egg dishes, such as omelets, scrambled eggs, and soufflés
Milk
use milk instead of water in drinks and in cooking
use in hot cereal, soups, cocoa, and pudding
Nonfat instant dry milk or protein powder
add to milk and milk drinks, such as pasteurized eggnog and milkshakes
mix with ice cream, milk, and fruit for a high-protein milkshake
use in:
casseroles
meatloaf
breads
muffins
sauces
cream soups
mashed potatoes
macaroni and cheese
pudding
custard
other milk-based desserts
Ice cream, yogurt, and frozen yogurt
add to:
carbonated drinks
milk drinks, such as milkshakes
cereal
fruit
gelatin (Jell-O)
pies
mix with soft or cooked fruits
make a sandwich of ice cream or frozen yogurt between cake slices, cookies, or graham crackers
mix with breakfast drinks and fruit, such as bananas
Eggs
add chopped hard-boiled eggs to salads, salad dressings, vegetables, casseroles, and creamed meats
make a rich custard with eggs, milk, and sugar
add extra hard-boiled yolks to deviled egg filling and sandwich spread
beat eggs into mashed potatoes, pureed vegetables, and sauces (make sure to keep cooking these dishes after adding the eggs because raw eggs may contain harmful bacteria)
add extra eggs or egg whites to:
custard
puddings
quiches
scrambled eggs
omelets
pancake or French toast batter
Nuts, seeds, and wheat germ
add to:
casseroles
breads
muffins
pancakes
cookies
waffles
sprinkle on:
fruit
cereal
ice cream
yogurt
vegetables
salads
toast
use in place of breadcrumbs in recipes
blend with parsley, spinach, or herbs and cream to make a sauce for noodle, pasta, or vegetable dishes
roll bananas in chopped nuts
Peanut butter and other nut butters
spread on:
sandwiches
toast
muffins
crackers
waffles
pancakes
fruit slices
use as a dip for raw vegetables
blend with milk and other drinks
swirl through soft ice cream and yogurt
Meat, poultry, and fish
add chopped, cooked meat or fish to:
vegetables
salads
casseroles
soups
sauces
biscuit dough
omelets
soufflés
quiches
sandwich fillings
chicken and turkey stuffings
wrap in pie crust or biscuit dough as turnovers
add to baked potatoes
Beans, legumes, and tofu
add to casseroles, pasta dishes, soups, salads, and grain dishes
The field of oral complications caused by cancer therapies continues to evolve for a number of reasons, including:
High-quality basic, translational, and clinical research.
Translation of selected clinical interventions into systematic reviews and clinical practice guidelines based on this research.
Advances in cancer treatment via precision medicine technology.
Increased understanding of the value of integration of tumor treatment with evidence-based supportive care.
The oral cavity represents a unique anatomic and functional site. Clinical prevention and management of oral complications in patients with cancer should be based on state-of-the-science and implemented in an interprofessional practice setting. The interprofessional team includes, but is not limited to, oncologists, oncology nurses and nurse navigators, dental generalists and specialists, dental hygienists, social workers, and dieticians.
The type and severity of oral complications vary by classification, intensity, and duration of cancer therapy. Table 1 shows examples of these oral complications.
Table 1. Medically Necessary Oral Interventions, by Type of Cancer Therapy
Cancer Therapy
Before Cancer Therapy
During Cancer Therapy
After Cancer Therapy
GVHD = graft versus host disease; HPV = human papillomavirus; HSCT = hematopoietic stem cell transplant; WBC = white blood cell.
Chemotherapy, high dose (e.g., <1,000 WBC/µL for more than 5 days) and chemotherapy, moderate to low dose (e.g., nadir of 2,500 WBC/µL)
Advanced dental caries, with potential for pulpal involvement
Maintain effective oral hygiene
Implement preventive and treatment protocols to optimize oral health
Dentition with moderate/severe periodontal disease
Periapical lesions secondary to dental pulpal infection that have been symptomatic within the past 90 days
Dental appliances (e.g., dentures, orthodontic appliances) that may traumatize oral mucosa
Patient education
Assess for possible acute infection of oral origin
Manage oral mucositis, including oral hygiene and pain management
HSCT, reduced intensity chemotherapy (e.g., nadir of 2,500 WBC/µL) and HSCT, myeloablative chemotherapy (e.g., <1,000 WBC/µL for more than 5 days)
Advanced dental caries, with potential for pulpal involvement
Maintain effective oral hygiene
Dentition with moderate/severe periodontal disease
Periapical lesions secondary to dental pulpal infection that have been symptomatic within the past 90 days
Assess for possible acute infection of oral origin
Dental appliances (e.g., dentures, orthodontic appliances) that may traumatize oral mucosa
Patient education
Manage oral mucositis, including oral hygiene and pain management
HSCT, GVHD
Determine likelihood of developing acute and/or chronic GVHD, depending on type of transplant
Differentiate oral mucosal injury caused by chemotherapy and acute oral GVHD
Monitor for emergence of chronic oral GVHD, potentially malignant mucosal disease, and/or oral squamous cell carcinoma
Patient education
Provide supportive care, including oral hygiene and pain control
Head and neck radiation, high dose
Determine need for medically necessary dental extractions and potential change in occlusal vertical dimension, based on the following:
Maintain oral hygiene and nutritional support
Implement preventive and treatment protocols to optimize oral health
• Advanced dental caries, with potential for pulpal involvement
• Dentition involved with moderate/severe periodontal disease
• Periapical lesions secondary to dental pulpal infection that have been symptomatic within the past 90 days
• Dental appliances (e.g., dentures, orthodontic appliances) that may traumatize oral mucosa
Patient education
Manage oral mucositis, including oral hygiene and pain management
Prescribe jaw opening and closing exercises to reduce risk of trismus
Monitor for risk of osteoradionecrosis, recurrent or new oral mucosal malignancy
Head and neck radiation, deintensification (HPV + oropharyngeal squamous cell carcinoma)
Same as high-dose head and neck radiation; risk for late effects appears to be reduced
Same as high-dose head and neck radiation
Same as high dose head and neck radiation; risk for late effects appears to be reduced
Patient education
Patient education
Immunotherapy and targeted cancer therapies
Document baseline oral mucosal status
Assess number and severity of oral mucosal lesions clinically documented to be caused by immunotherapy/targeted therapy
Monitor for possible late adverse oral effects
Patient education
Provide topical, intralesional, or systemic steroid treatment if oral pain is sufficiently severe
Bone-stabilizing agents
Eliminate advanced dental caries that approaches the dental pulp
Perform periodic systematic dental evaluations for compliance with oral hygiene and assessment of dentition, periodontium, and oral mucosa
Perform periodic systematic dental evaluations for compliance with oral hygiene and assessment of dentition, periodontium, and oral mucosa
Extract teeth with poor long-term prognosis due to periodontal disease and/or dental caries
Correct ill-fitting, removable dental prostheses that cause or could cause mucosal trauma and potential bone exposure
Patient education
Clinicians may consider many factors about oral interventions, including the following:
Patient’s immune status.
Pending time to initiation of cancer therapy.
Intensity and duration of cancer therapy.
Many of the oral complications that develop in oncology patients are characterized by considerable biological and clinical complexity.[1–12]
References
Mougeot JC, Stevens CB, Morton DS, et al.: Oral Microbiome and Cancer Therapy-Induced Oral Mucositis. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Lalla RV, Brennan MT, Gordon SM, et al.: Oral Mucositis Due to High-Dose Chemotherapy and/or Head and Neck Radiation Therapy. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Keefe DMK, Bateman EH: Potential Successes and Challenges of Targeted Cancer Therapies. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Carrozzo M, Eriksen JG, Bensadoun RJ, et al.: Oral Mucosal Injury Caused by Targeted Cancer Therapies. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Epstein JB, Miaskowski C: Oral Pain in the Cancer Patient. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Fall-Dickson JM, Pavletic SZ, Mays JW, et al.: Oral Complications of Chronic Graft-Versus-Host Disease. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Deng J, Wulff-Burchfield EM, Murphy BA: Late Soft Tissue Complications of Head and Neck Cancer Therapy: Lymphedema and Fibrosis. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Murphy BA, Wulff-Burchfield E, Ghiam M, et al.: Chronic Systemic Symptoms in Head and Neck Cancer Patients. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Spijkervet FKL, Brennan MT, Peterson DE, et al.: Research Frontiers in Oral Toxicities of Cancer Therapies: Osteoradionecrosis of the Jaws. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Jensen SB, Vissink A, Limesand KH, et al.: Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Migliorati CA, Brennan MT, Peterson DE: Medication-Related Osteonecrosis of the Jaws. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Elting LS, Chang YC: Costs of Oral Complications of Cancer Therapies: Estimates and a Blueprint for Future Study. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Oral Management of Patients Receiving Chemotherapy
Before Chemotherapy
Oral evaluation and management of patients scheduled to undergo myeloablative chemotherapy should occur as early as possible before initiation of therapy (see the list in Oral Disease Stabilization Before Chemotherapy and/or Hematopoietic Stem Cell Transplant [HSCT] and Table 1). The overall goal is to complete a comprehensive oral care plan that eliminates or stabilizes oral disease that could otherwise produce complications during or after chemotherapy. To maximize positive outcomes, the oncology team should inform the dentist about the patient’s medical status and oncology treatment plan. In turn, the dental team should delineate and communicate a plan for oral disease management before, during, and after chemotherapy.[1]
Data provided by dental providers to the oncology team includes the following:
Dental caries (number of teeth and severity, including number of teeth that should be treated before cancer treatment begins).
Endodontic disease:
Teeth with pulpal infection.
Teeth with periapical infection.
Periodontal disease status.
Number of teeth requiring extraction, as well as anticipated degree of surgical complexity.
Other urgent care required.
Time necessary to complete stabilization of oral disease.
The three categories of dental evaluation and treatment protocols before cancer therapy include the following:[2]
Complete protocols:
All dental pathologies are treated before antineoplastic chemotherapy and HSCT are initiated.
Partial protocols:
Teeth with apical periodontitis are managed only if they are symptomatic and if size of the periapical lesion is 5 mm or more.
Teeth are extracted only if they have severe periodontitis (probing depth of ≥8 mm) and/or Miller’s Class III mobility, they are expected to exfoliate within a few weeks, or if partially erupted third molars are symptomatic and with purulence.
Minimal protocols:
Patients are treated only if they are symptomatic.
Partial dental evaluation/treatment protocols may be appropriate when there is insufficient time for complete dental evaluation/treatment protocols.[3][Level of evidence: IV]
Periodontal therapy before and maintenance after cancer therapy (both head and neck radiation and antineoplastic chemotherapy) are suggested for general good oral health.[3]
During Chemotherapy
Oral complications during chemotherapy are common. Dentists play an important role on the cancer treatment team by evaluating patients before chemotherapy, with the goal of optimizing their oral health status, minimizing complications, and educating patients to maintain optimal oral hygiene. Routine, systematic oral hygiene is important to reduce incidence and severity of oral sequelae of cancer therapy. The patient must be informed of the rationale for the oral hygiene program, as well as the potential side effects of cancer chemotherapy. Effective oral hygiene is important during cancer treatment, with an emphasis on oral hygiene management before treatment starts.[1,4]
Variation exists across institutions relative to specific nonmedicated approaches to baseline oral care, given limited published evidence. Most nonmedicated oral care protocols use topical, frequent (every 4–6 hours) rinsing with 0.9% saline. Additional interventions include dental brushing with toothpaste, dental flossing, ice chips, and sodium bicarbonate rinses. Patient compliance with these agents can be maximized with monitoring by the health care team.[1][Level of evidence: IV]
Guidelines for the Management of Dentures and Orthodontic Appliances in Patients Receiving High-Dose Cancer Therapy
Minimize denture use during first 3 weeks posttransplant.[4]
Wear dentures only when eating.
Discontinue use at all other times.
Clean twice a day with a soft brush and rinse well.
Soak in antimicrobial solutions when not being worn.
Perform routine oral mucosal care procedures 3 to 4 times a day with the oral appliances out of the mouth.
Leave appliances out of the mouth when sleeping and during periods of significant mouth soreness.
Dentures may be used to hold medications needed for oral care (e.g., antifungals).
Discontinue use of removable appliances until oral mucositis has healed.
Remove orthodontic appliances (e.g., brackets, wires, retainers) before conditioning.
Dental brushing and flossing are simple, cost-effective approaches to control of bacterial dental plaque. This strategy is designed to reduce the risk of oral soft tissue infection during myeloablation. For more information, see the Infection section.
Patients skilled at flossing without traumatizing gingival tissues may continue to floss throughout chemotherapy administration. Flossing allows for interproximal removal of dental bacterial plaque and promotes gingival health.
The oral cavity should be cleaned after meals, as follows:
If dry mouth is present, plaque and food debris may accumulate secondary to reduced salivary function, and more frequent hygiene may be necessary.
Dentures need to be cleaned with denture cleanser every day and brushed and rinsed after meals.
Rinsing the oral cavity may not be sufficient for thorough cleansing of the oral tissues; mechanical plaque removal is often necessary.
Care must be taken in using mechanical hygiene aids; dental floss, interproximal brushes, and wooden wedges can injure oral tissues rendered fragile by chemotherapy.
Toothettes have limited ability to cleanse the dentition; however, they may be useful for cleaning maxillary/mandibular alveolar ridges of edentulous areas, palate, and tongue.
Preventing dry lips to reduce the risk of tissue injury is important. Mouth breathing and/or xerostomia secondary to anticholinergic medications used for nausea management can induce the condition. Graft-versus-host disease can also contribute to dry lips in allogeneic transplant patients. Lip care products containing petroleum-based oils and waxes can be useful. Lanolin-based creams and ointments may be more effective in moisturizing/lubricating the lips and protecting against trauma.
Oral mucositis (high-dose chemotherapy, HSCT, head and neck radiation)
Oral mucositis is one of the most common side effects of cytotoxic cancer regimens. The terms oral mucositis and stomatitis are often used interchangeably at the clinical level, but they do not reflect identical processes.
Oral Mucositis:
Inflammation of oral mucosa resulting from chemotherapeutic agents or ionizing radiation.[5,6]
Manifests as erythema or ulcerations.
May be exacerbated by local factors.
Stomatitis:
Any inflammatory condition of oral tissue, including mucosa, dentition/periapices, and periodontium.
Includes infections of oral tissues as well as mucositis.
The current model of oral mucositis involves a complex five-step trajectory of molecular, cellular, and tissue-based changes involving the oral microbiome.[7,5]
Patients receiving cycled chemotherapy or conditioning regimens before HSCT develop the first signs of mucositis 3 to 4 days after infusion. Oral ulcer formation begins during the second week of treatment—with the highest severity between days 7 and 14—and then resolves spontaneously in the week after cessation of cytotoxic chemotherapy.[8] Clinicians need to be alert to the potential for increased toxicity with escalating dose or treatment duration in clinical trials that demonstrate gastrointestinal mucosal toxicity.
Several health professional organizations have produced evidence-based guidelines for oral mucositis, including the following:
Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO).[9–11][Level of evidence: IV]
Many recommendations are similar across the organizations. The Cochrane Collaboration, however, uses a meta-analysis approach that provides a unique context for purposes of guideline construction.
Management of oral mucositis
Oral care protocols include atraumatically cleansing the oral mucosa, maintaining lubrication of the lips and oral tissues, and relieving pain and inflammation. Oral mucositis is minimized with the use of mild-flavored fluoridated toothpaste. Avoidance of spicy, acidic, hard, and hot foods and beverages will also decrease oral mucositis.
Management of oral mucositis via topical approaches should address efficacy, patient acceptance, and appropriate dosing. A stepped approach is typically used, with progression from one level to the next.
Gelclair (approved by the U.S. Food and Drug Administration as a device).
Caphosol.
Episil.
MuGard.
Analgesics:
Opioid drugs: oral, intravenous (e.g., bolus, continuous infusion, patient-controlled analgesia), patches, transmucosal. Morphine may be used to treat pain caused by oral mucositis in patients undergoing HSCT. Morphine mouthwash (0.2%) may be used in patients receiving chemoradiation for head and neck cancer. Transdermal fentanyl may be given to patients receiving conventional or high-dose chemotherapy, with or without total body irradiation.[14][Level of evidence: IV]
Growth factor (keratinocyte growth factor-1):
Palifermin for patients receiving high-dose chemotherapy and total body irradiation, followed by autologous stem cell transplant, for a hematological malignancy.[15]
Cryotherapy in patients receiving bolus fluorouracil chemotherapy.[16]
Low-level laser therapy to prevent oral mucositis in patients receiving HSCT conditioned with high-dose chemotherapy, with or without total body irradiation.[17][Level of evidence: IV]
Zinc supplements administered orally in oral cancer patients receiving radiation therapy or chemoradiation.[18][Level of evidence: IV]
A soft toothbrush that is replaced regularly should be used to maintain oral hygiene.[19][Level of evidence: IV] Foam-swab brushes do not effectively clean teeth and should not be considered a routine substitute for a soft, nylon-bristled toothbrush. Additionally, the rough sponge surface may irritate and damage the mucosal surfaces opposite the tooth surfaces being brushed.
Irrigation should be performed before topical medication is applied because removal of debris and saliva allows for better coating of oral tissues and prevents material from accumulating. Frequent rinsing cleans and lubricates tissues, prevents crusting, and palliates painful gingiva and mucosa.
Systemic analgesics are administered when topical anesthetic strategies are not sufficient for clinical relief. Nonsteroidal anti-inflammatory drugs that affect platelet adhesion and damage gastric mucosa are contraindicated, especially if thrombocytopenia is present.
MASCC/ISOO recommendations against specific practices include the following:
No PTA (polymyxin, tobramycin, amphotericin B) and BCoG (bacitracin, clotrimazole, gentamicin) for oral mucositis in patients receiving radiation therapy for head and neck cancer.[14][Level of evidence: IV]
Xerostomia and salivary hypofunction caused by antiemetics
Xerostomia is defined as the subjective feeling of oral dryness and can be accompanied by salivary gland hypofunction. Xerostomia is likely to occur when the salivary flow rate is less than the rate of fluid absorption across the oral mucosa plus the rate of fluid evaporation from the oral cavity.[21][Level of evidence: IV] (See Table 3.)
Table 3. Definitions of Xerostomia, Hyposalivation, and Salivary Gland Hypofunction and Dysfunction
Term
Definition
Xerostomia
Subjective feeling of oral dryness
Dry mouth
Xerostomia and/or salivary gland hypofunction
Hyposalivation
Decreased salivary output (whole saliva flow rate of ≤0.1 mL/min of unstimulated saliva and <0.7 mL/min of stimulated saliva)
Salivary gland hypofunction
Decreased salivary output
Salivary gland dysfunction
Changes in quantity and/or quality of saliva
Administration of antiemetic agents for the management of chemotherapy-induced nausea and vomiting is related to several toxicities, including gastrointestinal, renal, hepatic, and cardiovascular adverse events.[22] Some of these agents are reported to induce xerostomia or salivary gland hypofunction. (See Table 4.)
Table 4. Antiemetic Agents Associated With Xerostomia or Salivary Gland Hypofunction
After cancer therapy, routine systematic oral hygiene is also important for reducing incidence and severity of oral sequelae, restoring functional and aesthetic impairments, and removing the remaining foci of infection.
References
Schubert MM, Correa MEP, Peterson DE: Oral complications of hematopoietic cell transplantation. In: Forman SJ, Negrin RS, Antin JH, et al., eds.: Thomas’ Hematopoietic Cell Transplantation: Stem Cell Transplantation. 5th ed. John Wiley & Sons, Ltd, 2016, pp 1242-56.
Decker AM, Taichman LS, D’Silva NJ, et al.: Periodontal Treatment in Cancer Patients: An Interdisciplinary Approach. Curr Oral Health Rep 5 (1): 7-12, 2018. [PUBMED Abstract]
Hong CHL, Hu S, Haverman T, et al.: A systematic review of dental disease management in cancer patients. Support Care Cancer 26 (1): 155-174, 2018. [PUBMED Abstract]
Hong CHL, Gueiros LA, Fulton JS, et al.: Systematic review of basic oral care for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer 27 (10): 3949-3967, 2019. [PUBMED Abstract]
Bowen J, Al-Dasooqi N, Bossi P, et al.: The pathogenesis of mucositis: updated perspectives and emerging targets. Support Care Cancer 27 (10): 4023-4033, 2019. [PUBMED Abstract]
Lalla RV, Brennan MT, Gordon SM, et al.: Oral Mucositis Due to High-Dose Chemotherapy and/or Head and Neck Radiation Therapy. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Mougeot JC, Stevens CB, Morton DS, et al.: Oral Microbiome and Cancer Therapy-Induced Oral Mucositis. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Sonis ST: Oral mucositis in head and neck cancer: risk, biology, and management. Am Soc Clin Oncol Educ Book : , 2013. [PUBMED Abstract]
Elad S: The MASCC/ISOO Mucositis Guidelines 2019 Update: introduction to the first set of articles. Support Care Cancer 27 (10): 3929-3931, 2019. [PUBMED Abstract]
Elad S: The MASCC/ISOO mucositis guidelines 2019: the second set of articles and future directions. Support Care Cancer 28 (5): 2445-2447, 2020. [PUBMED Abstract]
Lalla RV, Bowen J, Barasch A, et al.: MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 120 (10): 1453-61, 2014. [PUBMED Abstract]
Bensinger W, Schubert M, Ang KK, et al.: NCCN Task Force Report. prevention and management of mucositis in cancer care. J Natl Compr Canc Netw 6 (Suppl 1): S1-21; quiz S22-4, 2008. [PUBMED Abstract]
Riley P, Glenny AM, Worthington HV, et al.: Interventions for preventing oral mucositis in patients with cancer receiving treatment: cytokines and growth factors. Cochrane Database Syst Rev 11: CD011990, 2017. [PUBMED Abstract]
Saunders DP, Epstein JB, Elad S, et al.: Systematic review of antimicrobials, mucosal coating agents, anesthetics, and analgesics for the management of oral mucositis in cancer patients. Support Care Cancer 21 (11): 3191-207, 2013. [PUBMED Abstract]
Logan RM, Al-Azri AR, Bossi P, et al.: Systematic review of growth factors and cytokines for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer 28 (5): 2485-2498, 2020. [PUBMED Abstract]
Riley P, Glenny AM, Worthington HV, et al.: Interventions for preventing oral mucositis in patients with cancer receiving treatment: oral cryotherapy. Cochrane Database Syst Rev 2015 (12): CD011552, 2015. [PUBMED Abstract]
Zadik Y, Arany PR, Fregnani ER, et al.: Systematic review of photobiomodulation for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer 27 (10): 3969-3983, 2019. [PUBMED Abstract]
Yarom N, Hovan A, Bossi P, et al.: Systematic review of natural and miscellaneous agents for the management of oral mucositis in cancer patients and clinical practice guidelines-part 1: vitamins, minerals, and nutritional supplements. Support Care Cancer 27 (10): 3997-4010, 2019. [PUBMED Abstract]
Keefe DM, Schubert MM, Elting LS, et al.: Updated clinical practice guidelines for the prevention and treatment of mucositis. Cancer 109 (5): 820-31, 2007. [PUBMED Abstract]
National Cancer Institute: Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Bethesda, Md: U.S. Department of Health and Human Services, National Institutes of Health, 2017. Available online. Last accessed Dec. 18, 2024.
Villa A, Wolff A, Narayana N, et al.: World Workshop on Oral Medicine VI: a systematic review of medication-induced salivary gland dysfunction. Oral Dis 22 (5): 365-82, 2016. [PUBMED Abstract]
Adel N: Overview of chemotherapy-induced nausea and vomiting and evidence-based therapies. Am J Manag Care 23 (14 Suppl): S259-S265, 2017. [PUBMED Abstract]
Moreno J, Sahade M, del Giglio A: Low-dose granisetron for prophylaxis of acute chemotherapy-induced nausea and vomiting: a pilot study. Support Care Cancer 13 (10): 850-3, 2005. [PUBMED Abstract]
Abas MN, Tan PC, Azmi N, et al.: Ondansetron compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol 123 (6): 1272-1279, 2014. [PUBMED Abstract]
Zuccato E, Bertolo C, Salomoni M, et al.: The effects of S(-) and R(+) sulpiride, metoclopramide, cisapride and domperidone on the small intestine suggest DA2-receptors are involved in the control of small intestinal transit time in rats. Pharmacol Res 26 (2): 179-85, 1992. [PUBMED Abstract]
Wolff A, Joshi RK, Ekström J, et al.: A Guide to Medications Inducing Salivary Gland Dysfunction, Xerostomia, and Subjective Sialorrhea: A Systematic Review Sponsored by the World Workshop on Oral Medicine VI. Drugs R D 17 (1): 1-28, 2017. [PUBMED Abstract]
Godoy T, Riva A, Ekström J: Atypical antipsychotics–effects of amisulpride on salivary secretion and on clozapine-induced sialorrhea. Oral Dis 18 (7): 680-91, 2012. [PUBMED Abstract]
Ekström J, Godoy T, Loy F, et al.: Parasympathetic vasoactive intestinal peptide (VIP): a likely contributor to clozapine-induced sialorrhoea. Oral Dis 20 (3): e90-6, 2014. [PUBMED Abstract]
Tollefson GD, Birkett MA, Kiesler GM, et al.: Double-blind comparison of olanzapine versus clozapine in schizophrenic patients clinically eligible for treatment with clozapine. Biol Psychiatry 49 (1): 52-63, 2001. [PUBMED Abstract]
Johnsen E, Jørgensen HA: Effectiveness of second generation antipsychotics: a systematic review of randomized trials. BMC Psychiatry 8: 31, 2008. [PUBMED Abstract]
Kumar A, Gupta M, Jiloha RC, et al.: Efficacy of olanzapine and sodium valproate given alone or as add-on therapy in acute mania. A comparative study. Methods Find Exp Clin Pharmacol 32 (5): 319-24, 2010. [PUBMED Abstract]
McIntyre RS, Cohen M, Zhao J, et al.: Asenapine versus olanzapine in acute mania: a double-blind extension study. Bipolar Disord 11 (8): 815-26, 2009. [PUBMED Abstract]
Bridle C, Palmer S, Bagnall AM, et al.: A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder. Health Technol Assess 8 (19): iii-iv, 1-187, 2004. [PUBMED Abstract]
Budman CL, Gayer A, Lesser M, et al.: An open-label study of the treatment efficacy of olanzapine for Tourette’s disorder. J Clin Psychiatry 62 (4): 290-4, 2001. [PUBMED Abstract]
Fulton B, Goa KL: Olanzapine. A review of its pharmacological properties and therapeutic efficacy in the management of schizophrenia and related psychoses. Drugs 53 (2): 281-98, 1997. [PUBMED Abstract]
Stauffer VL, Sniadecki JL, Piezer KW, et al.: Impact of race on efficacy and safety during treatment with olanzapine in schizophrenia, schizophreniform or schizoaffective disorder. BMC Psychiatry 10: 89, 2010. [PUBMED Abstract]
Jain T, Bhandari A, Ram V: Drug interactions and adverse drug reactions in hospitalized psychiatric patients: A critical element in providing safe medication use. German Journal of Psychiatry, 14: 26-34, 2011. Also available online.
Berlach DM, Shir Y, Ware MA: Experience with the synthetic cannabinoid nabilone in chronic noncancer pain. Pain Med 7 (1): 25-9, 2006. [PUBMED Abstract]
Skrabek RQ, Galimova L, Ethans K, et al.: Nabilone for the treatment of pain in fibromyalgia. J Pain 9 (2): 164-73, 2008. [PUBMED Abstract]
Ware MA, Fitzcharles MA, Joseph L, et al.: The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial. Anesth Analg 110 (2): 604-10, 2010. [PUBMED Abstract]
Huber SJ, Paulson GW: Efficacy of alprazolam for essential tremor. Neurology 38 (2): 241-3, 1988. [PUBMED Abstract]
Yamagishi H, Kawaguchi M: Characterization of central- and peripheral-type benzodiazepine receptors in rat salivary glands. Biochem Pharmacol 55 (2): 209-14, 1998. [PUBMED Abstract]
Wang X, Zhang ZY, Wang J, et al.: Pharmacokinetics, Safety, and Tolerability of Rolapitant Administered Intravenously Following Single Ascending and Multiple Ascending Doses in Healthy Subjects. Clin Pharmacol Drug Dev 8 (2): 160-171, 2019. [PUBMED Abstract]
Oral Management of Patients Receiving Hematopoietic Stem Cell Transplant
Hematopoietic stem cell transplant (HSCT) is a complex immune-based cellular therapy used to manage a wide range of malignant and nonmalignant conditions, including the following:[1]
Blood cancers.
Childhood immunodeficiency and metabolic disorders.
Hemoglobinopathies.
Autoimmune diseases.
Autologous transplant uses an individual’s own isolated hematopoietic cells as a “graft” to reconstitute bone marrow function after an intensive chemotherapy regimen that would otherwise cause irreversible marrow toxicity. While recipients of autologous HSCT are at risk of anticipated toxicities of high-dose chemotherapy (e.g., neutropenia, thrombocytopenia, mucositis, and nausea and vomiting), they are not at risk of developing the immune-related complications frequently associated with allogeneic HSCT. Allogeneic HSCT similarly functions by engraftment and restoration of bone marrow function, but in the case of hematologic malignancies the graft also provides a graft-versus-tumor sustained immunological response. This response is important for maintaining long-term remission but is also associated with development of graft-versus-host disease (GVHD).
Recipients of HSCT have unique oral health needs and considerations that span from pre-HSCT workup through survivorship.[2–7] Management requires coordinated multidisciplinary care. See Table 1 for management before, during, and after HSCT.
Pretransplant Dental Evaluation
Patients undergoing HSCT experience long-term myelosuppression and immunosuppression. The oral cavity may be a potential source of local as well as systemic inflammation and infection. To reduce risk, patients should undergo a comprehensive dental evaluation by an experienced dentist before undergoing HSCT.[2–5]
The dental evaluation consists of the following:
A thorough dental screening (caries, defective restorations, mobile teeth, teeth with deep pocketing, third molars, periapical pathology).
A soft tissue examination.
A full mouth series of intraoral radiographs (an orthopantomogram of the maxilla and mandible may be sufficient, and additional intraoral radiographs may be ordered, if necessary).
For children, oral care instructions and dental management are similar to those for adults.[3] When primary teeth with pulpal infection are involved, many clinicians choose to provide a more definitive treatment in the form of extraction. For more information, see the Special Considerations in Pediatric Populations section.
A dental evaluation is scheduled as early as possible to allow sufficient time to complete any necessary treatment and for tissues to heal after dental extractions and professional periodontal care. Patients who are thrombocytopenic and require invasive procedures, such as dental extractions, may require coordinated platelet transfusion support.
Table 5. Pretransplant Dental Evaluation
Finding
Management
Dental caries
Treat caries, provide endodontic therapy, or extract nonvital/abscessed teeth
Faulty or missing restorations
Replace restoration, eliminate sharp edges
Periapical pathology
Pulpitis: Provide endodontic treatment
Periapical periodontitis >5 mm: Provide endodontic therapy or extraction
No treatment necessary for previously endodontically treated teeth with persistent periapical pathology without evidence of infection
Periodontal disease
Perform scaling and root planing
Extract symptomatic teeth, teeth with advanced mobility, teeth with probings >8 mm
Pericoronitis
Extract associated third molar
Prosthetic treatment
Ensure adequate fit and function
Oral Care During Transplant
Maintenance of good oral hygiene is essential to reduce the risk of infection.[2,5] Gingival inflammation caused by oral bacteria increases the risk of gingival bleeding and bacteremia. Oral hygiene aims to remove plaque from all surfaces of the teeth. A dental/oral self-examination should be performed daily. Patients need to brush their teeth two to three times a day to reduce dental plaque, using a soft manual or electric toothbrush and a fluoride toothpaste. If possible, the patient’s teeth should be gently flossed daily. Removable dental prostheses are cleaned in a similar manner as teeth. Dentures are then placed in a cleaning solution overnight.
Bland oral rinses (0.9% saline and/or 0.5% sodium bicarbonate solution) can help remove debris and maintain moist and healthy mucosa, but they are not a substitute for mechanical cleaning. Chlorhexidine rinses are often prescribed for the duration of neutropenia. The nonalcoholic chlorhexidine digluconate (0.12%–0.2%) solution is easier to tolerate for patients with sensitive oral mucosa.
Infections are a frequent complication of HSCT during neutropenic periods. Infections may be fungal, viral, or bacterial. Coexistent oral conditions such as oral mucositis and GVHD often complicate prompt diagnosis of infections. For more information, see the Infection section.
Other common noninfectious oral findings
Hairy tongue is characterized by marked accumulation of keratin on the dorsum of the tongue, resulting in a hair-like appearance. This occurs largely because of limited oral intake, soft/liquid diet, and xerostomia. Similar hyperkeratosis (although not hair-like) may be observed on the hard palate and gingiva. Thrombocytopenia predisposes the oral mucosa to development of asymptomatic petechiae and ecchymoses and sometimes hematomas. The lesions may appear at the buccal mucosa, lateral tongue, and soft palate, secondary to chewing and swallowing, and resolve with the restoration of platelet count.
Oral Health After Transplant
Mouth care and dental care
Following hospital discharge after HSCT, patients are instructed to continue daily routine mouth care and see a dentist for a routine follow-up examination and dental prophylaxis approximately 6 months after a HSCT and every 6 months thereafter.[2,5][Level of evidence: IV]
GVHD
GVHD can be broadly classified as acute or chronic, with defining features being largely clinical rather than by time frame of onset.[9] (See Table 6 and Table 7.)
Maculopapular rash, erythroderma with or without bulla
Poikiloderma, lichen planus-like changes, scleroderma, nail dystrophy
Gastrointestinal
Nausea, vomiting, diarrhea, anorexia
Liver
Elevated bilirubin levels
Lung
Bronchiolitis obliterans
Genital
Lichen planus-like changes
Acute GVHD
Acute GVHD typically occurs within the first 100 days and classically presents with skin, liver, and gastrointestinal tract involvement. Infrequently, the mouth can be affected, presenting with erythema multiforme-like features, including lip crusting and diffuse intraoral erythema and ulcerations.[10]
Chronic GVHD
Chronic GVHD, which affects 50% to 80% of allogeneic HSCT recipients, is an autoimmune-like condition characterized by chronic inflammation, fibrosis, disability, and diminished quality of life.[9,11] The oral cavity is commonly affected and is often the initial site of involvement. GVHD can persist in the oral cavity after it has resolved in other affected areas.
Clinical features of oral chronic GVHD
Oral mucosal involvement resembles oral lichen planus, with characteristic lacy white striations, erythema, and ulcerations.[10,11] Lesions can present on all oral mucosal surfaces but most frequently affect the buccal mucosa and tongue. Lip involvement can also be prominent, ranging from hyperkeratosis and dryness to extensive ulceration. Superficial mucoceles—characterized by small, transient, clear-fluid–filled vesicles—are particularly common on the palate, which has a high concentration of minor salivary gland tissue. While oral mucosal chronic GVHD can be painful at rest, the most common symptom is sensitivity, defined as oral discomfort with stimulation, typically with acidic, spicy, or strongly flavored items (e.g., mint, chocolate), as well as hard and crusty foods.
Chronic GVHD affecting the salivary glands resembles Sjögren syndrome, and affected patients frequently have concurrent involvement of the lacrimal glands and associated ocular chronic GVHD. In addition to experiencing symptoms of xerostomia, patients are at increased risk of developing dental caries and recurrent oral candidiasis. Oral mucosal sensitivity, even in the absence of mucosal lichenoid changes, is common.
Sclerodermatous chronic GVHD affecting the oral cavity is uncommon but can be debilitating. Patients with cutaneous, sclerodermatous chronic GVHD may have extension to the perioral tissues, leading to limited mouth opening, as seen in patients with progressive systemic sclerosis. Intraoral fibrosis can also occur, typically in patients with long-standing oral mucosal chronic GVHD. This condition presents with tight bands in the buccal mucosa. In addition to experiencing pain and disability, patients can have difficulty maintaining oral hygiene, and provision of dental care can be challenging.
Diagnosis and management of oral chronic GVHD
The presence of lacy white changes in the oral cavity is diagnostic for chronic GVHD, according to the National Institutes of Health Consensus.[11] Biopsy is rarely necessary for diagnosis. Ancillary management of oral mucosal chronic GVHD includes topical steroids and topical tacrolimus. Patients often avoid bothersome foods and drinks.[12]
Table 8. Management of Oral Chronic Graft-Versus-Host Diseasea
Oral Complications
Management Considerations
Long-Term Follow-Up Considerations
aAdapted from Rizzo et al.[13] and Carpenter et al.2014,[12]
Mucosal lichenoid changes
Topical corticosteroids
Increased risk of oral squamous cell carcinoma; cancer screening
Intralesional corticosteroid therapy
Topical tacrolimus
Topical analgesics
Children’s toothpaste
Avoidance of spicy, acidic, and hard/crunchy foods and drinks
Salivary gland hypofunction
Topical fluoride
Dental follow-up at least annually (risk of dental caries); monitoring of tooth development in children
Sialogogue therapy
Over-the-counter dry mouth products
Sugar-free gum/candy
Education regarding preventive practices
Management of recurrent candidiasis
Sclerodermatous chronic graft-versus-host disease
Physical therapy
Other associated lesions
A wide range of oral mucosal lesions frequently arises in the context of chronic GVHD. These lesions include both benign (infectious and noninfectious) and malignant conditions.
Benign lesions
Herpes simplex virus and oral candidiasis can occur in the context of oral chronic GVHD owing to several factors, including generalized immunosuppression, salivary gland hypofunction, and the use of topical steroids. For more information, see the Infection section.
Malignant lesions
Recipients of allogeneic HSCT are at increased risk of various cancers. Posttransplant lymphoproliferative disease can present with oral features similar to those seen in other presentations of lymphoma (mass, ulceration), typically in the early posttransplant period. Patients with chronic GVHD are at increased risk of developing oral squamous cell carcinoma, with this risk increasing with time since HSCT. Cancerous and precancerous oral lesions can be difficult to distinguish from those of chronic GVHD.
Long-term follow-up
Recipients of HSCT (in particular, allogeneic HSCT) are encouraged to maintain good oral health and receive long-term oral health care.[3,13] Patients are instructed to brush and floss daily, and to visit a dentist at least every 6 months. Patients with GVHD and salivary hypofunction are at risk of developing dental caries and experiencing tooth loss. Children, especially those who were younger than 6 years at HSCT, are at risk of developmental abnormalities affecting the skeleton and teeth. There is a significantly increased risk of oral squamous cell carcinoma in allogeneic HSCT recipients, especially in those with a history of oral chronic GVHD.
Table 9. Diseases Commonly Treated With Hematopoietic Stem Cell Transplanta
Majhail NS, Farnia SH, Carpenter PA, et al.: Indications for Autologous and Allogeneic Hematopoietic Cell Transplantation: Guidelines from the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant 21 (11): 1863-1869, 2015. [PUBMED Abstract]
Elad S, Raber-Durlacher JE, Brennan MT, et al.: Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: a position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Support Care Cancer 23 (1): 223-36, 2015. [PUBMED Abstract]
Bogusławska-Kapała A, Hałaburda K, Rusyan E, et al.: Oral health of adult patients undergoing hematopoietic cell transplantation. Pre-transplant assessment and care. Ann Hematol 96 (7): 1135-1145, 2017. [PUBMED Abstract]
Bollero P, Passarelli PC, D’Addona A, et al.: Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur Rev Med Pharmacol Sci 22 (4): 876-887, 2018. [PUBMED Abstract]
Lalla RV, Bowen J, Barasch A, et al.: MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 120 (10): 1453-61, 2014. [PUBMED Abstract]
Sung L, Robinson P, Treister N, et al.: Guideline for the prevention of oral and oropharyngeal mucositis in children receiving treatment for cancer or undergoing haematopoietic stem cell transplantation. BMJ Support Palliat Care 7 (1): 7-16, 2017. [PUBMED Abstract]
Cinausero M, Aprile G, Ermacora P, et al.: New Frontiers in the Pathobiology and Treatment of Cancer Regimen-Related Mucosal Injury. Front Pharmacol 8: 354, 2017. [PUBMED Abstract]
Lee SJ: Classification systems for chronic graft-versus-host disease. Blood 129 (1): 30-37, 2017. [PUBMED Abstract]
Ion D, Stevenson K, Woo SB, et al.: Characterization of oral involvement in acute graft-versus-host disease. Biol Blood Marrow Transplant 20 (11): 1717-21, 2014. [PUBMED Abstract]
Jagasia MH, Greinix HT, Arora M, et al.: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant 21 (3): 389-401.e1, 2015. [PUBMED Abstract]
Carpenter PA, Kitko CL, Elad S, et al.: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. The 2014 Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 21 (7): 1167-87, 2015. [PUBMED Abstract]
Rizzo JD, Wingard JR, Tichelli A, et al.: Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation: joint recommendations of the European Group for Blood and Marrow Transplantation, Center for International Blood and Marrow Transplant Research, and the American Society for Blood and Marrow Transplantation (EBMT/CIBMTR/ASBMT). Bone Marrow Transplant 37 (3): 249-61, 2006. [PUBMED Abstract]
Copelan EA: Hematopoietic stem-cell transplantation. N Engl J Med 354 (17): 1813-26, 2006. [PUBMED Abstract]
Oral Management of Patients Receiving Targeted Therapy/Cancer Immunotherapy
Targeted Therapy
Targeted therapy acts either directly on specific tissues, cells, and/or genes or indirectly on growth-related tissues and the nutrition of cancer cells. Antiangiogenesis therapies can suppress the formation of new blood vessels that nourish cancer tissue, preventing its growth.[1,2]
Table 10. Oral Management of Patients Receiving Targeted Cancer Therapy or Immunotherapy
Before Cancer Therapy
During Cancer Therapy
After Cancer Therapy
Document baseline oral mucosal status
Assess number and severity of oral mucosal lesions clinically documented to be caused by targeted therapy/immunotherapy
Monitor for possible late adverse oral effects
Provide patient education
Provide topical, intralesional, or systemic steroid treatment if oral pain is severe
Targeted therapy: Monitor for and treat gingival bleeding, necrotizing ulcerative gingivitis, stomatitis, aphthous-like ulcers, hyperkeratosis
Immunotherapy: Monitor for and treat lichenoid reactions (ulcerative or reticular), benign membrane pemphigoid, xerostomia, taste changes
Oral lesions are common for both classes of medications; consider in differential diagnosis of candidiasis and herpes simplex infections, medication-related osteonecrosis of the jaw
As with other cancer therapy modalities, targeted therapy has toxicities inherent to the drug group. Among the most significant side effects are the cutaneous adverse effects.[3][Level of evidence: IV] The oral side effects are seen in more than 20% of patients. In severe cases, there is an indication of dose reduction or permanent treatment discontinuation.[3–5]
Table 11. Oral Toxicities of Cancer Drugs
Cancer Drug
Oral Side Effects
EGFR = epidermal growth factor receptor; MRONJ = medication-related osteonecrosis of the jaw; mTOR = mechanistic target of rapamycin; PDGF = platelet-derived growth factor; VEGF = vascular endothelial growth factor.
MRONJ, erythema and atrophy of tissue, pigmentary changes and lichenoid reaction, mucositis, dysgeusia
Cancer Immunotherapy
Immunotherapies have a different profile than targeted therapies and a new spectrum of toxicities compared with cytotoxic agents. The mechanism of action of immune checkpoint inhibitors involves triggering cytotoxic T-cell activation and inducing a specific toxicity profile that is primarily of immunologic origin. The most commonly reported immune-related systemic adverse events include the following:[11,12][Level of evidence: IV]
Dermatitis.
Enterocolitis.
Liver toxicities.
Endocrinopathies.
Pneumonitis.
Renal toxicity and other less common toxicities.
Reports of oral complications related to immunotherapies are sparse in the literature and most often include xerostomia, dysgeusia, and lichenoid reactions.[4,13] Other side effects are bullous skin eruptions. Two cases of Stevens-Johnson syndrome with severe hemorrhagic cheilitis and erosions have been reported.[14–16]
Table 12. Systemic and Oral Toxicities of Cancer Immunotherapy
Side Effects
Systemic Toxicities
Oral Toxicities
Acute side effects
Dermatitis
Lichenoid reactions; other immune-related lesions; xerostomia; taste changes; infections such as candidiasis and herpes simplex; osteonecrosis of the jaw
Lichenoid lesions
Bullous eruptions
Stevens-Johnson syndrome
Enterocolitis clinical expressed as diarrhea, liver toxicity
Endocrinopathies such as hypophysitis, thyroiditis, uveitis, pneumonitis, renal toxicity, infections, neurological events
Delayed events
Pneumonitis
The largest reported series of oral immune-related lichenoid reactions included ten cases.[17] Four patients also showed skin, nail, or genital lesions. Tenderness and/or irritation and xerostomia were present in three patients. The lesions were self-limited and low grade, did not lead to discontinuation or interruption in oncologic treatment, and improved after several weeks of topical corticosteroid treatment. The authors reported that oral lichenoid reactions were common in their clinical practice.
