Obstet Invest 64 (4): 204-7, 2007. [PUBMED Abstract]
Enderlin CA, Coleman EA, Stewart CB, et al.: Dietary soy intake and breast cancer risk. Oncol Nurs Forum 36 (5): 531-9, 2009. [PUBMED Abstract]
Anastasius N, Boston S, Lacey M, et al.: Evidence that low-dose, long-term genistein treatment inhibits oestradiol-stimulated growth in MCF-7 cells by down-regulation of the PI3-kinase/Akt signalling pathway. J Steroid Biochem Mol Biol 116 (1-2): 50-5, 2009. [PUBMED Abstract]
Quella SK, Loprinzi CL, Barton DL, et al.: Evaluation of soy phytoestrogens for the treatment of hot flashes in breast cancer survivors: A North Central Cancer Treatment Group Trial. J Clin Oncol 18 (5): 1068-74, 2000. [PUBMED Abstract]
Van Patten CL, Olivotto IA, Chambers GK, et al.: Effect of soy phytoestrogens on hot flashes in postmenopausal women with breast cancer: a randomized, controlled clinical trial. J Clin Oncol 20 (6): 1449-55, 2002. [PUBMED Abstract]
St Germain A, Peterson CT, Robinson JG, et al.: Isoflavone-rich or isoflavone-poor soy protein does not reduce menopausal symptoms during 24 weeks of treatment. Menopause 8 (1): 17-26, 2001 Jan-Feb. [PUBMED Abstract]
Nikander E, Kilkkinen A, Metsä-Heikkilä M, et al.: A randomized placebo-controlled crossover trial with phytoestrogens in treatment of menopause in breast cancer patients. Obstet Gynecol 101 (6): 1213-20, 2003. [PUBMED Abstract]
Newton KM, Reed SD, LaCroix AZ, et al.: Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial. Ann Intern Med 145 (12): 869-79, 2006. [PUBMED Abstract]
Reed SD, Newton KM, LaCroix AZ, et al.: Vaginal, endometrial, and reproductive hormone findings: randomized, placebo-controlled trial of black cohosh, multibotanical herbs, and dietary soy for vasomotor symptoms: the Herbal Alternatives for Menopause (HALT) Study. Menopause 15 (1): 51-8, 2008 Jan-Feb. [PUBMED Abstract]
Lethaby AE, Brown J, Marjoribanks J, et al.: Phytoestrogens for vasomotor menopausal symptoms. Cochrane Database Syst Rev (4): CD001395, 2007. [PUBMED Abstract]
Osmers R, Friede M, Liske E, et al.: Efficacy and safety of isopropanolic black cohosh extract for climacteric symptoms. Obstet Gynecol 105 (5 Pt 1): 1074-83, 2005. [PUBMED Abstract]
Pockaj BA, Gallagher JG, Loprinzi CL, et al.: Phase III double-blind, randomized, placebo-controlled crossover trial of black cohosh in the management of hot flashes: NCCTG Trial N01CC1. J Clin Oncol 24 (18): 2836-41, 2006. [PUBMED Abstract]
Fritz H, Seely D, McGowan J, et al.: Black cohosh and breast cancer: a systematic review. Integr Cancer Ther 13 (1): 12-29, 2014. [PUBMED Abstract]
Geller SE, Shulman LP, van Breemen RB, et al.: Safety and efficacy of black cohosh and red clover for the management of vasomotor symptoms: a randomized controlled trial. Menopause 16 (6): 1156-66, 2009 Nov-Dec. [PUBMED Abstract]
Wang C, Mäkelä T, Hase T, et al.: Lignans and flavonoids inhibit aromatase enzyme in human preadipocytes. J Steroid Biochem Mol Biol 50 (3-4): 205-12, 1994. [PUBMED Abstract]
Thompson LU, Chen JM, Li T, et al.: Dietary flaxseed alters tumor biological markers in postmenopausal breast cancer. Clin Cancer Res 11 (10): 3828-35, 2005. [PUBMED Abstract]
Thompson LU, Seidl MM, Rickard SE, et al.: Antitumorigenic effect of a mammalian lignan precursor from flaxseed. Nutr Cancer 26 (2): 159-65, 1996. [PUBMED Abstract]
Touillaud MS, Thiébaut AC, Fournier A, et al.: Dietary lignan intake and postmenopausal breast cancer risk by estrogen and progesterone receptor status. J Natl Cancer Inst 99 (6): 475-86, 2007. [PUBMED Abstract]
Haggans CJ, Hutchins AM, Olson BA, et al.: Effect of flaxseed consumption on urinary estrogen metabolites in postmenopausal women. Nutr Cancer 33 (2): 188-95, 1999. [PUBMED Abstract]
Haggans CJ, Travelli EJ, Thomas W, et al.: The effect of flaxseed and wheat bran consumption on urinary estrogen metabolites in premenopausal women. Cancer Epidemiol Biomarkers Prev 9 (7): 719-25, 2000. [PUBMED Abstract]
Lemay A, Dodin S, Kadri N, et al.: Flaxseed dietary supplement versus hormone replacement therapy in hypercholesterolemic menopausal women. Obstet Gynecol 100 (3): 495-504, 2002. [PUBMED Abstract]
Lewis JE, Nickell LA, Thompson LU, et al.: A randomized controlled trial of the effect of dietary soy and flaxseed muffins on quality of life and hot flashes during menopause. Menopause 13 (4): 631-42, 2006 Jul-Aug. [PUBMED Abstract]
Pruthi S, Thompson SL, Novotny PJ, et al.: Pilot evaluation of flaxseed for the management of hot flashes. J Soc Integr Oncol 5 (3): 106-12, 2007. [PUBMED Abstract]
Pruthi S, Qin R, Terstreip SA, et al.: A phase III, randomized, placebo-controlled, double-blind trial of flaxseed for the treatment of hot flashes: North Central Cancer Treatment Group N08C7. Menopause 19 (1): 48-53, 2012. [PUBMED Abstract]
Park H, Qin R, Smith TJ, et al.: North Central Cancer Treatment Group N10C2 (Alliance): a double-blind placebo-controlled study of magnesium supplements to reduce menopausal hot flashes. Menopause 22 (6): 627-32, 2015. [PUBMED Abstract]
Liu J, Burdette JE, Xu H, et al.: Evaluation of estrogenic activity of plant extracts for the potential treatment of menopausal symptoms. J Agric Food Chem 49 (5): 2472-9, 2001. [PUBMED Abstract]
Tamir S, Eizenberg M, Somjen D, et al.: Estrogenic and antiproliferative properties of glabridin from licorice in human breast cancer cells. Cancer Res 60 (20): 5704-9, 2000. [PUBMED Abstract]
Lau CB, Ho TC, Chan TW, et al.: Use of dong quai (Angelica sinensis) to treat peri- or postmenopausal symptoms in women with breast cancer: is it appropriate? Menopause 12 (6): 734-40, 2005 Nov-Dec. [PUBMED Abstract]
Rotem C, Kaplan B: Phyto-Female Complex for the relief of hot flushes, night sweats and quality of sleep: randomized, controlled, double-blind pilot study. Gynecol Endocrinol 23 (2): 117-22, 2007. [PUBMED Abstract]
Borud EK, Alraek T, White A, et al.: The Acupuncture on Hot Flushes Among Menopausal Women (ACUFLASH) study, a randomized controlled trial. Menopause 16 (3): 484-93, 2009 May-Jun. [PUBMED Abstract]
Hervik J, Mjåland O: Acupuncture for the treatment of hot flashes in breast cancer patients, a randomized, controlled trial. Breast Cancer Res Treat 116 (2): 311-6, 2009. [PUBMED Abstract]
Vincent A, Barton DL, Mandrekar JN, et al.: Acupuncture for hot flashes: a randomized, sham-controlled clinical study. Menopause 14 (1): 45-52, 2007 Jan-Feb. [PUBMED Abstract]
Borud EK, Alraek T, White A, et al.: The effect of TCM acupuncture on hot flushes among menopausal women (ACUFLASH) study: a study protocol of an ongoing multi-centre randomised controlled clinical trial. BMC Complement Altern Med 7: 6, 2007. [PUBMED Abstract]
Liljegren A, Gunnarsson P, Landgren BM, et al.: Reducing vasomotor symptoms with acupuncture in breast cancer patients treated with adjuvant tamoxifen: a randomized controlled trial. Breast Cancer Res Treat 135 (3): 791-8, 2012. [PUBMED Abstract]
Salehi A, Marzban M, Zadeh AR: Acupuncture for treating hot flashes in breast cancer patients: an updated meta-analysis. Support Care Cancer 24 (12): 4895-4899, 2016. [PUBMED Abstract]
Lesi G, Razzini G, Musti MA, et al.: Acupuncture As an Integrative Approach for the Treatment of Hot Flashes in Women With Breast Cancer: A Prospective Multicenter Randomized Controlled Trial (AcCliMaT). J Clin Oncol 34 (15): 1795-802, 2016. [PUBMED Abstract]
Garland SN, Xie SX, Li Q, et al.: Comparative effectiveness of electro-acupuncture versus gabapentin for sleep disturbances in breast cancer survivors with hot flashes: a randomized trial. Menopause 24 (5): 517-523, 2017. [PUBMED Abstract]
Latest Updates to This Summary (10/19/2022)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the pathophysiology and treatment of hot flashes and night sweats. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Hot Flashes and Night Sweats are:
Larry D. Cripe, MD (Indiana University School of Medicine)
Alison Palumbo, PharmD, MPH, BCOP (Oregon Health and Science University Hospital)
Edward B. Perry, MD (VA Connecticut Healthcare System)
Rachel A. Pozzar, PhD, RN (Dana-Farber Cancer Institute)
Megan Reimann, PharmD, BCOP (Total CME)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Hot Flashes and Night Sweats. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/hot-flashes-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389188]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Insomnia symptoms occur in about 33% to 50% of the adult population [1] and are often associated with situational stress, illness, aging, and drug treatment.[2] It is estimated that one-third to one-half of people with cancer experience sleep disturbances.[3,4] Physical illness, pain, hospitalization, drugs and other treatments for cancer, and the psychological impact of a malignant disease may disrupt the sleeping patterns of people with cancer.[5] Adequate sleep may increase the cancer patient’s pain tolerance. Poor sleep adversely affects daytime mood and performance. In the general population, persistent insomnia has been associated with a higher risk of developing clinical anxiety or depression.[6] Sleep disturbances and, ultimately, sleep-wake cycle reversals can be early signs of a developing delirium.
