
Screening is looking for cancer before a person has any symptoms. This can help detect cancer at an early stage. When abnormal tissue or cancer is found early, it may be easier to treat.
In the United States, there are no standard or routine screening tests to detect stomach cancer in people at average risk. Researchers are working to develop such tests. If a test reduces the number of deaths from stomach cancer, it may become a standard screening test.
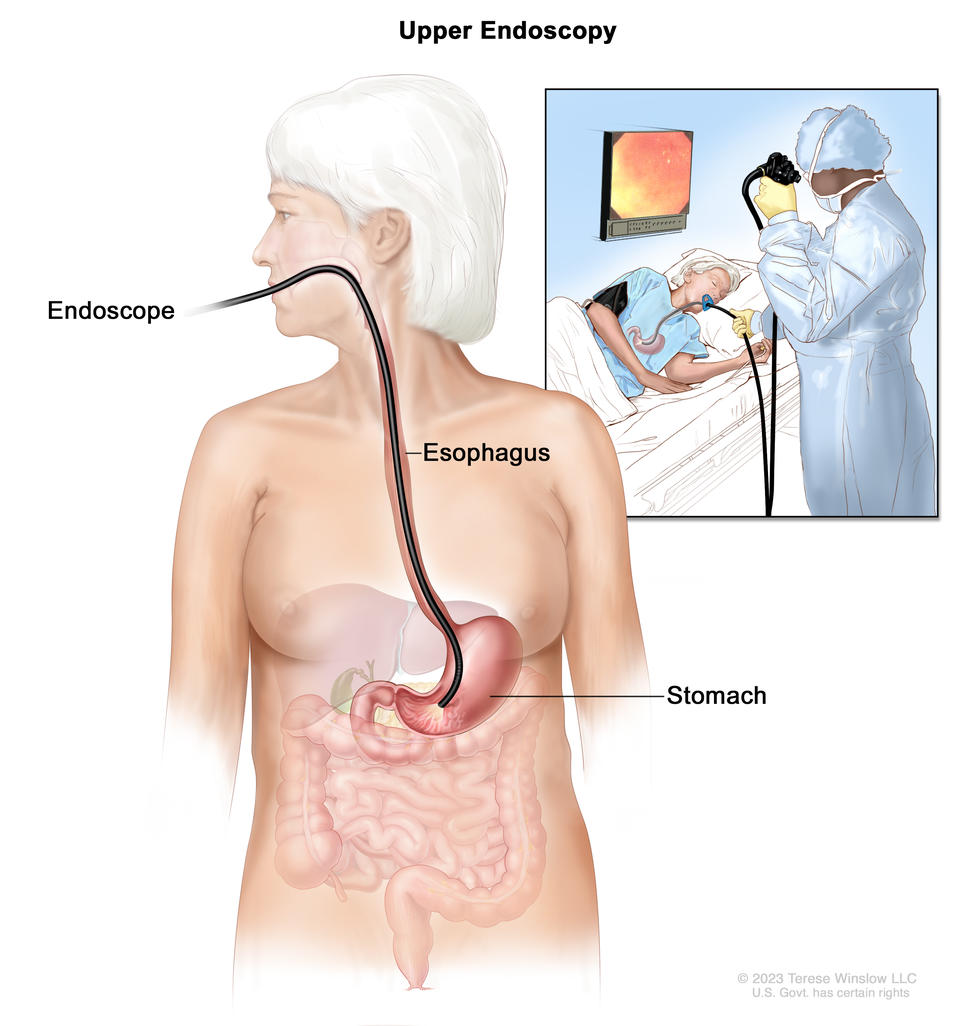
Upper endoscopy. A thin, lighted tube called an endoscope is inserted through the mouth and down the throat to check for abnormal areas in the esophagus, stomach, and first part of the small intestine.
Credit: © Terese Winslow
Tests to screen for stomach cancer
Some people who have a higher risk of stomach cancer may benefit from screening with upper endoscopy, including:
- older people with chronic gastric atrophy or pernicious anemia
- people who have had
- partial gastrectomy
- a family history of stomach cancer
- people who have certain genetic syndromes
- people from countries where stomach cancer is more common
Learn more about risk factors for stomach cancer.
Upper endoscopy
Upper endoscopy is a procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope is passed through the mouth and down the throat into the esophagus. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue, which is checked under a microscope for signs of disease.
Risks of stomach cancer screening
Talk with your doctor about whether stomach cancer screening is right for you.
Potential risks of stomach cancer screening include:
- False-negative test results. Screening test results may appear to be normal even though stomach cancer is present. A person who receives a false-negative test result (one that shows there is no cancer when there really is) may delay seeking medical care even if there are symptoms.
- False-positive test results. Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn’t) can cause anxiety and is usually followed by more tests and procedures which also have risks.
- Risks of the screening test itself. Upper endoscopy may cause the following rare, but serious, complications:
- a small hole (puncture) in the esophagus or stomach
- heart problems
- breathing problems
- lung infection from inhaling food, fluid, or stomach acid into the lung
- severe bleeding that needs to be treated at a hospital
- reactions to medicine used during the procedure

 to PD-1 (on the T cell), which keeps T cells from killing tumor cells in the body. Also shown are a tumor cell antigen and T cell receptor. The panel on the right shows immune checkpoint inhibitors (anti-PD-L1 and anti-PD-1) blocking the binding of PD-L1 to PD-1, which allows the T cells to kill tumor cells.")
, endometrium (inner lining of the uterus), ovaries, fallopian tubes, cervix, and vagina.")

 is shown passing a transducer (a device that makes sound waves that bounce off tissues inside the body) over the surface of the patient’s abdomen. A computer screen shows a sonogram (computer picture).")
 is shown inserted into the vagina. The bladder, uterus, right fallopian tube, and right ovary are also shown. The inset shows the diagnostic sonographer (a person trained to perform ultrasound procedures) examining a woman on a table, and a computer screen shows an image of the patient’s internal tissues.")
 compared to the size of a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm). Also shown is a 10-cm ruler and a 4-inch ruler.")

 shows cancer inside one ovary. The second panel (stage IB) shows cancer inside both ovaries. The third panel (stage IC) shows cancer inside both ovaries and (a) the tumor in the ovary on the left has ruptured (broken open), (b) there is cancer on the surface of the ovary on the right, and (c) there are cancer cells in the pelvic peritoneal fluid (inset).")
 shows cancer inside both ovaries that has spread to the fallopian tube and uterus. Also shown are the cervix and vagina. The second panel (stage IIB) shows cancer inside both ovaries that has spread to the colon. The third panel (primary peritoneal cancer) shows cancer in the pelvic peritoneum.")
 lymph nodes behind the peritoneum and (b) the omentum. The small intestine, colon, fallopian tubes, uterus, and bladder are also shown.")