Exacerbations of preexisting autoimmune disease have been reported and necessitated systemic treatment. A detailed history of preexisting autoimmune disease and vigilant clinical monitoring are important for these patients.[18–21]
Osteonecrosis related to immunotherapy alone has rarely been reported.[3,22] However, with the increasing use of combinations of medications, clinicians should remain alert for these complications.
Cancer immunotherapy can cause other side effects, which may be acute or delayed.
Consequences of cancer immunotherapy oral side effects and toxicities include the following:
Therapy dose modifications or discontinuation.
Inadequate food intake and diet changes.
Poor oral health.
Risk of oral infections.
Increased dental caries.
Need for dental extractions.
Weight loss.
Clinicians should be aware of immune-related oral adverse events. Routine evaluation of the oral cavity should be incorporated into the care of all patients, particularly those who are already at risk of oral complications—for example, patients with head and neck cancer who receive radiation therapy and patients who receive bone-targeting agents, targeted therapies (mainly inhibitors of angiogenesis), and other drugs.
Before targeted therapy/cancer immunotherapy
A patient’s medical history report will disclose any preexisting autoimmune oral disease. As in any cancer therapy, oral and dental examination and stabilization are mandatory. Patient education on the importance of good oral health and oral hygiene is needed.[23–25]
During targeted therapy/cancer immunotherapy
Oral management during targeted therapy follows the same guidelines as those used for chronic graft-versus-host disease in patients with hematological conditions after bone marrow transplant.[23] Patients are encouraged to maintain good oral hygiene and to report any symptoms. If an oral lesion is suspected or diagnosed, the dentist will refer the patient to an oral oncology clinic and communicate this information to the treating oncologist. Early intervention and continued monitoring are required to limit exacerbation of the oral changes. Mucosal changes may be managed with topical anti-inflammatory agents. Severe cases may require systemic steroids. Dysplasia in lichenoid lesions is possible. If mucosal pain is present, topical analgesics may be considered. Dry mouth may include treatment with mouth-wetting agents and management of dental caries risk in the presence of hyposalivation, as well as prevention and management of oral candidiasis, herpes simplex, or other oral infections.[26]
After targeted therapy/cancer immunotherapy
Follow-up after targeted therapy or immunotherapy is important, as late adverse events may develop. The increased use of combination treatment may disclose new adverse events that have not yet been recognized.
Having an oral specialist on the oncology team greatly helps in the description, identification, early diagnosis, and timely and successful management of oral side effects related to immunotherapies alone or combined with other biological therapies.
References
National Cancer Institute: Targeted Therapy to Treat Cancer. Bethesda, Md: National Institutes of Health, 2022. Available online. Last accessed Feb. 14, 2024.
Carrington C: Oral targeted therapy for cancer. Aust Prescr 38 (5): 171-6, 2015. [PUBMED Abstract]
Nicolatou-Galitis O, Kouri M, Papadopoulou E, et al.: Osteonecrosis of the jaw related to non-antiresorptive medications: a systematic review. Support Care Cancer 27 (2): 383-394, 2019. [PUBMED Abstract]
Vigarios E, Epstein JB, Sibaud V: Oral mucosal changes induced by anticancer targeted therapies and immune checkpoint inhibitors. Support Care Cancer 25 (5): 1713-1739, 2017. [PUBMED Abstract]
Lacouture M, Sibaud V: Toxic Side Effects of Targeted Therapies and Immunotherapies Affecting the Skin, Oral Mucosa, Hair, and Nails. Am J Clin Dermatol 19 (Suppl 1): 31-39, 2018. [PUBMED Abstract]
Gomez-Fernandez C, Garden BC, Wu S, et al.: The risk of skin rash and stomatitis with the mammalian target of rapamycin inhibitor temsirolimus: a systematic review of the literature and meta-analysis. Eur J Cancer 48 (3): 340-6, 2012. [PUBMED Abstract]
Boers-Doets CB, Epstein JB, Raber-Durlacher JE, et al.: Oral adverse events associated with tyrosine kinase and mammalian target of rapamycin inhibitors in renal cell carcinoma: a structured literature review. Oncologist 17 (1): 135-44, 2012. [PUBMED Abstract]
Watters AL, Epstein JB, Agulnik M: Oral complications of targeted cancer therapies: a narrative literature review. Oral Oncol 47 (6): 441-8, 2011. [PUBMED Abstract]
Martins F, de Oliveira MA, Wang Q, et al.: A review of oral toxicity associated with mTOR inhibitor therapy in cancer patients. Oral Oncol 49 (4): 293-8, 2013. [PUBMED Abstract]
Nicolatou-Galitis O, Migkou M, Psyrri A, et al.: Gingival bleeding and jaw bone necrosis in patients with metastatic renal cell carcinoma receiving sunitinib: report of 2 cases with clinical implications. Oral Surg Oral Med Oral Pathol Oral Radiol 113 (2): 234-8, 2012. [PUBMED Abstract]
Michot JM, Bigenwald C, Champiat S, et al.: Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer 54: 139-148, 2016. [PUBMED Abstract]
Wang PF, Chen Y, Song SY, et al.: Immune-Related Adverse Events Associated with Anti-PD-1/PD-L1 Treatment for Malignancies: A Meta-Analysis. Front Pharmacol 8: 730, 2017. [PUBMED Abstract]
Nikolaou V, Voudouri D, Tsironis G, et al.: Cutaneous toxicities of antineoplastic agents: data from a large cohort of Greek patients. Support Care Cancer 27 (12): 4535-4542, 2019. [PUBMED Abstract]
Jour G, Glitza IC, Ellis RM, et al.: Autoimmune dermatologic toxicities from immune checkpoint blockade with anti-PD-1 antibody therapy: a report on bullous skin eruptions. J Cutan Pathol 43 (8): 688-96, 2016. [PUBMED Abstract]
Saw S, Lee HY, Ng QS: Pembrolizumab-induced Stevens-Johnson syndrome in non-melanoma patients. Eur J Cancer 81: 237-239, 2017. [PUBMED Abstract]
Salati M, Pifferi M, Baldessari C, et al.: Stevens-Johnson syndrome during nivolumab treatment of NSCLC. Ann Oncol 29 (1): 283-284, 2018. [PUBMED Abstract]
Sibaud V, Eid C, Belum VR, et al.: Oral lichenoid reactions associated with anti-PD-1/PD-L1 therapies: clinicopathological findings. J Eur Acad Dermatol Venereol 31 (10): e464-e469, 2017. [PUBMED Abstract]
Johnson DB, Sullivan RJ, Ott PA, et al.: Ipilimumab Therapy in Patients With Advanced Melanoma and Preexisting Autoimmune Disorders. JAMA Oncol 2 (2): 234-40, 2016. [PUBMED Abstract]
Danlos FX, Voisin AL, Dyevre V, et al.: Safety and efficacy of anti-programmed death 1 antibodies in patients with cancer and pre-existing autoimmune or inflammatory disease. Eur J Cancer 91: 21-29, 2018. [PUBMED Abstract]
Ijaz A, Khan AY, Malik SU, et al.: Significant Risk of Graft-versus-Host Disease with Exposure to Checkpoint Inhibitors before and after Allogeneic Transplantation. Biol Blood Marrow Transplant 25 (1): 94-99, 2019. [PUBMED Abstract]
Economopoulou P, Nicolatou-Galitis O, Kotsantis I, et al.: Nivolumab-related lichen planus of the lip in a patient with head and neck cancer. Oral Oncol 104: 104623, 2020. [PUBMED Abstract]
Nifosì AF, Zuccarello M, Nifosì L, et al.: Osteonecrosis of the jaw in the era of targeted therapy and immunotherapy in oncology. J Korean Assoc Oral Maxillofac Surg 45 (1): 3-8, 2019. [PUBMED Abstract]
Epstein JB, Smutzer G, Doty RL: Understanding the impact of taste changes in oncology care. Support Care Cancer 24 (4): 1917-31, 2016. [PUBMED Abstract]
Elad S, Jensen SB, Raber-Durlacher JE, et al.: Clinical approach in the management of oral chronic graft-versus-host disease (cGVHD) in a series of specialized medical centers. Support Care Cancer 23 (6): 1615-22, 2015. [PUBMED Abstract]
Elad S, Raber-Durlacher JE, Brennan MT, et al.: Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: a position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Support Care Cancer 23 (1): 223-36, 2015. [PUBMED Abstract]
Rapoport BL, van Eeden R, Sibaud V, et al.: Supportive care for patients undergoing immunotherapy. Support Care Cancer 25 (10): 3017-3030, 2017. [PUBMED Abstract]
Orofacial Pain in Patients With Cancer
Orofacial pain may be present throughout the cancer continuum. In patients with head and neck cancer (HNC), orofacial pain has been reported to be as high as 85% at the time of cancer diagnosis.[1];[2][Level of evidence: II][3]
Orofacial pain is frequently associated with locoregional cancer, but it can also be a sign of systemic and distant cancers. It may arise from the onset of the disease and develops as the disease progresses. Orofacial pain is also highly associated with acute-treatment side effects and may continue after treatment ends due to persistence, recurrence, or metastasis of the primary cancer or acute and chronic toxicities of cancer therapy.[4] It is important to recognize not only the diverse symptoms of orofacial pain in patients with cancer, but also pain’s significant impact on their quality of life.
The management of head and neck pain and oral and oropharyngeal pain may be particularly challenging because the area is a highly innervated sensory region, and eating, speech, swallowing, and other motor functions of the head and neck and oropharynx are constant pain triggers. Classification of head and neck pain can assist in management.[5]
For more information on pain in patients with cancer, see Cancer Pain.
Orofacial Pain Caused by Cancer Persistence, Recurrence, or Metastasis
Etiology and epidemiology
Pain caused by cancer is often low intensity, but it typically becomes more frequent and increasingly severe with advancing disease. Cancer pain may be caused by local tumor effects via direct invasion of adjacent structures, leading to pressure, ulceration, tissue necrosis, and perineural invasion.[6,7]
Pain may also be aggravated by distant tumors or systemic cancer activity (e.g., blood and lymphatic cancers) due to nociceptive, inflammatory, and neuropathic mechanisms. For instance, oral manifestations of blood cancers such as leukemia, lymphoma, and multiple myeloma may cause pain and loss of function by infiltrating pain-sensitive structures [5] or inducing secondary oral infections due to a compromised immune system.[8] Furthermore, intracranial malignancies may give rise to orofacial pain and headaches due to pressure or infiltration of specific brain centers and structures.
Signs and symptoms
In the orofacial region, pain may present similarly to classic trigeminal neuralgia/neuropathic pain or musculoskeletal temporomandibular disorders. Symptoms range from acute, localized, sharp shooting episodes to chronic, diffuse, pressing, and aching pain.[5]
Patients with nasopharyngeal and oropharyngeal cancer may report pain in the temporomandibular joint region with limited mouth opening; ear blockage, ringing, or pain; headaches; facial numbness; and masticatory muscle stiffness. These signs and symptoms may result from direct tumor invasion or represent a pattern of referred pain that can masquerade as a temporomandibular joint disorder.[9,10]
Paraneoplastic neuropathies may present in cancer patients, particularly those with lung cancer or lymphoma.[11,12][Level of evidence: IV] This effect may manifest as difficulty swallowing, slurred speech, disturbed vision, seizures, facial muscle weakness, stiffness, or unusual involuntary contractions.[12][Level of evidence: IV]
Diagnosis and management strategies
Meticulous clinical examination is a critical step in reporting orofacial pain or dysfunction. Pain can be reported in any structure of the craniofacial region, such as a toothache or pain in the gingiva, tongue, face, neck, ear, and pharynx.[6] Management relies mainly on treating the malignancy. Since pain caused by cancer therapy is common, further pharmacotherapeutics and supportive treatment regimens may be needed. For more information on pharmacotherapeutic interventions and supportive regimens, see the Diagnostic investigations and management strategies section.
Orofacial Pain Caused by Cancer Management
Etiology and epidemiology
While surgical resection provides near complete relief of HNC-related pain, some patients require adjuvant therapies such as chemotherapy (i.e., cytotoxic agents and targeted biological agents) and/or radiation therapy to further combat the disease.[13][Level of evidence: IV] Other cancer patients may be restricted to nonsurgical interventions because of the type or extent of their cancers. Stem cell transplant, another approach for managing hematologic malignancies, can involve chemotherapy and/or total body radiation as part of the management regimen. These surgical and nonsurgical interventions, especially concomitant chemoradiotherapy, are tied to short- and long-lasting painful complications that may affect patient well-being and quality of life.[5]
More than 70% of patients with HNC report variable forms of pain during and after their cancer therapy.[5]
Signs and symptoms
Pain associated with surgical interventions
For patients with HNC undergoing surgical interventions, acute nociceptive regional orofacial pain, scar formation, and sensory impairment are inevitable. These complications increase dramatically with concomitant procedures, such as neck dissection, and may evolve to long-term, painful, postsurgical fibrosis and neuropathy.[5] Fifty percent to 90% of patients who undergo mandibulectomy or maxillectomy have regional hyperalgesia and allodynia. Pain scores following HNC surgery are the highest for the oral cavity, followed by the larynx, oropharynx, and nasopharynx. The most common locations for orofacial pain complaints are the oral cavity, followed by the temporomandibular joint, face, neck, and shoulders.[5] Musculoskeletal syndromes, including temporomandibular disorders associated with muscular fibrosis and limited jaw opening, lead to significant pain and loss of orofacial function. The persistence of these complications may severely impact cancer survivors’ quality of life and well-being.[14][Level of evidence: II];[15]Level of evidence: IV
Pain associated with chemotherapy and radiation therapy
Orofacial pain as a result of cancer chemotherapy and radiation therapy is a well-recognized complication that may longitudinally affect cancer survivors’ quality of life.[1,4,16,17] Generally, 60% to 80% of cancer patients experience pain during these interventions, with a significant number continuing to struggle from long-term, persistent pain complaints after the completion of therapy.[18]
Severe peripheral neurotoxicity leads to neuropathic orofacial pain, changes in taste, and loss of sensory perception and motor coordination. Localized oral burning pain, comparable to burning mouth syndrome, can also occur. Cytotoxic effects of chemotherapy and radiation therapy may cause oral mucositis. For more information, see the Oral mucositis (high-dose chemotherapy, HSCT, head and neck radiation) section. Oral ulcerations due to neutropenia or oral bacterial, fungal, and viral infections are other examples of common, acute, painful complications encountered during and after anticancer therapy.[13,19] In addition, compromised immune function may lead to reactivation of dormant herpes viruses, causing painful oral and para-oral lesions. Postherpetic neuralgia, if emerged, can cause chronic dysesthesias in the affected area that may persist for years.[20] Moreover, hyposalivation, especially in those receiving head and neck radiation, may enhance susceptibility to oral candidiasis and rampant caries.[21][Level of evidence: II]
Several targeted biological agents, such as tyrosine-kinase inhibitors and immune checkpoint inhibitors, have proven efficacy in managing patients with cancer. In the orofacial pain region, these therapies may cause taste alterations, aphthous-like ulceration, and mucosal lichenoid reactions.[22][Level of evidence: III];[23] Combinations of multiple agents may result in increasingly complex mucosal changes and related symptoms.[5,22] For more information, see the Oral management during targeted therapy/cancer immunotherapy section.
When they occur during cancer therapy, these complications can negatively affect patients’ nutritional status and lead to undesired interruption or reduction of the dose or frequency of the cancer treatment regimen.[17,24] Furthermore, the long-term impact of anticancer therapy may significantly compromise the physical, psychological, and financial well-being of cancer survivors.[25–27][Level of evidence: II]
Pain associated with stem cell transplant therapy
Graft-versus-host disease is a common complication of allogeneic hematopoietic stem cell transplant, occurring in 25% to 70% of patients and presenting in both acute and chronic forms. Head and neck involvement is manifested as mucosal striation/ulceration, superficial mucocele, and temporomandibular joint arthritic dysfunction that are often painful.[20,28] Additionally, increased thermal sensitivity has been observed in patients being treated with cyclosporine after their hematopoietic stem cell transplants.[29][Level of evidence: III]
Diagnostic investigations and management strategies
As cancer pain is mixed in nature and presentation, specific screening and assessment questionnaires are useful in differentiating nociceptive and neuropathic pain and help to better manage orofacial pain. In the oncology setting, it is important that a thorough health history and oral physical examination be performed when oral pain is present. The role of routine high-maintenance levels of oral hygiene cannot be understated. Radiographic imaging and vitality testing of the dental pulp are typically necessary.[13]
Persistent neuropathies are a common complication after HNC surgical interventions and radiation therapies.[13,30] Selected classes of chemotherapy, such as vinca alkaloids, vincristine, vinblastine, platinum-based drugs, taxanes, and targeted biological agents, can also cause direct neurotoxicity.[13,31] Additionally, drugs such as thalidomide and lenalidomide are associated with peripheral neuropathies that can affect the orofacial region. Deeply-seated mandibular pain may be of dental etiology as a consequence of pulpal neurotoxicity or necrosis.
Management of neuropathic orofacial pain is complex and challenging, often involving centrally and peripherally acting pharmacotherapeutic agents. Topical and systemic gabapentinoids, membrane stabilizers, small doses of tricyclic antidepressants, selective serotonin-norepinephrine reuptake inhibitors, vanilloid receptor inhibitors, and cannabinoids are often prescribed.[32][Level of evidence: I];[33][Level of evidence: IV];[34,35] Supportive approaches such as counseling, acupuncture, photobiomodulation, and neurosensory stents may also be considered. Preventive measures such as physical shielding and cryotherapy should be considered before and during anticancer therapy to reduce cytotoxic and neurotoxic outcomes.[36]
Dental hypersensitivity may occasionally arise in the weeks or months after the discontinuation of chemotherapy and/or radiation therapy.[13] Topical application of fluorides and desensitizing agents may ameliorate dental discomfort.[13] In most instances, thermal sensitivity observed in patients who received hematopoietic stem cell transplant is self-resolving after discontinuation of cyclosporine.[29][Level of evidence: III]
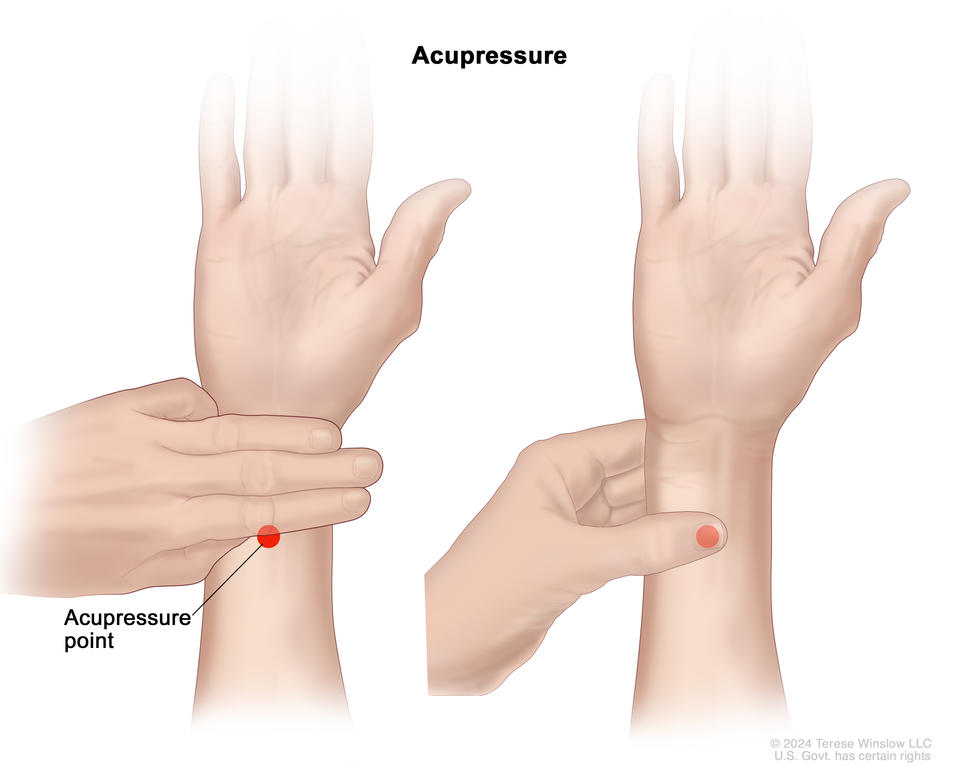
Patients may also experience musculoskeletal pain and dysfunction involving muscles of mastication, the neck, and/or the temporomandibular joints.[37] These conditions may be further aggravated by stress, sleep disturbance, and parafunctional habits (i.e., bruxism and clenching) after treatment of HNC.[38][Level of evidence: IV] Physical management of orofacial pain, including cold compresses or moist heat combined with physical therapy, custom occlusal splints, and masticatory/neck muscle exercises, help significantly. Judicious use of muscle relaxants or anxiolytic agents can be considered. Acupuncture, transcutaneous nerve stimulation, low-level laser use, and massage therapy are adjuvant modalities to alleviate pain in patients with cancer.[39,40][Level of evidence: I];[41][Level of evidence: I] For more information, see Acupuncture.
Additionally, psychological approaches such as counseling, distraction, relaxation techniques, biofeedback, group therapy, self-hypnosis, imagery, and cognitive behavioral training programs have shown promising results in randomized clinical trials.[39,42][Level of evidence: I];[43][Level of evidence: I]
References
Holländer-Mieritz C, Johansen J, Johansen C, et al.: Comparing the patients’ subjective experiences of acute side effects during radiotherapy for head and neck cancer with four different patient-reported outcomes questionnaires. Acta Oncol 58 (5): 603-609, 2019. [PUBMED Abstract]
Carpén T, Sjöblom A, Lundberg M, et al.: Presenting symptoms and clinical findings in HPV-positive and HPV-negative oropharyngeal cancer patients. Acta Otolaryngol 138 (5): 513-518, 2018. [PUBMED Abstract]
Saunders DP, Epstein JB, Elad S, et al.: Systematic review of antimicrobials, mucosal coating agents, anesthetics, and analgesics for the management of oral mucositis in cancer patients. Support Care Cancer 21 (11): 3191-207, 2013. [PUBMED Abstract]
Saunders DP, Rouleau T, Cheng K, et al.: Systematic review of antimicrobials, mucosal coating agents, anesthetics, and analgesics for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer 28 (5): 2473-2484, 2020. [PUBMED Abstract]
Epstein JB, Miaskowski C: Oral Pain in the Cancer Patient. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Romero-Reyes M, Teruel A, Ye Y: Cancer and Referred Facial Pain. Curr Pain Headache Rep 19 (8): 37, 2015. [PUBMED Abstract]
Schmidt BL: The Neurobiology of Cancer Pain. J Oral Maxillofac Surg 73 (12 Suppl): S132-5, 2015. [PUBMED Abstract]
Silva TD, Ferreira CB, Leite GB, et al.: Oral manifestations of lymphoma: a systematic review. Ecancermedicalscience 10: 665, 2016. [PUBMED Abstract]
Jamal Zohaib, Anjum Fatima: Oropharyngeal Squamous Cell Carcinoma. In: StatPearls [Internet]. StatPearls Publishing, 2024, Treasure Island, FL: StatsPearls [Internet], 2023. Available online. Last accessed October 10, 2023.
Shah Abdul B., Nagalli Shivaraj: Nasopharyngeal Carcinoma. In: StatPearls [Internet]. StatPearls Publishing, 2024, Treasure Island, FL: StatPearls [Internet], 2023. Available online. Last accessed October 10, 2023.
Zoccarato M, Grisold W, Grisold A, et al.: Paraneoplastic Neuropathies: What’s New Since the 2004 Recommended Diagnostic Criteria. Front Neurol 12: 706169, 2021. [PUBMED Abstract]
Sroussi HY, Epstein JB, Bensadoun RJ, et al.: Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med 6 (12): 2918-2931, 2017. [PUBMED Abstract]
Pauli N, Mejersjö C, Fagerberg-Mohlin B, et al.: Temporomandibular disorder in head and neck cancer patients undergoing radiotherapy: Clinical findings and patient-reported symptoms. Head Neck 41 (10): 3570-3576, 2019. [PUBMED Abstract]
Nicot R, Raoul G, Ferri J, et al.: Temporomandibular disorders in head and neck cancers: Overview of specific mechanisms and management. J Stomatol Oral Maxillofac Surg 121 (5): 563-568, 2020. [PUBMED Abstract]
Schmitd LB, Scanlon CS, D’Silva NJ: Perineural Invasion in Head and Neck Cancer. J Dent Res 97 (7): 742-750, 2018. [PUBMED Abstract]
Jones JA, Chavarri-Guerra Y, Corrêa LBC, et al.: MASCC/ISOO expert opinion on the management of oral problems in patients with advanced cancer. Support Care Cancer 30 (11): 8761-8773, 2022. [PUBMED Abstract]
Mirabile A, Airoldi M, Ripamonti C, et al.: Pain management in head and neck cancer patients undergoing chemo-radiotherapy: Clinical practical recommendations. Crit Rev Oncol Hematol 99: 100-6, 2016. [PUBMED Abstract]
Binczak M, Navez M, Perrichon C, et al.: Management of somatic pain induced by head-and-neck cancer treatment: definition and assessment. Guidelines of the French Oto-Rhino-Laryngology- Head and Neck Surgery Society (SFORL). Eur Ann Otorhinolaryngol Head Neck Dis 131 (4): 243-7, 2014. [PUBMED Abstract]
Vickers ER, Karsten E, Flood J, et al.: A preliminary report on stem cell therapy for neuropathic pain in humans. J Pain Res 7: 255-63, 2014. [PUBMED Abstract]
Lin A, Helgeson ES, Treister NS, et al.: The impact of head and neck radiotherapy on salivary flow and quality of life: Results of the ORARAD study. Oral Oncol 127: 105783, 2022. [PUBMED Abstract]
Shazib MA, Woo SB, Sroussi H, et al.: Oral immune-related adverse events associated with PD-1 inhibitor therapy: A case series. Oral Dis 26 (2): 325-333, 2020. [PUBMED Abstract]
Carrozzo M, Eriksen JG, Bensadoun RJ, et al.: Oral Mucosal Injury Caused by Targeted Cancer Therapies. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Hunter M, Kellett J, Toohey K, et al.: Toxicities Caused by Head and Neck Cancer Treatments and Their Influence on the Development of Malnutrition: Review of the Literature. Eur J Investig Health Psychol Educ 10 (4): 935-949, 2020. [PUBMED Abstract]
Han X, Zhao J, Zheng Z, et al.: Medical Financial Hardship Intensity and Financial Sacrifice Associated with Cancer in the United States. Cancer Epidemiol Biomarkers Prev 29 (2): 308-317, 2020. [PUBMED Abstract]
Yabroff KR, Bradley C, Shih YT: Understanding Financial Hardship Among Cancer Survivors in the United States: Strategies for Prevention and Mitigation. J Clin Oncol 38 (4): 292-301, 2020. [PUBMED Abstract]
Utley M, Adeyanju T, Bernardo B, et al.: The association between mental health, social support and physical health outcomes among older female cancer survivors. J Geriatr Oncol 13 (6): 834-838, 2022. [PUBMED Abstract]
Fall-Dickson JM, Pavletic SZ, Mays JW, et al.: Oral Complications of Chronic Graft-Versus-Host Disease. J Natl Cancer Inst Monogr 2019 (53): , 2019. [PUBMED Abstract]
Epstein JB, Raber-Durlacher JE, Epstein GL, et al.: Chronic oral graft-versus-host disease: induction and maintenance therapy with photobiomodulation therapy. Support Care Cancer 29 (3): 1387-1394, 2021. [PUBMED Abstract]
Van den Bosch L, van der Schaaf A, van der Laan HP, et al.: Comprehensive toxicity risk profiling in radiation therapy for head and neck cancer: A new concept for individually optimised treatment. Radiother Oncol 157: 147-154, 2021. [PUBMED Abstract]
Brook I: Early side effects of radiation treatment for head and neck cancer. Cancer Radiother 25 (5): 507-513, 2021. [PUBMED Abstract]
Smith DK, Cmelak A, Niermann K, et al.: Preventive use of gabapentin to decrease pain and systemic symptoms in patients with head and neck cancer undergoing chemoradiation. Head Neck 42 (12): 3497-3505, 2020. [PUBMED Abstract]
Häuser W, Finn DP, Kalso E, et al.: European Pain Federation (EFIC) position paper on appropriate use of cannabis-based medicines and medical cannabis for chronic pain management. Eur J Pain 22 (9): 1547-1564, 2018. [PUBMED Abstract]
Häuser W, Finnerup NB, Moore RA: Systematic reviews with meta-analysis on cannabis-based medicines for chronic pain: a methodological and political minefield. Pain 159 (10): 1906-1907, 2018. [PUBMED Abstract]
Mücke M, Phillips T, Radbruch L, et al.: Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst Rev 3 (3): CD012182, 2018. [PUBMED Abstract]
de Pauli Paglioni M, Alves CGB, Fontes EK, et al.: Is photobiomodulation therapy effective in reducing pain caused by toxicities related to head and neck cancer treatment? A systematic review. Support Care Cancer 27 (11): 4043-4054, 2019. [PUBMED Abstract]
Brook I: Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J 38 (2): 84-92, 2020. [PUBMED Abstract]
Buglione M, Cavagnini R, Di Rosario F, et al.: Oral toxicity management in head and neck cancer patients treated with chemotherapy and radiation: Xerostomia and trismus (Part 2). Literature review and consensus statement. Crit Rev Oncol Hematol 102: 47-54, 2016. [PUBMED Abstract]
Bennett MI, Eisenberg E, Ahmedzai SH, et al.: Standards for the management of cancer-related pain across Europe-A position paper from the EFIC Task Force on Cancer Pain. Eur J Pain 23 (4): 660-668, 2019. [PUBMED Abstract]
Wan Q, Chen H, Wang X, et al.: Effectiveness of different acupuncture therapies for chronic cancer pain: A protocol for systematic review and Bayesian network meta-analysis. Medicine (Baltimore) 101 (4): e27965, 2022. [PUBMED Abstract]
Dymackova R, Selingerova I, Kazda T, et al.: Effect of Acupuncture in Pain Management of Head and Neck Cancer Radiotherapy: Prospective Randomized Unicentric Study. J Clin Med 10 (5): , 2021. [PUBMED Abstract]
Abbas Q, Arooj N, Baig KB, et al.: A clinical trial of cognitive behavior therapy for psychiatric comorbidity and quality of life with Cancer Patients during Chemotherapy (CPdC). BMC Psychiatry 22 (1): 222, 2022. [PUBMED Abstract]
Okuyama T, Akechi T, Mackenzie L, et al.: Psychotherapy for depression among advanced, incurable cancer patients: A systematic review and meta-analysis. Cancer Treat Rev 56: 16-27, 2017. [PUBMED Abstract]
Infection
The intactness of skin and mucosa are physical barriers to infection. The epithelium of the oral mucosa impedes the attachment of pathogenic organisms by shedding dead cells and pathogens. This process limits the penetration of many compounds into the epithelium by maintaining a chemical barrier of antimicrobial molecules. These molecules are part of salivary protection and saliva, which are also responsible for protectively cleaning the teeth and mucosa and maintaining neutral pH, and lubrication.[1]
Oral infections in cancer patients could be caused by a preexisting acute oral infection before the therapy is administered; therefore, control and elimination of these infections play a crucial role.[2] Other infections typically arise in the setting of the immunocompromised host response during therapy.
Oral mucositis is a common complication of cancer therapy. In addition to causing severe pain and nutritional impairment, there is an increased risk of local and systemic infections.[3] Oral mucositis can be complicated by infection in immunocompromised patients. Importantly, disruption of the oral mucosa provides a major route of entry for pathological microorganisms. This situation can lead to various infections, including fatal septicemia.[4] For more information, see the Oral mucositis (high-dose chemotherapy, HSCT, head and neck radiation) section.
Both indigenous oral flora and hospital-acquired pathogens have been associated with bacteremias and systemic infection. As the absolute neutrophil count falls below 1,000/µL, the incidence and severity of infection rise. Patients with prolonged neutropenia are at higher risk of developing serious infectious complications. The rate and severity of these infections mostly depend on prolonged periods of neutropenia (more than 7 days).[5][Level of evidence: IV] Compromised salivary function and poor oral hygiene alter oral microbial flora and increase oral microbial load, making patients susceptible to opportunistic bacterial, viral, and fungal infections. Patients have a higher risk of developing odontogenic infections if they do not receive prompt care for any dental or periodontal disorder.[6]
Other oral sites, including the dentition, periapices, and periodontium, can also become acutely infected during myelosuppression secondary to high-dose chemotherapy.[2]
A literature search was conducted in the MEDLINE/PubMed and EMBASE databases for articles published between 2009 and 2016. Dental-related infections and abscesses during cancer therapy (primarily antineoplastic chemotherapy) were reported in six studies. The mean weighted prevalence was 5.4% (standard of error, 1.16; 95% confidence interval, 3.14–7.7).[7]
Dental management undertaken before cytoreductive therapy can substantially reduce the risk of infectious complications.[2] Researchers have shifted toward the idea that if there is a close relationship between the dental and oncology team, clearance of only acute infection before cancer therapy has similar results as completed dental management regarding oral infection during myelosuppression.[8][Level of evidence: II];[2,9][Level of evidence: III]
Bacterial Infections
Changes in infection profiles in patients with cancer-related myelosuppression have occurred over the past three decades. Multiple factors have caused this evolving epidemiology, including the use of prophylactic and therapeutic antimicrobial regimens and decreased depth and duration of myelosuppression.[10] Gram-positive organisms, including Viridans streptococci and Enterococci species, are associated with systemic infection of oral origin. In addition, gram-negative pathogens, including Pseudomonas aeruginosa, Neisseria species, and Escherichia coli, remain a concern.
Myeloablated cancer patients with chronic periodontal disease may develop acute periodontal infections, with associated systemic sequelae.[11–13]
Pulpal/periapical infections of dental origin can cause complications for the chemotherapy patient and need to be resolved before chemotherapy begins.[14,15]
Fungal Infections
Candidiasis
Candidiasis is typically caused by opportunistic overgrowth of Candida albicans, a normal inhabitant of the oral cavity in many individuals. Several variables contribute to its clinical expression, including drug- or disease-induced immunosuppression, mucosal injury, and salivary compromise. In addition, the use of antibiotics may alter the oral flora, creating a favorable environment for fungal overgrowth.[16,17][Level of evidence: IV]
The weighted mean prevalence of clinical oral fungal infection during chemotherapy or head and neck radiation therapy was found to be 31% in a retrospective multicenter study.[18][Level of evidence: III] The appearance of erythematous candidiasis is relatively nonspecific, and laboratory testing may be needed to confirm the diagnosis. It may be accompanied by a burning sensation of the affected tissues.[16]
Although topical agents may be helpful for superficial oral candidiasis, systemic agents are used for persistent fungal infections and in patients with significant immunosuppression. Systemic fluconazole is highly effective for prophylaxis and treatment of oral fungal infections in the oncology population.[19][Level of evidence: II];[20][Level of evidence: III]
Noncandidal fungal infections
Although most oral fungal infections involve Candida, there are occasional case reports of other oral fungal infections in immunosuppressed populations, including cancer patients. For example, a few cases of oral mucormycosis have been reported in patients with hematologic malignancies who receive a bone marrow transplant.[21] Such noncandidal oral fungal infections carry a high risk of fungemia and mortality in immunocompromised patients; systemic antifungal therapy must be promptly initiated.
Viral Infections
Herpes virus
Herpes group viral infections, including those caused by oral lesions, can cause a variety of diseases that range from mild to serious in patients undergoing treatment for cancer. The severity and impact of these lesions and systemic sequelae are directly related to the patient’s extent of immunocompromise. Comorbid oral conditions such as mucositis or graft-versus-host disease can dramatically increase the severity of oral lesions and significantly increase the difficulty of diagnosis.
A systematic review was conducted by the Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology.[22] Eighteen of 41 studies focused on outcome measures in preventing oral viral infection. This review reported findings to confirm the use of acyclovir and valacyclovir in preventing and treating oral herpetic infections.
Early diagnosis and prompt therapy remain hallmarks of management. As with other infections, the risk of systemic dissemination and morbidity/mortality increases with the degree and duration of immunocompromise. The infections can be fatal, depending on the degree of immunosuppression.
Herpes simplex virus (HSV)
Oral herpetic lesions can range from routine herpes labialis to severe stomatitis causing large, painful ulcerations throughout the mouth. Lesion severity increases with higher degrees of immunosuppression.
The introduction of valacyclovir appears to have reduced the incidence of breakthrough oral HSV infections. Topical therapy alone is generally not efficacious in patients who are immunocompromised.
In patients who are not receiving antiviral prophylaxis, oral lesions typically emerge concurrent with chemotherapy or chemoradiation therapy during the period of most significant immunosuppression (white blood cell nadir). Typically, in patients receiving a hematopoietic stem cell transplant, this represents the period a few days pretransplant through day 35 posttransplant. The risk of HSV reactivation remains higher than normal until immune reconstitution occurs. Similar patterns of risk are noted in patients receiving high-dose (immunosuppressive) chemotherapy.
Recurrent oral HSV infections occurring simultaneously with cancer therapy–induced oral mucositis can result in the development of extensive, confluent mucosal ulcerations clinically similar to primary herpetic stomatitis. Thus, HSV stomatitis can be confused with cancer therapy–induced ulcerative mucositis. Viral cultures from lesions in HSV-seropositive patients are essential for accurate diagnoses. Assays that produce more rapid results, including direct immunofluorescence, shell vial testing, and specific immunoassays for HSV antigen and/or biopsy, may also be useful.
Varicella-zoster virus (VZV)
VZV infection classically distributes via dermatomes, although the clinical manifestations can be altered in immunocompromised patients, and multiple dermatomes or more widespread distribution of lesions can be seen. In patients who are receiving high-dose chemotherapy, orofacial VZV lesions are typically observed several weeks after cessation of chemotherapy—unlike HSV, which often occurs within 2 to 3 weeks after chemotherapy is discontinued.
Cytomegalovirus
Oral lesions associated with cytomegalovirus have been documented in immunocompromised patients, including those who have undergone a bone marrow transplant.[23][Level of evidence: IV]
Appearance is not pathognomonic and is characterized by multiple mild to moderate ulcerations with irregular margins. The lesions initially present during early periods of marrow regeneration (e.g., 3 weeks after chemotherapy is discontinued) and are characterized by nonspecific pseudomembranous fibrin exudate–covered ulcerations with a granulomatous-appearing base. Surface swab cultures may yield false-negative results, perhaps because of viral propensity for infecting endothelial cells and fibroblasts, resulting in low levels of free virus.
Epstein-Barr virus (EBV)
EBV is linked to tumor development. In addition, oral hairy leukoplakia has been attributed to EBV infection in immunocompromised patients, as seen in HIV-infected patients and solid organ transplant patients. However, the lesion does not appear to be clinically significant in chemotherapy recipients.
Non–herpes group virus infections
Infections caused by non–herpes group viruses are more common in immunocompromised patients, with the risk of infection apparently increasing with the depth and duration of immunosuppression. Oral lesions caused by adenovirus and oral human papillomavirus (HPV) have been described.[23][Level of evidence: IV] Often, patients with increased cutaneous HPV lesions will develop oral lesions. These lesions can present as hyperkeratotic verrucoid lesions or as flat acuminata-like lesions.
Restoration of immune function often results in a digression and, possibly, the disappearance of the oral mucosal lesions. Laser surgery or cryotherapy are typically used to remove oral HPV lesions when medically or cosmetically required. Intralesional injections of interferon-alpha may prove effective for recurrent lesions. Infection with coxsackie viruses can occur but is generally uncommon. Although adenovirus infections are often implicated as a potential cause of oral lesions, their true incidence is not known.[23][Level of evidence: IV]
References
Pedersen AML, Sørensen CE, Proctor GB, et al.: Salivary secretion in health and disease. J Oral Rehabil 45 (9): 730-746, 2018. [PUBMED Abstract]
Spijkervet FKL, Schuurhuis JM, Stokman MA, et al.: Should oral foci of infection be removed before the onset of radiotherapy or chemotherapy? Oral Dis 27 (1): 7-13, 2021. [PUBMED Abstract]
de Oliveira MCQ, Lebre Martins BNF, Santos-Silva AR, et al.: Dental treatment needs in hospitalized cancer patients: a retrospective cohort study. Support Care Cancer 28 (7): 3451-3457, 2020. [PUBMED Abstract]
Hong BY, Sobue T, Choquette L, et al.: Chemotherapy-induced oral mucositis is associated with detrimental bacterial dysbiosis. Microbiome 7 (1): 66, 2019. [PUBMED Abstract]
Ullmann AJ, Schmidt-Hieber M, Bertz H, et al.: Infectious diseases in allogeneic haematopoietic stem cell transplantation: prevention and prophylaxis strategy guidelines 2016. Ann Hematol 95 (9): 1435-55, 2016. [PUBMED Abstract]
Villa A, Akintoye SO: Dental Management of Patients Who Have Undergone Oral Cancer Therapy. Dent Clin North Am 62 (1): 131-142, 2018. [PUBMED Abstract]
Hong CHL, Hu S, Haverman T, et al.: A systematic review of dental disease management in cancer patients. Support Care Cancer 26 (1): 155-174, 2018. [PUBMED Abstract]
Kishimoto M, Akashi M, Tsuji K, et al.: Intensity and duration of neutropenia relates to the development of oral mucositis but not odontogenic infection during chemotherapy for hematological malignancy. PLoS One 12 (7): e0182021, 2017. [PUBMED Abstract]
Mauramo M, Grolimund P, Egli A, et al.: Dissociations of oral foci of infections with infectious complications and survival after haematopoietic stem cell transplantation. PLoS One 14 (12): e0225099, 2019. [PUBMED Abstract]
Castagnola E, Mikulska M, Viscoli C: Prophylaxis and Empirical Therapy of Infection in Cancer Patients. In: Bennett JE, Dolin R, Blaser MJ, eds.: Principles and Practice of Infectious Diseases. 8th ed.: Elsevier, Inc., 2015, Elsevier, Inc., 2015, pp 3395-413. Available online. Last accessed October 10, 2023.
Ohbayashi Y, Imataki O, Uemura M, et al.: Oral microorganisms and bloodstream infection in allogeneic hematopoietic stem cell transplantation. Clin Oral Investig 25 (7): 4359-4367, 2021. [PUBMED Abstract]
Zecha JAEM, Raber-Durlacher JE, Laheij AMGA, et al.: The impact of the oral cavity in febrile neutropenia and infectious complications in patients treated with myelosuppressive chemotherapy. Support Care Cancer 27 (10): 3667-3679, 2019. [PUBMED Abstract]
Decker AM, Taichman LS, D’Silva NJ, et al.: Periodontal Treatment in Cancer Patients: An Interdisciplinary Approach. Curr Oral Health Rep 5 (1): 7-12, 2018. [PUBMED Abstract]
Bogusławska-Kapała A, Hałaburda K, Rusyan E, et al.: Oral health of adult patients undergoing hematopoietic cell transplantation. Pre-transplant assessment and care. Ann Hematol 96 (7): 1135-1145, 2017. [PUBMED Abstract]
Bollero P, Passarelli PC, D’Addona A, et al.: Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur Rev Med Pharmacol Sci 22 (4): 876-887, 2018. [PUBMED Abstract]
Hellstein JW, Marek CL: Candidiasis: Red and White Manifestations in the Oral Cavity. Head Neck Pathol 13 (1): 25-32, 2019. [PUBMED Abstract]
Lewis MAO, Williams DW: Diagnosis and management of oral candidosis. Br Dent J 223 (9): 675-681, 2017. [PUBMED Abstract]
Nishii M, Soutome S, Kawakita A, et al.: Factors associated with severe oral mucositis and candidiasis in patients undergoing radiotherapy for oral and oropharyngeal carcinomas: a retrospective multicenter study of 326 patients. Support Care Cancer 28 (3): 1069-1075, 2020. [PUBMED Abstract]
Singh GK, Capoor MR, Nair D, et al.: Spectrum of fungal infection in head and neck cancer patients on chemoradiotherapy. J Egypt Natl Canc Inst 29 (1): 33-37, 2017. [PUBMED Abstract]
Kawashita Y, Funahara M, Yoshimatsu M, et al.: A retrospective study of factors associated with the development of oral candidiasis in patients receiving radiotherapy for head and neck cancer: Is topical steroid therapy a risk factor for oral candidiasis? Medicine (Baltimore) 97 (44): e13073, 2018. [PUBMED Abstract]
Cheong HS, Kim SY, Ki HK, et al.: Oral mucormycosis in patients with haematologic malignancies in a bone marrow transplant unit. Mycoses 60 (12): 836-841, 2017. [PUBMED Abstract]
Elad S, Zadik Y, Hewson I, et al.: A systematic review of viral infections associated with oral involvement in cancer patients: a spotlight on Herpesviridea. Support Care Cancer 18 (8): 993-1006, 2010. [PUBMED Abstract]
Schubert MM, Correa MEP, Peterson DE: Oral complications of hematopoietic cell transplantation. In: Forman SJ, Negrin RS, Antin JH, et al., eds.: Thomas’ Hematopoietic Cell Transplantation: Stem Cell Transplantation. 5th ed. John Wiley & Sons, Ltd, 2016, pp 1242-56.