Rapid eye movement (REM) sleep: REM sleep, also known as dream sleep, is the active or paradoxic phase of sleep in which the brain is active.
Non-REM (NREM) sleep: NREM sleep is the quiet or restful phase of sleep. NREM, also referred to as slow-wave sleep, is divided into four stages of progressively deepening sleep based on electroencephalogram findings.
The stages of sleep occur in a repeated pattern or cycle of NREM followed by REM, with each cycle lasting approximately 90 minutes. The sleep cycle is repeated four to six times during a 7- to 8-hour sleep period.[7] The sleep-wake cycle is dictated by an inherent biological clock or circadian rhythm. Disruptions in individual sleep patterns can disrupt the circadian rhythm and impair the sleep cycle.[8]
The Sleep Disorders Classification Committee of the American Academy of Sleep Medicine has identified five major categories of sleep disorders:[9]
Disorders of initiating and maintaining sleep (insomnias).
Sleep-related breathing disorders (sleep apnea).
Disorders of excessive somnolence (hypersomnias).
Disorders of the sleep-wake cycle (circadian rhythm sleep disorders).
Dysfunctions associated with sleep, sleep stages, or partial arousals (parasomnias).
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
References
Schutte-Rodin S, Broch L, Buysse D, et al.: Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med 4 (5): 487-504, 2008. [PUBMED Abstract]
Sateia MJ, Pigeon WR: Identification and management of insomnia. Med Clin North Am 88 (3): 567-96, vii, 2004. [PUBMED Abstract]
Palesh OG, Roscoe JA, Mustian KM, et al.: Prevalence, demographics, and psychological associations of sleep disruption in patients with cancer: University of Rochester Cancer Center-Community Clinical Oncology Program. J Clin Oncol 28 (2): 292-8, 2010. [PUBMED Abstract]
Savard J, Morin CM: Insomnia in the context of cancer: a review of a neglected problem. J Clin Oncol 19 (3): 895-908, 2001. [PUBMED Abstract]
Berger AM: Update on the state of the science: sleep-wake disturbances in adult patients with cancer. Oncol Nurs Forum 36 (4): E165-77, 2009. [PUBMED Abstract]
Ohayon MM, Caulet M, Lemoine P: Comorbidity of mental and insomnia disorders in the general population. Compr Psychiatry 39 (4): 185-97, 1998 Jul-Aug. [PUBMED Abstract]
Hirshkowitz M: Normal human sleep: an overview. Med Clin North Am 88 (3): 551-65, vii, 2004. [PUBMED Abstract]
Hrushesky WJ, Grutsch J, Wood P, et al.: Circadian clock manipulation for cancer prevention and control and the relief of cancer symptoms. Integr Cancer Ther 8 (4): 387-97, 2009. [PUBMED Abstract]
American Academy of Sleep Medicine: The International Classification of Sleep Disorders: Diagnostic & Coding Manual. 2nd ed. American Academy of Sleep Medicine, 2005.
Sleep Disturbances in Cancer Patients
Cancer patients are at great risk of developing insomnia and disorders of the sleep-wake cycle. Insomnia, the most common sleep disturbance in this population, is most often secondary to physical and/or psychological factors related to cancer and/or cancer treatment.[1–6] Anxiety and depression—common psychological responses to the diagnosis of cancer, cancer treatment, and hospitalization—are highly correlated with insomnia.[7,8];[9][Level of evidence: II] In addition, sleep disturbances may be part of cancer-related symptom clusters. For more information, see Symptom Clusters in Cancer.
Sleep disturbances may be exacerbated by paraneoplastic syndromes associated with steroid production and by symptoms associated with tumor invasion, such as:
Draining lesions.
Gastrointestinal (GI) and genitourinary (GU) alterations.
Pain.
Fever.
Cough.
Dyspnea.
Pruritus.
Fatigue.
Sleep disturbance can also vary by diagnosis. In a study of patients with melanoma (n = 124), breast cancer (n = 124), and endometrial cancer (n = 82),[10][Level of evidence: II] symptom profiles differed by diagnosis. Four symptom profiles were identified: minimally symptomatic, insomnia-predominant, very sleepy with upper airway symptoms, and symptomatic with severe dysfunction. Using latent class profile analysis, group differences by cancer diagnosis were identified, as shown in Table 1:
Table 1. Sleep-Disturbance Symptom Profiles by Cancer Diagnosis
Cancer Type
Minimally Symptomatic
Insomnia-Predominant
Very Sleepy With Upper Airway Symptoms
Symptomatic With Severe Dysfunction
Melanoma
X
X
Breast
X
X
Endometrial
X
X
X
X
Differences by disease groups may be associated with treatment regimens and/or other factors.
Medications—including vitamins, corticosteroids, neuroleptics for nausea and vomiting, and sympathomimetics for the treatment of dyspnea—and other treatment factors can negatively impact sleep patterns.
Side effects of treatment that may affect the sleep-wake cycle include the following:[11];[9][Level of evidence: II]
GI disturbances (e.g., incontinence, diarrhea, constipation, or nausea).
GU disturbances (e.g., incontinence, retention, or GU irritation).
Respiratory disturbances.
Fatigue.
Sustained use of the following can cause insomnia:
Sedatives and hypnotics (e.g., glutethimide, benzodiazepines, pentobarbital, chloral hydrate, secobarbital sodium, and amobarbital sodium).
Anticonvulsants (e.g., phenytoin).
Corticosteroids.
Oral contraceptives.
Monoamine oxidase inhibitors.
Methyldopa.
Propranolol.
Atenolol.
Alcohol.
Thyroid preparations.
In addition, withdrawal from the following substances may cause insomnia:
Central nervous system depressants (e.g., barbiturates, opioids, glutethimide, chloral hydrate, methaqualone, ethchlorvynol, alcohol, and over-the-counter and prescription antihistamine sedatives).
Benzodiazepines.
Major tranquilizers.
Tricyclic and monamine oxidase inhibitor antidepressants.
Illicit drugs (e.g., marijuana, cocaine, phencyclidine, and opioids).
Hypnotics can interfere with rapid eye movement (REM) sleep, resulting in increased irritability, apathy, and diminished mental alertness. Abrupt withdrawal of hypnotics and sedatives may lead to symptoms such as:
Nervousness.
Jitteriness.
Seizures.
REM rebound.
REM rebound is a marked increase in REM sleep, with increased frequency and intensity of dreaming, including nightmares.[12] The increased physiological arousal that occurs during REM rebound may be dangerous for patients with peptic ulcers or a history of cardiovascular problems. Newer medications for insomnia have reduced adverse effects.[13]
The sleep of hospitalized patients is likely to be frequently interrupted by treatment schedules, hospital routines, and roommates, which singularly or collectively alter the sleep-wake cycle. Other factors influencing sleep-wake cycles in the hospital setting include patient age, comfort, pain, anxiety, environmental noise, and temperature.[14]
Consequences of sleep disturbances can influence outcomes of therapeutic and supportive care measures.[15] The patient with mild to moderate sleep disturbances may experience irritability and inability to concentrate, which may in turn affect compliance with treatment protocols, the ability to make decisions, and relationships with significant others. Sleep disturbances can also cause depression and anxiety. Supportive care measures are directed toward promoting quality of life and adequate rest.
