Alcohol is the common term for ethanol or ethyl alcohol, a chemical substance found in alcoholic beverages such as beer, hard cider, malt liquor, wines, and distilled spirits (liquor). Alcohol is produced by the fermentation of sugars and starches by yeast. Alcohol is also found in some medicines, mouthwashes, and household products (including vanilla extract and other flavorings). This fact sheet focuses on cancer risks associated with the consumption of alcoholic beverages.
According to the National Institute on Alcohol Abuse and Alcoholism, a standard alcoholic drink in the United States contains 14.0 grams (0.6 ounces) of pure alcohol. Generally, this amount of pure alcohol is found in:
12 ounces of beer
8–10 ounces of malt liquor
5 ounces of wine
1.5 ounces, or a “shot,” of 80-proof distilled spirits (liquor)
These amounts are used by public health experts in developing health guidelines about alcohol consumption and to provide a way for people to compare the amounts of alcohol they consume. However, they may not reflect the typical serving sizes people may encounter in daily life.
According to the federal government’s Dietary Guidelines for Americans, 2020–2025, individuals who do not drink alcohol should not start drinking for any reason. The Dietary Guidelines also recommends that people who drink alcohol do so in moderation by limiting consumption to 2 drinks or less in a day for men and 1 drink or less in a day for women. Heavy alcohol drinking is defined as having 4 or more drinks on any day or 8 or more drinks per week for women and 5 or more drinks on any day or 15 or more drinks per week for men.
What is the evidence that alcohol drinking can cause cancer?
There is a strong scientific consensus that alcohol drinking can cause several types of cancer (1, 2). In its Report on Carcinogens, the National Toxicology Program of the US Department of Health and Human Services lists consumption of alcoholic beverages as a known human carcinogen.
The evidence indicates that the more alcohol a person drinks—particularly the more alcohol a person drinks regularly over time—the higher his or her risk of developing an alcohol-associated cancer. Even those who have no more than one drink per day and binge drinkers (those who consume 4 or more drinks for women and 5 or more drinks for men in one sitting) have a modestly increased risk of some cancers (3–7). Based on data from 2009, an estimated 3.5% of cancer deaths in the United States (about 19,500 deaths) were alcohol related (8).
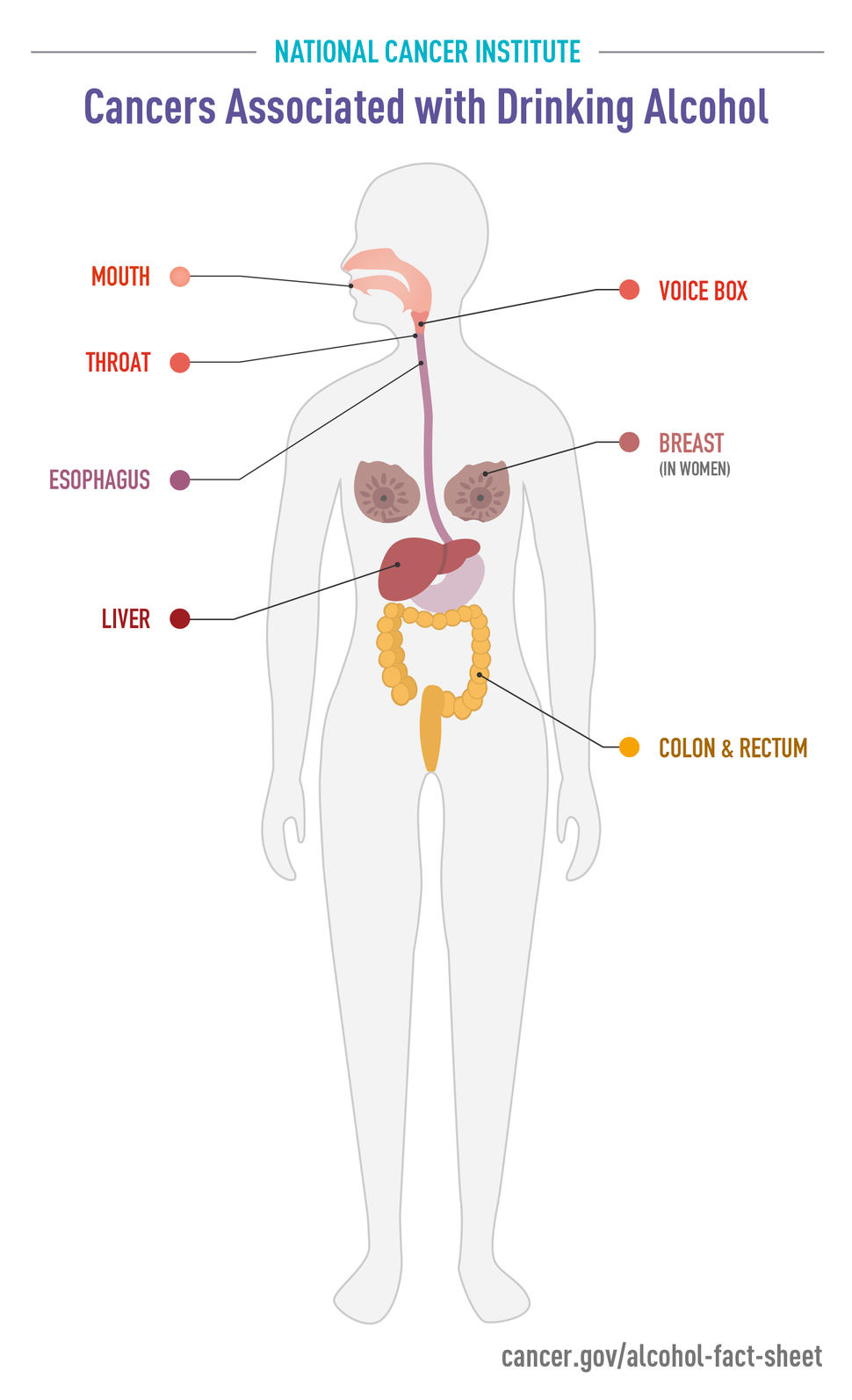
Clear patterns have emerged between alcohol consumption and the development of the following types of cancer:
Head and neck cancer: Moderate to heavy alcohol consumption is associated with higher risks of certain head and neck cancers. Moderate drinkers have 1.8-fold higher risks of oral cavity (excluding the lips) and pharynx (throat) cancers and 1.4-fold higher risks of larynx (voice box) cancers than non-drinkers, and heavy drinkers have 5-fold higher risks of oral cavity and pharynx cancers and 2.6-fold higher risks of larynx cancers (4, 9). Moreover, the risks of these cancers are substantially higher among persons who consume this amount of alcohol and also use tobacco (10).
Esophageal cancer: Alcohol consumption at any level is associated with an increased risk of a type of esophageal cancer called esophageal squamous cell carcinoma. The risks, compared with no alcohol consumption, range from 1.3-fold higher for light drinking to nearly 5-fold higher for heavy drinking (4, 9). In addition, people who inherit a deficiency in an enzyme that metabolizes alcohol have been found to have substantially increased risks of esophageal squamous cell carcinoma if they consume alcohol (11).
Breast cancer: Epidemiologic studies have consistently found an increased risk of breast cancer with increasing alcohol intake. Pooled data from 118 individual studies indicates that light drinkers have a slightly increased (1.04-fold higher) risk of breast cancer, compared with nondrinkers. The risk increase is greater in moderate drinkers (1.23-fold higher) and heavy drinkers (1.6-fold higher) (4, 9). An analysis of prospective data for 88,000 women participating in two US cohort studies concluded that for women who have never smoked, light to moderate drinking was associated with a 1.13-fold increased risk of alcohol-related cancers (mostly breast cancer) (5).
Colorectal cancer: Moderate to heavy alcohol consumption is associated with 1.2- to 1.5-fold increased risks of cancers of the colon and rectum compared with no alcohol consumption (4, 9, 14).
Numerous studies have examined whether there is an association between alcohol consumption and the risk of other cancers. For cancers of the ovary, prostate, stomach, uterus, and bladder, either no association with alcohol use has been found or the evidence for an association is inconsistent. However, evidence is accumulating that alcohol consumption is associated with increased risks of melanoma and of prostate and pancreatic cancers (4, 15).
Alcohol consumption has also been associated with decreased risks of kidney cancers (16–18) and non-Hodgkin lymphoma (19, 20) in multiple studies. However, any potential benefits of alcohol consumption for reducing the risks of some cancers are likely outweighed by the harms of alcohol consumption. In fact, a recent study that included data from more than 1,000 alcohol studies and data sources, as well as death and disability records from 195 countries and territories from 1990 to 2016, concluded that the optimal number of drinks to consume per day to minimize the overall risk to health is zero (21). That study did not include data on kidney cancer or non-Hodgkin lymphoma.
Alcohol consumption may also be associated with an increased risk of second primary cancers. For example, a meta-analysis of data from 19 studies showed that among patients with cancer of the upper aerodigestive tract (UADT)—which includes the oral cavity, pharynx, larynx, and esophagus—for every 10 grams of alcohol consumed per day before the first UADT cancer diagnosis there was a 1.09-fold higher risk of a second primary UADT cancer (22). It is less clear whether alcohol consumption increases the risk of second primary cancers at other sites, such as the breast (23–25).
How does alcohol affect the risk of cancer?
Researchers have hypothesized multiple ways that alcohol may increase the risk of cancer, including
metabolizing (breaking down) ethanol in alcoholic drinks to acetaldehyde, which is a toxic chemical and a probable human carcinogen; acetaldehyde can damage both DNA (the genetic material that makes up genes) and proteins
generating reactive oxygen species (chemically reactive molecules that contain oxygen), which can damage DNA, proteins, and lipids (fats) in the body through a process called oxidation
increasing blood levels of estrogen, a sex hormone linked to the risk of breast cancer
Alcoholic beverages may also contain a variety of carcinogenic contaminants that are introduced during fermentation and production, such as nitrosamines, asbestos fibers, phenols, and hydrocarbons.
The mechanisms by which alcohol consumption may decrease the risks of some cancers are not understood and may be indirect.
How does the combination of alcohol and tobacco affect cancer risk?
Epidemiologic research shows that people who use both alcohol and tobacco have much greater risks of developing cancers of the oral cavity, pharynx (throat), larynx, and esophagus than people who use either alcohol or tobacco alone. In fact, for oral and pharyngeal cancers, the risks associated with using both alcohol and tobacco are multiplicative; that is, they are greater than would be expected from adding the individual risks associated with alcohol and tobacco together (10, 26).
Can people’s genes affect their risk of alcohol-related cancers?
A person’s risk of alcohol-related cancers is influenced by their genes, specifically the genes that encode enzymes involved in metabolizing (breaking down) alcohol (27).
For example, one way the body metabolizes alcohol is through the activity of an enzyme called alcohol dehydrogenase, or ADH, which converts ethanol into the carcinogenic metabolite acetaldehyde, mainly in the liver. Recent evidence suggests that acetaldehyde production also occurs in the oral cavity and may be influenced by factors such as the oral microbiome (28, 29).
Many individuals of East Asian descent carry a version of the gene for ADH that codes for a “superactive” form of the enzyme. This superactive ADH enzyme speeds the conversion of alcohol (ethanol) to toxic acetaldehyde. Among people of Japanese descent, those who have this form of ADH have a higher risk of pancreatic cancer than those with the more common form of ADH (30).
Another enzyme, called aldehyde dehydrogenase 2 (ALDH2), metabolizes toxic acetaldehyde to nontoxic substances. Some people, particularly those of East Asian descent, carry a variant of the gene for ALDH2 that encodes a defective form of the enzyme. In people who produce the defective enzyme, acetaldehyde builds up when they drink alcohol. The accumulation of acetaldehyde has such unpleasant effects (including facial flushing and heart palpitations) that most people who have inherited the ALDH2 variant are unable to consume large amounts of alcohol and therefore have a low risk of developing alcohol-related cancers.
However, some individuals with the defective form of ALDH2 can become tolerant to the unpleasant effects of acetaldehyde and consume large amounts of alcohol. Epidemiologic studies have shown that such individuals have a higher risk of alcohol-related esophageal cancer, as well as of head and neck cancers, than individuals with the fully active enzyme who drink comparable amounts of alcohol (31). These increased risks are seen only among people who carry the ALDH2 variant and drink alcohol—they are not observed in people who carry the variant but do not drink alcohol.
Can drinking red wine help prevent cancer?
The plant secondary compound resveratrol, found in grapes used to make red wine and some other plants, has been investigated for many possible health effects, including cancer prevention. However, researchers have found no association between moderate consumption of red wine and the risk of developing prostate cancer (32) or colorectal cancer (33).
What happens to cancer risk after a person stops drinking alcohol?
Most of the studies that have examined whether cancer risk declines after a person stops drinking alcohol have focused on head and neck cancers and on esophageal cancer. In general, these studies have found that stopping alcohol consumption is not associated with immediate reductions in cancer risk. The cancer risks eventually decline, although it may take years for the risks of cancer to return to those of never drinkers.
For example, ex-drinkers still had higher risks of oral cavity and pharyngeal cancers than never drinkers even 16 years after they stopped drinking alcohol, although it was lower than before they stopped drinking (34). One study estimated that it would take more than 35 years for the higher risks of laryngeal and pharyngeal cancers associated with alcohol consumption to decrease to the level of never drinkers (35).
Is it safe for someone to drink alcohol while undergoing cancer chemotherapy?
As with most questions related to a specific individual’s cancer treatment, it is best for patients to check with their health care team about whether it is safe to drink alcohol during or immediately following chemotherapy treatment. The doctors and nurses administering the treatment will be able to give specific advice about whether it is safe to consume alcohol while undergoing specific cancer treatments.
Is there a link between antiperspirants or deodorants and breast cancer?
Because underarm antiperspirants or deodorants are applied near the breast and contain potentially harmful ingredients, several scientists and others have suggested a possible connection between their use and breast cancer (1, 2). However, no scientific evidence links the use of these products to the development of breast cancer.
What is known about the ingredients in antiperspirants and deodorants?
Aluminum-based compounds are used as the active ingredient in antiperspirants. These compounds form a temporary “plug” within the sweat duct that stops the flow of sweat to the skin’s surface. Some research suggests that aluminum-containing underarm antiperspirants, which are applied frequently and left on the skin near the breast, may be absorbed by the skin and have estrogen-like (hormonal) effects (3).
Because estrogen can promote the growth of breast cancer cells, some scientists have suggested that the aluminum-based compounds in antiperspirants may contribute to the development of breast cancer (3). In addition, it has been suggested that aluminum may have direct activity in breast tissue (4). However, no studies to date have confirmed any substantial adverse effects of aluminum that could contribute to increased breast cancer risks. A 2014 review concluded there was no clear evidence showing that the use of aluminum-containing underarm antiperspirants or cosmetics increases the risk of breast cancer (5).
Some research has focused on parabens, which are preservatives used in some deodorants and antiperspirants that have been shown to mimic the activity of estrogen in the body’s cells (6). It has been reported that parabens are found in breast tumors, but there is no evidence that they cause breast cancer. Although parabens are used in many cosmetic, food, and pharmaceutical products, most deodorants and antiperspirants in the United States do not currently contain parabens.
What is known about the relationship between antiperspirants or deodorants and breast cancer?
Only a few studies have investigated a possible relationship between breast cancer and underarm antiperspirants/deodorants. One study, published in 2002, did not show any increase in risk for breast cancer among women who reported using an underarm antiperspirant or deodorant (7). The results also showed no increase in breast cancer risk among women who reported using a blade (nonelectric) razor and an underarm antiperspirant or deodorant, or among women who reported using an underarm antiperspirant or deodorant within 1 hour of shaving with a blade razor. These conclusions were based on interviews with 813 women with breast cancer and 793 women with no history of breast cancer.
A subsequent study, published in 2006, also found no association between antiperspirant use and breast cancer risk, although it included only 54 women with breast cancer and 50 women without breast cancer (8).
A 2003 retrospective cohort study examining the frequency of underarm shaving and antiperspirant/deodorant use among 437 breast cancer survivors (2) reported younger age at breast cancer diagnosis for women who used antiperspirants/deodorants frequently or who started using them together with shaving at an earlier age. Because of the retrospective nature of the study, the results are not conclusive.
Because studies of antiperspirants and deodorants and breast cancer have provided conflicting results, additional research would be needed to determine whether a relationship exists (9).
Where can someone get more information on breast cancer risk?
People who are concerned about their breast cancer risk are encouraged to talk with their doctor.
Information about risk factors for breast cancer is available through NCI’s Cancer Information Service at 1–800–4–CANCER (1–800–422–6237).
Ionizing radiation consists of subatomic particles (that is, particles that are smaller than an atom, such as protons, neutrons, and electrons) and electromagnetic waves. These particles and waves have enough energy to strip electrons from, or ionize, atoms in molecules that they strike. Ionizing radiation can arise in several ways, including
from the spontaneous decay (breakdown) of unstable isotopes. Unstable isotopes, which are also called radioactive isotopes, give off (emit) ionizing radiation as part of the decay process. Radioactive isotopes occur naturally in the Earth’s crust, soil, atmosphere, and oceans. These isotopes are also produced in nuclear reactors and nuclear weapons explosions.
from cosmic rays originating in the sun and other extraterrestrial sources and from technological devices ranging from dental and medical x-ray machines to the picture tubes of old-style televisions
Everyone on Earth is exposed to low levels of ionizing radiation from natural and technological sources in varying proportions, depending on their geographic location, diet, occupation, and lifestyle.
What are the health hazards of exposure to ionizing radiation?
At high doses, ionizing radiation can cause immediate damage to a person’s body, including, at very high doses, radiation sickness and death. At lower doses, ionizing radiation can cause health effects such as cardiovascular disease and cataracts, as well as cancer. It causes cancer primarily because it damages DNA, which can lead to cancer-causing gene mutations.
Children and adolescents can be more sensitive to the cancer-causing effects of ionizing radiation than adults because their bodies are still growing and developing. Also, children and adolescents usually have more years of life following radiation exposure during which cancer may develop.
How are people exposed to ionizing radiation after a nuclear power plant accident?
Nuclear power plants use energy released by the decay of certain radioactiveisotopes to produce electricity. Additional radioactive isotopes are produced during this process. In nuclear power plants, specially designed fuel rods and containment structures enclose the radioactive materials to prevent them, and the ionizing radiation they produce, from contaminating the environment. If the fuel and surrounding containment structures are severely damaged, radioactive materials and ionizing radiation may be released, potentially posing a health risk for people. The actual risk depends on
the specific types and quantities of radioactive materials, or isotopes, released
how much radiation someone is exposed to and for how long
how a person comes in contact with the released radioactive materials (such as through contaminated food, water, air, or on the skin)
the person’s age (with those exposed at younger ages generally at higher risk of cancer)
The radioactive isotopes released in nuclear power plant accidents include iodine-131 (I-131), cesium-134 (Cs-134), and Cs-137. In the most severe kinds of accidents, such as the Chernobyl accident in 1986, other dangerous radioactive isotopes, such as strontium-90 (Sr-90) and plutonium-239, may also be released.
Human exposure to I-131 released from nuclear power plant accidents comes mainly from consuming contaminated water, milk, or foods. People may also be exposed by breathing dust particles in the air that are contaminated with I-131.