Hemorrhage
Hemorrhage is a concern for patients who are receiving high-dose chemotherapy or undergoing hematopoietic stem cell transplant. It may occur during treatment-induced thrombocytopenia and/or coagulopathy.[1] Spontaneous gingival oozing may occur when platelet counts drop below 20,000/µL, especially when there is preexisting gingivitis or periodontitis. Even normal function or routine oral hygiene (brushing and flossing) can induce gingival oozing with preexisting gingivitis and periodontitis, compounded by hematologic change and biochemical changes in coagulation. Management requires attention by a multidisciplinary team to local measures, platelet count and function, and coagulation.
Although rarely serious, oral bleeds can be of concern to the patient and family. Oral bleeding may be mild (e.g., petechiae located on the lips, soft palate, or floor of the mouth) or severe (e.g., persistent gingival hemorrhage or bleeding from herpes simplex virus ulcers in the face of severe thrombocytopenia).
Healthy gingival tissues do not bleed unless traumatized. Discontinuation of routine oral hygiene can increase the risk of gingival infection, which may promote bleeding and increase the risk of local and systemic infection due to accumulation of bacterial plaque. This may lead to periodontal infections and tissue breakdown.
The degree of health professional oversight of thrombocytopenic patients is an important consideration relative to risk of mechanical hygiene procedures. With comprehensive monitoring, patients can often safely use dental brushing and interdental cleaning throughout the thrombocytopenic episode.
Local measures to manage oral bleeds include the following:
Pressure application. Pressure can be applied by gauze or custom-made oral appliances; these can also be used to deliver and maintain topical agents at the site of bleeding.
Locally applied clot-forming agents. Topical thrombin and/or hemostatic collagen agents and tranexamic acid can be used to stabilize clots.
Vasoconstrictors. Epinephrine can be used topically to reduce blood flow rates through bleeding vessels, although vessel rebound is a potential concern.
Tissue protectants. Application of mucosal adherent products (including cyanoacrylate products) help seal bleeding sites and protect organized clots; platelet-rich plasma may be used.
Patients who tend to form friable and easily dislodged clots will benefit from topical application of aminocaproic acid. In some instances, intravenous administration can be considered to improve coagulation and the formation of stable clots.
Application of 3% hydrogen peroxide and 0.9% saline (1:2 to 1:3 by volume) can aid in wound cleansing and removal of superficial blood debris. Care must be taken not to disturb clots, which might promote bleeding.[1] Laser application for local coagulation may be considered.
References
Schubert MM, Correa MEP, Peterson DE: Oral complications of hematopoietic cell transplantation. In: Forman SJ, Negrin RS, Antin JH, et al., eds.: Thomas’ Hematopoietic Cell Transplantation: Stem Cell Transplantation. 5th ed. John Wiley & Sons, Ltd, 2016, pp 1242-56.
Relapse and Second Malignancy
Gingival infiltrates, oral infection, and/or bleeding disproportionate to local etiology can indicate a possible relapse, especially in patients treated for leukemias or lymphomas.
Relapse of non–head and neck solid tumors occurring as oral metastases is rarely observed. Second head and neck tumors are expected to occur in up to 15% of head and neck cancer patients in a stable incidence over the years, and human papillomavirus status may influence this outcome.[1] Locoregional recurrences usually occur in the first 2 years after treatment. The same follow-up protocol is indicated in cases of a second malignant event.[2]
References
Adjei Boakye E, Buchanan P, Hinyard L, et al.: Risk and outcomes for second primary human papillomavirus-related and -unrelated head and neck malignancy. Laryngoscope 129 (8): 1828-1835, 2019. [PUBMED Abstract]
Brands MT, Smeekens EAJ, Takes RP, et al.: Time patterns of recurrence and second primary tumors in a large cohort of patients treated for oral cavity cancer. Cancer Med 8 (12): 5810-5819, 2019. [PUBMED Abstract]
Taste Disorder
Dysgeusia, taste disorder, can be a prominent symptom in patients who are receiving chemotherapy or head/neck radiation.[1] Etiology is likely associated with several factors, including direct neurotoxicity to taste buds, xerostomia, infection, and psychologic conditioning. Also, cancer treatments may impair taste bud cell regeneration, leading to a diminished function.[2] In addition, taste dysfunction can be associated with damage caused by graft-versus-host disease to the taste perception units. For more information, see the GVHD section.
Patients receiving chemotherapy may experience unpleasant taste secondary to diffusion of drug into the oral cavity. In addition, patients often describe dysgeusia in the early weeks after cessation of cytotoxic therapy that has a negative impact on quality of life. Taste disturbances during chemotherapy are influenced by nausea and reduced appetite, so they can impact nutrition. This symptom is generally reversible, and taste sensation returns to normal in the ensuing months. For more information, see Nutrition in Cancer Care.
By comparison, a total fractionated radiation dose higher than 3,000 Gy reduces acuity of sweet, sour, bitter, and salt tastes. Damage to the microvilli and outer surface of taste cells has been proposed as the principal mechanism for loss of the sense of taste. Even patients with non-oral head and neck cancer frequently show disturbed taste when they are treated with mouth-sparing radiation therapy.[3]
References
Hovan AJ, Williams PM, Stevenson-Moore P, et al.: A systematic review of dysgeusia induced by cancer therapies. Support Care Cancer 18 (8): 1081-7, 2010. [PUBMED Abstract]
Epstein JB, Smutzer G, Doty RL: Understanding the impact of taste changes in oncology care. Support Care Cancer 24 (4): 1917-31, 2016. [PUBMED Abstract]
Barbosa da Silva JL, Doty RL, Miyazaki JVMK, et al.: Gustatory disturbances occur in patients with head and neck cancer who undergo radiotherapy not directed to the oral cavity. Oral Oncol 95: 115-119, 2019. [PUBMED Abstract]
Medication-Related Osteonecrosis of the Jaw
Overview
Bisphosphonates are potent inhibitors of osteoclasts. They are used in cancer patients with skeletal metastases, including breast, prostate, or lung cancer, and in patients with multiple myeloma. Bisphosphonates are also used to treat hypercalcemia of malignancy and to prevent osteoporosis in patients with cancer.[1,2] For more information on bisphosphonates, see the Bisphosphonates and denosumab section in Cancer Pain.
Clinical trials reveal that antiangiogenic drugs can be associated with the development of medication-related osteonecrosis of the jaw (MRONJ) when used as a single drug or in combination with bone-modifying agents (BMAs). When antiangiogenics are used with bisphosphonates, the risk of MRONJ increases significantly.[3–6]
Osteonecrosis of the jaw is no longer a problem exclusively associated with the use of bisphosphonates; it is also associated with the use of other drugs such as the monoclonal antibody denosumab and antiangiogenics such as bevacizumab and sorafenib. For this reason, the term MRONJ, rather than the term bisphosphonate-related osteonecrosis of the jaw, should be used to refer to bone necrosis associated with pharmacological therapies.[7,8]
Table 13. Cancer Drugs and Biologics Associated With Medication-Related Osteonecrosis of the Jaw
Generic Drug (Trade Name)
Indication
Class of Drug
Mode of Action
Reported to Cause MRONJ?
GIST = gastrointestinal stromal tumor; MRONJ = medication-related osteonecrosis of the jaw; RANKL = receptor activator of nuclear factor kappa beta ligand; VEGF = vascular endothelial growth factor.
Zoledronic acid
Bone metastasis; bone loss from cancer therapy)
Bisphosphonate
Inhibition of osteoclasts
Yes
Pamidronate
Bone loss from cancer therapy
Bisphosphonate
Inhibition of osteoclasts
Yes
Alendronate
Bone loss from cancer therapy
Bisphosphonate
Inhibition of osteoclasts
Yes
Denosumab
Bone metastasis; osteoporosis; bone loss from cancer therapy
Humanized monoclonal antibody
Suppression of bone remodeling by inhibition of RANKL
Inhibition of angiogenesis by blocking the action of VEGF
Yes
Sunitinib
Advanced renal cell carcinoma; GIST
Antiangiogenic
Inhibition of angiogenesis by blocking VEGF tyrosine kinase
Yes
Sorafenib
Renal cell carcinoma; hepatocellular carcinoma
Antiangiogenic
Inhibition of angiogenesis by blocking VEGF tyrosine kinase
Yes, when combined with bone-modifying agent
Incidence
The occurrence of MRONJ ranges between 1% and 8% in patients treated with a BMA for bone metastases or multiple myeloma, and between 0 and 1.8% in cancer patients treated with adjuvant BMA for osteoporosis prevention.[8] The prevalence of MRONJ varies according to study design, diagnostic criteria, type of BMA, and dosage. MRONJ lesions are also more prevalent in areas with thin mucosa overlying bone prominences, such as tori, exostoses, and the mylohyoid ridge.[9]
Diagnosis
A diagnosis of MRONJ is based on the following factors:[6,9]
Exposed bone or bone that can be probed through an intraoral or extra oral fistula(e) in the maxillofacial region and that does not heal within 8 weeks.
Patient has received a BMA or angiogenic inhibitor agent.
Patient has no history of head and neck radiation.
It is also possible that symptoms of dental disease, periodontal disease, or both may be present, without visible exposed bone.[6]
Table 14. Bone-Modifying Agents and Risk of Medication-Related Osteonecrosis of the Jawa
Drug
Indication
Route
Dose (mg)
Schedule
Frequency of MRONJ, %b
IV = intravenous; MRONJ = medication-related osteonecrosis of the jaw; SC = subcutaneous.
cThe estimate of 6.9% is from the open-label extension phase of two phase III studies.[7] It is not adjusted for patient-years of exposure or patient follow-up and does not include cases that occurred during the blinded treatment phase. The patient-year adjusted incidence of confirmed MRONJ was 1.1% during the first year of denosumab treatment, 3.7% in the second year, and 4.6% per year thereafter.
A well-established staging system should be used to quantify the severity and extent of MRONJ and to guide management decisions. The same system should be used throughout the patient’s MRONJ course of case. Diagnostic imaging may be used as an adjunct to these staging systems. Optimally, staging should be performed by a clinician who is experienced with the management of MRONJ.[8]
The following two staging systems represent the most frequently used scales, as reported in the literature:
American Association of Oral and Maxillofacial Surgeons (AAOMS) system.[6]
Osteonecrosis of the jaw severity scale (Common Terminology Criteria for Adverse Events).[20]
In 2009, AAOMS added a stage 0, which refers to any symptoms of bone pain, fistulous track formation, abscess formation, and altered sensory function. It also includes abnormal radiographic findings that, in the absence of a fistula to bone or frank bone exposure, extend beyond the confines of the alveolar bone as a definitive precursor to MRONJ in patients receiving BMA therapy. The risk of a patient’s stage 0 disease progressing to a higher disease stage remains unclear, although case studies suggest that such progression may occur in up to 50% of patients.[21]
The International Task Force of Osteonecrosis of the Jaw expressed concern that the use of stage 0 terminology may lead to overdiagnosis of MRONJ because initial presenting symptoms may ultimately lead to an alternative diagnosis.[22,23] The Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology/American Society of Clinical Oncology Expert Panel shares these concerns and suggests considering stage 0 as an indicator of increased risk of MRONJ. Identifying the increased risk status could prompt a referral to a dental specialist for close follow-up with assessment for early-stage MRONJ, should it develop, to optimize oral health.
Table 15. Staging and Treatment Strategies for Medication-Related Osteonecrosis of the Jawa
MRONJ Staging
Clinical and Radiographic Presentations
Treatment Strategies
IV = intravenous; MRONJ = medication-related osteonecrosis of the jaw.
aAdapted from Yarom et al.[8] and Ruggiero et al.[6]
At-risk category
No apparent necrotic bone in patients who have been treated with either oral or IV bisphosphonates
No treatment indicated; patient education and reduction of modifiable risk factors
Increased risk
No clinical evidence of necrotic bone, but nonspecific clinical findings and symptoms
Systemic management, including use of pain medication and close scrutiny and follow-up; refer to dental specialist and follow up every 8 wk with communication of lesion status to oncologist; patient education and reduction of modifiable risk factors
Stage 1
Exposed and necrotic bone in patients who are asymptomatic and have no evidence of infection
Antibacterial mouth rinse; clinical follow-up every 3 mo; patient education; review of indications for continued bisphosphonate therapy
Stage 2
Exposed and necrotic bone associated with infection, as evidenced by pain and erythema in the region of the exposed bone, with or without purulent drainage
Symptomatic treatment with oral antibiotics; oral antibacterial mouth rinse; pain control; superficial debridement to relieve irritation of soft tissue
Stage 3
Exposed and necrotic bone in patients with pain, infection, and one or more of the following: exposed and necrotic bone extending beyond the region of alveolar bone (i.e., inferior border and ramus in the mandible, maxillary sinus, and zygoma in the maxilla), resulting in pathological fracture, extraoral fistula, oral antral/oral nasal communication, or osteolysis extending to the inferior border of the mandible of sinus floor
Antibacterial mouth rinse; antibiotic therapy and pain control; surgical debridement/resection for longer-term palliation of infection and pain
Management of MRONJ measures
Aggressive surgical interventions (e.g., mucosal flap elevation, block resection of necrotic bone, soft tissue closer) may be used if MRONJ results in persistent symptoms or impacts function despite initial conservative treatment. Aggressive surgical intervention is not recommended for asymptomatic bone exposure. In advance of the aggressive surgical intervention, the multidisciplinary care team and the patient should thoroughly discuss the risks and benefits of the proposed intervention.[24]
Table 16. Proposed Terms to Characterize Osteonecrosis of the Jaw After Treatmenta
Significant improvement (>50% of mucosal coverage)
Significant improvement (>50% reduction of pain, VAS)
Significant improvement (no signs of infection/inflammation)
Improved trabecular pattern, signs of sequestra
Stable
Mild improvement (<50% of mucosal coverage)
Mild improvement (<50% reduction of pain, VAS)
Mild improvement (mild signs of infection/inflammation)
No changes
Progressive
No improvement or worsening
No improvement or worsening
No improvement
Lytic changes, decreasing trabeculation, increased size of radiographic lesion
Reducing Risk of Development of MRONJ
For cancer patients scheduled to receive a BMA in a nonurgent setting, oral care assessment (including a comprehensive dental, periodontal, and oral radiographic exam, when feasible to do so) is undertaken before therapy is initiated. After the assessment, the dentist and oncologist will develop and implement a dental care plan and coordinate with each other to ensure that medically necessary dental procedures are undertaken before a BMA is initiated. The dentist will follow up on a routine schedule once therapy with a BMA has started.
Table 17. Complete, Partial, and Minimal Dental Evaluation Protocols, Based on Dental and/or Periodontal Pathologya
bAdapted from Haytac et al.[26] and Melkos et al.[27]
cAdapted from Schuuhuis et al.[28] and Tsuji et al.[29]
dAdapted from Haytac et al.,[26] Melkos et al.,[27] Schuuhuis et al.,[28], Tsuji et al.[29], and Gurgan et al.[30]
Caries
Restore all teeth
Restore mild/moderate caries if time permits
Intervene only if symptomatic
Severe caries/pulp involvement/dental abscess
Perform root canal treatment or extraction
Apical periodontitis
Retreat
Treat symptomatic lesions and lesions >5 mm
Perform apicoectomy
Observe asymptomatic lesions and lesions <5 mm
Extract teeth
Advanced periodontal disease
Extract teeth with:
Extract teeth with:
– Probing depth >6 mm
– Probing depth >8 mm
– Furcation I, II, III; Mobility III
– Mobility III
– Severe inflammation
– Severe inflammation
Partially erupted third molars
Extract partially erupted third molars
Observe asymptomatic teeth
Extract partially erupted third molars with purulence of pericoronitis
Members of the multidisciplinary team should address modifiable risk factors for MRONJ with the patient as early as possible. These risk factors include:
Elective dentoalveolar surgical procedures (e.g., medically unnecessary extractions, alveoplasties, and implants) should not be performed during active therapy with a BMA at an oncologic dose. Exceptions may be considered when a dental specialist with expertise in prevention and treatment of MRONJ has reviewed the benefits and risks of the proposed invasive procedure with the patient and the oncology team.[8]
If dentoalveolar surgery is performed, the dental specialist must evaluate patients frequently until full mucosal coverage of the surgical site has occurred. Communication with the oncologist regarding the status of healing is encouraged, particularly when considering future use of BMA.[8]
For patients with cancer who are receiving a BMA at an oncologic dose, there is insufficient evidence to support or refute discontinuation of the BMA before dentoalveolar surgery. Administration of the BMA may be deferred at the discretion of the treating physician, in consultation with the patient and oral health-provider.[8,39]
Table 18. Daily Oral Care Plan for Patients (Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology)a
Floss at least once/d; waxed floss may be easier to use and minimize trauma to the gingivae.
If flossing causes bleeding of the gums that does not stop after 2 minutes, consult oncology team.
Brushing
Use a small, ultra-soft-headed, round-end, bristle toothbrush (an ultrasonic toothbrush may be acceptable).
Rinse toothbrush in hot water to soften brush before using.
Use prescription-strength fluoride toothpaste; spit out the foam but do not rinse the mouth.
Use remineralizing pastes and chewing gum containing calcium and phosphate.
Brush within 30 min after eating and before bed; include the gingival portion of the tooth and periodontal sulcus.
Brush tongue gently from back to front.
Rinse brush after use in hot water and allow to air dry.
Change toothbrush when bristles are not standing up straight.
For patients with dentures
Remove dentures before brushing.
Brush and rinse dentures after meals and at bedtime.
Remove from mouth for long periods (at least 8 hours per 24 hours) and soak in rinsing solution.
Rinsing
Rinse the oral cavity vigorously to help maintain moisture in the mouth, remove remaining debris, and reduce accumulation of plaque and infection.
Rinse, swish, and spit with a bland rinse (1 tsp salt and 1 tsp baking soda in 4 c water) several times a day.
Avoid club soda because of the presence of carbonic acids.
Commercial mouthwashes with alcohol base or astringent properties are not recommended for patients with oral complications.
Debride only if absolutely necessary and if loose tissue causes gagging or choking.
Moisturizing the oral cavity
Moisturize the mouth with water, artificial saliva products, or other water-soluble lubricants for use inside the mouth.
Avoid glycerin or lemon-glycerin swabs, as they dry the mouth and do not moisturize.
Apply lubricant after each cleaning, at bedtime, and as needed. Apply water-based lubricant more frequently.
Rinse often with basic mouth rinse.
Lip care
To keep lips lubricated and moisturized, use only animal- or plant-based oils such as beeswax, cocoa butter, and lanolin. Avoid petroleum-based products, as these cause drying and cracking.
Visit the dentist at least every 6 mo.
Notify dentist or oncologist of any oral signs or symptoms.
References
Shapiro CL, Van Poznak C, Lacchetti C, et al.: Management of Osteoporosis in Survivors of Adult Cancers With Nonmetastatic Disease: ASCO Clinical Practice Guideline. J Clin Oncol 37 (31): 2916-2946, 2019. [PUBMED Abstract]
Migliorati CA, Casiglia J, Epstein J, et al.: Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc 136 (12): 1658-68, 2005. [PUBMED Abstract]
Smidt-Hansen T, Folkmar TB, Fode K, et al.: Combination of zoledronic Acid and targeted therapy is active but may induce osteonecrosis of the jaw in patients with metastatic renal cell carcinoma. J Oral Maxillofac Surg 71 (9): 1532-40, 2013. [PUBMED Abstract]
Nicolatou-Galitis O, Kouri M, Papadopoulou E, et al.: Osteonecrosis of the jaw related to non-antiresorptive medications: a systematic review. Support Care Cancer 27 (2): 383-394, 2019. [PUBMED Abstract]
Otto S, Pautke C, Van den Wyngaert T, et al.: Medication-related osteonecrosis of the jaw: Prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treat Rev 69: 177-187, 2018. [PUBMED Abstract]
Ruggiero SL, Dodson TB, Fantasia J, et al.: American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw–2014 update. J Oral Maxillofac Surg 72 (10): 1938-56, 2014. [PUBMED Abstract]
Stopeck AT, Fizazi K, Body JJ, et al.: Safety of long-term denosumab therapy: results from the open label extension phase of two phase 3 studies in patients with metastatic breast and prostate cancer. Support Care Cancer 24 (1): 447-455, 2016. [PUBMED Abstract]
Yarom N, Shapiro CL, Peterson DE, et al.: Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J Clin Oncol 37 (25): 2270-2290, 2019. [PUBMED Abstract]
Khan A, Morrison A, Cheung A, et al.: Osteonecrosis of the jaw (ONJ): diagnosis and management in 2015. Osteoporos Int 27 (3): 853-859, 2016. [PUBMED Abstract]
Gimsing P, Carlson K, Turesson I, et al.: Effect of pamidronate 30 mg versus 90 mg on physical function in patients with newly diagnosed multiple myeloma (Nordic Myeloma Study Group): a double-blind, randomised controlled trial. Lancet Oncol 11 (10): 973-82, 2010. [PUBMED Abstract]
Jadu F, Lee L, Pharoah M, et al.: A retrospective study assessing the incidence, risk factors and comorbidities of pamidronate-related necrosis of the jaws in multiple myeloma patients. Ann Oncol 18 (12): 2015-9, 2007. [PUBMED Abstract]
Himelstein AL, Foster JC, Khatcheressian JL, et al.: Effect of Longer-Interval vs Standard Dosing of Zoledronic Acid on Skeletal Events in Patients With Bone Metastases: A Randomized Clinical Trial. JAMA 317 (1): 48-58, 2017. [PUBMED Abstract]
Vahtsevanos K, Kyrgidis A, Verrou E, et al.: Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J Clin Oncol 27 (32): 5356-62, 2009. [PUBMED Abstract]
Coleman RE, Collinson M, Gregory W, et al.: Benefits and risks of adjuvant treatment with zoledronic acid in stage II/III breast cancer. 10 years follow-up of the AZURE randomized clinical trial (BIG 01/04). J Bone Oncol 13: 123-135, 2018. [PUBMED Abstract]
Hershman DL, McMahon DJ, Crew KD, et al.: Zoledronic acid prevents bone loss in premenopausal women undergoing adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol 26 (29): 4739-45, 2008. [PUBMED Abstract]
Shapiro CL, Halabi S, Hars V, et al.: Zoledronic acid preserves bone mineral density in premenopausal women who develop ovarian failure due to adjuvant chemotherapy: final results from CALGB trial 79809. Eur J Cancer 47 (5): 683-9, 2011. [PUBMED Abstract]
Qi WX, Tang LN, He AN, et al.: Risk of osteonecrosis of the jaw in cancer patients receiving denosumab: a meta-analysis of seven randomized controlled trials. Int J Clin Oncol 19 (2): 403-10, 2014. [PUBMED Abstract]
Scagliotti GV, Hirsh V, Siena S, et al.: Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: subgroup analysis from a randomized phase 3 study. J Thorac Oncol 7 (12): 1823-1829, 2012. [PUBMED Abstract]
Gnant M, Pfeiler G, Dubsky PC, et al.: Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 386 (9992): 433-43, 2015. [PUBMED Abstract]
National Cancer Institute: Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Bethesda, Md: U.S. Department of Health and Human Services, National Institutes of Health, 2017. Available online. Last accessed Dec. 18, 2024.
Schiodt M, Reibel J, Oturai P, et al.: Comparison of nonexposed and exposed bisphosphonate-induced osteonecrosis of the jaws: a retrospective analysis from the Copenhagen cohort and a proposal for an updated classification system. Oral Surg Oral Med Oral Pathol Oral Radiol 117 (2): 204-13, 2014. [PUBMED Abstract]
Khan AA, Morrison A, Hanley DA, et al.: Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res 30 (1): 3-23, 2015. [PUBMED Abstract]
Khan AA, Morrison A, Kendler DL, et al.: Case-Based Review of Osteonecrosis of the Jaw (ONJ) and Application of the International Recommendations for Management From the International Task Force on ONJ. J Clin Densitom 20 (1): 8-24, 2017 Jan – Mar. [PUBMED Abstract]
El-Rabbany M, Sgro A, Lam DK, et al.: Effectiveness of treatments for medication-related osteonecrosis of the jaw: A systematic review and meta-analysis. J Am Dent Assoc 148 (8): 584-594.e2, 2017. [PUBMED Abstract]
Hong CHL, Hu S, Haverman T, et al.: A systematic review of dental disease management in cancer patients. Support Care Cancer 26 (1): 155-174, 2018. [PUBMED Abstract]
Haytac MC, Dogan MC, Antmen B: The results of a preventive dental program for pediatric patients with hematologic malignancies. Oral Health Prev Dent 2 (1): 59-65, 2004. [PUBMED Abstract]
Melkos AB, Massenkeil G, Arnold R, et al.: Dental treatment prior to stem cell transplantation and its influence on the posttransplantation outcome. Clin Oral Investig 7 (2): 113-5, 2003. [PUBMED Abstract]
Schuurhuis JM, Span LF, Stokman MA, et al.: Effect of leaving chronic oral foci untreated on infectious complications during intensive chemotherapy. Br J Cancer 114 (9): 972-8, 2016. [PUBMED Abstract]
Tsuji K, Shibuya Y, Akashi M, et al.: Prospective study of dental intervention for hematopoietic malignancy. J Dent Res 94 (2): 289-96, 2015. [PUBMED Abstract]
Gürgan CA, Özcan M, Karakuş Ö, et al.: Periodontal status and post-transplantation complications following intensive periodontal treatment in patients underwent allogenic hematopoietic stem cell transplantation conditioned with myeloablative regimen. Int J Dent Hyg 11 (2): 84-90, 2013. [PUBMED Abstract]
Barasch A, Cunha-Cruz J, Curro F, et al.: Dental risk factors for osteonecrosis of the jaws: a CONDOR case-control study. Clin Oral Investig 17 (8): 1839-45, 2013. [PUBMED Abstract]
Kato GF, Lopes RN, Jaguar GC, et al.: Evaluation of socket healing in patients undergoing bisphosphonate therapy: experience of a single Institution. Med Oral Patol Oral Cir Bucal 18 (4): e650-6, 2013. [PUBMED Abstract]
Schiodt M, Vadhan-Raj S, Chambers MS, et al.: A multicenter case registry study on medication-related osteonecrosis of the jaw in patients with advanced cancer. Support Care Cancer 26 (6): 1905-1915, 2018. [PUBMED Abstract]
Vidal-Real C, Pérez-Sayáns M, Suárez-Peñaranda JM, et al.: Osteonecrosis of the jaws in 194 patients who have undergone intravenous bisphosphonate therapy in Spain. Med Oral Patol Oral Cir Bucal 20 (3): e267-72, 2015. [PUBMED Abstract]
Tsao C, Darby I, Ebeling PR, et al.: Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J Oral Maxillofac Surg 71 (8): 1360-6, 2013. [PUBMED Abstract]
Smith MR, Saad F, Coleman R, et al.: Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial. Lancet 379 (9810): 39-46, 2012. [PUBMED Abstract]
Gabbert TI, Hoffmeister B, Felsenberg D: Risk factors influencing the duration of treatment with bisphosphonates until occurrence of an osteonecrosis of the jaw in 963 cancer patients. J Cancer Res Clin Oncol 141 (4): 749-58, 2015. [PUBMED Abstract]
Rabelo GD, Assunção JN, Chavassieux P, et al.: Bisphosphonate-Related Osteonecrosis of the Jaws and Its Array of Manifestations. J Maxillofac Oral Surg 14 (3): 699-705, 2015. [PUBMED Abstract]
Fusco V, Galassi C, Berruti A, et al.: Decreasing frequency of osteonecrosis of the jaw in cancer and myeloma patients treated with bisphosphonates: the experience of the oncology network of piedmont and aosta valley (north-Western Italy). ISRN Oncol 2013: 672027, 2013. [PUBMED Abstract]
Special Considerations in Pediatric Populations
There has been a marked increase in the survival rates of childhood cancers because of advances in cancer therapy. However, this progress has resulted in an increase in the number of the late effects from antineoplastic therapy observed in children.[1] Approximately 60% to 80% of childhood cancer survivors develop at least one chronic condition caused by previous cancer treatment.[1] Altered dental growth and craniofacial development is a frequent complication in childhood cancer survivors who received high-dose chemotherapy and/or head and neck radiation.[2,3] For more information, see Late Effects of Treatment for Childhood Cancer.
The severity and location of dental and craniofacial abnormalities are typically associated with the type of cancer modality used and the age at which cancer therapy began.
Dental Abnormalities
The reported incidence and types of dental abnormalities, such as hypodontia, may also alter craniofacial development and lead to malocclusion.
The following cancer modalities have been associated with higher incidence and more severe dental defects:
Head and neck radiation.[11][Level of evidence: II] For doses of 20 Gy or more, the odds ratio (OR) of developing at least one dental abnormality has been reported to be 5.6 (confidence interval [CI], 3.7–8.5) versus 1.3 (CI, 1.2–1.5) for radiation doses of 0 to 19 Gy.[4] Even though modern conformal intensity-modulated radiation therapy (IMRT) has been suggested to minimize these effects, reports have shown that IMRT still results in both dental and craniofacial developmental abnormalities.[12][Level of evidence: II];[13][Level of evidence: III]
The association between risk of dental abnormalities and age at time of cancer therapy ranges between age 3 years or younger to age 8 years.[10][Level of evidence: III][14][Level of evidence: II] However, there appear to be more reports documenting that children younger than 5 years at the time of chemotherapy are at increased risk of developing dental abnormalities. For head and neck radiation with doses 20 Gy or higher, the OR of having at least one dental abnormality was 5.6 for those aged 0 to 5 years and 9.6 for those aged 6 to 10 years.[4]
The impact of cancer therapy on dental age is unclear, with one study [15] reporting an advanced dental age and other studies reporting either no difference [16,17] or a delay in dental age.[18][Level of evidence: III];[19][Level of evidence: II]
References
Crowder SL, Douglas KG, Yanina Pepino M, et al.: Nutrition impact symptoms and associated outcomes in post-chemoradiotherapy head and neck cancer survivors: a systematic review. J Cancer Surviv 12 (4): 479-494, 2018. [PUBMED Abstract]
Effinger KE, Migliorati CA, Hudson MM, et al.: Oral and dental late effects in survivors of childhood cancer: a Children’s Oncology Group report. Support Care Cancer 22 (7): 2009-19, 2014. [PUBMED Abstract]
Gawade PL, Hudson MM, Kaste SC, et al.: A systematic review of dental late effects in survivors of childhood cancer. Pediatr Blood Cancer 61 (3): 407-16, 2014. [PUBMED Abstract]
Kaste SC, Goodman P, Leisenring W, et al.: Impact of radiation and chemotherapy on risk of dental abnormalities: a report from the Childhood Cancer Survivor Study. Cancer 115 (24): 5817-27, 2009. [PUBMED Abstract]
Hsieh SG, Hibbert S, Shaw P, et al.: Association of cyclophosphamide use with dental developmental defects and salivary gland dysfunction in recipients of childhood antineoplastic therapy. Cancer 117 (10): 2219-27, 2011. [PUBMED Abstract]
Nishimura S, Inada H, Sawa Y, et al.: Risk factors to cause tooth formation anomalies in chemotherapy of paediatric cancers. Eur J Cancer Care (Engl) 22 (3): 353-60, 2013. [PUBMED Abstract]
Maciel JC, de Castro CG, Brunetto AL, et al.: Oral health and dental anomalies in patients treated for leukemia in childhood and adolescence. Pediatr Blood Cancer 53 (3): 361-5, 2009. [PUBMED Abstract]
Kaste SC, Hopkins KP, Jones D, et al.: Dental abnormalities in children treated for acute lymphoblastic leukemia. Leukemia 11 (6): 792-6, 1997. [PUBMED Abstract]
Cubukcu CE, Sevinir B, Ercan I: Disturbed dental development of permanent teeth in children with solid tumors and lymphomas. Pediatr Blood Cancer 58 (1): 80-4, 2012. [PUBMED Abstract]
Hölttä P, Hovi L, Saarinen-Pihkala UM, et al.: Disturbed root development of permanent teeth after pediatric stem cell transplantation. Dental root development after SCT. Cancer 103 (7): 1484-93, 2005. [PUBMED Abstract]
Jaffe N, Toth BB, Hoar RE, et al.: Dental and maxillofacial abnormalities in long-term survivors of childhood cancer: effects of treatment with chemotherapy and radiation to the head and neck. Pediatrics 73 (6): 816-23, 1984. [PUBMED Abstract]
Owosho AA, Brady P, Wolden SL, et al.: Long-term effect of chemotherapy-intensity-modulated radiation therapy (chemo-IMRT) on dentofacial development in head and neck rhabdomyosarcoma patients. Pediatr Hematol Oncol 33 (6): 383-392, 2016. [PUBMED Abstract]
Paulino AC, Simon JH, Zhen W, et al.: Long-term effects in children treated with radiotherapy for head and neck rhabdomyosarcoma. Int J Radiat Oncol Biol Phys 48 (5): 1489-95, 2000. [PUBMED Abstract]
Hutton A, Bradwell M, English M, et al.: The oral health needs of children after treatment for a solid tumour or lymphoma. Int J Paediatr Dent 20 (1): 15-23, 2010. [PUBMED Abstract]
Vasconcelos NP, Caran EM, Lee ML, et al.: Dental maturity assessment in children with acute lymphoblastic leukemia after cancer therapy. Forensic Sci Int 184 (1-3): 10-4, 2009. [PUBMED Abstract]
Flores AP, Monti CF, Brunotto M: Dental and chronological age in children under oncological treatment. J Forensic Sci 60 (2): 453-6, 2015. [PUBMED Abstract]
Martin MB, Li CS, Rowland CC, et al.: Correlation of bone age, dental age, and chronological age in survivors of childhood acute lymphoblastic leukaemia. Int J Paediatr Dent 18 (3): 217-23, 2008. [PUBMED Abstract]
Bagattoni S, D’Alessandro G, Prete A, et al.: Oral health and dental late adverse effects in children in remission from malignant disease. A pilot case-control study in Italian children. Eur J Paediatr Dent 15 (1): 45-50, 2014. [PUBMED Abstract]
Purdell-Lewis DJ, Stalman MS, Leeuw JA, et al.: Long term results of chemotherapy on the developing dentition: caries risk and developmental aspects. Community Dent Oral Epidemiol 16 (2): 68-71, 1988. [PUBMED Abstract]
Special Considerations in Geriatric Populations
An aging population is living with more chronic diseases, comorbidities, multidrug use, and cancers. The special care needs of the geriatric population should be assessed and considered in the development of cancer treatment protocols.
Oncologists need to promote oral health in frail older adults when they are about to undergo a cancer therapy that could have permanent or temporary impacts on oral/dental health. Pretherapy oral/dental evaluation is mandatory, and the follow-up of an older adult with frailty involves close monitoring (face to face or telehealth) and education of caregivers regarding oral and dental hygiene.
Quality-of-life (QOL) considerations should be a fundamental component in cancer management, whatever a patient’s age. In the field of oncology, it is apparent that the geriatric cancer population has special oral/dental needs. Special precautions are advised for this patient group. Dental professionals need to be part of the geriatric oncology team for better support of QOL.
Latest Updates to This Summary (02/16/2024)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This summary was renamed from Oral Complications of Chemotherapy and Head/Neck Radiation.
This summary was comprehensively reviewed and extensively revised.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the pathophysiology and treatment of oral complications of cancer therapies. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Oral Complications of Cancer Therapies are:
Megan Reimann, PharmD, BCOP (Total CME)
Andrea Ruskin, MD (VA Connecticut Healthcare System)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Oral Complications of Cancer Therapies. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/mouth-throat/oral-complications-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389320]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Symptom Clusters in Cancer (PDQ®)–Health Professional Version
Overview
During and after treatment for cancer, patients experience an average of 10 to14 co-occurring symptoms.[1,2] Compared with patients with few or no symptoms, patients with multiple concurrent symptoms may experience worse decrements in physical and cognitive function,[3–6] quality of life,[3–6] and overall survival.[7] Symptoms that occur together over time may form a cluster.
A symptom cluster is two or more concurrent symptoms with the following properties:[1,8]
The concurrent symptoms within the cluster are stable (i.e., the same symptoms that comprise clusters are identified at different time points throughout the cancer care trajectory).
The symptoms within a cluster may share underlying mechanisms.
The symptoms within a cluster may share outcomes.
The symptom cluster may have a temporal dimension (i.e., the severity of the symptoms within the cluster may shift together over time).
Symptoms in a cluster may be related to each other in multiple ways. They may share a common set of biological, psychological, or social mechanisms, or they may cause or potentiate one another’s effects.[8] They may also be due to side effects of another treatment. The management of symptom clusters primarily involves identifying relationships among the symptoms. This approach supports strategies that may address multiple symptoms simultaneously. It also avoids unnecessary interventions that can worsen symptom burden and the patient’s quality of life. As advancements in symptom science research are achieved, better therapeutic targets will be identified for improved management of symptom clusters and outcomes.
References
Miaskowski C, Barsevick A, Berger A, et al.: Advancing Symptom Science Through Symptom Cluster Research: Expert Panel Proceedings and Recommendations. J Natl Cancer Inst 109 (4): , 2017. [PUBMED Abstract]
Harris CS, Dodd M, Kober KM, et al.: Advances in Conceptual and Methodological Issues in Symptom Cluster Research: A 20-Year Perspective. ANS Adv Nurs Sci 45 (4): 309-322, 2022 Oct-Dec 01. [PUBMED Abstract]
Dodd MJ, Cho MH, Cooper BA, et al.: Identification of latent classes in patients who are receiving biotherapy based on symptom experience and its effect on functional status and quality of life. Oncol Nurs Forum 38 (1): 33-42, 2011. [PUBMED Abstract]
Miaskowski C, Dunn L, Ritchie C, et al.: Latent Class Analysis Reveals Distinct Subgroups of Patients Based on Symptom Occurrence and Demographic and Clinical Characteristics. J Pain Symptom Manage 50 (1): 28-37, 2015. [PUBMED Abstract]
Neijenhuijs KI, Peeters CFW, van Weert H, et al.: Symptom clusters among cancer survivors: what can machine learning techniques tell us? BMC Med Res Methodol 21 (1): 166, 2021. [PUBMED Abstract]
Trudel-Fitzgerald C, Savard J, Ivers H: Longitudinal changes in clusters of cancer patients over an 18-month period. Health Psychol 33 (9): 1012-22, 2014. [PUBMED Abstract]
Kerrigan K, Patel SB, Haaland B, et al.: Prognostic Significance of Patient-Reported Outcomes in Cancer. JCO Oncol Pract 16 (4): e313-e323, 2020. [PUBMED Abstract]
Aktas A: Cancer symptom clusters: current concepts and controversies. Curr Opin Support Palliat Care 7 (1): 38-44, 2013. [PUBMED Abstract]
Identification of Symptom Clusters: Methods and Limitations
To identify cancer-related symptom clusters, investigators ask patients to complete valid, reliable symptom questionnaires.[1] Symptom data can also be obtained directly from clinicians and/or medical records. Symptom data are analyzed to identify symptoms that occur in clusters, using methods such as exploratory factor analysis (EFA).[2,3] The objective of an EFA is to identify groups of symptoms that are correlated with each other. These groups are known as factors or, in the field of symptom cluster research, symptom clusters. Factor analysis is consistent with a biopsychosocial theory [4] that the underlying mechanisms of symptoms are likely shared within symptom clusters.
Another method for identifying symptom clusters is through structural equation modeling (SEM).[3] Compared with factor analysis that retrospectively identifies clusters, SEM requires an a priori hypothesis about a common cause of the symptom cluster.[3] One benefit of SEM is that direct and indirect, as well as latent, associations between factors can be identified.[3] This method can help identify risk factors in future patients.
Once a symptom cluster has been identified, investigators perform additional analyses to describe patients’ experiences with a symptom cluster. A person-centered analytic approach, such as latent class profile analysis, is used to identify and describe subgroups of patients who are similarly burdened by a symptom cluster.[5,6] The symptom cluster burden has multiple dimensions, including the occurrence, frequency, severity, and distress associated with the symptom cluster.[6,7] Determining which patients are at risk for the highest level of symptom cluster burden and associated underlying mechanisms are ongoing areas of research.
Common characteristics associated with a higher symptom cluster burden include the following:[1,8–10]
Younger age.
Non-White race and ethnicity.
Unmarried/unpartnered.
Unemployed.
Lower annual income.
Child care responsibilities.
Higher comorbidity burden.
Lower functional status.
One limitation in identifying and managing symptom clusters is that symptom assessment tools and analytic approaches may vary across clinical practices. However, the consistency of symptom clusters identified across studies using different instruments supports the fact that core symptoms are being captured and that underlying mechanisms may be associated with symptoms within a cluster. For example, two symptom clusters common to multiple cancer diagnoses and treatment regimens are a sickness behavior syndrome (fatigue, sleep disturbance, lethargy, depression, loss of appetite) [11–13] and a psychoneurological symptom cluster (depression, cognitive disturbance, sleep disturbance, fatigue, pain).[14,15] Both of these symptom clusters are associated with underlying inflammatory mechanisms.[11,12,15]
Another limitation is that while some symptom clusters appear to be stable over time, [16,17] a patient’s symptom experience may vary widely.[7] Specifically, the occurrence of symptoms within a cluster, the level of symptom cluster severity, and the level of distress associated with one or more symptom clusters may shift over time in each individual. Symptom clusters can also persist long after treatment.[7,18]
Due to the complexity of symptom clusters, the symptoms within each cluster, and the temporal nature of symptoms/clusters that may shift over time, it is important to continually assess symptoms from diagnosis through the end of life. Retesting symptom clusters through repeated data-driven analyses (e.g., factor analysis,[2,3] SEM,[3]) can help health care professionals to better understand the stability and/or changes in symptom cluster experiences over time. In addition, symptom clusters may differ between individuals who are undergoing active treatment and those who have completed primary therapy.