References
Savard J, Morin CM: Insomnia in the context of cancer: a review of a neglected problem. J Clin Oncol 19 (3): 895-908, 2001. [PUBMED Abstract]
Savard J, Simard S, Blanchet J, et al.: Prevalence, clinical characteristics, and risk factors for insomnia in the context of breast cancer. Sleep 24 (5): 583-90, 2001. [PUBMED Abstract]
Savard J, Simard S, Hervouet S, et al.: Insomnia in men treated with radical prostatectomy for prostate cancer. Psychooncology 14 (2): 147-56, 2005. [PUBMED Abstract]
Otte JL, Carpenter JS, Russell KM, et al.: Prevalence, severity, and correlates of sleep-wake disturbances in long-term breast cancer survivors. J Pain Symptom Manage 39 (3): 535-47, 2010. [PUBMED Abstract]
Lee ES, Lee MK, Kim SH, et al.: Health-related quality of life in survivors with breast cancer 1 year after diagnosis compared with the general population: a prospective cohort study. Ann Surg 253 (1): 101-8, 2011. [PUBMED Abstract]
Wong AK, Wang D, Marco D, et al.: Prevalence, Severity, and Predictors of Insomnia in Advanced Colorectal Cancer. J Pain Symptom Manage 66 (3): e335-e342, 2023. [PUBMED Abstract]
Bardwell WA, Profant J, Casden DR, et al.: The relative importance of specific risk factors for insomnia in women treated for early-stage breast cancer. Psychooncology 17 (1): 9-18, 2008. [PUBMED Abstract]
Palesh OG, Roscoe JA, Mustian KM, et al.: Prevalence, demographics, and psychological associations of sleep disruption in patients with cancer: University of Rochester Cancer Center-Community Clinical Oncology Program. J Clin Oncol 28 (2): 292-8, 2010. [PUBMED Abstract]
Van Onselen C, Cooper BA, Lee K, et al.: Identification of distinct subgroups of breast cancer patients based on self-reported changes in sleep disturbance. Support Care Cancer 20 (10): 2611-9, 2012. [PUBMED Abstract]
Kairaitis K, Madut AS, Subramanian H, et al.: Cancer sleep symptom-related phenotypic clustering differs across three cancer specific patient cohorts. J Sleep Res 31 (5): e13588, 2022. [PUBMED Abstract]
Vena C, Parker K, Cunningham M, et al.: Sleep-wake disturbances in people with cancer part I: an overview of sleep, sleep regulation, and effects of disease and treatment. Oncol Nurs Forum 31 (4): 735-46, 2004. [PUBMED Abstract]
Chouinard G: Issues in the clinical use of benzodiazepines: potency, withdrawal, and rebound. J Clin Psychiatry 65 (Suppl 5): 7-12, 2004. [PUBMED Abstract]
Barbera J, Shapiro C: Benefit-risk assessment of zaleplon in the treatment of insomnia. Drug Saf 28 (4): 301-18, 2005. [PUBMED Abstract]
Boonstra L, Harden K, Jarvis S, et al.: Sleep disturbance in hospitalized recipients of stem cell transplantation. Clin J Oncol Nurs 15 (3): 271-6, 2011. [PUBMED Abstract]
Sateia MJ, Doghramji K, Hauri PJ, et al.: Evaluation of chronic insomnia. An American Academy of Sleep Medicine review. Sleep 23 (2): 243-308, 2000. [PUBMED Abstract]
Assessment
Assessment is the initial step in managing sleep disturbances in people with cancer. Assessment data should include the following:[1]
Documentation of predisposing factors.
Sleep patterns.
Emotional status.
Exercise and activity levels.
Diet.
Symptoms.
Medications.
Caregiver routines.
The sections below outline recommendations for a sleep history and physical examination. Data can be retrieved from multiple sources, such as:[2]
The patient’s subjective report of sleep difficulty.
Objective observations of behavioral and physiological manifestations of sleep disturbances.
Reports from the patient’s significant other regarding the patient’s quality of sleep.
The Insomnia Severity Index, which has been validated in adult oncology populations, is recommended when screening for insomnia in clinical settings.[3,4] In a 2021 study, the Insomnia Severity Index was validated in young adult (18–40 years of age) cancer survivors.[5]
The diagnosis of insomnia is primarily based on a careful, detailed medical and psychiatric history. The American Academy of Sleep Medicine has produced guidelines for the use of polysomnography as an objective tool in evaluating insomnia. The routine polysomnogram includes the monitoring of the following:
Electroencephalography.
Electro-oculography.
Electromyography.
Effort of breathing and air flow.
Oxygen saturation.
Electrocardiography.
Body position.
Polysomnography is the major diagnostic tool for assessment of sleep disorders. It is indicated in the evaluation of suspected sleep-related breathing disorders and periodic limb movement disorder, when the cause of insomnia is uncertain, or when behavioral or pharmacological therapy is unsuccessful.[6]
Sleep disturbances have been shown to change throughout the cancer trajectory, which supports the need to assess sleep throughout the patient’s cancer experience. One descriptive study [7][Level of evidence: II] involving 398 women with breast cancer used the General Sleep Disturbance Scale (GSDS) to identify three different sleep trajectories when self-reported sleep was evaluated beginning before surgery and continuing for 6 months. One group (55% of the sample) had a high level of sleep disturbance throughout the study, defined as scores on the GSDS of about 58 to 60 at all data points. A second group (40% of the sample) was considered to have a low level of sleep disturbance throughout, defined as scores on the GSDS in the low 30s at each data point. The final group (5% of the sample) started out high, with scores around 62, but their scores decreased to below 30 over the first 4 months and remained there through month 6. Participants identified as having a more severe sleep disorder were significantly younger, had more comorbidities, had a lower performance status, and experienced hot flashes. In another study, of 232 women with gynecologic cancers that assessed sleep using the GSDS at six time points over two cycles of chemotherapy, four distinct subgroups of patients with sleep disturbance were identified (Low, 18.5%; Moderate, 43.6%; High, 29.3%; Very High, 8.6%).[8][Level of evidence: II] Participants with the worst sleep disturbance were younger, had a higher body mass index, and were more likely to report depression or back pain.
Sleep disturbances frequently co-occur with cancer-related fatigue and may have common underlying mechanisms. Prospective and multidimensional assessments of these two symptoms were conducted in a study involving patients who were newly diagnosed with stage I through stage IIIA breast cancer (N = 152).[9] Assessments included validated sleep and fatigue questionnaires and objective sleep assessments using wrist actigraphy, which measure sleep-wake patterns and circadian rhythms. Assessments were conducted before initiation of chemotherapy (T1) and during the last week of the fourth cycle of anthracycline-based chemotherapy (T2). Most patients in the group characterized by severe symptoms at T1 were also in a higher-symptoms group at T2. Similarly, many patients in that group at T1 remained in the minimal-symptoms group at T2. From T1 to T2, the average-symptoms group was relatively unstable compared with the severe- and minimal-symptoms groups. At both time points, younger patients reported more severe symptoms, and married patients reported less severe symptoms. Patients who reported more comorbidities, more use of medications, and other indicators of worse health (e.g., higher BMI) were more likely to be in the group characterized by higher symptom severity at both time points.
In addition, stress can contribute to sleep disturbance. A study of 957 patients undergoing chemotherapy treatment for breast, lung, gastrointestinal, or gynecological cancer measured responses to validated stress/resilience assessment instruments (14-item Perceived Stress Scale, 22-item Impact of Event Scale-Revised, 30-item Life Stressor Checklist-Revised, and 10-item Connor-Davidson Resilience Scale). Compared with patients classified in a normative or resilient class, patients in the stressed class had significantly higher levels of sleep disturbance. Also, each of the domains of sleep disturbance within the validated 21-item GSDS (quantity, quality, sleep onset latency, mid-sleep awakening, early awakenings, and excessive daytime sleepiness) and use of medications to help with sleep were statistically significant and crossed clinically meaningful cutoff points for patients in the stressed class.[10]
Risk Factors for Sleep Disorders
Disease factors, including paraneoplastic syndromes with increased steroid production, and symptoms associated with tumor invasion (e.g., obstruction, pain, fever, shortness of breath, pruritus, and fatigue).
Treatment factors, including symptoms related to surgery (e.g., pain, frequent monitoring, and use of opioids), chemotherapy (e.g., exogenous corticosteroids), and symptoms related to chemotherapy.
Medications such as opioids; sedatives/hypnotics; steroids; caffeine/nicotine; some antidepressants; and dietary supplements, including some vitamins, diet pills, and other products promoting weight loss and appetite suppression.
Usual patterns of sleep, including usual bedtime, routine before retiring (e.g., food, bath, and medications), length of time before onset of sleep, and duration of sleep (waking episodes during night, ability to resume sleep, and usual time of awakening).
Characteristics of disturbed sleep (changes after diagnosis, treatment, and/or hospitalization).
The significant other’s perception of the patient’s quantity and quality of sleep.
Family history of sleep disorders.
References
American Academy of Sleep Medicine: The International Classification of Sleep Disorders: Diagnostic & Coding Manual. 2nd ed. American Academy of Sleep Medicine, 2005.
Perlis ML, Jungquist C, Smith MT, et al.: Cognitive Behavioral Treatment of Insomnia: A Session-by-Session Guide. Springer Science+Business Media LLC, 2008.