Inside the body, I-131 accumulates in the thyroid gland, which is an organ in the neck. The thyroid gland uses iodine to produce hormones that control how quickly the body uses energy. Because the thyroid does not distinguish between I-131 and nonradioactive iodine, the thyroid gland will accumulate either form. Exposure to radioactive iodine may increase the risk of thyroid cancer for many years, especially for children and adolescents.
Exposure to Cs-134 and Cs-137 can be external to the body or internal. External exposure comes from walking on contaminated soil or coming into contact with contaminated materials at nuclear accident sites. Internal exposure can come from breathing particles in the air that contain Cs-134 and Cs-137, such as dust originating from contaminated soil, or ingesting contaminated water or foods. Because Cs-134 and Cs-137 do not become concentrated in a particular tissue, the ionizing radiation that it releases can expose all tissues and organs of the body.
What have researchers learned about cancer risks from nuclear power plant accidents?
Much of what is known about cancer caused by radiation exposures from nuclear power plant accidents comes from research on the April 1986 nuclear power plant disaster at Chernobyl in Ukraine (Chornobyl in Ukrainian) (1, 2). The radioactive isotopes released during the Chernobyl accident included I-131, Cs-134, Cs-137, and Sr-90.
Power plant workers on-site at the time of the accident. Approximately 600 workers at the power plant during the emergency received very high doses of radiation and suffered from radiation sickness. All of those who received more than 6 grays (Gy) of radiation became very sick right away and subsequently died. Those who received less than 4 Gy had a better chance of survival. (A Gy is a measure of the amount of radiation absorbed by a person’s body.)
Cleanup workers. Hundreds of thousands of people who worked as part of the cleanup crews in the years after the accident were exposed to average external doses of ionizing radiation that ranged from approximately 0.14 Gy in 1986 to 0.04 Gy in 1989. Studies conducted in this group of people have found an increased risk of leukemia (3–5).
Residents near Chernobyl. From 1986 through 2005, approximately 5 million residents of the contaminated areas surrounding Chernobyl received an accumulated whole-body average dose of around 0.01 Gy (6). Studies that have followed children and adolescents exposed to I-131 from the Chernobyl accident showed an increased risk of developing thyroid cancer (7–9).
Recent studies have used genomic analysis of people affected by the Chernobyl accident to better understand how radiation exposure leads to cancer. In a 2021 study, investigators found that thyroid tumors in children who were exposed to fallout from the Chernobyl accident had higher levels of a particular kind of DNA damage that involves breaks in both DNA strands than tumors in unexposed individuals born more than 9 months after the accident (10). The more radiation the children had been exposed to, the more of this type of DNA damage was seen. This association was stronger the younger the children were at the time of exposure.
Another way in which radiation exposure could lead to cancer is through transgenerational effects, in which people exposed to ionizing radiation develop new genetic changes in their gametes (sperm or eggs) that are passed on to their future offspring, increasing cancer risk in those offspring. Transgenerational effects have been observed in some animal studies. However, genomic analysis of children born to people exposed to radiation at Chernobyl indicates that this exposure did not lead to an increase in new genetic changes in the children of exposed parents (11).
How long after exposure to I-131 is the risk of thyroid cancer increased?
Although the time it takes for the radiation to decrease by half (the half-life) of I-131 is only 8 days, the damage it causes can increase the risk of thyroid cancer for many years after the initial exposure.
A study led by NCI researchers followed more than 12,500 people who were younger than age 18 at the time they were exposed to a range of doses of I-131 (0.65 Gy on average) from the Chernobyl accident (7). A total of 65 new cases of thyroid cancer were found in this population between 1998 and 2007. The researchers found that the higher a person’s dose of I-131, the more likely they were to get thyroid cancer (with each Gy of exposure associated with a doubling of risk). They also found that this risk remained high for at least 30 years (9).
What can people do to protect themselves from health risks associated with exposure to contamination from a nuclear power plant accident?
What should cancer patients do if they live in an area that may be contaminated due to a nuclear power plant accident?
Cancer patients who are being treated with systemic chemotherapy or radiation therapy should be evacuated from the area where a nuclear power plant accident has occurred so their medical treatment can continue without interruption. Patients should always keep a record of the treatments they have had in the past and that they may be currently receiving, including the names of any drugs and their doses. These records may be important in the aftermath not only of a nuclear power plant accident but also after other large-scale events that may disrupt medical services, when medical records may be lost.
Local or national authorities may also advise certain people (newborns, infants, children, adolescents, and women who are pregnant) in areas with high I-131 contamination to take potassium iodide (KI) to prevent the accumulation of I-131 in their thyroid. KI should not pose a danger to someone who previously received radiation therapy or chemotherapy. Patients who are actively being treated for cancer and who are advised to take KI should consult with their doctor before taking the medication, so their doctor can evaluate their treatment plan and their health status, including their nutritional status, to determine the safety of KI treatment for them.
What research is NCI currently supporting on ionizing radiation and cancer risk?
Researchers at NCI and elsewhere continue to learn about the cancer risks from ionizing radiation by studying various groups of people, including those who were exposed as a result of the Chernobyl accident, survivors of the atomic bomb explosions in Japan during World War II, and people who were exposed to radiation during medical diagnostic procedures or as part of their job.
NCI conducts much of this research through the Radiation Epidemiology Branch of the Division of Cancer Epidemiology and Genetics (DCEG).
Through DCEG and the Division of Cancer Biology, NCI supports the Chernobyl Tissue Bank, which contains samples from the Chernobyl survivors. These are being used to investigate the effects of radioactive exposure from nuclear power plant accidents.
NCI collaborates with researchers from Japan’s Radiation Effects Research Foundation to learn about the health effects from the 1945 atomic bomb exposures in that country. This ongoing project is called the Life Span Study.
Health professionals can also find information about the medical management of exposed persons during radiation emergencies at the US Department of Health and Human Services’s Radiation Emergency Medical Management website.
Radon is a radioactive gas released from the normal decay of the elements uranium, thorium, and radium in rocks and soil. It is an invisible, odorless, tasteless gas that seeps up through the ground and diffuses into the air. In a few areas, depending on local geology, radon dissolves into ground water and can be released into the air when the water is used. Radon gas usually exists at very low levels outdoors. However, in areas without adequate ventilation, such as underground mines, radon can accumulate to levels that substantially increase the risk of lung cancer.
How is the general population exposed to radon?
Radon is present in nearly all air. Everyone breathes in radon every day, usually at very low levels. However, people who inhale high levels of radon are at an increased risk of developing lung cancer.
Radon can enter homes through cracks in floors, walls, or foundations, and collect indoors. It can also be released from building materials, or from water obtained from wells that contain radon. Radon levels can be higher in homes that are well insulated, tightly sealed, and/or built on soil rich in the elements uranium, thorium, and radium. Basement and first floors typically have the highest radon levels because of their closeness to the ground.
How does radon cause cancer?
Radon decays quickly, giving off tiny radioactive particles. When inhaled, these radioactive particles can damage the cells that line the lung. Long-term exposure to radon can lead to lung cancer, the only cancer proven to be associated with inhaling radon. There has been a suggestion of increased risk of leukemia associated with radon exposure in adults and children; however, the evidence is not conclusive.
How many people develop lung cancer because of exposure to radon?
Cigarette smoking is the most common cause of lung cancer. Radon represents a far smaller risk for this disease, but it is the second leading cause of lung cancer in the United States. Scientists estimate that 15,000 to 22,000 lung cancer deaths in the United States each year are related to radon.
Exposure to the combination of radon gas and cigarette smoke creates a greater risk of lung cancer than exposure to either factor alone. The majority of radon-related cancer deaths occur among smokers. However, it is estimated that more than 10 percent of radon-related cancer deaths occur among nonsmokers.
How did scientists discover that radon plays a role in the development of lung cancer?
Radon was identified as a health problem when scientists noted that underground uranium miners who were exposed to it died of lung cancer at high rates. The results of miner studies have been confirmed by experimental animal studies, which show higher rates of lung tumors among rodents exposed to high radon levels.
What have scientists learned about the relationship between radon and lung cancer?
Scientists agree that radon causes lung cancer in humans. Recent research has focused on specifying the effect of residential radon on lung cancer risk. In these studies, scientists measure radon levels in the homes of people who have lung cancer and compare them to the levels of radon in the homes of people who have not developed lung cancer.
Researchers have combined and analyzed data from all radon studies conducted in Canada and the United States. By combining the data from these studies, scientists were able to analyze data from thousands of people. The results of this analysis demonstrated a slightly increased risk of lung cancer for individuals with elevated exposure to household radon. This increased risk was consistent with the estimated level of risk based on studies of underground miners.
Techniques to measure a person’s exposure to radon over time have become more precise, thanks to a number of studies carried out in the 1990s and early 2000s.
How can people know if they have an elevated level of radon in their homes?
Testing is the only way to know if a person’s home has elevated radon levels. Indoor radon levels are affected by the soil composition under and around the house, and the ease with which radon enters the house. Homes that are next door to each other can have different indoor radon levels, making a neighbor’s test result a poor predictor of radon risk. In addition, rain or snow, barometric pressure, and other influences can cause radon levels to vary from month to month or day to day, which is why both short- and long-term tests are available.
Short-term detectors measure radon levels for 2 days to 90 days, depending on the device. Long-term tests determine the average concentration for more than 90 days. Because radon levels can vary from day to day and month to month, a long-term test is a better indicator of the average radon level. Both tests are relatively easy to use and inexpensive. A state or local radon official can explain the differences between testing devices and recommend the most appropriate test for a person’s needs and conditions.
The U.S. Environmental Protection Agency (EPA) recommends taking action to reduce radon in homes that have a radon level at or above 4 picocuries per liter (pCi/L) of air. About 1 in 15 U.S. homes is estimated to have radon levels at or above this EPA action level. Scientists estimate that lung cancer deaths could be reduced by 2 to 4 percent, or about 5,000 deaths, by lowering radon levels in homes exceeding the EPA’s action level.
Where can people find more information about radon?
The National Radon Program Services at Kansas State University is funded by the EPA and aimed at promoting public awareness of radon, increased testing, and the reduction of radon in homes, schools, and buildings. It provides a variety of resources, including the National Radon Hotlines, referrals to state radon programs, radon test kit orders, radon mitigation promotion, and other technical assistance and outreach activities.
Consumers can contact the National Radon Hotline at:
1–800–SOS–RADON (1–800–767–7236) to reach an automated system for ordering materials and listen to informational recordings
1–800–55–RADON (1–800–557–2366) to contact an information specialist, or by sending an e-mail
More information is also available online from the EPA.
Use the Thyroid Dose/Risk Calculator This calculator estimates radiation dose and risk of developing thyroid cancer from fallout exposure from nuclear tests.
Introduction
During the Cold War in the mid-1940s through early 1960s, the U.S. government conducted about 100 nuclear weapons (atomic bomb) tests in the atmosphere at a test site in Nevada, more than 100 in the Pacific, and one—the first ever—in New Mexico. The radioactive substances released by these tests are known as “fallout.” They were carried thousands of miles away from the test site by winds. As a result, people living in the United States at the time of the testing were exposed to varying levels of radiation.
Among the numerous radioactive substances released in fallout, there has been a great deal of concern about and study of one radioactive form of iodine–called iodine-131, or I-131. I-131 collects in the thyroid gland. People exposed to I-131, especially during childhood, may have an increased risk of thyroid disease, including thyroid cancer. Thyroid cancer is uncommon and is usually curable. Typically, it is a slow-growing cancer that is highly treatable. About 98 out of 100 people who are diagnosed with thyroid cancer survive the disease for at least five years after diagnosis.
The thyroid controls many body processes, including heart rate, blood pressure, and body temperature, as well as childhood growth and development. It is located in the front of the neck, just above the top of the breastbone and overlying the windpipe.
Although the potential of developing thyroid cancer from exposure to I-131 from nuclear weapons testing is small, it is important for Americans who grew up during the atomic bomb testing between 1945 and 1963 to be aware of risks.
How Americans Were Exposed to I-131
Because of wind and rainfall patterns, the distribution of I-131 fallout varied widely after each test. Therefore, although all areas of the United States received fallout from at least one nuclear weapons test, certain areas of North America received more fallout than others.
Scientists estimate that the larger amounts of I-131 from the Nevada test site fell over some parts of Utah, Colorado, Idaho, Nevada, and Montana. But I-131 traveled to all states, particularly those in the Midwestern, Eastern, and Northeastern United States. Some of the I-131 collected on pastures and on grasses. Depending on the location, grazing cows and goats sometimes consumed contaminated grasses resulting in I-131 collecting in the animals’ milk. Much of the health risk associated with I-131 occurred among milk-drinkers–usually children. From what is known about thyroid cancer and radiation, scientists think that people who were children during the period of atomic bomb testing are at higher risk for developing thyroid cancer.
In addition to nuclear testing in Nevada, the Pacific, and New Mexico, Americans were potentially exposed to I-131 from a number of events, including:
Nuclear testing by other nations elsewhere in the world (mainly in the 1950s and 1960s)
Nuclear power plant accidents (such as the Chernobyl accident in 1986 and the Fukushima accident in 2011 (primarily Americans in Japan)
Releases from atomic weapons production plants (such as the Hanford facility in Washington state from 1944 to 1957)
Scientists are working to find out more about ways to measure and address potential I-131 exposure. They are also working to find out more about other radioactive substances released by fallout and their possible effects on human health.
The Search for Answers
Congress directed government health agencies to investigate the I-131 problem many years ago, and to make recommendations to Americans who might have related health risks. Gathering information turned out to be very complicated. Record-keeping was incomplete at the time of the bomb testing. Much of the information needed to calculate an individual’s dose of I-131 and associated risk is either unreliable or unavailable.
Despite such challenges, government agencies organized expert scientific teams that have devoted many years to learning more about I-131. A number of reports have been published documenting what they have learned (1997, 1999). This information was put together to educate the American people about the potential health risks from exposure to I-131 from nuclear weapons testing.
I-131’s Rapid Breakdown
The “active” in “radioactive” means that unstable substances produced in nuclear reactions break down and change, so that they eventually become stable and no longer release radiation. The rate of breakdown can occur quickly in some radioactive substances, often within a few days. Half of the I-131 released during each atomic bomb test was gone in about 8 days. Almost all of it was gone (less than 1 percent remained) 80 days after the test.
Like all radioactive substances, I-131 releases radiation as it breaks down. It is this radiation that can injure human tissues. But I-131’s steady breakdown means that the amount of I-131 present in the environment after a bomb test steadily decreased. Therefore, farm animals that grazed in fields within a few days after a test would have consumed higher levels of I-131 than animals grazing later.
The Milk Connection
People younger than 15 at the time of aboveground testing (between 1945 and 1963) who drank milk, and who lived in the Mountain West, Midwestern, Eastern, and Northeastern United States, probably have a higher thyroid cancer risk from exposure to I-131 in fallout than people who lived in other parts of the United States, who were over the age of 15 in the 1940s, or who did not drink milk. Their thyroid glands were still developing during the testing period. And they were more likely to have consumed milk contaminated with I-131. The amount of I-131 people absorbed depends on:
Their age during the testing period (between 1945 and 1963)
The amount and source of milk they drank in those years
Where they lived during the testing period
Age and residence during those years are usually known. But few people can recall the exact amounts or sources of the milk they drank as children. While the amount of milk consumed is important in determining exposure to I-131, it is also important to know the source of the milk. Fresh milk from backyard or farm cows and goats usually contained more I-131 than store-bought milk. This is because processing and shipping milk allowed more time for the I-131 to break down.
About Thyroid Disease
There are two main types of thyroid diseases:
Noncancerous Thyroid Disease
Some thyroid diseases are caused by changes in the amount of thyroid hormones that enter the body from the thyroid gland. Doctors can screen for these with a simple blood test.
Noncancerous thyroid disease also includes lumps, or nodules, in the thyroid gland that are benign and not cancerous.
Thyroid Cancer
Thyroid cancer occurs when a lump, or nodule, in the thyroid gland is cancerous.
Thyroid Cancer and I-131
Thyroid cancer accounts for a little less than 4 percent of all cancers diagnosed in the United States. Incidence has been going up in recent years, in part due to increased detection. Researchers suspect that rising rates of obesity are also influencing rates. However, these two factors do not fully explain the increases. Typically, thyroid cancer is slow-growing, highly treatable, and usually curable. About 98 out of 100 people who are diagnosed with thyroid cancer survive the disease for at least five years, and about 92 out of 100 people survive the disease for at least 20 years after diagnosis.
The cause of most cases of thyroid cancer is not known. Exposure to I-131 can increase the risk of thyroid cancer. It is thought that risk is higher for people who have had multiple exposures and for people exposed at a younger age. But even among people who have documented exposures to I-131, few develop this cancer. It is known that children have a higher-than-average risk of developing thyroid cancer many years later if they were exposed to radiation. This knowledge comes from studies of people exposed to x-ray treatments for childhood cancer or noncancerous head and neck conditions, or as a result of direct radiation from the atomic bombings of Hiroshima and Nagasaki.
The thyroid gland in adults, however, appears to be more resistant to the effects of radiation. There appears to be little risk of developing thyroid cancer from exposure to I-131 or other radiation sources as an adult.
How can people reach a sound decision about their risk of thyroid cancer? When is it time to visit a doctor?
A “personal risk profile” includes four key points that may influence a person’s decision to visit a doctor or other health professional for evaluation:
Age—People who were born between 1936 and 1963 and were children at the time of testing are at higher risk.
Milk drinking—Childhood milk drinkers, particularly those who drank large quantities of milk or those who drank unprocessed milk from farm or backyard cows and goats, have increased risk.
Childhood residence—The Mountain West, Midwest, East, and Northeast areas of the United States generally were more affected by I-131 fallout from nuclear testing.
Medical signs—A lump or nodule that an individual can see or feel in the area of the thyroid gland requires attention. If you can see or feel a lump or nodule, it is important that you see a doctor.
Key Facts
Scientists know that:
I-131 breaks down rapidly in the atmosphere and environment
Exposure was highest in the first few days after each nuclear test explosion
Most exposure occurred through drinking fresh milk
People received little exposure from eating fruits and leafy vegetables as compared to drinking fresh milk because although I-131 was deposited on fruits and leafy vegetables, the I-131 in fallout was deposited only on the surface; people generally wash or peel fruits and leafy vegetables
Thyroid cancer is uncommon, usually curable, and approximately 2 to 3 times more common in women
Reliable information about I-131’s impact on human health has been difficult to collect, but scientists think that:
Risk for thyroid cancer increases with exposure, but even among people exposed to I-131, few develop this cancer
People exposed as children have a higher risk than people exposed as adults
Taking Care of Yourself
Key steps to estimating personal risk of thyroid cancer, and taking charge of personal thyroid health include:
Using the “personal risk profile” described above (see Who’s at Risk?)
Using the thyroid dose and risk calculator to estimate radiation dose and risk of developing thyroid cancer from fallout exposure from nuclear tests
Taking this material to a health care professional to discuss dose estimates and steps—if any—required for further evaluation
Getting more information by calling NCI’s Cancer Information Service at 1-800-4-CANCER
Radon test kits can be used to check the radon levels in homes and other buildings.
Credit: National Cancer Institute
What is radon?