Miaskowski C, Cooper BA, Paul SM, et al.: Subgroups of patients with cancer with different symptom experiences and quality-of-life outcomes: a cluster analysis. Oncol Nurs Forum 33 (5): E79-89, 2006. [PUBMED Abstract]
Skerman HM, Yates PM, Battistutta D: Identification of cancer-related symptom clusters: an empirical comparison of exploratory factor analysis methods. J Pain Symptom Manage 44 (1): 10-22, 2012. [PUBMED Abstract]
Olson K, Hayduk L, Thomas J: Comparing two approaches for studying symptom clusters: factor analysis and structural equation modeling. Support Care Cancer 22 (1): 153-61, 2014. [PUBMED Abstract]
Borrell-Carrió F, Suchman AL, Epstein RM: The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med 2 (6): 576-82, 2004. [PUBMED Abstract]
Miaskowski C, Dunn L, Ritchie C, et al.: Latent Class Analysis Reveals Distinct Subgroups of Patients Based on Symptom Occurrence and Demographic and Clinical Characteristics. J Pain Symptom Manage 50 (1): 28-37, 2015. [PUBMED Abstract]
Miaskowski C, Barsevick A, Berger A, et al.: Advancing Symptom Science Through Symptom Cluster Research: Expert Panel Proceedings and Recommendations. J Natl Cancer Inst 109 (4): , 2017. [PUBMED Abstract]
Doong SH, Dhruva A, Dunn LB, et al.: Associations between cytokine genes and a symptom cluster of pain, fatigue, sleep disturbance, and depression in patients prior to breast cancer surgery. Biol Res Nurs 17 (3): 237-47, 2015. [PUBMED Abstract]
Hammer MJ, Cooper B, Paul SM, et al.: Identification of Distinct Symptom Profiles in Cancer Patients Using a Pre-Specified Symptom Cluster. J Pain Symptom Manage 64 (1): 17-27, 2022. [PUBMED Abstract]
Pud D, Ben Ami S, Cooper BA, et al.: The symptom experience of oncology outpatients has a different impact on quality-of-life outcomes. J Pain Symptom Manage 35 (2): 162-70, 2008. [PUBMED Abstract]
Aktas A: Cancer symptom clusters: current concepts and controversies. Curr Opin Support Palliat Care 7 (1): 38-44, 2013. [PUBMED Abstract]
Chan CW, Lee PH, Molassiotis A, et al.: Symptom Clusters in Postchemotherapy Neutropenic Fever in Hematological Malignancy: Associations Among Sickness Behavior Symptom Cluster, Inflammatory Biomarkers of Procalcitonin and C-Reactive Protein, and Febrile Measures. J Pain Symptom Manage 59 (6): 1204-1211, 2020. [PUBMED Abstract]
Wood LJ, Weymann K: Inflammation and neural signaling: etiologic mechanisms of the cancer treatment-related symptom cluster. Curr Opin Support Palliat Care 7 (1): 54-9, 2013. [PUBMED Abstract]
Trudel-Fitzgerald C, Savard J, Ivers H: Longitudinal changes in clusters of cancer patients over an 18-month period. Health Psychol 33 (9): 1012-22, 2014. [PUBMED Abstract]
Kim HJ, Barsevick AM, Fang CY, et al.: Common biological pathways underlying the psychoneurological symptom cluster in cancer patients. Cancer Nurs 35 (6): E1-E20, 2012. [PUBMED Abstract]
Kim E, Jahan T, Aouizerat BE, et al.: Changes in symptom clusters in patients undergoing radiation therapy. Support Care Cancer 17 (11): 1383-91, 2009. [PUBMED Abstract]
Pozzar RA, Hammer MJ, Cooper BA, et al.: Stability of Symptom Clusters in Patients With Gynecologic Cancer Receiving Chemotherapy. Cancer Nurs 45 (4): E706-E718, 2022 Jul-Aug 01. [PUBMED Abstract]
Brant JM, Beck S, Dudley WN, et al.: Symptom trajectories in posttreatment cancer survivors. Cancer Nurs 34 (1): 67-77, 2011. [PUBMED Abstract]
Predictors and Outcomes of Select Symptom Clusters
Symptom cluster names are often based on symptoms of the cluster (e.g., psychoneurological[1] and gastrointestinal[2]), although names are not standardized across studies. One frequent unnamed cluster identified across cancer diagnoses includes pain, fatigue, sleep disturbance, and depression.[3] This general symptom cluster has been identified in patients with breast,[4,5] lung,[5,6] gastrointestinal,[5,7] and gynecologic [5,8] cancers. Symptom clusters can also reflect underlying disease (e.g., dyspnea, cough, and fatigue in patients with lung cancer) [9] and/or treatments (e.g., sensory neuropathy symptom cluster, mixed motor-sensory symptom cluster related to chemotherapy-induced peripheral neuropathy).[10]
References
Kim HJ, Barsevick AM, Fang CY, et al.: Common biological pathways underlying the psychoneurological symptom cluster in cancer patients. Cancer Nurs 35 (6): E1-E20, 2012. [PUBMED Abstract]
Harris CS, Miaskowski CA, Conley YP, et al.: Gastrointestinal Symptom Cluster is Associated With Epigenetic Regulation of Lymphotoxin Beta in Oncology Patients Receiving Chemotherapy. Biol Res Nurs 25 (1): 51-64, 2023. [PUBMED Abstract]
Trudel-Fitzgerald C, Savard J, Ivers H: Longitudinal changes in clusters of cancer patients over an 18-month period. Health Psychol 33 (9): 1012-22, 2014. [PUBMED Abstract]
Doong SH, Dhruva A, Dunn LB, et al.: Associations between cytokine genes and a symptom cluster of pain, fatigue, sleep disturbance, and depression in patients prior to breast cancer surgery. Biol Res Nurs 17 (3): 237-47, 2015. [PUBMED Abstract]
Miaskowski C, Cooper BA, Paul SM, et al.: Subgroups of patients with cancer with different symptom experiences and quality-of-life outcomes: a cluster analysis. Oncol Nurs Forum 33 (5): E79-89, 2006. [PUBMED Abstract]
Brant JM, Beck S, Dudley WN, et al.: Symptom trajectories in posttreatment cancer survivors. Cancer Nurs 34 (1): 67-77, 2011. [PUBMED Abstract]
Lin Y, Bailey DE, Docherty SL, et al.: Distinct morning and evening fatigue profiles in gastrointestinal cancer during chemotherapy. BMJ Support Palliat Care 13 (e2): e373-e381, 2023. [PUBMED Abstract]
Pozzar RA, Hammer MJ, Cooper BA, et al.: Symptom Clusters in Patients With Gynecologic Cancer Receiving Chemotherapy. Oncol Nurs Forum 48 (4): 441-452, 2021. [PUBMED Abstract]
Cheville AL, Novotny PJ, Sloan JA, et al.: Fatigue, dyspnea, and cough comprise a persistent symptom cluster up to five years after diagnosis with lung cancer. J Pain Symptom Manage 42 (2): 202-12, 2011. [PUBMED Abstract]
Wang M, Cheng HL, Lopez V, et al.: Redefining chemotherapy-induced peripheral neuropathy through symptom cluster analysis and patient-reported outcome data over time. BMC Cancer 19 (1): 1151, 2019. [PUBMED Abstract]
Symptom Clusters Common Across Heterogeneous Treatments
Several symptom clusters have been identified across cancer diagnoses and treatments in patients undergoing treatment and throughout survivorship. To date, most studies of symptom clusters in patients undergoing active treatment have analyzed data from patients receiving the same treatment. A limited number of studies suggest the same symptom clusters may occur in groups of patients receiving heterogeneous therapies. A pooled analysis included data from 1,561 patients with advanced cancer in 15 countries. Four symptom clusters were common in patients with myeloma and breast, colorectal, lung, and prostate cancer who were receiving chemotherapy, radiation therapy, analgesics, surgery, and other or no treatments.[1] These clusters included an emotional cluster comprised of feeling tense, worried, irritable, and depressed; a fatigue-pain cluster; a nausea-vomiting cluster; and a cognitive cluster comprised of difficulties with concentration and memory.
In another study of 93 Chinese patients with cervical cancer, mood-cognitive, gastrointestinal, sickness behavior, and pain-related symptom clusters were identified in patients receiving chemoradiation therapy, radiation therapy alone, and surgery followed by chemoradiation. Mean symptom severity scores were not significantly different across these three treatment groups.[2]
Finally, a longitudinal study of 92 patients with metastatic lung cancer assessed interrelationships between depressive symptoms and a sickness behavior symptom cluster. In this sample, 40.5% of participants were receiving chemotherapy, 35.7% were receiving immunotherapy, and 23.8% were receiving oral targeted therapies. All 12 sickness behavior symptoms were significantly associated with patients’ scores on the Patient Health Questionnaire-9 and Hospital Anxiety and Depression Scale depression subscale. Sickness behavior symptom severity was significantly higher in patients receiving chemotherapy than in those receiving oral targeted therapies. However, symptom severity among patients receiving immunotherapy did not differ significantly from symptom severity of the other two groups.[3]
In individuals who have completed primary therapy, psychological/cognitive/fatigue clusters are common (e.g., emotional distress, fatigue, cognitive dysfunction;[4] fatigue, difficulty concentrating, drowsiness[5]). In addition, there is evidence for long-term effects in a sickness behavior cluster (e.g., lethargy, sleepiness, depressed mood, hyperalgesia).[6]
In a study of 300 patients receiving palliative chemotherapy, one of the symptom clusters identified was fatigue-cognitive, which was associated with decreased functional status and poor quality of life.[5] The authors highlighted that fatigue is often included in other clusters (e.g., fatigue, dyspnea, drowsiness, pain). Fatigue has also been identified in sickness behavior clusters.[6] Because fatigue is prevalent across a number of symptom clusters, it may be helpful to target fatigue to mitigate the effects of symptom clusters across patient populations.
Additional research using a person-centered approach is needed to understand the individual experiences of symptom clusters over time. Interventions to mitigate a high symptom burden should be tailored to individual symptom cluster profiles.
References
Dong ST, Costa DS, Butow PN, et al.: Symptom Clusters in Advanced Cancer Patients: An Empirical Comparison of Statistical Methods and the Impact on Quality of Life. J Pain Symptom Manage 51 (1): 88-98, 2016. [PUBMED Abstract]
Wang CL, Wu WY, Lou HM, et al.: Analysis of symptom clusters in Chinese cervical cancer patients undergoing radiotherapy, chemoradiotherapy, or postoperative chemoradiotherapy. Eur J Gynaecol Oncol 38 (3): 398-403, 2017. [PUBMED Abstract]
McFarland DC, Walsh LE, Saracino R, et al.: The Sickness Behavior Inventory-Revised: Sickness behavior and its associations with depression and inflammation in patients with metastatic lung cancer. Palliat Support Care 19 (3): 312-321, 2021. [PUBMED Abstract]
Levkovich I, Cohen M, Alon S, et al.: Symptom cluster of emotional distress, fatigue and cognitive difficulties among young and older breast cancer survivors: The mediating role of subjective stress. J Geriatr Oncol 9 (5): 469-475, 2018. [PUBMED Abstract]
Rha SY, Lee J: Symptom clusters during palliative chemotherapy and their influence on functioning and quality of life. Support Care Cancer 25 (5): 1519-1527, 2017. [PUBMED Abstract]
Zick SM, Zwickey H, Wood L, et al.: Preliminary differences in peripheral immune markers and brain metabolites between fatigued and non-fatigued breast cancer survivors: a pilot study. Brain Imaging Behav 8 (4): 506-16, 2014. [PUBMED Abstract]
Pathogenesis of Symptom Clusters
The pathogenesis of symptom clusters has not been clearly established. However, some mechanisms (e.g., chronic inflammation) and interaction effects with patient-specific characteristics (e.g., clinical, environmental, behavioral) are beginning to unfold. Examples of evidence for common pathogenic mechanisms for selected symptom clusters are summarized below.
One or more symptoms associated with the sickness behavior syndrome (e.g., fatigue, sleep disturbance, lethargy, depression, loss of appetite) are common in a number of other symptom clusters.[1–3] It is a plausible model for understanding the pathogenesis of symptom clusters. The physiological and psychological stress of cancer may be an underlying trigger for the co-occurring symptoms identified in symptom clusters.[4] Central nervous system (CNS) activation of acute psychological stress engages the hypothalamic-pituitary-adrenal axis and sympathetic-adrenal-medullary system to produce increased levels of cortisol. Prolonged stress dampens the homeostatic circadian rhythm of cortisol, causing glucocorticoid resistance, in which immune cells become less sensitive to glucocorticoids.[5] Decreased sensitivity triggers increased levels of glucocorticoids [4,5] as well as epinephrine and norepinephrine.[4]
In addition, cellular responses to regain homeostasis, termed allostasis, include secreting catecholamines and cytokines.[5] With chronic stress, allostatic overload occurs with an increase in pro-inflammatory cytokines. In particular, interleukin (IL)-1-beta, IL-6, tumor necrosis factor-alpha (TNF-alpha), and others are secreted.[3–5] Prolonged secretion of IL-1-beta is associated with sickness behavior symptoms through inducing prostaglandins and activating T and B cells and antibodies.[3,5] In addition, IL-6,[6–8] TNF-alpha,[9–11], and nuclear-factor kappa B [12]—a transcription factor that induces multiple inflammatory cytokines to enter into circulation—have been associated with high symptom severity.
Given the psychological influence of CNS-triggered downstream responses that lead to chronic inflammatory-associated symptoms, individual coping mechanisms and levels of resilience to stress may explain some of the interindividual variability in symptom cluster experiences. Research is just beginning to capture the multiple social determinants of health (e.g., social, structural, environmental, behavioral) that may influence an individual’s perception of and response to stress. To best understand the pathogenesis associated with the symptom cluster phenotype, a person-centered approach to research and clinical care is warranted.
References
Aktas A: Cancer symptom clusters: current concepts and controversies. Curr Opin Support Palliat Care 7 (1): 38-44, 2013. [PUBMED Abstract]
Chan CW, Lee PH, Molassiotis A, et al.: Symptom Clusters in Postchemotherapy Neutropenic Fever in Hematological Malignancy: Associations Among Sickness Behavior Symptom Cluster, Inflammatory Biomarkers of Procalcitonin and C-Reactive Protein, and Febrile Measures. J Pain Symptom Manage 59 (6): 1204-1211, 2020. [PUBMED Abstract]
Wood LJ, Weymann K: Inflammation and neural signaling: etiologic mechanisms of the cancer treatment-related symptom cluster. Curr Opin Support Palliat Care 7 (1): 54-9, 2013. [PUBMED Abstract]
Cui B, Peng F, Lu J, et al.: Cancer and stress: NextGen strategies. Brain Behav Immun 93: 368-383, 2021. [PUBMED Abstract]
Zefferino R, Di Gioia S, Conese M: Molecular links between endocrine, nervous and immune system during chronic stress. Brain Behav 11 (2): e01960, 2021. [PUBMED Abstract]
Miaskowski C, Dodd M, Lee K, et al.: Preliminary evidence of an association between a functional interleukin-6 polymorphism and fatigue and sleep disturbance in oncology patients and their family caregivers. J Pain Symptom Manage 40 (4): 531-44, 2010. [PUBMED Abstract]
Hiensch AE, Mijwel S, Bargiela D, et al.: Inflammation Mediates Exercise Effects on Fatigue in Patients with Breast Cancer. Med Sci Sports Exerc 53 (3): 496-504, 2021. [PUBMED Abstract]
Lengacher CA, Reich RR, Paterson CL, et al.: A Large Randomized Trial: Effects of Mindfulness-Based Stress Reduction (MBSR) for Breast Cancer (BC) Survivors on Salivary Cortisol and IL-6. Biol Res Nurs 21 (1): 39-49, 2019. [PUBMED Abstract]
Calvo-Schimmel A, Kober KM, Paul SM, et al.: Sleep disturbance is associated with perturbations in immune-inflammatory pathways in oncology outpatients undergoing chemotherapy. Sleep Med 101: 305-315, 2023. [PUBMED Abstract]
Dhruva A, Aouizerat BE, Cooper B, et al.: Cytokine gene associations with self-report ratings of morning and evening fatigue in oncology patients and their family caregivers. Biol Res Nurs 17 (2): 175-84, 2015. [PUBMED Abstract]
Kober KM, Harris C, Conley YP, et al.: Perturbations in common and distinct inflammatory pathways associated with morning and evening fatigue in outpatients receiving chemotherapy. Cancer Med 12 (6): 7369-7380, 2023. [PUBMED Abstract]
Kober KM, Smoot B, Paul SM, et al.: Polymorphisms in Cytokine Genes Are Associated With Higher Levels of Fatigue and Lower Levels of Energy in Women After Breast Cancer Surgery. J Pain Symptom Manage 52 (5): 695-708.e4, 2016. [PUBMED Abstract]
Symptom Clusters by Treatment Modality
Cancerous tissue and treatment-related side effects are common causes of symptoms within a cluster. Of note, disease and treatments are not always directly related to symptom cluster experiences.[1] In a study of 582 patients receiving treatment for heterogenous types of cancer, the type of cancer diagnosis and treatment received did not predict symptom severity subgroups.[1] This finding suggests that multiple factors likely influence symptom cluster experiences. However, based on known contributors to some symptoms by the type of treatment (e.g., taxane-induced neuropathies [2]), the discussion below highlights symptom clusters identified in patients receiving specific therapies.
Chemotherapy
A substantial body of research has focused on the symptom experiences of people undergoing chemotherapy. To date, symptom clusters have been identified in patients undergoing chemotherapy for brain,[3] breast,[4–11] gastrointestinal,[12,13] gynecologic,[14,15] hematological,[16–19] and lung cancers.[20,21] Symptom clusters have also been identified in samples of patients undergoing chemotherapy for heterogenous cancer types.[22,23]
In a 2022 systematic review of studies of symptom clusters in patients undergoing chemotherapy, several common symptom clusters were identified across cancer diagnoses. The most common symptom cluster was comprised of psychological symptoms. “Feeling nervous” (or “feeling anxious”) and “feeling sad” (or “depressed mood”) were the most common symptoms in this cluster. Other common symptoms in this cluster included “feeling irritable,” “worrying,” and “difficulty concentrating.” The second most common symptom cluster involved gastrointestinal symptoms, including nausea and abdominal cramps. Additional symptom clusters identified across diagnoses included the following:[24]
A nutrition/weight-change symptom cluster, with symptoms such as weight gain, weight loss, decreased appetite, and increased appetite.
An epithelial/body-image symptom cluster, comprised of itching, hair loss, and skin change.
A respiratory symptom cluster, comprised of shortness of breath, difficulty breathing, and cough.
Certain symptom clusters are common across a limited number of cancer diagnoses. For example, a systematic review found that a vasomotor-hormonal symptom cluster was identified in studies of patients receiving chemotherapy for breast and gynecologic cancers.[24]
Radiation Therapy
Symptom clusters have been described in patients receiving radiation therapy (RT) for brain,[25] breast,[26,27] gastrointestinal,[28] head and neck,[29,30,30] and prostate cancers.[31,32] Other studies have found symptoms clusters in patients receiving RT for a number of cancers.[33,34]
In a study of 1,224 patients with breast cancer receiving RT, symptoms found to cluster together before, during, and after RT included depression and anxiety, nausea and appetite loss, pain and tiredness, and drowsiness, dyspnea, and tiredness.[26] A study of 100 patients with head and neck cancer in Taiwan who were undergoing postoperative RT identified two symptom clusters that were stable throughout treatment: a head and neck–specific cluster (including pain, dry mouth, appetite, sleep disturbance, fatigue, drowsiness, distress, and sadness) and a gastrointestinal cluster (including nausea, vomiting, numbness, dyspnea, and difficulty with memory).[35] In 843 patients undergoing RT for prostate cancer, seven symptom clusters were identified. Early symptoms, older age, and decreased physical function were associated with the severity of late symptom clusters.[32]
In addition, polymorphisms in cytokine genes were associated with symptom clusters in a sample of 157 patients receiving RT for breast and prostate cancer, suggesting that common symptom clusters may be related to inflammatory processes.[36] Polymorphisms in neurotransmitter genes were associated with the severity of sickness behavior, mood-cognitive, and treatment-related symptom clusters, suggesting that mechanisms other than inflammation may also contribute to the development of symptom clusters.[37]
Immunotherapy
Immunotherapies are a relatively new approach to cancer treatments, and numerous newly developed immunotherapy treatments are in phase I clinical trials. As a result, the scope of symptom clusters in patients receiving these therapies is yet to be understood.
References
Miaskowski C, Cooper BA, Melisko M, et al.: Disease and treatment characteristics do not predict symptom occurrence profiles in oncology outpatients receiving chemotherapy. Cancer 120 (15): 2371-8, 2014. [PUBMED Abstract]
Wang M, Cheng HL, Lopez V, et al.: Redefining chemotherapy-induced peripheral neuropathy through symptom cluster analysis and patient-reported outcome data over time. BMC Cancer 19 (1): 1151, 2019. [PUBMED Abstract]
Kim S: A Longitudinal Study of Lipid Peroxidation and Symptom Clusters in Patients With Brain Cancers. Nurs Res 67 (5): 387-394, 2018. [PUBMED Abstract]
Albusoul RM, Berger AM, Gay CL, et al.: Symptom Clusters Change Over Time in Women Receiving Adjuvant Chemotherapy for Breast Cancer. J Pain Symptom Manage 53 (5): 880-886, 2017. [PUBMED Abstract]
Berger AM, Kumar G, LeVan TD, et al.: Symptom Clusters and Quality of Life over 1 Year in Breast Cancer Patients Receiving Adjuvant Chemotherapy. Asia Pac J Oncol Nurs 7 (2): 134-140, 2020. [PUBMED Abstract]
Browall M, Brandberg Y, Nasic S, et al.: A prospective exploration of symptom burden clusters in women with breast cancer during chemotherapy treatment. Support Care Cancer 25 (5): 1423-1429, 2017. [PUBMED Abstract]
Li H, Sereika SM, Marsland AL, et al.: Symptom Clusters in Women With Breast Cancer During the First 18 Months of Adjuvant Therapy. J Pain Symptom Manage 59 (2): 233-241, 2020. [PUBMED Abstract]
Sullivan CW, Leutwyler H, Dunn LB, et al.: Stability of Symptom Clusters in Patients With Breast Cancer Receiving Chemotherapy. J Pain Symptom Manage 55 (1): 39-55, 2018. [PUBMED Abstract]
Wiggenraad F, Bolam KA, Mijwel S, et al.: Long-Term Favorable Effects of Physical Exercise on Burdensome Symptoms in the OptiTrain Breast Cancer Randomized Controlled Trial. Integr Cancer Ther 19: 1534735420905003, 2020. [PUBMED Abstract]
Vuttanon N, Finnegan L, Lojanapiwat B, et al.: Effect of progressive muscle relaxation on symptom clusters in breast cancer patients receiving chemotherapy: A quasi-experimental controlled trial. Complement Ther Clin Pract 37: 27-31, 2019. [PUBMED Abstract]
Li H, Sereika SM, Marsland AL, et al.: Impact of chemotherapy on symptoms and symptom clusters in postmenopausal women with breast cancer prior to aromatase inhibitor therapy. J Clin Nurs 28 (23-24): 4560-4571, 2019. [PUBMED Abstract]
Han CJ, Reding K, Cooper BA, et al.: Stability of Symptom Clusters in Patients With Gastrointestinal Cancers Receiving Chemotherapy. J Pain Symptom Manage 58 (6): 989-1001.e10, 2019. [PUBMED Abstract]
Han CJ, Reding K, Cooper BA, et al.: Symptom Clusters in Patients With Gastrointestinal Cancers Using Different Dimensions of the Symptom Experience. J Pain Symptom Manage 58 (2): 224-234, 2019. [PUBMED Abstract]
Pozzar RA, Hammer MJ, Cooper BA, et al.: Symptom Clusters in Patients With Gynecologic Cancer Receiving Chemotherapy. Oncol Nurs Forum 48 (4): 441-452, 2021. [PUBMED Abstract]
Pozzar RA, Hammer MJ, Cooper BA, et al.: Stability of Symptom Clusters in Patients With Gynecologic Cancer Receiving Chemotherapy. Cancer Nurs 45 (4): E706-E718, 2022 Jul-Aug 01. [PUBMED Abstract]
Lin DM, Yin XX, Wang N, et al.: Consensus in Identification and Stability of Symptom Clusters Using Different Symptom Dimensions in Newly Diagnosed Acute Myeloid Leukemia Patients Undergoing Induction Therapy. J Pain Symptom Manage 57 (4): 783-792, 2019. [PUBMED Abstract]
Chen F, Leng Y, Zhang L, et al.: The Correlation of Symptom Clusters and Functional Performance in Adult Acute Leukemia Patients Under Chemotherapy. Cancer Nurs 44 (5): E287-E295, 2021 Sep-Oct 01. [PUBMED Abstract]
Cherwin CH, Perkhounkova Y: Distress-Based Gastrointestinal Symptom Clusters and Impact on Symptom Interference and Quality of Life in Patients with a Hematologic Malignancy Receiving Chemotherapy. J Pain Symptom Manage 53 (4): 751-758, 2017. [PUBMED Abstract]
Sezgin MG, Bektaş H: Symptom Clustering and Its Effect on Functional Status in Lymphoma Patients. Florence Nightingale J Nurs 28 (2): 143-154, 2020. [PUBMED Abstract]
Russell J, Wong ML, Mackin L, et al.: Stability of Symptom Clusters in Patients With Lung Cancer Receiving Chemotherapy. J Pain Symptom Manage 57 (5): 909-922, 2019. [PUBMED Abstract]
Wong ML, Cooper BA, Paul SM, et al.: Differences in Symptom Clusters Identified Using Ratings of Symptom Occurrence vs. Severity in Lung Cancer Patients Receiving Chemotherapy. J Pain Symptom Manage 54 (2): 194-203, 2017. [PUBMED Abstract]
Matzka M, Köck-Hódi S, Jahn P, et al.: Relationship among symptom clusters, quality of life, and treatment-specific optimism in patients with cancer. Support Care Cancer 26 (8): 2685-2693, 2018. [PUBMED Abstract]
Papachristou N, Barnaghi P, Cooper B, et al.: Network Analysis of the Multidimensional Symptom Experience of Oncology. Sci Rep 9 (1): 2258, 2019. [PUBMED Abstract]
Harris CS, Kober KM, Conley YP, et al.: Symptom clusters in patients receiving chemotherapy: A systematic review. BMJ Support Palliat Care 12 (1): 10-21, 2022. [PUBMED Abstract]
Langegård U, Johansson B, Bjork-Eriksson T, et al.: Symptom Clusters in Patients With Brain Tumors Undergoing Proton Beam Therapy. Oncol Nurs Forum 46 (3): 349-363, 2019. [PUBMED Abstract]
Chow S, Wan BA, Pidduck W, et al.: Symptom clusters in patients with breast cancer receiving radiation therapy. Eur J Oncol Nurs 42: 14-20, 2019. [PUBMED Abstract]
Harris C, Kober KM, Paul SM, et al.: Neurotransmitter Gene Polymorphisms Are Associated with Symptom Clusters in Patients Undergoing Radiation Therapy. Semin Oncol Nurs 39 (4): 151461, 2023. [PUBMED Abstract]
Poon M, Dennis K, DeAngelis C, et al.: Symptom clusters of gastrointestinal cancer patients undergoing radiotherapy using the Functional Living Index-Emesis (FLIE) quality-of-life tool. Support Care Cancer 23 (9): 2589-98, 2015. [PUBMED Abstract]
Rosenthal DI, Mendoza TR, Fuller CD, et al.: Patterns of symptom burden during radiotherapy or concurrent chemoradiotherapy for head and neck cancer: a prospective analysis using the University of Texas MD Anderson Cancer Center Symptom Inventory-Head and Neck Module. Cancer 120 (13): 1975-84, 2014. [PUBMED Abstract]
Xiao W, Chan CWH, Fan Y, et al.: Symptom clusters in patients with nasopharyngeal carcinoma during radiotherapy. Eur J Oncol Nurs 28: 7-13, 2017. [PUBMED Abstract]
Kim E, Jahan T, Aouizerat BE, et al.: Changes in symptom clusters in patients undergoing radiation therapy. Support Care Cancer 17 (11): 1383-91, 2009. [PUBMED Abstract]
Lemanska A, Dearnaley DP, Jena R, et al.: Older Age, Early Symptoms and Physical Function are Associated with the Severity of Late Symptom Clusters for Men Undergoing Radiotherapy for Prostate Cancer. Clin Oncol (R Coll Radiol) 30 (6): 334-345, 2018. [PUBMED Abstract]
Ganesh V, Zhang L, Chan S, et al.: An update in symptom clusters using the Edmonton Symptom Assessment System in a palliative radiotherapy clinic. Support Care Cancer 25 (11): 3321-3327, 2017. [PUBMED Abstract]
Ganesh V, Zhang L, Wan BA, et al.: Symptom clusters using the EORTC QLQ-C15-PAL in palliative radiotherapy. Ann Palliat Med 7 (2): 192-204, 2018. [PUBMED Abstract]
Chiang SH, Ho KY, Wang SY, et al.: Change in symptom clusters in head and neck cancer patients undergoing postoperative radiotherapy: A longitudinal study. Eur J Oncol Nurs 35: 62-66, 2018. [PUBMED Abstract]
Harris CS, Miaskowski CA, Conley YP, et al.: Gastrointestinal Symptom Cluster is Associated With Epigenetic Regulation of Lymphotoxin Beta in Oncology Patients Receiving Chemotherapy. Biol Res Nurs 25 (1): 51-64, 2023. [PUBMED Abstract]
Management of Cancer-Related Symptom Clusters
General Approach
The first step in the management of symptom clusters involves an open-ended patient interview to identify symptoms that are bothersome. The next step is to identify the most distressing symptoms with significant negative impact on the patient’s quality of life and functioning. A subsequent step is to determine the frequency and severity of the predominant symptoms. This step can be accomplished with a guided interview and objective assessment of individual symptoms using validated questionnaires. For more information, see Fatigue, Depression, and Sleep Disorders.
Another important step is to identify the nature of relationships among the symptoms if one exists. This step is critical to minimize unnecessary interventions that might be burdensome for patients already struggling with multiple symptoms and quality-of-life issues. Associations among symptoms in a cluster inform management of symptoms in that cluster. Different ways that symptoms in a cluster may be related to each other include the following:
A primary symptom leading to other symptoms in a symptom cluster (e.g., insomnia leading to fatigue, anxiety, and depression; hot flashes causing insomnia, which in turn causes anxiety and fatigue; pain causing anxiety and insomnia). In such cases, management will involve first treating the primary symptom if it can be identified.
Symptoms as side effects of a treatment used to treat another symptom (e.g., daytime fatigue as a side effect of hypnotics used to treat insomnia or mirtazapine used to treat depression). Management in such cases involves identifying alternative treatments or optimizing the dose of the triggering medication to minimize the symptom/side effect.
Common biological mechanisms underlying multiple symptoms (e.g., an inflammatory mechanism underlying fatigue, depression, sleep disturbances, and cognitive issues). The underlying inflammatory process may be a treatment target. In some cases, management may involve optimizing cancer treatment regimens, considering the risk-benefit ratio.
Common psychological and/or social factors underlying symptom clusters (e.g., fear of cancer recurrence that causes anxiety, insomnia, and depression; financial or relationship issues as a trigger for insomnia, anxiety, and depression). Addressing the underlying psychological or social factor is the primary treatment strategy in these cases.
Most symptom management studies test the efficacy of the proposed intervention on a single target symptom as the primary outcome and evaluate secondary impact on a related set of symptoms or on the overall symptom burden.[1–4] A small number of studies have evaluated the efficacy of certain interventions on multiple co-occurring and related symptoms in symptom clusters. A randomized controlled trial using cognitive behavioral therapy for insomnia (CBT-I) showed improvement in insomnia, fatigue, and depression symptoms.[1,3,4] Another controlled trial found improvement in cognitive, gastrointestinal, and other symptom clusters using a multimodal intervention that included structured exercise, relaxation, and psychosocial support.[5]
An important part of managing symptom clusters involves patient and caregiver education. Such education includes discussion of co-occurrence of symptoms and their potential relationship to each other. Patients can also be informed that an intervention targeting a specific symptom may impact other, related symptoms. Another step involves identification of symptoms that may be due to side effects of another intervention. In these cases, addressing the target symptom involves optimizing the triggering intervention or, if possible, considering alternative treatments.
If an intervention is deemed necessary, pharmacological and nonpharmacological strategies can be considered (see Table 1).
Table 1. Effective Treatment Modalities Across Multiple Cancer Symptoms and Symptom Clusters
Studies investigating pharmacological interventions generally target a primary symptom while evaluating the impact on other, related symptoms as secondary outcomes. Certain pharmacological interventions have shown efficacy in the management of multiple symptoms in separate studies. For example, serotonin-norepinephrine reuptake inhibitors (SNRIs), specifically duloxetine and venlafaxine, are known to treat depression (see the Pharmacological Intervention section in Depression). SNRIs are also effective in the management of chemotherapy-induced peripheral neuropathy (CIPN) (see the Venlafaxine and duloxetine section in Cancer Pain).[6] Venlafaxine has also shown efficacy in the management of hot flashes in breast cancer survivors.[7] These efficacy studies targeting specific symptoms have been conducted in patients with cancer and in general patient populations.
When pharmacological interventions are considered, the primary goal is to optimize the medication regimen and minimize side-effect burden. Steps to achieve this goal include the following:
Review the patient’s medication list to check if the target symptom is due to side effects of a medication. If a triggering medication is identified, assess if the medication is necessary. If the medication is deemed necessary, examine the dose and/or frequency. Alternatively, consider a substitute medication with similar efficacy but fewer possible side effects causing the target symptom.
If a pharmacological intervention is considered, it is important to select a medication that can target multiple symptoms if possible. This strategy can help minimize the side-effect burden.
Nonpharmacological Interventions
Nonpharmacological interventions for the management of cancer-related symptom clusters may include exercise, mindfulness, and psychological therapies.
Exercise
Exercise has been defined as physical activity that is planned or structured and involves repetitive bodily movements to improve or maintain cardiorespiratory endurance, muscular strength, muscular endurance, flexibility, and body composition. Physical activity has been defined as bodily movements produced by skeletal muscles that result in energy expenditure.[8] Physical activity can include all levels of intensity, including light, moderate, moderate-to-vigorous, and vigorous.[9]
The American College of Sports Medicine’s published recommendations for exercise in cancer survivors suggest starting slowly and progressing to 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic exercise per week.[10] This aerobic exercise is accompanied by 20 to 30 minutes of strength training across all major muscle groups 2 to 3 times per week and regular stretching daily. Investigators have examined multiple forms of physical activity and their impact on cancer-related symptoms. This activity includes aerobic, anaerobic, muscle-strengthening, bone-strengthening, balance, and flexibility exercises, as well as yoga, tai chi, and qigong. However, most of this research has focused on a primary symptom versus a symptom cluster. A recent consensus statement regarding specific exercise guidelines for cancer survivors identified strong evidence for individual symptom management with exercise for anxiety, depression, and fatigue.[11] (Strong evidence was defined as having five or more randomized controlled trials with samples sizes of more than150 participants.) In addition, strong evidence was identified for better management of lymphedema, physical function, and health-related quality of life with exercise.[11] Of note, moderate evidence for bone health and sleep was identified, while insufficient evidence was found for cardiotoxicity, CIPN, pain, cognitive function, falls, nausea, sexual function, and treatment tolerance.[11]
The role of exercise in managing symptom clusters is more limited.[12–15] One study used a multimodal intervention of structured exercise, relaxation, and psychosocial support to address symptom clusters.[5] It noted improvement in gastrointestinal (nausea, vomiting, stomach pain, loss of appetite, diarrhea), cognitive (diminished concentration, memory problems, fatigue), functional (muscle and joint aches), and mucositis (mouth pain, throat pain, and difficulty swallowing) symptom clusters in the treatment group, but no improvement in an affective (nervousness, anxiety, and stress) symptom cluster, compared with usual care.
Mindfulness-based stress reduction (MBSR)
Studies investigating mindfulness commonly involve evaluation of its impact on a primary target symptom and on other, related symptoms as secondary outcomes. Studies that examined different approaches to MBSR–British Columbia (MBSR-BC) have found predominantly strong positive impacts on symptoms clusters, including combinations of the following:[16–26]
Perceived stress.
Anxiety.
Low energy and physical functioning.
Psychosocial health.
Fatigue.
Depression.
Feelings of helplessness.
Hostility/anger.
Fear of cancer recurrence.
Coping abilities.
Catastrophizing.
Many of the MBSR interventions involved multiweek programs in which participants were assessed for outcomes at 3-, 6- and 12-month intervals. During this time, survivors participated in mindfulness training and various exercises and were encouraged to continue using these skills on an ongoing basis. Improvement was measured using the following tools and scales:
Profile of Mood States.
Functional Assessment of Cancer Therapy–Endocrine Symptoms.
World Health Organization-5 Well-being Index.
Pain Intensity Scale.
Global Severity Index, SCL-90-R.
MBSR-BC consists of three components:
Educational material related to relaxation, meditation, the mind-body connection, and a healthy lifestyle for survivors.
Practice of meditation in group meetings and homework assignments.
Group processes related to barriers to the practice of meditation and supportive group interaction.
Many studies have evaluated mindfulness for improvement in anxiety and stress symptoms during cancer treatment. Patients who received MBSR while undergoing chemotherapy were shown to have reduced scores on an “overall suffering score.”[16–18,21–25] In two of the studies, technology was used to administer the intervention, one online [25] and another via smartphone.[22] These delivery methods provided more opportunities to incorporate mindfulness practices into the treatment of cancer survivors. In addition, some studies showed that the intervention groups had a lower symptom burden, compared with control groups, including more significant remission of both anxiety and depressive symptoms.[20] Measures of health-related quality of life (as demonstrated by the Functional Assessment of Cancer Therapy–Breast) were also significantly higher in the intervention group than in the control group.
Fatigue is a common complaint of cancer survivors at all stages, and it contributes to deterioration in many, if not all, psychosocial complaints. Integrating MBSR into cancer care can have many positive outcomes, including reduced fatigue.[17,18,22,26,27] Study participants experienced improvements in other psychosocial areas as well. Compared with control-group participants, those receiving MBSR had a statistically significant reduction in the overall suffering score, improvement in the total Hospital Anxiety and Depression Scale score, and improvement in the total Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being score.[28] In a randomized study of 92 patients, the intervention group experienced positive effects of concurrent MBSR on fatigue and coping while starting adjuvant paclitaxel.[26] While the interventions lasted 1 to 2 months in most cases, results at 6 to 12 months of follow-up showed maintained improvement.[17,18,22,26,27]
Another study, of 191 women with documented stress, showed an overall improvement in psychosocial stress and quality-of-life measures after receiving mindfulness-based art therapy (MBAT) versus standard education support groups. Significant improvements were observed immediately after intervention and 6 months later.[29] Patients with self-reported high levels of stress also experienced stress reduction with MBAT, compared with the standard education support groups.
Psychological therapies
Difficulty with sleep initiation and maintenance often co-occur with anxiety, depression, fatigue, and chronic pain.[30] There are a number of complex interactions with psychological disturbances mediating the relationship between pain and fatigue.[31] With these common symptoms, psychological therapies that target, or are known to create downstream effects on, multiple morbidities help patients address these issues through a single psychotherapeutic approach.
Cognitive behavioral therapy (CBT)
CBT specifically targets the patient’s maladaptive thoughts and behaviors that interfere with quality of life. CBT is a problem-focused form of therapy that encourages patients to take an active role in changing their thoughts and behaviors. This form of therapy can address several different cognitive, behavioral, and health targets. It can be provided in individual, group, or telehealth formats. Mobile apps based on cognitive behavioral principles have been successful in treating common psychological symptoms and psychological symptom clusters.[32]
In a multisite randomized controlled trial, 131 patients with cancer were randomly assigned to five sessions of standard CBT, five sessions of profile-tailored CBT, or usual care.[33] Assessments occurred at baseline, 1-month follow-up, and 6-month follow-up. Short- and long-term follow-ups suggested that the patients who received the profile-tailored CBT approach showed significant reductions in levels of pain, pain-associated sleep interference, confusion, bowel patterns, distress, functional status, and mental quality of life, compared with patients in the other two groups. Patients in the standard CBT group showed improvements in the common symptom clusters, compared with patients in the usual care group.
In another study, a cohort of 86 patients with mixed cancer diagnoses were randomly assigned to a 2-week, patient-directed intervention using cognitive behavioral principles or usual care.[34] The cognitive-behavioral intervention showed efficacy in treating a pain, fatigue, and sleep-disturbance symptom cluster. For patients experiencing this common symptom cluster acutely or mildly, a self-directed approach may be useful.
Acceptance and commitment therapy (ACT)
ACT is called a “Third Wave” CBT approach in that there are similarities to CBT, but the goal is to accept emotions and to understand situations that cannot be changed. This approach is considered an emotion-focused form of therapy. It comprises several techniques, including mindfulness and decreasing judgment about one’s thoughts and behaviors in any given situation.
Studies have shown strong empirical support for ACT’s positive benefits for the psychological symptom cluster (depression, anxiety, distress, quality of life) for patients at all stages of cancer. However, few studies have examined its effect on physical and health outcomes.[35] Those studies have shown no significant change in physical markers (pain, fatigue, sleep) after ACT therapy in patients with cancer. While there have been empirical studies of ACT in a number of cultures, countries, and ethnicities, most of the research has focused on female-specific cancers such as breast and ovarian.[36–39] There is limited empirical research on the applicability of ACT for males with cancer or patients experiencing physical symptoms.[38]
Meaning-centered psychotherapy
This form of psychotherapy, also called existential psychotherapy or meaning-making psychotherapy, is theoretically rooted in Victor Frankl’s book, Man’s Search for Meaning.[40] Empirical studies have shown that this approach may be useful for patients experiencing both psychological and common symptom clusters, especially in relation to end-of-life and survivorship concerns.[41]
A randomized controlled trial of 253 patients with stage III or IV solid-tumor cancer compared meaning-centered therapy with the active placebo of supportive group therapy. After 8 weekly group sessions, the group receiving meaning-centered therapy had stronger reductions in the psychological symptom clusters, as well as greater increases in spiritual well-being, than the placebo group.[42,43]
Meaning-centered psychotherapy has also been tested using an individual therapy approach. A group of 120 patients were randomly assigned to 7 weeks of individual manualized psychotherapy or therapeutic massage. At the end of treatment, patients who received meaning-centered psychotherapy showed improvement in both psychological-cluster symptoms (quality of life, spiritual well-being), as well as physical-cluster symptoms (physical symptom distress, number of physical symptoms).[44] A follow-up study randomly assigned 321 patients with advanced cancer to one of three arms: individual meaning-making psychotherapy, individual supportive psychotherapy, or enhanced usual care. After 8 weeks of treatment, patients receiving meaning-making psychotherapy showed significant improvements in the psychological-symptoms cluster, compared with those receiving enhanced usual care. They also had smaller but significant improvements in the physical-symptoms cluster, compared with those receiving supportive psychotherapy.[45]
Specific Evidence-Based Interventions
Managing Cancer and Living Meaningfully (CALM)
CALM is a brief (2–6 sessions), individual, manualized psychotherapy intervention that is designed to address the psychological symptom cluster in patients with advanced cancer. A randomized controlled trial of 305 patients were divided into CALM (n = 151) or usual care (n = 154) groups. At both the immediate and 6-month follow-up points, patients in the CALM group had fewer depressive symptoms, less end-of-life distress, and greater preparation for the end of life, compared with patients in the usual care group. When CALM outcomes were analyzed among patients with moderate anxiety about death, patients in the CALM group showed significantly greater spiritual well-being and lower levels of anxiety and demoralization at 6 months compared with patients in the usual care group. The brief, individual CALM intervention may be most useful for patients experiencing moderate anxiety about death and the psychological symptom cluster than for those with high or low anxiety about death.[46,47]
Cognitive behavioral therapy for insomnia (CBT-I)
CBT-I includes techniques such as stimulus control, sleep restriction, and relaxation training to address the cognitive and behavioral components that contribute to disrupted sleep. While CBT-I focuses on sleep, studies have shown that it has other psychological and physical impacts.[48] Studies of CBT-I in patients without cancer have found benefits with pain management, depression, and disability.[49]
A 2 x 2 randomized controlled trial of 67 cancer survivors assessed the effects of armodafinil and CBT-I on sleep quality, fatigue, and depression. Symptoms were assessed at three time points: before intervention, immediately after the 7-week intervention, and at the 3-month follow-up. Patients who received CBT-I had significantly improved sleep, fatigue, and depression levels, in addition to reduced hypnotic medication use, at both the post intervention and 3-month follow-up. Patients who received the pharmacological intervention experienced no changes to any of these variables. Path analysis showed that improvement in depressive symptoms was mediated by insomnia severity, suggesting that treatment of sleep disruptions with CBT-I can have a clinically meaningful effect on depressive symptoms.[3]
Studies of CBT-I in patients without cancer have found additional benefits for pain management, depression, and disability.[49] There is extremely limited data on the effect of CBT-I on pain outcomes in patients with cancer.
When patients with cancer are treated at the acute stage of insomnia, minimal and digital forms of CBT-I have also been found to be useful in randomized controlled trials. Minimal forms include psychoeducation booklets and three phone consultations with a sleep psychologist.[50] Digital forms include self-directed apps via computer or smartphone.[51] These studies have found an impact of CBT-I on sleep measures, as well as psychological-cluster symptoms (depression, anxiety, distress).
Psilocybin-assisted psychotherapy
A potential treatment to address the psychological and common symptom clusters is psilocybin-assisted psychotherapy. While more research is needed before it becomes an evidence-based practice, promising early research results have been disseminated widely on a number of news and blog sites, increasing patient interest in this approach to therapy.
In a double-blind randomized controlled trial, 29 patients with advanced cancer and related anxiety and depression received 7 weeks of psychotherapy and a single dose of either psilocybin or niacin. Patients who received the psilocybin plus psychotherapy showed significant reductions in the severity of symptoms in the psychological symptom cluster.[52] A follow-up study of patients who were still alive (n = 15) showed that these improvements were maintained for 3.2 to 4.5 years after the original study.[53] This emerging treatment continues to develop with wider groups of cancer patients and long-term assessments of multisymptom clusters.
References
Heckler CE, Garland SN, Peoples AR, et al.: Cognitive behavioral therapy for insomnia, but not armodafinil, improves fatigue in cancer survivors with insomnia: a randomized placebo-controlled trial. Support Care Cancer 24 (5): 2059-2066, 2016. [PUBMED Abstract]
Moss EL, Simpson JS, Pelletier G, et al.: An open-label study of the effects of bupropion SR on fatigue, depression and quality of life of mixed-site cancer patients and their partners. Psychooncology 15 (3): 259-67, 2006. [PUBMED Abstract]
Peoples AR, Garland SN, Pigeon WR, et al.: Cognitive Behavioral Therapy for Insomnia Reduces Depression in Cancer Survivors. J Clin Sleep Med 15 (1): 129-137, 2019. [PUBMED Abstract]
Roscoe JA, Garland SN, Heckler CE, et al.: Randomized placebo-controlled trial of cognitive behavioral therapy and armodafinil for insomnia after cancer treatment. J Clin Oncol 33 (2): 165-71, 2015. [PUBMED Abstract]
Jarden M, Nelausen K, Hovgaard D, et al.: The effect of a multimodal intervention on treatment-related symptoms in patients undergoing hematopoietic stem cell transplantation: a randomized controlled trial. J Pain Symptom Manage 38 (2): 174-90, 2009. [PUBMED Abstract]
Song SY, Ko YB, Kim H, et al.: Effect of serotonin-norepinephrine reuptake inhibitors for patients with chemotherapy-induced painful peripheral neuropathy: A meta-analysis. Medicine (Baltimore) 99 (1): e18653, 2020. [PUBMED Abstract]
Ramaswami R, Villarreal MD, Pitta DM, et al.: Venlafaxine in management of hot flashes in women with breast cancer: a systematic review and meta-analysis. Breast Cancer Res Treat 152 (2): 231-7, 2015. [PUBMED Abstract]
Caspersen CJ, Powell KE, Christenson GM: Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep 100 (2): 126-31, 1985. [PUBMED Abstract]
2018 Physical Activity Guidelines Scientific Committee: 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, 2018. Available online.