Bastien CH, Vallières A, Morin CM: Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med 2 (4): 297-307, 2001. [PUBMED Abstract]
Savard MH, Savard J, Simard S, et al.: Empirical validation of the Insomnia Severity Index in cancer patients. Psychooncology 14 (6): 429-41, 2005. [PUBMED Abstract]
Michaud AL, Zhou ES, Chang G, et al.: Validation of the Insomnia Severity Index (ISI) for identifying insomnia in young adult cancer survivors: comparison with a structured clinical diagnostic interview of the DSM-5 (SCID-5). Sleep Med 81: 80-85, 2021. [PUBMED Abstract]
Kushida CA, Littner MR, Morgenthaler T, et al.: Practice parameters for the indications for polysomnography and related procedures: an update for 2005. Sleep 28 (4): 499-521, 2005. [PUBMED Abstract]
Van Onselen C, Cooper BA, Lee K, et al.: Identification of distinct subgroups of breast cancer patients based on self-reported changes in sleep disturbance. Support Care Cancer 20 (10): 2611-9, 2012. [PUBMED Abstract]
Pozzar RA, Hammer MJ, Paul SM, et al.: Distinct sleep disturbance profiles among patients with gynecologic cancer receiving chemotherapy. Gynecol Oncol 163 (2): 419-426, 2021. [PUBMED Abstract]
Fox RS, Ancoli-Israel S, Roesch SC, et al.: Sleep disturbance and cancer-related fatigue symptom cluster in breast cancer patients undergoing chemotherapy. Support Care Cancer 28 (2): 845-855, 2020. [PUBMED Abstract]
Jakovljevic K, Kober KM, Block A, et al.: Higher Levels of Stress Are Associated With a Significant Symptom Burden in Oncology Outpatients Receiving Chemotherapy. J Pain Symptom Manage 61 (1): 24-31.e4, 2021. [PUBMED Abstract]
Management
Management of sleep disturbances should focus on treatment of problems such as:
Falling asleep.
Staying asleep.
Early-morning awakenings.
Other areas to manage include symptoms from cancer and its treatment and the identification and management of environmental and psychological factors. When sleep disturbances are caused by symptoms of cancer or its treatment, measures that control or alleviate symptoms are often the key to resolving sleep disturbances. Management of sleep disturbances combines nonpharmacological and pharmacological approaches individualized for the patient.
Nonpharmacological Management of Sleep Disturbances
Many people who experience insomnia have poor sleep hygiene (such as smoking and drinking excessive alcohol just before bedtime), which can exacerbate or perpetuate insomnia.[1][Level of evidence: III] A complete assessment of sleep hygiene (i.e., time in bed; napping during the day; intake of caffeine, alcohol, or foods that are heavy, spicy, or sugary; exercise; and sleep environment) and use of behavioral management strategies (i.e., fixed bedtime; restrictions on smoking, diet, and excessive alcohol 4–6 hours before bedtime; and increased exercise) may prove effective in reducing sleep disturbances.
Sleep hygiene in an inpatient setting involves modifying the sleep environment to decrease sleep disruption. Minimizing noise, dimming or turning off lights, adjusting room temperature, and consolidating patient care tasks to reduce the number of interruptions can increase the amount of uninterrupted sleep.[2][Level of evidence: IV]
Restructuring negative thoughts, beliefs, and attitudes related to sleep.
Preventing excessive monitoring or worrying about getting enough sleep.
Behavioral strategies include:
Stimulus control.
Sleep restriction.
Both of these strategies seek to limit the time spent in bed that does not involve sleeping.[3–5] Several large randomized trials and meta-analyses provide the evidence base for the efficacy of cognitive behavioral therapy (CBT) for insomnia (CBT-I).[3,6,7] Most of these trials have been in populations of patients without cancer.
Relaxation therapy can be used to achieve both behavioral and cognitive outcomes, particularly when it is combined with imagery. Educational objectives around sleep hygiene are also used to treat insomnia and include content on the following:[4]
Sleeping and waking up at regular times.
Relaxing before bedtime.
Creating a dark, comfortable sleep environment.
Avoiding watching television or working in the bedroom.
Getting ample daylight during nonsleep hours.
Avoiding naps.
Limiting caffeine.
Getting regular exercise but no closer than 3 hours before bedtime.
Practice guidelines from the American Academy of Sleep Medicine clearly state that multicomponent therapy is recommended over single therapies. Because of insufficient evidence about its efficacy, sleep hygiene education is not recommended as a single-modality management approach; other reviews state that sleep hygiene by itself is not effective.[6,8] Information about sleep hygiene should be included in patient education about sleep issues.
Several trials and meta-analyses have shown CBT-I to be at least as effective as conventional pharmacological therapies in treating primary chronic insomnia but without side effects.[6,7,9–11]
A four-arm study (conducted in patients with primary chronic insomnia) that evaluated zolpidem versus CBT versus zolpidem and CBT versus placebo reported a greater effect (P = .05) on sleep-onset latency for both groups involving CBT (change of 44%) versus the group receiving zolpidem alone (change of 29%).[12] Another study, also conducted in patients with primary chronic insomnia, evaluated CBT with temazepam alone versus a combination of CBT and temazepam versus placebo and found that all active treatments were significantly better than placebo and that there was a trend for the most improvement in the combined arm of CBT and temazepam.[13] Both arms with CBT demonstrated greater reductions in time to sleep onset than the pharmacotherapy-alone arm (64% in the combined arm, 55% in the CBT arm, and 47% in the temazepam arm). A meta-analysis examining pharmacological and behavioral studies for persistent insomnia found that pharmacological and behavioral treatments did not differ in magnitude of benefit except for latency to sleep onset, in which greater reductions were found with behavioral therapy.[7]
There are limited data evaluating elements of CBT-I in cancer survivors, and most data are about women with breast cancer. However, there have been at least four randomized controlled trials of CBT-I in cancer survivors.[14–17] The intervention was typically delivered over five to eight weekly, small-group, in-person sessions. One trial included patients with cancer diagnoses other than breast cancer,[16] and results did not differ by cancer diagnosis. All studies showed improvements in numerous sleep parameters over time in the groups receiving CBT-I and demonstrated continued benefits 6 and 12 months later. Two of the four trials did not use active control arms.[14,16]
Most studies using active control arms were in breast cancer survivors. One study compared CBT-I with sleep education and hygiene in 72 women,[15] while the other study used a healthy-eating education control group.[17] In the first study, both groups significantly improved over time, with some significant differences between groups favoring CBT-I for time to fall asleep, time awake after sleep, total sleep time, and overall sleep quality. For example, the group receiving CBT-I improved by 30 minutes in time to fall asleep, compared with 11 minutes in the sleep education and hygiene group.[15]
In the second study, 219 women were randomly assigned to a behavioral therapy group consisting of stimulus control, general sleep hygiene (limiting naps, going to bed and rising at consistent times), and relaxation or to a healthy-eating education control group. The interventions were delivered by trained nurses in person, 2 days before the initiation of chemotherapy, before each chemotherapy treatment, and 30 days after the last chemotherapy treatment. The nurses worked with women assigned to behavioral therapy to individualize and reinforce the behaviors. The Pittsburgh Sleep Quality Index (PSQI) was used to measure subjective sleep quality, complemented by use of a sleep diary and wrist actigraph. Sleep quality significantly improved in the group receiving behavioral therapy, compared with the control group. These differences were also seen in data from the sleep diary and actigraph, with both showing significantly fewer awakenings in the behavioral therapy group.[18] Sleep quality was significantly better at 90 days and at 1 year in the behavioral therapy group, as measured by the PSQI but not the diary or actigraph.[17]
In some places, patients may not have access to in-person, professionally delivered CBT-I. A randomized controlled trial conducted with breast cancer survivors demonstrated that CBT-I delivered via digital media can also produce meaningful clinical improvements, although improvements are not as robust as those produced with professionally delivered CBT-I. This three-armed trial compared video-based CBT-I (VCBT-I) and professionally delivered CBT-I (PCBT-I) with a no-treatment control group in 242 breast cancer survivors. Both the VCBT-I and PCBT-I groups had significantly greater improvements in diary-measured sleep variables, compared with the control group. The patients in the PCBT-I group reported greater improvements in some sleep outcomes and in fatigue and depression levels than did the VCBT-I group.[19]
Table 2. Evidence for Cognitive Behavioral Therapy for Insomnia (CBT-I) in Cancer Survivors
aActigraphy: A technique that uses a small instrument called an actigraph (a watch-like sensory unit) worn on the wrist or ankle to measure body gross motor activity. It is helpful in determining sleep patterns and daytime activity.
bPolysomnography: A test used to diagnose sleep disorders on the basis of sleep-related biophysiological changes.