Radon is a radioactive gas that is released from the normal decay of the elements uranium, thorium, and radium in rocks and soil. The invisible, odorless gas seeps up through the ground and diffuses into the air. In a few areas, depending on local geology, radon dissolves into ground water and can be released into the air when the water is used. Radon gas usually exists at very low levels outdoors, but the gas can accumulate in areas without adequate ventilation, such as underground mines.
How are people exposed to radon?
Radon is present in nearly all air, so everyone breathes in radon every day, usually at very low levels. Radon can enter homes through cracks in floors, walls, or foundations, and collect indoors. It can also be released from building materials or from water obtained from wells that contain radon. Radon levels may be higher in homes that are well insulated, tightly sealed, and/or built on soil rich in the elements uranium, thorium, and radium. Basements and first floors typically have the highest radon levels because of their closeness to the ground.
Workers employed in uranium, hard rock, and phosphate mining potentially are exposed to radon at high concentrations. Uranium miners generally are believed to have the highest exposures.
Which cancers are associated with exposure to radon?
Radon was identified as a health problem when scientists noted that underground uranium miners who were exposed to it died of lung cancer at high rates. Experimental studies in animals confirmed the results of the miner studies by showing higher rates of lung tumors among rodents exposed to high levels of radon. There has been a suggestion of an increased risk of leukemia associated with radon exposure in adults and children; the evidence, however, is not conclusive.
How can exposures be reduced?
Check the radon levels in your home regularly. The U.S. Environmental Protection Agency has more information about residential radon exposure and what people can do about it in its Consumer’s Guide to Radon Reduction: How to Fix Your Home.
Selected References:
International Agency for Research on Cancer. Man-Made Mineral Fibres and Radon, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 43. Lyon, France: World Health Organization, 1988. Also available online. Last accessed June 6, 2023.
National Toxicology Program. Ionizing Radiation, Report on Carcinogens, Fifteenth Edition. Triangle Park, NC: National Institute of Environmental Health and Safety, 2021. Also available online. Last accessed June 6, 2023.
U.S. Environmental Protection Agency. A Citizen’s Guide to Radon: The Guide to Protecting Yourself and Your Family from Radon. Washington, DC: U.S. Environmental Protection Agency, 2016. Available online. Last accessed June 6, 2023.
World Health Organization. WHO Handbook on Indoor Radon: A Public Health Perspective. Geneva, Switzerland: World Health Organization, 2009. Also available online. Last accessed June 6, 2023.
Radiation of certain wavelengths, called ionizing radiation, has enough energy to damage DNA and cause cancer. Ionizing radiation includes radon, x-rays, gamma rays, and other forms of high-energy radiation. Lower-energy, non-ionizing forms of radiation, such as visible light and the energy from cell phones, have not been found to cause cancer in people.
Radon
Radon is a radioactive gas given off by rocks and soil. Radon is formed when the radioactive element radium breaks down. Radium in turn is formed when the radioactive elements uranium and thorium break down. People who are exposed to high levels of radon have an increased risk of lung cancer.
If you live in an area of the country that has high levels of radon in its rocks and soil, you may wish to test your home for this gas. Home radon tests are easy to use and do not cost much. Most hardware stores sell test kits. There are many ways to lessen the amount of radon in a home to a safe level. For more information on radon, see the Radon page and the Radon and Cancer fact sheet.
X-Rays and Other Sources of Radiation
High-energy radiation, such as x-rays, gamma rays, alpha particles, beta particles, and neutrons, can damage DNA and cause cancer. These forms of radiation can be released in accidents at nuclear power plants and when atomic weapons are made, tested, or used.
Certain medical procedures, such as chest x-rays, computed tomography (CT) scans, positron emission tomography (PET) scans, and radiation therapy can also cause cell damage that leads to cancer. However, the risks of cancer from these medical procedures are very small, and the benefit from having them is almost always greater than the risks.
Talk with your doctor if you think you may be at risk for cancer because you were exposed to radiation. People considering CT scans should talk with their doctors about whether the procedure is necessary for them and about its risks and benefits. Cancer patients may want to talk with their doctors about how radiation treatment could increase their risk for a second cancer later on.
Electric and magnetic fields are invisible areas of energy (also called radiation) that are produced by electricity, which is the movement of electrons, or current, through a wire.
An electric field is produced by voltage, which is the pressure used to push the electrons through the wire, much like water being pushed through a pipe. As the voltage increases, the electric field increases in strength. Electric fields are measured in volts per meter (V/m).
A magnetic field results from the flow of current through wires or electrical devices and increases in strength as the current increases. The strength of a magnetic field decreases rapidly with increasing distance from its source. Magnetic fields are measured in microteslas (μT, or millionths of a tesla).
Electric fields are produced whether or not a device is turned on, whereas magnetic fields are produced only when current is flowing, which usually requires a device to be turned on. Power lines produce magnetic fields continuously because current is always flowing through them. Electric fields are easily shielded or weakened by walls and other objects, whereas magnetic fields can pass through buildings, living things, and most other materials.
Electric and magnetic fields together are referred to as electromagnetic fields, or EMFs. The electric and magnetic forces in EMFs are caused by electromagnetic radiation. There are two main categories of EMFs:
Higher-frequency EMFs, which include x-rays and gamma rays. These EMFs are in the ionizing radiation part of the electromagnetic spectrum and can damage DNA or cells directly.
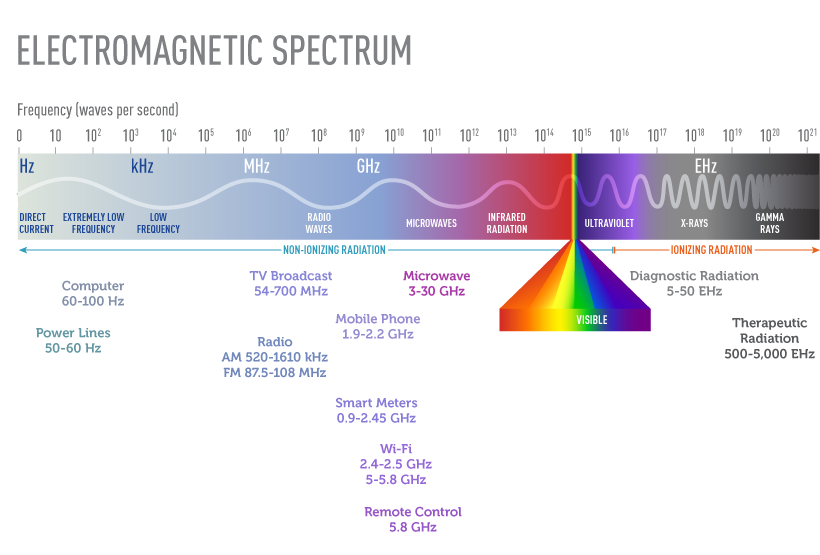
Low- to mid-frequency EMFs, which include static fields (electric or magnetic fields that do not vary with time), magnetic fields from electric power lines and appliances, radio waves, microwaves, infrared radiation, and visible light. These EMFs are in the non-ionizing radiation part of the electromagnetic spectrum and are not known to damage DNA or cells directly. Low- to mid-frequency EMFs include extremely low frequency EMFs (ELF-EMFs) and radiofrequency EMFs. ELF-EMFs have frequencies of up to 300 cycles per second, or hertz (Hz), and radiofrequency EMFs range from 3 kilohertz (3 kHz, or 3,000 Hz) to 300 gigahertz (300 GHz, or 300 billion Hz). Radiofrequency radiation is measured in watts per meter squared (W/m2).
The electromagnetic spectrum represents all of the possible frequencies of electromagnetic energy. It ranges from extremely long wavelengths (extremely low frequency exposures such as those from power lines) to extremely short wavelengths (x-rays and gamma rays) and includes both non-ionizing and ionizing radiation.
What are common sources of non-ionizing EMFs?
There are both natural and human-made sources of non-ionizing EMFs. The earth’s magnetic field, which causes the needle on a compass to point North, is one example of a naturally occurring EMF.
Human-made EMFs fall into both the ELF and radiofrequency categories of non-ionizing part of the electromagnetic spectrum. These EMFs can come from a number of sources.
Extremely low frequency EMFs (ELF-EMFs). Sources of ELF-EMFs include power lines, electrical wiring, and electrical appliances such as shavers, hair dryers, and electric blankets.
Radiofrequency radiation. The most common sources of radiofrequency radiation are wireless telecommunication devices and equipment, including cell phones, smart meters, and portable wireless devices, such as tablets and laptop computers (1). In the United States, cell phones currently operate in a frequency range of about 1.8 to 2.2 GHz (2). (For more information about cell phones, see the NCI fact sheet Cell Phones and Cancer Risk.)
Other common sources of radiofrequency radiation include:
Radio and television signals. AM/FM radios and older VHF/UHF televisions operate at lower radiofrequencies than cell phones. Radio signals are AM (amplitude-modulated) or FM (frequency-modulated). AM radio is used for broadcasting over very long distances, whereas FM radio covers more localized areas. AM signals are transmitted from large arrays of antennas that are placed at high elevation on sites that are off limits to the general public because exposures close to the source can be high. Maintenance workers could receive substantial radiofrequency exposures from AM radio antennas, but the general public would not. FM radio antennas and TV broadcasting antennas, which are much smaller than AM antennas, are generally mounted at the top of high towers. Radiofrequency exposures near the base of these towers are below guideline limits (3), so exposure of the general population is very low. Sometimes small local radio and TV antennas are mounted on the top of a building; access to the roof of such buildings is usually controlled.
Radar, satellite stations, magnetic resonance imaging (MRI) devices, and industrial equipment.These operate at somewhat higher radiofrequencies than cell phones (1).
Microwave ovens used in homes, which also operate at somewhat higher radiofrequencies than cell phones (1). Microwave ovens are manufactured with effective shielding that has reduced the leakage of radiofrequency radiation from these appliances to barely detectable levels.
Cordless telephones, which can operate on analogue or DECT (Digital Enhanced Cordless Telecommunications) technology and typically emit radiofrequencies similar to those of cell phones. However, because cordless phones have a limited range and require a nearby base, their signal strengths are generally much lower than those of cell phones (1).
Cell phone base stations. Antenna towers or base stations, including those for mobile phone networks and for broadcasting for radio and for television, emit various types of radiofrequency energy. Because the majority of individuals in the general population are exposed only intermittently to base stations and broadcast antennas, it is difficult to estimate exposures for a population (4). The strength of these exposures varies based on the population density of the region, the average distance from the source, and the time of day or the day of the week (lower exposures on the weekends or at night) (1). A study that used using personal portable exposure meters to assess exposures to different sources of radiofrequency EMFs among children in Europe found that the single largest contributor to the total radiofrequency EMF exposure was the proximity to base stations (5).
In general, exposures decrease with increasing distance from the source (6). Exposures among maintenance workers have been found to vary depending on their tasks, the type of antenna, and the location of the worker in relation to the source (1). Cumulative exposures of such workers are very difficult to estimate.
Televisions and computer screens produce electric and magnetic fields at various frequencies, as well as static electric fields. The liquid crystal displays found in some laptop and desktop computers do not produce substantial electric or magnetic fields. Modern computers have conductive screens that reduce static fields produced by the screen to normal background levels.
Wireless local area networks, commonly known as Wi-Fi. These are specific types of wireless networking systems and an increasingly common source of radiofrequency radiation. Wireless networks use radio waves to connect Wi-Fi–enabled devices to an access point that is connected to the internet, either physically or through some form of data connection. Most Wi-Fi devices operate at radiofrequencies that are broadly similar to cell phones, typically 2.4 to 2.5 GHz, although in recent years Wi-Fi devices that operate at somewhat higher frequencies (5, 5.3, or 5.8 GHz) have appeared (7). Radiofrequency radiation exposure from Wi-Fi devices is considerably lower than that from cell phones (8). Both sources emit levels of radiofrequency radiation that are far below the guideline of 10 W/m2 as specified by the International Commission on Non-Ionizing Radiation Protection (3).
Digital electric and gas meters, also known as “smart meters.” These devices, which operate at about the same radiofrequencies as cell phones, transmit information on consumption of electricity or gas to utility companies. Smart meters produce very low level fields that sometimes cannot be distinguished from the total background radiofrequency radiation levels inside a home (9).
For household appliances and other devices used in the home that require electricity, magnetic field levels are highest near the source of the field and decrease rapidly the farther away the user is from the source. Magnetic fields drop precipitously at a distance of about 1 foot from most appliances. For computer screens, at a distance of 12–20 inches from the screen that most persons using computers sit, magnetic fields are similarly dramatically lower.
Why are non-ionizing EMFs studied in relation to cancer?
Power lines and electrical appliances that emit non-ionizing EMFs are present everywhere in homes and workplaces. For example, wireless local networks are nearly always “on” and are increasingly commonplace in homes, schools, and many public places.
No mechanism by which ELF-EMFs or radiofrequency radiation could cause cancer has been identified. Unlike high-energy (ionizing) radiation, EMFs in the non-ionizing part of the electromagnetic spectrum cannot damage DNA or cells directly. Some scientists have speculated that ELF-EMFs could cause cancer through other mechanisms, such as by reducing levels of the hormone melatonin. There is some evidence that melatonin may suppress the development of certain tumors.
Studies of animals have not provided any indications that exposure to ELF-EMFs is associated with cancer (10–13). The few high-quality studies in animals have provided no evidence that Wi-Fi is harmful to health (8).
Although there is no known mechanism by which non-ionizing EMFs could damage DNA and cause cancer, even a small increase in risk would be of clinical importance given how widespread exposure to these fields is.
What have studies shown about possible associations between non-ionizing EMFs and cancer in children?
Numerous epidemiologic studies and comprehensive reviews of the scientific literature have evaluated possible associations between exposure to non-ionizing EMFs and risk of cancer in children (13–15). (Magnetic fields are the component of non-ionizing EMFs that are usually studied in relation to their possible health effects.) Most of the research has focused on leukemia and brain tumors, the two most common cancers in children. Studies have examined associations of these cancers with living near power lines, with magnetic fields in the home, and with exposure of parents to high levels of magnetic fields in the workplace. No consistent evidence for an association between any source of non-ionizing EMF and cancer has been found.
Exposure from power lines. Although a study in 1979 pointed to a possible association between living near electric power lines and childhood leukemia (16), more recent studies have had mixed findings (17–25). Most of these studies did not find an association or found one only for those children who lived in homes with very high levels of magnetic fields, which are present in few residences.
Several studies have analyzed the combined data from multiple studies of power line exposure and childhood leukemia:
A pooled analysis of nine studies reported a twofold increase in risk of childhood leukemia among children with exposures of 0.4 μT or higher. Less than 1% of the children in the studies experienced this level of exposure (26).
A meta-analysis of 15 studies observed a 1.7-fold increase in childhood leukemia among children with exposures of 0.3 μT or higher. A little more than 3% of children in the studies experienced this level of exposure (27).
More recently, a pooled analysis of seven studies published after 2000 reported a 1.4-fold increase in childhood leukemia among children with exposures of 0.3 μT or higher. However, less than one half of 1% of the children in the studies experienced this level of exposure (28).
For the two pooled studies and the meta-analysis, the number of highly exposed children was too small to provide stable estimates of the dose–response relationship. This means that the findings could be interpreted to reflect linear increases in risk, a threshold effect at 0.3 or 0.4 μT, or no significant increase.
The interpretation of the finding of increased childhood leukemia risk among children with the highest exposures (at least 0.3 μT) is unclear.
Exposure from electrical appliances. Another way that children can be exposed to magnetic fields is from household electrical appliances. Although magnetic fields near many electrical appliances are higher than those near power lines, appliances contribute less to a person’s total exposure to magnetic fields because most appliances are used for only short periods of time. And moving even a short distance from most electrical appliances reduces exposure dramatically. Again, studies have not found consistent evidence for an association between the use of household electrical appliances and risk of childhood leukemia (29).
Exposure to Wi-Fi. In view of the widespread use of Wi-Fi in schools, the UK Health Protection Agency (now part of Public Health England) has conducted the largest and most comprehensive measurement studies to assess exposures of children to radiofrequency electromagnetic fields from wireless computer networks (30, 31). This agency concluded that radiofrequency exposures were well below recommended maximum levels and that there was “no reason why Wi-Fi should not continue to be used in schools and in other places” (32).
A review of the published literature concluded that the few high-quality studies to date provide no evidence of biological effects from Wi-Fi exposures (7).
Exposure from cell phone base stations. Few studies have examined cancer risk in children living close to cell phone base stations or radio or television transmitters. Mobile phone base stations transmit and receive radiofrequency signals to and from mobile phones near the station. None of the studies that estimated exposures on an individual level found an increased risk of pediatric tumors (33–35).
Parental exposure and risk in offspring. Several studies have examined possible associations between maternal or paternal exposure to high levels of magnetic fields before conception and/or during pregnancy and the risk of cancer in their future children. The results to date have been inconsistent (36, 37). This question requires further evaluation.
Exposure and cancer survival. A few studies have investigated whether magnetic field exposure is associated with prognosis or survival of children with leukemia. Several small retrospective studies of this question have yielded inconsistent results (38–40). An analysis that combined prospective data for more than 3,000 children with acute lymphoid leukemia from eight countries showed that ELF magnetic field exposure was not associated with their survival or risk of relapse (41).
What have studies shown about possible associations between non-ionizing EMFs and cancer in adults?
Many studies have examined the association between non-ionizing EMF exposure and cancer in adults, of which few studies have reported evidence of increased risk (1).
Residential exposures. The majority of epidemiologic studies have shown no relationship between breast cancer in women and exposure to extremely low frequency EMFs (ELF-EMFs) in the home (42–45), although a few individual studies have suggested an association; only one reported results that were statistically significant (46).
Workplace exposures to ELF radiation. Several studies conducted in the 1980s and early 1990s reported that people who worked in some electrical occupations that exposed them to ELF radiation (such as power station operators and telephone line workers) had higher-than-expected rates of some types of cancer, particularly leukemia, brain tumors, and male breast cancer (13). Most of the results were based on participants’ job titles and not on actual measurements of their exposures. More recent studies, including some that considered exposure measurements as well as job titles, have generally not shown an increasing risk of leukemia, brain tumors, or female breast cancer with increasing exposure to magnetic fields at work (46–51).
Workplace exposures to radiofrequency radiation. A limited number of studies have evaluated risks of cancer in workers exposed to radiofrequency radiation. A large study of U.S. Navy personnel found no excess of brain tumors among those with a high probability of exposure to radar (including electronics technicians, aviation technicians, and fire control technicians); however, nonlymphocytic leukemia, particularly acute myeloid leukemia, was increased in electronics technicians in aviation squadrons, but not in Navy personnel in the other job categories (52). A case–control study among U.S. Air Force personnel found the suggestion of an increased risk of brain cancer among personnel who maintained or repaired radiofrequency or microwave-emitting equipment (53). A case–control study found the suggestion of an increased risk of death from brain cancer among men occupationally exposed to microwave and/or radiofrequency radiation, with all of the excess risk among workers in electrical and electronics jobs involving design, manufacture, repair, or installation of electrical or electronics equipment (54). There was no evidence that electrical utility workers who were exposed to pulsed electromagnetic fields produced by power lines were more likely to develop brain tumors or leukemia than the general population (55). Employees of a large manufacturer of wireless communication products were not more likely to die from brain tumors or cancers of the hematopoietic or lymphatic system than the general population (56). A large prospective study among police officers in Great Britain found no evidence for an association between radiofrequency EMF exposure from personal radio use and the risk of all cancers combined (57). A large multinational population-based case–control study found no clear evidence that occupational exposures to radiofrequency radiation are associated with increased risks of glioma or meningioma (58).