Schmitz KH, Courneya KS, Matthews C, et al.: American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 42 (7): 1409-26, 2010. [PUBMED Abstract]
Campbell KL, Winters-Stone KM, Wiskemann J, et al.: Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med Sci Sports Exerc 51 (11): 2375-2390, 2019. [PUBMED Abstract]
Zhi WI, Baser RE, Zhi LM, et al.: Yoga for cancer survivors with chemotherapy-induced peripheral neuropathy: Health-related quality of life outcomes. Cancer Med 10 (16): 5456-5465, 2021. [PUBMED Abstract]
Carson JW, Carson KM, Porter LS, et al.: Yoga of Awareness program for menopausal symptoms in breast cancer survivors: results from a randomized trial. Support Care Cancer 17 (10): 1301-9, 2009. [PUBMED Abstract]
Cho MH, Dodd MJ, Cooper BA, et al.: Comparisons of exercise dose and symptom severity between exercisers and nonexercisers in women during and after cancer treatment. J Pain Symptom Manage 43 (5): 842-54, 2012. [PUBMED Abstract]
Dodd MJ, Cho MH, Miaskowski C, et al.: A randomized controlled trial of home-based exercise for cancer-related fatigue in women during and after chemotherapy with or without radiation therapy. Cancer Nurs 33 (4): 245-57, 2010. [PUBMED Abstract]
Henderson VP, Massion AO, Clemow L, et al.: A randomized controlled trial of mindfulness-based stress reduction for women with early-stage breast cancer receiving radiotherapy. Integr Cancer Ther 12 (5): 404-13, 2013. [PUBMED Abstract]
Hoffman CJ, Ersser SJ, Hopkinson JB, et al.: Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: a randomized, controlled trial. J Clin Oncol 30 (12): 1335-42, 2012. [PUBMED Abstract]
Johns SA, Brown LF, Beck-Coon K, et al.: Randomized controlled pilot study of mindfulness-based stress reduction for persistently fatigued cancer survivors. Psychooncology 24 (8): 885-93, 2015. [PUBMED Abstract]
Lengacher CA, Johnson-Mallard V, Post-White J, et al.: Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psychooncology 18 (12): 1261-72, 2009. [PUBMED Abstract]
Liu W, Liu J, Ma L, et al.: Effect of mindfulness yoga on anxiety and depression in early breast cancer patients received adjuvant chemotherapy: a randomized clinical trial. J Cancer Res Clin Oncol 148 (9): 2549-2560, 2022. [PUBMED Abstract]
Park S, Sato Y, Takita Y, et al.: Mindfulness-Based Cognitive Therapy for Psychological Distress, Fear of Cancer Recurrence, Fatigue, Spiritual Well-Being, and Quality of Life in Patients With Breast Cancer-A Randomized Controlled Trial. J Pain Symptom Manage 60 (2): 381-389, 2020. [PUBMED Abstract]
Shao D, Zhang H, Cui N, et al.: The efficacy and mechanisms of a guided self-help intervention based on mindfulness in patients with breast cancer: A randomized controlled trial. Cancer 127 (9): 1377-1386, 2021. [PUBMED Abstract]
Sheikhzadeh M, Zanjani Z, Baari A: Efficacy of Mindfulness-Based Cognitive Therapy and Cognitive Behavioral Therapy for Anxiety, Depression, and Fatigue in Cancer Patients: A Randomized Clinical Trial. Iran J Psychiatry 16 (3): 271-280, 2021. [PUBMED Abstract]
Würtzen H, Dalton SO, Elsass P, et al.: Mindfulness significantly reduces self-reported levels of anxiety and depression: results of a randomised controlled trial among 336 Danish women treated for stage I-III breast cancer. Eur J Cancer 49 (6): 1365-73, 2013. [PUBMED Abstract]
Yıldırım D, Çiriş Yıldız C: The Effect of Mindfulness-Based Breathing and Music Therapy Practice on Nurses’ Stress, Work-Related Strain, and Psychological Well-being During the COVID-19 Pandemic: A Randomized Controlled Trial. Holist Nurs Pract 36 (3): 156-165, 2022 May-Jun 01. [PUBMED Abstract]
Gok Metin Z, Karadas C, Izgu N, et al.: Effects of progressive muscle relaxation and mindfulness meditation on fatigue, coping styles, and quality of life in early breast cancer patients: An assessor blinded, three-arm, randomized controlled trial. Eur J Oncol Nurs 42: 116-125, 2019. [PUBMED Abstract]
Salvador C, Mark P, Hoenemeyer T, et al.: Prospective feasibility study of a mindfulness-based program for breast cancer patients in the southeastern US. Complement Ther Clin Pract 49: 101639, 2022. [PUBMED Abstract]
Tan SB, Chee CH, Ngai CF, et al.: Mindfulness-based supportive therapy on reducing suffering in patients with advanced cancer: randomised controlled trial. BMJ Support Palliat Care 13 (e3): e1117-e1125, 2024. [PUBMED Abstract]
Marzorati C, Riva S, Pravettoni G: Who Is a Cancer Survivor? A Systematic Review of Published Definitions. J Cancer Educ 32 (2): 228-237, 2017. [PUBMED Abstract]
Calvo-Schimmel A, Paul SM, Cooper BA, et al.: Oncology Outpatients With Worse Anxiety and Sleep Disturbance Profiles Are at Increased Risk for a Higher Symptom Burden and Poorer Quality of Life. Cancer Nurs 46 (6): 417-431, 2023 Nov-Dec 01. [PUBMED Abstract]
Bonhof CS, van de Poll-Franse LV, Vissers PAJ, et al.: Anxiety and depression mediate the association between chemotherapy-induced peripheral neuropathy and fatigue: Results from the population-based PROFILES registry. Psychooncology 28 (9): 1926-1933, 2019. [PUBMED Abstract]
Kwekkeboom KL, Abbott-Anderson K, Wanta B: Feasibility of a patient-controlled cognitive-behavioral intervention for pain, fatigue, and sleep disturbance in cancer. Oncol Nurs Forum 37 (3): E151-9, 2010. [PUBMED Abstract]
Dalton JA, Keefe FJ, Carlson J, et al.: Tailoring cognitive-behavioral treatment for cancer pain. Pain Manag Nurs 5 (1): 3-18, 2004. [PUBMED Abstract]
Kwekkeboom KL, Abbott-Anderson K, Cherwin C, et al.: Pilot randomized controlled trial of a patient-controlled cognitive-behavioral intervention for the pain, fatigue, and sleep disturbance symptom cluster in cancer. J Pain Symptom Manage 44 (6): 810-22, 2012. [PUBMED Abstract]
Zhao C, Lai L, Zhang L, et al.: The effects of acceptance and commitment therapy on the psychological and physical outcomes among cancer patients: A meta-analysis with trial sequential analysis. J Psychosom Res 140: 110304, 2021. [PUBMED Abstract]
Najvani BD, Neshatdoost HT, Abedi MR: The effect of acceptance and commitment therapy on depression and psychological flexibility in women with breast cancer. Zahedan J Res Med Sci. 17 (4): e965, 2015. Available online.
Montazer A, Nemati F, Dehghani F: Efficacy of acceptance and commitment therapy on breast cancer female patients’ hope. Iranian Journal of Cancer Prevention. 10 (2): e5526, 2017. Available online.
Mosher CE, Secinti E, Li R, et al.: Acceptance and commitment therapy for symptom interference in metastatic breast cancer patients: a pilot randomized trial. Support Care Cancer 26 (6): 1993-2004, 2018. [PUBMED Abstract]
Rost AD, Wilson K, Buchanan E: Improving psychological adjustment among late-stage ovarian cancer patients: examining the role of avoidance in treatment. Cognitive and Behavioral Practice. 19 (4): 508-17, 2012. Available online.
van der Spek N, Vos J, van Uden-Kraan CF, et al.: Meaning making in cancer survivors: a focus group study. PLoS One 8 (9): e76089, 2013. [PUBMED Abstract]
Breitbart W, Rosenfeld B, Gibson C, et al.: Meaning-centered group psychotherapy for patients with advanced cancer: a pilot randomized controlled trial. Psychooncology 19 (1): 21-8, 2010. [PUBMED Abstract]
Breitbart W, Rosenfeld B, Pessin H, et al.: Meaning-centered group psychotherapy: an effective intervention for improving psychological well-being in patients with advanced cancer. J Clin Oncol 33 (7): 749-54, 2015. [PUBMED Abstract]
Breitbart W, Poppito S, Rosenfeld B, et al.: Pilot randomized controlled trial of individual meaning-centered psychotherapy for patients with advanced cancer. J Clin Oncol 30 (12): 1304-9, 2012. [PUBMED Abstract]
Breitbart W, Pessin H, Rosenfeld B, et al.: Individual meaning-centered psychotherapy for the treatment of psychological and existential distress: A randomized controlled trial in patients with advanced cancer. Cancer 124 (15): 3231-3239, 2018. [PUBMED Abstract]
Lo C, Hales S, Jung J, et al.: Managing Cancer And Living Meaningfully (CALM): phase 2 trial of a brief individual psychotherapy for patients with advanced cancer. Palliat Med 28 (3): 234-42, 2014. [PUBMED Abstract]
Rodin G, Lo C, Rydall A, et al.: Managing Cancer and Living Meaningfully (CALM): A Randomized Controlled Trial of a Psychological Intervention for Patients With Advanced Cancer. J Clin Oncol 36 (23): 2422-2432, 2018. [PUBMED Abstract]
Matthews EE, Berger AM, Schmiege SJ, et al.: Cognitive behavioral therapy for insomnia outcomes in women after primary breast cancer treatment: a randomized, controlled trial. Oncol Nurs Forum 41 (3): 241-53, 2014. [PUBMED Abstract]
Enomoto K, Adachi T, Fujino H, et al.: Comparison of the effectiveness of cognitive behavioral therapy for insomnia, cognitive behavioral therapy for pain, and hybrid cognitive behavioral therapy for insomnia and pain in individuals with comorbid insomnia and chronic pain: A systematic review and network meta-analysis. Sleep Med Rev 66: 101693, 2022. [PUBMED Abstract]
Casault L, Savard J, Ivers H, et al.: A randomized-controlled trial of an early minimal cognitive-behavioural therapy for insomnia comorbid with cancer. Behav Res Ther 67: 45-54, 2015. [PUBMED Abstract]
Ritterband LM, Bailey ET, Thorndike FP, et al.: Initial evaluation of an Internet intervention to improve the sleep of cancer survivors with insomnia. Psychooncology 21 (7): 695-705, 2012. [PUBMED Abstract]
Ross S, Bossis A, Guss J, et al.: Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. J Psychopharmacol 30 (12): 1165-1180, 2016. [PUBMED Abstract]
Agin-Liebes GI, Malone T, Yalch MM, et al.: Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. J Psychopharmacol 34 (2): 155-166, 2020. [PUBMED Abstract]
Latest Updates to This Summary (07/11/2024)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the identification and management of symptom clusters. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Symptom Clusters in Cancer are:
Marilyn J. Hammer, PhD, DC, RN, FAAN (Dana-Farber Cancer Institute)
Jayesh Kamath, MD, PhD (University of Connecticut Health Center)
Edward B. Perry, MD (VA Connecticut Healthcare System)
Rachel A. Pozzar, PhD, RN (Dana-Farber Cancer Institute)
Diane Von Ah, PhD, RN, FAAN (The Ohio State University)
Amy Wachholtz, PhD, MDiv, MS, ABPP (University of Colorado)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Symptom Clusters in Cancer. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/cancer-symptom-clusters-hp-pdq. Accessed <MM/DD/YYYY>.
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Cancer-related fatigue (CRF) is a distressing, persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with usual functioning.[1] Fatigue is the most common side effect of cancer treatment with chemotherapy, radiation therapy, bone marrow transplantation, or selected biologic response modifiers.[2] Clinically significant levels of fatigue may also negatively impact survival.[3][Level of evidence: III] The specific mechanisms underlying a common pathophysiology for CRF are unknown.
Cancer treatment–related fatigue is a commonly reported symptom, with 80% of patients reporting fatigue while receiving chemotherapy or radiation therapy.[4] The condition generally improves after therapy is completed, but some level of fatigue may persist for months or years after treatment. For a subset of patients, fatigue may be a significant issue long into survivorship.[5,6] For example, a longitudinal study assessed fatigue in individuals with stage I to stage III breast cancer over three time points postdiagnosis (1 year, n = 5,640; 2 years, n = 5,000; 4 years, n = 3,400). The study found that over 30% of patients at each time point experienced severe global fatigue.[7][Level of evidence: III] Physical fatigue (35%) occurred more often than emotional fatigue (25%) or cognitive fatigue (13%).[8] Fatigue is also seen as a presenting symptom in cancers that cause complications such as anemia, endocrine dysfunction, neuromuscular complications, psychological distress, and end-organ dysfunction (e.g., renal, pulmonary, or cardiac dysfunction). Fatigue is common in people with advanced cancer who are not undergoing active cancer treatment. Cancer treatment–related fatigue has been reported in 39% to more than 90% of patients undergoing cancer treatment [9–13] and in 19% to 82% of patients posttreatment.[4,14]
Fatigue experienced as a side effect of cancer treatment is differentiated from fatigue experienced by healthy people in their daily lives. Healthy fatigue is frequently described as acute fatigue that is eventually relieved by sleep and rest; cancer treatment–related fatigue is categorized as chronic fatigue because it is present over a long period of time, interferes with functioning, and is not completely relieved by sleep and rest.[15] Also, the level of CRF is often disproportionate to the level of activity or energy exerted.[15] Although the label chronic fatigue is accurate, it does not mean that people with cancer who experience fatigue have chronic fatigue syndrome. Using this phrase can be confusing to both patients and health professionals. Terms such as cancer fatigue, cancer-related fatigue, and cancer treatment–related fatigue have all been used in the clinical literature, research literature, and educational materials for patients and the public.
Fatigue, like pain, is a self-perceived state and patient-reported outcome. Patients may describe fatigue as feeling:[16]
Tired.
Weak.
Exhausted.
Lazy.
Weary.
Worn-out.
Heavy.
Slow.
Like they have no energy or get-up-and-go.
Health professionals have included fatigue within concepts such as:
Asthenia.
Lassitude.
Malaise.
Prostration.
Exercise intolerance.
Lack of energy.
Weakness.
Studies of women with breast cancer have attempted to define specific fatigue trajectories. For example, some patients experience a high degree of fatigue during treatment and recovery, while others deteriorate over time. In contrast, some patients suffer from little fatigue throughout treatment. Suggested fatigue trajectories include the following:[8,17]
Very low fatigue.
Low fatigue.
Late or deteriorating fatigue (initially low symptoms that increase over time).
Recovery (initially high symptoms that decrease over time).
High fatigue.
Research on fatigue in people with cancer has included primarily self-reports of fatigue, with increasing data exploring biological or physiological correlates. Such correlates have included measures of muscle weakness, maximal oxygen uptake, cytokines, cortisol, and genetic biomarkers.[10]
Fatigue has a negative impact on all areas of function, including the following:[18–21]
Activities of daily living in older cancer survivors.[23]
The pattern of fatigue associated with cancer treatment varies according to the type and schedule of treatment. For example, people treated with cyclic chemotherapy regimens generally exhibit peak fatigue in the days following treatment, then lower levels of fatigue until the next treatment. However, patients undergoing external-beam radiation therapy report gradually increasing fatigue over the course of therapy of the largest treatment field. Few studies of people undergoing cancer treatment have addressed the issue of fatigue as a result of the emotional distress associated with undergoing a diagnostic evaluation for cancer and the effects of medical and surgical procedures used for evaluation and for initial treatment. Because most adults enter the cancer care system following at least one surgical procedure, and because surgery and emotional distress are both associated with fatigue, it is likely that most people beginning nonsurgical treatment are experiencing fatigue at the beginning of treatment.[21,24]
Fatigue management focuses on identifying and treating the underlying factors that may be contributing to fatigue. Most clinical recommendations for managing the symptoms of fatigue caused by something other than chemotherapy-induced anemia rely on careful development of clinical hypotheses, as outlined in the National Comprehensive Cancer Network (NCCN) guidelines on fatigue.[1] NCCN category 1 interventions for CRF include the following:
For more information, see the Interventions section.
Although much progress has been made, further research is needed to better define fatigue and its trajectory, understand its physiology, and determine the best ways to prevent and treat it.
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
References
National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Cancer-Related Fatigue. Version 2.2024. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2024. Available online with registration. Last accessed July 17, 2024.
Prue G, Rankin J, Allen J, et al.: Cancer-related fatigue: A critical appraisal. Eur J Cancer 42 (7): 846-63, 2006. [PUBMED Abstract]
Mo J, Darke AK, Guthrie KA, et al.: Association of Fatigue and Outcomes in Advanced Cancer: An Analysis of Four SWOG Treatment Trials. JCO Oncol Pract 17 (8): e1246-e1257, 2021. [PUBMED Abstract]
Aapro M, Scotte F, Bouillet T, et al.: A Practical Approach to Fatigue Management in Colorectal Cancer. Clin Colorectal Cancer 16 (4): 275-285, 2017. [PUBMED Abstract]
Henry DH, Viswanathan HN, Elkin EP, et al.: Symptoms and treatment burden associated with cancer treatment: results from a cross-sectional national survey in the U.S. Support Care Cancer 16 (7): 791-801, 2008. [PUBMED Abstract]
Bower JE, Ganz PA, Desmond KA, et al.: Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer 106 (4): 751-8, 2006. [PUBMED Abstract]
Di Meglio A, Havas J, Soldato D, et al.: Development and Validation of a Predictive Model of Severe Fatigue After Breast Cancer Diagnosis: Toward a Personalized Framework in Survivorship Care. J Clin Oncol 40 (10): 1111-1123, 2022. [PUBMED Abstract]
Vaz-Luis I, Di Meglio A, Havas J, et al.: Long-Term Longitudinal Patterns of Patient-Reported Fatigue After Breast Cancer: A Group-Based Trajectory Analysis. J Clin Oncol 40 (19): 2148-2162, 2022. [PUBMED Abstract]
Fosså SD, Dahl AA, Loge JH: Fatigue, anxiety, and depression in long-term survivors of testicular cancer. J Clin Oncol 21 (7): 1249-54, 2003. [PUBMED Abstract]
Saligan LN, Olson K, Filler K, et al.: The biology of cancer-related fatigue: a review of the literature. Support Care Cancer 23 (8): 2461-78, 2015. [PUBMED Abstract]
Detmar SB, Aaronson NK, Wever LD, et al.: How are you feeling? Who wants to know? Patients’ and oncologists’ preferences for discussing health-related quality-of-life issues. J Clin Oncol 18 (18): 3295-301, 2000. [PUBMED Abstract]
Costantini M, Mencaglia E, Giulio PD, et al.: Cancer patients as ‘experts’ in defining quality of life domains. A multicentre survey by the Italian Group for the Evaluation of Outcomes in Oncology (IGEO). Qual Life Res 9 (2): 151-9, 2000. [PUBMED Abstract]
Cella D, Lai JS, Chang CH, et al.: Fatigue in cancer patients compared with fatigue in the general United States population. Cancer 94 (2): 528-38, 2002. [PUBMED Abstract]
Stone PC, Minton O: Cancer-related fatigue. Eur J Cancer 44 (8): 1097-104, 2008. [PUBMED Abstract]
Barsevick AM, Whitmer K, Walker L: In their own words: using the common sense model to analyze patient descriptions of cancer-related fatigue. Oncol Nurs Forum 28 (9): 1363-9, 2001. [PUBMED Abstract]
Bower JE, Wiley J, Petersen L, et al.: Fatigue after breast cancer treatment: Biobehavioral predictors of fatigue trajectories. Health Psychol 37 (11): 1025-1034, 2018. [PUBMED Abstract]
Glaus A: Assessment of fatigue in cancer and non-cancer patients and in healthy individuals. Support Care Cancer 1 (6): 305-15, 1993. [PUBMED Abstract]
Given B, Given CW, McCorkle R, et al.: Pain and fatigue management: results of a nursing randomized clinical trial. Oncol Nurs Forum 29 (6): 949-56, 2002. [PUBMED Abstract]
Curt GA: The impact of fatigue on patients with cancer: overview of FATIGUE 1 and 2. Oncologist 5 (Suppl 2): 9-12, 2000. [PUBMED Abstract]
Passik SD, Kirsh KL: A pilot examination of the impact of cancer patients’ fatigue on their spousal caregivers. Palliat Support Care 3 (4): 273-9, 2005. [PUBMED Abstract]
Rao AV, Cohen HJ: Fatigue in older cancer patients: etiology, assessment, and treatment. Semin Oncol 35 (6): 633-42, 2008. [PUBMED Abstract]
Ancoli-Israel S, Liu L, Marler MR, et al.: Fatigue, sleep, and circadian rhythms prior to chemotherapy for breast cancer. Support Care Cancer 14 (3): 201-9, 2006. [PUBMED Abstract]
Pathogenesis of Fatigue
Except for chemotherapy-induced anemia, the mechanisms responsible for fatigue in people with cancer are not known. Understanding the causes of fatigue in people with cancer is especially challenging because each individual may experience multiple possible causes of fatigue simultaneously. Multiple underlying etiological factors beyond the type and treatment of cancer have been proposed, including psychological distress, life demands, sleep disturbance, neurophysiological changes, disruption of circadian rhythms, cardiac issues, neuroimmunological changes, and genetic variations.[1]
Growing evidence, particularly for women with breast cancer and men with prostate cancer, suggests that fatigue is associated with markers of increased immune inflammatory activity. When fatigued individuals with a history of breast cancer are compared with breast cancer survivors without fatigue, different patterns emerge with respect to interleukin-6, interleukin-1 receptor antagonist, C-reactive protein, neopterin, and soluble tumor necrosis factor receptor-II.[2–5] Although the precise relationships—and the clinical meaning of those relationships—are not yet known, increased cytokines likely contribute to the symptoms of asthenia, fatigue, and lethargy. However, so far no large, well-controlled studies have evaluated the effects of general anti-inflammatory agents on fatigue or cytokine biomarkers.
Other studies demonstrate a change in the regulation of cortisol by the hypothalamic pituitary adrenal axis. One key study put fatigued and nonfatigued breast cancer survivors through a stress battery in a laboratory setting. Nonfatigued survivors mounted a significant cortisol increase in response to acute stress, while fatigued survivors had a very blunted response.[6] Another study has shown that fatigued breast cancer survivors have flattened cortisol slopes, having higher levels of cortisol at the end of the day than do nonfatigued survivors.[7] It is the dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis that may account for the prolonged inflammatory cytokine milieu. Understanding the body’s response to numerous chronic stressors in cancer may help in managing fatigue.
Finally, another theory is that chronic exposure to proinflammatory cytokines negatively impacts serotonin levels. One hypothesis is that the relationship between central nervous system concentrations of serotonin and fatigue have a U-shaped relationship, suggesting that very high and very low levels of serotonin may be associated with cancer-related fatigue.[8] However, studies that have evaluated serotonergic agents have not demonstrated a benefit for fatigue.[9] The role and relationship of many important neurotransmitters such as dopamine, norepinephrine, and serotonin with HPA axis functioning and cytokine expression have yet to be fully understood.
Bower JE, Ganz PA, Aziz N, et al.: Fatigue and proinflammatory cytokine activity in breast cancer survivors. Psychosom Med 64 (4): 604-11, 2002 Jul-Aug. [PUBMED Abstract]
Evans WJ, Lambert CP: Physiological basis of fatigue. Am J Phys Med Rehabil 86 (1 Suppl): S29-46, 2007. [PUBMED Abstract]
Bower JE, Ganz PA, Tao ML, et al.: Inflammatory biomarkers and fatigue during radiation therapy for breast and prostate cancer. Clin Cancer Res 15 (17): 5534-40, 2009. [PUBMED Abstract]
Bower JE, Wiley J, Petersen L, et al.: Fatigue after breast cancer treatment: Biobehavioral predictors of fatigue trajectories. Health Psychol 37 (11): 1025-1034, 2018. [PUBMED Abstract]
Bower JE, Ganz PA, Aziz N: Altered cortisol response to psychologic stress in breast cancer survivors with persistent fatigue. Psychosom Med 67 (2): 277-80, 2005 Mar-Apr. [PUBMED Abstract]
Bower JE, Ganz PA, Dickerson SS, et al.: Diurnal cortisol rhythm and fatigue in breast cancer survivors. Psychoneuroendocrinology 30 (1): 92-100, 2005. [PUBMED Abstract]
Jager A, Sleijfer S, van der Rijt CC: The pathogenesis of cancer related fatigue: could increased activity of pro-inflammatory cytokines be the common denominator? Eur J Cancer 44 (2): 175-81, 2008. [PUBMED Abstract]
Morrow GR, Andrews PL, Hickok JT, et al.: Fatigue associated with cancer and its treatment. Support Care Cancer 10 (5): 389-98, 2002. [PUBMED Abstract]
Contributing Factors
Although fatigue is clearly prevalent in patients with cancer, it has been difficult to identify consistent correlates of fatigue in this population. The factors most often implicated include the following:[1,2]
Fatigue has also been identified as a common symptom in symptom clusters associated with cancer, e.g., fatigue-pain and fatigue-cognitive clusters. For more information, see Symptom Clusters in Cancer.
Cancer Treatment
The association of fatigue with the major cancer treatment modalities of surgery, chemotherapy, radiation therapy, endocrine therapy, and biologic response modifier therapy caused speculation that fatigue resulted from tissue damage or accumulation of the products of cell death. Interest in the effects of cancer treatment on the production of proinflammatory cytokines is based on recognition of the strong fatigue-inducing effect of some biologic response modifiers such as interferon-alpha and the finding of elevated levels of proinflammatory cytokines in people experiencing persistent fatigue after cancer treatment.[9,10] In longitudinal studies of patients undergoing radiation therapy, polymorphisms in tumor necrosis factor-alpha and interleukin-6 were associated with elevated fatigue before, during, and for 4 months after completion of treatment.[11,12]
Many people with cancer undergo surgery for diagnosis or treatment. Despite the high incidence of postoperative fatigue observed in these patients in clinical practice, few investigators have examined its causes and correlates. It is clear, however, that fatigue postsurgery improves with time and is compounded by fatigue caused by other cancer treatments.[13,14]
Fatigue has long been associated with radiation exposure and is reportedly one of the most common and activity-limiting side effects of radiation therapy for cancer.[15,16] Up to 90% of patients undergoing radiation therapy experience fatigue during the course of their treatment.[17] Most of the research describing the fatigue trajectory during radiation therapy has been conducted in women with breast cancer and men with prostate cancer.[3,18]
Fatigue increases throughout radiation therapy, peaking around mid-course and remaining at this level until radiation therapy is completed. It then improves somewhat during the 2 months after treatment ends. A study that investigated the trajectory of fatigue in men who were undergoing radiation therapy for prostate cancer (N = 82) found significant interindividual variability.[3] The authors used hierarchical linear modeling, a highly sophisticated analytical method, to identify predictors for prolonged fatigue trajectories. Younger men with high levels of fatigue at the initiation of radiation therapy were at increased risk of developing higher levels of morning and evening fatigue during radiation therapy. In addition, the level of depression at the initiation of radiation therapy predicted the level of morning fatigue during radiation therapy.[3]
A second study of 73 women who were undergoing adjuvant radiation therapy for breast cancer found similar differences in the patterns and predictors of morning versus evening fatigue.[7] Participants were recruited to the study at their simulation visits and completed baseline questionnaires. Data were then collected on 2 subsequent days, in the morning and at bedtime, each week during radiation therapy; every 2 weeks for 2 months after radiation therapy; and once a month for 2 additional months thereafter. Fatigue was measured with the Lee Fatigue Scale. For the group as a whole, over the 25 weeks of data collection, morning fatigue decreased slightly during radiation therapy and was constant for 4 months afterwards, while evening fatigue increased through radiation therapy and then declined slightly after treatment. Evening fatigue was higher for those who:
Were working.
Had children at home.
Had higher depression scores.
Morning fatigue was higher for those who:
Had more trait anxiety.
Were experiencing sleep disturbance.
Were younger.
Had lower body mass indices.
Advanced disease and comorbidities also added to the severity of morning fatigue.[7][Level of evidence: III]
Several research studies document a fatigue syndrome that is not specific to disease type or radiation site and that demonstrates a gradual decline in fatigue in the patient after treatment is completed.[19,20] Some of these studies suggest, however, that not all patients return to pretreatment energy levels. Risk factors for persistent low energy in cancer patients include pretreatment fatigue, psychological distress, high BMI, tumor location, advanced disease, and combination-modality therapy.[8,14,21]
Fatigue is a dose-limiting toxicity of treatment with a variety of biotherapeutic agents. Biotherapy exposes patients with cancer to exogenous and endogenous cytokines.[22] Biotherapy-related fatigue usually occurs as part of a constellation of symptoms called flulike syndrome.
Mental fatigue and cognitive deficits have also been identified as biotherapy side effects. The type of biotherapeutic agent used may influence the type and pattern of fatigue.[23,24]
Treatment with chemotherapy is a predictor of fatigue and can be exacerbated by the coexistence of pain, depression, and/or anxiety.[25][Level of evidence: II]; [26] A longitudinal, descriptive study reported the highest levels of fatigue at the midpoint of a patient’s chemotherapy cycles, with fatigue improving after treatment but not quite returning to baseline levels 30 days after the last treatment.[25] In another longitudinal study of women with stage 0 to stage II breast cancer who received chemotherapy with or without radiation therapy (n = 103) versus radiation therapy alone (n = 102) versus a control group (n = 193),[27] increases in fatigue were demonstrated 3 years posttreatment for the group that received chemotherapy with or without radiation therapy, compared with the two other groups. Mean scores for fatigue severity measured by the Fatigue Symptom Inventory (range, 0–10) increased over the 3 years.
A longitudinal, descriptive study of 78 women with gynecological cancer examined the daily and intraday changes and interrelationships among fatigue, depression, and disruptions in sleep and activity, before and after each individual chemotherapy treatment, for three treatments. Significant changes in symptoms were noted over time. Before infusions, fatigue was associated with depression; after infusions, fatigue was significantly associated with increased depression and sleep/wake irregularities (increases in minutes awake at night and decreases in daytime activity and sleep/wake activity).[28]
Aromatase inhibitors—the recommended first-line adjuvant endocrine therapy in postmenopausal women with hormone receptor–positive breast cancer—have been linked to cancer-related fatigue (CRF). In one study of survivors of stage 0 to III breast cancer who were receiving adjuvant aromatase inhibitor therapy at an outpatient breast oncology clinic, 616 of 1,103 participants (55.8%) had moderate to severe CRF.[29] In addition, breast cancer survivors who were younger (age ≤55 years), were college educated, had higher body mass indices, and reported more pain and insomnia were more likely to have moderate to severe CRF than were their counterparts.
Treatment with immune checkpoint inhibitors has been associated with clinically significant fatigue. Reviews of outcomes data demonstrated that fatigue is the most common adverse event incorporating anti–programmed death 1 (PD-1)/programmed death-ligand 1 (PD-L1) agents. In the first phase I studies of nivolumab, 16% to 24% of patients had treatment-related fatigue, and 1% to 2% had grade 3 or 4 severity. Single-agent immune checkpoint studies have reported an incidence of 16% to 37% with anti–PD-1 agents, and 12% to 24% with anti–PD-L1 agents. Clinical studies that combined anti–PD-1/PD-L1 agents with other immune checkpoint inhibitors reported even higher rates of fatigue, in up to 71% of patients. The specific mechanism by which immune checkpoint inhibitors cause fatigue is not known; however, when fatigue symptoms occur during treatment, clinicians should be vigilant in assessing for early symptoms of endocrine dysfunction, such as hypothyroidism.[30–33]
Anemia
Evidence suggests that anemia may be a major factor in CRF and quality of life in cancer patients.[34–36] Anemia can be related to the disease itself or caused by therapy. Occasionally, anemia is simply a co-occurring medical finding that is related to neither disease nor therapy. Anemia is often a significant contributor to symptoms in people with cancer. For individual patients, it can be difficult to discern the actual impact of anemia because there are often other problems that confound the ability to weigh the specific impact of anemia.[37]
A retrospective review was conducted to understand anemia in patients undergoing radiation therapy. Anemia was found in 48% of the patients initially and increased to 57% during therapy. It was more common in women than in men (64% vs. 51%); however, men with prostate cancer experienced the greatest increase in anemia during radiation therapy.[38] In certain cancers, such as cancer of the cervix and cancer of the head and neck, anemia has been found to predict poor survival and diminished quality of life in patients undergoing radiation therapy.[39–41]
Nutrition Factors
Fatigue often occurs when the body’s energy requirements exceed the supply of energy sources. In people with cancer, three major mechanisms may be involved:
Alteration in the body’s ability to process nutrients efficiently.
Increase in the body’s energy requirements.
Decrease in intake of energy sources.
Causes of nutritional alterations are listed in Table 1.
Table 1. Nutrition/Energy Factors in Cancer
Mechanisms
Causes
Altered ability to process nutrients
Impaired glucose, lipid, and protein metabolism
Increased energy requirements
Tumor consumption of and competition for nutrients
Hypermetabolic state due to tumor growth
Infection/fever
Dyspnea
Decreased intake of energy sources
Anorexia
Nausea/vomiting
Diarrhea
Bowel obstruction
A randomized controlled trial compared a plant-based, high-protein diet to usual care in 103 patients with newly diagnosed breast cancer who were undergoing adjuvant chemotherapy.[42][Level of evidence: I] Patients were assessed over three time points (T0: baseline, T1: end of third chemotherapy infusion, T2: 3 weeks after last treatment). Fatigue was measured using the Fatigue Symptom Inventory, which has a clinically meaningful fatigue level threshold of more than 3. Patients in the control group (n = 51) had an increase in mean fatigue score from 4.2 + 1.64 to 5.37 + 1.87, while patients in the intervention group (n = 52) had a decrease in mean fatigue score from 4.2 + 1.94 to 2.47 + 1.31 (P < .001). Of note, the intervention group’s fatigue level decreased to below a clinically meaningful level between T0 and T2, while the control group’s fatigue level stayed above the clinically meaningful threshold and slightly worsened. In addition, while both groups had a decrease in BMI (intervention group, 0.7 + 0.8 kg/m2; control group, 0.4 + 1.3 kg/m2), the control group had a decrease in muscle mass, and the intervention group had an increase in muscle mass and a decrease in fat mass (P < .001). A plant-based, high protein diet may be an effective approach to fatigue management.
Psychological Factors
Numerous factors related to the moods, beliefs, attitudes, and reactions to stressors of people with cancer can also contribute to the development of chronic fatigue. Anxiety and depression are the most common comorbid psychiatric disorders of CRF.[43][Level of evidence: II] Often, fatigue is the final common pathway for a range of physical and emotional etiologies.
Depression can be a comorbid, disabling syndrome that affects approximately 15% to 25% of people with cancer.[28,44] Multiple studies show that pretreatment depression increases fatigue during and after cancer treatment.[9,45,46] The presence of depression—manifested by loss of interest in normal activities, difficulty concentrating, lethargy, and feelings of hopelessness—can compound the physical causes of fatigue in these individuals and persist long past the time when physical causes have resolved.[47] A history of stressful experiences in childhood, including abuse and neglect, has also been associated with higher levels of fatigue in breast cancer survivors.[48]
The anxiety and fear associated with a cancer diagnosis—and the impact of that diagnosis on a person’s physical, psychosocial, and financial well-being—are sources of emotional stress. Distress associated with the cancer diagnosis alone may trigger fatigue. A study of 74 early-stage breast cancer patients with no history of affective disorder assessed various symptoms of adjustment approximately 2 weeks after diagnosis. About 45% of participants noted moderate or high levels of fatigue. This fatigue may have been secondary to the increased cognitive strain of dealing with the diagnosis or to insomnia, reported as moderate to severe by about 60% of patients. Therefore, fatigue may begin before treatment as a result of worry or other cognitive factors, both primary and secondary to insomnia. Various forms of treatment may compound this fatigue.[49]
In cancer survivors, fatigue may also be above levels seen in the general population.[50,51] A Brazilian study found that in patients who had advanced cancer but were not undergoing therapy, those with anxiety and depression had higher fatigue levels.[51] A Dutch study found a correlation between anxiety, depression, and CRF.[52] Despite psychological care, those with poorer physical health and mood disturbances reported more fatigue. For more information, see Depression and Adjustment to Cancer: Anxiety and Distress.
Psychological and symptom distress have also been found to be significant predictors of fatigue.[53,54] In a study of 101 women about to undergo surgery for breast cancer, younger age, presurgery distress, and expectations about fatigue significantly predicted fatigue levels 1 week after surgery. In the regression model, age, distress, and expectancy each uniquely contributed to fatigue, with distress and expectancy accounting for 25% of the variance.[53][Level of evidence: III] In a longitudinal study with women who had gynecological cancer, symptom and psychological distress significantly predicted fatigue before, during, and after treatment with chemotherapy, explaining up to 80% of the variance in fatigue scores after chemotherapy treatment.[54] In another study, posttreatment colorectal cancer patients were found to have more fatigue when they had catastrophizing thoughts (rumination, magnification, and helplessness).[55] Factors similar to those seen in patients with early-stage cancer also contribute to fatigue in patients with advanced, incurable cancer.[56]
Cognitive Factors
Impairment in cognitive functioning, including decreased attention span and impaired perception and thinking, is commonly associated with fatigue.[57] Although fatigue and cognitive impairments are linked, the mechanism underlying this association is unclear. The mental demands inherent in the diagnosis and treatment of cancer have been well documented, but little is known about the concomitant problem of attention fatigue in people with cancer. Attention problems are common during and after cancer treatment.[57] Some of these problems may be caused by the fatigue of directed attention.[57,58] Attention fatigue may be relieved by activities that promote rest and restore directed attention.[58] Although sleep is necessary for relieving attention fatigue and restoring attention, it is insufficient when attention demands are high. Research in this area is limited and most commonly conducted in breast cancer patients, potentially limiting its application across diverse populations. Empirical literature suggests that exposure to the natural environment may help restore directed attention and relieve attention fatigue.
Sleep Disorders and Inactivity
Causative or contributing factors in CRF may be:
Disrupted sleep.
Poor sleep hygiene.
Decreased nighttime sleep or excessive daytime sleep.
Patients with less daytime activity, restless sleep, and obesity were noted to have consistently higher levels of CRF.[59]
Sleep disorders clearly contribute to fatigue [60] and may differentially affect fatigue ratings, depending on the time of the rating. A study that evaluated fatigue in women undergoing radiation therapy for breast cancer found that sleep had a greater influence on fatigue values in the morning than in the evening.[7] However, fatigue and sleep can also be distinct problems. One study found that the use of cognitive behavioral therapy resulted in significant improvement in sleep quality but did not significantly affect CRF.[61] For more information, see Sleep Disorders.
Other Medications That Contribute to Fatigue
Medications other than chemotherapy drugs may contribute to fatigue. Opioids used to treat cancer-related pain are often associated with sedation, though the degree varies among individuals. Opioids are known to alter the normal function of the hypothalamic secretion of gonadotropin-releasing hormone.[62] Hypogonadism may be found in patients with advanced cancer and can contribute to fatigue during cancer treatment.[63,64] One case-control study examined the effects of chronic oral opioid administration in survivors of cancer and, consistent with the research on intrathecal administration, found marked central hypogonadism among the opioid users with significant symptoms of sexual dysfunction, depression, and fatigue.[65] In patients with hypogonadism and symptoms of fatigue, testosterone replacement over a month had mixed results in clinical trials, with benefit for fatigue occurring around the 70-day mark, but with no improvement in quality of life.[66]
Other medications—including tricyclic antidepressants, neuroleptics, beta blockers, benzodiazepines, and antihistamines—may produce side effects of sedation. In addition, concurrent medications such as analgesics, hypnotics, antidepressants, antiemetics, steroids, or anticonvulsants—many of which act on the central nervous system—can significantly compound the problem of fatigue. The coadministration of multiple drugs with varying side effects may compound fatigue symptoms.