Both groups improved over time; significant improvement between groups favored CBT-I group in time to fall asleep, time awake after sleep onset, total sleep time, sleep quality (as measured by ISI)
Sleep diary; actigraphy; fatigue, depression/anxiety, and QOL assessments
Significant improvement in time to fall asleep, time awake after sleep onset, sleep efficiency, fatigue, specific QOL outcomes for CBT-I group, compared with control group
Sleep diary; polysomnographyb; ISI; fatigue, depression/anxiety, and QOL assessments
Significant improvement in time to fall asleep, time awake after sleep onset, sleep efficiency, depression/anxiety, and QOL outcomes for CBT group, compared with control group
Sleep diary; ISI; actigraphy; fatigue, depression/anxiety, and QOL assessments
Compared with control group, PCBT-I and VCBT-I groups associated with significant improvement in sleep diary–measured sleep variables; compared with VCBT-I group, PCBT-I group had more improvement in sleep, fatigue, and depression/anxiety outcomes and had higher remission rates for insomnia
CBT-I content: Similar for both groups (stimulus control, sleep restriction, sleep education and hygiene, cognitive restructuring)
Inpatient nonpharmacological management
CBT delivered by psychologists has shown promise for the treatment of insomnia in patients with cancer.[14][Level of evidence: I] A randomized controlled study investigated the effectiveness of a protocol-driven cognitive behavioral intervention for insomnia delivered by oncology nurses.[16][Level of evidence: I] This group intervention consisted of standard CBT components such as stimulus control and sleep restriction. Participants included patients with heterogeneous cancers randomly assigned to receive the intervention (n = 100) or treatment as usual (n = 50). Primary outcomes were sleep diary measures at baseline, posttreatment, and at 6-month follow-up. CBT was associated with significant and sustained improvements in several sleep aspects. These improvements were seen for both subjective (sleep diary) and objective (actigraphy) assessments. Additionally, patients who received CBT showed significant improvements in fatigue, anxiety, and depressive symptoms and reported improved quality of life, compared with patients who received treatment as usual.[16][Level of evidence: I]
A study conducted in cancer survivors demonstrated the benefits of a specialized yoga program to improve sleep quality and reduce medication use. A total of 410 cancer survivors with moderate to severe sleep disturbances were randomly assigned to receive standard care or standard care plus a 4-week yoga intervention delivered in two weekly sessions by trained yoga instructors. The yoga participants showed significant improvement in sleep quality, daytime dysfunction, nighttime awakening, and sleep efficiency, compared with standard-care participants. One major limitation of this study was its limited population generalizability, as most study participants were female, White, married, and well-educated breast cancer survivors. Another major limitation was the lack of an adequate control group with respect to nonspecific effects such as group support and attention.[20]
Exercise interventions have shown positive effects on subjective and objective sleep quality in patients with cancer. A study conducted in Taiwanese patients with lung cancer investigated the effects of a 12-week exercise intervention on sleep quality and rest-activity rhythms.[21] The intervention included a home-based walking exercise regimen (walking at a moderate intensity for 40 minutes, 3 times per week) and weekly exercise counseling. Participants were randomly assigned to either the intervention group (n = 56) or the usual-care group (n = 55). Assessments conducted at baseline, 3 months, and 6 months included a subjective sleep assessment using the PSQI and objective sleep and rest-activity assessment using actigraphy.
Over time, the walking exercise group showed significant improvement in subjective sleep quality (lower PSQI scores) compared with the usual-care group. The walking exercise group also showed improvement in total sleep time (TST), an important objective measure of sleep quality, compared with the usual-care group. Additionally, the positive effects on TST (i.e., increase in TST) were greater in patients with poor rest-activity rhythm at baseline, suggesting more benefits in patients with poor circadian sleep-activity rhythms. The limitations of the study included a lack of blinding, hence a possible placebo effect in the intervention group. Also, despite randomization, the mean amount of baseline moderate physical activity was higher in the usual-care group than in the intervention group.
Other actions or interventions that may promote rest in the hospital or extended-care setting include the following:[22,23]
Keeping the patient’s skin clean and dry.
Giving back rubs and/or massaging areas of the body to bring comfort to the patient (e.g., bony prominences, head and scalp, shoulders, hands, and feet).
Keeping bedding and/or surfaces of support devices (chairs and pillows) clean, dry, and wrinkle-free.
Ensuring adequate bedcovers for warmth.
Regulating fluid intake to avoid frequent awakening for elimination.
Encouraging bowel and bladder elimination before sleep.
Promoting optimal bowel function (increased fluids, dietary fiber, and use of stool softeners and laxatives).
Using a condom catheter for nocturnal incontinence.
Providing a high-protein snack 2 hours before bedtime (e.g., milk, turkey, or other foods high in tryptophan).
Avoiding beverages with caffeine and other stimulants, including dietary supplements that promote metabolism changes and appetite suppression.
Encouraging the patient to dress in loose, soft clothing.
Facilitating comfort through repositioning and support with pillows as needed.
Encouraging activity and being out of bed as much as possible during waking hours.
Encouraging the patient to keep regular bedtime and waking hours and avoid napping during the day.
Minimizing and coordinating necessary bedside contacts.
Psychological interventions are directed toward facilitating the patient’s coping processes through education, support, and reassurance. As the patient learns to cope with the stresses of illness, hospitalization, and treatment, sleep may improve.[24][Level of evidence: IV] Communication, verbalization of concerns, and openness between the patient, family, and health care team should be encouraged. Relaxation exercises and self-hypnosis performed at bedtime can help promote calm and sleep. Cognitive-behavioral interventions that diminish the distress associated with early insomnia and change the goal from “need to sleep” to “just relax” can diminish anxiety and promote sleep.[25]
Pharmacological Management of Sleep-Wake Cycle Disturbances
When cancer survivors experience sleep-wake disturbances, cognitive behavioral intervention counseling should be the first consideration for management. For more information, see the Nonpharmacological Management of Sleep Disturbances section. Resources for education and training in CBT may not be readily available in many cancer centers; therefore, community resources need to be investigated. If CBT is not available or has not been successful, pharmacological management can be considered. In addition, when patients have comorbidities contributing to sleep-wake cycle disturbances (such as hot flashes, uncontrolled pain, anxiety, depression, or other mood disturbances),[26,27] then pharmacological management will probably be necessary. While many pharmacological agents are approved for primary insomnia and many others are used off-label to manage sleep and related symptoms, most of the approved sleep aids have not been studied in cancer populations; therefore, the risk/benefit profiles of these drugs are not delineated in this setting.
Despite the lack of evidence in cancer populations, clinicians widely use pharmacological interventions. Therefore, the following discussion of pharmacological agents and recommendations for use is based on evidence from studies conducted in patients with primary insomnia and clinical experience.[4,28,29]
Several classes of medications are used to treat sleep-wake cycle disturbances, including the following:
Antidepressants (e.g., trazodone) and antipsychotics (e.g., quetiapine) that have sedative effects.
Drug characteristics to consider before a drug is chosen to treat an individual patient include the following:
Absorption.
Time to reach maximum concentration.
Elimination half-life.
Receptor activity.
Ability to cross the blood-brain barrier.
Dose and frequency.
Formulation (short-acting versus long-acting).
These pharmacokinetic principles are important to match the agent to the type of sleep disturbance (e.g., problems falling asleep versus problems staying asleep). There are also safety issues to be considered, such as potentials for tolerance, abuse, dependence, withdrawal (including risk of rebound insomnia), and drug-drug and drug-disease interactions. Medications for sleep-wake cycle disturbances should be used short term and/or as needed.
General considerations for the use of hypnotics
Medications used to induce sleep are intended for the short-term management of sleep disorders. The use of these medications for longer periods is poorly studied. They are usually combined with lifestyle changes that reinforce good sleep habits and negate the need for chronic hypnotic medications.
Most research studies of current and historic hypnotic medications rarely exceed a duration of 12 to 16 weeks. Additionally, no current hypnotic re-creates normal sleep architecture, and variations from normal periods of rapid eye movement (REM) sleep and non-REM sleep are common. It is important to taper hypnotic medications slowly, or the variations in normal sleep patterns can become even more pronounced, with the majority of time spent in REM sleep in a condition known as REM rebound.[30,31]
Table 3 lists the drug categories and specific medications, including doses, commonly used to treat sleep disturbances.
Table 3. Medications Commonly Used to Promote Sleep
Drug Category
Medication
Dose
Comments
Reference
CR = controlled-release; FDA = U.S. Food and Drug Administration; REM = rapid eye movement.
Biphasic release; useful for problems both falling asleep and staying asleep. Do not crush or split tablets. Maximum suggested dose for women: 6.25 mg.
Risk of weight gain, metabolic syndrome, abnormal/involuntary movements; possible cardiovascular effects (e.g., prolonged QT interval). Generally not a preferred agent due to side effects.
All agents in this class are FDA approved for primary insomnia. These agents promote sleep by enhancing the effects of gamma-aminobutyric acid (GABA) at the GABA type A (GABAA) receptor. Unlike traditional benzodiazepines, these agents preferentially target specific GABAA receptor subtypes. Zolpidem and zaleplon bind predominantly to the alpha-1 subtype of GABAA, and eszopiclone preferentially targets the alpha-3 receptor subtype. This selective receptor subtype targeting has both advantages and disadvantages. These agents have mainly hypnotic/sedative effects and lack the anxiolytic, anticonvulsant, and myorelaxant effects seen with benzodiazepines. Conversely, because of the selective receptor subtype targeting, these agents have fewer effects on cognitive and psychomotor function and carry less risk of tolerance, dependence, and withdrawal (especially physical withdrawal) than benzodiazepines.[4,28,29]
These agents may be preferred for use in patients with cancer when only hypnotic effects are desired and should be taken just before bedtime (or even in bed) because they enter the brain very quickly. Some of these agents (e.g., zaleplon) have a short elimination half-life. Because of their longer-lasting effects, zolpidem extended-release and eszopiclone are preferred in the treatment of difficulty staying asleep. However, these agents carry a higher risk of residual morning sedation and cognitive/motor impairments than do agents with shorter elimination half-lives (e.g., zaleplon and immediate-release zolpidem).