What do expert organizations conclude about the cancer risk from EMFs?
In 2002, the International Agency for Research on Cancer (IARC), a component of the World Health Organization, appointed an expert Working Group to review all available evidence on static and extremely low frequency electric and magnetic fields (13). The Working Group classified ELF-EMFs as “possibly carcinogenic to humans,” based on limited evidence from human studies in relation to childhood leukemia. Static electric and magnetic fields and extremely low frequency electric fields were determined “not classifiable as to their carcinogenicity to humans” (13).
In 2015, the European Commission Scientific Committee on Emerging and Newly Identified Health Risks reviewed electromagnetic fields in general, as well as cell phones in particular. It found that, overall, epidemiologic studies of extremely low frequency fields show an increased risk of childhood leukemia with estimated daily average exposures above 0.3 to 0.4 μT, although no mechanisms have been identified and there is no support from experimental studies that explains these findings. It also found that the epidemiologic studies on radiofrequency exposure do not show an increased risk of brain tumors or other cancers of the head and neck region, although the possibility of an association with acoustic neuroma remains open (59).
Where can people find additional information on EMFs?
The National Institute of Environmental Health Sciences (NIEHS) website has information about EMFs and cancer.
The Occupational Safety and Health Administration website has information about workplace exposures to ELF-EMF.
The US Environmental Protection Agency website has information on power lines and other sources of EMF.
The European Commission also has general information on EMF.
The World Health Organization website also has information on EMF.
Why has there been concern that cell phones may cause cancer?
There are two main reasons why people are concerned that cell (or mobile) phones might have the potential to cause certain types of cancer or other health problems: Cell phones emit radiation (in the form of radiofrequency radiation, or radio waves), and cell phone use is widespread. Even a small increase in cancer risk from cell phones would be of concern given how many people use them.
Brain and central nervous system cancers have been of particular concern because hand-held phones are used close to the head and because ionizing radiation—a higher energy form of radiation than what cell phones emit—has been found to cause some brain cancers. Many different kinds of studies have been carried out to try to investigate whether cell phone use is dangerous to human health.
However, the evidence to date suggests that cell phone use does not cause brain or other kinds of cancer in humans.
Is the radiation from cell phones harmful?
Cell phones emit radiation in the radiofrequency region of the electromagnetic spectrum. Second-, third-, and fourth-generation cell phones (2G, 3G, 4G) emit radiofrequency in the frequency range of 0.7–2.7 GHz. Fifth-generation (5G) cell phones are anticipated to use the frequency spectrum up to 80 GHz.
These frequencies all fall in the nonionizing range of the spectrum, which is low frequency and low energy. The energy is too low to damage DNA. By contrast, ionizing radiation, which includes x-rays, radon, and cosmic rays, is high frequency and high energy. Energy from ionizing radiation can damage DNA. DNA damage can cause changes to genes that may increase the risk of cancer.
The human body does absorb energy from devices that emit radiofrequency radiation. The only consistently recognized biological effect of radiofrequency radiation absorption in humans that the general public might encounter is heating to the area of the body where a cell phone is held (e.g., the ear and head). However, that heating is not sufficient to measurably increase core body temperature. There are no other clearly established dangerous health effects on the human body from radiofrequency radiation.
Has the incidence of brain and central nervous system cancers changed during the time cell phone use increased?
No. Investigators have studied whether the incidence of brain or other central nervous system cancers (that is, the number of new cases of these cancers diagnosed each year) has changed during the time that cell phone use increased dramatically. These studies found:
stable incidence rates for adult gliomas in the United States (1), Nordic countries (2) and Australia (3) during the past several decades
stable incidence rates for pediatric brain tumors in the United States during 1993–2013 (4)
stable incidence rates for acoustic neuroma (5), which are nonmalignant tumors, and meningioma (6), which are usually nonmalignant, among US adults since 2009
In addition, studies using cancer incidence data have tested different scenarios (simulations) determining whether the incidence trends are in line with various levels of risk as reported in studies of cell phone use and brain tumors between 1979 and 2008 (7, 8). These simulations showed that many risk changes reported in case–control studies were not consistent with incidence data, implying that biases and errors in the study may have distorted the findings.
Because these studies examine cancer incidence trends over time in populations rather than comparing risk in people who do and don’t use cell phones, their ability to observe potential small differences in risk among heavy users or susceptible populations is limited. Observational/epidemiologic studies—including case–control and cohort studies (described below)—are designed to measure individual exposure to cell phone radiation and ascertain specific health outcomes.
How is radiofrequency radiation exposure measured in studies of groups of people?
Epidemiologic studies use information from several sources, including questionnaires and data from cell phone service providers, to estimate radiofrequency radiation exposure in groups of people. Direct measurements are not yet possible outside of a laboratory setting. Estimates from studies reported to date take into account the following:
How regularly study participants use cell phones (the number of calls per week or month)
The age and the year when study participants first used a cell phone and the age and the year of last use (allows calculation of the duration of use and time since the start of use)
The average number of cell phone calls per day, week, or month (frequency)
The average length of a typical cell phone call
The total hours of lifetime use, calculated from the length of typical call times, the frequency of use, and the duration of use
What has research shown about the link between cell phone use and cancer risk?
Researchers have carried out several types of population studies to investigate the possibility of a relationship between cell phone use and the risk of tumors, both malignant (cancerous) and nonmalignant (not cancer). Epidemiologic studies (also called observational studies) are research studies in which investigators observe groups of individuals (populations) and collect information about them but do not try to change anything about the groups.
Two main types of epidemiologic studies—cohort studies and case–control studies—have been used to examine associations between cell phone use and cancer risk. In a case–control study, cell phone use is compared between people who have tumors and people who don’t. In a cohort study, a large group of people who do not have cancer at the beginning of the study is followed over time and tumor development in people who did and didn’t use cell phones is compared. Cohort studies are limited by the fact that they may only be able to look at cell phone subscribers, who are not necessarily the cell phone users.
The tumors that have been investigated in epidemiologic studies include malignant brain tumors, such as gliomas, as well as nonmalignant tumors, such as acoustic neuroma (tumors in the cells of the nerve responsible for hearing that are also known as vestibular schwannomas), meningiomas (usually nonmalignant tumors in the membranes that cover and protect the brain and spinal cord), parotid gland tumors (tumors in the salivary glands), skin cancer, and thyroid gland tumors.
Four large epidemiologic studies have examined the possible association between cell phone use and cancer: Interphone, a case–control study, and three cohort studies, the Danish Study, the Million Women Study, and the Cohort Study on Mobile Phones and Health (COSMOS). The findings of these studies are mixed, but overall, they do not show an association between cell phone use and cancer (9–23).
Interphone Case–Control Study
How the study was done: This is the largest case–control study of cell phone use and the risk of head and neck tumors. It was conducted by a consortium of researchers from 13 countries. The data came from questionnaires that were completed by study participants in Europe, Israel, Canada, Australia, New Zealand, and Japan.
What the study showed: Most published analyses from this study have shown no increases overall in brain or other central nervous system cancers (glioma and meningioma) related to higher amounts of cell phone use. One analysis showed a statistically significant, although small, increase in the risk of glioma among study participants who spent the most total time on cell phone calls. However, for a variety of reasons the researchers considered this finding inconclusive (11–13).
An analysis of data from all 13 countries reported a statistically significant association between intracranial distribution of tumors within the brain and self-reported location of the phone (14). However, the authors of this study noted that it is not possible to draw firm conclusions about cause and effect based on their findings.
An analysis of data from five Northern European countries showed an increased risk of acoustic neuroma in those who had used a cell phone for 10 or more years (15).
In subsequent analyses of Interphone data, investigators investigated whether tumors were more likely to form in areas of the brain with the highest exposure. One analysis showed no relationship between tumor location and level of radiation (16). However, another found evidence that glioma and, to a lesser extent, meningioma were more likely to develop where exposure was highest (17).
Danish Cohort Study
How the study was done: This cohort study linked billing information from more than 358,000 cell phone subscribers with brain tumor incidence data from the Danish Cancer Registry.
What the study showed: No association was observed between cell phone use and the incidence of glioma, meningioma, or acoustic neuroma, even among people who had been cell phone subscribers for 13 or more years (18–20).
Million Women Cohort Study
How the study was done: This prospective cohort study conducted in the United Kingdom used data obtained from questionnaires that were completed by study participants.
What the study showed: Self-reported cell phone use was not associated with an increased risk of glioma, meningioma, or non-central nervous system tumors. Although the original published findings reported an association with an increased risk of acoustic neuroma (21), it was not observed with additional years of follow-up of the cohort (22).
Cohort Study of Mobile Phones and Health (COSMOS)
How the study was done: This large prospective cohort study conducted in Denmark, Finland, Sweden, the Netherlands, and the United Kingdom used data on health, lifestyle, and current and past cell phone use obtained from a questionnaire completed by participants when they joined the study. That information was supplemented with cancer occurrence data obtained from linkage to national cancer registries and cell phone records obtained from mobile network operators.
What the study showed: Among 264,574 participants with a median follow-up of just over 7 years, the cumulative amount of mobile phone call-time was not associated with the risk of developing glioma, meningioma, or acoustic neuroma (23). No associations with cancer risk were seen in the heaviest mobile phone users or among among those with the longest history of mobile phone use (15 or more years).
Other Epidemiologic Studies
In addition to these four large studies, other, smaller epidemiologic studies have looked for associations between cell phone use and individual cancers in both adults and children. These include:
Two NCI-sponsored case–control studies, each conducted in multiple US academic medical centers or hospitals between 1994 and 1998 that used data from questionnaires (24) or computer-assisted personal interviews (25). Neither study showed a relationship between cell phone use and the risk of glioma, meningioma, or acoustic neuroma in adults.
The CERENAT study, another case–control study conducted in multiple areas in France from 2004 to 2006 using data collected in face-to-face interviews using standardized questionnaires (26). This study found no association for either gliomas or meningiomas when comparing adults who were regular cell phone users with non-users. However, the heaviest users had significantly increased risks of both gliomas and meningiomas.
A pooled analysis of two case–control studies conducted in Sweden that reported statistically significant trends of increasing brain cancer risk for the total amount of cell phone use and the years of use among people who began using cell phones before age 20 (27).
Another case–control study in Sweden, part of the Interphone pooled studies, did not find an increased risk of brain cancer among long-term cell phone users between the ages of 20 and 69 (28).
The CEFALO study, an international case–control study of children diagnosed with brain cancer between ages 7 and 19, found no relationship between their cell phone use and risk for brain cancer (29).
The MOBI-Kids study, a large international case–control study of young people ages 10 to 24 years diagnosed with brain tumors, found no evidence of an association between wireless phone use and the risk of brain tumors (30).
A population-based case–control study conducted in Connecticut found no association between cell phone use and the risk of thyroid cancer (31).
What are the findings from studies of the human body?
Researchers have carried out several kinds of studies to investigate possible effects of cell phone use on the human body. In 2011, two small studies were published that examined brain glucose metabolism in people after they had used cell phones. The results were inconsistent. One study showed increased glucose metabolism in the region of the brain close to the antenna compared with tissues on the opposite side of the brain (32); the other study (33) found reduced glucose metabolism on the side of the brain where the phone was used.
The authors of these studies noted that the results were preliminary and that possible health outcomes from changes in glucose metabolism in humans were unknown. Such inconsistent findings are not uncommon in experimental studies of the physiological effects of radiofrequencyelectromagnetic radiation in people (11). Some factors that can contribute to inconsistencies across such studies include assumptions used to estimate doses, failure to consider temperature effects, and investigators not being blinded to exposure status.
Another study investigated blood flow in the brain of people exposed to radiofrequency radiation from cell phones and found no evidence of an effect on blood flow in the brain (34).
What are the findings from experiments in laboratory animals?
Early studies involving laboratory animals showed no evidence that radiofrequency radiation increased cancer risk or enhanced the cancer-causing effects of known chemical carcinogens (35–38).
Because of inconsistent findings from epidemiologic studies in humans and the lack of clear data from previous experimental studies in animals, in 1999 the Food and Drug Administration (FDA) nominated radiofrequency radiation exposure associated with cell phone exposures for study in animal models by the US National Toxicology Program (NTP). NTP is an interagency program that coordinates toxicology research and testing across the US Department of Health and Human Services and is headquartered at the National Institute of Environmental Health Sciences, part of NIH.
The NTP studied radiofrequency radiation (2G and 3G frequencies) in rats and mice (39, 40). This large project was conducted in highly specialized labs. The rodents experienced whole-body exposures of 3, 6, or 9 watts per kilogram of body weight for 5 or 7 days per week for 18 hours per day in cycles of 10 minutes on, 10 minutes off. A research overview of the rodent studies, with links to the peer-review summary, is available on the NTP website. The primary outcomes observed were a small number of cancers of Schwann cells in the heart and non-cancerous changes (hyperplasia) in the same tissues for male rats, but not female rats, nor in mice overall.
These experimental findings raise new questions because cancers in the heart are extremely rare in humans. Schwann cells of the heart in rodents are similar to the kind of cells in humans that give rise to acoustic neuromas (also known as vestibular schwannomas), which some studies have suggested are increased in people who reported the heaviest use of cell phones. The NTP plans to continue to study radiofrequency exposure in animal models to provide insights into the biological changes that might explain the outcomes observed in their study.
Another animal study, in which rats were exposed 7 days per week for 19 hours per day to radiofrequency radiation at 0.001, 0.03, and 0.1 watts per kilogram of body weight was reported by investigators at the Italian Ramazzini Institute (41). Among the rats with the highest exposure levels, the researchers noted an increase in heart schwannomas in male rats and nonmalignant Schwann cell growth in the heart in male and female rats. However, key details necessary for interpretation of the results were missing: exposure methods, other standard operating procedures, and nutritional/feeding aspects. The gaps in the report from the study raise questions that have not been resolved.
ICNIRP (an independent nonprofit organization that provides scientific advice and guidance on the health and environmental effects of nonionizing radiation) critically evaluated both studies. It concluded that both followed good laboratory practice, including using more animals than earlier research and exposing the animals to radiofrequency radiation throughout their lifetimes. However, it also identified what it considered major weaknesses in how the studies were conducted and statistically analyzed and concluded that these limitations prevent drawing conclusions about the ability of radiofrequency exposures to cause cancer (42).
Why are the findings from different studies of cell phone use and cancer risk inconsistent?
A few studies have shown some evidence of statistical association of cell phone use and brain tumor risks in humans, but most studies have found no association. Reasons for these discrepancies include the following:
Recall bias, which can occur when data about prior habits and exposures are collected from study participants using questionnaires administered after diagnosis of a disease in some of the participants. Study participants who have brain tumors, for example, may remember their cell phone use differently from individuals without brain tumors.
Inaccurate reporting, which can happen when people say that something has happened more often or less often than it actually did. For example, people may not remember how much they used cell phones in a given time period.
Morbidity and mortality among study participants who have brain cancer. Gliomas are particularly difficult to study because of their high death rate and the short survival of people who develop these tumors. Patients who survive initial treatment are often impaired, which may affect their responses to questions.
Participation bias, which can happen when people who are diagnosed with brain tumors are more likely than healthy people (known as controls) to enroll in a research study.
Changing technology. Older studies evaluated radiofrequency radiation exposure from analog cell phones. Today, cell phones use digital technology, which operates at a different frequency and a lower power level than analog phones, and cellular technology continues to change (43).
Exposure assessment limitations. Different studies measure exposure differently, which makes it difficult to compare the results of different studies (44). Investigations of sources and levels of exposure, particularly in children, are ongoing (45).
Insufficient follow-up of highly exposed populations. It may take a very long time to develop symptoms after exposure to radiofrequency radiation, and current studies may not yet have followed participants long enough.
Inadequate statistical power and methods to detect very small risks or risks that affect small subgroups of people specifically
Chance as an explanation of apparent effects may not have been considered.
What are other possible health effects from cell phone use?
The most consistent health risk associated with cell phone use is distracted driving and vehicle accidents (46, 47). Several other potential health effects have been reported with cell phone use. Neurologic effects are of particular concern in young persons. However, studies of memory, learning, and cognitive function have generally produced inconsistent results (48–51).
What have expert organizations said about the cancer risk from cell phone use?
In 2011, the International Agency for Research on Cancer (IARC), a component of the World Health Organization, appointed an expert working group to review all available evidence on the use of cell phones. The working group classified cell phone use as “possibly carcinogenic to humans,” based on limited evidence from human studies, limited evidence from studies of radiofrequency radiation and cancer in rodents, and inconsistent evidence from mechanistic studies (11).
The working group indicated that, although the human studies were susceptible to bias, the findings could not be dismissed as reflecting bias alone, and that a causal interpretation could not be excluded. The working group noted that any interpretation of the evidence should also consider that the observed associations could reflect chance, bias, or confounding variables rather than an underlying causal effect. In addition, the working group stated that the investigation of brain cancer risk associated with cell phone use poses complex research challenges.
The American Cancer Society’s cell phones page states “It is not clear at this time that RF (radiofrequency) waves from cell phones cause dangerous health effects in people, but studies now being done should give a clearer picture of the possible health effects in the future.”
The US Food and Drug Administration (FDA) notes that studies reporting biological changes associated with radiofrequency radiation have failed to be replicated and that the majority of human epidemiologic studies have failed to show a relationship between exposure to radiofrequency radiation from cell phones and health problems. FDA, which originally nominated this exposure for review by the NTP in 1999, issued a statement on the draft NTP reports released in February 2018, saying “based on this current information, we believe the current safety limits for cell phones are acceptable for protecting the public health.” FDA and the Federal Communications Commission (FCC) share responsibility for regulating cell phone technologies.
The Federal Communications Commission (FCC) concludes that currently no scientific evidence establishes a definite link between wireless device use and cancer or other illnesses.
In 2015, the European Commission Scientific Committee on Emerging and Newly Identified Health Risks concluded that, overall, the epidemiologic studies on cell phone radiofrequency electromagnetic radiation exposure do not show an increased risk of brain tumors or of other cancers of the head and neck region (9). The committee also stated that epidemiologic studies do not indicate increased risk for other malignant diseases, including childhood cancer (9).
Has radiofrequency radiation from cell phone use been associated with cancer risk in children?
There are theoretical considerations as to why the potential health effects of cell phone use should be investigated separately in children. Their nervous systems are still developing and, therefore, more vulnerable to factors that may cause cancer. Their heads are smaller than those of adults and consequently have a greater proportional exposure to radiation emitted by cell phones. And, children have the potential of accumulating more years of cell phone exposure than adults.
Thus far, the data from studies of children with cancer do not suggest that children are at increased risk of developing cancer from cell phone use. The first published analysis came from a large case–control study called CEFALO, which was conducted in Europe. The study included 352 children who were diagnosed with brain tumors between 2004 and 2008 at the ages of 7 to 19 years. They were matched by age, sex, and geographical region with 646 young people randomly selected from population registries. Researchers did not find an association between cell phone use and brain tumor risk by amount of use or by the location of the tumor (29).