References
Campos MP, Hassan BJ, Riechelmann R, et al.: Cancer-related fatigue: a practical review. Ann Oncol 22 (6): 1273-9, 2011. [PUBMED Abstract]
Yennurajalingam S, Palmer JL, Zhang T, et al.: Association between fatigue and other cancer-related symptoms in patients with advanced cancer. Support Care Cancer 16 (10): 1125-30, 2008. [PUBMED Abstract]
Miaskowski C, Paul SM, Cooper BA, et al.: Trajectories of fatigue in men with prostate cancer before, during, and after radiation therapy. J Pain Symptom Manage 35 (6): 632-43, 2008. [PUBMED Abstract]
Vaz-Luis I, Di Meglio A, Havas J, et al.: Long-Term Longitudinal Patterns of Patient-Reported Fatigue After Breast Cancer: A Group-Based Trajectory Analysis. J Clin Oncol 40 (19): 2148-2162, 2022. [PUBMED Abstract]
Bortolon C, Krikorian A, Carayol M, et al.: Cancer-related fatigue in breast cancer patients after surgery: a multicomponent model using partial least squares-path modeling. Psychooncology 23 (4): 444-51, 2014. [PUBMED Abstract]
Wang XS, Zhao F, Fisch MJ, et al.: Prevalence and characteristics of moderate to severe fatigue: a multicenter study in cancer patients and survivors. Cancer 120 (3): 425-32, 2014. [PUBMED Abstract]
Dhruva A, Dodd M, Paul SM, et al.: Trajectories of fatigue in patients with breast cancer before, during, and after radiation therapy. Cancer Nurs 33 (3): 201-12, 2010 May-Jun. [PUBMED Abstract]
Pertl MM, Hevey D, Boyle NT, et al.: C-reactive protein predicts fatigue independently of depression in breast cancer patients prior to chemotherapy. Brain Behav Immun 34: 108-19, 2013. [PUBMED Abstract]
Xiao C, Miller AH, Felger J, et al.: Depressive symptoms and inflammation are independent risk factors of fatigue in breast cancer survivors. Psychol Med 47 (10): 1733-1743, 2017. [PUBMED Abstract]
Wang XS, Williams LA, Krishnan S, et al.: Serum sTNF-R1, IL-6, and the development of fatigue in patients with gastrointestinal cancer undergoing chemoradiation therapy. Brain Behav Immun 26 (5): 699-705, 2012. [PUBMED Abstract]
Aouizerat BE, Dodd M, Lee K, et al.: Preliminary evidence of a genetic association between tumor necrosis factor alpha and the severity of sleep disturbance and morning fatigue. Biol Res Nurs 11 (1): 27-41, 2009. [PUBMED Abstract]
Miaskowski C, Dodd M, Lee K, et al.: Preliminary evidence of an association between a functional interleukin-6 polymorphism and fatigue and sleep disturbance in oncology patients and their family caregivers. J Pain Symptom Manage 40 (4): 531-44, 2010. [PUBMED Abstract]
Reinertsen KV, Engebraaten O, Loge JH, et al.: Fatigue During and After Breast Cancer Therapy-A Prospective Study. J Pain Symptom Manage 53 (3): 551-560, 2017. [PUBMED Abstract]
Kuhnt S, Szalai C, Erdmann-Reusch B, et al.: [Cancer Related Fatigue in Rehabilitation Care]. Rehabilitation (Stuttg) 56 (5): 337-343, 2017. [PUBMED Abstract]
Donovan KA, Jacobsen PB, Andrykowski MA, et al.: Course of fatigue in women receiving chemotherapy and/or radiotherapy for early stage breast cancer. J Pain Symptom Manage 28 (4): 373-80, 2004. [PUBMED Abstract]
Hickok JT, Morrow GR, McDonald S, et al.: Frequency and correlates of fatigue in lung cancer patients receiving radiation therapy: implications for management. J Pain Symptom Manage 11 (6): 370-7, 1996. [PUBMED Abstract]
Hofman M, Ryan JL, Figueroa-Moseley CD, et al.: Cancer-related fatigue: the scale of the problem. Oncologist 12 (Suppl 1): 4-10, 2007. [PUBMED Abstract]
Kishan AU, Wang PC, Sharif J, et al.: Clinical Indicators of Psychosocial Distress Predict for Acute Radiation-Induced Fatigue in Patients Receiving Adjuvant Radiation Therapy for Breast Cancer: An Analysis of Patient-Reported Outcomes. Int J Radiat Oncol Biol Phys 95 (3): 946-955, 2016. [PUBMED Abstract]
Hsiao CP, Daly B, Saligan LN: The Etiology and management of radiotherapy-induced fatigue. Expert Rev Qual Life Cancer Care 1 (4): 323-328, 2016. [PUBMED Abstract]
Goedendorp MM, Gielissen MF, Verhagen CA, et al.: Development of fatigue in cancer survivors: a prospective follow-up study from diagnosis into the year after treatment. J Pain Symptom Manage 45 (2): 213-22, 2013. [PUBMED Abstract]
Bower JE, Lamkin DM: Inflammation and cancer-related fatigue: mechanisms, contributing factors, and treatment implications. Brain Behav Immun 30 (Suppl): S48-57, 2013. [PUBMED Abstract]
Weber JS, Yang JC, Atkins MB, et al.: Toxicities of Immunotherapy for the Practitioner. J Clin Oncol 33 (18): 2092-9, 2015. [PUBMED Abstract]
Wick W, Hertenstein A, Platten M: Neurological sequelae of cancer immunotherapies and targeted therapies. Lancet Oncol 17 (12): e529-e541, 2016. [PUBMED Abstract]
Berger AM, Lockhart K, Agrawal S: Variability of patterns of fatigue and quality of life over time based on different breast cancer adjuvant chemotherapy regimens. Oncol Nurs Forum 36 (5): 563-70, 2009. [PUBMED Abstract]
So WK, Marsh G, Ling WM, et al.: The symptom cluster of fatigue, pain, anxiety, and depression and the effect on the quality of life of women receiving treatment for breast cancer: a multicenter study. Oncol Nurs Forum 36 (4): E205-14, 2009. [PUBMED Abstract]
Goedendorp MM, Andrykowski MA, Donovan KA, et al.: Prolonged impact of chemotherapy on fatigue in breast cancer survivors: a longitudinal comparison with radiotherapy-treated breast cancer survivors and noncancer controls. Cancer 118 (15): 3833-41, 2012. [PUBMED Abstract]
Jim HS, Small B, Faul LA, et al.: Fatigue, depression, sleep, and activity during chemotherapy: daily and intraday variation and relationships among symptom changes. Ann Behav Med 42 (3): 321-33, 2011. [PUBMED Abstract]
Mao H, Bao T, Shen X, et al.: Prevalence and risk factors for fatigue among breast cancer survivors on aromatase inhibitors. Eur J Cancer 101: 47-54, 2018. [PUBMED Abstract]
Topalian SL, Hodi FS, Brahmer JR, et al.: Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 366 (26): 2443-54, 2012. [PUBMED Abstract]
Brahmer JR, Tykodi SS, Chow LQ, et al.: Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 366 (26): 2455-65, 2012. [PUBMED Abstract]
Rizvi NA, Mazières J, Planchard D, et al.: Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol 16 (3): 257-65, 2015. [PUBMED Abstract]
Naidoo J, Page DB, Li BT, et al.: Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol 26 (12): 2375-91, 2015. [PUBMED Abstract]
Cella D, Lai JS, Chang CH, et al.: Fatigue in cancer patients compared with fatigue in the general United States population. Cancer 94 (2): 528-38, 2002. [PUBMED Abstract]
Jacobsen PB, Garland LL, Booth-Jones M, et al.: Relationship of hemoglobin levels to fatigue and cognitive functioning among cancer patients receiving chemotherapy. J Pain Symptom Manage 28 (1): 7-18, 2004. [PUBMED Abstract]
Blair S, Bardwell WA, Podbelewicz-Schuller Y, et al.: Correlation between hemoglobin and fatigue in women undergoing adjuvant chemotherapy without erythropoietin-stimulating-agent support. Clin Breast Cancer 8 (6): 522-6, 2008. [PUBMED Abstract]
Jacobsen PB, Thors CL: Fatigue in the radiation therapy patient: current management and investigations. Semin Radiat Oncol 13 (3): 372-80, 2003. [PUBMED Abstract]
Bush RS: The significance of anemia in clinical radiation therapy. Int J Radiat Oncol Biol Phys 12 (11): 2047-50, 1986. [PUBMED Abstract]
Girinski T, Pejovic-Lenfant MH, Bourhis J, et al.: Prognostic value of hemoglobin concentrations and blood transfusions in advanced carcinoma of the cervix treated by radiation therapy: results of a retrospective study of 386 patients. Int J Radiat Oncol Biol Phys 16 (1): 37-42, 1989. [PUBMED Abstract]
Dubray B, Mosseri V, Brunin F, et al.: Anemia is associated with lower local-regional control and survival after radiation therapy for head and neck cancer: a prospective study. Radiology 201 (2): 553-8, 1996. [PUBMED Abstract]
Dunst J: Hemoglobin level and anemia in radiation oncology: prognostic impact and therapeutic implications. Semin Oncol 27 (2 Suppl 4): 4-8; discussion 16-7, 2000. [PUBMED Abstract]
Sathiaraj E, Afshan K, R S, et al.: Effects of a Plant-Based High-Protein Diet on Fatigue in Breast Cancer Patients Undergoing Adjuvant Chemotherapy – a Randomized Controlled Trial. Nutr Cancer 75 (3): 846-856, 2023. [PUBMED Abstract]
Williams AM, Khan CP, Heckler CE, et al.: Fatigue, anxiety, and quality of life in breast cancer patients compared to non-cancer controls: a nationwide longitudinal analysis. Breast Cancer Res Treat 187 (1): 275-285, 2021. [PUBMED Abstract]
Krebber AM, Buffart LM, Kleijn G, et al.: Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments. Psychooncology 23 (2): 121-30, 2014. [PUBMED Abstract]
Goldstein D, Bennett BK, Webber K, et al.: Cancer-related fatigue in women with breast cancer: outcomes of a 5-year prospective cohort study. J Clin Oncol 30 (15): 1805-12, 2012. [PUBMED Abstract]
Andrykowski MA, Donovan KA, Laronga C, et al.: Prevalence, predictors, and characteristics of off-treatment fatigue in breast cancer survivors. Cancer 116 (24): 5740-8, 2010. [PUBMED Abstract]
Cella D, Davis K, Breitbart W, et al.: Cancer-related fatigue: prevalence of proposed diagnostic criteria in a United States sample of cancer survivors. J Clin Oncol 19 (14): 3385-91, 2001. [PUBMED Abstract]
Fagundes CP, Lindgren ME, Shapiro CL, et al.: Child maltreatment and breast cancer survivors: social support makes a difference for quality of life, fatigue and cancer stress. Eur J Cancer 48 (5): 728-36, 2012. [PUBMED Abstract]
Cimprich B: Pretreatment symptom distress in women newly diagnosed with breast cancer. Cancer Nurs 22 (3): 185-94; quiz 195, 1999. [PUBMED Abstract]
Bower JE, Ganz PA, Desmond KA, et al.: Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer 106 (4): 751-8, 2006. [PUBMED Abstract]
Rodrigues AR, Trufelli DC, Fonseca F, et al.: Fatigue in Patients With Advanced Terminal Cancer Correlates With Inflammation, Poor Quality of Life and Sleep, and Anxiety/Depression. Am J Hosp Palliat Care 33 (10): 942-947, 2016. [PUBMED Abstract]
Zhu L, Ranchor AV, van der Lee M, et al.: Co-morbidity of depression, anxiety and fatigue in cancer patients receiving psychological care. Psychooncology 26 (4): 444-451, 2017. [PUBMED Abstract]
Montgomery GH, Schnur JB, Erblich J, et al.: Presurgery psychological factors predict pain, nausea, and fatigue one week after breast cancer surgery. J Pain Symptom Manage 39 (6): 1043-52, 2010. [PUBMED Abstract]
Prue G, Allen J, Gracey J, et al.: Fatigue in gynecological cancer patients during and after anticancer treatment. J Pain Symptom Manage 39 (2): 197-210, 2010. [PUBMED Abstract]
Müller F, Stephenson E, DeLongis A, et al.: The reciprocal relationship between daily fatigue and catastrophizing following cancer treatment: Affect and physical activity as potential mediators. Psychooncology 27 (3): 831-837, 2018. [PUBMED Abstract]
Peters ME, Goedendorp MM, Verhagen SA, et al.: Exploring the contribution of psychosocial factors to fatigue in patients with advanced incurable cancer. Psychooncology 23 (7): 773-9, 2014. [PUBMED Abstract]
Minton O, Stone PC: A comparison of cognitive function, sleep and activity levels in disease-free breast cancer patients with or without cancer-related fatigue syndrome. BMJ Support Palliat Care 2 (3): 231-8, 2012. [PUBMED Abstract]
Von Ah D, Storey S, Crouch A, et al.: Relationship of Self-reported Attentional Fatigue to Perceived Work Ability in Breast Cancer Survivors. Cancer Nurs 40 (6): 464-470, 2017 Nov/Dec. [PUBMED Abstract]
Berger AM: Update on the state of the science: sleep-wake disturbances in adult patients with cancer. Oncol Nurs Forum 36 (4): E165-77, 2009. [PUBMED Abstract]
Ancoli-Israel S, Liu L, Marler MR, et al.: Fatigue, sleep, and circadian rhythms prior to chemotherapy for breast cancer. Support Care Cancer 14 (3): 201-9, 2006. [PUBMED Abstract]
Berger AM, Kuhn BR, Farr LA, et al.: One-year outcomes of a behavioral therapy intervention trial on sleep quality and cancer-related fatigue. J Clin Oncol 27 (35): 6033-40, 2009. [PUBMED Abstract]
Katz N, Mazer NA: The impact of opioids on the endocrine system. Clin J Pain 25 (2): 170-5, 2009. [PUBMED Abstract]
Strasser F, Palmer JL, Schover LR, et al.: The impact of hypogonadism and autonomic dysfunction on fatigue, emotional function, and sexual desire in male patients with advanced cancer: a pilot study. Cancer 107 (12): 2949-57, 2006. [PUBMED Abstract]
Dev R, Hui D, Del Fabbro E, et al.: Association between hypogonadism, symptom burden, and survival in male patients with advanced cancer. Cancer 120 (10): 1586-93, 2014. [PUBMED Abstract]
Rajagopal A, Vassilopoulou-Sellin R, Palmer JL, et al.: Symptomatic hypogonadism in male survivors of cancer with chronic exposure to opioids. Cancer 100 (4): 851-8, 2004. [PUBMED Abstract]
Del Fabbro E, Garcia JM, Dev R, et al.: Testosterone replacement for fatigue in hypogonadal ambulatory males with advanced cancer: a preliminary double-blind placebo-controlled trial. Support Care Cancer 21 (9): 2599-607, 2013. [PUBMED Abstract]
Assessment
The first step in the assessment of fatigue is screening.[1] Patients can be screened for fatigue at the initial visit, at the beginning and end of primary cancer treatments, and at least annually (or as clinically indicated) during follow-up care. Evidence indicates that brief, self-report, quantitative, and single-item assessments with empirically established cut-off scores can measure fatigue levels in an expedited manner.[2] These tools include assessments such as the National Comprehensive Cancer Network (NCCN) intensity tool [2] and the visual analog scale (VAS),[3] which are 0-to-10 numeric rating scales (0 = no fatigue; 10 = worst fatigue imaginable). Ratings are categorized as none to mild (score, 0–3), moderate (score, 4–6), and severe (score, 7–10). Fatigue is considered clinically significant when rated in the moderate-to-severe range (score, 4–10).[4]
Patients with moderate-to-severe levels of fatigue require further evaluation. One study of ambulatory outpatients with solid tumors (n = 148) evaluated the usefulness of single-item screening for symptoms such as fatigue and pain.[5] Investigators found that the single-item assessment can help identify patients who require comprehensive assessments of their symptoms. Patients identified through single-item screening tools undergo comprehensive assessments to detect clinically relevant symptomatology.[5,6]
Cancer-related fatigue (CRF) is multifactorial. The purpose of an in-depth evaluation is to assess diverse factors that can cause or contribute to fatigue.[7–10] Such an evaluation may identify factors that can be reversed or treated (e.g., hypothyroidism, sleep disturbances, or depression). In addition, fatigue can be part of a symptom cluster. For more information, see Symptom Clusters in Cancer.
A comprehensive assessment of a fatigued patient starts with carefully obtaining a history to fully characterize the patient’s fatigue pattern and to identify all factors that contribute to its development. An in-depth evaluation of fatigue includes the following:
Status of cancer and cancer treatments: recurrence or progression of disease, type and length of cancer treatments, and capacity of treatments to induce fatigue.
Review of systems to assess impact of cancer and cancer treatments on other organs and systems.
Comprehensive physical examination, including gait, posture, and range of motion.
Assessment of causative or contributing factors:[1]
Anemia.
Hypothyroidism.
Fluid/electrolyte imbalance.
Weight/caloric intake.
Sleep disturbances (e.g., insomnia, hypersomnia, sleep apnea, and restless legs syndrome).
Emotional disturbances (depression or anxiety), including psychiatric history and adversity during childhood.[11]
Pain.
Other treatment-related side effects (e.g., neuropathy or hot flashes).
Review of medication effects and effects caused by drug interactions (e.g., exacerbation of fatigue due to sedation or insomnia, worsening of depression, and cardiovascular effects).
Assessment of other comorbidities (e.g., alcohol and drug misuse and illicit substance use, cardiovascular or pulmonary diseases, endocrine dysfunction, neurological disorders, renal or hepatic dysfunction, infections, and gastrointestinal dysfunction).
Assessment of social, economic, and spiritual factors that can directly or indirectly exacerbate fatigue levels (by worsening emotional distress).
Assessment of functional status: physical activity levels and deconditioning.
An in-depth fatigue evaluation also includes an assessment of specific aspects of fatigue based on patient self-report:
Onset.
Duration.
Pattern.
Change in intensity and frequency over time.
Exacerbating or alleviating factors.
Associated patient distress.
Interference with functioning.
Although there is no universally accepted standard for the measurement of fatigue, a variety of instruments can assess fatigue and related sequelae.[10,12–15][Level of evidence: II]; [16–19] These instruments range from single-item instruments screening tools to multi-item, multidimensional instruments used to conduct in-depth evaluations of fatigue. These instruments can be generally divided into three major categories:
Very brief, single-item instruments that can be used for fatigue screening and longitudinal monitoring of fatigue (e.g., the VAS).
Brief, multi-item but unidimensional instruments (e.g., the Brief Fatigue Inventory [BFI]).
Comprehensive, multi-item, and multidimensional instruments (e.g., the Multidimensional Fatigue Inventory).
Table 2 delineates several instruments that are commonly used (in research and clinical practice) and have known psychometric properties. The use of a specific instrument in clinical practice is informed by what the instrument assesses and the objective of fatigue assessment at a specific time. For example, the VAS is used to screen for the presence or absence of fatigue in an expedited manner and to get a quick assessment of its severity. Multi-item but unidimensional assessments such as the BFI can be used to conduct an in-depth fatigue assessment, including fatigue severity, patterns, and impact on functioning. The multidimensional instruments can be used to conduct a comprehensive evaluation of fatigue in patients with complex fatigue patterns. These instruments assess fatigue severity, patterns, and impact on functioning, similar to the unidimensional assessments. Additionally, these instruments can be used in multiple fatigue domains (e.g., physical, affective, and cognitive).
Table 2. Commonly Used Fatigue Instruments
Instrument
Description
Reference
NCCN = National Comprehensive Cancer Network; QOL = quality of life.
Single-item screening instruments
Visual analog scale (VAS) for fatigue
Uses a 10-cm, 0- to 100-mm line; assesses severity only
Proposed criteria for CRF are listed below. These criteria have been adopted for inclusion in the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Clinical Modification (ICD-10-CM).[21]
Defining CRF as a diagnostic syndrome has potential advantages and disadvantages.[22] One of the possible advantages is that clinicians can document the presence or absence of fatigue in a reproducible fashion. The syndrome-based approach may also be useful in establishing appropriate reimbursement for the management of this finding. The potential disadvantage of this approach is that it may deter management of fatigue that does not reach the threshold of an ICD-10 diagnosis. The alternative to the syndrome-based approach (commonly used for depression) is a symptom-based approach, which is commonly used for phenomena such as pain and nausea. The utility of the following ICD-10 criteria for CRF has not been validated.
ICD-10 Criteria for CRF
CRF exists when the following symptoms have been present every day or nearly every day during the same 2-week period in the past month:
Significant fatigue, diminished energy, or increased need to rest, disproportionate to any recent change in activity level, plus five or more of the following:
Complaints of generalized weakness or limb heaviness.
Diminished concentration or attention.
Decreased motivation or interest to engage in usual activities.
Insomnia or hypersomnia.
Experience of sleep as unrefreshing or nonrestorative.
Perceived need to struggle to overcome inactivity.
Marked emotional reactivity (e.g., sadness, frustration, or irritability) to feeling fatigued.
Difficulty completing daily tasks attributed to feeling fatigued.
Perceived problems with short-term memory.
Postexertional fatigue lasting several hours.
Clinically significant distress or impairment in social, occupational, or other important areas of functioning caused by the symptoms.
Evidence from the history, physical examination, or laboratory findings that the symptoms are a consequence of cancer or cancer therapy.
Symptoms not primarily a consequence of comorbid psychiatric disorders such as major depression, somatization disorder, somatoform disorder, or delirium.
As with other self-reported symptoms such as pain, it may be necessary to encourage the patient and other family members to report symptoms of fatigue to the medical staff. Information regarding the potential for fatigue due to the underlying disease or treatments, possible options for management, and the importance of reporting these symptoms is given to patients at the initiation of treatment.[23] Patients may not mention the fatigue they experience unless prompted by a health professional.
Several barriers hamper appropriate management of CRF. Some of these barriers were identified in phase 1 of an ongoing three-phase project related to the implementation of evidence-based guidelines for fatigue management from NCCN.[24] The most commonly identified barriers were the following:[24,25]
The patient’s belief that the physician would introduce the subject of fatigue if it were important (patient barrier).
Lack of fatigue documentation (professional barrier).
Lack of supportive care referrals (system barrier).
Evaluation of Anemia
The proper evaluation of anemia in cancer patients includes the following:
A careful history and physical examination.
An evaluation of the complete blood count and red blood cell indices.
An examination of the peripheral blood smear.
In combination, the information from these investigations is often diagnostic.
One commonly used method for classifying anemia is to categorize the anemia by the size of the red blood cell, as measured by the mean corpuscular volume (MCV).
Microcytic anemias are associated with an MCV of 79 fL or lower and include iron-deficiency anemia, thalassemia, and anemia of chronic disease.
Macrocytic anemias are associated with an MCV higher than 101 fL and include anemias related to vitamin B12 or folate deficiency, myelodysplasia, and liver disease.
Most anemias are normocytic, meaning that the MCV is in the normal range. This category includes the following:[26]
Myelophthisic anemia (i.e., anemia due to neoplastic replacement of the bone marrow).
Most chemotherapy-related anemias.
Anemia due to renal or hepatic dysfunction.
Hemolytic anemia.
Aplastic anemia.
However, a mixed red blood cell population consisting of both microcytic and macrocytic cells (anisocytosis) may indicate a combined etiology, for example, chronic blood loss (microcytic) with resultant reticulocytosis (macrocytic). In this situation, the MCV may be in the normal range, but the red blood cell size distribution width would be elevated.
The peripheral blood smear examination, though often overlooked, remains an important step in the evaluation of anemia. For example, nucleated blood cells and teardrop-shaped red blood cells suggest myelophthisic anemia. Macro-ovalocytes and hypersegmented neutrophils often indicate megaloblastic anemia. Small target cells and basophilic stippling are associated with thalassemia.
Additional studies that are sometimes required to characterize anemia in a given patient include tests for the following:
Vitamin B12 or folate levels.
Serum iron, transferrin, and ferritin levels.
Erythropoietin level, the direct and indirect Coombs test, and/or examination of a bone marrow aspirate and biopsy.
In cancer patients, the underlying etiology is often multifactorial.
References
National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Cancer-Related Fatigue. Version 2.2024. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2024. Available online with registration. Last accessed July 17, 2024.
Mock V, Atkinson A, Barsevick AM, et al.: Cancer-related fatigue. Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 5 (10): 1054-78, 2007. [PUBMED Abstract]
Glaus A: Assessment of fatigue in cancer and non-cancer patients and in healthy individuals. Support Care Cancer 1 (6): 305-15, 1993. [PUBMED Abstract]
Fabi A, Bhargava R, Fatigoni S, et al.: Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann Oncol 31 (6): 713-723, 2020. [PUBMED Abstract]
Butt Z, Wagner LI, Beaumont JL, et al.: Use of a single-item screening tool to detect clinically significant fatigue, pain, distress, and anorexia in ambulatory cancer practice. J Pain Symptom Manage 35 (1): 20-30, 2008. [PUBMED Abstract]
Kirsh KL, Passik S, Holtsclaw E, et al.: I get tired for no reason: a single item screening for cancer-related fatigue. J Pain Symptom Manage 22 (5): 931-7, 2001. [PUBMED Abstract]
Yellen SB, Cella DF, Webster K, et al.: Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J Pain Symptom Manage 13 (2): 63-74, 1997. [PUBMED Abstract]
Smets EM, Garssen B, Bonke B, et al.: The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res 39 (3): 315-25, 1995. [PUBMED Abstract]
Weis J, Arraras JI, Conroy T, et al.: Development of an EORTC quality of life phase III module measuring cancer-related fatigue (EORTC QLQ-FA13). Psychooncology 22 (5): 1002-7, 2013. [PUBMED Abstract]
Piper BF, Dibble SL, Dodd MJ, et al.: The revised Piper Fatigue Scale: psychometric evaluation in women with breast cancer. Oncol Nurs Forum 25 (4): 677-84, 1998. [PUBMED Abstract]
Bower JE, Wiley J, Petersen L, et al.: Fatigue after breast cancer treatment: Biobehavioral predictors of fatigue trajectories. Health Psychol 37 (11): 1025-1034, 2018. [PUBMED Abstract]
Lee KA, Hicks G, Nino-Murcia G: Validity and reliability of a scale to assess fatigue. Psychiatry Res 36 (3): 291-8, 1991. [PUBMED Abstract]
Mendoza TR, Wang XS, Cleeland CS, et al.: The rapid assessment of fatigue severity in cancer patients: use of the Brief Fatigue Inventory. Cancer 85 (5): 1186-96, 1999. [PUBMED Abstract]
Okuyama T, Akechi T, Kugaya A, et al.: Development and validation of the cancer fatigue scale: a brief, three-dimensional, self-rating scale for assessment of fatigue in cancer patients. J Pain Symptom Manage 19 (1): 5-14, 2000. [PUBMED Abstract]
Hann DM, Denniston MM, Baker F: Measurement of fatigue in cancer patients: further validation of the Fatigue Symptom Inventory. Qual Life Res 9 (7): 847-54, 2000. [PUBMED Abstract]
Cella D: The Functional Assessment of Cancer Therapy-Anemia (FACT-An) Scale: a new tool for the assessment of outcomes in cancer anemia and fatigue. Semin Hematol 34 (3 Suppl 2): 13-9, 1997. [PUBMED Abstract]
Cella D: Manual of the Functional Assessment of Chronic Illness Therapy (FACIT) Scales. Version 4. Evanston Northwestern Healthcare, 1997.
Schwartz AL: The Schwartz Cancer Fatigue Scale: testing reliability and validity. Oncol Nurs Forum 25 (4): 711-7, 1998. [PUBMED Abstract]
McNair D, Lorr M, Droppelman L, et al.: Profile of Mood States. Educational and Industrial Testing Service, 1971.
Hann DM, Jacobsen PB, Azzarello LM, et al.: Measurement of fatigue in cancer patients: development and validation of the Fatigue Symptom Inventory. Qual Life Res 7 (4): 301-10, 1998. [PUBMED Abstract]
Portenoy RK, Itri LM: Cancer-related fatigue: guidelines for evaluation and management. Oncologist 4 (1): 1-10, 1999. [PUBMED Abstract]
Sadler IJ, Jacobsen PB, Booth-Jones M, et al.: Preliminary evaluation of a clinical syndrome approach to assessing cancer-related fatigue. J Pain Symptom Manage 23 (5): 406-16, 2002. [PUBMED Abstract]
Cella D, Peterman A, Passik S, et al.: Progress toward guidelines for the management of fatigue. Oncology (Huntingt) 12 (11A): 369-77, 1998. [PUBMED Abstract]
Borneman T, Piper BF, Sun VC, et al.: Implementing the Fatigue Guidelines at one NCCN member institution: process and outcomes. J Natl Compr Canc Netw 5 (10): 1092-101, 2007. [PUBMED Abstract]
Passik SD, Kirsh KL, Donaghy K, et al.: Patient-related barriers to fatigue communication: initial validation of the fatigue management barriers questionnaire. J Pain Symptom Manage 24 (5): 481-93, 2002. [PUBMED Abstract]
Bohlius J, Bohlke K, Castelli R, et al.: Management of Cancer-Associated Anemia With Erythropoiesis-Stimulating Agents: ASCO/ASH Clinical Practice Guideline Update. J Clin Oncol 37 (15): 1336-1351, 2019. [PUBMED Abstract]
Interventions
Much of the information regarding interventions for fatigue relates to healthy subjects, people in whom muscle fatigue is the primary etiology of the problem, or people in whom fatigue is secondary to treatment-related anemia.[1,2][Level of evidence: II]; [3,4] Without a determination of the causative mechanisms of fatigue in oncology patients, interventions must be directed to symptom management and emotional support. Although some recommendations for the management of fatigue in oncology patients have been made, these are theoretical or anecdotal in nature and in general have not been the focus of scientific evaluation.
Published in 2013, a study conducted in patients with advanced cancer (N = 152) demonstrated that managing symptoms (e.g., pain, nausea, and decreased appetite) can have a significant positive impact on fatigue.[5] In this 12-week study, patients were randomly assigned to receive either monitoring and protocolized treatment of physical symptoms coordinated by a nurse or usual care (symptom management included in the standard oncologic care). Patients in the intervention group received tailored treatment for any of the identified troublesome symptoms. Fatigue levels, as measured by the Multidimensional Fatigue Inventory, showed significant improvement in the intervention group compared with the group receiving usual care. The intervention group also showed improvements in the following:[5]
Specific fatigue dimensions.
Interference by fatigue with daily life.
Overall symptom burden.
Symptoms of depression and anxiety.
Assessing patients for the appropriate target symptom for intervention is probably the most efficient way to help them improve their health-related quality of life and manage their fatigue symptoms.
Because the etiology and mechanisms regarding fatigue in cancer patients are varied, there is considerable need to personalize symptom management to provide goal-concordant care. Medical management is often directed at identifying specific and potentially reversible correlated symptoms, as in the following examples:
Patients with fatigue and pain may benefit from titration of pain medications.
Patients with fatigue and anemia may receive a transfusion of packed red blood cells (RBCs), nutritional interventions including iron-rich foods, supplemental iron or vitamins to correct an underlying deficiency, or injections of epoetin alfa.
Patients with depressed mood and fatigue may be treated with antidepressants or psychostimulants.
Treatment of Anemia
Anemia in patients with cancer is best managed by treatment of the underlying cause. When the cause is obscure or there is no specific remedy, then treatment is supportive. Nutritional interventions, including the intake of nutrient-rich foods and supplements, are considered in addition to other treatment modalities.
The transfusion of packed RBCs is the most widely used and most rapid way to alleviate symptoms in cancer patients with symptomatic anemia. The likelihood of raising a patient’s hemoglobin level is very high with transfusion, and the risks of complications are low. Nevertheless, repeated transfusions can be cumbersome, and the risk of blood-borne infection can be worrisome. Other risks include an acute transfusion reaction, transfusion-associated graft-versus-host disease, subtle immune modulation that occurs with transfusion, and iron overload in patients who receive repeated transfusions.[6]
The management of cancer-associated anemia using erythropoiesis-stimulating agents (ESAs) was established in the 2019 American Society of Clinical Oncology (ASCO)/American Society of Hematology (ASH) guidelines, which recommended the following:[7]
ESAs (including biosimilars) may be offered to patients with chemotherapy-associated anemia whose cancer treatment is not curative in intent and whose hemoglobin levels have declined to lower than 10 g/dL. RBC transfusion is also an option.
With the exception of selected patients with myelodysplastic syndromes, ESAs should not be offered to most patients with non–chemotherapy-associated anemia.
During ESA treatment, hemoglobin may be increased to the lowest concentration needed to avoid transfusions.
Iron replacement may be used to improve hemoglobin response and reduce RBC transfusions for patients with or without iron deficiency who are receiving ESAs.
ESAs increase the risk of thromboembolism, and clinicians should carefully weigh the risks of thromboembolism and use caution and clinical judgment when considering the use of these agents.[7]
Psychostimulants
Psychostimulants are a common pharmacological intervention for cancer-related fatigue (CRF); however, the evidence for their efficacy is mixed. Psychostimulants are drugs that interact with neurotransmitters and receptors in the brain to increase cortical function. Different types of psychostimulants work through various mechanisms to produce activity in the brain consistent with short-term improvement in energy level and psychomotor activity. These medications may also improve mood, attention, and concentration in some populations. Psychostimulant clinical trials for the management of fatigue include the following therapies (for information about levels of evidence and dosing used in the clinical trials, see Table 3):
Methylphenidate.
Dextroamphetamine.
Modafinil.
Armodafinil.
Psychostimulants are not approved by the U.S. Food and Drug Administration (FDA) for the treatment of CRF. However, preliminary evidence from randomized controlled studies [8–10] suggests that these medications might be helpful in a subpopulation of patients experiencing moderate to severe fatigue. Of the psychostimulants, methylphenidate is the most studied pharmacological agent for fatigue, yet the evidence for its efficacy is mixed.[11]
Table 3. Centrally Acting Stimulants for Adult Cancer Patients
Drug
Dosage
Outcome
Comments/Primary Side Effects
AUC = area under the curve; bid = twice daily; CAD = coronary artery disease; CRF = cancer-related fatigue; LHRH = luteinizing hormone-releasing hormone; MAOI = monoamine oxidase inhibitor; PO = by mouth; prn = as needed; q2h = every 2 hours; qd = every day; SR = sustained release; SSRI = selective serotonin reuptake inhibitor; tid = three times daily.
aAs defined by the U.S. Controlled Substances Act.
Schedule II.a Major potential interactions with citalopram and venlafaxine. Avoid in patients with uncontrolled hypertension, underlying CAD, and tachyarrhythmias.[13]
Schedule II.a High-fat meals may increase AUC. Peak concentration 102 h postingestion. Do not use with MAOIs as it can precipitate hypertensive crisis. Antidepressants that increase norepinephrine can increase amphetamine side effects. Concomitant use with SSRI can increase SSRI concentrations. Avoid in patients with uncontrolled hypertension, underlying CAD, and tachyarrhythmias.[13]
Titrate up to 54 mg/d PO (27 mg D-isomer) over 4 wk
CRF improved in patients receiving chemotherapy with severe fatigue, but not mild/moderate fatigue.[10]
Schedule IV.a Avoid driving or operating machinery until effects are known. Do not take at bedtime. Peak concentration in 2–4 h. Food slows absorption by about 1 h but does not affect bioavailability. Decreases efficacy of birth control pills.
100 mg PO bid (up to 400 mg/d) x6 wk
Did not improve CRF over placebo in patients with primary brain tumors.[21]
200 mg PO qd x15 d
Did not improve CRF over placebo in patients receiving docetaxel.[22]
100 mg PO qd on days 1–14 and 200 mg qd on days 15–28
Did not improve CRF over placebo in patients with lung cancer.[23]
Armodafinil (Nuvigil)
50 mg PO bid
Did not improve daytime fatigue over placebo in cancer survivors with insomnia.[24]
Schedule IV.a Avoid driving or operating machinery until effects are known. Do not take at bedtime. Peak concentration in 2 h if fasting, slowed to as many as 4 h if fed; food does not affect bioavailability. Decreases efficacy of birth control pills.
150 mg PO qd x56 d
Did not improve CRF over placebo in patients with multiple myeloma.[25]
Methylphenidate
Among all pharmacological treatment options for CRF, methylphenidate has the best evidence based on studies to date. The evidence for methylphenidate remains mixed, but it may play an important role in a subpopulation of cancer survivors.
One of the studies that demonstrated significant improvements over placebo for CRF used a mean dose of 27.7 mg of the D-isomer of methylphenidate as a study intervention.[8] The population that benefited was women who had completed chemotherapy for breast or ovarian cancer. The study design incorporated a titration to effect, so some patients who may have benefited may have received more than 27.7 mg of the drug. Furthermore, 11% of trial participants withdrew because of adverse events, compared with 1% in the placebo arm.
Conversely, an equally large randomized controlled trial assigned patients with early and advanced disease, who were either receiving treatment or not receiving treatment, to receive 54 mg of a long-acting methylphenidate preparation equaling 27 mg of the D-isomer or a placebo. This trial found no differences between the two groups in any of the fatigue outcomes.[15][Level of evidence: I] There were significant differences between groups for nervousness and appetite loss, with the methylphenidate arm scoring worse on both of those side effects.
Another large randomized placebo-controlled trial (n = 163) in patients with advanced cancer investigated immediate-release methylphenidate, starting at 5 mg twice daily.[14][Level of evidence: I] The dose was titrated up to 20 mg three times daily over a 6-week period. Improvement in fatigue and depression was nominally higher in the methylphenidate group than in the placebo group, but the differences did not reach clinically meaningful levels. There were no differences in adverse events between the two groups, including side effects such as anxiety, insomnia, loss of appetite, or heart palpitations.
Methylphenidate continues to show mixed results as a treatment for fatigue in patients with cancer. Several factors may cause this situation, including high placebo response, differential formulation and dosing, and heterogeneity of patient-related factors (e.g., early stage versus advanced stage of cancer, heterogeneity of cancer, cancer treatments, co-morbidities, and concomitant medications). Based on the mixed trial results to date, methylphenidate may treat fatigue in specific subpopulations of cancer survivors. Immediate-release formulations with a shorter half-life appear to have a better safety and tolerability profile, with a lower risk of side effects, compared with longer-acting formulations.
Modafinil and armodafinil
The newer so-called wake-promoting agents, modafinil and armodafinil, are just beginning to be studied for CRF. Modafinil is a centrally acting, nonamphetamine central nervous system stimulant.[26] Armodafinil is the R-enantiomer of modafinil and an alpha-1 adrenoceptor agonist.[27] The FDA has approved modafinil and armodafinil for the treatment of narcolepsy, obstructive sleep apnea, and shift-work disorders but not for the treatment of CRF. These agents are also not indicated for use in children and adolescents.
The mechanism of action of modafinil and armodafinil is different from that of amphetamines, but the exact mechanisms by which these agents improve wakefulness are not known. On the basis of two promising open-label pilot trials,[28,29] a large randomized controlled trial evaluated modafinil for the treatment of CRF using 200 mg versus placebo in more than 850 patients who were receiving chemotherapy.[10] Patients had to have fatigue ratings of at least 2 out of 10 to be eligible for this study. During four cycles of chemotherapy, there were no significant differences between arms.
A randomized placebo-controlled trial (four-arm factorial study) comparing cognitive behavioral therapy (CBT) for insomnia (CBT-I) versus armodafinil (50 mg by mouth twice a day) found that CBT-I with and without armodafinil resulted in a clinically and statistically significant reduction of subjective daytime fatigue in cancer survivors with chronic insomnia.[24] Armodafinil alone did not show a statistically significant effect on fatigue for cancer survivors.
For both methylphenidate and modafinil, exploratory data have suggested that patients with more severe fatigue or more advanced disease may benefit from these drugs.[10,15] A small (N = 23), randomized, placebo-controlled study [9] using methylphenidate (titrated up to 30 mg/d) as an intervention failed to show statistical difference on the primary outcome measure, the Brief Fatigue Inventory (BFI) total score, or activity interference subscale. However, the methylphenidate group showed significant reductions in the BFI severity subscale scores compared with the reductions seen in the placebo group. The mean severity score at baseline was 6.5 for the methylphenidate group and 5.7 for the placebo group, placing these patients in a more severe fatigue category. A secondary analysis of the phase III trial that evaluated modafinil versus placebo for CRF also revealed that patients with more severe fatigue may have benefited from modafinil.[10] More research is needed to further evaluate whether psychostimulants are beneficial for patients experiencing more severe CRF.
Clinical considerations
The side effects most commonly described with the use of psychostimulants include the following:[8,10,15,30,31]
Insomnia.
Euphoria.
Headache.
Nausea.
Anxiety.
Mood lability.
High doses and long-term use may produce:
Anorexia.
Nightmares.
Insomnia.
Euphoria.
Paranoia.
Risk of cardiovascular complications.
Patients with cancer carry a higher risk of cardiovascular complications, depending on the type of cancer and cancer treatment (i.e., cardiotoxic chemotherapy regimens). Cardiovascular complications with psychostimulants can arise even in patients without any significant risk factors.[9] In the study using methylphenidate to treat CRF in patients with prostate cancer, 6 of 16 subjects (27%) in the methylphenidate group were withdrawn because of increased blood pressure and tachycardia. Notably, none of these subjects were being treated with known cardiotoxic chemotherapeutic regimens such as anthracyclines.[9]
Careful and continuous monitoring of certain cardiovascular parameters (mainly blood pressure and heart rate) is critical when psychostimulants are used to treat CRF. In certain complex cases, consultation with cardiology services may be considered. Cardiovascular issues are thought to be less of a risk with modafinil and armodafinil. The risk-benefit ratio may be considered, and patients may be evaluated for response and side effects, when these agents are used to treat CRF.
The package inserts for all Schedule IV stimulant medications (as defined by the U.S. Controlled Substances Act) carry boxed warnings that indicate the risk of abuse potential and/or risk of psychological dependence. In addition, boxed warnings for certain stimulant medications (methylphenidate and dexmethylphenidate products) indicate the risk of psychotic episodes.[30] Other stimulant medications (amphetamine, dextroamphetamine, lisdexamfetamine dimesylate, methamphetamine, and mixed salts of amphetamine products) carry boxed warnings alerting clinicians that misuse of these medications may cause serious cardiovascular adverse events, including sudden death.[32]
On the basis of limited clinical experience and a lack of evidence in randomized controlled trials, it might be reasonable to consider a psychostimulant such as methylphenidate or modafinil for the treatment of severe fatigue, particularly for short periods of time (a couple of weeks) in patients with advanced disease. When the use of these medications is being considered, clinicians should obtain informed consent, with a careful discussion of risks, benefits, and alternatives. Continuous monitoring of cardiovascular parameters is crucial when these medications are used, especially in patients with preexisting cardiovascular issues and in patients being treated with known cardiotoxic chemotherapeutic regimens (e.g., anthracyclines).
Longer-term psychostimulant therapy is not advisable at this time because there is limited information about its potential negative effects and longer-term benefits. Further research is needed in the form of CRF studies using psychostimulants in patients with depression or with drowsiness and sleep disturbance. In the design of these studies, it is important to consider patients with moderate to severe fatigue. These studies should also be performed for a longer period (>4 weeks) to account for the placebo wash-in period.[11]
Other Pharmacological Interventions
Bupropion
Bupropion is a stimulating antidepressant with a primarily dopaminergic and noradrenergic mechanism of action. Preliminary evidence from a small open-label study (N = 21) suggests that the sustained-release (SR) form of bupropion has potential as an effective therapeutic agent for treating CRF, with or without comorbid depressive symptoms.[33][Level of evidence: II] Seizure, a rare but serious side effect of this agent, did not occur in this study (the maximum dose of bupropion SR used was 300 mg).
A small, double-blind, placebo-controlled trial of bupropion SR 150 mg daily versus placebo in a heterogeneous group of patients with cancer (N = 40) [34] demonstrated improvement in fatigue and quality of life as measured by the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale (P = .000) at 4 weeks, compared with baseline assessments of symptoms. Adjustments for fatigue severity, depression, and cancer type did not modify the treatment effect on fatigue outcomes. No differences in adverse outcomes were noted between groups; however, the group receiving bupropion had a higher incidence of nausea and vomiting.[34]
Corticosteroids
Corticosteroids are by far one of the most commonly used medications for symptom control in patients with advanced cancer. These agents have potent anti-inflammatory effects and act by binding to cytoplasmic steroid hormone receptor and modulation of inflammatory gene transcription.[11] Dexamethasone is a potent anti-inflammatory agent that has been evaluated for the treatment of fatigue in patients with advanced cancer.[35] Eighty-four patients were randomly assigned to receive either dexamethasone 4 mg twice per day or a placebo for 14 days. The primary endpoint was improvement in fatigue from baseline to day 15, as measured by the FACIT-F scale. Investigators also evaluated depression, anxiety, and symptom distress. In the group who received dexamethasone, mean scores on the FACIT-F scale were significantly improved by day 8 (P = .005) and at day 15 (P = .008). Physical well-being and physical distress were also significantly better in the group who received dexamethasone. Emotional scores and overall symptom distress were not significantly different. Adverse events, as measured by the Common Terminology Criteria for Adverse Events, version 3.0, did not differ between groups.
One limitation of this study was that it was only 2 weeks long, and longer-term use of dexamethasone is well known to be associated with unwanted side effects. Therefore, the risk versus benefit of treating fatigue with dexamethasone for more than 2 weeks requires investigation. Because fatigue has been associated with high levels of inflammation, this study is noteworthy in its evaluation of dexamethasone as an anti-inflammatory agent to alleviate fatigue.[35] The investigators did not assess inflammatory biomarkers; therefore, the proof of concept that modifying inflammation can reduce fatigue needs replication.
Dietary supplements
Dietary supplements comprise other, often popular, pharmacological interventions for CRF.
American ginseng
Ginseng, a popular supplement used to treat fatigue, has been evaluated in large, multisite clinical trials. On the basis of a promising phase II dose-finding study,[36] a phase III, randomized, placebo-controlled trial involved 364 patients with cancer who either were undergoing anticancer treatment or had completed treatment. Participants were randomly assigned to receive either 2,000 mg of American ginseng (specifically, Wisconsin ginseng) in the form of ground root in a capsule or a matching placebo. The primary endpoint was change in fatigue scores, as measured by the Multidimensional Fatigue Symptom Inventory-Short Form. At 4 weeks, the group receiving ginseng showed a trend toward significant improvement, while at 8 weeks, there was a significant and clinically meaningful difference favoring the ginseng group. There were no discernible side effects during the course of the trial, either within or between groups.[37–39]
Other supplements
Two additional supplements, coenzyme Q10 and levocarnitine (L-carnitine), have been tested in large, randomized trials for the treatment of fatigue; however, they have failed to yield positive effects.
L-carnitine, a widely used dietary supplement, is believed to be helpful for the treatment of CRF because of its role in cellular energy metabolism and carnitine’s ability to decrease pro-inflammatory cytokines. Promising pilot data led to the development and completion of a large (N = 376) phase III study in a multisite cooperative group setting.[40] Participants with moderate to severe fatigue were randomly assigned to receive either 10 g L-carnitine or a placebo for 4 weeks. The primary endpoint was change in average fatigue. Despite increases in mean levels of L-carnitine, there was not a statistically significant difference in fatigue between arms, with both arms reporting improvement during the study.[40]
Similarly, 300 mg of coenzyme Q10 was tested against placebo in a double-blind randomized controlled trial of 236 breast cancer patients. Although supplementation led to sustained increases in plasma coenzyme Q10, there were no significant differences between the groups over the 24-week study.[41] For more information, see Coenzyme Q10.
Exercise
Studies suggest that exercise or physical activity has a beneficial effect on fatigue in patients during and after cancer treatment. The National Comprehensive Cancer Network (NCCN) guidelines [42] identify physical activity as an intervention for patients during and after treatment (category 1 intervention). Researchers have noted reductions in fatigue of about 35% and improvements in vitality of 30% in randomized trials.[43,44] Other documented benefits of exercise or physical activity include the following:
Improved physical energy.
Appetite stimulation.
Improved memory.
Enhanced functional capacity.
Enhanced psychosocial well-being (improved outlook, sense of well-being, and quality of life).
Initial trials of exercise programs focused on women with breast cancer, but subsequent studies included men with prostate cancer and patients with multiple myeloma, lung cancer, nasopharyngeal cancer, non-Hodgkin lymphoma, colorectal cancer, and advanced cancers.[45–47]
Some studies had methodological weaknesses, including the following:[48][Level of evidence: I]; [49]
Selection biases and nonrepresentative samples.
Varied type (aerobic, anaerobic, or combined), dose (frequency and duration), and timing (during or after cancer treatment) of exercise prescription.
Poor adherence to exercise interventions.
Highly varied assessments of research variables and outcome measures.
Lack of adequate control groups.
In a study of 545 breast cancer survivors who were, on average, 6 months postdiagnosis, increased physical activity was consistently related to both improved physical functioning and reduced fatigue and bodily pain. Prediagnosis physical activity was associated with better physical functioning at 39 months but generally unrelated to symptoms. Increased physical activity after cancer was related to less fatigue and pain and better physical functioning. Significant positive associations were found with moderate to vigorous recreational physical activity but not household activity. This study suggests that breast cancer survivors may be able to decrease fatigue and bodily pain and to better pursue daily activities by increasing their recreational physical activities after cancer.[50][Level of evidence: II]
A similar study of breast cancer survivors (N = 222) who were randomly assigned to a 3-month, multicomponent physical activity and behavior change intervention (Better Exercise Adherence after Treatment for Cancer [BEAT Cancer]) demonstrated reduced fatigue, depression, and anxiety symptomatology.[51]
A study of 1,033 patients with breast, gynecological, gastrointestinal, or lung cancer who had received chemotherapy in the past 2 weeks identified associations between level of exercise and fatigue and co-occurring sleep disturbance.[52][Level of evidence: II] Three subgroups of patients were classified: no exercise, less exercise (<150 minutes per week), and recreational exercise (≥150 minutes per week). The most common reported exercise was walking. Compared with the other two groups, the no-exercise group had higher levels of morning fatigue, lower levels of morning and evening energy, and higher levels of sleep disturbance. Patients in the no-exercise group had fewer years of education, were more likely to be non-White, and had a higher body mass index and more comorbidities.[52][Level of evidence: II] These findings suggest associations among patient characteristics, engagement in exercise, and risk for fatigue.