Benzodiazepines
Benzodiazepines target several GABAA receptor subtypes, including alpha-1, -2, -3, and -5, and work by enhancing GABA effects at these receptors. In addition to hypnotic/sedative effects, these agents also have anxiolytic, anticonvulsant, and myorelaxant effects. Benzodiazepines are preferred when other effects (such as antianxiety or muscle relaxation) are desirable with or without the hypnotic effects.[4,28,29]
Benzodiazepines carry a much higher risk of tolerance, dependence, and withdrawal than nonbenzodiazepine receptor agonists. Benzodiazepine withdrawal has been associated with the risk of seizures, delirium tremens, autonomic instability, and death. These agents should be used with extreme caution and close monitoring in patients with histories of significant substance use because of potential tolerance and dependence issues. Benzodiazepines have also been associated with cognitive impairment and difficulties with motor coordination.
Generally, benzodiazepines with longer half-lives (e.g., clonazepam) are associated with a higher risk of residual morning sedation and cognitive/motor impairments. Agents with shorter elimination half-lives (e.g., lorazepam) are generally preferred for short-term anxiolytic effects and difficulties falling asleep and in older patients. Agents with longer half-lives (e.g., clonazepam) are preferred for the treatment of persistent anxiety and difficulties falling and staying asleep. All benzodiazepines are associated with risk of respiratory depression and should be used with caution in patients with preexisting respiratory disorders.
Melatonin receptor agonists: Ramelteon and tasimelteon
Ramelteon and tasimelteon work by binding to the melatonin receptor types MT1 and MT2. Ramelteon is useful only for the treatment of difficulties falling asleep and does not have any other effects, such as anxiolytic or myorelaxant effects. Tasimelteon is indicated for use in circadian sleep disorder. These agents do not treat difficulties staying asleep but also carry much less risk of cognitive/motor impairments and dependence.[28,29,39]
Antihistamines
Diphenhydramine and hydroxyzine decrease arousal by blockading histamine receptors. Antihistamines are sold over the counter and are useful for treating difficulties in falling asleep only. There is limited evidence for the use of antihistamines to treat insomnia; these agents are used when traditional hypnotics or benzodiazepines are less suitable because of the risk of cross-dependence or other issues, such as vulnerability of a patient to addictions. The anticholinergic properties of antihistamines may also be beneficial in the treatment of nausea and vomiting. The sedative and anticholinergic properties of these agents increase the risk of delirium, especially in older patients.[28,29]
Antidepressants
Sedating antidepressants are considered first-line agents when insomnia is comorbid with depression/anxiety symptomatology. These drugs include tricyclic antidepressants (e.g., amitriptyline) and second-generation antidepressants (e.g., mirtazapine). The sedating effects of tricyclic antidepressants are caused mainly by histamine receptor blockading and partially by blockading of 5-HT2 and muscarinic receptors. The sedating effects of mirtazapine are caused by its blocking of 5-HT2 and histamine receptors, while those of trazodone are caused by its blocking actions at the at histamine, 5-HT, and noradrenaline receptors.[4,28,29] For more information, see the Pharmacological Intervention section in Depression.
Tricyclic antidepressants have a small therapeutic window and can be lethal in overdose, compared with second-generation antidepressants such as mirtazapine. Additionally, tricyclics carry other risks, such as weight gain, anticholinergic side effects, and cardiovascular side effects, and should be used under close supervision. These agents sometimes are used in low doses (see Table 3) as adjuncts to other antidepressants to treat insomnia comorbid with depression/anxiety. This helps to avoid the side effects associated with higher doses while delivering the needed sedating effects. Tricyclics can also boost appetite and may be the treatment of choice for insomnia in patients with comorbid cachexia. Certain tricyclics (amitriptyline and nortriptyline) can also be beneficial in the treatment of pain syndromes (e.g., neuropathic pain) and headaches when these issues are comorbid with insomnia. Low doses of antidepressants (subtherapeutic for depression) are frequently used to treat insomnia without any comorbidities.
Mirtazapine has appetite-stimulating and antiemetic properties in addition to sedating effects. It is frequently used in insomniac patients with depression (therapeutic dose for depression, 15–45 mg) or without depression (subtherapeutic dose for depression, 7.5–15 mg) with comorbid nausea or loss of appetite. In low doses, trazodone (50–100 mg) can promote sleep and is often combined with other antidepressants (e.g., fluoxetine 20 mg in the morning) in depressed patients with insomnia.
Antipsychotics
Antipsychotics such as quetiapine have sedating effects caused mainly by the blockade of histamine receptors. However, these agents should be considered as a last resort and as a short-term treatment because of their serious side-effect profile. The use of antipsychotics has been associated with the following:
Weight gain.
Metabolic syndrome.
Diabetes.
Cardiovascular risks.
The risk of extrapyramidal side effects, including tardive dyskinesia.
Antipsychotics can be considered for treatment-refractory insomnia, especially with comorbid anxiety symptomatology.[28]
Chloral derivative: Chloral hydrate
Chloral hydrate has sleep-promoting effects resulting from its effects on GABA systems. It is associated with risk of withdrawal symptoms similar to those of benzodiazepines and with rapid development of tolerance. Additionally, chloral hydrate carries the risk of gastric irritation and multiple drug interactions, and it is lethal in overdose. Like antipsychotics, chloral hydrate is usually considered only in cases of treatment-refractory insomnia because of its serious side-effect profile and the availability of safer alternatives.[28]
Botanical/dietary supplements
Melatonin
Melatonin, a hormone produced by the pineal gland during the hours of darkness, plays a major role in the sleep-wake cycle and has been linked to the circadian rhythm. A review found that short-term use of melatonin appears to be safe; however, the studies were not conducted in the context of cancer therapy.[40] Adjuvant melatonin may also improve sleep disruption caused by drugs known to alter normal melatonin production (e.g., beta-blockers and benzodiazepines).[41][Level of evidence: IV] However, a meta-analysis of 25 studies exploring the efficacy and safety of melatonin in managing secondary sleep disorders or sleep disorders accompanying sleep restriction found that melatonin was not effective in these conditions.[42]
Evidence suggests that circulating melatonin levels are significantly lower in physically healthy older people and in insomniacs than in age-matched control subjects. In view of these findings, melatonin replacement therapy may be beneficial in the initiation and maintenance of sleep in older patients.[43][Level of evidence: II] A slow-release formulation of melatonin is licensed in Europe and is approved as monotherapy for patients aged 55 years or older for the short-term treatment (up to 13 weeks) of primary insomnia characterized by poor-quality sleep. However, melatonin replacement as a treatment for insomnia has not been studied in older people with cancer. Ramelteon and tasimelteon work via the melatonin receptor system: ramelteon to support the initiation of sleep, and tasimelteon to correct circadian sleep disorder.
Melatonin may interact with certain chemotherapeutic regimens via the cytochrome P450 enzyme and other systems.[44] It may augment the effects of some chemotherapeutic agents metabolized via the enzyme CYP1A2 and may exert inhibitory effects on P-glycoprotein–mediated doxorubicin efflux.
Clinical studies in individuals with renal, breast, colon, lung, and brain cancer suggest that melatonin exerts anticancer effects in conjunction with chemotherapy and radiation therapy; however, evidence remains inconclusive.[45,46] All of the studies suggesting antitumor effects of melatonin have been conducted by the same group of investigators and were open label. Efforts by independent groups of investigators are under way to investigate these effects in carefully designed, randomized, blinded studies.[45] In vitro and animal studies have demonstrated the anticancer effects of exogenous melatonin, and lower melatonin levels are associated with tumor growth.[47] Human studies have yet to substantiate any causal or associative relationships.
Cannabis and cannabinoids
No studies have been conducted to specifically evaluate the effects of Cannabis inhalation or other Cannabis products in patients with primary or secondary sleep disturbances. Limited data from in vitro studies, animal studies, and small populations of healthy individuals or chronic Cannabis users are beginning to elucidate some of the relationships among various neurotransmitters, the sleep-wake cycle, and related effects of Cannabis pharmacology.[48,49]
Cannabis-based medicines are under development as a treatment for chronic pain syndromes, including cancer-related pain. One such medication is nabiximols (Sativex), an oromucosal formulation (delta-9-tetrahydrocannabinol and cannabidiol mixed in a 1:1 ratio). Studies conducted with nabiximols, primarily focusing on pain syndromes, have shown improvement in subjective sleep quality when sleep was measured as a secondary outcome.[50] Comorbidities such as pain are common reasons for sleep disturbances. Concerns have been raised about the abuse and dependence potential of nabiximols, especially in the subpopulation of patients with histories of Cannabis use.[51] Nabiximols is approved in Canada for the treatment of central neuropathic pain in patients with multiple sclerosis. In the United States, it is only available for investigational use and is currently under investigation for the treatment of intractable cancer pain. For more information, see Cannabis and Cannabinoids.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Jefferson CD, Drake CL, Scofield HM, et al.: Sleep hygiene practices in a population-based sample of insomniacs. Sleep 28 (5): 611-5, 2005. [PUBMED Abstract]
Savard J, Morin CM: Insomnia in the context of cancer: a review of a neglected problem. J Clin Oncol 19 (3): 895-908, 2001. [PUBMED Abstract]
Morin CM, Bootzin RR, Buysse DJ, et al.: Psychological and behavioral treatment of insomnia:update of the recent evidence (1998-2004). Sleep 29 (11): 1398-414, 2006. [PUBMED Abstract]
Becker PM: Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 23 (4): 1149-63, 2005. [PUBMED Abstract]
Jacobs GD, Benson H, Friedman R: Home-based central nervous system assessment of a multifactor behavioral intervention for chronic sleep-onset insomnia. Behav Ther 24 (1): 159-74, 1993.