The largest case–control study among children, a 14-country study known as MOBI-Kids, included 899 young people ages 10 to 24 years who were diagnosed with brain tumors between 2010 and 2015. They were matched by sex, age, and region with 1,910 young people who were undergoing surgery for appendicitis. Researchers found no evidence of an association between wireless phone use and brain tumors in young people (30).
Which US federal agencies have a role in evaluating the effects of or regulating cell phones?
The National Institutes of Health (NIH), including the National Cancer Institute (NCI), conducts research on cell phone use and the risks of cancer and other diseases.
FDA and FCC share regulatory responsibilities for cell phones. FDA is responsible for testing and evaluating electronic product radiation and providing information for the public about the radiofrequency energy emitted by cell phones. FCC sets limits on the emissions of radiofrequency energy by cell phones and similar wireless products.
Where can I find more information about radiofrequency radiation from my cell phone?
The dose of the energy that people absorb from any source of radiation is estimated using a measure called the specific absorption rate (SAR), which is expressed in watts per kilogram of body weight (52). The SAR decreases very quickly as the distance to the exposure source increases. For cell phone users who hold their phones next to their head during voice calls, the highest exposure is to the brain, acoustic nerve, salivary gland, and thyroid.
The FCC provides information about the SAR of cell phones produced and marketed within the previous 1 to 2 years. Consumers can access this information using the phone’s FCC ID number, which is usually located on the case of the phone, and the FCC’s ID search form. SARs for older phones can be found by checking the phone settings or by contacting the manufacturer.
What can cell phone users do to reduce their exposure to radiofrequency radiation?
Reduce the amount of time spent using your cell phone.
Use speaker mode, head phones, or ear buds to place more distance between your head and the cell phone.
Avoid making calls when the signal is weak as this causes cell phones to boost RF transmission power.
Consider texting rather than talking, but don’t text while you are driving.
Use of wired or wireless headsets reduces the amount of radiofrequency radiation exposure to the head because the phone is not placed against the head (53). Exposures decline dramatically when cell phones are used hands-free. For example, wireless (Bluetooth) devices (such as headphones and earbuds) use short-range signals that typically transmit radiofrequency waves at power levels 10–400 times lower than cell phones (54).
The cancer prevention summaries in PDQ refer to cancer prevention, defined as a reduction in the incidence of cancer. The PDQ includes summaries generally classified by histological type of cancer, especially when there are known risk factors for the specific types of cancer. This summary addresses a specific risk factor, tobacco use, which is associated with a large number of different cancers (and other chronic diseases) and unequivocally contains human carcinogens.[1] The focus of this summary is on clinical interventions by health professionals that decrease the use of tobacco.
Effects of Smoking Cessation
Based on solid evidence, cigarette smoking causes cancers of the lung, oral cavity and pharynx, larynx, esophagus, bladder, kidney, pancreas, stomach, uterine cervix, colon and rectum, liver, and acute myeloid leukemia.[2] Smoking avoidance and smoking cessation result in decreased incidence and mortality from cancer.[3]
Description of the Evidence
Study Design: Evidence obtained from a randomized controlled trial (RCT).
Internal Validity: Good.
Consistency: Good.
Magnitude of Effects on Health Outcomes: The relative risk (RR) of several cancers is much greater in cigarette smokers compared with nonsmokers (depending on the anatomical site of the cancer and the intensity and duration of smoking, the RR can range from twofold to tenfold or greater in smoking populations). A reduction of 15% is seen in the RR of all-cause mortality in heavy smokers subjected to intensive clinical cessation interventions.
External Validity: Good.
Physician or Nurse Advice and Smoking Cessation
Based on solid evidence, brief advice from a physician or nurse to stop smoking improves smoking cessation rates.
Description of the Evidence
Study Design: Evidence obtained from RCTs.
Internal Validity: Good.
Consistency: Good.
Magnitude of Effects on Health Outcomes: Physician advice improves cessation rates (RR, 1.66; 95% confidence interval [CI], 1.42–1.94).[4] Nurse advice improves cessation rates (RR, 1.29; 95% CI, 1.21–1.38).[5]
External Validity: Good.
Counseling and Smoking Cessation
Based on solid evidence, counseling by a health professional improves smoking cessation rates.
Description of the Evidence
Study Design: Evidence obtained from RCTs.
Internal Validity: Good.
Consistency: Good.
Magnitude of Effects on Health Outcomes: Counseling improves cessation rates (odds ratio [OR], 1.44; 95% credibility interval, 1.22–1.70).[6]
External Validity: Good.
Pharmacological Treatment and Smoking Cessation
Based on solid evidence, drug treatments, including nicotine replacement therapies (NRTs) (gum, patch, spray, lozenge, and inhaler), selected antidepressant therapies (e.g., bupropion hydrochloride [HCI]), and nicotinic receptor agonist therapy (varenicline), result in better smoking cessation rates than placebo.
Description of the Evidence
Study Design: Evidence obtained from RCTs.
Internal Validity: Good.
Consistency: Good.
Magnitude of Effects on Health Outcomes: NRTs, alone or in combination, improve cessation rates over placebo after 6 months (RR, 1.55; 95% CI, 1.49–1.61).[7] Treatment with bupropion HCI improves cessation rates over placebo after 6 months (OR, 1.94; 95% CI, 1.72–2.19; RR, 1.60; 95% CI, 1.49–1.72).[8] Varenicline therapy treatment improves cessation rates over placebo after 6 months (RR, 2.32; 95% CI, 2.15–2.51).[9]
External Validity: Good.
Pharmacological Treatment Combined With Counseling and Smoking Cessation
Based on solid evidence, drug treatments combined with counseling by a health professional result in better smoking cessation rates than drug treatments with minimal or no counseling support.
Description of the Evidence
Study Design: Evidence obtained from RCTs.
Internal Validity: Good.
Consistency: Good.
Magnitude of Effects on Health Outcomes: Drug treatments combined with counseling (behavioral support) improve cessation rates over drug treatments combined with minimal or no counseling support after 6 months (RR, 1.83; 95% CI, 1.68–1.98).[5,10]
External Validity: Good.
References
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans: Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum 83: 1-1438, 2004. [PUBMED Abstract]
U.S. Department of Health and Human Services: The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. U.S. Department of Health and Human Services, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. Also available online. Last accessed December 30, 2024.
U.S. Department of Health and Human Services: Smoking Cessation: A Report of the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2020. Also available online. Last accessed February 20, 2025.
Stead LF, Buitrago D, Preciado N, et al.: Physician advice for smoking cessation. Cochrane Database Syst Rev 2013 (5): CD000165, 2013. [PUBMED Abstract]
Hartmann-Boyce J, Livingstone-Banks J, Ordóñez-Mena JM, et al.: Behavioural interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev 1: CD013229, 2021. [PUBMED Abstract]
Hartmann-Boyce J, Chepkin SC, Ye W, et al.: Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev 5 (5): CD000146, 2018. [PUBMED Abstract]
Hajizadeh A, Howes S, Theodoulou A, et al.: Antidepressants for smoking cessation. Cochrane Database Syst Rev 5 (5): CD000031, 2023. [PUBMED Abstract]
Livingstone-Banks J, Fanshawe TR, Thomas KH, et al.: Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev 5 (5): CD006103, 2023. [PUBMED Abstract]
Stead LF, Koilpillai P, Fanshawe TR, et al.: Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database Syst Rev 3 (3): CD008286, 2016. [PUBMED Abstract]
Evidence of Benefit
Background
In the United States, smoking-related illnesses accounted for an estimated 480,000 deaths each year.[1,2] On average, these deaths occur 12 years earlier than would be expected, so the aggregate annual loss exceeds 5 million life-years.[3] These deaths are primarily due to smoking’s role as a major cause of cancer, cardiovascular disease, and chronic lung disease. The known adverse health effects also include other respiratory diseases and symptoms, nuclear cataract, hip fractures, reduced female fertility, diabetes, erectile dysfunction, rheumatoid arthritis, and diminished health status. Maternal smoking during pregnancy is associated with fetal growth restriction, low birth weight, and complications of pregnancy.[2] About 50% of cancer deaths in the United States are attributable to modifiable behavioral risk factors, one of which is smoking.[4]
Tobacco products are the leading avoidable cause of cancer, causing more than 155,000 deaths among smokers in the United States annually due to various cancers.[5] Most cancers of the lung, trachea, bronchus, larynx, pharynx, oral cavity, nasal cavity, and esophagus are attributable to tobacco products, particularly cigarettes. Smoking is also causally associated with cancers of the pancreas, kidney, bladder, stomach, colon, rectum, liver, and cervix, and with myeloid leukemia.[2,6]
Smoking also has substantial effects on the health of nonsmokers. Environmental or secondhand tobacco smoke is implicated in causing lung cancer, coronary heart disease, stroke, nasal irritation, and reproductive effects in women (low birth weight in newborns of these women).[2] Among children, secondhand smoke exposure is causally associated with sudden infant death syndrome, lower respiratory tract illnesses, otitis media, middle ear effusion, exacerbated asthma, and respiratory effects such as cough, wheeze, and dyspnea.[2]
Environmental tobacco smoke has the same components as inhaled mainstream smoke, although in lower absolute concentrations, between 1% and 10%, depending on the constituent. Carcinogenic compounds in tobacco smoke include the polycyclic aromatic hydrocarbons (PAHs), including the carcinogen benzo[a]pyrene (BaP) and the nicotine-derived tobacco-specific nitrosamine, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK).[7] Elevated biomarkers of tobacco exposure, including urinary cotinine, tobacco-related carcinogen metabolites, and carcinogen-protein adducts, are seen in passive or secondhand smokers.[8–11]
In 2021, 13.1% of adult men and 10.1% of adult women in the United States were current smokers, and 24.1% of adult men and 13.6% of adult women reported the use of any tobacco product.[12] Cigarette smoking is particularly common among American Indian and Alaska Native individuals. The prevalence of smoking also varies inversely with education, and was highest among adults who had earned a General Educational Development diploma (30.1%) and generally decreased with increasing years of education.[12] From 2011 to 2014, significant declines occurred in the use of cigarettes among middle school (4.3% to 2.5%) and high school (15.8% to 9.2%) students.[13] Cigarette smoking prevalence among male and female high school students increased substantially during the 1990s in all ethnic groups, with rates between 20% and 30%. However, by 2023, the cigarette smoking rate in high school students declined to 2%.[4,14,15] (Also available online.)
The effect of tobacco use on population-level health outcomes is illustrated by the example of lung cancer mortality trends. Smoking by women increased between 1940 and the early 1960s, resulting in a greater than 600% increase in female lung cancer mortality since 1950. Lung cancer is now the leading cause of cancer death in women.[14,16] In the last 30 years, prevalence of current cigarette use has generally decreased, though far more rapidly in men. Lung cancer mortality in men peaked in the 1980s, and has been declining since then; this decrease has occurred predominantly in squamous cell and small cell carcinomas, the histological types most strongly associated with smoking.[14] Variations in lung cancer mortality rates by state also more or less parallel long-standing state-specific differences in tobacco use. Among men, the average annual age-adjusted lung cancer death rates from 2018 to 2022 were highest in Mississippi (63.1 per 100,000),[4] where 22% of men in Mississippi were current smokers in 2021, and lowest in Utah (18.0 per 100,000), where only 8% of men smoked. Among women, lung cancer death rates were highest in Kentucky (43.2 per 100,000), where 21% of women were current smokers, and lowest in Utah (13.5 per 100,000), where only 6% of women smoked.[4,14,17,18]
Tobacco Use Interventions
Many health risks related to tobacco smoking can be reduced by smoking cessation. People who quit smoking before age 50 years have up to half the risk of dying within 15 years compared with people who continue to smoke. In addition, the risk of dying is reduced substantially even among people who stop smoking after age 70 years.[19] After 10 years of abstinence from smoking, the risk of lung cancer is 30% to 50% lower than that of continuing smokers, and the risk of oral and esophageal cancer is halved within 5 years of cessation.[19] People who quit smoking also lower their risk of acute myeloid leukemia and cancers of the cervix, stomach, larynx, pancreas, colon and rectum, liver, kidney, and bladder.[16,19–21]
In a randomized trial of heavy smokers, the long-term follow-up results demonstrated that compared with the nonintervention group (n = 1,964), those randomly assigned to a smoking cessation intervention (n = 3,923) experienced a 15% reduction in all-cause mortality rates (8.83 vs. 10.38 per 1,000 person-years; P = .03).[22] The smoking cessation intervention consisted of a strong physician message plus 12 group sessions and nicotine gum administered during a 10-week period. Decreases in the risk of lung cancer and other cancers, coronary heart disease, cardiovascular disease, and respiratory disease contributed to the benefit in the patients randomly assigned to the smoking cessation intervention.
The most recent Surgeon General’s Report on the benefits of smoking cessation also outlined the accumulated evidence about health benefits associated with tobacco cessation for chronic cardiovascular diseases, respiratory diseases, and reproductive outcomes. Smoking cessation reduces the risk of morbidity and mortality from cardiovascular disease and stroke, reduces the risk of an abdominal aortic aneurysm and coronary heart disease, reduces the levels of inflammatory and hypercoagulability markers, leads to a reduction in the development of atherosclerosis, and reduces the burden of cardiovascular disease. Smoking cessation also reduces the risk of developing chronic obstructive pulmonary disease (COPD) and is the only recognized intervention to attenuate the loss of lung function among people with COPD. Smoking cessation benefits the health of pregnant women and their child. Benefits include a reduced risk of birthing a small-for-gestational-age infant and a reduced effect of smoking on fetal growth.[21]
Several approaches at the policy, legislative, and regulatory levels have been attempted to effect widespread reduction in or prevention of commencement of tobacco use. Various efforts at the community, state, and national level have been credited with reducing the prevalence of smoking over time. These efforts include reducing minors’ access to tobacco products, disseminating effective school-based prevention curricula together with media strategies, raising the cost of tobacco products, using tobacco excise taxes to fund community-level interventions such as mass media, providing proven quitting strategies through health care organizations, and adopting smoke-free laws and policies.[23,24]
As discussed in more detail below, clinical interventions targeted at individuals have shown promising results. A meta-analysis of randomized controlled trials (RCTs) showed that 6-month cessation rates were significantly improved with the use of nicotine replacement therapy (NRT) products compared with placebo or no intervention (relative risk [RR], 1.55; 95% confidence interval [CI], 1.49–1.61).[25] The benefits of using NRT products have been consistently observed regardless of whether the product used was the patch, gum, nasal spray, inhaler, or lozenge.[25] Smoking cessation counseling alone is also effective.[26] Even a brief intervention by a health care professional significantly increases the smoking cessation rate.[27]
Tobacco cessation guidelines
In 1996, the Agency for Health Care Policy and Research (AHCPR), now the Agency for Healthcare Research and Quality, released a landmark set of clinical smoking-cessation guidelines for helping nicotine-dependent patients and health care providers. Now sponsored by the U.S. Public Health Service, the updated 2008 guidelines, “Treating Tobacco Use and Dependence” are available online.[28] The broad elements of these guidelines are:
Clinicians should document the tobacco-use status of every patient.
Clinicians should assess the readiness to quit of patients who use tobacco and assist those who wish to quit in setting a quit date.
Patients using tobacco should be provided with at least one of the effective brief cessation interventions that are available.
In general, more intense interventions are more effective than less intense interventions in producing long-term tobacco abstinence, reflecting the dose-response relationship between the intervention and its outcome.
One or more of the three treatment elements identified as being particularly effective should be included in smoking-cessation treatment:
Social support from clinicians in the form of encouragement and assistance.
Pharmacotherapy, such as NRT products (e.g., patches, gum).
To be effective, health care systems must make institutional changes resulting in systematic identification of tobacco users and intervention with these patients at every visit.
For individual interventions, these guidelines [28] suggested a model based on outcomes from six major clinical trials of physician-delivered smoking intervention conducted in the late 1980s:[29] the ASK, ADVISE, ASSESS, ASSIST, and ARRANGE model. The physician provides a brief intervention that entails asking about smoking status at every visit, advising abstinence, assisting by setting a quit date, providing self-help materials and recommending use of NRT, and arranging for a follow-up visit. See below for brief intervention outlines. The recommendations also strongly supported the value of referral to more intensive counseling.
Ask, Advise, Assess, Assist, Arrange: Key Elements
Ask
Screen for smoking status at every visit or admission.
Advise
Minimal Advice: “As your physician, I must advise you that smoking is bad for your health, and it would be important for you to stop.”
Augmented Advice: “Because of your (__________) condition, it is particularly important for you to stop. If you stop now, (briefly educate patient about basic health benefits from quitting).”
Assess
Minimal Assessment: Ask every tobacco user if he/she is willing to make a quit attempt at this time.
Augmented Assessment: Assess characteristics of smoking history and patterns.
Amount smoked.
Quit history.
Assist/Counsel
Minimal Assistance: Provide self-help materials; assess interest in quitting; and assess interest in and appropriateness of pharmacological aids.
Augmented Assistance: Provide brief 5- to 7-minute patient-centered counseling.
Arrange Follow-Up Support
Minimal Follow-Up Support: Arrange for single follow-up contact by visit or by telephone in about 2 weeks; provide referral to a smoking counselor or group.
Extended Follow-Up Support: Establish “quit smoking” contract with quit date. Arrange three or more follow-up contacts by visit or by telephone.
In 2021, the U.S. Preventive Services Task Force (USPSTF) published an updated recommendation statement based on a systematic review that included 67 reviews addressing behavioral and pharmacological interventions for smoking cessation among the general population of adults that are largely in line with previous guidelines. In addition to asking all patients about tobacco use and advising them to abstain, the USPSTF recommended that clinicians provide evidence-based behavioral interventions and one or more of the seven pharmacotherapies approved by the U.S. Food and Drug Administration (FDA) for adults who use tobacco.[30]
The USPSTF recommendation was based on robust evidence that a variety of behavioral interventions (such as brief advice or support, counseling in various modalities, internet-based interventions, and financial incentives); all forms of NRT, bupropion hydrochloride (HCI), and varenicline; and the combination of behavioral and pharmacological interventions were significantly associated with increased abstinence rates of more than 6 months when compared with usual care or a minimal intervention. The USPSTF concluded with high certainty (the evidence was assigned an A grade) that the net benefit of evidence-based behavioral interventions and FDA-approved pharmacotherapy for tobacco cessation, alone or combined, is significant in adults who smoke.[31] Of note, the guidelines for pregnant women are similar, in that they recommend that clinicians ask all patients about tobacco use, advise them to abstain, and provide evidence-based behavioral interventions. However, the guidelines indicated that the evidence is insufficient to assess the benefits and harms of pharmacotherapy. The 2020 Surgeon General’s Report on smoking cessation, based on an independent evidence review, similarly concluded that evidence-based behavioral and pharmacological interventions for smoking cessation are safe and effective treatments.[21] The World Health Organization, the American College of Cardiology, the American Thoracic Society, and other similar organizations have issued guidance that is consistent with the USPSTF’s recommendations.[32–34]
Promoting smoking cessation among cancer patients and survivors is also essential because the deleterious health effects of cigarette smoking may impact prognosis in both the short term and long term. In an RCT of a peer-delivered smoking cessation intervention among childhood cancer survivors, a significantly higher 12-month quit rate was observed in the intervention group (15% vs. 9%; P < .01).[35] Continued smoking after a cancer diagnosis increases all-cause and cancer-specific mortality. Continued smoking is also associated with a higher risk of a recurrence or a second primary cancer, a poorer response to treatment, and increased treatment-related side effects.[2] Consistent with the tobacco cessation guidelines noted previously in the general adult population, the National Comprehensive Cancer Network Clinical Practice Guidelines for Smoking Cessation recommend that all cancer patients be assessed for tobacco use at regular intervals. They also recommend that patient treatment plans include evidence-based behavioral/motivational counseling, pharmacotherapy, and follow-up (with additional treatment if needed).[36]
Behavioral Interventions to Assist in Tobacco Cessation
A wide array of behavioral interventions for smoking cessation that vary in content, mode of delivery, intensity, and duration have demonstrated various degrees of efficacy. Behavioral interventions may include advice to quit, cognitive, behavioral, and motivational counseling, internet or mobile applications, self-help materials, and financial incentives.[26,31]
The following sections summarize the evidence for the effect of these interventions on abstinence rates.