Exercise for patients with advanced or terminal disease is difficult to study but may yield similar benefits. The ability of patients with advanced cancer who are in hospice care and on a physical therapy regimen to carry out activities of daily living reportedly improved in one study.[53][Level of evidence: III] Improved satisfaction with the physical therapy regimen was reported when family involvement in the program increased. A randomized study suggested that exercise improved fatigue during breast cancer treatment.[54][Level of evidence: I] An observational study of patients with advanced cancer found that fatigue was less severe in those who engaged in physical exercise.[55]
When educating patients about activity with respect to CRF, one important goal to consider is inclusion of 3 to 5 hours per week of moderate activity. It is critical that:
Patients choose a type of exercise they enjoy.
Providers discuss specific implementation strategies (type of exercise, time of day, days of the week, location of activity) to enable patients to make frequent activity a reality.
Beginning with lighter activity for shorter periods of time and building in intensity and length of time may be required. Studies have confirmed this can be safely done both during active treatment and after treatment is completed.[43]
Aerobic exercise
Two randomized controlled trials demonstrated the benefit of exercise in reducing fatigue during breast cancer treatment. A trial of a 12-week aerobic exercise program compared with usual care showed a nonsignificant improvement in fatigue 3 and 6 months later.[56][Level of evidence: I] Another trial that compared low-intensity and moderate- to high-intensity physical exercise with usual care showed that higher-intensity exercise (30 min/d, 5 d/wk) was beneficial in reducing fatigue.[57]
Limitations of both studies included the lack of a placebo control group and low participation rates. Low participation is a common finding in exercise studies of cancer patients, suggesting the need for tailored approaches to overcome barriers. The benefits shown in these studies are buttressed by a Cochrane review of 56 studies (including 4,068 participants), which concluded that aerobic exercise significantly reduced fatigue during or after cancer treatment.[58]
Anaerobic (resistance-training) exercise
Studies have also examined the use of resistance training to improve fatigue. In one large randomized controlled trial, 160 breast cancer patients (stages 0–III) were randomly assigned to a progressive resistance training intervention or a relaxation control intervention, twice weekly for 12 weeks. The primary endpoint was perceived fatigue, and the secondary endpoint was evaluated quality of life.[59]
Adherence to this group-based intervention program was as high as 97%. Significant improvements were noted between groups, favoring the resistance-training group for general fatigue (P = .044), especially for the physical fatigue subscale (mean difference = –0.8; 95% confidence interval, –1.5 to –0.2, P = .013), but not for affective fatigue (P = .91) or cognitive fatigue (P = .65). For quality of life, significantly larger improvements regarding role function (P = .035) and pain (P = .040) were noted among exercisers compared with controls. This study demonstrated that resistance training was a feasible and efficacious strategy for improving fatigue and other components of quality of life.
Meta-analyses of aerobic, anaerobic, and combined exercise studies
Several literature reviews and meta-analyses have explored, with mixed results, the effect of exercise on fatigue. They have begun to examine which type of exercise—aerobic (cardio), anaerobic (resistance training), or a combination of the two—is most beneficial in ameliorating fatigue.
One large meta-analysis of breast cancer survivors identified 25 randomized controlled trials (including 3,418 patients) and examined the efficacy of exercise interventions for fatigue and physical functioning during and after treatment and at a 6-month follow-up.[60] Walking was noted to be the most prevalent exercise prescription among the studies reviewed. Improvements in physical functioning and fatigue were observed in the exercise studies during and after treatment, with slightly higher improvements in patients who received the intervention posttreatment. Although combined aerobic and anaerobic groups demonstrated slightly more improvement in physical functioning compared with controls, there were not significant differences in physical functioning and fatigue when all three groups were compared.
A 2018 systematic review and meta-analysis identified 245 studies of all cancer types, explored nonpharmaceutical interventions for fatigue during and after treatment, and conducted an indirect-comparisons meta-analysis among intervention types.[61] In this analysis, aerobic and anaerobic exercise improved fatigue more than usual care, with moderate to large effect sizes noted (standardized mean difference [SMD] for aerobic exercise, –0.53; 95% credible interval [CrI], –0.80 to –0.26; SMD for anaerobic exercise, –0.53; 95% CrI, –1.02 to –0.03). However, combined aerobic and anaerobic exercise demonstrated the most improvement, with a large effect size (SMD, –0.67; 95% CrI, –1.01 to –0.34).
A study of pooled baseline data from three studies (n = 436) investigated reallocating sedentary time to an equal amount of light or moderate-to-vigorous engagement in physical activity in patients with breast cancer. The study showed that fatigue improved in these patients.[62][Level of evidence: III] Specifically, 30 minutes of reallocated light activity improved motivation and engagement in activity (β = -0.21). Engagement in moderate-to-vigorous activity reduced general fatigue (β = -0.34) and physical fatigue (β = -0.47) and improved activity (β = -0.48). However, quality of life did not improve for any level of engagement in physical activity, as highlighted in other studies. Evidence suggests that reallocating sedentary behavior to engagement in physical activity can improve fatigue.
Limitations remain regarding the need to identify a more exacting exercise prescription, including the need to identify the type, intensity, frequency, and resting intervals to fully incorporate into cancer practice and survivorship care plans.[47]
Other exercise modalities
Variations of exercises that have a mind-body component are being studied for their effects on CRF; popular interventions include complementary modalities such as yoga, qigong, and tai chi.[63–65] These modalities are unique in that they incorporate cognitive and spiritual elements with movement, stretching, and balance.
Yoga
Yoga is an ancient system of practices used to balance the mind and body through exercise, meditation (focusing thoughts), and control of breathing and emotions. Yoga has been shown to improve fatigue in cancer survivors in several pilot and larger randomized controlled trials (NCCN category 1 intervention).[66]
In one pilot study, 12 weeks of yoga was compared with a health education intervention in a control group in 31 breast cancer survivors.[67] The primary outcome was change in fatigue measured at baseline, immediately posttreatment, and 3 months after completion of treatment. Fatigue severity declined significantly from baseline to posttreatment and over a 3-month follow-up in the yoga group, relative to controls (P = .032). In addition, the yoga group had significant increases in vigor relative to controls (P = .011).
Similarly, in a larger randomized controlled trial, investigators examined the effect of two 90-minute hatha yoga sessions per week for 12 weeks delivered in a group setting, compared with a wait-list control in 181 breast cancer survivors.[68] Fatigue and vitality immediately posttreatment and at 3 months posttreatment were the endpoints of the study. Investigators noted significant improvement in fatigue at 3 months posttreatment, as well as improved vitality immediately posttreatment and at 3 months posttreatment. However, the study failed to find significant differences in fatigue immediately posttreatment.
In one large, multicenter phase III randomized controlled trial, investigators examined the effect of a standardized 4-week yoga therapy program (Yoga for Cancer Survivors [YOCAS]) on fatigue compared with standard survivorship care in 410 cancer survivors.[66] Compared with participants receiving standard survivorship care, the YOCAS participants demonstrated significantly greater improvements in fatigue (P < .01), as well as decreased interference of fatigue in walking, physical activity, and quality of life (all P < .05). Improvements in fatigue resulting from yoga accounted for significant proportions of the improvements in walking (44%), physical activity (53%), and quality of life (45%; all P < .05). Improvements in overall sleep quality and reductions in daytime dysfunction (e.g., excessive napping) resulting from yoga significantly mediated the effect of yoga on fatigue (22% and 37%, respectively, both P < .01).
A meta-analysis (including 10 studies of cancer survivors) examining yoga for fatigue found that yoga demonstrated a significant improvement in fatigue over usual care, with a moderate effect size (SMD, –0.68; 95% CrI, –0.93 to –0.43).[61]
The limitations of these studies include study designs that varied in the type of yoga and its duration, frequency, and number of weeks; failed to include attention control comparisons; and varied in fatigue assessment measures.
Qigong
Qigong is a traditional Chinese mind/body exercise and meditation that uses slow and precise body movements with controlled breathing and mental focusing to improve balance, flexibility, muscle strength, and overall health. One fairly large study evaluated medical qigong for CRF in a heterogeneous group of 162 patients during or after cancer treatment.[63] This study reported significant improvements in fatigue and several other aspects of quality of life for the intervention group versus usual care.
The qigong intervention was delivered in 90-minute group sessions, twice a week for 10 weeks, for 1,800 minutes of treatment. The usual-care group did not receive any group meetings or additional provider interaction. It is therefore difficult to say what qigong uniquely provided over and above nonspecific or group-interaction effects. It is also not known how much survivors would need to continue performing qigong to maintain benefits. There were no adverse events in this study, so other than time and resource expenditure, it is difficult to pinpoint a downside to encouraging patients to adopt such an activity. One important strength of the study was the collection of serum to measure markers of inflammation. At the end of 10 weeks, the C-reactive protein level of patients in the medical qigong group decreased by 3.6 mg/L, while patients in the usual-care group experienced an increase of 19.57 mg/L, a statistically significant difference.[63]
A second smaller study (N = 96) that compared a qigong group to a wait-list control group evaluated fatigue using the BFI as a secondary outcome; it also assessed a biological measure, salivary cortisol.[64] This study did not find any significant difference in fatigue or cortisol between groups. The intervention dose in this study, comprising five 40-minute sessions over 6 weeks of radiation therapy in women diagnosed with breast cancer, was much lower than the intervention dose in the larger study described above.
The major weakness limiting interpretation and integration of both of these studies, despite differing results, is that there was no attempt to control for attention or any of the social aspects of the intervention.
In a third small study (N = 76), men with prostate cancer undergoing radiation therapy were randomly assigned to qigong/tai chi, light exercise, or a waiting list.[65] The qigong/tai chi group reported improvements in sleep duration midway during radiation therapy treatment (6.7 hours vs. 7 hours); however, this effect was not durable. There were no differences between groups in fatigue or sleep outcomes, suggesting that this may not be an effective intervention during radiation therapy for prostate cancer. The symptoms of fatigue and poor sleep were highly correlated with the physical symptom burden of men with prostate cancer.[65]
Tai chi
Tai chi is a Chinese martial arts activity that involves deep breathing, exercise, and slow movement with a meditative aspect, connecting the individual’s physical, mental, and emotional states. Tai chi has been examined for its effect on cancer symptoms, including CRF.
Investigators conducted a randomized controlled trial to compare the effect of tai chi versus low-impact exercise on CRF during treatment for 91 lung cancer patients.[69] Tai chi sessions were conducted every other day for 12 weeks during each course of chemotherapy across four courses of treatment. Study assessments were conducted before the first and third courses of chemotherapy and at the end of the fourth course. Fatigue scores increased in all patients. However, in the tai chi group at 6 weeks, general and physical fatigue subscale scores were lower (P < .05) and vigor subscale scores were higher, compared with the scores of the exercise group (P < .05). These scores were also better in the tai chi group at 12 weeks (P < .05). No other differences existed between groups.[69]
In a subsequent meta-analysis, including six studies and more than 370 cancer patients, researchers noted significant and positive improvement in short-term CRF in patients with breast and lung cancer, but not in patients with prostate cancer.[70] A longer intervention period (>8 weeks) demonstrated greater improvements in CRF, and these effects were noted to be superior to the effects of physical exercise and psychological support. However, the effects of tai chi on long-term CRF remain unclear.
CBT
CBT has long been used to treat a variety of psycho-physiological problems, with therapy focusing on the thoughts (cognition) and functional behaviors relevant to the presenting problems. While most of the CBT research for CRF has focused on the survivor period, CBT and CBT variants (e.g., CBT-I and mindfulness-based cognitive therapy) have been shown to be useful during both active treatment and the survivor period.[46]
In the context of active treatment (e.g., chemotherapy, radiation therapy, surgery), CBT plus hypnosis may be effective for patients struggling with CRF.[71] Significant decreases in fatigue were reported over a 6-week course of psychotherapy during radiation therapy, compared with a control group. At a 6-month follow-up, the CBT group continued to experience significantly improved fatigue, compared with the control group.
In a randomized clinical trial, 98 mixed-type cancer survivors (intervention group = 50, wait-list control = 48) experiencing severe fatigue not attributable to a specific somatic cause were provided individual CBT.[72][Level of evidence: I] The CBT focused on each participant’s unique pattern of the following six possible factors that might perpetuate their post–cancer treatment fatigue:
Insufficient coping with the experience of cancer.
Fear of disease recurrence.
Dysfunctional cognition regarding fatigue.
Dysregulation of sleep.
Dysregulation of activity.
Low social support/negative social interactions.
The number of therapy sessions varied according to the number of perpetuating factors (range, 5–26 one-hour sessions; mean: 12.5 sessions). Results showed a clinically significant decrease in fatigue severity and functional impairment.
Fatigue-related improvements that occur during CBT for CRF can be maintained for extremely long periods of time, even without periodic, long-term follow-up (booster) sessions that are usually a component of CBT. In a 10-year follow-up of 81 individuals who completed a CRF CBT protocol,[73] fatigue levels increased among cancer survivors over the 10-year follow-up period, compared with the initial post-CBT assessment. In addition, at the 10-year follow-up, fatigue levels continued to be higher among cancer survivors compared with general-population controls. However, more than half of the cancer survivors (52%) who recovered from severe fatigue at the time of the post-CBT assessment maintained their low fatigue levels at the 10-year follow-up. While levels of fatigue deteriorated over time, the strong maintenance gains for more than half of the study population suggest that CBT for CRF can help control fatigue over long periods of time.
While CBT and medication therapy may often work hand in hand, some studies show that CBT alone has a more powerful impact on fatigue than medication alone. In a 7-week, double-blind treatment study,[24] 96 cancer survivors with cancer-related insomnia and fatigue were randomly divided into four groups:
CBT-I plus placebo (twice a day).
CBT-I plus armodafinil (50 mg twice a day).
Placebo alone (twice a day).
Armodafinil alone (50 mg twice a day).
The study found a significant reduction of fatigue with CBT alone or with CBT plus armodafinil (though the drug provided limited additive benefit compared with CBT alone), and no improvement with armodafinil alone.[24] Furthermore, the armodafinil group showed significantly less improvement than did the placebo-alone group.
Patient Education
Informing patients about the risk of fatigue and educating them about strategies to reduce fatigue are valuable adjuncts to other management strategies. However, a Cochrane review of educational interventions for CRF in adults cautions that educational interventions should be part of a more-comprehensive approach to managing fatigue.[74]
Specific techniques for the management of fatigue include the following:
Differentiation of fatigue from depression.
Assessment for presence of correctable correlates or causes of fatigue (e.g., dehydration, electrolyte imbalance, dyspnea, anemia).
Evaluation of patterns of rest and activity during the day as well as over time.
Determination of the level of attention fatigue and encouragement of attention-restoring activities (e.g., walking, gardening, bird watching).
Providing anticipatory guidance regarding the likelihood of experiencing fatigue and the fatigue patterns associated with particular treatments.
Encouragement of activity/planned exercise programs within individual limitations; making goals realistic by keeping in mind the state of disease and treatment regimens.
Education of individuals and families about fatigue related to cancer and its treatment.
Helping people with cancer and their families identify fatigue-promoting activities and develop specific strategies to modify these activities.
Suggesting individualized environmental or activity changes that may offset fatigue.
Maintaining adequate hydration and nutrition.
Recommending physical therapy referral for people with specific neuromusculoskeletal deficits.
Recommending respiratory therapy referral for people with dyspnea that is a contributing factor to fatigue.
Scheduling important daily activities during times of least fatigue and eliminating nonessential, stress-producing activities.
Addressing the negative impact of psychological and social stressors and how to avoid or reduce them.
Evaluating the efficacy of fatigue interventions on a regular and systematic basis.
In a controlled trial of patients who reported the symptom cluster of pain and fatigue while receiving chemotherapy, a nursing behavioral intervention produced improvements in quality of life and decreased symptom burden relative to usual care.[75,76][Level of evidence: I] These intriguing results need to be further explored in patient populations other than women with breast or gynecological malignancies.
As researchers and practitioners have learned with pain, misconceptions and a lack of knowledge may prove to be patient- and provider-related barriers to successful assessment and management. A quasi-experimental study tested a multisystem educational approach to improving both pain and fatigue management.[77] The approach consisted of the following:
Education and assessment of patients regarding the management of pain and fatigue, with phone calls every 2 weeks for 3 months.
Education of providers about pain and fatigue assessment and management, including monthly newsletters.
An effort to engage with an internal advisory board.
Efforts aimed toward research nurses to refer earlier to supportive care services.
Over a 3-month period, the educational intervention resulted in increases in knowledge and a decrease in barriers related to management of pain and fatigue. Of note, important patient barriers related to fatigue management included the following beliefs:[77][Level of evidence: II]
Fatigue is inevitable.
Fatigue can indicate worsening of disease.
Treating the cancer is more important than treating fatigue.
Reporting fatigue will cause a patient to be perceived as a complainer.
Providing patient education about strategies to reduce fatigue may help eliminate the barriers related to managing fatigue.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References
Arendt J, Borbely AA, Franey C, et al.: The effects of chronic, small doses of melatonin given in the late afternoon on fatigue in man: a preliminary study. Neurosci Lett 45 (3): 317-21, 1984. [PUBMED Abstract]
Glaspy J, Bukowski R, Steinberg D, et al.: Impact of therapy with epoetin alfa on clinical outcomes in patients with nonmyeloid malignancies during cancer chemotherapy in community oncology practice. Procrit Study Group. J Clin Oncol 15 (3): 1218-34, 1997. [PUBMED Abstract]
Gibson H, Edwards RH: Muscular exercise and fatigue. Sports Med 2 (2): 120-32, 1985 Mar-Apr. [PUBMED Abstract]
Hart LK: Fatigue in the patient with multiple sclerosis. Res Nurs Health 1 (4): 147-57, 1978.
de Raaf PJ, de Klerk C, Timman R, et al.: Systematic monitoring and treatment of physical symptoms to alleviate fatigue in patients with advanced cancer: a randomized controlled trial. J Clin Oncol 31 (6): 716-23, 2013. [PUBMED Abstract]
Armitage JO: Management of anemia in patients with cancer. Clinical Oncology Updates 1: 1-12, 1998.
Bohlius J, Bohlke K, Castelli R, et al.: Management of Cancer-Associated Anemia With Erythropoiesis-Stimulating Agents: ASCO/ASH Clinical Practice Guideline Update. J Clin Oncol 37 (15): 1336-1351, 2019. [PUBMED Abstract]
Lower EE, Fleishman S, Cooper A, et al.: Efficacy of dexmethylphenidate for the treatment of fatigue after cancer chemotherapy: a randomized clinical trial. J Pain Symptom Manage 38 (5): 650-62, 2009. [PUBMED Abstract]
Roth AJ, Nelson C, Rosenfeld B, et al.: Methylphenidate for fatigue in ambulatory men with prostate cancer. Cancer 116 (21): 5102-10, 2010. [PUBMED Abstract]
Jean-Pierre P, Morrow GR, Roscoe JA, et al.: A phase 3 randomized, placebo-controlled, double-blind, clinical trial of the effect of modafinil on cancer-related fatigue among 631 patients receiving chemotherapy: a University of Rochester Cancer Center Community Clinical Oncology Program Research base study. Cancer 116 (14): 3513-20, 2010. [PUBMED Abstract]
Yennurajalingam S, Bruera E: Review of clinical trials of pharmacologic interventions for cancer-related fatigue: focus on psychostimulants and steroids. Cancer J 20 (5): 319-24, 2014 Sep-Oct. [PUBMED Abstract]
Auret KA, Schug SA, Bremner AP, et al.: A randomized, double-blind, placebo-controlled trial assessing the impact of dexamphetamine on fatigue in patients with advanced cancer. J Pain Symptom Manage 37 (4): 613-21, 2009. [PUBMED Abstract]
Stone PC, Minton O, Richardson A, et al.: Methylphenidate Versus Placebo for Treating Fatigue in Patients With Advanced Cancer: Randomized, Double-Blind, Multicenter, Placebo-Controlled Trial. J Clin Oncol 42 (20): 2382-2392, 2024. [PUBMED Abstract]
Moraska AR, Sood A, Dakhil SR, et al.: Phase III, randomized, double-blind, placebo-controlled study of long-acting methylphenidate for cancer-related fatigue: North Central Cancer Treatment Group NCCTG-N05C7 trial. J Clin Oncol 28 (23): 3673-9, 2010. [PUBMED Abstract]
Kerr CW, Drake J, Milch RA, et al.: Effects of methylphenidate on fatigue and depression: a randomized, double-blind, placebo-controlled trial. J Pain Symptom Manage 43 (1): 68-77, 2012. [PUBMED Abstract]
Bruera E, Yennurajalingam S, Palmer JL, et al.: Methylphenidate and/or a nursing telephone intervention for fatigue in patients with advanced cancer: a randomized, placebo-controlled, phase II trial. J Clin Oncol 31 (19): 2421-7, 2013. [PUBMED Abstract]
Escalante CP, Meyers C, Reuben JM, et al.: A randomized, double-blind, 2-period, placebo-controlled crossover trial of a sustained-release methylphenidate in the treatment of fatigue in cancer patients. Cancer J 20 (1): 8-14, 2014 Jan-Feb. [PUBMED Abstract]
Richard PO, Fleshner NE, Bhatt JR, et al.: Phase II, randomised, double-blind, placebo-controlled trial of methylphenidate for reduction of fatigue levels in patients with prostate cancer receiving LHRH-agonist therapy. BJU Int 116 (5): 744-52, 2015. [PUBMED Abstract]
Mitchell GK, Hardy JR, Nikles CJ, et al.: The Effect of Methylphenidate on Fatigue in Advanced Cancer: An Aggregated N-of-1 Trial. J Pain Symptom Manage 50 (3): 289-96, 2015. [PUBMED Abstract]
Boele FW, Douw L, de Groot M, et al.: The effect of modafinil on fatigue, cognitive functioning, and mood in primary brain tumor patients: a multicenter randomized controlled trial. Neuro Oncol 15 (10): 1420-8, 2013. [PUBMED Abstract]
Hovey E, de Souza P, Marx G, et al.: Phase III, randomized, double-blind, placebo-controlled study of modafinil for fatigue in patients treated with docetaxel-based chemotherapy. Support Care Cancer 22 (5): 1233-42, 2014. [PUBMED Abstract]
Spathis A, Fife K, Blackhall F, et al.: Modafinil for the treatment of fatigue in lung cancer: results of a placebo-controlled, double-blind, randomized trial. J Clin Oncol 32 (18): 1882-8, 2014. [PUBMED Abstract]
Heckler CE, Garland SN, Peoples AR, et al.: Cognitive behavioral therapy for insomnia, but not armodafinil, improves fatigue in cancer survivors with insomnia: a randomized placebo-controlled trial. Support Care Cancer 24 (5): 2059-2066, 2016. [PUBMED Abstract]
Berenson JR, Yellin O, Shamasunder HK, et al.: A phase 3 trial of armodafinil for the treatment of cancer-related fatigue for patients with multiple myeloma. Support Care Cancer 23 (6): 1503-12, 2015. [PUBMED Abstract]
Medication Guide: PROVIGIL (modafinil) Tablets. North Wales, Pa: Teva Pharmaceuticals USA, Inc., 2015. Available online. Last accessed July 17, 2024.
Medication Guide: NUVIGIL (armodafinil) Tablets. North Wales, Pa: Teva Pharmaceuticals USA, Inc., 2017. Available online. Last accessed July 17, 2024.
Blackhall L, Petroni G, Shu J, et al.: A pilot study evaluating the safety and efficacy of modafinal for cancer-related fatigue. J Palliat Med 12 (5): 433-9, 2009. [PUBMED Abstract]
Spathis A, Dhillan R, Booden D, et al.: Modafinil for the treatment of fatigue in lung cancer: a pilot study. Palliat Med 23 (4): 325-31, 2009. [PUBMED Abstract]
CONCERTA (methylphenidate HCl) Extended-release Tablets. Titusville, NJ: Janssen Pharmaceuticals, Inc., 2023. Available online. Last accessed July 17, 2024.
Prommer E: Modafinil: is it ready for prime time? J Opioid Manag 2 (3): 130-6, 2006 May-Jun. [PUBMED Abstract]
ADDERALL XR (mixed salts of a single-entity amphetamine product), Extended-release Capsules, for Oral Use, CII. Lexington, Mass: Takeda Pharmaceutical America, Inc., 2023. Available online. Last accessed July 17, 2024.
Moss EL, Simpson JS, Pelletier G, et al.: An open-label study of the effects of bupropion SR on fatigue, depression and quality of life of mixed-site cancer patients and their partners. Psychooncology 15 (3): 259-67, 2006. [PUBMED Abstract]
Ashrafi F, Mousavi S, Karimi M: Potential Role of Bupropion Sustained Release for Cancer-Related Fatigue: a Double-Blind, Placebo-Controlled Study Asian Pac J Cancer Prev 19 (6): 1547-1551, 2018. [PUBMED Abstract]
Yennurajalingam S, Frisbee-Hume S, Palmer JL, et al.: Reduction of cancer-related fatigue with dexamethasone: a double-blind, randomized, placebo-controlled trial in patients with advanced cancer. J Clin Oncol 31 (25): 3076-82, 2013. [PUBMED Abstract]
Barton DL, Soori GS, Bauer BA, et al.: Pilot study of Panax quinquefolius (American ginseng) to improve cancer-related fatigue: a randomized, double-blind, dose-finding evaluation: NCCTG trial N03CA. Support Care Cancer 18 (2): 179-87, 2010. [PUBMED Abstract]
Barton DL, Liu H, Dakhil SR, et al.: Wisconsin Ginseng (Panax quinquefolius) to improve cancer-related fatigue: a randomized, double-blind trial, N07C2. J Natl Cancer Inst 105 (16): 1230-8, 2013. [PUBMED Abstract]
Budzinski JW, Foster BC, Vandenhoek S, et al.: An in vitro evaluation of human cytochrome P450 3A4 inhibition by selected commercial herbal extracts and tinctures. Phytomedicine 7 (4): 273-82, 2000. [PUBMED Abstract]
King ML, Adler SR, Murphy LL: Extraction-dependent effects of American ginseng (Panax quinquefolium) on human breast cancer cell proliferation and estrogen receptor activation. Integr Cancer Ther 5 (3): 236-43, 2006. [PUBMED Abstract]
Cruciani RA, Zhang JJ, Manola J, et al.: L-carnitine supplementation for the management of fatigue in patients with cancer: an eastern cooperative oncology group phase III, randomized, double-blind, placebo-controlled trial. J Clin Oncol 30 (31): 3864-9, 2012. [PUBMED Abstract]
Lesser GJ, Case D, Stark N, et al.: A randomized, double-blind, placebo-controlled study of oral coenzyme Q10 to relieve self-reported treatment-related fatigue in newly diagnosed patients with breast cancer. J Support Oncol 11 (1): 31-42, 2013. [PUBMED Abstract]
National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Cancer-Related Fatigue. Version 2.2024. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2024. Available online with registration. Last accessed July 17, 2024.
Cramp F, Daniel J: Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev (2): CD006145, 2008. [PUBMED Abstract]
Jacobsen PB, Donovan KA, Vadaparampil ST, et al.: Systematic review and meta-analysis of psychological and activity-based interventions for cancer-related fatigue. Health Psychol 26 (6): 660-7, 2007. [PUBMED Abstract]
Arring NM, Barton DL, Brooks T, et al.: Integrative Therapies for Cancer-Related Fatigue. Cancer J 25 (5): 349-356, 2019 Sep/Oct. [PUBMED Abstract]
Berger AM, Mitchell SA, Jacobsen PB, et al.: Screening, evaluation, and management of cancer-related fatigue: Ready for implementation to practice? CA Cancer J Clin 65 (3): 190-211, 2015 May-Jun. [PUBMED Abstract]
Pickett M, Mock V, Ropka ME, et al.: Adherence to moderate-intensity exercise during breast cancer therapy. Cancer Pract 10 (6): 284-92, 2002 Nov-Dec. [PUBMED Abstract]
Carayol M, Delpierre C, Bernard P, et al.: Population-, intervention- and methodology-related characteristics of clinical trials impact exercise efficacy during adjuvant therapy for breast cancer: a meta-regression analysis. Psychooncology 24 (7): 737-47, 2015. [PUBMED Abstract]
Alfano CM, Smith AW, Irwin ML, et al.: Physical activity, long-term symptoms, and physical health-related quality of life among breast cancer survivors: a prospective analysis. J Cancer Surviv 1 (2): 116-28, 2007. [PUBMED Abstract]
Rogers LQ, Courneya KS, Anton PM, et al.: Effects of a multicomponent physical activity behavior change intervention on fatigue, anxiety, and depressive symptomatology in breast cancer survivors: randomized trial. Psychooncology 26 (11): 1901-1906, 2017. [PUBMED Abstract]
Moy S, Kober KM, Viele C, et al.: Level of Exercise Influences the Severity of Fatigue, Energy Levels, and Sleep Disturbance in Oncology Outpatients Receiving Chemotherapy. Cancer Nurs 45 (1): 3-11, 2022 Jan-Feb 01. [PUBMED Abstract]
Yoshioka H: Rehabilitation for the terminal cancer patient. Am J Phys Med Rehabil 73 (3): 199-206, 1994. [PUBMED Abstract]
Mock V, Frangakis C, Davidson NE, et al.: Exercise manages fatigue during breast cancer treatment: a randomized controlled trial. Psychooncology 14 (6): 464-77, 2005. [PUBMED Abstract]
Peters ME, Goedendorp MM, Verhagen SA, et al.: Exploring the contribution of psychosocial factors to fatigue in patients with advanced incurable cancer. Psychooncology 23 (7): 773-9, 2014. [PUBMED Abstract]
Mutrie N, Campbell AM, Whyte F, et al.: Benefits of supervised group exercise programme for women being treated for early stage breast cancer: pragmatic randomised controlled trial. BMJ 334 (7592): 517, 2007. [PUBMED Abstract]
van Waart H, Stuiver MM, van Harten WH, et al.: Effect of Low-Intensity Physical Activity and Moderate- to High-Intensity Physical Exercise During Adjuvant Chemotherapy on Physical Fitness, Fatigue, and Chemotherapy Completion Rates: Results of the PACES Randomized Clinical Trial. J Clin Oncol 33 (17): 1918-27, 2015. [PUBMED Abstract]
Cramp F, Byron-Daniel J: Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev 11: CD006145, 2012. [PUBMED Abstract]
Steindorf K, Schmidt ME, Klassen O, et al.: Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: results on cancer-related fatigue and quality of life. Ann Oncol 25 (11): 2237-43, 2014. [PUBMED Abstract]
Juvet LK, Thune I, Elvsaas IKØ, et al.: The effect of exercise on fatigue and physical functioning in breast cancer patients during and after treatment and at 6 months follow-up: A meta-analysis. Breast 33: 166-177, 2017. [PUBMED Abstract]
Hilfiker R, Meichtry A, Eicher M, et al.: Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: a systematic review incorporating an indirect-comparisons meta-analysis. Br J Sports Med 52 (10): 651-658, 2018. [PUBMED Abstract]
Mazzoni AS, Strandberg E, Börjeson S, et al.: Reallocating sedentary time to physical activity: effects on fatigue and quality of life in patients with breast cancer in the Phys-Can project. Support Care Cancer 31 (2): 151, 2023. [PUBMED Abstract]
Oh B, Butow P, Mullan B, et al.: Impact of medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: a randomized controlled trial. Ann Oncol 21 (3): 608-14, 2010. [PUBMED Abstract]
Chen Z, Meng Z, Milbury K, et al.: Qigong improves quality of life in women undergoing radiotherapy for breast cancer: results of a randomized controlled trial. Cancer 119 (9): 1690-8, 2013. [PUBMED Abstract]
McQuade JL, Prinsloo S, Chang DZ, et al.: Qigong/tai chi for sleep and fatigue in prostate cancer patients undergoing radiotherapy: a randomized controlled trial. Psychooncology 26 (11): 1936-1943, 2017. [PUBMED Abstract]
Lin PJ, Kleckner IR, Loh KP, et al.: Influence of Yoga on Cancer-Related Fatigue and on Mediational Relationships Between Changes in Sleep and Cancer-Related Fatigue: A Nationwide, Multicenter Randomized Controlled Trial of Yoga in Cancer Survivors. Integr Cancer Ther 18: 1534735419855134, 2019 Jan-Dec. [PUBMED Abstract]
Bower JE, Garet D, Sternlieb B, et al.: Yoga for persistent fatigue in breast cancer survivors: a randomized controlled trial. Cancer 118 (15): 3766-75, 2012. [PUBMED Abstract]
Kiecolt-Glaser JK, Bennett JM, Andridge R, et al.: Yoga’s impact on inflammation, mood, and fatigue in breast cancer survivors: a randomized controlled trial. J Clin Oncol 32 (10): 1040-9, 2014. [PUBMED Abstract]
Zhang LL, Wang SZ, Chen HL, et al.: Tai Chi Exercise for Cancer-Related Fatigue in Patients With Lung Cancer Undergoing Chemotherapy: A Randomized Controlled Trial. J Pain Symptom Manage 51 (3): 504-11, 2016. [PUBMED Abstract]
Song S, Yu J, Ruan Y, et al.: Ameliorative effects of Tai Chi on cancer-related fatigue: a meta-analysis of randomized controlled trials. Support Care Cancer 26 (7): 2091-2102, 2018. [PUBMED Abstract]
Montgomery GH, David D, Kangas M, et al.: Randomized controlled trial of a cognitive-behavioral therapy plus hypnosis intervention to control fatigue in patients undergoing radiotherapy for breast cancer. J Clin Oncol 32 (6): 557-63, 2014. [PUBMED Abstract]
Gielissen MF, Verhagen S, Witjes F, et al.: Effects of cognitive behavior therapy in severely fatigued disease-free cancer patients compared with patients waiting for cognitive behavior therapy: a randomized controlled trial. J Clin Oncol 24 (30): 4882-7, 2006. [PUBMED Abstract]
Van Gessel LD, Abrahams HJG, Prinsen H, et al.: Are the effects of cognitive behavior therapy for severe fatigue in cancer survivors sustained up to 14 years after therapy? J Cancer Surviv 12 (4): 519-527, 2018. [PUBMED Abstract]
Bennett S, Pigott A, Beller EM, et al.: Educational interventions for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev 11: CD008144, 2016. [PUBMED Abstract]
Given B, Given CW, McCorkle R, et al.: Pain and fatigue management: results of a nursing randomized clinical trial. Oncol Nurs Forum 29 (6): 949-56, 2002. [PUBMED Abstract]
Ream E, Richardson A, Alexander-Dann C: Supportive intervention for fatigue in patients undergoing chemotherapy: a randomized controlled trial. J Pain Symptom Manage 31 (2): 148-61, 2006. [PUBMED Abstract]
Borneman T, Koczywas M, Sun VC, et al.: Reducing patient barriers to pain and fatigue management. J Pain Symptom Manage 39 (3): 486-501, 2010. [PUBMED Abstract]
Latest Updates to This Summary (11/06/2024)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Updated Table 3, Centrally Acting Stimulants for Adult Cancer Patients, to add new information about methylphenidate to treat cancer-related fatigue (cited Stone et al. as reference 14 and level of evidence I).
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the pathophysiology and treatment of fatigue. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Supportive and Palliative Care Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Fatigue are:
Katharine Brock, MD, MS (Children’s Healthcare of Atlanta)
Marilyn J. Hammer, PhD, DC, RN, FAAN (Dana-Farber Cancer Institute)
Jayesh Kamath, MD, PhD (University of Connecticut Health Center)
Diane Von Ah, PhD, RN, FAAN (The Ohio State University)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Supportive and Palliative Care Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Supportive and Palliative Care Editorial Board. PDQ Fatigue. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /side-effects/fatigue/fatigue-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389484]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Good nutrition during cancer treatment is important to help you stay strong.
Credit: iStock
What is nutrition?
Nutrition is what you eat and drink and how your body uses it. Good nutrition is important for good health. A healthy diet includes a variety of foods and liquids that have nutrients (vitamins, minerals, proteins, carbohydrates, fats, and water) your body needs.
Good nutrition for people with cancer may differ from what we think of as healthy
People with cancer often need to follow diets that are different from what we think of as healthy. For most people, a healthy diet includes lots of whole grains, fruits and vegetables, modest amounts of protein, and small amounts of sugar, alcohol, salt, and unhealthy fats.
When you have cancer, though, you may need extra protein and calories. To eat enough protein and calories, your diet may need to include more meat, fish, eggs, dairy, fats, and plant-based proteins than someone without cancer. The extra protein and calories will help you keep your strength up to deal with the side effects of treatment, prevent malnutrition, and maintain your best possible quality of life.
A registered dietitian can help make sure you get the right amount of protein and calories during and after cancer treatment. They will work with you, your family, and the rest of your medical team to help manage your diet.
During treatment, you may be tired and not feel well. Being tired can make it harder to grocery shop, cook, and eat. Planning meals before treatment will make it easier to eat during treatment.
To plan meals and snacks before treatment, try these tips.
Shopping tips:
Fill the refrigerator, pantry, and freezer with healthy foods, especially those high in protein and calories.
Stock up on foods that need little or no cooking, such as frozen foods.
Use online grocery shopping and save your list for easy reordering.
Use delivery or shop-from-home grocery stores.
Meal prep tips:
Keep easy-to-digest snacks on hand for when you feel sick. Pretzels and crackers are good examples.
Cook foods ahead of time and freeze them in meal-sized portions.
Tips for accepting help from others:
Ask friends or family to help you shop and cook during treatment.
If people offer to grocery shop for you, let them.
Create a grocery list of items to give to friends and family.
Both cancer and cancer treatments may cause side effects that affect your taste, smell, appetite, and ability to eat enough food or absorb the nutrients from food. This can lead to malnutrition.
People with certain cancers are more likely to have problems eating. These cancers include those that affect your digestive system directly, such as cancers of the head and neck, esophagus, stomach, pancreas, liver, or colon. But people with any type of cancer can find it hard to eat well because of the effects of cancer treatment.
When malnutrition is not managed in people having cancer treatment, it can lead to cancer cachexia. Cancer cachexia is a wasting syndrome that can cause weakness, weight loss, and fat and muscle loss. It can occur even when you are eating well.
Chemotherapy uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. But these drugs may also kill healthy cells that grow and divide quickly, such as cells in the mouth and digestive tract. This can cause eating problems and other side effects, including:
Hormone therapy may be used to slow or stop cancers that rely on hormones to grow, like breast, ovarian, and prostate cancer. Hormone therapy adds, blocks, or removes these hormones. These drugs can cause weight gain and other side effects, including:
Immunotherapy uses your immune system to fight cancer. The side effects of immunotherapy are different for each person and depend on the type of immunotherapy drug.
Immunotherapy may cause fatigue, which can lead to a poor appetite. Learn more about Cancer Fatigue.
Common nutrition-related side effects caused by immunotherapy include:
Radiation therapy kills cancer cells and healthy cells in the area that is being treated.
Radiation therapy to any part of your digestive system has side effects that cause eating problems. Most of the side effects begin 2 to 3 weeks after radiation therapy begins and go away a few weeks after it is finished. But some side effects can last for months or years after treatment ends. Learn more about Late Effects of Cancer Treatment.
Fatigue, which can lead to a poor appetite, is a common side effect of radiation therapy. Learn more about Cancer Fatigue.
Radiation therapy to the brain or head and neck may cause:
loss of appetite
nausea and vomiting
dry mouth or thick saliva
sore mouth and gums
changes in the way food tastes
trouble swallowing
pain when swallowing
being unable to fully open the mouth
Radiation therapy to the chest may cause:
loss of appetite
nausea and vomiting
trouble swallowing
pain when swallowing
choking or breathing problems caused by changes in the upper esophagus
People who have a stem cell transplant have special nutrition needs. Medications used before or during a stem cell transplant may cause side effects that keep you from eating and digesting food as usual.
Common nutrition-related side effects caused by stem cell transplant include:
mouth and throat sores
diarrhea
If you have a stem cell transplant, you have a high risk of infection, including from food (foodborne illness). That is because treatment given before your transplant reduces the number of your white blood cells, which fight infection. It is important that you and your caregivers learn about how to safely prepare food and how to avoid foods that may cause infection.
After a stem cell transplant, you are also at risk of acute or chronic graft-versus-host disease (GVHD). GVHD may affect your digestive tract, skin, or liver and change your ability to eat or absorb nutrients from food.
Surgery is a common part of cancer treatment. Surgery that removes all or part of certain organs can affect your ability to eat and digest food. After any surgery, your body needs extra energy and nutrients to heal wounds, fight infection, and recover. If you are malnourished before surgery, you may have trouble healing.
Common nutrition-related side effects caused by surgery include:
loss of appetite
trouble chewing
trouble swallowing
feeling full after eating a small amount of food, also known as early satiety
Targeted therapy is a type of cancer treatment that targets proteins that control how cancer cells grow, divide, and spread. It may disturb normal function of your digestive system and cause:
Some cancer treatments make it easier for you to get sick from contaminated food. Our 8 tips for food safety during cancer treatment can help you properly handle and prepare food to reduce your risk of foodborne illness.
Some cancer treatments can weaken your immune system. This makes it harder for you to fight infections, including foodborne illnesses. So, you need to take special care in the way you handle and prepare food during your cancer treatment. Keep foods at safe temperatures, scrub raw vegetables and fruits, and be careful to use separate utensils, plates, and cutting boards when preparing meats and produce. Learn more about food safety for people with weakened immune systems.
Nutrition screening and assessment during cancer treatment
If you have trouble eating and maintaining your weight, your nurse, doctor, or registered dietitian may ask you a series of questions to find out if you are malnourished or are likely to become so.
To assess your nutrition status, you may be asked about:
weight changes
changes in the amount of food you eat
changes in types of food you eat
problems with eating, like nausea or vomiting
your ability to walk or do other daily activities
If you are at risk of poor nutrition or malnutrition, your doctor will refer you to a registered dietitian. A registered dietitian can do an assessment, which reviews your:
food and diet history
medication history
personal, medical, family, and social history
height and weight
lab tests
side effects of treatment
physical exam
Based on this information, the registered dietitian will create a nutrition care plan. This plan includes ways you and your family can improve your eating and address any nutrition problems that you are having.
Ways to manage nutrition problems caused by cancer treatments
When side effects of cancer or cancer treatment affect normal eating, there are ways to help you get the nutrients you need.
Ways to manage appetite loss, weight loss, and early satiety
If you have loss of appetite, weight loss, or feel full too quickly, these tips may help:
Drink most of your fluids between meals, not during meals. Small sips at mealtime are okay.
Drink milkshakes, smoothies, juices, or soups if you do not feel like eating solid foods.
Eat foods that smell good.
Try new foods and new recipes.
Use a blender to make high-calorie, high-protein drinks.
Try nutrition supplements, such as Ensure or Boost.
Aim to eat smaller meals and snacks five to six times a day.
Eat your largest meal when your appetite is strongest, whether that’s breakfast, lunch, or dinner.
Make and store small amounts of your favorite foods so they are ready to eat when you are hungry.
Find a physical activity you enjoy and will stick with to help increase your appetite.
If you continue to struggle to eat and keep up your weight, you and your treatment team can discuss other nutrition support options. These options may include tube feeding or IV nutrition.
Nausea is when you feel sick to your stomach, as if you have the urge to throw up. Vomiting is when you throw up. Nausea and vomiting are common side effects of cancer treatments, including chemotherapy and radiation therapy. But there are medicines that often prevent or relieve nausea and vomiting before they start or become a problem.
When you vomit, you may become dehydrated and lose a lot of electrolytes. Electrolytes are minerals, such as potassium, sodium, and calcium that help balance body fluids and support your heart, nerve, and muscle functions. Talk to your dietitian about which drinks can help prevent dehydration and how much you should drink.
Dry mouth occurs when you have less saliva than you used to. Having less saliva can make it harder to talk, chew, and swallow food. Dry mouth can also change the way food tastes.
Chemotherapy and radiation therapy to the head or neck can damage the glands that make saliva. Immunotherapy and some medicines can also cause dry mouth.
If you have dry mouth:
Moisten food with sauce, salsa, gravy, or salad dressing.
Cancer treatments can harm fast-growing cells in your mouth. Radiation therapy to the head or neck, chemotherapy, and immunotherapy can cause mouth sores (little cuts or ulcers in your mouth) and tender gums. Dental problems or mouth infections, such as thrush, can also make your mouth sore. Visit a dentist at least 2 weeks before starting immunotherapy, chemotherapy, or radiation therapy to the head and neck.
Your mouth and gums will most likely feel better once cancer treatment ends.
Use a blender or food processor to make food smooth.
Suck on ice chips to numb and soothe your mouth.