Morin CM, Culbert JP, Schwartz SM: Nonpharmacological interventions for insomnia: a meta-analysis of treatment efficacy. Am J Psychiatry 151 (8): 1172-80, 1994. [PUBMED Abstract]
Smith MT, Perlis ML, Park A, et al.: Comparative meta-analysis of pharmacotherapy and behavior therapy for persistent insomnia. Am J Psychiatry 159 (1): 5-11, 2002. [PUBMED Abstract]
Morgenthaler T, Kramer M, Alessi C, et al.: Practice parameters for the psychological and behavioral treatment of insomnia: an update. An american academy of sleep medicine report. Sleep 29 (11): 1415-9, 2006. [PUBMED Abstract]
Edinger JD, Wohlgemuth WK, Radtke RA, et al.: Cognitive behavioral therapy for treatment of chronic primary insomnia: a randomized controlled trial. JAMA 285 (14): 1856-64, 2001. [PUBMED Abstract]
Berger AM, VonEssen S, Kuhn BR, et al.: Adherence, sleep, and fatigue outcomes after adjuvant breast cancer chemotherapy: results of a feasibility intervention study. Oncol Nurs Forum 30 (3): 513-22, 2003 May-Jun. [PUBMED Abstract]
Berger AM, VonEssen S, Khun BR, et al.: Feasibilty of a sleep intervention during adjuvant breast cancer chemotherapy. Oncol Nurs Forum 29 (10): 1431-41, 2002 Nov-Dec. [PUBMED Abstract]
Jacobs GD, Pace-Schott EF, Stickgold R, et al.: Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 164 (17): 1888-96, 2004. [PUBMED Abstract]
Morin CM, Colecchi C, Stone J, et al.: Behavioral and pharmacological therapies for late-life insomnia: a randomized controlled trial. JAMA 281 (11): 991-9, 1999. [PUBMED Abstract]
Savard J, Simard S, Ivers H, et al.: Randomized study on the efficacy of cognitive-behavioral therapy for insomnia secondary to breast cancer, part I: Sleep and psychological effects. J Clin Oncol 23 (25): 6083-96, 2005. [PUBMED Abstract]
Epstein DR, Dirksen SR: Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 34 (5): E51-9, 2007. [PUBMED Abstract]
Espie CA, Fleming L, Cassidy J, et al.: Randomized controlled clinical effectiveness trial of cognitive behavior therapy compared with treatment as usual for persistent insomnia in patients with cancer. J Clin Oncol 26 (28): 4651-8, 2008. [PUBMED Abstract]
Berger AM, Kuhn BR, Farr LA, et al.: One-year outcomes of a behavioral therapy intervention trial on sleep quality and cancer-related fatigue. J Clin Oncol 27 (35): 6033-40, 2009. [PUBMED Abstract]
Berger AM, Kuhn BR, Farr LA, et al.: Behavioral therapy intervention trial to improve sleep quality and cancer-related fatigue. Psychooncology 18 (6): 634-46, 2009. [PUBMED Abstract]
Savard J, Ivers H, Savard MH, et al.: Is a video-based cognitive behavioral therapy for insomnia as efficacious as a professionally administered treatment in breast cancer? Results of a randomized controlled trial. Sleep 37 (8): 1305-14, 2014. [PUBMED Abstract]
Mustian KM, Sprod LK, Janelsins M, et al.: Multicenter, randomized controlled trial of yoga for sleep quality among cancer survivors. J Clin Oncol 31 (26): 3233-41, 2013. [PUBMED Abstract]
Chen HM, Tsai CM, Wu YC, et al.: Effect of walking on circadian rhythms and sleep quality of patients with lung cancer: a randomised controlled trial. Br J Cancer 115 (11): 1304-1312, 2016. [PUBMED Abstract]
Page M: Sleep pattern disturbance. In: McNally JC, Stair JC, Somerville ET, eds.: Guidelines for Cancer Nursing Practice. Grune and Stratton, Inc., 1985, pp 89-95.
Kaempfer SH: Insomnia. In: Baird SB, ed.: Decision Making in Oncology Nursing. B.C. Decker, Inc., 1988, pp 78-9.
Berlin RM: Management of insomnia in hospitalized patients. Ann Intern Med 100 (3): 398-404, 1984. [PUBMED Abstract]
Horowitz SA, Breitbart W: Relaxation and imagery for symptom control in cancer patients. In: Breitbart W, Holland JC, eds.: Psychiatric Aspects of Symptom Management in Cancer Patients. American Psychiatric Press, 1993, pp 147-71.
Jim HS, Small B, Faul LA, et al.: Fatigue, depression, sleep, and activity during chemotherapy: daily and intraday variation and relationships among symptom changes. Ann Behav Med 42 (3): 321-33, 2011. [PUBMED Abstract]
Savard MH, Savard J, Trudel-Fitzgerald C, et al.: Changes in self-reported hot flashes and their association with concurrent changes in insomnia symptoms among women with breast cancer. Menopause 18 (9): 985-93, 2011. [PUBMED Abstract]
Wilson SJ, Nutt DJ, Alford C, et al.: British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders. J Psychopharmacol 24 (11): 1577-601, 2010. [PUBMED Abstract]
Sullivan SS: Insomnia pharmacology. Med Clin North Am 94 (3): 563-80, 2010. [PUBMED Abstract]
Ramakrishnan K, Scheid DC: Treatment options for insomnia. Am Fam Physician 76 (4): 517-26, 2007. [PUBMED Abstract]
Schutte-Rodin S, Broch L, Buysse D, et al.: Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med 4 (5): 487-504, 2008. [PUBMED Abstract]
Howell M, Avidan AY, Foldvary-Schaefer N, et al.: Management of REM sleep behavior disorder: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med 19 (4): 759-768, 2023. [PUBMED Abstract]
Alford C, Rombaut N, Jones J, et al.: Acute effects of hydroxyzine on nocturnal sleep and sleep tendency the following day: a C-EEG study. Hum Psychopharmacol Clin Exp 7 (1): 25-35, 1992.
Wilson S, Nutt D: Management of insomnia: treatments and mechanismsi. Br J Psychiatry 191: 195-7, 2007. [PUBMED Abstract]
Pagel JF, Parnes BL: Medications for the Treatment of Sleep Disorders: An Overview. Prim Care Companion J Clin Psychiatry 3 (3): 118-125, 2001. [PUBMED Abstract]
James SP, Mendelson WB: The use of trazodone as a hypnotic: a critical review. J Clin Psychiatry 65 (6): 752-5, 2004. [PUBMED Abstract]
Chakravorty S, Hanlon AL, Kuna ST, et al.: The effects of quetiapine on sleep in recovering alcohol-dependent subjects: a pilot study. J Clin Psychopharmacol 34 (3): 350-4, 2014. [PUBMED Abstract]
Johnsa JD, Neville MW: Tasimelteon: a melatonin receptor agonist for non-24-hour sleep-wake disorder. Ann Pharmacother 48 (12): 1636-41, 2014. [PUBMED Abstract]
Buscemi N, Vandermeer B, Hooton N, et al.: Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta-analysis. BMJ 332 (7538): 385-93, 2006. [PUBMED Abstract]
Dawson D, Encel N: Melatonin and sleep in humans. J Pineal Res 15 (1): 1-12, 1993. [PUBMED Abstract]
van Geijlswijk IM, Korzilius HP, Smits MG: The use of exogenous melatonin in delayed sleep phase disorder: a meta-analysis. Sleep 33 (12): 1605-14, 2010. [PUBMED Abstract]
Haimov I, Lavie P, Laudon M, et al.: Melatonin replacement therapy of elderly insomniacs. Sleep 18 (7): 598-603, 1995. [PUBMED Abstract]
Seely D, Stempak D, Baruchel S: A strategy for controlling potential interactions between natural health products and chemotherapy: a review in pediatric oncology. J Pediatr Hematol Oncol 29 (1): 32-47, 2007. [PUBMED Abstract]
Lissoni P, Barni S, Mandalà M, et al.: Decreased toxicity and increased efficacy of cancer chemotherapy using the pineal hormone melatonin in metastatic solid tumour patients with poor clinical status. Eur J Cancer 35 (12): 1688-92, 1999. [PUBMED Abstract]
Mills E, Wu P, Seely D, et al.: Melatonin in the treatment of cancer: a systematic review of randomized controlled trials and meta-analysis. J Pineal Res 39 (4): 360-6, 2005. [PUBMED Abstract]
Mirick DK, Davis S: Melatonin as a biomarker of circadian dysregulation. Cancer Epidemiol Biomarkers Prev 17 (12): 3306-13, 2008. [PUBMED Abstract]
Schierenbeck T, Riemann D, Berger M, et al.: Effect of illicit recreational drugs upon sleep: cocaine, ecstasy and marijuana. Sleep Med Rev 12 (5): 381-9, 2008. [PUBMED Abstract]
Murillo-Rodriguez E, Poot-Ake A, Arias-Carrion O, et al.: The emerging role of the endocannabinoid system in the sleep-wake cycle modulation. Cent Nerv Syst Agents Med Chem 11 (3): 189-96, 2011. [PUBMED Abstract]
Barnes MP: Sativex: clinical efficacy and tolerability in the treatment of symptoms of multiple sclerosis and neuropathic pain. Expert Opin Pharmacother 7 (5): 607-15, 2006. [PUBMED Abstract]
Robson P: Abuse potential and psychoactive effects of δ-9-tetrahydrocannabinol and cannabidiol oromucosal spray (Sativex), a new cannabinoid medicine. Expert Opin Drug Saf 10 (5): 675-85, 2011. [PUBMED Abstract]
Special Considerations
The Patient With Pain
Since enhanced pain control improves sleep, appropriate analgesics or nonpharmacological pain management should be administered before introducing sleep medications. Tricyclic antidepressants can be particularly useful for the treatment of insomnia in patients with neuropathic pain and depression. Patients on high-dose opioids for pain may be at increased risk for the development of delirium and organic mental disorders. Such patients may benefit from the use of low-dose neuroleptics as sleep agents (e.g., haloperidol 0.5–1 mg).