Physician or nurse advice and smoking cessation
The importance of health care providers in the identification of individuals who use tobacco and the provision of advice to quit has been consistently highlighted in evidence-based smoking cessation guidelines.[30] In an analysis pooling data from 17 trials, brief physician advice versus no advice (or usual care) was associated with a significant increase in abstinence rates at 6 months (RR, 1.66; 95% CI, 1.42–1.94). Although there was no statistical difference in abstinence rates between minimal advice and more intensive subgroups, the estimated effect was higher for the more intensive interventions (RR, 1.84; 95% CI, 1.60–2.13).[27] Similarly, a separate review reported moderate-quality evidence suggesting that compared with usual care, behavioral support/advice delivered by nurses resulted in increased abstinence rates (RR, 1.29; 95% CI, 1.21–1.38).[37] The analysis found no evidence that high-intensity interventions or interventions with additional follow-up increased abstinence rates. Even though the absolute effects of brief advice from a physician or nurse may be smaller than other interventions for smoking cessation, the impact on public health can still be substantial if a large volume of these clinicians offer advice to quit to people who use tobacco.
Financial incentive programs for smoking cessation
Financial incentive programs can offer additional support for smoking cessation efforts and may involve incentives for program engagement, compliance with program processes or milestones, and/or tobacco or smoking abstinence outcomes. Results from a randomized trial suggest that the efficacy of such programs may be influenced greatly by the way rewards are disbursed.[38,39]
The trial randomly assigned 2,538 participants to either one of four incentive programs or usual care. The four programs were combinations of scope (two programs targeted individuals, and two targeted groups of six participants) and incentive structure (one of the individual-focused programs and one of the group-focused programs provided rewards of approximately $800 to participants who achieved cessation at 6 months; the others required an initial refundable deposit of $150, supplemented with $650 in reward payments for successful cessation). The rationale for the four intervention arms was based on behavioral observations that 1) people are more loss averse than gain seeking and 2) collaboration/competition with others can bolster intervention efficacy.[38]
Two main dimensions of the intervention effects were explored:
Acceptance of the intervention.
Efficacy of the intervention.
Both intent-to-treat and per-protocol analyses were performed, with an in-depth sensitivity analysis for potential biases accompanying the latter. In the intent-to-treat analyses (which evaluated the overall efficacy of the interventions), all of the financial incentive arms demonstrated significantly higher 6-month abstinence rates than the usual care arm (9.4%–16%, compared with 6% for usual care). The 6-month abstinence rates were similar between the group-focused and individual-focused arms (13.7% and 12.1%, respectively; P = .29), but the reward-based programs were associated with higher abstinence rates than were the deposit-based ones (15.7% vs. 10.2%; P < .001).[38]
However, per-protocol analyses that accounted for the dramatically lower acceptance rate for the deposit-based interventions than for the reward-based interventions (14% vs. 90%) estimated that 6-month abstinence rates could be 13.2 percentage points (95% CI, 3.1–22.8) higher in the deposit-based programs than in the reward-based programs among the estimated 13.7% of participants who would participate in either type of program. That is, deposit-based interventions may be more efficacious than reward-based interventions, but it is harder to get people to commit to them.[38]
A systematic review of 33 trials included more than 21,000 participants. The pooled RR for quitting with incentives at 6 months was 1.49 (95% CI, 1.28–1.73; 31 RCTs; adjusted N = 20,097; I2 = 33%), compared with controls, indicating that there is high certainty evidence that the use of incentives improves abstinence rates.[40] After excluding six studies that offered incentives at the 6-month follow-up time point, the results remained consistent (RR, 1.40; 95% CI, 1.16–1.69; 25 RCTs; adjusted N = 17,058; I2 = 36%), suggesting that the effect of those incentives persisted after the incentives ended. The authors noted that the financial value of the incentives varied across studies (including some that involved redeemable self-deposits), but there were no clear effects related to incentive value. They also examined the effect of incentives on smoking cessation in people who were pregnant and reported moderate-quality evidence (limited by the risk of bias) that incentive programs initiated at the end of pregnancy or postpartum led to increased abstinence rates at 24 weeks postpartum (RR, 2.38; 95% CI, 1.54–3.69; N = 2,273; I2 = 41%).
A subsequent component network meta-analysis assessed the effect of behavioral interventions on abstinence across 33 systematic reviews, which included 312 RCTs and more than 250,000 participants. Results indicated that the only interventions that demonstrated benefit were the provision of financial incentives and the provision of counseling.[26]
Pharmacological Interventions to Assist in Tobacco Cessation
Pharmacological agents have been used successfully to aid in the cessation of smoking in the general population.[41] Since the original AHCPR guidelines [42] were published in 1996, various nicotine replacement products have been approved for over-the-counter sale, and additional evidence of the effectiveness of therapies for smoking cessation has been published.[43–46] Pharmacotherapy of smoking cessation, including NRTs (gum, patch, spray, lozenge, and inhaler) and non-nicotine medications (e.g., bupropion HCI and varenicline), results in statistically significant increases in smoking cessation rates over those of a placebo.[47]
A growing number of smoking cessation pharmacotherapies have demonstrated efficacy in significantly increasing rates of smoking cessation. The choice of therapy should be individualized based on several factors, including past experience, patient and/or physician preference, and potential agent side effects. As more is learned about specific genetic variants that influence a smoker’s response to smoking cessation pharmacotherapies—such as polymorphisms in genes encoding enzymes involved in nicotine metabolism—this information could eventually be integrated into smoking cessation treatment planning.[48] Presently, the evidence is not yet sufficient to be integrated into clinical practice.
The following sections summarize available pharmacological interventions to assist in tobacco cessation. More comprehensive information is available from product package inserts.
Nicotine replacement therapy (NRT)
NRT products, including nicotine patches, gums, lozenges, inhalers, and nasal sprays, are designed to relieve nicotine withdrawal symptoms. There are several precautions before initiating therapy, but these precautions do not constitute absolute contraindications. Special considerations are necessary in some patient groups (e.g., those with medical conditions such as arrhythmias, uncontrolled hypertension, esophagitis, peptic ulcer disease, insulin-treated diabetes, or asthma; pregnant or breast-feeding women; and adolescent smokers).[49] Commonly reported side effects differ by product type. These side effects include erythema, pruritus, local irritation, stomatitis, sore throat, jaw soreness, gastrointestinal complaints (including nausea and vomiting), heart palpitations, insomnia, hiccups, and coughing.[50]
Based on a synthesis of the results of 133 randomized trials, researchers found that NRTs, alone or in combination, improved cessation rates over placebos after 6 months (RR, 1.55; 95% CI, 1.49–1.61). In addition, similar benefits of NRT product use were observed regardless of the product type (patch, gum, nasal spray, inhaler, or lozenge).[25] When compared directly, the use of a single fast-acting NRT (such as nicotine lozenges or gum) or the nicotine patch results in similar 6-month cessation rates (RR, 0.90; 95% CI, 0.77–1.05).[51] The results of an analysis that included 16 randomized trials concluded that combining a fast-acting NRT with the nicotine patch resulted in higher 6-month cessation rates compared with the nicotine patch alone (RR, 1.27; 95% CI, 1.17–1.37).[51] However, not all trials supported this conclusion.[52]
Current guidelines generally recommend 8 to 12 weeks of transdermal nicotine therapy, starting on the quit day. Findings from two randomized placebo-controlled trials of transdermal therapy differed in their findings as to whether extended therapy (22–24 weeks vs. 8 weeks) improves quit rates.[53,54]
Non-nicotine products
Bupropion hydrochloride (HCI)
Also used as an antidepressant, bupropion HCl is a non-nicotine aid to smoking cessation. It is a relatively weak inhibitor of the neuronal uptake of norepinephrine, serotonin, and dopamine, and does not inhibit monoamine oxidase. The exact mechanism by which bupropion HCl enhances the ability of patients to abstain from smoking is unknown. However, it is presumed that this action is mediated by noradrenergic or dopaminergic mechanisms. Based on the results of 50 randomized trials that compared bupropion HCI with placebo, after 6 months of follow-up, bupropion was associated with a statistically significant increase in the likelihood of quitting smoking (RR, 1.60; 95% CI, 1.49–1.72).[55] There was insufficient evidence to support the idea that combining bupropion HCI with NRT increases smoking cessation rates over those of NRT alone (RR, 1.17; 95% CI, 0.95–1.44). However, results (based on three trials) indicated that the combination of bupropion HCI and varenicline may result in higher 6-month cessation rates compared with varenicline alone (RR, 1.21; 95% CI, 0.95–1.55). Although there was no difference in the efficacy of bupropion HCI compared with single-form NRT (RR, 1.03; 95% CI, 0.93–1.13), there was evidence that the use of bupropion HCI resulted in lower cessation rates than varenicline (RR, 0.73; 95% CI, 0.67–0.80) and combination NRT (RR, 0.74; 95% CI, 0.55–0.98), and higher cessation rates than the antidepressant, nortriptyline (RR, 1.30; 95% CI, 0.93–1.82).[55] Commonly reported side effects of bupropion HCI include insomnia, dry mouth, dizziness, and rhinitis. A higher incidence of seizures was also reported in patients being treated for bulimia/anorexia.
Varenicline
Varenicline is a selective partial agonist at the alpha-4-beta-2 nicotinic acetylcholine receptor, which mediates nicotine dependence through dopamine release. Varenicline prevents nicotine from binding to the receptor and reduces both the rewarding effects of smoking and withdrawal symptoms. The most commonly reported side effects of varenicline include nausea, abnormal dreams, and insomnia. In two of the initial RCTs for smoking cessation, varenicline was titrated to a dose of 1 mg twice a day and compared with bupropion HCI sustained-release (SR) 150 mg twice a day and a placebo group.[56,57] Treatment lasted for 12 weeks, with an additional 40 weeks of posttreatment follow-up. In both studies, varenicline was more efficacious than bupropion HCI and placebo for continuous abstinence from smoking at 9 to 12 weeks and at 9 to 24 weeks of follow-up. For 9 to 52 weeks of follow-up, varenicline was more efficacious than placebo in both studies.[56,57] At 52 weeks of follow-up, the 7-day point prevalence of smoking abstinence was 46% higher in the varenicline group than in the bupropion HCI SR group (odds ratio [OR], 1.46; 95% CI, 1.04–2.06).[56] The other study also showed a 46% higher continuous abstinence in the varenicline group (OR, 1.46; 95% CI, 0.99–2.17).[57] Approximately 30% of the participants who were randomly assigned to receive varenicline reported nausea, more than double the rate in the bupropion HCI groups, and triple the rate seen in the placebo groups.
In a randomized trial comparing varenicline with transdermal nicotine, continuous abstinence was greater in the varenicline group than in the transdermal nicotine group at the end of treatment (56% vs. 43%; P < .001) and during posttreatment follow-up (26% vs. 20%; P = .06).[58] The prevalence of nausea in the varenicline group (37%) was more than triple that in the transdermal nicotine group (10%). However, this result was not confirmed in a subsequent randomized trial that compared varenicline with the nicotine patch.[52] There was little difference in 7-day point-prevalence abstinence after 26 weeks (24% vs. 23%; P = .82) or 52 weeks (19% vs. 21%; P = .61) between those randomly assigned to the varenicline intervention and those assigned to the nicotine-patch intervention.
The results of a synthesis of 41 randomized trials indicated that varenicline results in increased 6-month cessation rates when compared with placebo (RR, 2.32; 95% CI, 2.15–2.51), bupropion HCI (RR, 1.36; 95% CI, 1.25–1.49), and single-form NRT (RR, 1.25; 95% CI, 1.14–1.37), but provided no clear evidence that varenicline was superior to dual NRT (RR, 1.02; 95% CI, 0.87–1.20 ).[59]
After a period of postmarketing surveillance, on July 1, 2009, the FDA required additions to the Boxed Warnings for both bupropion HCI and varenicline to describe the risk of serious neuropsychiatric symptoms associated with these products. Symptoms include: “changes in behavior, hostility, agitation, depressed mood, suicidal thoughts and behavior, and attempted suicide.”[60] The FDA further advised that the important health benefits of quitting smoking “should be weighed against the small, but real, risk of serious adverse events with the use of varenicline or bupropion.”[60] Subsequently, the FDA required the manufacturers of bupropion HCI and varenicline to conduct a clinical trial to evaluate the neuropsychiatric safety of these medications in patients with and without a history of psychiatric disorders (EAGLES trial). This randomized, double-blind, triple-dummy, placebo-controlled and active-controlled (nicotine patch) trial of varenicline and bupropion HCI included over 8,000 cigarette smokers (one-half of which had current or a history of psychiatric disorders) from 140 sites in 16 countries. In the nonpsychiatric cohort, the varenicline-placebo and bupropion-placebo risk differences (RDs) for moderate and severe neuropsychiatric adverse events were -1.28 (95% CI, -2.40 to -0.15) and -0.08 (95% CI, -1.37 to 1.21), respectively. In the psychiatric cohort, the varenicline-placebo and bupropion-placebo RDs were 1.59 (95% CI, -0.42 to 3.59) and 1.78 (95% CI, -0.24 to 3.81), respectively. The most frequent adverse events by treatment group were nausea (varenicline, 25%), insomnia (bupropion HCI, 12%), abnormal dreams (nicotine patch, 12%), and headache (placebo, 10%). The results of the trial did not show a significant increase in rates of moderate-to-severe neuropsychiatric adverse events with either varenicline or bupropion HCI in those with or without psychiatric disorders [61] and were supported by other studies analyzing data from multiple cessation trials.[62–64] These results prompted the FDA to remove the Boxed Warnings for both bupropion HCI and varenicline in 2016, noting that although the risk of mental health side effects is still present, particularly for individuals with some mental illnesses, the “results of the trial confirm that the benefits of stopping smoking outweigh the risks of these medicines.”[65]
A meta-analysis of double-blind, placebo-controlled, randomized trials of varenicline administered for at least 1 week (N = 14 trials) indicated that varenicline was associated with an increased risk of serious adverse cardiovascular events (RR, 1.72; 95% CI, 1.09–2.71).[66] This finding is particularly noteworthy because almost all of the randomized trials included in the meta-analysis had the following in common: they excluded patients with cardiovascular disease (CVD) at baseline; the usual average age of the patient populations (early 40s) was young for CVD; varenicline was usually given for 12 weeks or less; and varenicline is efficacious for smoking cessation, which would act to decrease CVD risk. A subsequent extension study to the EAGLES trial,[61] described above, evaluated the time to development of major adverse cardiovascular events (MACE: cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) across treatment groups (placebo, NRT, bupropion HCI, and varenicline) as a primary outcome. The extension study reported no significant difference in time to onset of MACE for varenicline or bupropion HCI, compared with placebo (varenicline: hazard ratio [HR], 0.29; 95% CI, 0.05–1.68 and bupropion HCI: HR, 0.50; 95% CI, 0.10–2.50) and no significant differences in the incidence of cardiovascular events during treatment by treatment group.[67] An analysis of 18 studies reported that while more people taking varenicline experienced cardiac serious adverse events compared with placebo or no medication (RR, 1.20; 95% CI, 0.79–1.8), conclusions about harm are limited because of imprecision in the estimates.[59]
Fluoxetine
Although Zyban (bupropion HCl) is the only antidepressant approved by the FDA for smoking cessation, Prozac (fluoxetine HCl) has been shown to be effective in some studies.[68] Pooled results from two RCTs indicated no significant difference in cessation rates after 6 months between selective serotonin reuptake inhibitor users (including fluoxetine HCI) and the control arms in two studies (RR, 0.93; 95% CI, 0.71–1.22). There was also no significant increase in cessation rates when fluoxetine HCI was added to NRT in three studies (RR, 0.70; 95% CI, 0.64–1.82).[69] The most commonly reported side effects of fluoxetine HCI include insomnia, dizziness, anorexia, sexual dysfunction, and confusion.
Cytisine
Cytisine is a naturally occurring compound isolated more than 50 years ago from the plant Cytisus laburnum, a partial nicotinic acetylcholine receptor agonist.[70] It has a long history of use for smoking cessation in Bulgaria and other eastern European nations, including clinical trials published in the 1970s. As this older evidence has been uncovered, it has led to more recent trials in western nations. A systematic review and meta-analysis showed clear benefit for cytisine compared with placebo.[70] For all trials combined (n = 9 trials; 2,141 cytisine participants, 1,879 placebo participants), the pooled RR for abstinence from smoking at the longest follow-up for cytisine was 1.59 (95% CI, 1.43–1.75), compared with placebo. When the analyses were limited to two high-quality trials published since 2008, the pooled RR for smoking abstinence was 3.29 (95% CI, 1.84–5.90).[70] There was no evidence of serious adverse events, but gastrointestinal symptoms were more common in the cytisine (12%) group than in the placebo (7%) group.[70]
A randomized trial in New Zealand compared cytisine (n = 655) with NRT (n = 655).[71] Compared with the NRT group, the cytisine group had higher continued abstinence at 1 month (40% vs. 31%; RD, 9%; 95% CI, 4%–15%), 2 months (31% vs. 22%; RD, 9%; 95% CI, 4%–14%), and 6 months (22% vs. 15%; RD, 7%; 95% CI, 2%–11%).[71] There were no differences between treatment groups, but nausea and vomiting (28 events vs. 2 events) and sleep disorders (28 events vs. 2 events) were more common in the cytisine group, compared with the NRT group.[71] This trial is noteworthy because of the following results:
It considerably strengthened an already substantial body of evidence indicating that cytisine is an efficacious smoking cessation pharmacotherapy.
It showed that cytisine is more efficacious than NRT products that are known to be effective.
Based on a synthesis of the results of four randomized trials (4,623 participants), researchers found that cytisine improved cessation rates over placebo after 6 months (RR, 1.30; 95% CI, 1.15–1.61), with no evidence of an increase in serious adverse events (RR, 1.04; 95% CI, 0.78–1.37). Pooled results from two studies indicated no significant difference in cessation rates after 6 months between cytisine and varenicline (RR, 1.00; 95% CI, 0.79–1.26).[59] In a subsequent randomized noninferiority trial, cytisine was associated with lower cessation rates (OR, 0.63; 95% CI, 0.39–0.98) and fewer total adverse events (incidence rate ratio, 0.59; 95% CI, 0.43–0.81) than varenicline.[72] The most commonly reported side effects of cytisine include nausea, vomiting, and sleep disturbance.