Eat foods cold or at room temperature. Hot foods can hurt your mouth.
Drink with a straw to move liquid past the painful parts of your mouth.
Use a small spoon to help you take smaller bites, which are easier to chew.
Check your mouth each day for sores, white patches, or puffy and red areas.
Rinse your mouth three to four times a day. Mix ¼ teaspoon baking soda, ⅛ teaspoon salt, and 1 cup warm water for a mouth rinse.
Talk to your doctor about medicine to numb your mouth. This may make eating easier.
Avoid:
citrus fruits, such as oranges, lemons, and limes
spicy foods
tomatoes and ketchup
salty foods
raw vegetables
sharp and crunchy foods
drinks with alcohol
mouthwash that contains alcohol
tobacco products
electronic cigarettes
toothpicks or sharp objects
Ways to manage sore throat and trouble swallowing
Chemotherapy and radiation therapy to the head and neck can make the lining of your throat inflamed and sore, a problem called esophagitis. It may feel as if you have a lump in your throat or that your chest or throat is burning. You may also have trouble swallowing. These problems may make it hard to eat and cause weight loss.
Some types of chemotherapy and radiation to the head and neck can harm fast-growing cells, such as those in the lining of your throat. Your risk of sore throat, trouble swallowing, or other throat problems depends on:
how much radiation you are getting
if you are getting chemotherapy and radiation therapy at the same time
whether you use tobacco or drink alcohol during cancer treatment
Sit upright and bend your head slightly forward when you eat or drink. Stay upright for at least 30 minutes after eating.
Do not use tobacco or electronic cigarettes.
Stay away from the foods and drinks that can burn or scratch your throat, such as:
hot foods and drinks
spicy foods
foods and juices that are high in acid, such as citrus, pineapple, and tomatoes
sharp or crunchy foods
drinks with alcohol
carbonated drinks
Talk to your doctor about tube feedings if you cannot eat enough to stay strong.
Ways to manage taste and smell changes
Improving Taste and Smell During Cancer Treatment
Cancer and its treatment can cause changes in taste or smell that can make it hard to eat. Try our tips to deal with these changes.
Cancer treatment, dental problems, or the cancer itself can cause changes in your sense of taste or smell. Food may have less taste or certain foods (like meat) may be bitter or taste like metal. Sometimes, foods that used to smell good to you no longer do.
Although there is no way to prevent these problems, there are things you can do to manage them. And often they get better after treatment ends.
Ways to manage a salty taste:
Try low-sodium or sodium-free seasoning products, like Mrs. Dash.
Use herbs, spices, and seasonings in place of salt when cooking.
Pick naturally sweet foods, like fresh or dried fruit.
Avoid eating out or getting take-out because restaurants often prepare foods with a lot of salt.
Boil food, as this reduces salty flavors.
Add a pinch of sugar or honey to foods.
Ways to manage an overly sweet taste:
Eat more vegetables.
Add water and ice to dilute sweet juices. Try mixing half juice and half water.
Eat sour foods, like grapefruit.
Add a pinch of salt to food to offset the sweetness.
Add vinegar or citrus to foods to reduce sweetness.
Ways to manage a loss of taste or “off” taste:
Choose fresh produce.
Try foods with fruity, tart, or salty flavors.
Use marinades on meats to add flavor. Marinate the meat in your refrigerator overnight for more flavor.
Add vinegars, fresh fruit juices, cheese, salad dressing, and sauces to foods.
Add fresh or dried herbs, like basil, oregano, thyme, rosemary, mint, or sage.
Add spices, like onion and garlic powder, paprika, ground turmeric, ground ginger, or curry powder.
Add condiments, like mayonnaise, relish, ketchup, mustard, or salsa.
Chew food longer to allow more contact with taste buds.
Ways to manage bitter and metallic tastes:
Use plastic, silicone, wooden, or bamboo silverware.
Suck or chew on sugar-free candies, mints, or gum.
Do not buy prepackaged food in metal containers, such as canned beans. Look for cardboard, glass, or plastic packaging.
Do not drink from metal containers or use metal silverware.
Try plant-based protein sources, like tofu, nuts, or beans.
If red meat tastes metallic, try chicken, turkey, or dairy foods.
Find nonmeat, high-protein recipes in vegetarian, Chinese, or Indian cookbooks.
Drink sweet or sour beverages, like cherry, cranberry, pineapple, or grape juice.
Eat fresh and dried fruits, like mango, peaches, watermelon, dates, or figs.
Add sweetness to foods with a pinch of sugar, honey, or maple syrup.
Ways to manage smell changes:
Keep foods covered until ready to eat.
Drink from cups with lids and drink through a straw.
Turn a kitchen fan on when cooking, or cook outdoors if smells bother you.
Avoid strong odors, such as brussels sprouts or fish.
Make or eat foods that don’t need to be cooked, such as:
protein shakes
protein bars
smoothies
cereal with fruit and milk
pudding
Greek yogurt parfaits
sandwiches
Types of nutrition support if you cannot eat
Sometimes, despite your best efforts, you may not be able to eat enough to stay strong. If this happens, nutrition support through a feeding tube may be a good option. Nutrition support helps if you cannot eat or digest enough food to stay nourished. Staying nourished helps increase the chance of receiving treatment without unplanned breaks.
Your doctor or dietitian will discuss nutrition support with you if they think it will help.
There are two types of nutrition support, enteral and parenteral nutrition.
Enteral nutrition
Enteral nutrition gives you nutrients in liquid form through a tube that is placed into the stomach or small intestine. There are two types of feeding tubes:
A nasogastric tube is inserted through the nose and down the throat into the stomach or small intestine. This is used when nutrition support is needed for only a few weeks.
A gastrostomy tube is inserted into the stomach, or a jejunostomy tube is inserted into the small intestine through an opening made on the outside of the abdomen. Feeding tubes of this type are usually used for long-term enteral feeding or for people who cannot use a tube in the nose and throat.
A central venous catheter is a thin, flexible tube that is inserted into a vein, usually below the right collarbone, and guided into a large vein above the right side of the heart called the superior vena cava.
The type of formula used is based on your specific nutritional needs. There are formulas for people with special health conditions, such as diabetes, or with other needs, such as observing religious or cultural norms.
Some people can still eat by mouth when using enteral nutrition. Before doing so, it is important to ask your doctor if it is safe for you.
Parenteral nutrition
Parenteral nutrition is used when you cannot take food by mouth or use a feeding tube. Parenteral feeding does not use the stomach or intestines to digest food. Nutrients are given to you directly into the blood through a catheter inserted into a vein. These nutrients include proteins, fats, vitamins, and minerals.
As with enteral feeding, some people can eat by mouth when using parenteral nutrition. Ask your doctor if it is safe to eat by mouth while receiving parenteral nutrition.
The catheter may be placed into a vein in the chest or in the arm.
A central venous catheter is placed beneath your skin and into a large vein in the upper chest. The catheter is put in place by a surgeon. This type of catheter is used for long-term parenteral feeding.
A peripheral venous catheter is a thin, flexible tube that is inserted into a vein. It is usually inserted into the lower part of the arm or the back of the hand.
A peripheral venous catheter is placed into your vein in the arm. A peripheral venous catheter is put in place by trained medical staff. This type of catheter is usually used for short-term parenteral feeding or if you do not have a central venous catheter.
You will be checked often for infection or bleeding at the place where the catheter enters the body.
Nutrition therapy for the end of life
If you are nearing the end of life, the goal is to provide the best possible quality of life and control symptoms that cause discomfort. Your nutrition goals will be specific to you.
Common symptoms that can occur at the end of life include:
The focus is on relieving these symptoms, rather than getting enough nutrients.
You and your family can decide how much nutrition and fluids you will be given at the end of life
People at the end of life often do not feel much hunger at all and may want very little food. Sips of water, ice chips, and mouth care can help with thirst. Food and fluids should not be forced on someone who is at the end of life. Doing so can cause discomfort or choking.
You and your loved ones have the right to make informed decisions. Your religious and cultural preferences may affect your decisions. The health care team and a registered dietitian can explain nutrition needs and the benefits and risks of using tube feeding or IV nutrition at the end of life.
Possible benefits of nutrition support for people expected to live longer than a month include:
improved quality of life
less risk of death due to malnutrition
fewer physical and mental problems
The risks of nutrition support at the end of life include:
Many medicines are available to prevent and control nausea and vomiting from cancer treatments. Your doctor will help you find medicines and other ways of managing these side effects that work best for you.
Credit: iStock
What are nausea and vomiting?
Nausea is when you feel sick to your stomach, as if you have the urge to throw up. Vomiting is when you throw up. Nausea and vomiting are common side effects of cancer treatments, including chemotherapy (chemo) and radiation therapy, but antinausea medicines often prevent or relieve nausea and vomiting before they start or become a problem.
If uncontrolled, vomiting can lead to serious health problems such as dehydration, electrolyte imbalances, and weight loss. Before you begin treatment, your doctor may suggest medications and tips to prevent and control these side effects.
Nausea and vomiting can occur at different times during cancer treatment:
Acute nausea and vomiting happen within 24 hours after treatment starts.
Delayed nausea and vomiting happen 1 to 7 days after treatment. This is also called late nausea and vomiting.
Anticipatory nausea and vomiting happen before treatment begins. If you have had nausea and vomiting after an earlier treatment session, the smells, sights, and sounds of the treatment room during a later session may trigger nausea and vomiting before the session begins.
Chronic nausea and vomiting are ongoing after treatment ends.
Nausea and vomiting may also be described based on how well antinausea medicines work against them:
Breakthrough nausea and vomiting happen within 5 days of starting antinausea treatment.
Refractory nausea and vomiting do not get better with antinausea medications.
What causes nausea and vomiting in people with cancer?
Cancer and cancer treatments can cause nausea and vomiting. Other causes include anxiety, pain medicines, taking certain medications on an empty stomach, and other medical conditions.
Nausea and vomiting from cancer
Nausea and vomiting may be a sign or symptom of some types and stages of cancer:
Many cancer treatments cause nausea and vomiting, but antinausea medicines (also known as antiemetics) given before treatment sessions work well to prevent or reduce these side effects.
Chemotherapy often causes nausea and vomiting. Nausea and vomiting from chemo may begin a few minutes to a few hours after treatment begins or be delayed and occur a day or more after treatment. Nausea and vomiting from chemotherapy usually last 24 to 48 hours, but some people may feel sick for up to 7 days after treatment. You will usually receive antinausea medicines before chemotherapy starts because once nausea and vomiting from chemotherapy develop, they are more difficult to treat.
Radiation therapy can cause nausea and vomiting, especially when radiation is directed at the brain, upper abdomen, or whole body. People receiving higher doses of radiation may be more likely to experience these side effects. You may begin feeling sick a few hours after each treatment session, and nausea and vomiting may last for three to four weeks.
Targeted therapy and immunotherapy drugs can bring on nausea and vomiting. You may start to feel sick during treatment or after it has ended. As with chemotherapy, it’s important to prevent nausea and vomiting by taking antinausea medicines before treatment starts.
Bone marrow or stem cell transplant can cause nausea and vomiting because you will receive large amounts of chemo, radiation, or both before a transplant. Nausea and vomiting can also be signs of graft-versus-host disease or infection, which are possible complications of bone marrow transplants.
Surgery may lead to nausea and vomiting caused by side effects of anesthesia and pain medicines given after surgery. Nausea and vomiting after surgery may last 24 to 48 hours.
How to prevent and stop nausea and vomiting
Medicines for nausea and vomiting
Medicines called antiemetics (or antinausea drugs) work well to prevent and relieve nausea and vomiting in people with cancer. Your doctor may prescribe multiple types of antiemetics you can take depending on the severity of your nausea and vomiting. Your doctor will also tell you when to take the antiemetics, such as before or after chemotherapy treatments or a certain amount of time before eating.
Many types of antiemetics can prevent or help you get relief from nausea and vomiting, and you may be prescribed these or others that are not listed:
drugs that block dopamine, a chemical in the brain that can trigger nausea and vomiting: chlorpromazine, prochlorperazine (Compazine), promethazine (Phenergan), metoclopramide (Reglan)
drugs that block the NK-1 receptor, a protein in the brain that can trigger nausea and vomiting: aprepitant or fosaprepitant (Emend)
antipsychotics, which block multiple areas in the brain that can cause nausea and vomiting: olanzapine (Zyprexa)
cannabinoids, which contain THC and can help relieve nausea and vomiting: dronabinol (Marinol)
Tips for managing nausea and vomiting
In addition to prescribing antinausea medicines, your doctor may suggest tips for managing nausea and vomiting. These tips may sometimes be called natural nausea relief.
Drink plenty of fluids. Drinking water or clear liquids will help prevent dehydration, a serious problem that happens when your body loses too much fluid from vomiting and you are not drinking enough. Try to sip on water, broth, fruit juices, ginger ale, tea, and/or sports drinks throughout the day. If you are losing weight without trying, drink fluids with calories instead of water.
Eat foods that are easy on your stomach. Try cold foods such as popsicles, pudding, yogurt, and gelatin. Try bland, starchy foods such as toast, rice, plain pasta, crackers, and pretzels. Foods and beverages with ginger, such as ginger ale and ginger tea, may also ease nausea and vomiting. Learn more about eating tips to help you avoid nausea and vomiting while you are undergoing cancer treatment at Nutrition in Cancer Care in the Treatment of Symptoms section.
Avoid certain foods. Don’t eat greasy, fried, sweet, or spicy foods if you feel sick after eating them.
Avoid strong odors when eating. Foods with strong odors you may want to avoid include coffee, fish, onions, and garlic. If the smell of food bothers you, ask others to make your food. Eating in a well-ventilated room free of strong food smells, perfume, or scented candles may also help.
Eat smaller meals more frequently throughout the day. Try to eat five to six small meals rather than three larger meals.
Eat in a peaceful, relaxing space. After eating, try resting while seated upright or lying down with your head elevated for 30 minutes to help reduce nausea and vomiting.
Keep a record of when you feel nauseous and what you did or ate before that. This can help your doctor or nurse figure out what brings on nausea and vomiting.
Acupressure can help relieve nausea when used together with medication. One easy-to-find acupressure point is on your wrist. Before trying acupressure, ask your doctor if it’s safe for you.
Practice relaxation techniques. Deep breathing, guided imagery, hypnosis, massages, listening to music, and meditating can all help reduce nausea and vomiting in people with cancer. Ask your nurse about programs that may be available in your community or at the hospital where you are receiving treatment.
Ask your doctor about acupuncture and acupressure. Acupuncture uses needles to stimulate certain points in the body that can help relieve symptoms and must be done by a professional acupuncturist. You can do acupressure on yourself by finding a specific point in your wrist and applying pressure. You can also wear Sea-Band wristbands, which stimulate acupressure points, and may help relieve nausea.
If you want to try supplements or complementary and alternative medicines to ease nausea and vomiting, always check with your doctor first. Some supplements and alternative therapies may cause cancer treatments to work less well.
How a caregiver can help
Make meals for the person you are caring for if they are feeling nauseous or if the smell of food makes their symptoms worse. Be sure the kitchen is ventilated to decrease food smells.
Have the person eat with plastic utensils instead of metal ones, which can taste bitter. Finger foods are also an option.
Ask the person’s doctor about medicines that can help reduce or prevent nausea and vomiting.
Help the person you are caring for take their antinausea medicine at the right times. For example, the doctor may recommend some medicines be taken before or after treatment or a certain amount of time before a meal.
Monitor the person for dizziness, weakness, or confusion, which are all signs of dehydration.
Encourage the person to sip clear liquids slowly throughout the day to avoid constipation and dehydration, which can worsen nausea and vomiting.
Nausea and vomiting in children being treated for cancer
Nausea and vomiting are serious side effects of cancer treatment for children. You can learn about how to help your child avoid nausea and vomiting during cancer treatment in our booklet Children with Cancer: A Guide for Parents in the section Common Health Problems.
Nausea and vomiting in children can be treated with many of the same medicines and techniques used in adults. But not all medicines for adults are safe for children to take, and children are often given lower doses.
Doctors have also found that several integrative therapies may be especially effective for treating nausea and vomiting in children:
hypnosis and guided imagery
music therapy
support groups
virtual reality games
Be aware of delayed nausea and vomiting in children being treated for cancer
Delayed nausea, or nausea and vomiting that happens more than 24 hours after a cancer treatment, may be more difficult to notice in children than in adults. A change in the child’s eating pattern may be the only sign of a problem. In addition, most chemotherapy treatments for children are scheduled over several days. This makes the timing and risk of delayed nausea difficult to predict.
Talk with your child’s health care team if your child has nausea or vomiting or if you notice a sudden change in their eating habits. Your child’s doctors can help you determine if these changes are related to the cancer treatment and identify strategies to help manage them.
Talking with your doctor about nausea and vomiting
If you are experiencing nausea and vomiting or are worried about having these side effects, tell your health care team. They can help you find ways to get relief or prevent nausea and vomiting before it starts.
Questions to ask your provider about nausea and vomiting:
What symptoms or problems should I call you about?
What medicine could help me? When should I take this medicine?
How much liquid should I drink each day? What should I do if I throw up?
What foods would be easy on my stomach? What foods should I avoid?
What specialists could I see to learn about acupuncture and other natural treatments that could improve my symptoms?
Radiation Therapy Audio Transcript
What To Do About Nausea and Vomiting
Narrator: What to do about nausea and vomiting during radiation therapy.
Do you have an upset stomach or are you vomiting? Rodney offers tips from his nurse that helped him. Let’s hear what he has to say.
Rodney: I think there is one thing we can all agree on—vomiting is no good. There were days during radiation therapy that I was just so sick. So, I called my doctor, and he prescribed some medicine that helped a lot.
In addition to getting and taking medicine that helped a lot, my nurse gave me 3 tips. I did these things on days when it was hard to keep food down, and I want to share them with you.
Tip 1: Eat small meals – 5 or 6 small meals stayed down easier for me than 3 big meals.
Tip 2: Try drinks and foods that are easy on the stomach. Clear soft drinks, crackers, and plain toast are easy to digest.
Tip 3: Sit up or go for a short walk after eating.
Try these tips. They worked for me. I hope they can help you prevent nausea and vomiting, too.
Oh, it also helped to have a small snack before treatment. That seemed to work best for me. But one of the guys in the waiting room said that it worked best for him to avoid eating or drinking before treatment. Talk with your doctor to learn what might work best for you.
Narrator Summary: Feeling sick to your stomach and vomiting can cause you to lose fluids that your body needs. Talk with your doctor or nurse if you are vomiting and cannot keep down fluids. There is medicine that can help. So can following the 3 tips from Rodney’s nurse:
Tip number 1: Eat 5 or 6 small meals a day.
Tip number 2: When you are feeling sick to your stomach, choose drinks and foods that are easy to digest, such as clear soft drinks, crackers, and plain toast.
Tip number 3: It can help to sit up or take a short walk after eating.
Finally, be sure to talk with your doctor or nurse to learn more about how to manage nausea and vomiting.
Getting support if you have nausea and vomiting
Side effects like nausea and vomiting can be hard to deal with, both physically and emotionally. It’s important to ask for support from your health care team. They can help you prepare for and make it through difficult times. Learn more about ways to cope with cancer.
Cachexia can make you feel tired and unable to do your daily activities. Your family and friends will want to know how to help you. If people offer help, accept it.
Credit: iStock
What is cancer cachexia?
Cancer cachexia is a wasting syndrome that leads to weakness, fatigue, and loss of skeletal muscle (also called sarcopenia) and fat. Unlike malnutrition, it cannot be reversed with nutrition support alone. Cancer cachexia must be treated with medicines and is hard to reverse once it starts. Cancer cachexia is most common in people with advanced cancer.
There are three stages of cancer cachexia:
Pre-cachexia. In this stage, you may have appetite loss and weight loss. Treatments for cachexia are most likely to be effective at this stage. Your doctor and dietitian will discuss how to improve your symptoms or prevent them from getting worse.
Cachexia. You may move from pre-cachexia to cachexia depending on the type and stage of your cancer, how you respond to cancer treatment, and your eating habits. In the cachexia stage, you may lose interest in eating and continue to lose weight and muscle. Other symptoms include fatigue and reduced strength.
Refractory cachexia. In this stage, you have severe muscle loss and continue to lose weight. Refractory cachexia affects many people with advanced cancer that is not responding to cancer treatment.
Scientists don’t fully understand how cachexia occurs in people with cancer. But they think that inflammation is the main cause. Increased metabolism, insulin resistance, and hormone changes may also play roles.
Inflammation
Inflammation can cause appetite loss, loss of muscle and fat, changes in how the body uses nutrients, decreased eating, and increased metabolism. Lab tests show that certain cancers, such as breast, ovarian, and esophageal cancer, can cause inflammation in the body.
Changes in metabolism
Some cancers can change your metabolism, or how your body uses carbohydrates, protein, and fat from food. Changes may include rapid breakdown of protein and fat stores in the body, causing muscle and fat loss. An increased metabolism also means your body uses more energy. This makes it harder for your body to meet its energy and protein needs, leading to weight loss and possible cachexia.
People with cancer may have insulin resistance. Normally, after you eat food, insulin tells your cells to allow glucose (sugar) to move from your blood into your cells. But with insulin resistance, the cells no longer respond to insulin. When your cells can’t respond to insulin, glucose can’t enter your cells and it builds up in your blood, causing high blood sugar (a condition called hyperglycemia). And when glucose cannot get into your cells, it is not available to be used by the cells for energy. This can lead to weight loss and possible cachexia.
Changes in hormones
Cancer cachexia may also be caused by a change in hormones, chemical messengers that tell your cells what to do. Two groups of hormones are linked with cancer cachexia: catabolic and anabolic hormones. Catabolic hormones break down tissue, and anabolic hormones build tissue. In cancer cachexia, your body has more working catabolic hormones than anabolic hormones. This imbalance leads to muscle breakdown, making cancer cachexia worse.
Symptoms of cancer cachexia
Learning about cachexia can help you know what to expect, which can ease distress.
These symptoms can have many causes and may not be a sign of cachexia. It’s important to talk with your doctor if you notice these changes. Your doctor can help you manage them and decide if other tests are needed.
Ways to prevent cancer cachexia
Spotting and treating malnutrition early is the best way to prevent cancer cachexia. Talk to your doctor about regular nutrition screenings during treatment to see if you are at risk of malnutrition and cancer cachexia. Learn more at Weight Changes, Malnutrition, and Cancer.
Ways to manage cancer cachexia
You need the help of many types of health care providers to manage cachexia.
Your doctor may prescribe medicines such as appetite stimulants and anti-inflammatory drugs. They might refer you to a registered dietitian who can suggest nutrition supplement drinks, such as Ensure or Boost. Dietitians can provide nutrition counseling and education for you and your caregivers. If you need it, dietitians oversee nutrition support such as tube feeding (enteral nutrition) and IV nutrition (parenteral nutrition). Learn more about tube feeding and IV nutrition at Nutrition During Cancer Treatment.
Your doctor might refer you to physical therapy. Physical therapy can help improve strength and endurance. Getting stronger can help you move better and take part in daily activities, which can help improve your quality of life.
If swallowing becomes an issue, your doctor can refer you to a speech therapist. If mouth sores or other mouth problems are getting in the way of eating and drinking, your doctor may suggest you see a dentist. Learn more about managing mouth problems during cancer treatment at Mouth and Throat Problems During Cancer Treatment.
Getting support for cancer cachexia
Support from family and friends. Cachexia can make you feel tired and unable to do your daily activities. Reach out to your family and friends to help with meal planning, grocery shopping, cooking, and cleaning. Your family and friends will want to know how to help you. If people offer help, accept it.
Support from your health care providers. Be sure that your doctor knows about problems you are having. Your doctor can prescribe medicine and refer you to other health care providers as needed.
Support for caregivers. It is normal to feel distress when a loved one has cachexia. You might be upset about their weight loss, loss of physical function, and changing appearance.
There may be days when your loved one does not want to eat or drink. Offer gentle support rather than pushing your loved one to eat. Ask the doctor for referrals to a dietitian and physical therapist to help your loved one with cachexia. Meet with them together so you know how best to help your loved one.
Learning about cachexia can help you know what to expect, which can ease your distress. Learn more about getting support at Support for Caregivers of Cancer Patients.
Cancer cachexia often happens at the end of life. To prepare, it might help to talk with the doctor or nurse about what to expect during this time. Learn more at Advanced Cancer.
When you have appetite loss, eat every 2 to 3 hours and have snacks that are high in calories and protein.
Credit: iStock
Appetite loss, weight loss, and cancer
Appetite loss and weight loss are common side effects of cancer and cancer treatments. Anyone with cancer might lose their appetite and lose weight. But you are more likely to lose weight if you have head and neck, lung, pancreatic, or liver cancer or cancer in the upper digestive system. Upper digestive system cancers include cancers in the throat, esophagus, stomach, and the first part of the small intestine.
Appetite loss often leads to eating less than your body needs, which leads to weight loss. Weight loss can also occur when you burn more calories than you are taking in. Weight loss can lead to malnutrition.
Although cachexia also causes weight loss, cachexia and weight loss are different and treated differently. Learn more at Cancer Cachexia.
Side effects of cancer treatment that cause problems with eating include:
Other factors that may cause appetite loss and weight loss during cancer treatment include anxiety, pain, depression, and fatigue. Learn more about Emotions and Cancer.
Ways to manage appetite loss and weight loss in people with cancer
If you start to lose your appetite, talk with your doctor or registered dietitian. Speak with them right away if you start to lose weight. Your dietitian can help you and your family manage your weight loss. Here are some tips that may help.
Ways to Deal with Appetite Loss During Cancer Treatment
Lack of appetite, or not feeling like eating, is a common problem caused by cancer and its treatment. Try these 10 tips for people with cancer who are experiencing appetite loss.
Add higher calorie condiments to meals and snacks.
Other tips to help improve eating:
Be as active as possible so that you will have a good appetite.
Brush your teeth and rinse your mouth to relieve symptoms and aftertaste.
Create a relaxing eating environment. Try adding candles and music and eating with your loved ones.
Medicine to manage appetite loss from cancer and cancer treatment
If you are not able to keep your appetite up, talk with your doctor about appetite stimulants. These are medicines that increase appetite and can cause weight gain.
Increased appetite, weight gain, and cancer
Although many people with cancer have appetite loss and lose weight, you may gain weight during cancer treatment.
Weight gain is more common if you have ovarian, breast, or prostate cancer. Each person is different, so even if you have one of these cancers, it does not mean you will gain weight. And you may gain weight if you have a different type of cancer.
If you gain weight during your cancer treatment, let your doctor know so they can assess the cause and type of weight gain. Small weight fluctuations during cancer treatment are normal and expected. But if weight gain is sudden, such as 5 pounds in a week, or does not stop, tell your doctor right away.
Causes of weight gain in people with cancer
Fluid retention.Some cancers may cause weight gain due to the size of the tumor or the buildup of fluid. There are different types of fluid buildup, but they all can cause you to gain weight. Learn more at Edema (Swelling) and Cancer Treatment.
Increased appetite. Increased appetite and food cravings that result in weight gain may occur from the cancer itself, cancer treatment, or medicines used with cancer treatment.
Metabolic changes.Hormone therapy may cause weight gain by lowering sex hormones. When you have lower levels of sex hormones, your metabolism slows. Our metabolism is the rate at which we burn energy. A slower metabolism means you burn less energy, which makes it easier to gain weight.
Some hormone therapies and chemotherapy may lead to early menopause in women. Early menopause may decrease your metabolism and cause weight gain.
Medications. Steroids, which are often given during cancer treatment, increase appetite and make you want to eat more. When we eat more calories than our body burns, we gain weight. If you take steroids, try to eat foods high in fiber and protein at each meal to help you stay full.
Steroids may also cause weight gain by causing your body to hold onto water (fluid retention). If you retain water, you may look and feel swollen. Learn more about fluid retention at Edema (Swelling) and Cancer Treatment.
Decreased activity. Many cancer treatments can cause fatigue and pain, making it hard to be active. Being less active may in turn lead to weight gain. Talk to your doctor about how to manage problems like fatigue or pain to stay as active as possible. Learn more at Cancer Fatigue and Pain and Cancer.
Ways to manage increased appetite and weight gain in people with cancer
Here are some tips to manage increased appetite and slow or stop weight gain. Talk with your doctor or dietitian about these tips and which ones are right for you.
Tips about foods to eat:
To help with weight changes, keep the pantry and refrigerator stocked with healthy snacks, such as overnight oats.
Credit: iStock
Eat foods high in fiber, such as fruits, vegetables, and whole-grain breads, cereals, and pasta.
Eat fish, lean meats, such as lean beef, pork trimmed of fat, and poultry (chicken or turkey) without skin.
Eat plant-based proteins, such as beans, nuts, seeds, and tofu.
Eat low-fat dairy products, such as 1% and skim.
Eat foods that you enjoy so you feel satisfied.
Tips about foods to limit:
Eat less fat.
Cook with and use less salt to reduce fluid retention.
Reduce sugary drinks like fruit juices and soda. Try diluting fruit juice with water.
Limit or do not drink alcohol.
Grocery shopping tips:
Buy ground meat that is 93% lean or higher.
Buy leaner cuts of meat, such as “loin,” “sirloin,” or “round.”
To help control portions, buy food in single-serving containers, such as single-serve yogurts.
Meal prep tips:
Limit cooking oils. As a general guideline, use 1 teaspoon if cooking for yourself. Use 1 to 2 tablespoons if cooking for more than just yourself.
Use cooking methods that reduce fat, like baking, broiling, air frying, roasting, and boiling.
Other ways to help with weight gain:
Plan meals and snacks ahead of time.
Keep your pantry and refrigerator stocked with healthy snacks.
Eat only when hungry.
Find activities you enjoy, if you eat out of boredom.
Eat more slowly. It takes about 15 minutes for the stomach and brain to know if you are full. Slowing down when you are eating can help you know if you are full or not.
Eat smaller amounts of food at meals. Use smaller plates.
Exercise daily.
Keep a food diary. This can help you see what foods and drinks you eat that help you to manage your weight.
If you have swelling from steroids, try limiting or avoiding foods that are high in sodium, such as:
breads that have a long shelf life
sauces
dressings
cheese
deli and canned meats
olives
certain frozen foods, such as pizza and frozen dinners
canned foods (look for low-sodium options)
table salt
seasonings with salt
If you don’t want to cut out these foods, look for lower sodium options. You can look at the front of a product to see if it says, “low sodium,” “very low sodium,” or “sodium free.”
Instead of using the saltshaker, use dried or fresh spices like garlic and onion powder or fresh basil and oregano.
Talk with your doctor and dietitian before going on a diet to lose weight. If you eat because of stress, fear, or depression, think about talking with a counselor. Your doctor might also prescribe medicine to help with these feelings. Learn more about Emotions and Cancer.
Malnutrition and cancer
Malnutrition is when your body doesn’t get enough energy, protein, vitamins, and minerals.
Causes of malnutrition in cancer
Malnutrition can be caused by the cancer itself, the side effects of cancer treatment, or both.
Cancer and its treatment can cause malnutrition in many ways. They can decrease your appetite, make you feel full quickly, and change your sense of taste and smell. These changes may cause you to eat less. In fact, decreased appetite or appetite loss is a main cause of malnutrition in people with cancer. Cancer may also lead to malnutrition by causing problems with swallowing, digestion, and absorption of your food.
Common treatment side effects that increase the risk of malnutrition are:
Cancer and cancer treatments may also cause fatigue, pain, anxiety, distress, and depression, all of which can make eating a challenge, both physically and emotionally. Talk to your doctor and registered dietitian about any of your side effects and concerns. Your team is there to support you and help you manage these challenges.
Problems caused by malnutrition
Malnutrition can cause you to be weak, tired, and not able to fight infection or even finish cancer treatment. Studies show that malnutrition can decrease your quality of life and become life-threatening.
Screening for malnutrition
Your health care team may use nutrition screenings and assessments to catch eating problems early and measure your risk of malnutrition. Ask your doctor about a nutrition screening before treatment starts and when you should be screened again during treatment.
Use nutrition supplement drinks, such as Ensure or Boost.
Tips on when to eat:
Eat small meals spaced throughout the day. Aim for five to six small meals each day.
Eat every 2 to 3 hours.
Tips on talking with your doctor or dietitian:
Report loss of appetite and other eating problems to your doctor right away.
Ask your doctor about a referral to a registered dietitian. A registered dietitian can do a nutrition assessment and provide a nutrition care plan.
Ask your dietitian about high-calorie and high-protein nutrition supplement drinks.
Report weight loss of more than 3 to 5 pounds in one week to your doctor.
If you continue to have trouble eating and are losing weight, your doctor or dietitian might suggest tube feeding (enteral nutrition) or IV nutrition (parenteral nutrition). Learn more about tube feeding and IV nutrition at Nutrition During Cancer Treatment.
Getting support for weight changes and malnutrition
Support from family and friends. Ask your family and friends to help with meal planning, grocery shopping, cooking, and cleaning. Provide them with a list of your favorite foods and meals they can prepare for you.
Support from your health care providers. If you’re having trouble with eating and drinking, your doctor and dietitian can help. Your doctor can help you find medicines to manage certain problems and refer you to a registered dietitian. Your registered dietitian is your nutrition expert. They can help you with eating and drinking habits before, during, and after treatment.
Support for caregivers. Do not be surprised or upset if your loved one’s food preferences change from day to day. There may be days when they do not want a favorite food or say it now tastes bad. Offer gentle support rather than pushing your loved one to eat. Talk with your loved one about ways to manage eating problems. Ask the doctor for a referral to a dietitian and meet with them together. Talk through problems and seek other advice that can help you both feel more in control. Learn more about getting support when your loved one is being treated for cancer at Support for Caregivers of Cancer Patients.
If you have appetite loss, constipation, diarrhea, or vomiting, your doctor or dietitian may suggest that you have plenty of clear liquids. Get ideas on what to drink from this list of clear liquids.
Soups
bouillon
clear, fat-free broth
consommé
Drinks
clear apple juice
clear carbonated beverages
fruit-flavored drinks
fruit punch
sports drinks
water
weak, caffeine-free tea
Sweets
fruit ices made without fruit pieces or milk
gelatin (Jell-O)
honey
jelly
popsicles
Nutritional supplements
clear nutrition supplements, such as Boost Breeze and Ensure Clear
Drink water and other clear liquids to help prevent dehydration caused by diarrhea.
Credit: iStock
What is diarrhea?
Diarrhea means having bowel movements (stools) more often than normal. The stool may also be soft, loose, or watery. Diarrhea is a common side effect of many cancer treatments, such as chemotherapy, immunotherapy, and radiation therapy.
When you have severe diarrhea, your body does not absorb enough water and nutrients. This can lead to serious health problems such as dehydration. Dehydration can be life-threatening, so tell your doctor or nurse if you have diarrhea.
Your doctor will find the diarrhea’s cause and recommend ways to feel better, which may include medicines and food that help decrease or stop diarrhea.
Learn about other digestive system problems in people with cancer
Chemotherapy. Many types of chemo can cause diarrhea because they destroy not only cancer cells but also rapidly dividing healthy cells, including those that line your digestive tract.
Immunotherapy. Some immunotherapy drugs, especially immune checkpoint inhibitors, can cause inflammation. An inflamed colon (colitis) can lead to diarrhea.
Radiation therapy. Radiation directed at the abdomen, pelvis, or rectum can cause diarrhea by damaging healthy tissue in the digestive tract. Diarrhea from radiation therapy is a symptom of radiation enteritis.
Medicines. Diarrhea can be a side effect of some medicines, including antibiotics and anti-inflammatory drugs. Drugs used to treat diabetes, depression, mood disorders, and heartburn may also cause diarrhea.
Supplements and herbal products. Some supplements can cause diarrhea. Tell your health care team if you are taking any supplements or herbal products or if you start a new supplement.
Infections. Infections are a common cause of diarrhea. When being treated for cancer, you are more vulnerable to viral and bacterial infections, including foodborne illness, because treatments such as chemo can weaken your immune system.
feeling an urgent need to have a bowel movement that is difficult to control
stomach pain or cramps
excessive gas
People with diarrhea may also:
have blood or mucus in the stools
feel dizzy or lightheaded
have a fever
experience weight loss
Your doctor will talk with you about your symptoms to figure out the severity, or grade, of your diarrhea. Grade is based on how many bowel movements you have per day, relative to your normal number of bowel movements. Grades 1 and 2 (having up to six bowel movements above your normal daily number) can usually be managed at home, but grades 3 and 4 (having seven or more bowel movements above your normal daily number) can be life-threatening and may require treatment in a hospital.
How is diarrhea diagnosed in people with cancer?
Finding the cause of diarrhea is important so you can get relief before it interferes with your cancer treatment or causes life-threatening dehydration. Your doctor may ask questions such as:
How many bowel movements have you had in the past day?
What was your last bowel movement like (how much, how hard or soft, what color, was there blood or mucus)?
Have you had any dizziness, fever, or weight loss?
What are you eating and drinking each day?
Your doctor will do a physical exam and may also use tests and procedures to diagnose the cause of diarrhea and suggest treatment options:
Stool tests: Tests that check the stool for blood, viruses, bacteria, and other issues that may cause diarrhea.
Urinalysis: A test to check the color of urine and its contents, such as sugar, protein, red blood cells, and white blood cells.
Digital rectal exam: A test in which your doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel for anything that seems unusual.
Ways to treat and control diarrhea
Treatment of diarrhea in people with cancer depends on its cause and severity (grade). Your doctor may suggest changes to your diet and prescribe medications. You may also receive intravenous (IV) fluids to help replace the fluids you lost. If chemo is causing severe diarrhea, your doctor may reduce your dose or have you stop taking it until your diarrhea gets better.
Tips for managing diarrhea
Drink lots of water or other fluids. Ask your doctor or nurse how much fluid you should drink. Drinking clear liquids, such as water or broth, helps replace fluids and electrolytes your body loses when you have diarrhea. Room temperature liquids are easiest on the stomach.
Eat small meals. It may help to eat frequent small meals or snacks throughout the day, instead of three larger meals.
Eat low-fiber foods. Eating foods that are low in fiber can help reduce diarrhea. Foods such as white bread, pasta, and canned fruit are good choices.
Eat foods that are high in sodium and potassium. You lose these minerals when you have diarrhea, so it’s a good idea to eat foods that help replace them. Peeled and boiled potatoes, soup, bananas, applesauce, and crackers are good options.
Avoid foods and drinks that can make diarrhea worse. These include alcohol, milk and dairy products, spicy foods, caffeinated drinks, dried beans, foods high in fat, fruit juices, and sugar-free gum or candies. Learn more about how changing your diet can help you manage side effects of cancer treatment at Nutrition During Cancer Treatment.
Keep your anal area clean and dry. Try using warm water and baby wipes to stay clean. Taking a sitz bath—a warm, shallow bath—can also be soothing to your anal area.
Keep a record of your bowel movements. Show this record to your health care team and talk to them about what is normal for you. This can help your doctor treat the diarrhea you are having.
Medicines for diarrhea
For severe diarrhea that happens while you are getting cancer treatment, your doctor may recommend medication. Your doctor may prescribe loperamide (Imodium) or a combination of diphenoxylate and atropine (Lomotil) to prevent or treat diarrhea. Doctors may also recommend probiotics that help with digestion and bowel function or fiber supplements (e.g., Metamucil). Check with your doctor before taking these or other medicines and supplements.
How a caregiver can help
Encourage the person you are caring for to drink water or other fluids their doctor suggests. Make sure they have a water bottle they can carry and refill throughout the day.
Keep a record of the person’s bowel movements. Ask the health care team about when you should call them if the diarrhea lasts or becomes more severe.
Try to keep the person’s pantry stocked with foods that can help relieve diarrhea.
Encourage the person to take warm, shallow baths to relieve pain and irritation from diarrhea.
Talking with your doctor about diarrhea
Tell your doctor or nurse if you are having diarrhea. They can help you find ways to prevent and control this side effect of cancer and cancer treatment.
Questions to ask your provider about diarrhea:
What symptoms or problems should I call you about?
What medicines can I take for diarrhea?
What can help decrease rectal pain and irritation?
How much and what types of liquid should I drink each day?
What foods should I eat while I have diarrhea? What foods should I avoid?
Narrator: What to do when you have diarrhea from radiation therapy.
Let’s listen in as support group members and the group’s leader, Janet, talk about coping with diarrhea.
Miguel: I don’t know about the rest of you, but I’m beginning to feel like I live in the bathroom. Some days diarrhea keeps me close to home when I’d rather be out.
Janet: I’m glad you brought this topic up, Miguel. Many people getting radiation therapy to the pelvis, stomach, or abdomen have diarrhea. The good news is that there are things you can do to manage it. Let’s go over 3 steps that can help.
Miguel: Thanks. That would be great.
Janet: First, drink lots of clear liquids like water, ginger ale and clear broth. Most people need to drink more liquids when they have diarrhea – 8 to 12 glasses a day. Check with your doctor to see how much liquid you should drink. Keep in mind that this won’t stop the diarrhea, but it will help replace the fluids you are losing.
Second, eat small meals every 2 or 3 hours that are easy on the stomach. Anyone ever heard of the BRAT diet?
Gina: Yeah. Let’s see… “B” is for bananas, then there’s “R” for rice, “A” for applesauce, and… oh, then there’s “T” for toast.
Janet: That’s it – bananas, rice, applesauce, and toast.
OK, on to the third step – avoid things that can make your diarrhea worse, like milk, alcohol, and drinks with caffeine in them. Stay away from raw fruits and vegetables that have a lot of fiber in them and stay away from fried or greasy foods. Ask your doctor about other foods you may need to avoid.
Gina: Is there medicine that can help?
Janet: Yes, medicine can help some people. Ask your doctor or nurse about medicine that would be best for you.
Folks, one last thing – be sure to call your doctor or nurse right away if you’re dizzy or have diarrhea or stomach pain for more than a day. Okay?
Gina: Okay. Thanks for the information, Janet – I think I can do those things you mentioned.
Narrator Summary: Drink lots of clear liquids each day. Most people need to drink 8 to 12 glasses. Check with your doctor to see how much liquid you should drink each day.
It may also help to follow the BRAT diet. Bananas, rice, applesauce, and toast are easy on the stomach.
Avoid greasy or spicy foods. They can make your diarrhea worse, so can milk, alcohol, and drinks with caffeine in them.
Ask about medicine that can help, and be sure to let your doctor or nurse know if you’re dizzy or have diarrhea or stomach pain for more than a day.
Talk with your nurse to learn more about how to manage diarrhea during radiation therapy.
Getting support if you have diarrhea
Side effects like diarrhea can be hard to deal with, both physically and emotionally. It’s important to ask for support from your health care team. They can help you prepare for and make it through difficult times. Learn more about ways to cope with cancer, including ways to adjust to daily life during cancer treatment.
Narrator: What to do when you have diarrhea from radiation therapy.
Let’s listen in as support group members and the group’s leader, Janet, talk about coping with diarrhea.
Miguel: I don’t know about the rest of you, but I’m beginning to feel like I live in the bathroom. Some days diarrhea keeps me close to home when I’d rather be out.
Janet: I’m glad you brought this topic up, Miguel. Many people getting radiation therapy to the pelvis, stomach, or abdomen have diarrhea. The good news is that there are things you can do to manage it. Let’s go over 3 steps that can help.
Miguel: Thanks. That would be great.
Janet: First, drink lots of clear liquids like water, ginger ale and clear broth. Most people need to drink more liquids when they have diarrhea – 8 to 12 glasses a day. Check with your doctor to see how much liquid you should drink. Keep in mind that this won’t stop the diarrhea, but it will help replace the fluids you are losing.
Second, eat small meals every 2 or 3 hours that are easy on the stomach. Anyone ever heard of the BRAT diet?
Gina: Yeah. Let’s see… “B” is for bananas, then there’s “R” for rice, “A” for applesauce, and… oh, then there’s “T” for toast.
Janet: That’s it – bananas, rice, applesauce, and toast.
OK, on to the third step – avoid things that can make your diarrhea worse, like milk, alcohol, and drinks with caffeine in them. Stay away from raw fruits and vegetables that have a lot of fiber in them and stay away from fried or greasy foods. Ask your doctor about other foods you may need to avoid.
Gina: Is there medicine that can help?
Janet: Yes, medicine can help some people. Ask your doctor or nurse about medicine that would be best for you.
Folks, one last thing – be sure to call your doctor or nurse right away if you’re dizzy or have diarrhea or stomach pain for more than a day. Okay?
Gina: Okay. Thanks for the information, Janet – I think I can do those things you mentioned.
Narrator Summary: Drink lots of clear liquids each day. Most people need to drink 8 to 12 glasses. Check with your doctor to see how much liquid you should drink each day.
It may also help to follow the BRAT diet. Bananas, rice, applesauce, and toast are easy on the stomach.
Avoid greasy or spicy foods. They can make your diarrhea worse, so can milk, alcohol, and drinks with caffeine in them.
Ask about medicine that can help, and be sure to let your doctor or nurse know if you’re dizzy or have diarrhea or stomach pain for more than a day.
Talk with your nurse to learn more about how to manage diarrhea during radiation therapy.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.