The Older Patient
Older patients frequently have insomnia due to age-related changes in sleep. The sleep cycle in this population is characterized by lighter sleep, more frequent awakenings, and less total sleep time. Anxiety, depression, loss of social support, and a diagnosis of cancer are contributory factors in sleep disturbances in older patients.[1]
Sleep problems in older adults are so common that nearly one-half of all hypnotic prescriptions written are for people older than 65 years. Although normal aging affects sleep, the clinician should evaluate the many factors that cause insomnia, such as:[2]
Medical illness.
Psychiatric illness.
Dementia.
Alcohol and/or polypharmacy.
Restless legs syndrome.
Periodic leg movements.
Sleep apnea syndrome.
Nonpharmacological treatment of sleep disorders is the preferred initial management, with the use of medication when indicated and referral to a sleep disorder center when specialized care is necessary.[2]
Providing a regular schedule of meals, discouraging daytime naps, and encouraging physical activity may improve sleep. Hypnotic prescriptions for older patients must be adjusted for variations in metabolism, increased fat stores, and increased sensitivity. Dosages should be reduced by 30% to 50%. Problems associated with drug accumulation (especially flurazepam) must be weighed against the risks of more severe withdrawal or rebound effects associated with short-acting benzodiazepines. An alternate drug for older patients is chloral hydrate.[1]
Sleep Apnea After Mandibulectomy
Anterior mandibulectomy can result in the development of sleep apnea. All patients with head and neck tumors who have had extensive anterior oral cavity resection should be evaluated before decannulation of the tracheostomy tube. Subsequent flap and/or reconstruction of the lower jaw seems to prevent the development of sleep apnea. In contrast, facial sling suspension of the lower lip does not prevent the development of sleep apnea.[3] Assessment for symptoms and preparation for the appearance of symptoms in this population provide indications for interventions related to sleep apnea.
References
Berlin RM: Management of insomnia in hospitalized patients. Ann Intern Med 100 (3): 398-404, 1984. [PUBMED Abstract]
Johnston JE: Sleep problems in the elderly. J Am Acad Nurse Pract 6 (4): 161-6, 1994. [PUBMED Abstract]
Panje WR, Holmes DK: Mandibulectomy without reconstruction can cause sleep apnea. Laryngoscope 94 (12 Pt 1): 1591-4, 1984. [PUBMED Abstract]
Latest Updates to This Summary (07/17/2024)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the pathophysiology and treatment of sleep disorders. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Sleep Disorders are:
Marilyn J. Hammer, PhD, DC, RN, FAAN (Dana-Farber Cancer Institute)
Jayesh Kamath, MD, PhD (University of Connecticut Health Center)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Sleep Disorders. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/sleep-disorders-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389467]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.


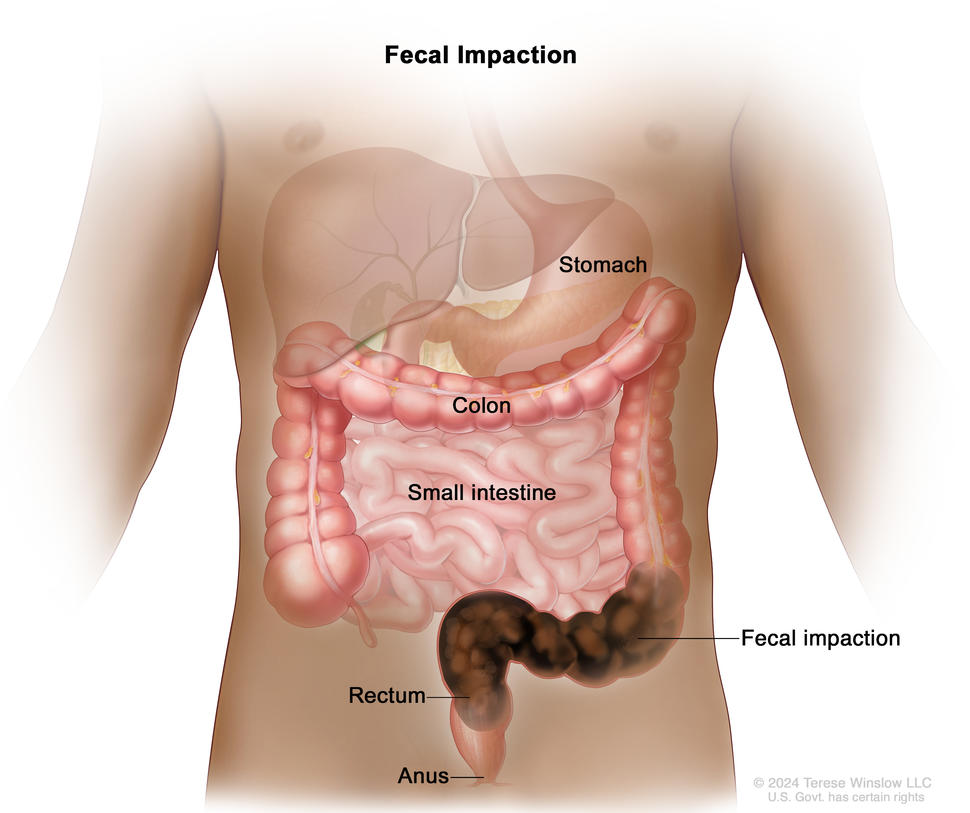

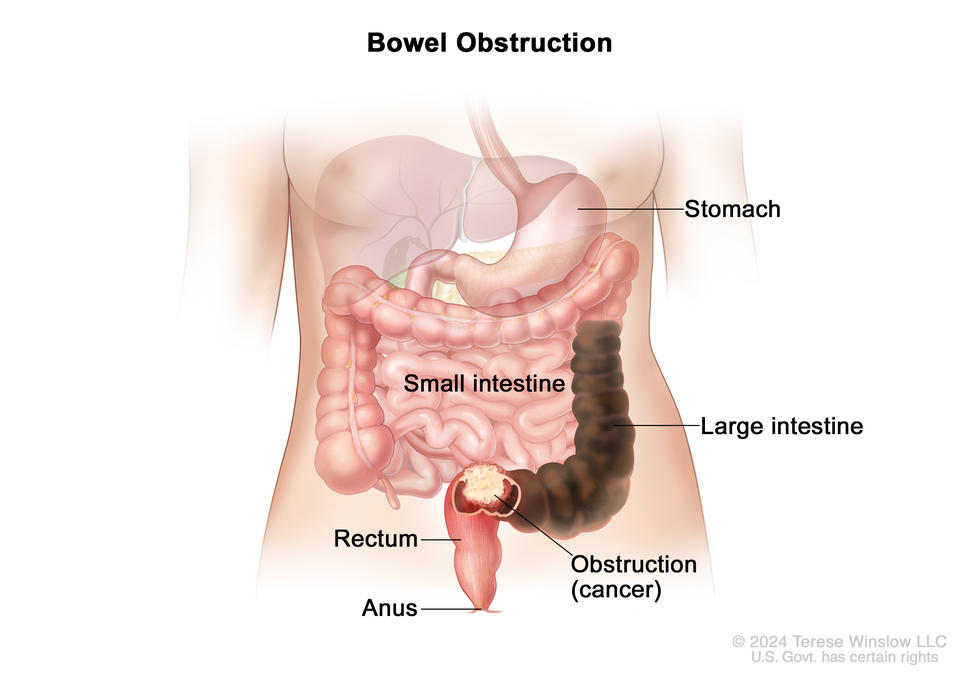
. There are also two pullouts: one showing a close up of the inside structure of a lymph node and the attached artery, vein, and lymph vessels with arrows showing how the lymph (clear, watery fluid) moves into and out of the lymph node, and another showing a close up of bone marrow with blood cells.")