Other agents
Nortriptyline has been suggested as a possibly useful second-line pharmacotherapy but is not approved for smoking cessation by the FDA. Nortriptyline is an antidepressant that does not contain nicotine. A meta-analysis of five RCTs found that smokers who received nortriptyline were 2.4 times more likely (95% CI, 1.7–3.6) than smokers who received a placebo to remain abstinent from smoking after 6 months.[73] Pooled results from six studies indicated that nortriptyline improved cessation rates over placebo after 6 months (RR, 2.03; 95% CI, 1.48–2.78), including limited evidence that bupropion HCI improved cessation rates over nortriptyline (RR, 1.30; 95% CI, 0.93–1.82).[55]
Lobeline (Bantron) is classified as a category III agent by the FDA, safe but not proven effective. This product is not recommended for use in any smoking cessation program due to its lack of efficacy.[74]
Pharmacotherapy Combinations and Adaptations
Strategies to enhance the effectiveness of pharmacotherapy for smoking cessation have been explored, including combining medications and adjusting dosages and/or treatment duration.[75] As noted previously, a recent meta-analysis concluded that combining a fast-acting NRT with the nicotine patch (i.e., combined NRT) resulted in higher 6-month cessation rates compared with the nicotine patch alone (RR, 1.27; 95% CI, 1.17–1.37). The analysis included moderate-certainty evidence (limited by imprecision) indicating that 21 mg patches are more effective than 14 mg patches (RR, 1.48; 95% CI, 1.06–2.08) but that 42 mg patches are just as effective as 21 mg (24-hour) patches (RR, 1.09; 95% CI, 0.93–1.29). A subset of studies tested the effect of preloading NRT before quit day versus starting NRT on the quit day. In that subset, there was moderate-certainty evidence, limited by risk of bias, of a positive effect of preloading NRT on abstinence (RR, 1.25; 95% CI, 1.08–1.44). There was no reliable evidence of an effect of duration of single or combined NRT use on abstinence.[51] In another meta-analysis, results (based on three trials) indicated that the combination of bupropion HCI and varenicline may result in higher 6-month cessation rates compared with varenicline alone (RR, 1.21; 95% CI, 0.95–1.55). However, there was insufficient evidence to suggest that combining bupropion HCI plus NRT increases smoking cessation rates over those of NRT alone (RR, 1.17; 95% CI, 0.95–1.44).[55]
A 2015 meta-analysis included randomized trials that compared the combination of varenicline and NRT therapy with varenicline alone. The analysis showed a statistically significant association with a smoking cessation benefit for the combination treatment, especially if a nicotine patch was given before treatment with varenicline.[76] In a subsequent double-blind, 2 × 2 factorial RCT, 1,251 individuals who smoked were randomly assigned to receive smoking cessation counseling and varenicline monotherapy for 12 weeks, varenicline plus NRT (patch) for 12 weeks, varenicline monotherapy for 24 weeks, or varenicline plus NRT for 24 weeks.[77] For the primary outcome of abstinence at 52 weeks, there was no significant interaction between medication type and medication duration (OR, 1.03; 95% CI, 0.91–1.17; P = .66). The abstinence rate was 24.8% for individuals randomly assigned to 24-week treatment duration versus 24.3% for those randomly assigned to 12-week treatment duration (risk difference, -0.4%; 95% CI, -5.2% to 4.3%; OR, 1.01; 95% CI, 0.89–1.15). The abstinence rate was 24.3% for individuals randomly assigned to varenicline-combination therapy versus 24.8% for those randomly assigned to varenicline monotherapy (risk difference, 0.4%; 95% CI, -4.3% to 5.2%; OR, 0.99; 95% CI, 0.87–1.12). Adverse effects across the four treatment groups included nausea (24.0%–30.9%) and insomnia (24.4%–30.5%). These findings do not support the addition of NRT to varenicline or the extension of varenicline or combination therapy beyond the standard 12 weeks.[77]
In a double-blind, placebo-controlled, sequential, multiple-assignment randomized trial (SMART), 490 individuals who smoked were randomly assigned to receive 6 weeks of varenicline (2 mg/d) or combined NRT (21 mg/d patch and 2 mg lozenges as needed) and smoking cessation counseling. After 6 weeks, abstainers continued their assigned medication and nonabstainers were randomly assigned again to continue the initially assigned medication at the initial dose, switch between varenicline and combined NRT at the initial dose, or increase the varenicline (3 mg/d) or combined NRT (42 mg/d patch) dose for an additional 6 weeks.[78]
At 12 weeks, the probability of abstinence for those initially randomly assigned to varenicline who were abstinent at 6 weeks and continued on treatment (not randomized again) was 72% (95% credible interval [Crl], 65%–78%) compared with 78% (95% Crl, 69%–85%) for those initially randomly assigned to combined NRT who were abstinent at 6 weeks and continued on treatment. The posterior probability of a nonzero difference between these two conditions was 88% (absolute risk difference [ARD], 6%; 95% CrI, -5% to 16%). The probability of abstinence at 12 weeks (end of treatment) for the individuals initially assigned to varenicline who were not abstinent at 6 weeks was 20% (95% CrI, 16%–26%) for those who increased their varenicline dosage, 0% for those who switched to combined NRT, and 3% (95% CrI, 1%–4%) for those who were assigned to the continued-varenicline treatment group (ARD, -3%; 95% CrI, -4% to -1%). There was a more than 99% posterior probability that continuing varenicline at the initial dosage was worse than switching to a higher dosage. Increasing the varenicline dosage had an ARD of 18% (95% CrI, 13%–24%) and a more than 99% posterior probability of conferring benefit. The probability of abstinence at 12 weeks for the individuals initially assigned to combined NRT who were not abstinent at 6 weeks was 8% (95% CrI, 6%–10%) for those who continued at the initial dosage, 14% (95% CrI, 10%–18%) for those who increased their dosage, and 14% (95% CrI, 10%–18%) for those who switched to varenicline (ARD, 6%; 95% CrI, 6%–11%). There was a more than 99% posterior probability that either strategy conferred benefit over continuing at the initial dosage. The secondary outcome of continuous abstinence at 6-months post-quit indicated that only increased dosages of varenicline and combined NRT provided benefit over continuation of the initial treatment dosages. Relative to continuing the same medication, there was no evidence indicating an increased risk of adverse events associated with the dosage increases for either medication. Additionally, no major differences in treatment adherence were reported between treatment groups.
In summary, these results suggest that individuals who are not able to abstain from smoking after initial treatment with varenicline benefit most from increasing the varenicline dose. For the individuals who continue to smoke after initial treatment with combined NRT, switching to varenicline or increasing the dose of combined NRT resulted in similar end-of-treatment abstinence probabilities. The secondary outcome of continuous abstinence at 6 months favored the dose-increase conditions for both varenicline and combined NRT, relative to continuation.[78]
On the other hand, in an RCT of 392 Black adults who smoked daily, switching from the nicotine patch to varenicline at 2 weeks or to bupropion HCI plus the nicotine patch at 6 weeks (adapted care) for individuals who did not quit smoking at those respective time points did not significantly improve abstinence rates, compared with standard treatment with the nicotine patch at 12 weeks (17.4% vs. 11.7%; OR, 1.58; 95% CI, 0.89–2.80; P = .12), 18 weeks (16.3% vs. 15.8%; OR, 1.04; 95% CI, 0.61–1.78; P = .89), or 26 weeks (12.2% vs. 13.3%; OR, 0.91; 95% CI, 0.50–1.65; P = .76).[79] The results also indicated that those who quit smoking within the first 2 weeks of treatment were significantly more likely to be abstinent at subsequent assessment points. However, the overall study abstinence rates were lower than those found in similar studies that included Black adults who were using the nicotine patch for smoking cessation.[80,81]
Smoking Reduction
Among smokers who are interested in quitting but not ready to make an immediate quit attempt, gradually decreasing the number of cigarettes smoked per day leading up to a quit attempt may prove to be a viable intervention strategy. This reduce to quit approach was tested in the context of an RCT. In this study, both the intervention group and control group received counseling, with the goals of reducing the number of cigarettes smoked per day by 75% or greater by week 8 and to quit smoking entirely by week 12.[82] The intervention group (n = 760) also received smoking cessation pharmacotherapy (varenicline at a maintenance dose of 1 mg bid for 24 weeks), whereas the control group (n = 750) received placebo tablets. For the primary end point of self-reported smoking abstinence during weeks 15 through 24, a statistically significant RD of 25.2% (varenicline group, 32.1% vs. placebo group, 6.9%; 95% CI, 21.4%–29.0%) was observed. The clinical significance of this finding is that it provides evidence of benefit for a pharmacotherapy-enhanced intervention aimed to motivate smokers who are interested in quitting, but not yet ready to quit, to start by cutting down on the number of cigarettes per day as a lead-in to a subsequent quit attempt.
For a smoker who wants to quit, an important practical question is whether a quit attempt is more likely to successfully result in smoking cessation if it involves abruptly stopping smoking or gradually decreasing the number of cigarettes smoked per day leading up to a quit attempt. U.S. evidence-based guidelines recommend abrupt quitting as the preferred approach,[83] but guidelines from other countries vary on this matter. To directly test this question, 697 smokers who wanted to quit were recruited from 31 primary care clinics in England, and randomly assigned to either a gradual or abrupt smoking cessation intervention.[84] In this noninferiority trial, both groups were provided with access to NRT during the two weeks before the planned quit date. In the gradual cessation group, plans were made to cut down the number of cigarettes per day by 75% by the planned quit date. However, the abrupt cessation group was advised to follow usual smoking patterns until stopping smoking entirely on the planned quit date. Both groups were provided with NRT after the quit date and throughout the trial. For the primary end point of prolonged validated smoking abstinence at 4 weeks, the gradual cessation arm was less likely to quit smoking than the abrupt cessation arm (39.2% vs. 49.0%); the difference was statistically significant (RD, -9.8%; 95% CI, 2.5%–17.1%). The statistically significantly lower likelihood of smoking cessation in the gradual versus abrupt intervention arms persisted during follow-up at 8 weeks (29.2% vs. 36.6%; RD, -7.4%; 95% CI, 0.4%–14.3%) and 6 months (15.5% vs. 22.0%; RD, -6.5%; 95% CI, 0.7%–12.2%). Baseline patient preferences for a gradual or abrupt quit attempt indicated that smokers who preferred the gradual quitting approach had a lower likelihood of smoking abstinence at 4 weeks (38% vs. 52%), suggesting that patient preferences for these methods may be a marker for other factors associated with successful quitting, such as motivation to quit. However, even when stratified by baseline patient preferences, the gradual cessation method resulted in lower likelihood of cessation both among those who preferred the gradual approach (34.6% vs. 42.0%) and those who preferred the abrupt approach (45.8% vs. 58.1%). The overall clinical significance of this study is that it provides evidence that in the setting of a pharmacotherapy-aided quit attempt among smokers interested in quitting, quitting abruptly is a more effective smoking cessation strategy than gradually cutting down on the number of cigarettes smoked before making a quit attempt. This result holds true regardless of smoker preferences in methods. A quit attempt regardless of method should never be discouraged, but abrupt cessation appears to be the most effective strategy. In this context, abrupt cessation is distinct from making an unaided quit attempt (i.e., quitting “cold turkey”).[85]
A systematic review of this topic revealed substantial heterogeneity in the results across studies, but the results showed that gradual cessation was associated with a 6% lower likelihood of smoking cessation than abrupt cessation, although this finding was not statistically significant (RR, 0.94; 95% CI, 0.79–1.13).[85] In an updated review of 51 trials that included more than 22,000 participants, the authors concluded, with moderate-certainty evidence, that long-term (≥ 6 months) abstinence rates did not differ in participants who were randomly assigned to either a gradual cessation intervention or an abrupt quitting intervention (RR, 1.01; 95% CI, 0.87–1.17; I2 = 29%; 22 studies, 9,219 participants).[86] When comparing the effects of a gradual cessation intervention with no smoking cessation intervention on abstinence rates, the authors reported low-certainty evidence (limited by inconsistency, imprecision, and risk of bias) that was inconclusive (RR, 1.74; 95% CI, 0.90–3.38; I2 = 45%; 6 studies, 1,599 participants). The authors also reported low-certainty evidence that suggested gradual reduction methods may be more effective when combined with pharmacotherapy (RR, 1.68; 95% CI, 1.09–2.58; I2 = 78%; 11 studies, 8,636 participants). A subgroup analysis of these 11 studies reported the same conclusions, with moderate-certainty evidence, specifically when fast-acting NRTs or varenicline was used as pharmacotherapy (P < .001, I2 = 80% for subgroup differences).[86]
Among dependent smokers, complete abstinence from smoking is the ultimate goal. Even in instances when complete abstinence from smoking is not achieved, smoking cessation pharmacotherapies may benefit individual health—and ultimately the public’s health—if the smoker reduces the number of cigarettes smoked. The relationship between cigarette smoking and lung cancer, and other smoking-associated malignancies, is strongly dose-dependent. Thus, an individual smoker who is unable to achieve abstinence or who is not motivated to quit smoking may benefit by using pharmacotherapies (or other means) to reduce the number of cigarettes smoked per day. NRT has thus generated attention as a viable means of harm reduction. In studies that included smokers who were not trying to quit and were randomly assigned to receive either NRT or placebo, a greater proportion of those who received NRT reduced the number of cigarettes per day, compared with placebo.[87,88] However, the impact of NRT on smoking reduction appears not to be sustained in the long run.[89] Less evidence is available for bupropion HCI, varenicline, and psychosocial interventions as a means of harm reduction. A potential problem with such a harm reduction strategy would be if it prevented cessation among smokers who would have otherwise quit smoking. Evidence shows that smoking reduction is actually associated with increased likelihood of future cessation.[88,90] Another potential negative aspect of harm reduction would be if smokers reduced the number of cigarettes smoked per day but modified the way the cigarettes were smoked in such a way that exposure to tobacco toxins was not actually reduced (e.g., by inhaling more deeply). Compensatory behaviors such as inhaling more deeply or smoking more of a cigarette are attempts by the smoker to try to maintain nicotine levels, so the use of supplemental NRT presumably safeguards against this. Evidence from studies of smoking reduction with NRT that measured smoking biomarkers indicates that compensation occurs, but not to such an extent that it would be expected to outweigh the reduction in exposure from the reduced number of cigarettes per day.[87]
School-Based Interventions
School-based interventions alone have not demonstrated a long-term impact on smoking prevention.[91] One of the highest-quality studies was a large randomized trial in which children received a theory-based program that incorporated various social-influence approaches from grade 3 through grade 12. There was no difference in smoking outcomes observed either at grade 12 or at 2 years after high school between school districts who received the intervention and those in the control arm.[92]
Community Intervention Trial for Smoking Cessation (COMMIT)
The Community Intervention Trial for Smoking Cessation (COMMIT) was a National Cancer Institute–funded, large-scale study to assess a combination of community-based interventions designed to help smokers cease using tobacco. COMMIT involved 11 matched pairs of communities in North America, which were randomly assigned to an arm offering an active community-wide intervention or a control arm (no active intervention).[93] The 4-year intervention included messaging through existing media channels, major community organizations, and social institutions capable of influencing smoking behavior in large groups of people. The interventions were implemented in each community through a local community board that provided oversight and management of COMMIT activities.
In COMMIT, there was no difference in the mean quit rate of heavy smokers in the intervention communities (18.0%), compared with the control communities (18.7%). The difference in light-to-moderate smoker quit rates were statistically significant: averages of 30.6% for the intervention communities and 27.5% for the control communities (P = .004). Although no significant differences in quit rates between the sexes were observed, less-educated light-to-moderate smokers were more responsive to the intervention than were college-educated light-to-moderate smokers.[94,95]
A Changing Marketplace for Tobacco Products and Nicotine-Delivery Devices
The expansion in the marketplace of tobacco products and devices that deliver nicotine poses new challenges to tobacco control.[96–100] Examples of nontraditional tobacco products in the U.S. market include small cigars, water pipe tobacco smoking (hookah), and new types of flavored, smokeless tobacco products modeled after Swedish snus. Prominent among non–tobacco-containing nicotine delivery devices are electronic cigarettes (or e-cigarettes) that have experienced a rapid upsurge in use and are now marketed by the major U.S. tobacco companies.[96,97] Monitoring this expansion in products, how the products are used (e.g., product switching, multiple use, and use for tobacco cigarette smoking cessation), and the harms and benefits associated with their use compared with the use of tobacco cigarettes is critical to the development of more effective tobacco control strategies.
Research to determine the potential risks and benefits of these new products is emerging, and initial findings are mixed.[101,102] The potential benefits of e-cigarettes as a smoking cessation aid for adult smokers is further complicated by two additional factors. First, there has been a marked increase in the use of e-cigarettes by adolescents, with current (past 30 days) e-cigarette use by high school seniors rising dramatically over the last 3 years, to 27.5% in 2019.[103] Second, the product has evolved rapidly, with newer electronic nicotine delivery systems, such as JUUL, more quickly and effectively delivering nicotine to the lungs and more closely mimicking cigarettes in terms of their pharmacokinetics.
In one study, 886 adults who attended the U.K. National Health Service stop-smoking services were randomly assigned to either starter packs of nicotine replacement medication or e-cigarettes. At 1 year, biochemically confirmed abstinence was 18.0% in the e-cigarette group compared with 9.9% in the nicotine-replacement group (P < .001). However, at 1 year, 80% of abstinent e-cigarette users were still using e-cigarettes, compared with 9% of abstinent nicotine-replacement medication users still using their products.[104] In contrast, a recent pragmatic trial randomly assigned smokers who were employed at 54 companies to access one of four interventions, which included usual care (information and motivational text messages), FDA-approved cessation medications, e-cigarettes, and financial incentives. The authors found that financial incentives added to free FDA-approved cessation medications resulted in higher quit rates than cessation medications alone. Among smokers who received usual care, the addition of free cessation medications or e-cigarettes did not provide an added benefit.[105]
Evidence suggests that cessation interventions delivered during children’s pediatric visits to parents who smoked boost cessation rates.[83] A recent cluster randomized clinical trial [106] demonstrated higher quit rates 2 years after cessation interventions were delivered during pediatric visits, although there were a limited number of clusters (n = 10) included in the trial.
References
Le TTT, Méndez D, Warner KE: New Estimates of Smoking-Attributable Mortality in the U.S. From 2020 Through 2035. Am J Prev Med 66 (5): 877-882, 2024. [PUBMED Abstract]
U.S. Department of Health and Human Services: The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. U.S. Department of Health and Human Services, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. Also available online. Last accessed December 30, 2024.
Centers for Disease Control and Prevention (CDC): Smoking-attributable mortality, years of potential life lost, and productivity losses–United States, 2000-2004. MMWR Morb Mortal Wkly Rep 57 (45): 1226-8, 2008. [PUBMED Abstract]
American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
Centers for Disease Control and Prevention: Targeting Tobacco Use: The Nation’s Leading Cause of Death 2005. CDC, 2005.
Ontario Task Force on the Primary Prevention of Cancer: Recommendations for the Primary Prevention of Cancer. Queen’s Printer for Ontario, 1995.
Cinciripini PM, Hecht SS, Henningfield JE, et al.: Tobacco addiction: implications for treatment and cancer prevention. J Natl Cancer Inst 89 (24): 1852-67, 1997. [PUBMED Abstract]
Finette BA, O’Neill JP, Vacek PM, et al.: Gene mutations with characteristic deletions in cord blood T lymphocytes associated with passive maternal exposure to tobacco smoke. Nat Med 4 (10): 1144-51, 1998. [PUBMED Abstract]
Benowitz NL: Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol Rev 18 (2): 188-204, 1996. [PUBMED Abstract]
Hecht SS: Human urinary carcinogen metabolites: biomarkers for investigating tobacco and cancer. Carcinogenesis 23 (6): 907-22, 2002. [PUBMED Abstract]
U.S. Department of Health and Human Services: The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2006. Also available online. Last accessed February 20, 2025.
Cornelius ME, Loretan CG, Jamal A, et al.: Tobacco Product Use Among Adults – United States, 2021. MMWR Morb Mortal Wkly Rep 72 (18): 475-483, 2023. [PUBMED Abstract]
Youth and Tobacco Use. Atlanta, Ga: Centers for Disease Control and Prevention, 2015. Available online. Last accessed February 20, 2025.
Jemal A, Thun MJ, Ries LA, et al.: Annual report to the nation on the status of cancer, 1975-2005, featuring trends in lung cancer, tobacco use, and tobacco control. J Natl Cancer Inst 100 (23): 1672-94, 2008. [PUBMED Abstract]
Johnston LD, O’Malley PM, Bachman JG: Monitoring the Future: National Survey Results on Drug Use, 1975-2001. Volume I: Secondary School Students. National Institute on Drug Abuse, 2002. NIH Pub. No. 02-5106. Also available online. Last accessed February 20, 2025.
U.S. Preventive Services Task Force: Guide to Clinical Preventive Services: Report of the U.S. Preventive Services Task Force. 2nd ed. Williams & Wilkins, 1996.
American Cancer Society: Cancer Prevention & Early Detection Facts & Figures 2023-2024. American Cancer Society, 2024. Available online. Last accessed February 20, 2025.
Schoenborn CA, Adams PF, Peregoy JA: Health behaviors of adults: United States, 2008-2010. Vital Health Stat 10 (257): 1-184, 2013. [PUBMED Abstract]
U.S. Department of Health and Human Services: The Health Benefits of Smoking Cessation. A Report of the Surgeon General. U.S. Department of Health and Human Services, 1990. DHHS Publ No. (CDC) 90-8416.
The Health Consequences of Smoking: A Report of the Surgeon General. U.S. Department of Health and Human Services, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004. Also available online. Last accessed April 9, 2025.
U.S. Department of Health and Human Services: Smoking Cessation: A Report of the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2020. Also available online. Last accessed February 20, 2025.
Anthonisen NR, Skeans MA, Wise RA, et al.: The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med 142 (4): 233-9, 2005. [PUBMED Abstract]
Wingo PA, Ries LA, Giovino GA, et al.: Annual report to the nation on the status of cancer, 1973-1996, with a special section on lung cancer and tobacco smoking. J Natl Cancer Inst 91 (8): 675-90, 1999. [PUBMED Abstract]
Koh HK: The end of the “tobacco and cancer” century. J Natl Cancer Inst 91 (8): 660-1, 1999. [PUBMED Abstract]
Hartmann-Boyce J, Chepkin SC, Ye W, et al.: Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev 5 (5): CD000146, 2018. [PUBMED Abstract]
Hartmann-Boyce J, Livingstone-Banks J, Ordóñez-Mena JM, et al.: Behavioural interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev 1: CD013229, 2021. [PUBMED Abstract]
Stead LF, Buitrago D, Preciado N, et al.: Physician advice for smoking cessation. Cochrane Database Syst Rev 2013 (5): CD000165, 2013. [PUBMED Abstract]
Fiore MC, Jaén CR, Baker TB: Treating Tobacco Use and Dependence [Electronic Resource] : 2008 Update. Rockville, Md: Public Health Service, U.S. Department of Health and Human Services, 2008. Available online. Last accessed February 20, 2025.
Glynn TJ, Manley MW, Pechacek TF: Physician-initiated smoking cessation program: the National Cancer Institute trials. Prog Clin Biol Res 339: 11-25, 1990. [PUBMED Abstract]
Krist AH, Davidson KW, Mangione CM, et al.: Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Persons: US Preventive Services Task Force Recommendation Statement. JAMA 325 (3): 265-279, 2021. [PUBMED Abstract]
Patnode CD, Henderson JT, Coppola EL, et al.: Interventions for Tobacco Cessation in Adults, Including Pregnant Persons: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 325 (3): 280-298, 2021. [PUBMED Abstract]
World Health Organization: WHO Clinical Treatment Guideline for Tobacco Cessation in Adults. Geneva, Switzerland: World Health Organization, 2024. Available online. Last accessed February 7, 2025.
Barua RS, Rigotti NA, Benowitz NL, et al.: 2018 ACC Expert Consensus Decision Pathway on Tobacco Cessation Treatment: A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 72 (25): 3332-3365, 2018. [PUBMED Abstract]
Leone FT, Zhang Y, Evers-Casey S, et al.: Initiating Pharmacologic Treatment in Tobacco-Dependent Adults. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med 202 (2): e5-e31, 2020. [PUBMED Abstract]
Emmons KM, Puleo E, Park E, et al.: Peer-delivered smoking counseling for childhood cancer survivors increases rate of cessation: the partnership for health study. J Clin Oncol 23 (27): 6516-23, 2005. [PUBMED Abstract]
Shields PG, Bierut L, Arenberg D, et al.: Smoking Cessation, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 21 (3): 297-322, 2023. [PUBMED Abstract]
Halpern SD, French B, Small DS, et al.: Randomized trial of four financial-incentive programs for smoking cessation. N Engl J Med 372 (22): 2108-17, 2015. [PUBMED Abstract]
Sunstein CR: Nudging smokers. N Engl J Med 372 (22): 2150-1, 2015. [PUBMED Abstract]
Okuyemi KS, Ahluwalia JS, Harris KJ: Pharmacotherapy of smoking cessation. Arch Fam Med 9 (3): 270-81, 2000. [PUBMED Abstract]
Fiore MC, Bailey WC, Cohen SJ, et al.: Smoking Cessation: Clinical Practice Guideline No 18. US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research, 1996. AHCPR Publ No 96-0692.
Tang JL, Law M, Wald N: How effective is nicotine replacement therapy in helping people to stop smoking? BMJ 308 (6920): 21-6, 1994. [PUBMED Abstract]
Hurt RD, Sachs DP, Glover ED, et al.: A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med 337 (17): 1195-202, 1997. [PUBMED Abstract]
Jorenby DE, Leischow SJ, Nides MA, et al.: A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med 340 (9): 685-91, 1999. [PUBMED Abstract]
Hughes JR, Goldstein MG, Hurt RD, et al.: Recent advances in the pharmacotherapy of smoking. JAMA 281 (1): 72-6, 1999. [PUBMED Abstract]
Cahill K, Stevens S, Perera R, et al.: Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev 5: CD009329, 2013. [PUBMED Abstract]
Ray R, Schnoll RA, Lerman C: Pharmacogenetics and smoking cessation with nicotine replacement therapy. CNS Drugs 21 (7): 525-33, 2007. [PUBMED Abstract]
Fincham JE: Smoking cessation products. In: Covington TR, Berardi RR, Young LL, et al., eds.: Handbook of Nonprescription Drugs. 11th ed. American Pharmaceutical Association, 1996, pp 715-723.
Mills EJ, Wu P, Lockhart I, et al.: Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis 8 (1): 8, 2010. [PUBMED Abstract]
Theodoulou A, Chepkin SC, Ye W, et al.: Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 6 (6): CD013308, 2023. [PUBMED Abstract]
Baker TB, Piper ME, Stein JH, et al.: Effects of Nicotine Patch vs Varenicline vs Combination Nicotine Replacement Therapy on Smoking Cessation at 26 Weeks: A Randomized Clinical Trial. JAMA 315 (4): 371-9, 2016. [PUBMED Abstract]
Schnoll RA, Patterson F, Wileyto EP, et al.: Effectiveness of extended-duration transdermal nicotine therapy: a randomized trial. Ann Intern Med 152 (3): 144-51, 2010. [PUBMED Abstract]
Tønnesen P, Paoletti P, Gustavsson G, et al.: Higher dosage nicotine patches increase one-year smoking cessation rates: results from the European CEASE trial. Collaborative European Anti-Smoking Evaluation. European Respiratory Society. Eur Respir J 13 (2): 238-46, 1999. [PUBMED Abstract]
Hajizadeh A, Howes S, Theodoulou A, et al.: Antidepressants for smoking cessation. Cochrane Database Syst Rev 5 (5): CD000031, 2023. [PUBMED Abstract]
Jorenby DE, Hays JT, Rigotti NA, et al.: Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA 296 (1): 56-63, 2006. [PUBMED Abstract]
Gonzales D, Rennard SI, Nides M, et al.: Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA 296 (1): 47-55, 2006. [PUBMED Abstract]
Aubin HJ, Bobak A, Britton JR, et al.: Varenicline versus transdermal nicotine patch for smoking cessation: results from a randomised open-label trial. Thorax 63 (8): 717-24, 2008. [PUBMED Abstract]
Livingstone-Banks J, Fanshawe TR, Thomas KH, et al.: Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev 5 (5): CD006103, 2023. [PUBMED Abstract]
U.S. Food and Drug Administration: Information for Healthcare Professionals: Varenicline (Marketed as Chantix) and Bupropion (Marketed as Zyban, Wellbutrin, and Generics). Rockville, Md: U.S. Food and Drug Administration, 2009. Archived page available online. Last accessed February 20, 2025.
Anthenelli RM, Benowitz NL, West R, et al.: Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet 387 (10037): 2507-20, 2016. [PUBMED Abstract]
Thomas KH, Martin RM, Knipe DW, et al.: Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ 350: h1109, 2015. [PUBMED Abstract]
Gibbons RD, Mann JJ: Varenicline, smoking cessation, and neuropsychiatric adverse events. Am J Psychiatry 170 (12): 1460-7, 2013. [PUBMED Abstract]
U.S. Food and Drug Administration: FDA Drug Safety Communication: FDA Revises Description of Mental Health Side Effects of the Stop-Smoking Medicines Chantix (varenicline) and Zyban (bupropion) to Reflect Clinical Trial Findings. U.S. Food and Drug Administration, 2016. Available online. Last accessed February 20, 2025.
Singh S, Loke YK, Spangler JG, et al.: Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ 183 (12): 1359-66, 2011. [PUBMED Abstract]
Benowitz NL, Pipe A, West R, et al.: Cardiovascular Safety of Varenicline, Bupropion, and Nicotine Patch in Smokers: A Randomized Clinical Trial. JAMA Intern Med 178 (5): 622-631, 2018. [PUBMED Abstract]
Drug Facts and Comparisons. 54th ed. Facts and Comparisons, 2000.
Hajek P, McRobbie H, Myers K: Efficacy of cytisine in helping smokers quit: systematic review and meta-analysis. Thorax 68 (11): 1037-42, 2013. [PUBMED Abstract]
Walker N, Howe C, Glover M, et al.: Cytisine versus nicotine for smoking cessation. N Engl J Med 371 (25): 2353-62, 2014. [PUBMED Abstract]
Oreskovic T, Percac-Lima S, Ashburner JM, et al.: Cytisine Versus Varenicline for Smoking Cessation in a Primary Care Setting: A Randomized Non-inferiority Trial. Nicotine Tob Res 25 (9): 1547-1555, 2023. [PUBMED Abstract]
Wagena EJ, Knipschild P, Zeegers MP: Should nortriptyline be used as a first-line aid to help smokers quit? Results from a systematic review and meta-analysis. Addiction 100 (3): 317-26, 2005. [PUBMED Abstract]
Drug Facts and Comparisons. Facts and Comparisons, 1998.
Patnode CD, Henderson JT, Melnikow J, et al.: Interventions for Tobacco Cessation in Adults, Including Pregnant Women: an Evidence Update for the U.S. Preventive Services Task Force. Rockville, Md: Agency for Healthcare Research and Quality, 2021. Also available online. Last accessed February 20, 2025.
Chang PH, Chiang CH, Ho WC, et al.: Combination therapy of varenicline with nicotine replacement therapy is better than varenicline alone: a systematic review and meta-analysis of randomized controlled trials. BMC Public Health 15: 689, 2015. [PUBMED Abstract]
Baker TB, Piper ME, Smith SS, et al.: Effects of Combined Varenicline With Nicotine Patch and of Extended Treatment Duration on Smoking Cessation: A Randomized Clinical Trial. JAMA 326 (15): 1485-1493, 2021. [PUBMED Abstract]
Cinciripini PM, Green CE, Shete S, et al.: Smoking Cessation After Initial Treatment Failure With Varenicline or Nicotine Replacement: A Randomized Clinical Trial. JAMA 331 (20): 1722-1731, 2024. [PUBMED Abstract]
Nollen NL, Ahluwalia JS, Mayo MS, et al.: Multiple Pharmacotherapy Adaptations for Smoking Cessation Based on Treatment Response in Black Adults Who Smoke: A Randomized Clinical Trial. JAMA Netw Open 6 (6): e2317895, 2023. [PUBMED Abstract]
Nollen NL, Ahluwalia JS, Sanderson Cox L, et al.: Assessment of Racial Differences in Pharmacotherapy Efficacy for Smoking Cessation: Secondary Analysis of the EAGLES Randomized Clinical Trial. JAMA Netw Open 4 (1): e2032053, 2021. [PUBMED Abstract]
Ahluwalia JS, McNagny SE, Clark WS: Smoking cessation among inner-city African Americans using the nicotine transdermal patch. J Gen Intern Med 13 (1): 1-8, 1998. [PUBMED Abstract]
Ebbert JO, Hughes JR, West RJ, et al.: Effect of varenicline on smoking cessation through smoking reduction: a randomized clinical trial. JAMA 313 (7): 687-94, 2015. [PUBMED Abstract]
Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff: A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med 35 (2): 158-76, 2008. [PUBMED Abstract]
Lindson-Hawley N, Banting M, West R, et al.: Gradual Versus Abrupt Smoking Cessation: A Randomized, Controlled Noninferiority Trial. Ann Intern Med 164 (9): 585-92, 2016. [PUBMED Abstract]
Lindson-Hawley N, Aveyard P, Hughes JR: Gradual reduction vs abrupt cessation as a smoking cessation strategy in smokers who want to quit. JAMA 310 (1): 91-2, 2013. [PUBMED Abstract]
Lindson N, Klemperer E, Hong B, et al.: Smoking reduction interventions for smoking cessation. Cochrane Database Syst Rev 9 (9): CD013183, 2019. [PUBMED Abstract]
Hughes JR, Carpenter MJ: The feasibility of smoking reduction: an update. Addiction 100 (8): 1074-89, 2005. [PUBMED Abstract]
Batra A, Klingler K, Landfeldt B, et al.: Smoking reduction treatment with 4-mg nicotine gum: a double-blind, randomized, placebo-controlled study. Clin Pharmacol Ther 78 (6): 689-96, 2005. [PUBMED Abstract]
Etter JF, Laszlo E: Postintervention effect of nicotine replacement therapy for smoking reduction: a randomized trial with a 5-year follow-up. J Clin Psychopharmacol 27 (2): 151-5, 2007. [PUBMED Abstract]
Hughes JR, Carpenter MJ: Does smoking reduction increase future cessation and decrease disease risk? A qualitative review. Nicotine Tob Res 8 (6): 739-49, 2006. [PUBMED Abstract]
Thomas R, Perera R: School-based programmes for preventing smoking. Cochrane Database Syst Rev 3: CD001293, 2006. [PUBMED Abstract]
Peterson AV, Kealey KA, Mann SL, et al.: Hutchinson Smoking Prevention Project: long-term randomized trial in school-based tobacco use prevention–results on smoking. J Natl Cancer Inst 92 (24): 1979-91, 2000. [PUBMED Abstract]
Community Intervention Trial for Smoking Cessation (COMMIT): summary of design and intervention. COMMIT Research Group. J Natl Cancer Inst 83 (22): 1620-8, 1991. [PUBMED Abstract]
Community Intervention Trial for Smoking Cessation (COMMIT): I. cohort results from a four-year community intervention. Am J Public Health 85 (2): 183-92, 1995. [PUBMED Abstract]
Community intervention trial for smoking cessation (COMMIT): II. Changes in adult cigarette smoking prevalence. Am J Public Health 85 (2): 193-200, 1995. [PUBMED Abstract]
Popova L, Ling PM: Alternative tobacco product use and smoking cessation: a national study. Am J Public Health 103 (5): 923-30, 2013. [PUBMED Abstract]
Kamerow D: Big Tobacco lights up e-cigarettes. BMJ 346: f3418, 2013. [PUBMED Abstract]
Schuster RM, Hertel AW, Mermelstein R: Cigar, cigarillo, and little cigar use among current cigarette-smoking adolescents. Nicotine Tob Res 15 (5): 925-31, 2013. [PUBMED Abstract]
Jawad M, McEwen A, McNeill A, et al.: To what extent should waterpipe tobacco smoking become a public health priority? Addiction 108 (11): 1873-84, 2013. [PUBMED Abstract]
Centers for Disease Control and Prevention (CDC): Consumption of cigarettes and combustible tobacco–United States, 2000-2011. MMWR Morb Mortal Wkly Rep 61 (30): 565-9, 2012. [PUBMED Abstract]
Bullen C, Howe C, Laugesen M, et al.: Electronic cigarettes for smoking cessation: a randomised controlled trial. Lancet 382 (9905): 1629-37, 2013. [PUBMED Abstract]
National Academies of Sciences, Engineering, and Medicine. Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems: Public Health Consequences of E-Cigarettes. The National Academies Press, 2018. Also available online. Last accessed February 20, 2025.
Cullen KA, Gentzke AS, Sawdey MD, et al.: e-Cigarette Use Among Youth in the United States, 2019. JAMA 322 (21): 2095-2103, 2019. [PUBMED Abstract]
Hajek P, Phillips-Waller A, Przulj D, et al.: A Randomized Trial of E-Cigarettes versus Nicotine-Replacement Therapy. N Engl J Med 380 (7): 629-637, 2019. [PUBMED Abstract]
Halpern SD, Harhay MO, Saulsgiver K, et al.: A Pragmatic Trial of E-Cigarettes, Incentives, and Drugs for Smoking Cessation. N Engl J Med 378 (24): 2302-2310, 2018. [PUBMED Abstract]
Nabi-Burza E, Drehmer JE, Hipple Walters B, et al.: Treating Parents for Tobacco Use in the Pediatric Setting: The Clinical Effort Against Secondhand Smoke Exposure Cluster Randomized Clinical Trial. JAMA Pediatr 173 (10): 931-939, 2019. [PUBMED Abstract]
Latest Updates to This Summary (02/21/2025)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
This summary was comprehensively reviewed and extensively revised.
This summary is written and maintained by the PDQ Screening and Prevention Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® Cancer Information for Health Professionals pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the prevention and cessation of cigarette smoking and the control of tobacco use. It is intended as a resource to inform and assist clinicians in the care of their patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Screening and Prevention Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
be discussed at a meeting,
be cited with text, or
replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Screening and Prevention Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Cigarette Smoking. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: /causes-prevention/risk/tobacco/quit-smoking-hp-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389444]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Leaving ChemoPrescribe
You are now leaving ChemoPrescribe website.
To return to the website, click on the back arrow on your browser.